ICU · pharmacology
ICU Antihypertensive Drugs — Comprehensive
Also known as IV antihypertensives · Hypertensive emergency drugs · Labetalol · Nicardipine · Sodium nitroprusside · Clevidipine · Esmolol · Hydralazine · Phentolamine · Fenoldopam · Cyanide toxicity · Unopposed alpha stimulation
IV antihypertensives for the ICU — the nine agents every intensivist must master: LABETALOL (combined alpha+beta blocker — versatile first-line for most hypertensive emergencies; 10-20 mg IV bolus q10min or infusion 0.5-2 mg/min; contraindicated in severe asthma/heart block), NICARDIPINE (dihydropyridine CCB — smooth titratable infusion — ideal for most HTN emergencies including stroke; onset 5-15 min), HYDRALAZINE (direct arteriolar vasodilator — pregnancy/pre-eclampsia favourite; slow/unpredictable onset 10-30 min; CAUTION reflex tachycardia), SODIUM NITROPRUSSIDE (arteriolar + venous NO donor — most potent — CYANIDE TOXICITY if 4 mcg/kg/min or 48h — now largely superseded), NITROGLYCERIN (venous arteriolar NO donor — for ACS/acute pulmonary oedema; tachyphylaxis), CLEVIDIPINE (ultra-short DHP CCB — 1-2 min onset/offset — metabolised by esterases; VELOCITY trial), ESMOLOL (beta-1 selective — 9 min half-life — aortic dissection, tachyarrhythmia), FENOLDOPAM (D1 agonist — 'renal protective' — controversial; no proven benefit), PHENTOLAMINE (non-selective alpha-blocker — pheochromocytoma crisis FIRST). Oral agents for chronic ICU BP control (ACEi/ARB, CCB, beta-blockers, diuretics, alpha-blockers). Scenario-specific rules that MUST be memorised: AORTIC DISSECTION = beta-blocker FIRST then vasodilator (prevent reflex tachycardia → propagation; target HR <60, SBP 100-120); HYPERTENSIVE ENCEPHALOPY = labetalol or nicardipine (reduce MAP 10-20% first hour); PRE-ECLAMPSIA = hydralazine or labetalol + magnesium sulphate; PHEOCHROMOCYTOMA = phentolamine FIRST then beta-blocker (alpha before beta to prevent unopposed alpha → worsening hypertensive crisis); COCAINE = benzodiazepines FIRST (avoid beta-blockers — unopposed alpha).
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags
Overview & definition
[1]
Emergency vs urgency — the first decision
Hypertensive emergency vs urgency — the defining distinction
| Feature | Hypertensive EMERGENCY | Hypertensive URGENCY |
|---|---|---|
| Acute HMOD | YES (the defining feature) | NO |
| Setting | ICU admission, arterial line | Ward / short-stay / clinic |
| Route | IV titratable agent, continuous infusion | Oral agents (e.g. amlodipine, captopril, clonidine) |
| Goal | Controlled BP reduction over minutes-hours | BP reduction over 24-48 h |
| Risk of rapid drop | High — cerebral/renal/coronary ischaemia | Low |
| Examples | Encephalopathy, aortic dissection, pre-eclampsia/eclampsia, pulmonary oedema, ACS, ICH/SAH, AKI with scleroderma, catecholamine surge | Asymptomatic BP >180/120, mild headache, anxiety |
The absolute BP number does not determine emergency vs urgency — only the presence of acute end-organ damage does. A patient at 240/140 with no organ damage has urgency; a previously normotensive patient at 160/100 with new encephalopathy and papilloedema has an emergency.[2]
Cerebral autoregulation — why controlled reduction matters
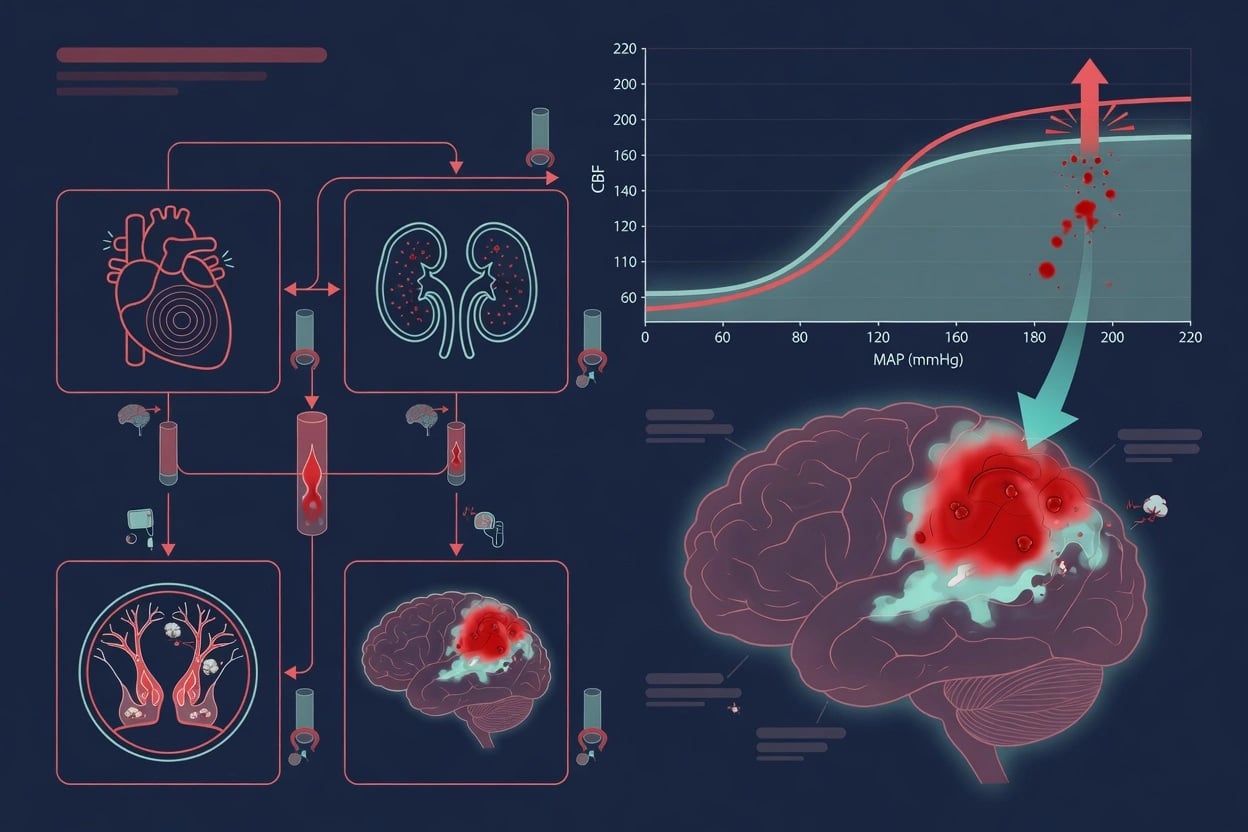
Chronic hypertensives shift their cerebral autoregulation curve to the right. The lower limit of autoregulation sits around a MAP of 110-120 mmHg (vs ~60 in normotensives). Precipitous BP reduction below this autoregulatory floor → cerebral hypoperfusion → watershed infarction. Likewise, the rightward shift means a "normal" MAP of 70-80 can be ischaemic for a chronically hypertensive brain during an acute event. Hence the rule: reduce MAP by 10-20% in the first hour, then gradually to ~160/100 over 2-6 h.[6]
IV antihypertensive agents — the comprehensive comparison
The nine IV antihypertensives — mechanism, dosing, and niche
| Drug | Mechanism | Onset | Duration after stop | Dose | Best indication | Key caution |
|---|---|---|---|---|---|---|
| Labetalol | Combined alpha-1 + non-selective beta blocker (α:β ≈ 1:7 oral, 1:3 IV) | 2-5 min | 3-6 h | 10-20 mg IV q10min (max 300 mg) OR infusion 0.5-2 mg/min | Versatile first-line — encephalopathy, aortic dissection, pregnancy/pre-eclampsia, post-op | Bradycardia, heart block, bronchospasm (asthma), severe LV failure (negative inotrope) |
| Nicardipine | Dihydropyridine L-type Ca channel blocker (vascular selectivity) | 5-15 min | 4-6 h (long offset) | 5 mg/h, ↑ by 2.5 mg/h q5min to max 15 mg/h | Most HTN emergencies — especially acute stroke (cerebroselective), renal failure | Reflex tachycardia (less than hydralazine), headache, phlebitis (central line preferred for long use) |
| Clevidipine | Ultra-short-acting DHP CCB — esterase-metabolised (independent of renal/hepatic) | 1-2 min | 1-2 min (true ultra-short) | 1-2 mg/h, double q90sec to max 32 mg/h | Peri-operative/peri-procedural BP, rapid titration; needs accurate pressure tubing (drug adsorbs to PVC) | Hypertriglyceridaemia/lipid load (formulated as lipid emulsion), egg/soy allergy contraindication |
| Esmolol | Beta-1 selective — RBC esterases → ultra-short | 1-2 min | 9 min (t½) | Load 500 mcg/kg over 1 min, then 50-300 mcg/kg/min | Aortic dissection (HR control), supraventricular tachycardia with HTN | Bradycardia, hypotension; beta-1 selectivity lost at high dose; avoid in decompensated HF |
| Enalaprilat | IV ACE inhibitor | 15-30 min | 6-12 h (long) | 1.25-5 mg IV q6h | Scleroderma renal crisis | AKI (esp. bilateral RAS), hyperkalaemia, dry cough; unpredictable — rarely used acutely |
| Hydralazine | Direct arteriolar vasodilator (K-channel / NO) | 10-30 min (slow/unpredictable) | 3-8 h (long, poorly titratable) | 5-20 mg IV q4-6h | Pre-eclampsia/eclampsia (established obstetric favourite) | Reflex tachycardia (dangerous in CAD/dissection), tachyphylaxis, drug-induced lupus, headache |
| Nitroglycerin | Venous > arteriolar NO donor | 2-5 min | 5-10 min | 5-200 mcg/min | ACS (coronary vasodilation + preload reduction), acute pulmonary oedema | Weak antihypertensive (mainly preload), tachyphylaxis (12-24h), headache, methaemoglobinaemia, hypoxaemia (V/Q mismatch) |
| Sodium nitroprusside | Arteriolar + venous NO donor (releases cyanide) | <30 sec | 1-2 min (true ultra-short) | 0.25-10 mcg/kg/min | Reserved for refractory cases; rapid titration | CYANIDE TOXICITY (>4 mcg/kg/min or >48h or renal/hepatic impairment), thiocyanate in renal failure, cerebral steal (increases ICP), coronary steal |
| Fenoldopam | Selective dopamine-1 (D1) agonist — renal + mesenteric + peripheral vasodilation | 5-10 min | 10-15 min | 0.1-1.6 mcg/kg/min | Theoretically renal-protective in AKI with HTN (natriuresis) — benefit unproven | Reflex tachycardia, intraocular pressure rise (avoid glaucoma), expensive; no outcome advantage |
| Phentolamine | Non-selective competitive alpha-1 + alpha-2 blocker | 1-2 min | 10-30 min | 1-5 mg IV bolus, repeat; or infusion | Pheochromocytoma crisis, catecholamine surge (MAOI-tyramine), noradrenaline extravasation reversal | Reflex tachycardia, orthostatic hypotension; must be paired with beta-blocker AFTER alpha-blockade |
Mechanistic grouping — three families
- Sympathetic blockers — labetalol (α+β), esmolol (β1), phentolamine (α1+α2). Reduce sympathetic drive and contractility; key for tachyarrhythmia-prone scenarios.
- Calcium channel blockers — nicardipine, clevidipine (both DHP, vascular selectivity). Smooth, titratable; favoured for stroke and most emergencies.
- NO-donor vasodilators — nitroprusside (arteriole+vein, potent), nitroglycerin (vein>arteriole), hydralazine (arteriole, direct). Potent but each carries a signature toxicity. [1]
Exam shortcut: the three "fast and short" agents for fine titration are nitroprusside, clevidipine, and esmolol (sub-minute to minute kinetics). The "slow and long" agents you commit to are hydralazine (10-30 min onset, 3-8 h duration — you cannot titrate it off quickly) and enalaprilat (15-30 min onset, 6-12 h duration). Labetalol and nicardipine are the "middle ground" — versatile and forgiving.[5]
Detailed agent pharmacology
Labetalol — the versatile workhorse
Mechanism: competitive non-selective beta-blocker (β1 + β2) AND selective alpha-1 blocker. The IV preparation has an α:β blocking ratio of approximately 1:3 (oral ≈1:7). Net effect: lower BP without reflex tachycardia (the beta-blockade suppresses the reflex tachycardia that a pure vasodilator would provoke), and without a marked fall in cardiac output or cerebral/renal blood flow. [1]
Pharmacokinetics: onset 2-5 min, peak 5-15 min, duration 3-6 h. Hepatic metabolism (glucuronidation) — excreted as inactive metabolites (usable in renal failure). [1]
Dosing:
- Bolus regimen: 10-20 mg IV over 1-2 min, repeat every 10 min to a maximum of 300 mg total.
- Infusion regimen: 0.5-2 mg/min (some protocols to 8 mg/min), titrated to target. A common loading approach is 20 mg, then 40 mg, then 80 mg at 10-min intervals. [1]
Where it shines: aortic dissection (combined rate + BP control — but esmolol allows finer HR titration), hypertensive encephalopathy, pre-eclampsia/eclampsia (classified as pregnancy category C but extensive safe-use history; first-line in obstetric protocols), post-operative hypertension after cardiac/vascular surgery. [1]
Contraindications/cautions: asthma/severe bronchospasm (β2 effect), second/third-degree heart block, severe bradycardia, overt congestive cardiac failure from negative inotropy (use with care — it is not absolutely contraindicated in HF as the alpha-blockade reduces afterload), severe reactive airway disease. [1]
Nicardipine — the smooth titrator
Mechanism: dihydropyridine L-type voltage-gated calcium channel antagonist with high vascular selectivity — relaxes arteriolar smooth muscle with negligible effect on the myocardium or conduction (unlike verapamil/diltiazem). [1]
Pharmacokinetics: onset 5-15 min, duration 4-6 h after stopping (the long offset is a drawback if overshoot occurs). Hepatic metabolism; renal excretion of inactive metabolites. [1]
Dosing: start 5 mg/h, increase by 2.5 mg/h every 5 min to a maximum of 15 mg/h. Onset of adequate control typically within 15-30 min. Can transition to oral amlodipine. [1]
Where it shines: acute ischaemic and haemorrhagic stroke (maintains cerebral perfusion, cerebroselective vasodilation, predictable response), most generic hypertensive emergencies, renal failure (no accumulation of toxic metabolites unlike nitroprusside), peri-operative BP control. [1]
Cautions: reflex tachycardia (less pronounced than hydralazine — usually acceptable), phlebitis at the peripheral cannula site with prolonged infusion (use a central line for runs >12 h), headache/flushing. Avoid in acute heart failure with severe LV dysfunction if heart rate rises precipitously. [1]
Clevidipine — the ultra-short DHP
Mechanism: third-generation ultra-short-acting DHP CCB — arteriolar vasodilation. Rapidly hydrolysed by blood and tissue esterases to an inactive metabolite — metabolism is independent of renal and hepatic function. [1]
Pharmacokinetics: onset 1-2 min, offset 1-2 min (the only true ultra-short DHP). This makes it the most precisely titratable agent available. [1]
Dosing: start 1-2 mg/h, double the dose every 90 seconds to a maximum of 32 mg/h. The drug is light-sensitive and adsorbs to plastic tubing — must be delivered through a non-PVC (polyethylene) administration set and the syringe/bag protected from light. [1]
Where it shines: peri-operative/peri-procedural BP control, rapid up/down titration in fast-changing haemodynamics, transition to oral therapy. [1]
Cautions: the lipid-emulsion formulation means every mL delivers lipid load — monitor triglycerides if used >24 h; contraindicated in egg/soy allergy; does not protect against awareness (no analgesic/sedative effect). The VELOCITY trial (Peacock, Blood Press 2014) established efficacy and safety in acute severe HTN with very low rates of overshoot. [1]
Esmolol — aortic dissection and SVT
Mechanism: cardioselective beta-1 adrenergic antagonist. Metabolised by red blood cell esterases (t½ ≈ 9 minutes) — the shortest half-life of any beta-blocker. [1]
Pharmacokinetics: onset 1-2 min, offset within 10-20 min of stopping. Independence from renal/hepatic clearance (RBC esterase) makes it predictable in organ failure. [1]
Dosing: loading bolus 500 mcg/kg over 1 min, then infusion 50-300 mcg/kg/min (titrate up in 50 mcg/kg/min steps). For pure HR control (aortic dissection) esmolol is titrated to heart rate <60 bpm. [1]
Where it shines: acute aortic dissection (precise HR reduction is the primary therapeutic goal — the single most important determinant of flap propagation is dP/dt, driven by HR and SBP), supraventricular tachycardia with hypertension, thyroid storm (beta-blockade), peri-intubation hypertension/tachycardia. [1]
Cautions: bradycardia, hypotension, bronchospasm (beta-1 selectivity is lost at higher doses), negative inotropy in decompensated HF. Always pair with a vasodilator in aortic dissection once HR is controlled (esmolol alone may not achieve SBP 100-120). [1]
Hydralazine — the obstetric favourite
Mechanism: direct-acting arteriolar vasodilator — opens vascular smooth muscle K-channels (hyperpolarisation → relaxation) and may release NO. Acts predominantly on arterioles (afterload) with minimal venous effect. [1]
Pharmacokinetics: onset 10-30 min (slow and unpredictable — a major limitation), peak 20-40 min, duration 3-8 h (long and poorly titratable — once given you cannot "switch it off"). [1]
Dosing: 5-20 mg IV every 4-6 h (bolus dosing only — there is no effective infusion titration given the kinetics). Onset too slow and duration too long for fine BP control. [1]
Where it shines: pre-eclampsia/eclampsia — the drug with the longest, best-documented obstetric safety record (extensive cohort data; no teratogenicity; used alongside magnesium sulphate). In many UK/Australasian units it remains the preferred first-line IV agent in pregnancy alongside labetalol. [1]
Cautions: reflex tachycardia (can precipitate myocardial ischaemia — AVOID as monotherapy in aortic dissection or ACS), tachyphylaxis on repeated dosing, drug-induced lupus-like syndrome with chronic use (ANA-positive, resolves on withdrawal), headache, flushing, fluid retention. The unpredictable onset/duration is why it is discouraged in most non-obstetric emergencies where nicardipine or labetalol offer superior control. [1]
Nitroglycerin — for the heart, not for the BP
Mechanism: NO donor — predominantly a venodilator (preload reduction) with arteriolar effect only at higher doses. The venodilation reduces LV end-diastolic pressure and myocardial wall stress → reduced myocardial oxygen demand, and dilates coronary conduits (including collaterals) → improved coronary perfusion. [1]
Pharmacokinetics: onset 2-5 min, duration 5-10 min after stopping. Hepatic metabolism; tachyphylaxis develops within 12-24 h of continuous infusion. [1]
Dosing: start 5 mcg/min, titrate up by 5 mcg/min every 3-5 min to 200 mcg/min (arteriolar vasodilation typically requires >100 mcg/min). [1]
Where it shines: acute coronary syndromes (unstable angina/NSTEMI/STEMI with hypertension and ongoing ischaemia) and acute pulmonary oedema with hypertension (preload reduction is the mechanism — the BP falls as a side-benefit). It is NOT a primary antihypertensive — at low doses it does little to BP. [1]
Cautions: tachyphylaxis (must escalate dose), headache (venous sinus distension), methaemoglobinaemia at high/long doses (haemoglobin oxidised to metHb → functional anaemia, chocolate-brown blood; treat with methylene blue), worsening V/Q mismatch and hypoxaemia (vasodilates poorly-ventilated lung units), right-to-left shunt reversal in PFO. Absolutely AVOID in right ventricular infarction (preload-dependent) and in phosphodiesterase-5 inhibitor use (sildenafil — catastrophic hypotension). [1]
Sodium nitroprusside — potent but toxic
Mechanism: NO donor acting on both arterioles (afterload) and veins (preload) — the most potent IV antihypertensive available. Each molecule of nitroprusside releases five cyanide ions alongside NO. [1]
Pharmacokinetics: onset <30 seconds, offset 1-2 min — the fastest and most titratable agent (true second-by-second control). [1]
Dosing: 0.25 mcg/kg/min, titrate to effect up to a maximum of 10 mcg/kg/min. To minimise cyanide accumulation, keep infusion <4 mcg/kg/min and <48 h total wherever possible. [1]
Where it shines: now a drug of last resort — reserved for refractory hypertension unresponsive to nicardipine/labetalol/clevidipine, and for controlled hypotension in neurosurgery. Its speed and potency are unmatched, but its toxicity profile has displaced it from routine first-line use. [1]
Toxicity — the cyanide cascade:
- Cyanide toxicity manifests as rising lactate + metabolic acidosis with a normal/high PaO₂ (the "venous hyperoxia" — tissue extraction fails because cyanide poisons cytochrome c oxidase → histotoxic hypoxia). AV oxygen-difference narrows. Tachyphylaxis to escalating doses is an early warning sign.
- Risk factors: dose >4 mcg/kg/min, duration >48 h, renal/hepatic impairment (impaired cyanide→thiocyanate conversion and thiocyanate clearance), malnutrition (low thiosulfate stores).
- Treatment: stop the infusion; give sodium thiosulfate (a sulfur donor — converts cyanide to thiocyanate) ± hydroxocobalamin (binds cyanide → cyanocobalamin, excreted renally — the preferred antidote in smoke-inhalation cyanide poisoning); in severe cases sodium nitrite (induces methaemoglobinaemia — but contraindicated in concurrent CO poisoning).
- Thiocyanate toxicity (separate entity): accumulates in renal failure with prolonged infusion → confusion, psychosis, seizures, hyperreflexia, tinnitus. Removed by dialysis. [1]
Other cautions: cerebral vasodilation raises intracranial pressure (avoid in raised ICP/TBI), coronary steal (dilates non-stenosed vessels preferentially — avoid in ACS), rebound hypertension on abrupt withdrawal.[5][6]
Fenoldopam — the renal claim (controversial)
Mechanism: selective dopamine-1 (D1) receptor agonist — vasodilates renal, mesenteric, coronary and peripheral beds. Promotes natriuresis and increases renal blood flow. [1]
Pharmacokinetics: onset 5-10 min, duration 10-15 min. [1]
Dosing: 0.1-1.6 mcg/kg/min, titrated to BP target. [1]
Where it (theoretically) shines: the only IV antihypertensive that increases renal blood flow and natriuresis, prompting interest in hypertensive emergency with AKI. [1]
Reality check: despite physiological promise, no trial has demonstrated a clinical outcome benefit (no reduction in AKI progression, dialysis, or mortality) versus other agents. Reflex tachycardia, intraocular pressure rise (contraindicated in glaucoma), and high cost limit its use. It is a reasonable second-line option in hypertensive emergency with concomitant AKI but is not a first-line agent.[5]
Phentolamine — the alpha answer to catecholamine surges
Mechanism: competitive, non-selective alpha-1 and alpha-2 adrenergic antagonist — blocks catecholamine-mediated vasoconstriction at both receptor subtypes. [1]
Pharmacokinetics: onset 1-2 min, duration 10-30 min. [1]
Dosing: 1-5 mg IV bolus, repeat as needed (observe for dramatic BP response), or an infusion of 0.2-0.5 mg/min. [1]
Where it shines — the non-negotiable indication: pheochromocytoma crisis — the FIRST agent. Also: monoamine-oxidase inhibitor (MAOI)–tyramine hypertensive crisis, sympathomimetic overdose (amphetamines, cocaine — though benzodiazepines are first-line there), and reversal of noradrenaline/vasopressor extravasation (5-10 mg in 10 mL saline infiltrated subcutaneously around the extravasation site to reverse alpha-1 vasoconstriction and save the tissue). [1]
Critical sequencing rule: in pheochromocytoma you MUST establish alpha-blockade BEFORE beta-blockade. A beta-blocker given first leaves alpha-1-mediated vasoconstriction unopposed → catastrophic worsening hypertension and pulmonary oedema. Start phentolamine (or phenoxybenzamine orally pre-op, or the titratable IV alternative), achieve BP control, then add esmolol/labetalol for the tachyarrhythmia. [1]
Oral agents for chronic ICU blood pressure control
Once the acute emergency is controlled and the patient is ready to transition (typically when stable on a low IV infusion rate), convert to oral agents. The principles of chronic ICU BP control are identical to outpatient: combination therapy, attention to comorbidities (renal, cardiac, diabetes), and avoidance of drug interactions in the polypharmacy ICU patient. [1]
Oral antihypertensive classes for chronic ICU / step-down therapy
| Class | Mechanism | Representative agents | Best for | Key ICU cautions |
|---|---|---|---|---|
| ACE inhibitor | Blocks ACE → ↓AngII + ↑bradykinin | Enalapril, ramipril, lisinopril | HFrEF, post-MI, CKD (proteinuria), diabetes | AKI (esp. bilateral renal artery stenosis), hyperkalaemia, cough (bradykinin), angioedema; hold in AKI; contraindicated in pregnancy (fetopathy) |
| ARB | Blocks AngII type-1 receptor | Valsartan, losartan, candesartan | ACEi intolerance (cough/angioedema), HFrEF, CKD | Same renal/K+ cautions as ACEi; no cough/angioedema; NEVER combine ACEi + ARB |
| DHP calcium channel blocker | Vascular L-type Ca channel block | Amlodipine, nifedipine (long-acting), felodipine | Elderly, isolated systolic HTN, stroke prevention, AF | Ankle oedema, flushing, headache, gingival hyperplasia; safe in pregnancy |
| Non-DHP CCB | Cardiac L-type Ca channel (rate/inotropy) | Verapamil, diltiazem | Rate control (AF), angina | Bradycardia, heart block, constipation (verapamil), negative inotropy — avoid in HFrEF; avoid combination with beta-blocker (severe bradycardia) |
| Beta-blocker | β1 (cardioselective) / non-selective + alpha | Bisoprolol, metoprolol, carvedilol, nebivolol | HFrEF (the mortality-reducing trio), post-MI, AF rate control, ischaemic heart disease | Bradycardia, bronchospasm, masking hypoglycaemia, fatigue; do NOT stop abruptly (rebound); most are NOT first-line for uncomplicated HTN in the elderly |
| Thiazide / thiazide-like diuretic | Na-Cl cotransporter in DCT → natriuresis | Chlorthalidone, hydrochlorothiazide, indapamide | Volume-overload HTN, heart failure, elderly, stroke prevention | Hypokalaemia, hyponatraemia, hyperuricaemia (gout), hyperglycaemia, hypercalcaemia; chlorthalidone > HCTZ for potency/duration |
| Loop diuretic | Na-K-2Cl in loop of Henle | Furosemide, bumetanide, torsemide | HFrEF with congestion, CKD (when GFR too low for thiazide) | Hypokalaemia, hypomagnesaemia, contraction alkalosis, ototoxicity (high-dose IV) |
| Aldosterone antagonist | Competitive mineralocorticoid receptor block | Spironolactone, eplerenone | Resistant HTN, HFrEF (mortality), primary hyperaldosteronism | Hyperkalaemia (esp. with ACEi/ARB + AKI), gynaecomastia (spironolactone) |
| Alpha-1 blocker | Selective alpha-1 blockade | Doxazosin, prazosin, terazosin | Benign prostatic hyperplasia + HTN; resistant HTN 4th-line | First-dose syncope (postural hypotension), NOT first-line HTN monotherapy (ALLHAT — more heart failure events) |
| Centrally acting | Alpha-2 agonist → ↓sympathetic outflow | Clonidine, methyldopa, moxonidine | Resistant HTN; methyldopa = pregnancy HTN; clonidine patch for adherence | Rebound hypertension on abrupt withdrawal (clonidine); sedation, dry mouth; methyldopa → Coombs-positive haemolysis, drug-induced hepatitis |
| Direct vasodilator (oral) | Arteriolar K-channel / NO | Minoxidil, hydralazine (oral) | Resistant/refractory HTN (minoxidil = last-line oral) | Reflex tachycardia (MUST combine with beta-blocker + diuretic), sodium retention, hypertrichosis (minoxidil), drug-lupus (hydralazine) |
Resistant hypertension = BP above target despite three agents at optimal doses including a diuretic. The fourth-line additions are spironolactone (the most effective, PATHWAY-2), then a beta-blocker or an alpha-blocker. Always exclude a secondary cause before labelling "resistant" — especially primary aldosteronism (the most common curable cause), renal artery stenosis, obstructive sleep apnoea, and (the exam favourite) phaeochromocytoma.[1]
Scenario-specific management — the critical "drug-first" rules

Hypertensive emergency — scenario-specific drug selection, target and timeframe
-
GENERAL PRINCIPLE (applies to all emergencies except aortic dissection):
- Reduce MAP by 10-20% in the first hour.
- Then gradually reduce to ~160/100 mmHg over the next 2-6 hours.
- Use a titratable IV infusion (labetalol, nicardipine, clevidipine) via arterial line.
- Do NOT normalise BP in the first hour (risk of watershed infarction from dropping below the autoregulatory floor).[2]
-
AORTIC DISSECTION — the exception (rapid + aggressive):
- STEP 1 — BETA-BLOCKER FIRST (to reduce dP/dt — the propagating force on the flap). Esmolol (titrate to HR <60 bpm) or labetalol. Give this BEFORE any vasodilator.
- STEP 2 — VASODILATOR once HR controlled: add nicardipine or clevidipine (or nitroprusside) to bring SBP to 100-120 mmHg.
- Target: HR <60, SBP 100-120 — and maintain until pain resolves and surgery/TEVAR is performed.
- WHY beta-first: a pure vasodilator → reflex tachycardia → increased dP/dt → propagation of the dissection. This sequence is non-negotiable.[4]
-
HYPERTENSIVE ENCEPHALOPATHY:
- Drug: labetalol or nicardipine (maintain cerebral perfusion; avoid cerebral vasodilators that raise ICP, i.e. nitroprusside).
- Target: reduce MAP by 10-20% in the first hour, then 160/100 over 2-6 h.
- The rightward-shifted autoregulation curve means excessive reduction → watershed cerebral infarction. [1]
-
ACUTE ISCHAEMIC STROKE:
- Do NOT lower BP unless: BP >220/120, or patient is a candidate for thrombolysis (then lower to <185/110 before, and <180/105 for 24 h after).
- Drug: nicardipine or labetalol (labetalol may reduce cerebral perfusion in some). Avoid nitroprusside (raises ICP). [1]
-
ACUTE INTRACEREBRAL HAEMORRHAGE (ICH):
- Lower SBP to 140-160 mmHg (INTERACT2/ATACH2 — modest reduction is safe; over-aggressive reduction <130 may worsen).[2]
- Drug: nicardipine (first-line), labetalol.
-
ACUTE CORONARY SYNDROME (ACS):
- Drug: nitroglycerin (coronary vasodilation + preload reduction) ± a beta-blocker (esmolol/metoprolol — reduces myocardial oxygen demand; but AVOID in acute decompensated HF, hypotension, second-degree block).
- Target: reduce SBP to <140 mmHg while preserving coronary perfusion; relieve ongoing ischaemia.
- Do NOT use hydralazine (reflex tachycardia → ischaemia) or nitroprusside (coronary steal). [1]
-
ACUTE PULMONARY OEDEMA (cardiogenic):
- Drug: nitroglycerin (preload reduction) + loop diuretic (furosemide) ± an arteriolar vasodilator (clevidipine/nicardipine) if BP remains high.
- Avoid: labetalol/carvedilol (negative inotrope — until the acute decompensation is treated), hydralazine (reflex tachycardia in failing heart). [1]
-
PRE-ECLAMPSIA / ECLAMPSIA:
- Drug: labetalol (first-line in many protocols) or hydralazine (the traditional favourite). Nifedipine (oral) is an accepted alternative/adjunct. AVOID ACEi/ARB (fetotoxic) and nitroprusside (fetal cyanide).
- Target: SBP <160 and DBP <110 (avoid overshoot → placental hypoperfusion).
- ALWAYS give magnesium sulphate for seizure prophylaxis (eclampsia prevention/treatment) — this is the priority intervention alongside BP control. [1]
-
PHEOCHROMOCYTOMA CRISIS — the cardinal sequence:
- STEP 1 — ALPHA-BLOCKER FIRST: phentolamine (IV bolus 1-5 mg, repeat) — establish alpha-blockade and control BP.
- STEP 2 — BETA-BLOCKER (esmolol/labetalol) ONLY AFTER adequate alpha-blockade — to control the reflex tachycardia/tachyarrhythmia.
- NEVER give a beta-blocker FIRST — unopposed alpha-1 stimulation → catastrophic hypertension + pulmonary oedema.
- Pre-operative preparation uses oral phenoxybenzamine (irreversible alpha-blocker) for 1-2 weeks before adrenalectomy, followed by beta-blocker. [1]
-
COCAINE / SYMPATHOMIMETIC-induced hypertension:
- FIRST-LINE: benzodiazepines (diazepam/lorazepam) — reduce central sympathetic drive; lowers BP and reduces agitation/mydriasis/tremor.
- AVOID beta-blockers — unopposed alpha stimulation (beta-blockade unmasks alpha-mediated vasoconstriction) → paradoxical worsening hypertension and vasospasm. (Modern evidence: labetalol/ carvedilol with alpha activity may be safer, but the conservative, exam-correct answer is benzodiazepines first; add a pure alpha-blocker like phentolamine if refractory.)
- Avoid nitroprusside if possible (coronary steal in cocaine-induced vasospasm). [1]
-
ACUTE RENAL FAILURE / SCLERODERMA RENAL CRISIS:
- Scleroderma renal crisis: ACE inhibitor is the disease-modifying drug (enalaprilat IV acutely, then oral captopril/enalapril) — dramatically changed prognosis. Do not withhold even in AKI.
- For BP control in AKI: nicardipine, clevidipine, or fenoldopam (theoretical renal advantage); avoid nitroprusside (thiocyanate/cyanide accumulate).
Clinical pearls
SAQ — Hypertensive emergency drug selection
10 minutes · 10 marks
A 58-year-old man presents with sudden tearing chest pain radiating to the back. BP 210/118 (right arm), HR 112, equal femoral pulses. CT confirms acute Stanford type A aortic dissection. He is transferred to your ICU while cardiac surgery prepares the theatre.
Key evidence and trials
Perez & Musini — Cochrane review of IV antihypertensives (PMID 18254026)
Systematic review — 15 RCTs, 869 patients
Population: Adults presenting with a hypertensive emergency
Key finding
NO RCT evidence that any IV antihypertensive reduces mortality or morbidity in hypertensive emergency. Insufficient evidence to determine which drug or class is most effective. Minor differences in degree of BP lowering between classes (clinical significance unknown).
Practice change
Drug choice in hypertensive emergency is driven by PATHOPHYSIOLOGY and the type of organ damage, pharmacological properties, and expert consensus — NOT by head-to-head mortality trials. The scenario-specific rules (beta-first in dissection, alpha-first in pheochromocytoma) are physiologically mandated, not RCT-derived.
van den Born et al. — ESC Council on Hypertension position document (PMID 30165588)
Expert position document (European Society of Cardiology Council on Hypertension)
Population: Adults with hypertensive emergencies
Key finding
The type of acute HMOD is the principal determinant of: (i) the drug of choice, (ii) the target BP, and (iii) the timeframe for reduction. Patients without acute HMOD do NOT have an emergency — treat with oral agents and observe. Recommends labetalol, nicardipine, clevidipine, and esmolol as the modern titratable workhorses; relegates nitroprusside on toxicity grounds.
Practice change
Map the DRUG, TARGET, and TIMEFRAME to the specific organ damage. Labetalol/nicardipine for most; esmolol + vasodilator for dissection; nitroglycerin for ACS/oedema; hydralazine/labetalol for pre-eclampsia.
Hiratzka et al. — ACCF/AHA Thoracic Aortic Disease guideline (PMID 20233780)
Multisociety clinical practice guideline
Population: Patients with thoracic aortic disease, including acute aortic dissection
Key finding
Class I recommendation: in acute aortic dissection, reduce heart rate to ≤60 bpm and SBP to 100-120 mmHg with IV beta-blockade first, then add titratable vasodilators. Beta-blockade must precede vasodilation to prevent reflex tachycardia and increased dP/dt propagating the dissection.
Practice change
The beta-blocker-first rule in aortic dissection is a Class I guideline mandate. HR control (≤60) is as important as BP control (SBP 100-120), and the sequence (beta then vasodilator) is non-negotiable.
Red flags
Prognosis
Outcomes by scenario and the impact of correct drug selection
| Scenario | Target / timeframe | Correct first drug | Consequence of wrong choice |
|---|---|---|---|
| General hypertensive emergency | MAP −10-20% in 1 h → 160/100 over 2-6 h | Labetalol or nicardipine | Precipitous drop → watershed infarct; too slow → ongoing organ damage |
| Aortic dissection | HR <60 + SBP 100-120 (rapid) | Esmolol/labetalol FIRST, then vasodilator | Vasodilator alone → reflex tachycardia → flap propagation → death |
| Hypertensive encephalopathy | MAP −10-20% in 1 h | Labetalol or nicardipine | Nitroprusside → raised ICP; over-reduction → cerebral infarction |
| Pheochromocytoma crisis | Controlled BP + HR | Phentolamine FIRST, then beta-blocker | Beta-blocker alone → unopposed alpha → catastrophic hypertension |
| Cocaine / sympathomimetic | BP control + sedation | Benzodiazepines FIRST | Beta-blocker → unopposed alpha → vasospasm, MI |
| Acute ischaemic stroke | Treat only if >220/120 (or <185/110 for lysis) | Nicardipine, labetalol | Over-reduction → infarct core extension |
| ICH | SBP 140-160 | Nicardipine | SBP <130 (ATACH-2) → possible renal dysfunction, no benefit |
| ACS | SBP <140 + relieve ischaemia | Nitroglycerin + beta-blocker | Hydralazine → reflex tachycardia → ischaemia; nitroprusside → coronary steal |
| Acute pulmonary oedema | Reduce preload + BP | Nitroglycerin + loop diuretic | Labetalol/hydralazine (negative inotrope/reflex tachy) in failing heart |
| Pre-eclampsia/eclampsia | SBP <160, DBP <110 | Labetalol or hydralazine + magnesium | ACEi/ARB → fetotoxicity; nitroprusside → fetal cyanide |
| Scleroderma renal crisis | Controlled BP | ACE inhibitor (disease-modifying) | Withholding ACEi → irreversible renal failure |
Drug-toxicity outcomes — the signature adverse effects
| Drug | Signature toxicity | Consequence if missed |
|---|---|---|
| Nitroprusside | Cyanide (lactate↑, acidosis, normal PaO₂) + thiocyanate (renal failure) | Fatal histotoxic hypoxia; psychosis/seizures |
| Nitroglycerin | Tachyphylaxis (12-24h) + methaemoglobinaemia | Loss of BP/ischaemia control; functional cyanosis (chocolate blood) |
| Hydralazine | Reflex tachycardia + drug-induced lupus (chronic) | Myocardial ischaemia in CAD/dissection; lupus syndrome |
| ACEi/ARB | AKI (bilateral RAS), hyperkalaemia, cough/angioedema | Dialysis-requiring AKI; life-threatening angioedema |
| Clonidine | Rebound hypertension on abrupt withdrawal | Hypertensive emergency on withdrawal |
| Minoxidil | Reflex tachycardia + pericardial effusion + hypertrichosis | Pericardial tamponade; tachyarrhythmia |
Bottom line for the exam: the fellowship candidate must know (1) the emergency/urgency distinction, (2) the general controlled-reduction target with the aortic dissection exception, (3) the receptor-level reason for alpha-before-beta in pheochromocytoma and beta-before-vasodilator in aortic dissection, (4) the cyanide signature of nitroprusside, (5) that benzodiazepines, not beta-blockers, come first in cocaine-induced hypertension, and (6) the pregnancy rules (labetalol/hydralazine + magnesium; ACEi/ARB contraindicated).[1][2][6]
References
- [1]Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines Hypertension, 2018.PMID 29133356
- [2]van den Born BH, Lip GYH, Brguljan-Hitij J, et al. ESC Council on hypertension position document on the management of hypertensive emergencies Eur Heart J Cardiovasc Pharmacother, 2019.PMID 30165588
- [3]Perez MI, Musini VM. Pharmacological interventions for hypertensive emergencies Cochrane Database Syst Rev, 2008.PMID 18254026
- [4]Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine Circulation, 2010.PMID 20233780
- [5]Varon J. Treatment of acute severe hypertension: current and newer agents Drugs, 2008.PMID 18257607
- [6]Marik PE, Varon J. Clinical review: the management of hypertensive crises Crit Care, 2003.PMID 12974970