ICU · Pharmacology
Antimicrobials (by Class) — Mechanisms, Spectrum & Resistance
Also known as Antimicrobials · Antibiotics · Bactericidal · Bacteriostatic · Mechanism of action · Antibiotic resistance
Antimicrobials by class and mechanism: cell wall (beta-lactams, glycopeptides — bactericidal), protein synthesis (aminoglycosides 30S, macrolides 50S, tetracyclines 30S, linezolid 50S), DNA (fluoroquinolones DNA gyrase), RNA (rifampicin RNA polymerase), folic acid (trimethoprim/sulfamethoxazole). Time-dependent (beta-lactams, macrolides — T above MIC) vs concentration-dependent (aminoglycosides, fluoroquinolones — Cmax/MIC). PK/PD principles. Resistance mechanisms.
On this page & tools
Your progress
Saved locally on this device.
Target exams

Overview & definition
Antimicrobials — by the target: the cell wall, the protein synthesis, the DNA, the RNA, the folic acid. The bactericidal vs the bacteriostatic. The PK/PD (the time-dependent vs the concentration-dependent). The resistance.[1]
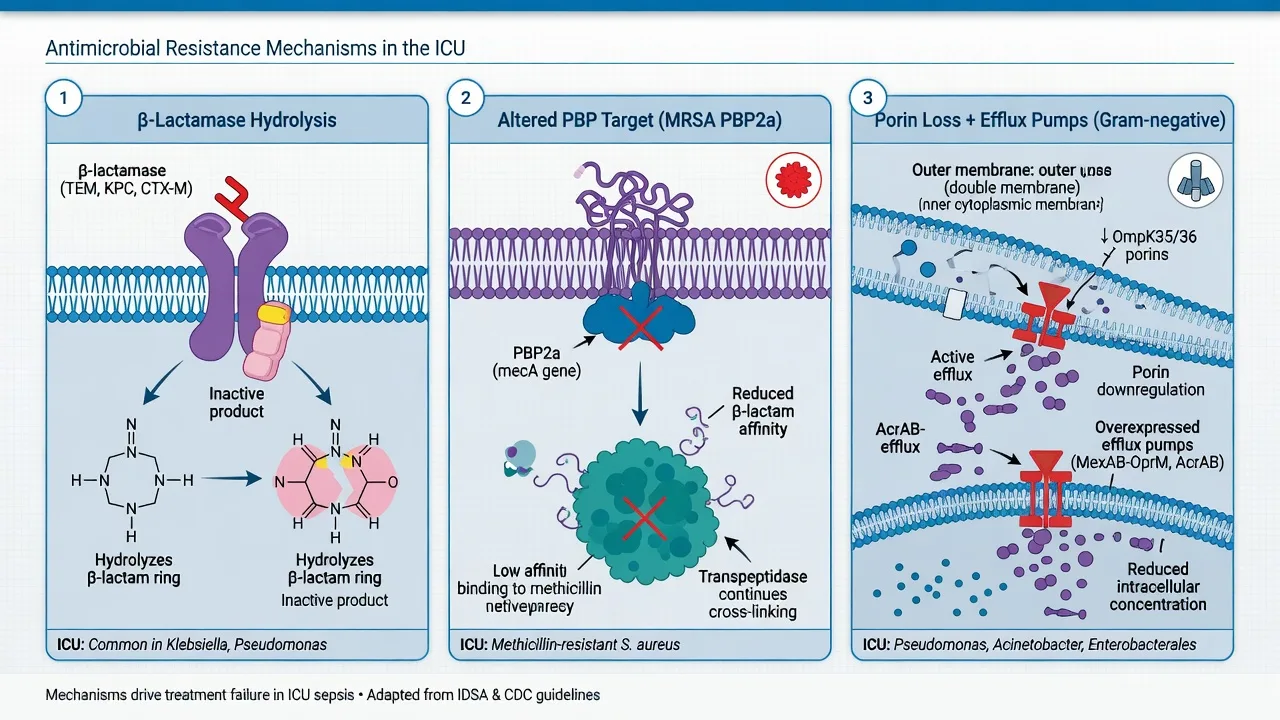
The ICU intensivist must know: (1) which class covers which organism; (2) the mechanism at the target (cell wall, ribosome, DNA, RNA, folate) — this predicts synergy, antagonism and resistance; (3) the PK/PD index that drives killing — T>MIC (time-dependent) vs Cmax/MIC or AUC/MIC (concentration-dependent) — because this dictates dosing strategy (prolonged/continuous infusion vs once-daily); (4) the toxicity profile (nephrotoxicity, QT, marrow suppression, C. difficile); and (5) the resistance mechanism (beta-lactamases, target modification, porin loss, efflux) — because this dictates escalation to newer agents (ceftazidime-avibactam, ceftolozane-tazobactam, colistin, plazomicin).[1][13]
By target
| Target | Class | Mechanism | Example |
|---|---|---|---|
| Cell wall | Beta-lactams | Transpeptidase (PBP) | Penicillins, cephalosporins, carbapenems |
| Cell wall | Glycopeptides | D-Ala-D-Ala binding | Vancomycin |
| Cell membrane | Lipopeptides | Membrane depolarisation | Daptomycin |
| 30S ribosome | Aminoglycosides | Misreading (bactericidal) | Gentamicin |
| 30S ribosome | Tetracyclines | Block tRNA binding | Doxycycline, tigecycline |
| 50S ribosome | Macrolides | Block translocation | Azithromycin |
| 50S ribosome | Oxazolidinones | Block initiation | Linezolid |
| DNA | Fluoroquinolones | DNA gyrase/topoisomerase IV | Ciprofloxacin |
| RNA | Rifampicin | RNA polymerase | Rifampicin |
| Folic acid | TMP-SMX | DHFR/DHPS | Cotrimoxazole |
| DNA | Nitroimidazoles | Radical DNA damage | Metronidazole |
Beta-lactam antibiotics
All share the beta-lactam ring; all bind penicillin-binding proteins (PBPs) — transpeptidases that cross-link peptidoglycan — and are bactericidal (autolysis of a defective wall). Bacterial killing is time-dependent (T>MIC). The four sub-families differ in their ring fusion (and therefore PBP affinity and beta-lactamase stability).[1]
Penicillins (thiazolidine + beta-lactam = penam ring)
| Sub-class | Examples | Spectrum |
|---|---|---|
| Narrow | Benzylpenicillin, phenoxymethylpenicillin | Streptococci, enterococci, meningococci, syphilis, leptospirosis, listeria |
| Anti-staphylococcal (Mssa only — stable to staph penicillinase) | Flucloxacillin, dicloxacillin, nafcillin, oxacillin | MSSA, streptococci — NOT MRSA, NOT enterococci, NOT gram-negatives |
| Aminopenicillins | Amoxicillin, ampicillin | As narrow + E. coli, H. influenzae, Listeria, enterococci, Proteus |
| Anti-pseudomonal (ureidopenicillins) | Piperacillin (±tazobactam), ticarcillin (±clavulanate) | Gram-negatives incl. Pseudomonas, anaerobes (Bacteroides), enterococci |
Beta-lactamase inhibitors (suicidal, "suicide substrates"): clavulanate, tazobactam, sulbactam — inhibit class A serine beta-lactamases (staph penicillinase, TEM, SHV) but NOT AmpC or carbapenemases; avibactam and relebactam (diazabicyclooctanes) additionally restore activity against some AmpC and KPC carbapenemases; vaborbactam (boronic acid) inhibits KPC.[13]
Cephalosporins (dihydrothiazine + beta-lactam = cephem ring)
Generated by successive modification; each generation broadens gram-negative cover (incl. Pseudomonas from the 3rd) at some cost to gram-positive activity (especially 4th-gen loses staph cover). Cross the placenta and BBB (1st-gen poorly; 3rd-gen well — used in meningitis).[3]
| Generation | Examples | Key spectrum | Note |
|---|---|---|---|
| 1st | Cephalexin, cefazolin, cefadroxil | Gram-positives (MSSA, strep), some enterobacterales — NOT Pseudomonas, NOT listeria, NOT enterococci | Surgical prophylaxis; staph skin/soft tissue |
| 2nd | Cefuroxime, cefoxitin, cefotetan | Gram-pos + gram-neg (H. influenzae, Neisseria, some enterobacterales); cefoxitin/cefotetan = anti-anaerobe (Ceph-2 used in pelvic) | Cefoxitin = inducer screen for AmpC |
| 3rd | Ceftriaxone, cefotaxime, ceftazidime | Broad gram-neg incl. Pseudomonas (ceftazidime only), listeria/meningitis (ceftriaxone/cefotaxime); biliary (ceftriaxone), pyelonephritis, meningitis, gonorrhoea | Ceftriaxone = once-daily (biliary); ceftazidime = Pseudomonas but NO gram-positive; ceftazidime-avibactam (KPC) |
| 4th | Cefepime, cefpirome | Broad gram-pos + gram-neg incl. Pseudomonas; zwitterion = faster porin entry (stable to AmpC) | Cefepime neurotoxicity — encephalopathy/myoclonus/NCSE in renal failure (reduce dose for CrCl)[7] |
| 5th | Ceftaroline | As 3rd + MRSA (binds PBP2a); NOT Pseudomonas, NOT ESBL | The ONLY beta-lactam active against MRSA |
Ceftaroline is unique: its bulky side-chain binds the PBP2a of MRSA (ceftaroline-fosamil is the prodrug). It has no anti-pseudomonal activity and is not stable against ESBL/AmpC/carbapenemases.[4]
Carbapenems (carbon replacing sulphur + trans double bond — small, penetrates porins)
| Drug | Spectrum |
|---|---|
| Imipenem | Broadest beta-lactam — gram-pos, gram-neg (incl. ESBL, AmpC), anaerobes, Pseudomonas, Acinetobacter — inactivated by renal dehydropeptidase-I (given with cilastatin); seizures at high dose/CrCl |
| Meropenem | As imipenem, dehydropeptidase-stable (no cilastatin), lower seizure risk — drug of choice for ESBL/AmpC sepsis, nosocomial meningitis |
| Ertapenem | As imipenem BUT NO Pseudomonas, NO Acinetobacter, NO Enterococcus — once-daily; useful for ESBL urinary/abdominal, ESBLStep — cheap, Pseudomonas-sparing |
| Doripenem | As meropenem; lower seizure risk |
Carbapenems are the workhorse for ESBL and AmpC; they are NOT reliable when a carbapenemase (KPC, NDM, VIM, IMP, OXA-48) is present.[6][12]
Monobactams (single beta-lactam ring, no fusion)
Aztreonam — the only monobactam. Binds PBP3 of gram-negatives only; active against Pseudomonas, ESBL Enterobacterales, H. influenzae; no gram-positive cover, no anaerobe cover. Unique: minimal cross-reactivity with other beta-lactams (the side-chain, not the ring, drives allergy) — therefore safe in penicillin/cephalosporin allergy (including anaphylaxis), and is the renal-friendly option in patients needing ceftazidime-like cover. Ceftazidime and aztreonam share a side-chain, so avoid if ceftazidime-allergic.[3]
Glycopeptides — vancomycin & teicoplanin
Bind D-Ala-D-Ala terminus of the peptidoglycan precursor, sterically blocking transglycosylation/transpeptidation (cell wall). Bactericidal (slow, time-dependent — AUC/MIC driver). Active only against gram-positive organisms (the large molecule cannot cross the gram-negative outer membrane).[1][4]
- Vancomycin — MRSA, MRSE, ampicillin-resistant enterococci, Clostridioides difficile (oral, non-absorbed). Loading 25-30 mg/kg (IBW), then 15-20 mg/kg q8-12h guided by trough 15-20 mg/L (severe/MRSA bacteraemia) or AUC/MIC 400-600 (now preferred — Bayesian dosing). Nephrotoxicity (especially with piperacillin-tazobactam — "vanc-piptazo AKI"), infusion-related histamine release (red-man syndrome — rate-related, NOT IgE; slow infusion, antihistamine), ototoxicity (rare, at high levels), thrombocytopenia.
- Teicoplanin — longer half-life (so once-daily), less nephrotoxic than vancomycin, no red-man syndrome (can bolus). Used where available (Europe/ANZ, NOT USA). Needs loading (6 mg/kg q12h ×3, then daily).[4]
Lipopeptides — daptomycin
Binds the bacterial cytoplasmic membrane (calcium-dependent insertion) → depolarisation, potassium efflux, cell death — a mechanism independent of cell wall or ribosome, so no cross-resistance with beta-lactams/glycopeptides. Bactericidal, concentration-dependent (Cmax/MIC). Active against gram-positive only (cannot cross gram-negative membrane): MRSA, VRE (E. faecium), penicillin-resistant pneumococci. 4-6 mg/kg IV once-daily (10 mg/kg for endocarditis).[4]
Killed by surfactant → CONTRAINDICATED in pneumonia (use vancomycin/linezolid). Monitor creatine kinase weekly (skeletal-muscle toxicity — rhabdomyolysis rare); statins potentiate. Eosinophilic pneumonia is rare but reported with prolonged therapy.[6]
Aminoglycosides — gentamicin, amikacin, tobramycin
Bind the 30S ribosomal subunit (16S rRNA, A-site) → misreading of mRNA → faulty proteins inserted into the membrane → bactericidal (one of the few static-ribosomal agents that is cidal). Concentration-dependent killing + significant post-antibiotic effect (PAE) → once-daily extended-interval dosing (e.g. 5-7 mg/kg gentamicin, Hartford nomogram) optimises Cmax/MIC and reduces accumulation/ototoxicity. Active against gram-negative aerobes (Enterobacterales, Pseudomonas) and synergy with cell-wall agents for enterococci/streptococci (gentamicin + ampicillin in enterococcal endocarditis); no anaerobic activity (needs aerobic uptake — oxygen-dependent transport).[1]
Toxicity (both concentration-and duration-dependent): (1) nephrotoxicity — proximal tubular (accumulates in renal cortex) — usually reversible on stopping; potentiated by vancomycin, amphotericin, loop diuretics, hypovolaemia; (2) ototoxicity — cochlear (amikacin) and vestibular (gentamicin) hair-cell destruction — irreversible; (3) neuromuscular blockade (rare, myasthenia). Avoid in pregnancy (8th-nerve foetal damage). TDM essential (trough <1 mg/L, or area-under-curve monitoring). Amikacin is least susceptible to aminoglycoside-modifying enzymes.[1]
Fluoroquinolones — ciprofloxacin, levofloxacin, moxifloxacin
Inhibit DNA gyrase (gram-negatives) and topoisomerase IV (gram-positives) → double-strand DNA breaks → bactericidal, concentration-dependent (AUC/MIC). Excellent tissue penetration (intracellular — Legionella, Mycoplasma, Chlamydia, Mycobacteria; prostate, bone, lung) and high oral bioavailability (PO ≈ IV).[1]
| Drug | Spectrum |
|---|---|
| Ciprofloxacin | Best gram-negative (incl. Pseudomonas); weak gram-positive; poor streptococcal/pneumococcal — NOT for CAP |
| Levofloxacin | Better pneumococcus + atypicals (respiratory FQ); still Pseudomonas |
| Moxifloxacin | Best pneumococcus/atypicals + anaerobes; NO Pseudomonas, NO urinary tract (biliary/faecal elimination) |
Adverse effects (the FQ "boxed warnings"): QT prolongation (torsades — avoid with other QT drugs, hypokalaemia); tendinopathy/tendon rupture (Achilles — risk within weeks, worse with steroids, age >60); aortic dissection/aneurysm (Marfan/Ehlers-Danlos caution); CNS (confusion, seizures, psychosis — lower threshold with theophylline); dysglycaemia (both hypo and hyper); C. difficile. Avoid in pregnancy/children (cartilage damage in animal studies). Chelates with Ca/Mg/Fe/Al/sucralfate (separate by 2 h).[5]
Macrolides — azithromycin, clarithromycin
Bind the 50S ribosomal subunit (23S rRNA, P-site of peptidyl transferase) → block translocation → bacteriostatic (bactericidal at high concentration). Cover: gram-positives (strep, pneumococcus), atypicals (Legionella, Mycoplasma, Chlamydia), Bordetella, Helicobacter, some non-tuberculous mycobacteria. CYP3A4 inhibitors (clarithromycin > erythromycin; azithromycin does NOT inhibit CYP3A4 — preferred for drug-interaction risk).[1]
Adverse: QT prolongation (erythro > azithro; torsades risk); nausea/diarrhoea (motilin-agonist — erythromycin used as a prokinetic); cholestatic hepatitis; ototoxicity (high dose, renal failure); clarithromycin interacts with statins (rhabdomyolysis), warfarin (↑INR), calcineurin inhibitors (↑levels), tacrolimus. P450 inhibition — avoid with many drugs.[13]
Tetracyclines & glycylcyclines — doxycycline, tigecycline
Bind the 30S ribosomal subunit (A-site) → block tRNA binding → bacteriostatic. Wide spectrum: atypicals, Rickettsia, Borrelia (Lyme), Chlamydia, Mycoplasma, Vibrio, Leptospira, Plasmodium (doxy malaria prophylaxis), MRSA, Acinetobacter; anaerobes (tigecycline).[1]
- Doxycycline — once/twice-daily, well-tolerated, the atypical/rickettsial agent; oesophagitis (take with water, upright); photosensitivity; chelation (Ca/Mg/Fe — separate); avoid in pregnancy/children <8 (tooth discolouration, bone).
- Tigecycline (glycylcycline, broad-spectrum, IV only) — active against MRSA, VRE, ESBL, anaerobes, atypicals; NOT Pseudomonas, NOT Proteus/Providencia/Morganella (intrinsic resistance). FDA black-box: increased mortality in ventilator-acquired pneumonia (VAP) — failure of Acinetobacter/Pseudomonas; reserve for cSSTI/cIAI. Nausea common; hypoalbuminaemia lowers unbound levels.[10]
Oxazolidinones — linezolid
Bind the 50S ribosomal subunit (23S rRNA, A-site) → block initiation complex formation (distinct site from macrolides/chloramphenicol) → bacteriostatic. Active against gram-positives only: MRSA, VRE (E. faecium, E. faecalis), penicillin-resistant pneumococci; 100% oral bioavailability (PO ≡ IV).[4]
Adverse (duration-dependent): thrombocytopenia (and anaemia/neutropenia) — risk >14 days, monitor FBC; peripheral + optic neuropathy (long courses); serotonin syndrome (linezolid is a weak reversible MAO inhibitor — avoid/co-monitor with SSRIs, tramadol, linezolid-tyramine foods); lactic acidosis (mitochondrial toxicity); non-specific Cheyne-Stokes reported. No renal dose adjustment (linezolid metabolites cleared renally but active drug is hepatic). Teixobactin (investigational) — unrelated membrane-acting agent, no cross-resistance.[11]
Nitroimidazoles — metronidazole
Prodrug — reduced inside the organism (anaerobes, microaerophilic; ferredoxin) → cytotoxic radical intermediates damage DNA → bactericidal, concentration-dependent. Cover: anaerobes (Bacteroides, Clostridium, Fusobacterium), protozoa (Giardia, Entamoeba, Trichomonas), H. pylori, C. difficile (oral for CDI). 100% bioavailability. Disulfiram-like reaction with alcohol; peripheral neuropathy (long courses); encephalopathy/cerebellar signs (rare); metallic taste. Warfarin potentiation (CYP2C9 inhibition). Excellent CSF penetration (brain abscess).[5]
Antifungals — azoles, amphotericin, echinocandins
| Class | Mechanism | Agents | Spectrum / notes |
|---|---|---|---|
| Polyenes | Bind ergosterol → membrane pore → leak/death (bactericidal/fungicidal) | Amphotericin B (deoxycholate); liposomal amphotericin (AmBisome); lipid complex | Broadest antifungal (Candida, Aspergillus, Cryptococcus, Mucorales, Histoplasma). Nephrotoxicity (afferent arteriole vasoconstriction + distal tubule — distal RTA, K/Mg wasting); infusion reactions; anaemia. Lipid forms reduce nephrotoxicity. Mucormycosis needs high-dose lipo-AmB. Saline pre-load + electrolyte repletion limit AKI. |
| Azoles | Inhibit lanosterol 14-alpha-demethylase (ergosterol synthesis, cytochrome P450) | Fluconazole (Candida/Crypto — NOT moulds; CSF; good bioavail); voriconazole (Aspergillus + some Scedosporium/Fusarium; CSF; photosensitivity; visual disturbance; hepatotoxic); posaconazole (Mucorales, Aspergillus, Candida prophylaxis); isavuconazole (moulds incl. Mucorales; SHORTENS QT — opposite of others; better tolerated); itraconazole | All CYP3A4 inhibitors (voriconazole strong; fluconazole moderate) — interact with tacrolimus/sirolimus/warfarin/statins. QT prolongation (except isavuconazole). Hepatotoxicity. Voriconazole TDM (target 1-5.5 mg/L). |
| Echinocandins | Inhibit beta-1,3-glucan synthase → cell wall (no mammalian target → low toxicity) | Caspofungin, micafungin, anidulafungin | First-line for Candida (incl. azole-resistant C. glabrata/krusei); candidemia, intra-abdominal candidiasis; salvage aspergillosis. Fungicidal for Candida. Minimal toxicity — infusion reaction (histamine), transaminitis, headache. Hepatic metabolism (caspofungin — reduce dose in Child-Pugh B/C). |
| Flucytosine (5-FC) | Converted to 5-FU → inhibits DNA/RNA synthesis | Flucytosine | Used with amphotericin for Cryptococcus meningitis (clears CSF faster). Bone marrow toxicity (cytopenias); always combined (mono → rapid resistance); reduce dose in renal failure. |
Empiric candidemia in non-neutropenic ICU: echinocandin (caspofungin/micafungin/anidulafungin) is first-line; step-down to fluconazole when C. albicans and stable.[8] Invasive aspergillosis: voriconazole is first-line.[9]
PK/PD principles
- Time-dependent (beta-lactams, macrolides, linezolid) — the efficacy depends on the TIME the free drug exceeds the MIC (T above MIC). The prolonged infusion / the continuous infusion optimises.[1][3]
- Concentration-dependent (aminoglycosides, fluoroquinolones, daptomycin, metronidazole, amphotericin) — the efficacy depends on the PEAK (Cmax/MIC). The once-daily dosing (the aminoglycoside) optimises.[1]
- Concentration-dependent with time component (fluoroquinolones, linezolid, vancomycin, azithromycin, tigecycline, daptomycin) — the AUC/MIC ratio is the best PK/PD predictor (vancomycin AUC/MIC 400-600 for MRSA; fluoroquinolone AUC/MIC >125 gram-neg / >30 gram-pos).[4]
ICU empiric therapy principles — broad spectrum then narrow
In sepsis/septic shock, the priority is to deliver effective antibiotics within 1 hour of recognition — each hour of delay in hypotensive septic shock increases mortality ~4-8% (Kumar 2006; Seymour 2017). The Surviving Sepsis Campaign 2021 gives a strong recommendation for empiric broad-spectrum therapy within one hour for septic shock or high-likelihood sepsis.[2][13]
Principles:[6]
- Broad-spectrum empiric cover from the first dose — aim to cover all likely pathogens at the suspected source. The regimen is dictated by source, patient risk, local resistance — not by "strongest drug". Typical regimens:
- Community sepsis (lung/urine/biliary) — benzylpenicillin/amoxycillin + gentamicin ± metronidazole; or ceftriaxone ± azithromycin (CAP); or amoxycillin-clavulanate (biliary).
- Hospital-acquired / VAP / intra-abdominal / neutropenic sepsis — anti-pseudomonal beta-lactam (piperacillin-tazobactam, ceftazidime, cefepime, meropenem) ± second agent for MRSA (vancomycin/linezolid) ± aminoglycoside/fluoroquinolone for resistant gram-negatives; cover anaerobes (metronidazole or a carbapenem/piperacillin-tazobactam already covers them).
- Suspected MRSA (line infection, healthcare exposure, severe CAP) — add vancomycin or linezolid.[4]
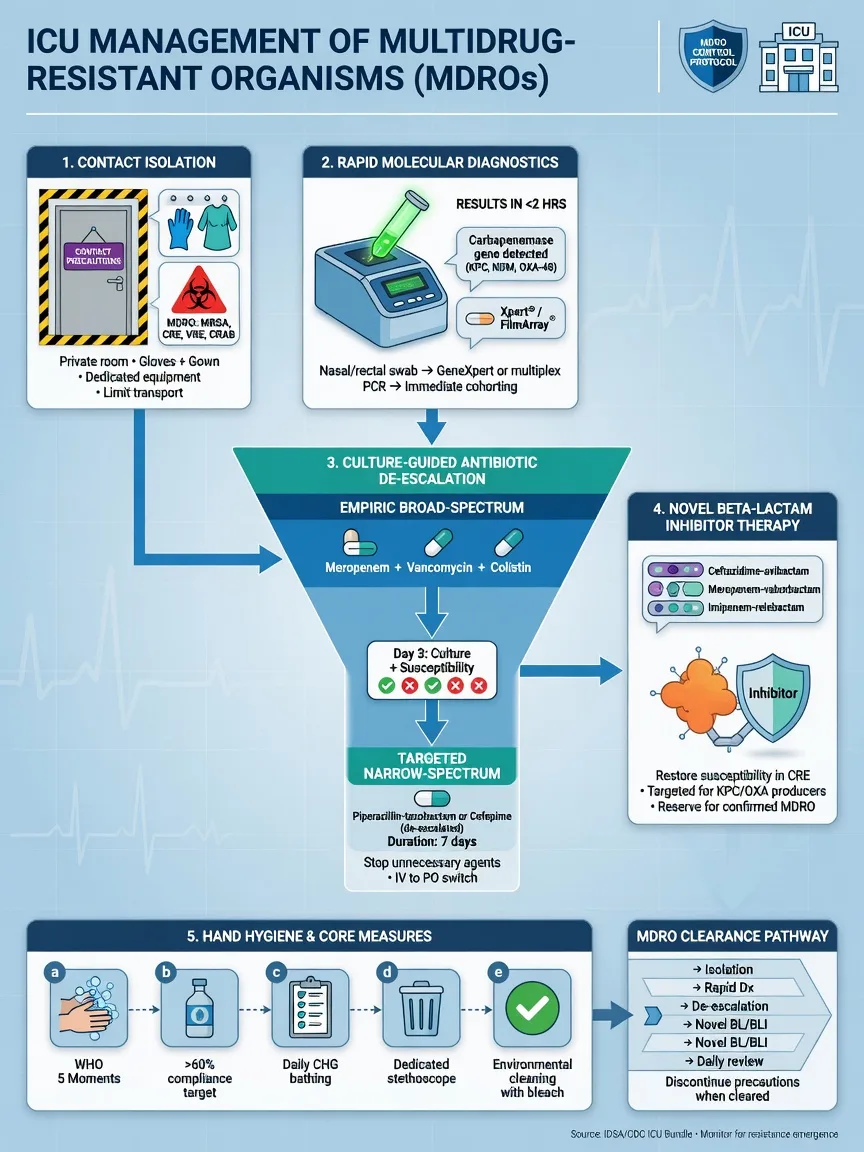
- Suspected ESBL/CRE (recent healthcare, known colonisation, prior carbapenem, travel to endemic regions) — meropenem; if carbapenemase suspected, colistin/polymyxin B + meropenem ± fosfomycin/aminoglycoside, consult ID.[6][12]
- Neutropenic sepsis — anti-pseudomonal beta-lactam monotherapy (piperacillin-tazobactam, ceftazidime, cefepime, meropenem); empiric vancomycin only if line infection/soft tissue/severe sepsis/mucositis.[13]
- Invasive fungal risk (prolonged neutropenia, transplant, ICU >7 days + TPN + broad-spectrum antibiotics + multiple sites colonised) — add echinocandin empiric for candidemia.[8]
- Source control within 6-12 hours (drain infected fluid, debride necrotic tissue, remove infected device) — antibiotics fail without it.
- De-escalate at 48-72 hours — once cultures and susceptibilities return: narrow to the narrowest effective agent, stop if no infection (negative cultures + alternative diagnosis), shorten duration (procalcitonin-guided, e.g. PRORATA).[2][10]
- Reassess daily — every antibiotic day counts for resistance, C. difficile, AKI and cost.
- Dose for the patient — loading dose in sepsis (increased Vd), augmented renal clearance (need MORE), RRT/Crrt (drug-specific dosing), obesity (consider IBW/adjusted), hepatic failure, protein binding.
PK/PD considerations in the ICU
| Situation | What changes | Consequence |
|---|---|---|
| Augmented renal clearance (ARC) (CrCl >130, young trauma, burns, sepsis early) | Increased renal clearance of renally-cleared drugs | Sub-therapeutic levels of beta-lactams (T<MIC), vancomycin (AUC<400), aminoglycosides — risk treatment failure + resistance selection. Use higher doses / continuous infusion / TDM. |
| Renal failure / RRT | Reduced clearance; varying clearance by modality | Toxicity (accumulation) — vancomycin, aminoglycosides, beta-lactams (cefepime neurotoxicity). Dose-adjust by CrCl; CRRT clears most beta-lactams (drug- and filter-specific), IHD clears in pulses (give post-HD). Cefepime NCSE in renal failure is classic.[7] |
| Sepsis / capillary leak | ↑Vd (third-space), hypoalbuminaemia (↑free fraction for highly-bound drugs — teicoplanin, ceftriaxone, flucloxacillin, daptomycin, voriconazole) | Loading dose needed; consider unbound concentration |
| Obesity | ↑Vd, altered clearance | Aminoglycosides/vancomycin dosed on IBW or adjusted (not total); linezolid, beta-lactams may need higher dose |
| Burns | ↑Cl, ↑Vd, changing skin flora | Sub-therapeutic beta-lactam/aminoglycoside levels — dose escalation + TDM |
| Hepatic failure | Reduced clearance of hepatically-cleared drugs (clindamycin, tigecycline, metronidazole, caspofungin, voriconazole, macrolides) | Hypoalbuminaemia (↑free fraction); reduce caspofungin in Child-Pugh B/C; voriconazole erratic (TDM) |
Continuous / prolonged infusion of beta-lactams — for time-dependent drugs, maximising T>MIC by prolonged (over 3-4 h) or continuous (over 24 h) infusion improves PK/PD target attainment, particularly with ARC, severe sepsis and resistant organisms. BLING II (Dulhunty 2015, n=432) compared continuous vs intermittent piperacillin-tazobactam/ticarcillin-clavulanate/meropenem in severe sepsis: no difference in 90-day ICU-free days (primary) but improved 14-day clinical cure in the sickest patients.[3] Recommended for severe sepsis with Pseudomonas, ESBL, ARC, or VAP; give a loading dose first.
Time-dependent (T>MIC)
beta-lactams, macrolides, linezolid
- Killing depends on DURATION free drug exceeds MIC
- Maximise by SHORTENING the interval, PROLONGED infusion (3-4 h) or CONTINUOUS infusion (24 h)
- BLING II: continuous beta-lactam infusion — no primary-outcome benefit, improved cure in severe sepsis
- Target fT>MIC 40-70% of dosing interval
- Penicillins, cephalosporins, carbapenems, azithromycin
Concentration-dependent (Cmax/MIC)
aminoglycosides, FQ, daptomycin, metronidazole
- Killing depends on PEAK concentration relative to MIC
- Maximise by HIGH dose ONCE daily (the Hartford aminoglycoside nomogram)
- Large post-antibiotic effect (PAE) allows wide interval
- Target Cmax/MIC 8-10 (aminoglycoside)
- Aminoglycosides, fluoroquinolones, daptomycin, metronidazole, amphotericin
AUC/MIC driver
vancomycin, fluoroquinolones, linezolid, azithro
- Total EXPOSURE relative to MIC predicts killing (composite of peak and time)
- Vancomycin AUC/MIC 400-600 for serious MRSA (Bayesian TDM)
- Fluoroquinolone AUC/MIC >125 (gram-neg), >30 (gram-pos)
- Linezolid AUC/MIC >80
- Drive BOTH dose and interval; TDM-guided where available
Adverse effects — the high-yield toxicity table
| Toxicity | Classic agents | Mechanism / notes |
|---|---|---|
| Nephrotoxicity | Aminoglycosides (proximal tubule, reversible), vancomycin (interstitial/oxidative — worse with piperacillin-tazobactam), amphotericin B (afferent arteriole vasoconstriction + distal tubule RTA/K/Mg wasting — liposomal less toxic), colistin/polymyxin B (dose-dependent), pentamidine | Avoid combinations; saline load for amphotericin; replace K/Mg; TDM for aminoglycosides/vancomycin |
| QT prolongation / torsades | Fluoroquinolones (moxifloxacin > cipro), macrolides (erythro > azithro > clarithro), fluconazole/voriconazole/posaconazole (NOT isavuconazole — shortens QT), pentamidine, azoles + FQ stacked | Cumulative with other QT drugs (antiarrhythmics, antipsychotics, ondansetron), hypokalaemia, hypomagnesaemia, structural heart disease. ECG before/after. |
| Bone-marrow suppression | Linezolid (thrombocytopenia, anaemia, neutropenia — >14 days), trimethoprim (megaloblastic — folate antagonist), chloramphenicol (aplastic anaemia, grey baby), flucytosine (cytopenias), ganciclovir, sulphonamides (agranulocytosis) | Monitor FBC weekly on long linezolid; give folinic acid with TMP/5-FC |
| C. difficile infection | Clindamycin (classic), fluoroquinolones, cephalosporins (esp. 2nd/3rd), broad-spectrum penicillins, carbapenems — ANY antibiotic (and proton-pump inhibitors) | Stop offending antibiotic; fidaxomicin or oral vancomycin (severe: vanco + bezlotoxumab; fulminant: surgical).[5] |
| Neurotoxicity | Cefepime (encephalopathy, myoclonus, NCSE — renal failure), penicillins (seizures at very high dose/CrCl), metronidazole (encephalopathy, cerebellar, peripheral neuropathy), isoniazid (neuropathy, seizures), linezolid (serotonin syndrome — MAOI; peripheral/optic neuropathy), polymyxins/colistin | Dose-adjust for CrCl; EEG for cefepime; stop/replace |
| Hepatotoxicity | Azoles (fluconazole, voriconazole, itraconazole — transaminitis, hepatitis), macrolides (cholestatic — erythro), flucloxacillin/co-amoxiclav (cholestatic hepatitis — delayed, weeks post-exposure), nitrofurantoin, tetracyclines (fatty liver high dose IV), rifampicin/hydrazides, pyrazinamide | Monitor LFTs; stop if ALT >5×ULN or jaundice |
| Tendinopathy / aortic rupture | Fluoroquinolones (boxed warning) — Achilles rupture, aortic dissection/aneurysm | Avoid in Marfan, recent AA, concomitant steroids |
| Infusion reactions | Vancomycin (red-man syndrome — histamine, rate-related — NOT IgE; slow, antihistamine), amphotericin (rigors, fever, hypotension), echinocandins (histamine flush) | Slow infusion; premedicate amphotericin; stop/slow |
| Photosensitivity / pigment | Tetracyclines (doxycycline — photosensitivity, oesophagitis), fluoroquinolones (photosensitivity), voriconazole (photosensitivity, SCC risk long-term) | Sun protection; switch long-term |
| Serotonin syndrome | Linezolid (MAOI — interacts with SSRIs, tramadol, MAOIs, tyramine foods) | Identify interacting drugs; review; supportive care |
| Allergy / anaphylaxis | Beta-lactams (penicillins > cephems > carbapenems — side-chain cross-reactivity low; aztreonam safe), sulphonamides (HIV patients), vancomycin (IgE rare, usually red-man) | Allergy history; skin test/desensitise; aztreonam when severe beta-lactam allergy |
| Cartilage / teeth / bone | Tetracyclines (teeth/bone — child/pregnancy), fluoroquinolones (cartilage — avoid pregnancy/children when possible) | Avoid pregnancy/paeds |
Resistance mechanisms
[12] [12]Landmark antimicrobial trials & guidelines — what they showed
Time-dependent — beta-lactams
T>MIC driver
- Maximise time above MIC — short q-interval OR prolonged/continuous infusion
- BLING II: continuous infusion improved cure in sickest severe sepsis
- Loading dose in sepsis (↑Vd); watch ARC (sub-therapeutic) and RRT (toxic)
- Cefepime neurotoxicity (NCSE) in renal failure — dose for CrCl
- Carbapenem = first-line for ESBL/AmpC
Concentration-dependent — aminoglycosides
Cmax/MIC driver
- Once-daily extended-interval (5-7 mg/kg gent) optimises peak + PAE
- Nephrotoxicity (proximal tubule — reversible) + ototoxicity (IRREVERSIBLE) + neuromuscular blockade
- TDM: trough <1 mg/L; no anaerobic cover (oxygen-dependent uptake)
- Synergy with cell-wall agents for enterococcal endocarditis (gent + amp)
- Avoid pregnancy (foetal 8th-nerve damage)
AUC/MIC — vancomycin
Gram-positive only
- AUC/MIC 400-600 for serious MRSA (Bayesian TDM) — trough 15-20 surrogate
- Loading 25-30 mg/kg; nephrotoxicity (worse with pip-tazo)
- Red-man syndrome = histamine (rate-related), NOT IgE — slow infusion
- Oral (non-absorbed) for C. difficile; IV for systemic gram-positive
- Teicoplanin alternative — once-daily, less nephrotoxic, no red-man
Daptomycin
Membrane — NOT pneumonia
- Binds membrane → depolarisation; bactericidal, concentration-dependent
- Gram-positive only: MRSA, VRE, penicillin-resistant pneumococcus
- INACTIVATED BY SURFACTANT — never for pneumonia
- Monitor creatine kinase (rhabdomyolysis); avoid with statins
- Eosinophilic pneumonia with prolonged use
Linezolid
50S — gram-positive only
- 100% oral bioavailability; MRSA/VRE; preferred for MRSA VAP
- Thrombocytopenia/anaemia/neutropenia >14 days — monitor FBC
- Weak MAO inhibitor — SEROTONIN SYNDROME with SSRIs/tramadol/MAOIs
- Peripheral + optic neuropathy, lactic acidosis (mitochondrial) long courses
- No renal dose adjustment
SAQ — Empiric antibiotic choice in septic shock from a urinary source
10 minutes · 10 marks
A 68-year-old woman is admitted to the ICU with septic shock (lactate 4.2 mmol/L, MAP 58 mmHg on noradrenaline 0.3 mcg/kg/min) from a urinary tract source. She has had two courses of antibiotics in the last 3 months (ciprofloxacin, then amoxycillin-clavulanate for a prior UTI), and recently returned from a 6-week hospital admission in India. Blood and urine cultures are pending. Outline your empiric antibiotic strategy and justify your choices.
SAQ — Antibiotic de-escalation and stewardship on day 3 of ICU admission
10 minutes · 10 marks
A 72-year-old man was admitted 3 days ago with community-acquired pneumonia and septic shock. He was started empirically on ceftriaxone, azithromycin and vancomycin. He is now off vasopressors, afebrile for 24 hours, and his blood cultures have grown MSSA (methicillin-sensitive Staphylococcus aureus) sensitive to flucloxacillin. Discuss the principles of antibiotic de-escalation and outline your revised antibiotic plan.
Clinical pearls
[3]Red flags
[3]References
- [1]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [2]Evans L, Rhodes A, Alhazzani W, et al Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med, 2021.PMID 34605781
- [3]Dulhunty JM, Roberts JA, Davis JS, et al A Multicenter Randomized Trial of Continuous versus Intermittent Beta-Lactam Infusion in Severe Sepsis (BLING II). Am J Respir Crit Care Med, 2015.PMID 26200166
- [4]Liu C, Bayer A, Cosgrove SE, et al Clinical practice guidelines by the IDSA for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis, 2011.PMID 21217178
- [5]Bartlett JG Clostridium difficile Infection. Infectious disease clinics of North America, 2017.PMID 28779831
- [6]Endimiani A, Paterson DL Optimizing therapy for infections caused by enterobacteriaceae producing extended-spectrum beta-lactamases. Semin Respir Crit Care Med, 2007.PMID 18095228
- [7]Triplett JD, Lawn ND, Chan J, et al Cephalosporin-related neurotoxicity: metabolic encephalopathy or non-convulsive status epilepticus? J Clin Neurosci, 2019.PMID 31201049
- [8]Pappas PG, Kauffman CA, Andes DR, et al Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the IDSA. Clin Infect Dis, 2016.PMID 26810419
- [9]Patterson TF, Thompson GR 3rd, Denning DW, et al Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the IDSA. Clin Infect Dis, 2016.PMID 27481947
- [10]Kalil AC, Metersky ML, Klompas M, et al Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 IDSA Clinical Practice Guidelines. Clin Infect Dis, 2016.PMID 27418577
- [11]Harris PNA, Tambyah PA, Lye DC, et al (MERINO) Effect of Piperacillin-Tazobactam vs Meropenem on 30-Day Mortality for Patients With E coli or Klebsiella pneumoniae Bloodstream Infection and Ceftriaxone Resistance (MERINO). JAMA, 2018.PMID 30208454
- [12]Kumarasamy KK, Toleman MA, Walsh TR, et al Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study (NDM-1). Lancet Infect Dis, 2010.PMID 20705517
- [13]Boucher HW, Talbot GH, Bradley JS, et al Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America. Clin Infect Dis, 2009.PMID 19035777