ICU · Rehabilitation
ICU-acquired weakness (critical illness myopathy/polyneuropathy)
Also known as ICU-acquired weakness (ICUAW) · Critical illness myopathy (CIM) · Critical illness polyneuropathy (CIP) · Critical illness neuromyopathy (CINM) · Sarcopenia in ICU
ICU-acquired weakness (ICUAW) affects 25-50% of ICU patients ventilated 7 days. Comprises critical illness myopathy (CIM — muscle), critical illness polyneuropathy (CIP — peripheral nerves), or both (CINM). Risk factors: sepsis, prolonged mechanical ventilation, hyperglycaemia, immobilisation, corticosteroids, neuromuscular blocking agents. Diagnosis: clinical (MRC score <48/60), confirmed by electrophysiology (nerve conduction studies, EMG) and sometimes muscle biopsy. Prevention: glycaemic control (avoid hyperglycaemia, target 6-10 mmol/L), minimise sedation (daily SAT), early mobilisation, minimise steroids/NMBAs, adequate nutrition (avoid overfeeding — refeeding syndrome). Outcomes: prolonged ventilation, increased mortality, long-term disability.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Types of ICU-acquired weakness
CIM (myopathy)
Muscle involvement
- Primary myopathy (muscle fibre dysfunction)
- More common than CIP in ICU
- Electrophysiology: reduced CMAP amplitude, normal sensory studies
- Muscle biopsy: myosin filament loss, muscle fibre atrophy/necrosis
- Associated with: corticosteroids, NMBAs, sepsis, hyperglycaemia
CIP (polyneuropathy)
Nerve involvement
- Axonal sensorimotor polyneuropathy
- Electrophysiology: reduced CMAP and SNAP amplitudes (axonal pattern)
- Often coexists with CIM (CINM — critical illness neuromyopathy)
- Associated with: sepsis, multi-organ failure, prolonged ICU stay
Diagnosis
Clinical — MRC score
[2]Electrophysiology
Diagnostic approach
Clinical assessment
MRC score <48/60 in a cooperative patient who has been in ICU for >7 days. Weakness is diffuse, symmetrical, and spares facial muscles (unlike GBS or MG). Areflexia/hyporeflexia may be present but is not required.
Exclude other causes
GBS (acute ascending paralysis, CSF albuminocytological dissociation), MG (fatigable weakness, positive AChR antibody), electrolyte disturbance (check K, Mg, Ca, phosphate), spinal cord lesion (sensory level, sphincter involvement), prolonged effects of NMBAs.
Electrophysiology (nerve conduction studies + EMG)
CIM: reduced CMAP amplitude, normal SNAP (sensory), myopathic EMG changes. CIP: reduced CMAP AND SNAP (axonal), denervation on EMG. CINM: features of both. Electrophysiology differentiates CIM from CIP.
Muscle biopsy (rarely needed)
Reserved for research or diagnostic uncertainty. Shows: myosin filament loss (selective loss of thick myosin filaments — characteristic of CIM), fibre atrophy, fibre necrosis, fatty degeneration.
Prevention
ICUAW prevention — the modifiable risk factors
Glycaemic control — the #1 modifiable factor
Hyperglycaemia directly causes muscle dysfunction (osmotic damage, oxidative stress, protein catabolism). Target: 6-10 mmol/L. Avoid severe hyperglycaemia (>10). NICE-SUGAR trial: moderate control (6-10) better than tight (4.4-6.1) — tight control risks hypoglycaemia. Insulin infusion for persistently elevated glucose.
Minimise sedation
Daily sedation interruption (SAT) + spontaneous breathing trial (SBT). Use light sedation (RASS -1 to 0). Avoid benzodiazepines (increase delirium and immobilisation). Prefer dexmedetomidine or propofol. Immobilisation causes rapid muscle wasting — 1.5-2% per day.
Early mobilisation
PASSIVE range of motion from day 1. Sit on edge of bed when haemodynamically stable. Stand/walk when possible (within 72h if safe). Requires coordinated effort: nursing, physiotherapy, medical staff. Reduces ICUAW, delirium, and ventilator days.<Cite id="3" />
Minimise corticosteroids and NMBAs
Corticosteroids cause myopathy (especially high-dose, prolonged use). NMBAs cause prolonged weakness (especially with concurrent steroids — ‘acute quadriplegic myopathy’). Use the shortest duration possible. Monitor with train-of-four if using NMBAs.
Nutrition
Adequate protein: 1.2-1.5 g/kg/day. Avoid overfeeding (refeeding syndrome, hyperglycaemia). Start enteral nutrition early (within 48h). Check phosphate, magnesium, potassium before starting feed. Do NOT restrict protein — muscle catabolism is already maximally stimulated by critical illness.
Risk factors
ICU-acquired weakness risk factors
Clinical pearls
Red flags
Pathophysiology — how critical illness damages nerve and muscle
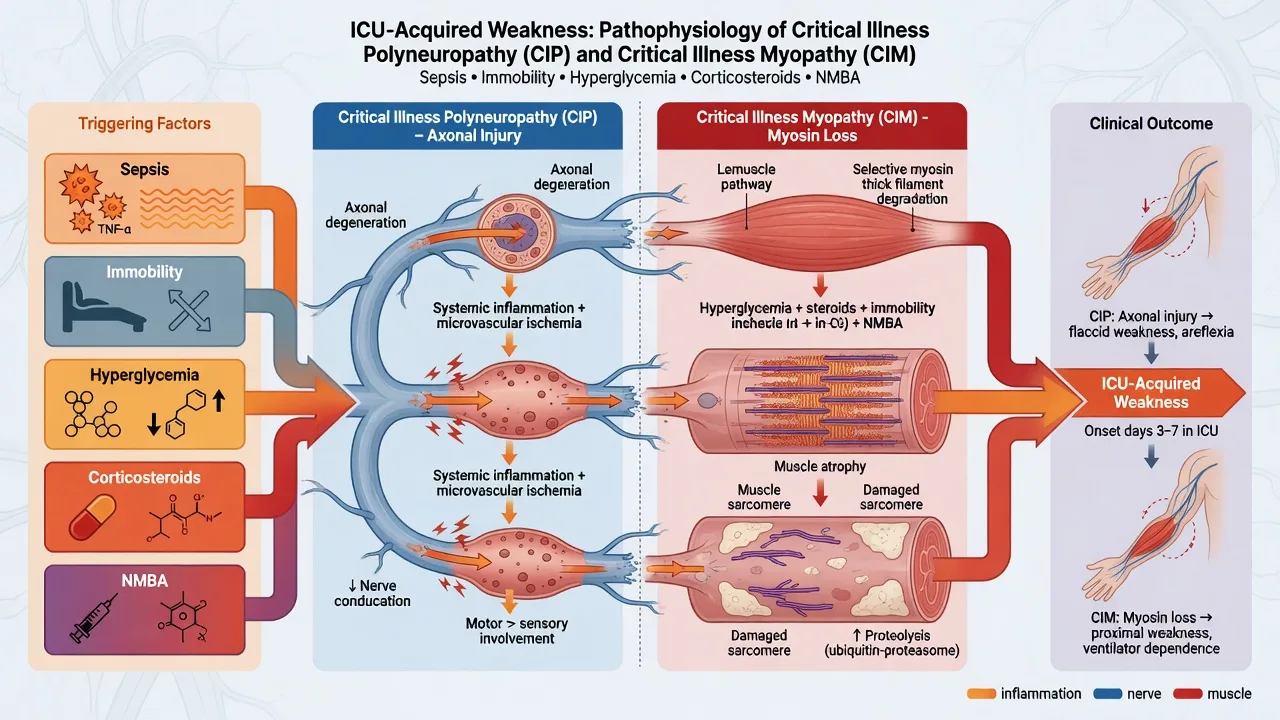
ICU-acquired weakness is not a single disease but the convergent end-result of several parallel injury pathways triggered by systemic inflammation, immobility, metabolic derangement, and drug toxicity. Three overlapping mechanisms dominate: critical illness myopathy (skeletal-muscle fibre dysfunction), critical illness polyneuropathy (axonal peripheral-nerve injury), and — when both coexist, as they do in over half of electrophysiologically-confirmed cases — critical illness neuromyopathy (CINM).[1]
Muscle (CIM)
Myocyte injury
- Catabolic state: resistance to insulin/IGF-1 + ↑ TNF-α/IL-1/IL-6 → ubiquitin-proteasome and autophagy-lysosome proteolysis of contractile proteins
- Preferential loss of THICK (myosin) filaments → selective myosin loss (hallmark histology); later type II fibre atrophy
- Sodium-channel dysfunction + membrane depolarisation → inexcitable sarcolemma (reduced/absent CMAP on direct muscle stimulation)
- Mitochondrial dysfunction (impaired oxidative phosphorylation, ↓ ATP) → energy failure, impaired Ca²⁺ handling, oxidative stress
- Triggered by: immobilisation, corticosteroids, NMBAs, hyperglycaemia, sepsis
Nerve (CIP)
Axonal degeneration
- Distal, symmetrical, AXONAL (not demyelinating) sensorimotor polyneuropathy
- Microvascular dysfunction → endoneurial ischaemia + increased blood-nerve-barrier permeability
- Sepsis/inflammation → activation of Schwann cells, mitochondrial injury, energy failure of the axon
- Electrophysiology: reduced CMAP AND SNAP amplitudes (both motor AND sensory affected — the key discriminator from CIM)
- Triggered by: sepsis, multi-organ failure, prolonged stay; axonal degeneration is the dominant lesion
Combined (CINM)
Most common in practice
- Coincident myopathy + polyneuropathy — found in >50% of electrophysiologically-confirmed ICUAW
- Sensory studies often "normal-ish" in pure CIM but abnormal in CINM — direct muscle stimulation resolves ambiguity
- Clinically indistinguishable from isolated CIM/CIP at the bedside — needs electrophysiology to separate
- Worse functional outcomes and slower recovery than either alone
- Risk profile = union of CIM and CIP risks (sepsis + steroids + NMBAs + immobility + hyperglycaemia)
The pathophysiological cascade — from sepsis to weakness
Trigger: systemic inflammation (sepsis, MODS, ARDS)
Cytokine storm (TNF-α, IL-1β, IL-6), microcirculatory failure, oxidative stress, and mitochondrial dysfunction are the upstream drivers. Sepsis is the single strongest risk factor for ICUAW.
Catabolic dominance in muscle
Insulin/IGF-1 resistance + cytokine-driven proteolysis (ubiquitin-proteasome, autophagy-lysosome) → net breakdown of myofibrillar protein, preferential loss of thick myosin filaments, and type II fibre atrophy.
Sarcolemmal inexcitability
Sodium-channel dysfunction and partial membrane depolarisation render muscle fibres electrically silent → reduced/absent CMAP. This is reversible and underlies the rapid fluctuation seen early in recovery.
Axonal degeneration in nerve (CIP)
Microvascular ischaemia, blood-nerve-barrier breakdown, and Schwann-cell mitochondrial failure produce distal axonal sensorimotor polyneuropathy → secondary muscle denervation.
Amplifiers: immobility, drugs, glucose
Bed rest alone causes ~1.5-2% quadriceps loss/day. Corticosteroids + NMBAs synergise to cause "acute quadriplegic myopathy". Hyperglycaemia damages nerve (osmotic/oxidative) and muscle (protein catabolism).
Clinical phenotype: diffuse, flaccid, symmetric weakness
Limbs > trunk > face (facial sparing). Hyporeflexia/areflexia. Respiratory muscle involvement → failed weaning. Sensation intact or only mildly impaired (unlike the marked weakness).
CIP vs CIM vs CINM — discriminating the overlap at the bedside
Pure CIM and pure CIP are conceptually distinct but overlap so frequently in practice that CINM is the most common reality. The distinction matters for prognosis and for understanding trial populations, but the management is identical: there is no specific treatment for any of the three — only prevention and rehabilitation.[1]
[9]Diagnosis in depth — the ATS framework
The 2014 American Thoracic Society guideline defines ICUAW as symmetrical, diffuse, clinically detected weakness developing during critical illness that cannot be explained by a pre-existing condition. The MRC sum score is the core bedside criterion, with electrophysiology as confirmation when feasible and exclusion of mimics as mandatory.[10]
Diagnostic algorithm (ATS 2014)
Step 1 — Suspect ICUAW
Any patient ventilated >48-72 h, or with sepsis/MODS, prolonged sedation, steroid + NMBA exposure, or difficulty weaning from ventilation. Screen actively — ICUAW is under-recognised.
Step 2 — Cooperative? Perform MRC sum score
Arouse the patient (RASS ≥ -1), ensure no residual NMBA effect (train-of-four ≥ 4/4), then score 6 muscle groups bilaterally (shoulder abduction, elbow flexion, wrist extension, hip flexion, knee extension, ankle dorsiflexion) 0-5 each. MRC <48/60 (and definitely <36) = ICUAW. Average of bilateral scores if asymmetric.
Step 3 — Uncooperative? Use surrogate measures
Hand-grip dynamometry (<11 kg female / <27 kg male = weakness), MRC of available groups, or wait for cooperation. New inability to lift arms off the bed, weak hand squeeze, or facial weakness ALL away from ICUAW.
Step 4 — Exclude mimics (mandatory)
Guillain-Barré (acute ascending, areflexic, CSF albuminocytological dissociation, may involve face), myasthenia gravis (fatigable, ocular/bulbar, +AChR/MuSK Ab), electrolyte disorder (K⁺, Mg²⁺, Ca²⁺, phosphate), spinal cord lesion (sensory level, sphincter signs), prolonged NMBA effect (train-of-four), steroid myopathy, motor neuron disease.
Step 5 — Electrophysiology (confirm + phenotype)
Nerve conduction studies + needle EMG differentiate CIM (normal SNAP, ↓CMAP, myopathic EMG) from CIP (↓SNAP + ↓CMAP, denervation) and identify CINM. Direct muscle stimulation (tibialis anterior) is the most specific discriminator when sensory studies are confounded.
Step 6 — Muscle biopsy (rarely needed)
Reserved for research or genuine diagnostic uncertainty. Hallmark of CIM: selective loss of thick myosin filaments, fibre atrophy, and (in severe cases) fibre necrosis with fatty replacement.
Diagnostic thresholds — the numbers to know
Risk factors in depth
[8]ICUAW risk — the numbers to quote in a viva
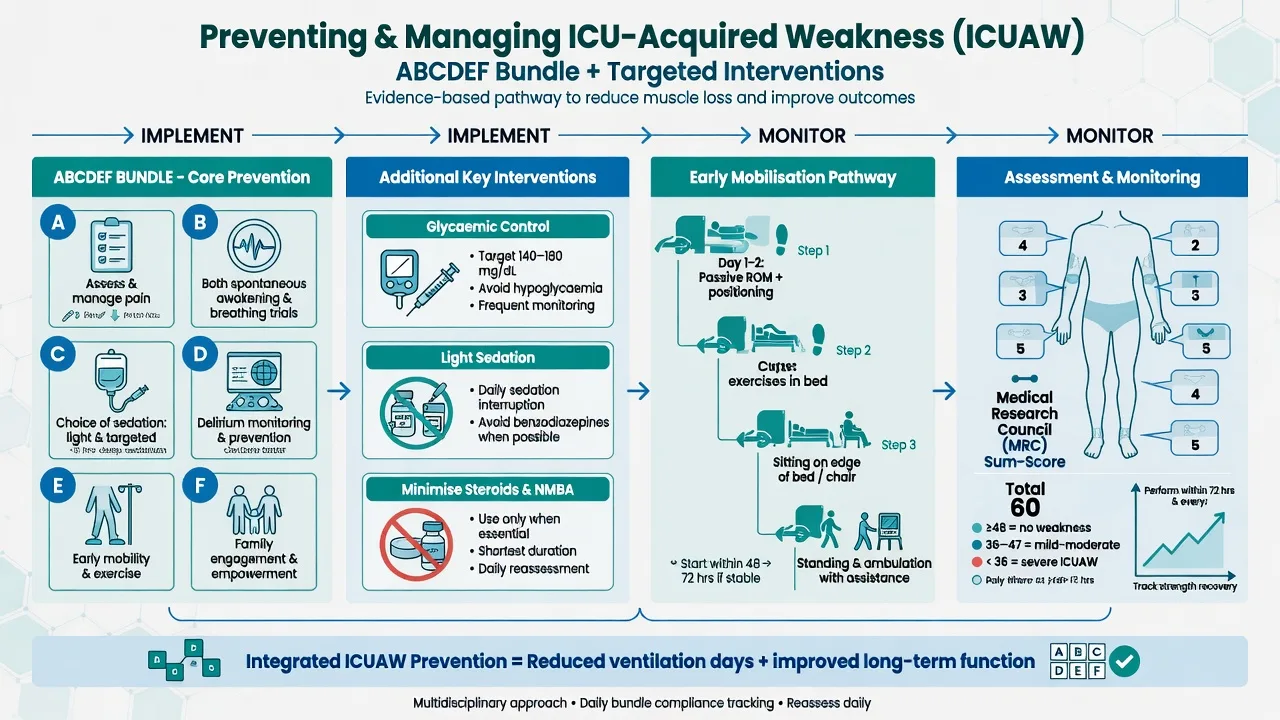
Prevention — the ABCDEF bundle applied to ICUAW
Because no treatment reverses established ICUAW, prevention is the entire game. The SCCM ICU Liberation ABCDEF bundle is the single best-evidenced, multidisciplinary strategy and addresses every major modifiable risk factor.[12]
ICUAW prevention — the ABCDEF bundle, component by component
A — Assess and manage pain
Untreated pain drives immobility, hyperglycaemia (stress response) and delirium. Use CPOT (intubated) or NRS (extubated). Analgesia-first sedation reduces opioid and benzodiazepine burden.
B — Both SAT and SBT
Daily spontaneous awakening trial + spontaneous breathing trial. Shorter ventilation = less ventilator-induced diaphragm dysfunction and less immobility. Pair the two (SAT-and-SBT protocol) for synergy.
C — Choice of sedation
Prefer dexmedetomidine or propofol over benzodiazepines. Target light sedation (RASS -1 to 0). Avoid prolonged deep sedation, which is an independent risk factor for ICUAW.
D — Delirium assessment and management
Monitor with CAM-ICU or ICDSC. Prevent delirium (pain control, light sedation, sleep, mobilisation, family). Delirium and ICUAW are tightly linked — both reflect and worsen critical illness.
E — Early mobility
The single most effective ICUAW-specific intervention. Passive ROM day 1 → in-bed cycling → sit on edge of bed → stand → walk, as soon as haemodynamically safe (often within 72 h, even while ventilated). Coordinated nursing + physiotherapy + medical staff.
F — Family engagement and empowerment
Family presence and participation in mobilisation and care; flexible visiting; ICU diaries. Reduces sedation needs, supports rehabilitation, and addresses PICS-F.
Recovery timeline and prognostic factors
Recovery from ICUAW is variable and often incomplete. CIM (membrane repolarisation + refeeding of muscle) tends to recover faster than CIP (axonal regrowth at ~1 mm/day). The MRC sum score at ICU discharge is the single best early predictor of long-term function.[2]
Recovery trajectory — how ICUAW recovers over time (click each)
Rehabilitation phase
Functional gains accelerate with active rehabilitation. Many patients regain independent ambulation if weakness was predominantly myopathic. Axonal regrowth (CIP) continues slowly.
Key trials and evidence
van den Berghe 2001 — Intensive insulin therapy (Leuven surgical) (PMID 11794168)
NICE-SUGAR 2009 — Glucose control in ICU (PMID 19318384)
Schweickert 2009 — Early mobilisation in ventilated patients (PMID 19446324)
De Jonghe 2004 — ICU-acquired paresis and weaning (PMID 14767593)
Pun 2019 — ABCDEF bundle in >15,000 ICU patients (PMID 30339549)
Exam practice
SAQ — ICU-acquired weakness
10 minutes · 10 marks
A 67-year-old man with severe community-acquired pneumonia and septic shock has been in ICU for 9 days. He required vasopressors for 3 days, has received hydrocortisone 200 mg/day for 5 days, a 48-hour cisatracurium infusion for ARDS, and remains mechanically ventilated. Sedation has been weaned and he is now cooperative (RASS 0). On examination he has flaccid, symmetric limb weakness; facial strength is normal. His glucose has ranged 8-16 mmol/L despite an insulin infusion. Train-of-four shows 4/4 twitches.
SAQ — CIP versus CIM: differentiating the electrophysiology
10 minutes · 10 marks
A 54-year-old woman with severe ARDS from H1N1 influenza has been ventilated for 12 days. She received hydrocortisone 200 mg/day for 7 days and a 48-hour cisatracurium infusion. Sedation has been weaned; she is cooperative (RASS 0) but has flaccid, symmetric limb weakness and has failed two spontaneous breathing trials despite radiological resolution of her pneumonia. MRC sum score is 36/60. Nerve conduction studies show reduced compound muscle action potential (CMAP) amplitudes in all limbs with normal conduction velocities and normal distal latencies.
SAQ — Preventing and rehabilitating ICU-acquired weakness
10 minutes · 10 marks
A 62-year-old man is admitted to ICU with septic shock from a perforated diverticulum. He is intubated, on noradrenaline 0.3 mcg/kg/min, and has been started on hydrocortisone 200 mg/day for refractory vasoplegia. His glucose is 14 mmol/L. He is sedated with propofol and fentanyl. Outline your strategy to prevent ICU-acquired weakness and to rehabilitate him if it occurs.
Additional clinical pearls — examiner depth
Red flags — what must not be missed
References
- [1]Stevens RD, Marshall SA, Cornblath DR, Hoke A, et al. A framework for diagnosing and classifying intensive care unit-acquired weakness. Critical care medicine, 2009.PMID 20046114
- [2]Kress JP, Hall JB. ICU-acquired weakness and recovery from critical illness. New England Journal of Medicine, 2014.PMID 25014703
- [3]Tipping CJ, Harrold M, Holland A, Romero L, et al. The effects of active mobilisation and rehabilitation in ICU on mortality and function: a systematic review. Intensive care medicine, 2017.PMID 27864615
- [4]Hermans G, De Jonghe B, Bruyninckx F, Van den Berghe G, et al. Interventions for preventing critical illness polyneuropathy and critical illness myopathy. Cochrane Database of Systematic Reviews, 2014.PMID 24477672
- [5]van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. New England Journal of Medicine, 2001.PMID 11794168
- [6]NICE-SUGAR Study Investigators, Finfer S, Chittock DR, et al. Intensive versus conventional glucose control in critically ill patients. New England Journal of Medicine, 2009.PMID 19318384
- [7]Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. The Lancet, 2009.PMID 19446324
- [8]De Jonghe B, Bastuji-Garin S, Sharshar T, Outin H, et al. Does ICU-acquired paresis lengthen weaning from mechanical ventilation? Intensive care medicine, 2004.PMID 14767593
- [9]Lefaucheur JP, Nordine T, Rodriguez P, et al. Origin of ICU acquired paresis determined by direct muscle stimulation. Journal of neurology, neurosurgery, and psychiatry, 2006.PMID 16306155
- [10]Fan E, Cheek F, Chlan L, Gosselink R, et al. An official American Thoracic Society Clinical Practice guideline: the diagnosis of intensive care unit-acquired weakness in adults. American Journal of Respiratory and Critical Care Medicine, 2014.PMID 25496103
- [11]Latronico N, Shehu I, Guarneri B Use of electrophysiologic testing. Critical care medicine, 2009.PMID 20046116
- [12]Marra A, Ely EW, Pandharipande PP, Patel MB. The ABCDEF Bundle in Critical Care. Critical Care Clinics, 2017.PMID 28284292
- [13]Pun BT, Balas MC, Barnes-Daly MA, Thompson JL, et al. Caring for Critically Ill Patients with the ABCDEF Bundle: Results of the ICU Liberation Collaborative in Over 15,000 Adults. Critical care medicine, 2019.PMID 30339549
- [14]Hiser SL, Casey K, Nydahl P, Hodgson CL. Intensive care unit acquired weakness and physical rehabilitation in the ICU. BMJ, 2025.PMID 39870417