ICU · neurocritical-care
Acute Intermittent Porphyria — Comprehensive ICU Management
Also known as Acute intermittent porphyria · AIP · Acute porphyria · Porphobilinogen deaminase deficiency · HMBS deficiency · Acute neurovisceral porphyria · Port wine urine · Haem arginate
Acute intermittent porphyria (AIP) — autosomal dominant defect in porphobilinogen deaminase (PBGD/HMBS enzyme) in the haem biosynthesis pathway → accumulation of porphyrin precursors (ALA — aminolaevulinic acid, PBG — porphobilinogen) → neurotoxicity. Classic triad: ABDOMINAL PAIN (severe, persistent, out of proportion to examination — no peritonism) + NEUROLOGICAL symptoms (peripheral neuropathy, motor weakness, bulbar palsy, seizures) + PSYCHIATRIC symptoms (anxiety, hallucinations, paranoia). Urine turns DARK (port-wine/dark red) on standing or exposure to light (from porphobilinogen oxidation). Diagnosis: ELEVATED urinary porphobilinogen (PBG) and ALA (aminolaevulinic acid) — random spot urine (significantly elevated — 5-100x normal). Treatment: (1) IV HAEM ARGINATE 3 mg/kg once daily for 4 days (or haemin 3-4 mg/kg — reconstituted with human albumin — suppresses ALA synthase → reduces porphyrin precursor production), (2) CARBOHYDRATE LOADING (300-500 g/day glucose IV if haem arginate unavailable — inhibits ALA synthase), (3) STOP ALL PRECIPITATING DRUGS (barbiturates, sulfonamides, OCP, griseofulvin, rifampicin, phenytoin, carbamazepine, alcohol — check EVERY drug against the safe drug list), (4) SYMPTOMATIC: opiate analgesia (morphine/fentanyl — SAFE), antiemetics (ondansetron — SAFE; AVOID metoclopramide, phenothiazines), beta-blocker for tachycardia/hypertension (propranolol/labetalol — SAFE), levetiracetam for seizures (SAFE — AVOID barbiturates/phenytoin/valproate). ICU admission for: respiratory muscle weakness (motor neuropathy → ventilatory failure — like GBS), severe hyponatraemia (SIADH — common in acute porphyria), seizures, autonomic instability. Prognosis: acute attack resolves over days-weeks with treatment. Mortality 5-10% (from respiratory failure, seizures, arrhythmia).
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview
AIP is the "great mimicker" — it presents with abdominal pain (mimics surgical abdomen), motor neuropathy (mimics GBS), psychiatric symptoms (mimics psychosis), and SIADH (mimics brain pathology). The intensivist encounters AIP in three scenarios: (1) the patient with unexplained severe abdominal pain + neurological symptoms (the diagnostic challenge — many have had negative laparotomies before the diagnosis is made), (2) the patient with known AIP in acute attack (management of the attack + identifying the precipitant), (3) the patient with motor neuropathy and ventilatory failure (distinguishing from GBS — both cause ascending paralysis). The KEY: check urinary PBG/ALA in ANY patient with unexplained abdominal pain + neurological symptoms.[3][4]
Pathophysiology — the haem biosynthesis pathway
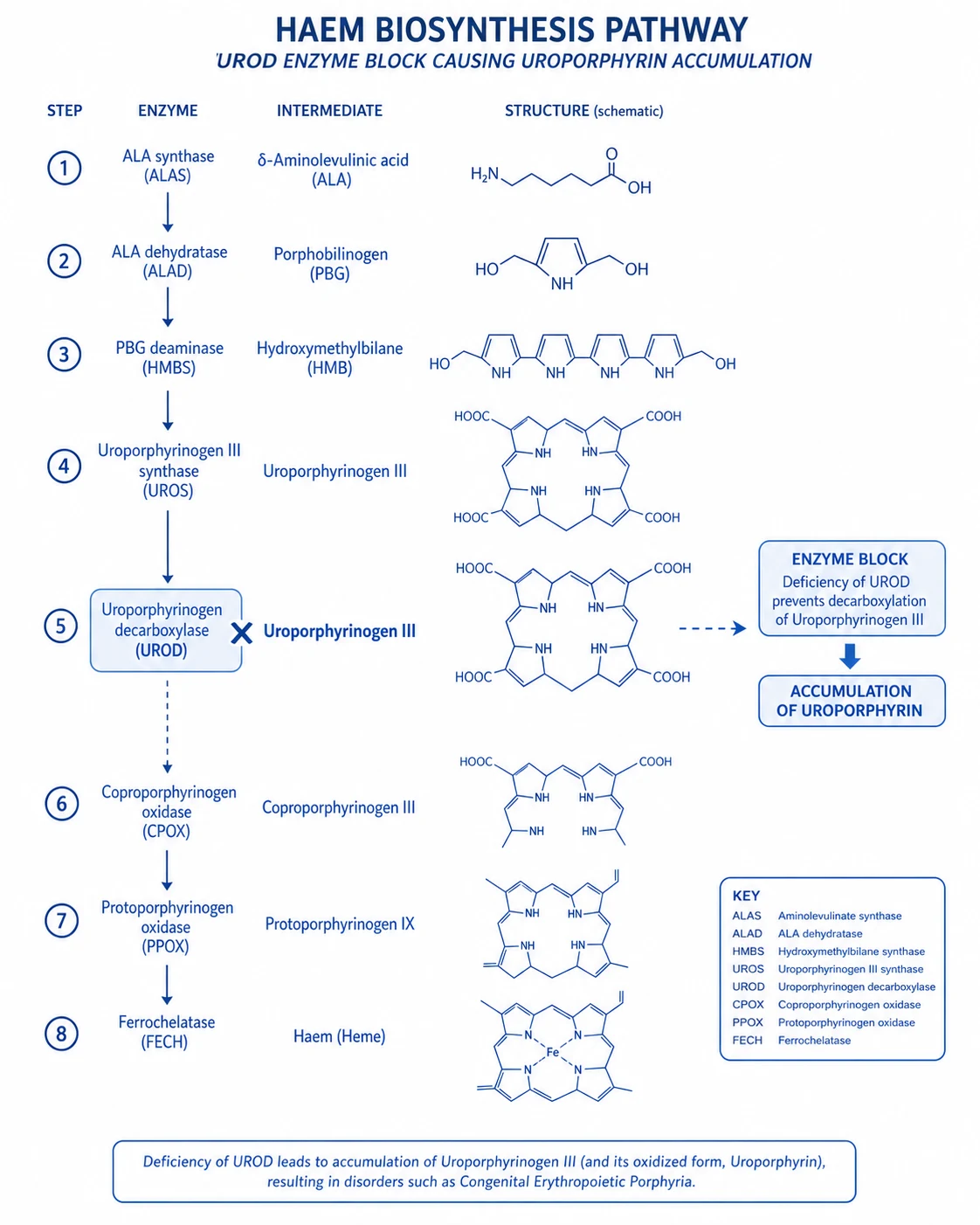
Haem is synthesised in every cell (for cytochromes, catalase, etc.) but primarily in bone marrow (haemoglobin) and liver (cytochrome P450). The pathway has 8 enzymatic steps, starting from glycine + succinyl-CoA → ALA (aminolaevulinic acid) → PBG (porphobilinogen) → hydroxymethylbilane → uroporphyrinogen → ... → haem.
[4]AIP = deficiency in step 3: porphobilinogen deaminase (PBGD, also called hydroxymethylbilane synthase — HMBS, or uroporphyrinogen I synthase). This is an autosomal dominant condition (HMBS gene on chromosome 11q23) with incomplete penetrance — most carriers NEVER have an attack (latent porphyria — 90% are asymptomatic). The attack is TRIGGERED by factors that increase hepatic ALA synthase (the rate-limiting and first enzyme of the pathway — ALAS1):[3]
[6]Clinical presentation — the neurovisceral triad
[4]Diagnosis — urinary PBG is the key
[6]Management — haem arginate and drug avoidance
[6]Clinical pearls
Red flags
Prognosis
[6]Key trials and evidence
Haem arginate for acute porphyria — systematic review (PMID 30198482)
Detailed haem arginate administration protocol
[4] [6]Detailed safe drug list for porphyria — the exam favourites
[4]The 4-step safe drug check protocol
[4]Molecular pathophysiology — the exam depth
The haem biosynthesis pathway has 8 enzymatic steps. In AIP, step 3 (porphobilinogen deaminase / hydroxymethylbilane synthase / HMBS) is deficient. The pathway:
[4]Glycine + Succinyl-CoA → [ALAS1 — rate-limiting, mitochondrial, feedback-inhibited by haem] → ALA → [ALAD] → PBG → [PBGD/HMBS — DEFICIENT in AIP] → hydroxymethylbilane → uroporphyrinogen III → ... → haem
[4]When PBGD is deficient: PBG accumulates → ALA accumulates (ALAS1 continues working because haem feedback is reduced — the pathway can't complete → less haem → less feedback inhibition → MORE ALA production → vicious cycle). ALA and PBG are NEUROTOXIC (mechanism: ALA structurally resembles GABA → may interfere with GABAergic neurotransmission → explains abdominal pain, neuropathy, psychiatric symptoms).
[4]Haem arginate breaks the cycle: exogenous haem → feedback inhibits ALAS1 → reduces ALA and PBG production → symptoms resolve.
[4]Glucose loading works by the same mechanism: glucose represses ALAS1 gene transcription (via carbohydrate response element in ALAS1 promoter) → reduces ALA production. But haem arginate is MORE effective and faster than glucose.
[4]Exam SAQ — densified leaf
10 minutes · 10 marks
In structured CICM/FFICM style: (1) define the core entity in one sentence; (2) list three immediate ICU priorities; (3) state two investigations that change management; (4) name one evidence landmark or guideline anchor; (5) give one fatal exam trap.
Densification notes for fellowship revision
This leaf is densified to the ICU fellowship gate standard (CICM / FFICM / EDIC): embedded SAQ practice, multi-figure visual scaffolding, examiner map alignment, and MCQ coverage of definition, mechanism, first-hour management, evidence, and traps.
[4]- Revision checkpoint 1: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 2: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 3: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 4: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 5: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 6: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 7: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 8: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
References
- [1]Besur S, et al. Acute Porphyrias. J Emerg Med, 2015.PMID 26159905
- [2]Stein PE, et al. Acute intermittent porphyria: fatal complications of treatment. Clin Med (Lond), 2012.PMID 22783787
- [3]Wang B, et al. Acute Hepatic Porphyrias: Review and Recent Progress. Hepatol Commun, 2019.PMID 30766957
- [4]Pischik E, et al. An update of clinical management of acute intermittent porphyria. Appl Clin Genet, 2015.PMID 26366103
- [5]Thunell S, et al. Guide to drug porphyrogenicity prediction and drug prescription in the acute porphyrias. Br J Clin Pharmacol, 2007.PMID 17578481
- [6]Anderson KE Acute hepatic porphyrias: Current diagnosis & management. Mol Genet Metab, 2019.PMID 31311713