ICU · Neurocritical care / seizures
Status Epilepticus & Refractory Status Epilepticus
Also known as Status epilepticus · Convulsive status epilepticus · Refractory status epilepticus · Super-refractory status epilepticus · Non-convulsive status epilepticus · ESETT · RAMPART · Anti-NMDA receptor encephalitis · Burst suppression
Status epilepticus (SE) is a continuous seizure lasting more than 5 minutes, or two or more seizures without full recovery between them — a neurological emergency where the longer the seizure lasts, the harder it becomes to terminate and the worse the outcome. First line is a benzodiazepine (lorazepam 4 mg IV or midazolam 10 mg IM). Second line is levetiracetam 60 mg/kg, fosphenytoin 20 mg PE/kg, or valproate 40 mg/kg (ESETT showed all three equivalent). Refractory SE (failure of first and second line) requires anaesthetic intubation with propofol, midazolam, ketamine, or thiopent infusions titrated to burst suppression on continuous EEG. Non-convulsive SE and autoimmune causes such as anti-NMDA receptor encephalitis must not be missed.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview & definition
Status epilepticus (SE) is a condition resulting either from the failure of the mechanisms responsible for seizure termination or from the initiation of mechanisms that lead to abnormally prolonged seizures — a continuous seizure lasting more than 5 minutes, or two or more discrete seizures between which there is incomplete recovery of consciousness. It is the most common medical neurological emergency, with an annual incidence of around 10 to 40 per 100,000, and carries a mortality of 10 to 30 per cent that rises sharply once the seizure becomes refractory.[5][7]
The ILAE operational definition (Trinka 2015) introduced two time points that translate the pathophysiology into a practical rule for the clinician. t1 is the time beyond which the seizure should be treated as continuous (the point at which the intrinsic seizure-terminating mechanisms fail): 5 minutes for the generalised convulsive SE. t2 is the time beyond which there is a risk of long-term consequences (the neuronal injury and the pharmacoresistance): 30 minutes for the generalised convulsive SE. The window between t1 and t2 — the 5 to 30 minute window — is the therapeutic window in which the seizure is most likely to respond and before the permanent harm accrues.[5]

Classification — the four stages of status epilepticus
Status epilepticus is classified along two axes: by semiology (convulsive vs non-convulsive, focal vs generalised) and by the response to treatment, which defines the four stages that drive the management ladder.[6]
Stages of status epilepticus (click each)
Refractory SE (RSE)
A seizure continuing despite a first-line benzodiazepine and a second-line antiepileptic. Treatment: anaesthetic intubation with a continuous infusion (propofol, midazolam, ketamine, or thiopent) titrated to burst suppression.
Pathophysiology
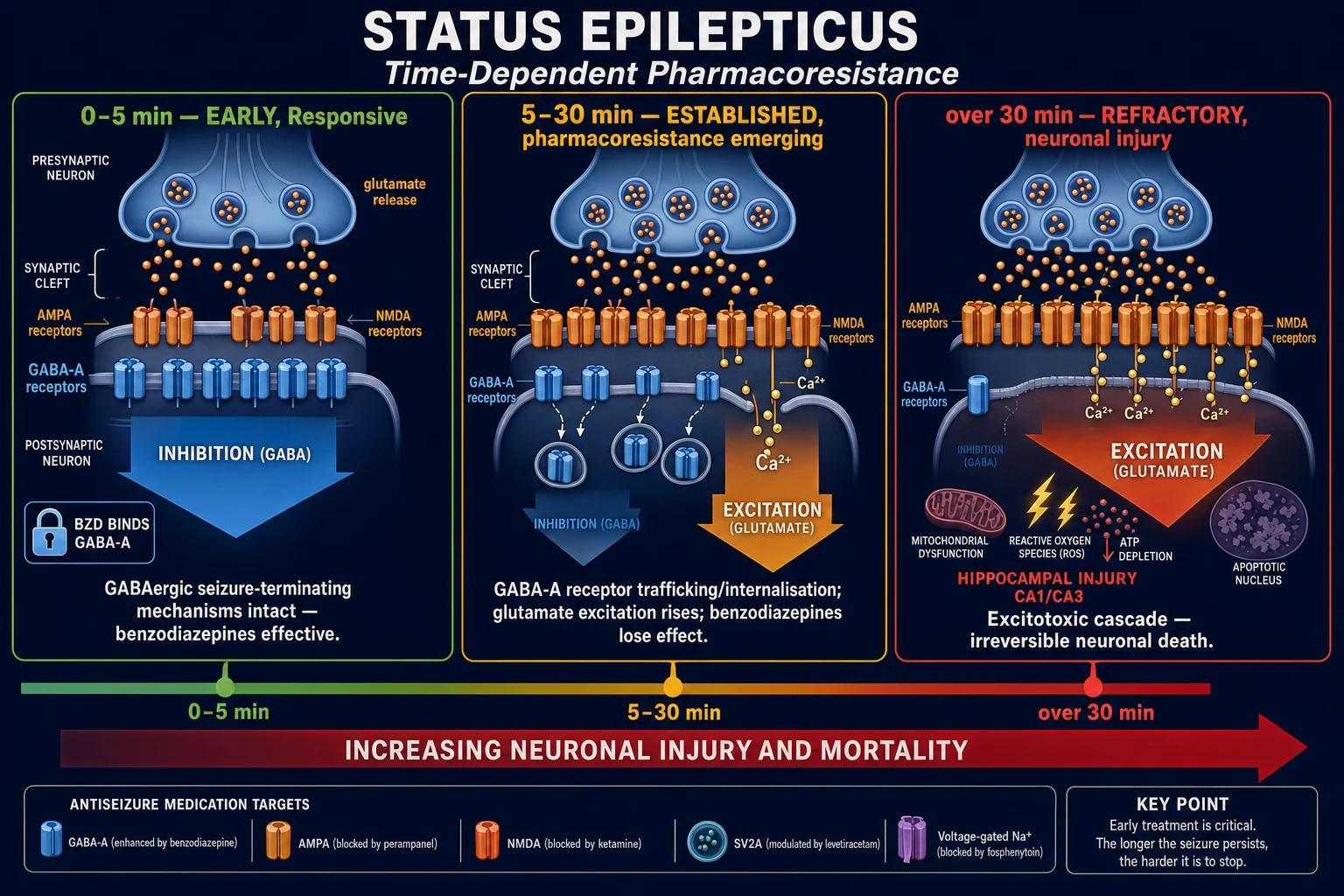
The seizure is sustained by a failure of the balance between the cortical excitation and the inhibition. The excitation is mediated by the glutamatergic NMDA and AMPA receptors; the inhibition by the GABA-A (fast, the benzodiazepine and the barbiturate target) and the GABA-B (slow, the baclofen target) receptors. Three pathophysiological processes run in parallel as the seizure continues:[5][6]
-
Receptor trafficking (the molecular pharmacoresistance). The sustained depolarisation causes the GABA-A receptors to be internalised from the synaptic membrane into the endosome, while the NMDA and AMPA receptors are trafficked to the surface. The result is that the inhibitory synapse is functionally weakened and the excitatory synapse strengthened — a self-reinforcing loop that makes the seizure increasingly resistant to the GABAergic drugs (the benzodiazepines, the barbiturates, the propofol) and increasingly amenable to the glutamate antagonists (the ketamine). This is the rationale for the late use of ketamine in the refractory and super-refractory SE. [1]
-
Failure of the seizure termination. The endogenous adenosine surge, the glial potassium buffering, and the neuronal Na-K-ATPase activity that normally terminate a seizure are overwhelmed. The glial cells swell (the cytotoxic oedema), the extracellular potassium rises, and the further depolarisation is facilitated. [1]
-
Systemic decompensation. The early sympathetic surge (the hypertension, the tachycardia, the hyperglycaemia, the leukocytosis) gives way after about 30 minutes to the autonomic failure — the hypotension, the hyperpyrexia, the respiratory failure, the rhabdomyolysis, and the lactic acidosis. The hypoxia, the hypoglycaemia, and the hypotension each compound the primary neuronal injury. [1]
Clinical presentation
The clinical presentation depends on the stage and the type. [1]
-
Generalised convulsive SE — the most common and the most easily recognised: the bilateral tonic-clonic motor activity, the loss of consciousness, the eyes deviated, the pallor then the cyanosis, the urinary incontinence, the tongue biting. The autonomic features (the tachycardia, the hypertension, the hyperpyrexia, the hypersalivation) are prominent. This is the emergency that drives the staged protocol. [1]
-
Focal SE with impaired awareness (previously the complex partial SE) — the recurrent or the continuous focal seizures with the altered awareness; the patient may wander, the lip-smack, the automatisms. It is under-recognised and is a common cause of the fluctuating confusion in the elderly. [1]
-
Subtle SE — the late stage of the generalised convulsive SE in which the overt convulsions have stopped (or the patient has been given a partial dose of the benzodiazepine) but the seizure continues: the subtle twitching of the face, the eyelid, the hand, or the foot; the nystagmoid eye movements; the sustained eye deviation. The patient has not stopped seizing — the convulsions have simply become subtle. This is the presentation that demands the continuous EEG. [1]
-
Non-convulsive SE (NCSE) — the continuous epileptiform activity on the EEG without the motor convulsions, producing a persistent impaired consciousness. The patient is simply comatose, indistinguishable from the post-ictal state, the metabolic encephalopathy, or the sedation. It is detected only by the EEG.[8]
Investigations
The investigations run in parallel with the resuscitation and the first-line treatment — never delay the benzodiazepine for the tests. [1]
Immediate (bedside, within the first minute):
- Capillary glucose — the hypoglycaemia is the single most important reversible cause; if the bedside glucose is low, give 50 mL of the 50 per cent dextrose IV (or the 25 per cent in the child) immediately, with the thiamine 100 mg IV if the alcohol misuse is suspected.[7]
- ABG — the hypoxia, the hypercarbia, and the acidosis (the lactic acidosis is universal after a convulsion and resolves; the persistent acidosis suggests the rhabdomyolysis or the sepsis).
- ECG — the arrhythmia, the ischaemia, the long QT (the drug effect, the congenital).
Urgent (within the first hour):
- Bloods — the FBC, the U&E (the hyponatraemia, the hypocalcaemia, the hypomagnesaemia, the uraemia), the LFTs, the CK (the rhabdomyolysis), the glucose, the calcium, the magnesium, the CRP, the troponin, the beta-HCG in the woman of the child-bearing age.
- Drug levels — the antiepileptic drug levels if the patient is on the long-term therapy (the non-adherence and the subtherapeutic level is the commonest single precipitant of the SE in the known epileptic); the toxicology screen (the alcohol, the tricyclic, the cocaine, the amphetamine).
- Cultures — the blood and the urine cultures, the chest X-ray — the occult infection (the meningoencephalitis, the pneumonia, the urosepsis) is the commonest cause in the adult without the epilepsy. [1]
Definitive (after the seizure is controlled and the patient is stable):
- CT brain — the first-line imaging in the acute presentation, to exclude the intracranial haemorrhage, the mass, the infarct, or the oedema. Do not send an unstable or an unintubated actively-seizing patient to the CT scanner.
- Lumbar puncture — if the meningoencephalitis is suspected (the fever, the meningism, the confusion) and there is no contraindication on the CT; send the cell count, the protein, the glucose, the PCR (the herpes simplex), and the culture.
- Continuous EEG (cEEG) — the definitive investigation for the NCSE and the subtle SE, and the mandatory monitor for the anaesthetised patient. Start it as early as possible in the refractory phase.
- Autoimmune and paraneoplastic antibodies — the anti-NMDA, the anti-LGI1, the anti-GABA-B, the anti-GAD, the anti-voltage-gated potassium channel complex, in the patient with the new-onset refractory SE (the NORSE) without a clear cause.[9][10]
Management — the staged protocol
The management is a time-critical staged protocol, each stage with a defined drug and a defined time window. The aim is to terminate the seizure before it crosses from the established into the refractory stage, because every minute of the delay increases the pharmacoresistance and the neuronal injury.[7][6]
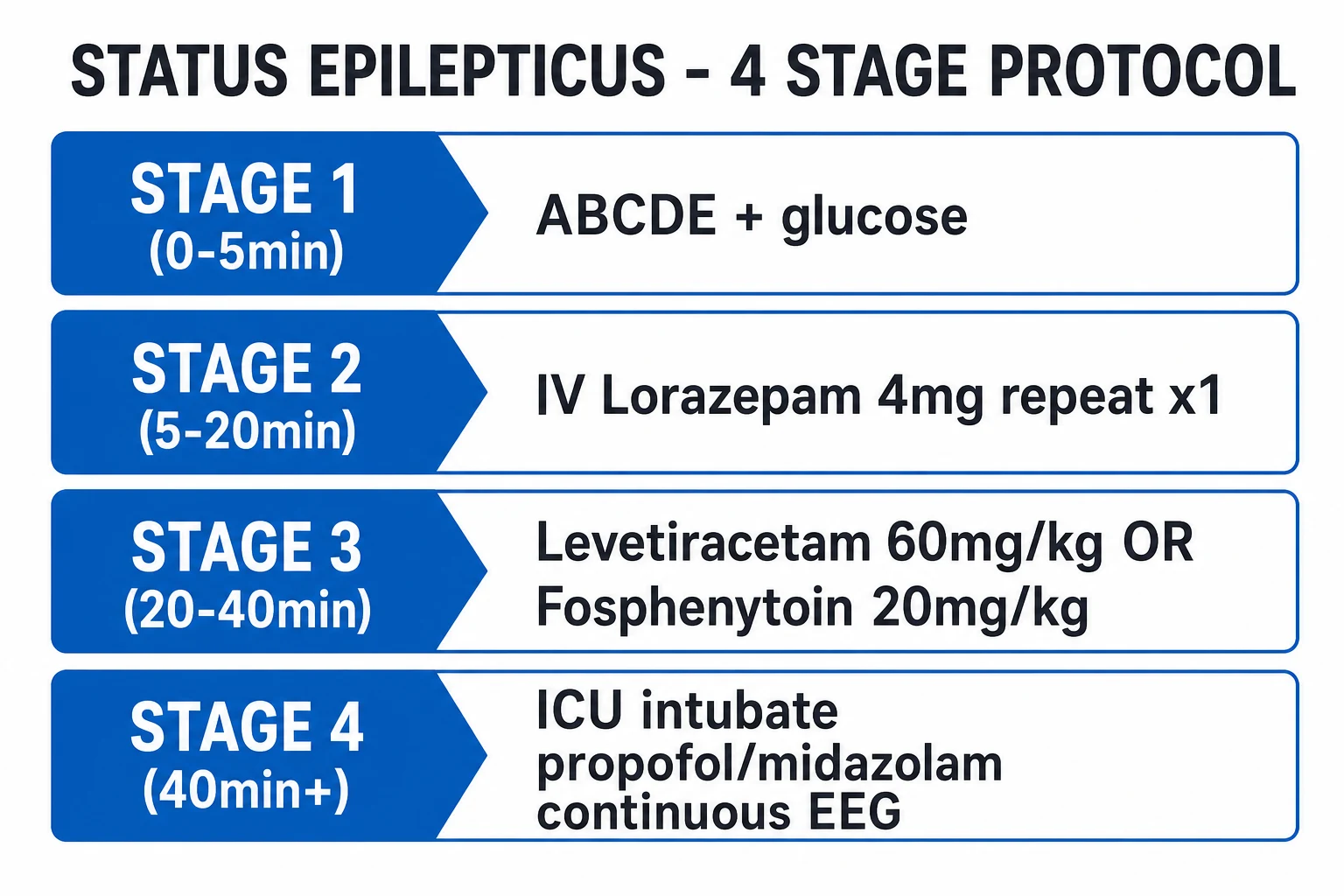
The staged management of status epilepticus
0 to 5 min — Stabilise
Airway (recovery position, suction, oxygen 15 L/min non-rebreather), Breathing (saturation, intubate if the airway or the ventilation fails), Circulation (IV access, BP), Disability (capillary glucose immediately, treat the hypoglycaemia), check the temperature. Do not delay the benzodiazepine.
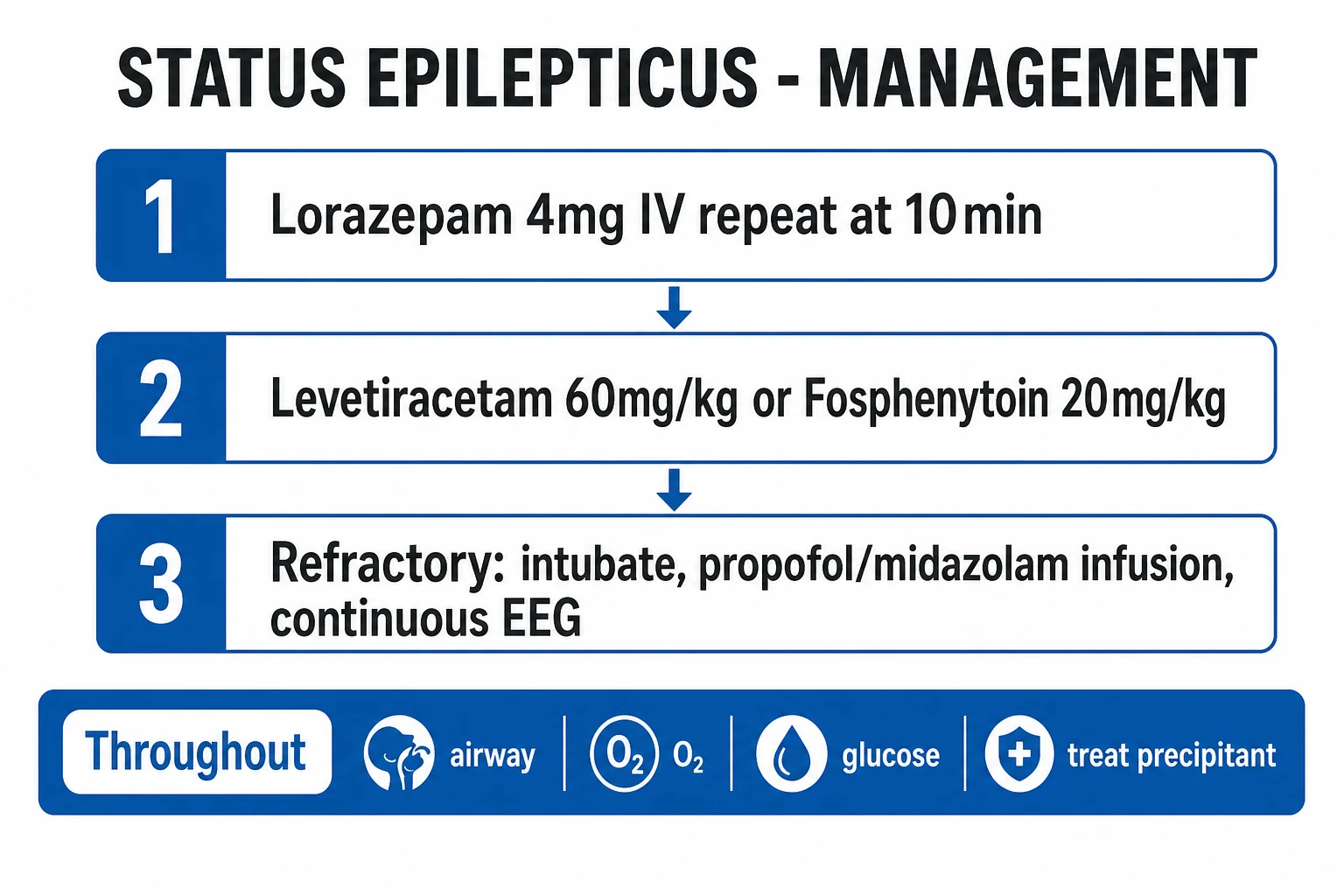
5 to 10 min — First line: a benzodiazepine
Lorazepam 4 mg IV (0.1 mg/kg), repeated once after 5 to 10 minutes if still seizing. If no IV access: midazolam 10 mg IM (the RAMPART dose). Alternatives: diazepam 10 mg IV (but it redistributes fast and recurs) or clonazepam 1 mg IV. The benzodiazepines are the most effective drugs but only in the first 10 to 20 minutes — beyond that, the GABA-A receptor internalisation reduces their efficacy.
20 to 40 min — Second line: an IV antiepileptic
Give regardless of whether the benzodiazepine worked, to prevent the recurrence. Levetiracetam 60 mg/kg IV (max 4.5 g), OR fosphenytoin 20 mg PE/kg IV (max 1.5 g PE, at 150 mg PE/min), OR valproate 40 mg/kg IV (max 3 g). ESETT showed all three equivalent (~half stopped seizing within 10 minutes). Valproate is avoided in the woman of the child-bearing age and in the liver failure.
40 to 60 min — Refractory SE: anaesthetic intubation
If still seizing after the benzodiazepine and the second-line agent, the SE is refractory. Induce, intubate, and ventilate. Start a continuous anaesthetic infusion titrated to the burst suppression on the continuous EEG: propofol OR midazolam first-line, ketamine or thiopent as the alternatives. Admit to the ICU. The EEG is the only way to confirm the seizure has stopped.
After 24 h — Super-refractory SE
If the seizure continues or recurs for more than 24 hours after the anaesthetic (including on weaning), the SE is super-refractory. Maintain the anaesthesia, add the ketamine, consider the immunotherapy (the methylprednisolone, the IVIG, the plasma exchange) for the autoimmune cause, the ketogenic diet, the surgery, and the hypothermia. Prolonged ICU stay.
First-line therapy — the benzodiazepines
The benzodiazepines are the most effective drugs in the early SE (the first 10 to 20 minutes), acting on the GABA-A receptor to potentiate the chloride influx and the hyperpolarisation. Three trials anchor the evidence: [1]
- The VA Cooperative Study (Treiman 1998) — the landmark trial of the first-line therapy in the overt GCSE. Lorazepam was superior to phenytoin, phenobarbital, and diazepam for the termination of the overt SE (the lorazepam terminated 65 per cent, the phenytoin 58 per cent, the phenobarbital 56 per cent, the diazepam 42 per cent). Lorazepam became the first-line agent because it is more effective, longer-acting than the diazepam, and easy to give.[3]
- The PHTSE / Alldredge 2001 trial — the prehospital study comparing the IV lorazepam, the IV diazepam, and the placebo for the out-of-hospital SE. Both the benzodiazepines were better than the placebo; the lorazepam tended to be the best. The prehospital benzodiazepine reduced the seizures before the arrival and improved the outcome.[4]
- The RAMPART (Silbergleit 2012) — the non-inferiority trial of the IM midazolam (10 mg IM for the adult over 40 kg, 5 mg for the 13 to 40 kg) versus the IV lorazepam (4 mg IV). The IM midazolam was at least as effective as the IV lorazepam, because the IV access was often difficult and delayed. The practice change: the IM midazolam is the first-line prehospital drug when the IV access is not available.[2]
Second-line therapy — the IV antiepileptics (ESETT)
The ESETT (Kapur 2019) is the definitive second-line trial. It randomised the patients with the established SE (the benzodiazepine-refractory convulsive SE) to levetiracetam 60 mg/kg, fosphenytoin 20 mg PE/kg, or valproate 40 mg/kg. The trial was stopped early at the interim analysis for the futility — there was no difference between the three drugs. Each stopped the seizure in about half of the patients within 10 minutes (levetiracetam 47 per cent, fosphenytoin 45 per cent, valproate 46 per cent).[1]
ESETT
NEJM 2019
Double-blind RCT; convulsive SE refractory to benzodiazepines; levetiracetam 60 mg/kg vs fosphenytoin 20 mg PE/kg vs valproate 40 mg/kg; n=384
Key finding
No difference: seizure stopped within 10 min in 47% (levetiracetam), 45% (fosphenytoin), 46% (valproate). Stopped early for futility. All three equivalent and all inadequate alone in roughly half.
Practice change
Any of the three is acceptable second line; choose by the patient (valproate avoided in pregnancy and hepatic failure; fosphenytoin in cardiac disease; levetiracetam preferred if the cause or the organ function is unknown).
Levetiracetam
60 mg/kg IV (max 4.5 g)
- The broad-spectrum, the favoured default — no hepatic metabolism, no cardiac, no interaction
- Commonest choice when the cause and the organ function are unknown
- Side effects: the sedation, the agitation, the thrombocytopenia (rare)
- Loading over 5 minutes; well tolerated
Fosphenytoin
20 mg PE/kg IV (max 1.5 g PE)
- The water-soluble prodrug of the phenytoin — can be given faster (150 mg PE/min) and via the IM route
- Less tissue necrosis and the purple-glove than the phenytoin
- Monitor the ECG (the PR prolongation, the QRS widening, the hypotension) — give via a large vein, stop if the arrhythmia
- Avoid in the heart block and the severe cardiac disease
Valproate
40 mg/kg IV (max 3 g)
- Effective across the broad spectrum — the generalised, the focal, the absence
- Avoid in the woman of the child-bearing age (the teratogenicity) and the hepatic failure (the hepatotoxicity)
- Monitor the ammonia (the hyperammonaemic encephalopathy)
- Platelet inhibitor — caution with the bleeding and the thrombocytopenia
Refractory status epilepticus — the anaesthetic infusions
When the seizure continues despite the benzodiazepine and the second-line agent, the SE is refractory and the patient requires the anaesthetic intubation, the ventilation, and the continuous infusion of an anaesthetic agent titrated to the burst suppression on the continuous EEG. The goal is the EEG burst suppression (the bursts of the activity alternating with the flat suppression) maintained for 24 to 48 hours before the weaning and the re-assessment.[6][7]
Propofol
GABA agonist
- Fast onset, fast offset (the easy titration and the rapid wean) — the most-used first-line anaesthetic for the RSE
- Bolus 1 to 2 mg/kg, infusion 30 to 200 mcg/kg/min
- Risk: the propofol infusion syndrome (PRIS) — the metabolic acidosis, the rhabdomyolysis, the bradycardia, the cardiac arrest, especially over 4 mg/kg/h for over 48 hours
- Monitor the lactate, the CK, the triglycerides, and the ECG; cap the dose in the child
Midazolam
GABA agonist
- Fast onset, water-soluble; the reliable continuous infusion
- Bolus 0.2 mg/kg, infusion 0.05 to 2 mg/kg/h
- Risk: the tachyphylaxis (the rapid receptor tolerance — the dose escalates), the hypotension
- The seizure often recurs on the weaning — the slow taper required
Ketamine
NMDA antagonist
- The NMDA-receptor antagonist — the rationale strengthens as the seizure persists (the NMDA receptors externalise)
- Bolus 1 to 2 mg/kg (or 0.5 mg/kg/h to start), infusion 1 to 10 mg/kg/h (up to 15 mg/kg/h in the super-RSE)
- Preserves the BP and the sympathetic tone (the inotropic — avoids the hypotension of the other anaesthetics)
- Evidence: a 2018 systematic review found it stopped or reduced the seizures in roughly two-thirds of the RSE, with a favourable haemodynamic profile
- Side effects: the hallucination (irrelevant in the intubated), the hypertension, the sialorrhoea, the theoretical raised ICP
Thiopental / Pentobarbital
GABA agonist (barbiturate)
- The most potent and the longest-acting — reserved for the super-refractory after the propofol, the midazolam, and the ketamine fail
- Bolus 5 mg/kg, infusion 1 to 5 mg/kg/h (or the pentobarbital 1 mg/kg/h to 3 mg/kg/h)
- Profound burst suppression but the severe side effects: the hypotension, the ileus, the immunosuppression, the pneumonia, the prolonged coma
- Long half-life — the slow wean over days; the drug accumulates and the level is hard to interpret
RAMPART
NEJM 2012
Double-blind non-inferiority RCT; prehospital SE; IM midazolam 10 mg (adult over 40 kg) vs IV lorazepam 4 mg; n=893 (892 adults)
Key finding
IM midazolam was superior to IV lorazepam — seizure terminated before arrival in 63% vs 53% (no IV access in 23%). Fewer recurrences and fewer intubations with IM midazolam.
Practice change
IM midazolam is the first-line prehospital therapy when IV access is not yet established — give it early, do not struggle for a line.
VA Cooperative Study
NEJM 1998
Open-label randomised trial; overt and subtle GCSE; lorazepam vs phenytoin vs phenobarbital vs diazepam; n=518 (384 overt)
Key finding
In overt GCSE, lorazepam was most effective (seizure stopped in 65%) and superior to diazepam (42%); in subtle SE all four were poor (~10-25%).
Practice change
Lorazepam became the preferred first-line IV benzodiazepine for established SE; phenobarbital and phenytoin are not superior first-line agents.
Continuous EEG — the mandatory monitor
In the refractory and the super-refractory SE, the EEG is the only way to know whether the seizure has stopped, because the patient is paralysed and sedated and the clinical signs are abolished. The continuous EEG (the cEEG) serves three purposes:[8]
- To confirm the seizure termination — the ictal rhythm resolves and the background returns, or (in the anaesthetised patient) the burst suppression is achieved.
- To titrate the anaesthetic — the infusion is adjusted to maintain the burst suppression (or the suppression-burst, or the complete suppression, depending on the protocol). The target is typically the burst suppression with the inter-burst intervals of 5 to 10 seconds, maintained for 24 to 48 hours before the weaning.
- To detect the non-convulsive SE — the patient who fails to wake up after the convulsive SE may be in the NCSE (the continuing epileptiform activity without the motor convulsions). The cEEG detects it; the bedside examination cannot. [1]
Claassen (2004) showed that the continuous EEG in the critically ill patient detected the non-convulsive seizures in 8 per cent and the NCSE in 18 per cent of the comatose patients monitored — many of whom had no clinical sign of the ongoing seizure.[8]
Weaning the anaesthetic
After 24 to 48 hours of the burst suppression, the anaesthetic is weaned (the infusion reduced by a quarter to a third every 6 to 12 hours) with the continuous EEG running. If the seizures or the ictal pattern recur, the infusion is restarted, the duration extended to 48 to 72 hours, and an additional agent considered (the ketamine, the immunotherapy, the ketogenic diet). The super-refractory SE (the recurrence or the persistence beyond 24 hours of the anaesthetic) may require weeks of the coma and is associated with the high morbidity and the mortality.[6]
Non-convulsive status epilepticus (NCSE)
The non-convulsive status epilepticus is the continuous or the recurring epileptiform activity on the EEG without the motor convulsions, producing a persistent impaired consciousness. It is common — affecting 10 to 30 per cent of the comatose ICU patients, especially after a convulsive SE, a severe traumatic brain injury, a subarachnoid haemorrhage, a cardiac arrest, or in the hepatic and the renal encephalopathy. It is detected only by the continuous EEG — the clinical examination cannot distinguish it from the metabolic encephalopathy, the post-ictal state, or the sedation.[8]
The Salzburg criteria (the consensus criteria for the NCSE diagnosis) require the epileptiform activity on the EEG (the spikes, the sharp waves, the rhythmic activity of an epileptiform morphology) plus one of: a response to the IV antiepileptic (the benzodiazepine or the valproate — the EEG improves), a subtle clinical improvement, or a typical EEG pattern (the ictal-interictal continuum). [1]
The treatment of the NCSE is the same staged ladder as the convulsive SE, but the urgency is debated — the NCSE is less immediately life-threatening than the convulsive SE, and the aggressive anaesthetic therapy (with its hypotension and its immunosuppression) may harm as much as the seizure. Most authorities treat the NCSE with the benzodiazepine and the second-line agent, but reserve the anaesthetic infusion for the NCSE that is clearly worsening the patient or that is refractory.[7][6]
New-onset refractory SE (NORSE) and the immune-mediated causes
The new-onset refractory status epilepticus (NORSE) is the refractory SE in a patient with no prior epilepsy and no clear acute cause — the term flags the patient in whom the occult autoimmune, the paraneoplastic, or the infectious cause must be sought. The febrile infection-related epilepsy syndrome (FIRES) is the NORSE preceded by a febrile illness (often a mild respiratory or a gastrointestinal infection) in the days before the SE. The prognosis is guarded — the mortality and the morbidity are high, and many survivors have the chronic epilepsy and the cognitive impairment. [1]
Anti-NMDA receptor encephalitis
The anti-NMDA receptor encephalitis is the prototypical autoimmune encephalitis — an antibody-mediated attack on the GluN1 subunit of the NMDA receptor, producing a characteristic syndrome that the intensivist must recognise. The typical patient is a young woman (the median age around 20 to 25 years, but it occurs in the children and the men). The clinical course unfolds in stages:[9][10]
- A prodrome — a low-grade fever, a headache, a fatigue, a gastrointestinal or an upper respiratory symptom, lasting a few days (often dismissed as a viral illness).
- A psychiatric phase — the anxiety, the insomnia, the paranoia, the hallucinations, the bizarre behaviour, the mutism, the memory loss. Many patients are first admitted to the psychiatric unit before the seizures and the movement disorder reveal the diagnosis.
- Seizures and the movement disorder — the focal or the generalised seizures (often the SE or the refractory SE), the orofacial dyskinesias (the lip-smacking, the grimacing, the chewing), the choreoathetosis, the dystonia, the rigidity.
- Dysautonomia and the hypoventilation — the fever, the salivation, the cardiac instability (the tachycardia, the bradycardia, the fluctuating blood pressure), the central hypoventilation requiring the mechanical ventilation, the catatonia and the coma. [1]
The diagnosis is on the antibody in the CSF and the serum (the CSF is more sensitive), the MRI (the medial temporal and the multifocal cortical T2/FLAIR hyperintensity, but the MRI may be normal), the EEG (the diffuse slowing, the extreme delta brush — the pathognomonic but not universal pattern), and the search for the occult ovarian teratoma (the pelvic ultrasound and the MRI — the teratoma is found in roughly half of the adult women and is the driver of the antibody production).[9][10]
The treatment is the immunotherapy — the sooner the better, as the early treatment predicts the better outcome. The first-line is the methylprednisolone (1 g IV daily for 3 to 5 days), the IVIG (0.4 g/kg daily for 5 days), and the plasma exchange (3 to 5 sessions), often in combination. If the teratoma is found, the resection is essential. If the patient does not improve in 2 to 4 weeks, the second-line immunotherapy is the rituximab and/or the cyclophosphamide. Titulaer (2013) showed that the early (within the first month) and the second-line immunotherapy predicted the good outcome, and that the late or the no immunotherapy predicted the poor outcome and the relapse. The prognosis overall is favourable — about 75 to 80 per cent recover to a good functional outcome, but the recovery is slow (months) and the relapses occur in 10 to 20 per cent.[9][10]
Evidence & guidelines
The evidence base for the SE management is anchored by four landmark trials and two guidelines: [1]
PHTSE / Alldredge
NEJM 2001
Randomised double-blind trial; out-of-hospital SE; IV lorazepam vs IV diazepam vs placebo; n=205
Key finding
Both benzodiazepines stopped the SE before arrival more often than placebo (lorazepam 59%, diazepam 43%, placebo 21%). The benzodiazepine was safe and effective prehospital.
Practice change
Established the role of prehospital IV benzodiazepine (especially lorazepam) for out-of-hospital SE.
- The ILAE operational definition (Trinka 2015) — the consensus definition with the t1 (5 min) and the t2 (30 min) time points that turned the SE into the time-critical emergency. The five-minute threshold is the treatment trigger for the generalised convulsive SE.[5]
- The Neurocritical Care Society guideline (Brophy 2012) — the comprehensive guideline for the evaluation and the management of the SE, endorsing the staged protocol (the benzodiazepine, the second-line agent, the anaesthetic infusion) and the cEEG for the refractory and the unexplained-coma patient.[7]
- The ESETT (2019), the RAMPART (2012), the VA Cooperative (1998), and the Alldredge (2001) — the four trials that define the first- and the second-line therapy (described above).
Special situations
Eclampsia (the pregnant patient)
The eclampsia is the tonic-clonic seizure in the pregnant woman with the pre-eclampsia (the hypertension, the proteinuria, the oedema after 20 weeks). The first-line drug is the magnesium sulfate, not the benzodiazepine — the magnesium is both the treatment and the prophylaxis. Give the magnesium sulfate 4 g IV over 5 minutes (the loading), followed by the 1 to 2 g/h infusion for 24 hours, monitoring the reflexes (the loss of the patellar reflex is the early sign of the magnesium toxicity), the respiratory rate, and the serum magnesium. The benzodiazepine (the lorazepam) and the second-line agent are added if the magnesium fails. The definitive treatment is the delivery of the fetus — expedite it. The eclampsia can occur postpartum (up to 6 weeks) and in the atypical patient without the hypertension or the proteinuria.[7]
The alcohol-withdrawal SE
The alcohol withdrawal is a common precipitant of the SE — the patient presents 6 to 48 hours after the last drink (sometimes up to a week) with the tremor, the agitation, the hallucination, the autonomic hyperactivity, and the seizure. Give the thiamine 100 mg IV before any glucose (the glucose without the thiamine can precipitate the Wernicke encephalopathy), then the benzodiazepine and the second-line agent by the standard ladder. The long-term management is the benzodiazepine taper (the diazepam or the lorazepam by the symptom-triggered CIWA protocol) and the thiamine replacement. The prognosis is good if the seizure is terminated.[6]
The hepatic and the renal failure
In the hepatic failure, the valproate is avoided (the hepatotoxicity) and the benzodiazepine doses are reduced and the intervals extended (the impaired clearance and the encephalopathy). In the renal failure, the levetiracetam dose is reduced (it is renally cleared — halve the dose in the creatinine clearance below 30, give after the dialysis) and the valproate and the fosphenytoin need no renal adjustment. The rapid correction of the hyponatraemia must be avoided (the osmotic demyelination) — correct slowly, at under 8 to 10 mmol/L over 24 hours, except in the severe symptomatic (the seizure from the acute hyponatraemia) where the 3 per cent saline is given to raise the sodium by 4 to 6 mmol/L.[7]
The paediatric SE
In the child, the first-line is the same benzodiazepine (the lorazepam 0.1 mg/kg IV, or the midazolam 0.3 mg/kg IM, or the diazepam 0.3 mg/kg IV/PR). The second line is the levetiracetam 60 mg/kg, the fosphenytoin 20 mg PE/kg, or the valproate 40 mg/kg — the ESETT included the children over 2 years and showed the same equivalence. The febrile infection-related epilepsy syndrome (FIRES) is the catastrophic refractory SE in the child after a febrile illness, often needing the prolonged anaesthesia and the ketogenic diet — the prognosis is guarded. The propofol is contraindicated for the prolonged sedation in the child under 16 (the risk of the propofol infusion syndrome is higher in the child).[6][11]
The drug-induced and the toxic SE
The tricyclic antidepressant overdose produces the seizure and the QRS widening — give the sodium bicarbonate (the QRS over 100 ms or the arrhythmia). The cocaine and the amphetamine produce the sympathetic SE — the benzodiazepine is the first line (avoid the haloperidol and the beta-blocker in the cocaine). The isoniazid overdose produces the refractory SE unresponsive to the benzodiazepine — give the pyridoxine (vitamin B6) gram-for-gram matched to the ingested isoniazid (or 5 g empirically). The antibiotic (the cefepime, the carbapenem) can precipitate the SE in the renal failure — review the drug chart.[7]
Complications
The complications of the SE arise from the seizure itself, from the treatment, and from the prolonged ICU stay: [1]
- Neurological — the neuronal injury (the hippocampal sclerosis, the cortical atrophy on the follow-up MRI), the chronic epilepsy (the SE lowers the seizure threshold permanently), the cognitive impairment, the persistent disorder of consciousness.
- Systemic (the seizure) — the hypoxia and the hypercarbia, the lactic acidosis, the rhabdomyolysis (the CK, the renal failure), the hyperpyrexia, the aspiration pneumonitis, the tongue biting, the fractures (the vertebral, the shoulder), the cardiac arrhythmia and the ischaemia, the disseminated intravascular coagulation.
- Systemic (the treatment) — the propofol infusion syndrome (the propofol), the hypotension and the immunosuppression and the nosocomial infection (the thiopent and the prolonged anaesthesia), the hepatic and the haematological (the valproate), the tissue necrosis (the phenytoin extravasation).
- The prolonged ICU stay — the critical illness polyneuromyopathy, the decubitus ulcers, the deep vein thrombosis, the ventilator-associated pneumonia, the malnutrition. [1]
Prognosis
The prognosis of the SE depends overwhelmingly on the aetiology and the duration — the two factors that outweigh the choice of the drug. The overall mortality is around 10 to 30 per cent, but it rises steeply with the refractory (30 to 40 per cent) and the super-refractory (40 to 50 per cent) stages, and with the poor aetiology (the anoxic SE after the cardiac arrest, the stroke, the CNS infection, the metabolic).[6][12]
Status epilepticus — the numbers
The early predictors of the refractory SE (Sutter 2015, the international two-centre study) are the younger age, the absence of the structural lesion, the subtle SE, the non-convulsive SE, and the longer duration before the presentation — these identify the patient at the high risk of needing the anaesthetic infusion, and they should prompt the early escalation and the cEEG.[12]
The aetiology-specific prognosis is critical. The anoxic SE (the myoclonic SE after the cardiac arrest) carries a mortality of over 80 per cent and is a marker of the severe anoxic injury; the alcohol-withdrawal and the drug-related SE have a good prognosis if treated; the autoimmune (the anti-NMDA) SE has a favourable prognosis with the early immunotherapy. The aetiology, not the drug choice, is the dominant determinant of the outcome.[6]
Exam practice
Convulsive status epilepticus — the staged management
15 minutes · 20 marks
A 56-year-old man is brought to the emergency department by ambulance with a generalised tonic-clonic seizure that began 12 minutes ago at home. The paramedics gave 10 mg of intramuscular midazolam at the scene with no effect. On arrival he is convulsing, oxygen saturation 88% on room air, blood pressure 170/95, heart rate 120, temperature 38.2°C, capillary glucose 6.4 mmol/L. Two large-bore IV cannulae are in situ. You are the intensive care registrar called to manage him.
SAQ — Refractory convulsive SE requiring anaesthetic intubation
10 minutes · 10 marks
A 34-year-old woman with no prior history has been convulsing for 35 minutes despite 8 mg IV lorazepam and levetiracetam 60 mg/kg IV. She is in the emergency department, oxygen saturation 90% on a non-rebreather, BP 105/65, HR 130, temperature 38.5C, capillary glucose 7.2 mmol/L. Two large-bore cannulae are in place. You are the ICU registrar taking over her care.
SAQ — Non-convulsive status epilepticus on continuous EEG
10 minutes · 10 marks
A 62-year-old man is admitted to the ICU 24 hours after a generalised convulsive seizure that terminated in the emergency department with lorazepam. He has not regained consciousness (GCS 8). Examination shows no motor seizure activity and occasional subtle eyelid twitching. Continuous EEG reveals continuous rhythmic activity with lateralised periodic discharges and superimposed ictal rhythms over the left temporal region.
Clinical pearls — the high-yield exam points
[1] [1]Red flags
References
- [1]Kapur J, Elm J, Chamberlain JM, et al.; NETT and ESETT Investigators. Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus N Engl J Med, 2019.PMID 31774955
- [2]Silbergleit R, Durkalski V, Lowenstein D, et al.; NETT Investigators. Intramuscular versus intravenous therapy for prehospital status epilepticus N Engl J Med, 2012.PMID 22335736
- [3]Treiman DM, Meyers PD, Walton NY, et al.; DVA Status Epilepticus Cooperative Study Group. A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group N Engl J Med, 1998.PMID 9738086
- [4]Alldredge BK, Gelb AM, Isaacs SM, et al. A comparison of lorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus N Engl J Med, 2001.PMID 11547716
- [5]Trinka E, Cock H, Hesdorffer D, et al. A definition and classification of status epilepticus--Report of the ILAE Task Force on Classification of Status Epilepticus Epilepsia, 2015.PMID 26336950
- [6]Trinka E, Leitinger M. Management of Status Epilepticus, Refractory Status Epilepticus, and Super-refractory Status Epilepticus Continuum (Minneap Minn), 2022.PMID 35393970
- [7]Brophy GM, Bell R, Claassen J, et al.; Neurocritical Care Society Status Epilepticus Guideline Writing Committee. Guidelines for the evaluation and management of status epilepticus Neurocrit Care, 2012.PMID 22528274
- [8]Claassen J, Mayer SA, Kowalski RG, Emerson RG, Hirsch LJ. Detection of electrographic seizures with continuous EEG monitoring in critically ill patients Neurology, 2004.PMID 15159471
- [9]Titulaer MJ, McCracken L, Gabilondo I, et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study Lancet Neurol, 2013.PMID 23290630
- [10]Dalmau J, Armangué T, Planagumà J, et al. An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models Lancet Neurol, 2019.PMID 31326280
- [11]Rosati A, De Masi S, Guerrini R. Ketamine for Refractory Status Epilepticus: A Systematic Review CNS Drugs, 2018.PMID 30232735
- [12]Sutter R, Kaplan PW, Marsch S, et al. Early predictors of refractory status epilepticus: an international two-center study Eur J Neurol, 2015.PMID 25104078