ICU · Rehabilitation
Pulmonary rehabilitation and functional recovery after ICU admission
Also known as Pulmonary rehabilitation after critical illness · Post-ICU rehabilitation · Exercise training after critical illness · Respiratory muscle training · Early mobilisation in ICU · Post-intensive care syndrome - physical domain · ICU-acquired weakness rehabilitation · Inspiratory muscle training
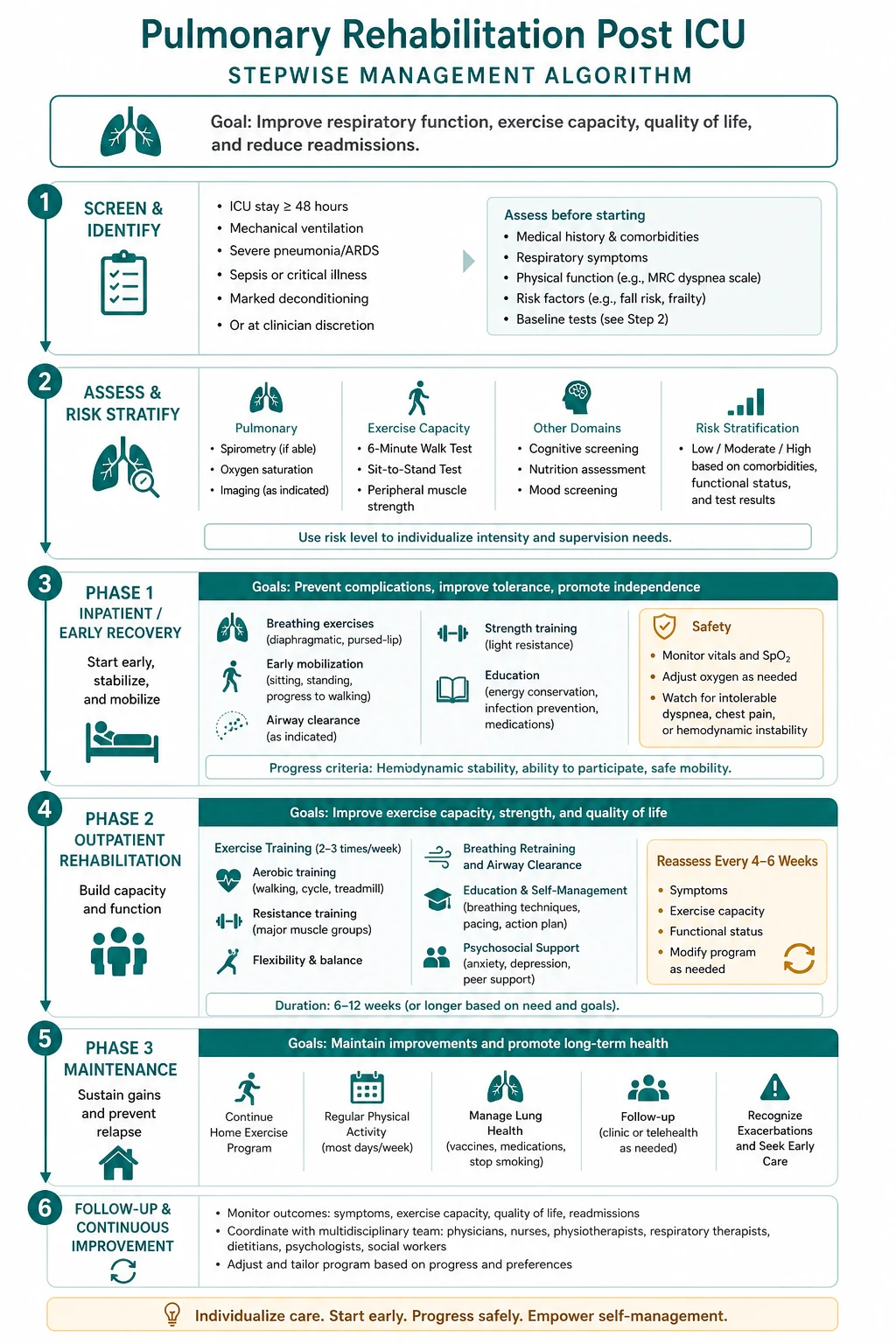
Pulmonary and functional rehabilitation after critical illness targets the physical deconditioning, respiratory and limb-muscle weakness, and reduced exercise tolerance that persist long after the acute insult resolves. It is the active treatment arm of the PHYSICAL DOMAIN of the post-intensive care syndrome (PICS). Components: (1) early mobilisation begun IN the ICU (passive range of motion → active-assisted → active → sitting → standing → walking); (2) exercise training — aerobic (walking, cycling, arm ergometry) plus resistance (8-10 muscle groups); (3) respiratory/inspiratory muscle training (incentive spirometry, threshold IMT); (4) education, psychological support, nutritional counselling. Assessment tools: MRC sum score (ICU-acquired weakness), handgrip dynamometry, 6-minute walk test (6MWT), PFIT-s / FSS-ICU / CPAX, Barthel/FIM. ICU-acquired weakness (CIP/CIM) affects 25-50% of patients ventilated 7 days and is the dominant reversible physical deficit. Evidence is mixed and nuanced: Schweickert 2009 (Lancet) and Burtin 2009 showed early mobilisation improves function, but the larger TEAM trial (Hodgson, NEJM 2022) found routine aggressive early active mobilisation did NOT improve 180-day outcomes and caused more adverse events — practice has shifted to SELECTIVE, goal-directed mobilisation. Timing: begin in ICU → continue on ward → formal pulmonary rehab programme 4-8 weeks post-discharge for 6-12 weeks. 30-50% of survivors never return to baseline physical function; structured rehabilitation is essential.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags


Overview
The deconditioning imposed by critical illness is rapid, profound, and disproportionate to anything seen in ordinary medicine. Healthy older adults lose ~0.5-1% of muscle mass per year; a critically ill patient loses 2-3% per day in the first week of ICU admission, with up to ~13% loss of quadriceps cross-sectional area over 10 days (Puthucheary 2013).[7] The diaphragm, uniquely, atrophies even faster under controlled mechanical ventilation — experimentally, ~50% reduction in diaphragm fibre force-generating capacity is measurable after as little as 6-18 hours of complete diaphragm inactivity. This dual limb and respiratory muscle wasting, combined with critical-illness neuropathy/myopathy, produces the constellation called the physical domain of PICS, and it is what pulmonary and functional rehabilitation exists to reverse.[2][10]
The post-intensive care syndrome (PICS) — physical domain
PICS, defined at the 2010 SCCM stakeholders' conference (Needham 2012), is the new or worsening impairment in physical, cognitive, or mental health status that persists after acute critical illness and beyond the acute hospital stay.[2] The physical domain dominates the early recovery period and is the most accessible to rehabilitation:
The three domains of PICS
| Domain | What it looks like | Onset / course | Interventions |
|---|---|---|---|
| Physical (this topic) | ICU-acquired weakness, muscle wasting, ↓ exercise capacity, ↓ ADLs, dysphagia, joint contractures | Earliest and most prominent; peaks at ICU discharge, improves over 1-2 yr but many never full recovery | Early mobilisation, exercise training, IMT, nutrition, swallowing therapy |
| Cognitive | Impaired memory, attention, executive function, visuospatial ability (~30-50% at 1 yr) | Persists; slowly improves over years; resembles mild traumatic brain injury | Cognitive rehabilitation, cognitive baselines, avoiding deliriogenic drugs |
| Mental health | Depression (~30%), anxiety (~40%), PTSD (~20%), vivid delusional memories | Can worsen after discharge as memories consolidate | Screening (HADS, IES-6), CBT, peer support, ICU diaries |
The three domains are interlinked: physical weakness limits activity → social isolation → depression → reduced engagement with rehab → worse physical outcome. Treating the physical domain in isolation is less effective than treating all three; this is why modern post-ICU programmes are multidisciplinary and holistic.[2][12]
ICU-acquired weakness (ICUAW) — the dominant reversible deficit
ICU-acquired weakness is the acquired muscle and nerve dysfunction that develops during critical illness, affecting 25-50% of patients ventilated for more than 7 days (and up to 50-100% of those with sepsis, prolonged ARDS, or multi-organ failure).[8][11] It is the single biggest contributor to the physical domain of PICS and the main target of post-ICU rehabilitation.
Critical illness polyneuropathy (CIP) vs critical illness myopathy (CIM)
| Feature | CIP (polyneuropathy) | CIM (myopathy) | CINM (combined — commonest in practice) |
|---|---|---|---|
| Pathology | Axonal degeneration of motor AND sensory nerves (distal > proximal) | Selective loss of thick (myosin) filaments in skeletal muscle | Both nerve axon damage and myosin loss |
| Mechanism | Systemic inflammation + microvascular ischaemia + mitochondrial energy failure → axonal degeneration | Steroids + NMBA + immobility → ubiquitin-proteasome-driven myosin breakdown | Inflammation + immobilisation + drug toxicity acting together |
| Top risk factors | Sepsis/MODS (#1), prolonged ventilation, hyperglycaemia | STEROIDS (#1), NMBA (prolonged), immobility | Sepsis + steroids + prolonged sedation |
| Weakness pattern | DISTAL > proximal (stocking-glove; feet/hands first) | PROXIMAL > distal (shoulder/hip girdle — hard to stand from chair) | Mixed proximal + distal |
| Sensation | REDUCED (sensory nerves affected) | PRESERVED (nerves intact) | Reduced |
| Tendon reflexes | Decreased/absent | Decreased (may be normal early) | Decreased |
| Nerve conduction | ↓ CMAP + ↓ SNAP (axonal pattern) | ↓ CMAP + NORMAL SNAP | ↓ CMAP ± SNAP |
| Recovery | Slow (months-years; axonal regrowth ~1 mm/day) | Faster (weeks-months; muscle protein resynthesis) | Slow, often incomplete |
Assessment — measuring weakness and functional capacity
You cannot rehabilitate what you cannot measure. A structured assessment drives the prescription and tracks recovery. The ATS ICU-AW diagnosis guideline (Fan 2014) and the ATS/ERS pulmonary rehabilitation statement (Spruit 2013) define the core toolset.[11][12]
Assessment instruments for post-ICU rehabilitation
| Tool | What it measures | Score / threshold | Setting | Strengths / limits |
|---|---|---|---|---|
| MRC sum score | Voluntary limb muscle power | 6 muscle groups × bilaterally, 0-5 each → total 0-60. <48 = ICU-AW; <36 = severe | ICU (awake/cooperative) | Bedside, validated; cannot use in sedated/uncooperative patient |
| Handgrip dynamometry | Global muscle strength proxy | Male <11 kg, Female <7 kg = low (ICU/prognostic); EWGSOP2 sarcopenia male <27, female <16 kg | ICU / ward / clinic | Simple, prognostic; dominant hand; effort-dependent |
| Medical Research Council dyspnoea (mMRC) | Activity-related breathlessness | 0 (none) to 4 (too breathless to leave house) | Clinic | Subjective but reproducible |
| 6-Minute Walk Test (6MWT) | Submaximal functional exercise capacity | Per ATS 2002; healthy ~500-700 m; <300 m severely impaired; MCID ~25-35 m | Ward / clinic (not acutely unwell) | Objective, correlates with survival; needs walking ability |
| CPET (cardiopulmonary exercise testing) | Peak VO2, anaerobic threshold | Gold-standard fitness measure | Pre-surgery / clinic | Most precise; needs equipment, not ICU-suitable |
| PFIT-s / FSS-ICU / CPAX | ICU-specific physical function | Structured scoring of assisted-active tasks | ICU (even ventilated) | Designed for critically ill; usable early |
| Barthel Index / FIM | Activities of daily living | Barthel 0-100 (lower = more dependent) | Ward / discharge / rehab | Functional endpoint; tracks toward independence |
| EQ-5D / SGRQ | Generic / disease-specific quality of life | SGRQ lower = better (MCID ~4 units) | Clinic / follow-up | Patient-reported; captures the whole-PICS picture |
MRC sum score in detail — the bedside workhorse for ICU-AW. Assess six movements scored 0-5 on each side (12 measurements): shoulder abduction, elbow flexion, wrist extension, hip flexion, knee extension, ankle dorsiflexion.[11]
- 0 = no visible contraction
- 1 = flicker/trace of contraction
- 2 = active movement with gravity eliminated
- 3 = movement against gravity
- 4 = movement against gravity plus moderate resistance
- 5 = normal power
Total 0-60. Sum <48 (mean of assessable items) = ICU-acquired weakness; <36 = severe weakness, predicting poor 1-year outcome. Its principal limitation is the requirement for an awake, cooperative, command-following patient — impossible in the deeply sedated, exactly the group at highest risk. [1]
Early mobilisation — the staged protocol
Early mobilisation is delivered as a functional progression, escalating the patient one rung at a time and stepping back if they cannot tolerate the current rung.[3][13]
ICU early mobilisation ladder — passive → active → walking
- PASSIVE range of motion (day 1, any patient) — nurse/physio moves each joint through full ROM; prevents contractures, stimulates proprioception, is feasible even on NMBA/ECMO.
- ACTIVE-ASSISTED movement — patient attempts movement with assistance (e.g., assisted limb lifting, rolling in bed, assisted sit-up in bed).
- ACTIVE movement in bed — patient moves limbs unaided; ankle pumps, quadriceps sets, gluteal sets, resisted bands (low resistance).
- SITTING over edge of bed — feet on floor or footplate; major cardiovascular and vestibular challenge after prolonged lying; first upright posture.
- BED → chair transfer / chair sitting — hoist or assisted transfer; tolerates longer upright time; enables eating, communication, chest physio.
- STANDING / weight-bearing — sit-to-stand with frame/staff; reconditions antigravity muscles and orthostatic tolerance.
- MARCHING on spot / stepping — prepares for gait; assesses balance and weight-bearing endurance.
- WALKING (with/without aid; ventilator on portable support if needed) — the goal; even a few steps on day 3-5 of ventilation is achievable with a mobilisation team.
- PROGRESSIVE ambulation and ADL retraining — increase distance daily; add stairs, ADLs (washing, dressing), resistive exercises; bridge to ward and formal rehab programme.
Safety criteria — when you CAN vs when you must NOT mobilise
| You MAY mobilise if… | Do NOT mobilise (or seek senior review) if… |
|---|---|
| FiO2 <0.6 and PEEP <10 cmH2O (stable vent settings) | FiO2 ≥0.6 or rapidly escalating ventilator demands |
| RASS −1 to +1 (awake/cooperative or calmly resting) | RASS −3 to −5 (deeply sedated) or severe agitation (RASS +3/+4) |
| Noradrenaline <0.5 mcg/kg/min and stable haemodynamics | High/rising vasopressor doses, unstable arrhythmia, active myocardial ischaemia |
| Stable respiratory status (SpO2 ≥92%, no active desaturation) | Active life-threatening hypoxaemia, unstable airway, active massive haemorrhage |
| No unstable fracture / spinal precaution | Unstable spinal injury, untreated raised ICP, unstable pelvic/femoral fracture |
| Delirium screen performed; pain controlled | Uncontrolled pain, unsafe to self or staff |
Inspiratory (respiratory) muscle training
Limb-muscle training alone does not recondition the diaphragm. The diaphragm atrophies rapidly under fully controlled ventilation, and respiratory muscle weakness is a major cause of weaning failure and persisting dyspnoea.[17] Inspiratory muscle training (IMT) targets this directly.
Inspiratory muscle training (IMT) protocol
- Baseline measure — maximal inspiratory pressure (MIP / PImax) at residual volume; <−60 cmH2O (male) or <−50 cmH2O (female) suggests weakness.
- Choose device — Threshold IMT (flow-independent, fixed resistive load) or PFLEX (variable resistance); incentive spirometry (Voldyne) for volumetric training is simpler but less load-specific.
- Set load — start at ~30-50% of MIP; progress load as strength improves.
- Prescription — typically 5 sets of 5-10 inspiratory manoeuvres, once or twice daily, 5-7 days/week; rest between sets.
- Progress — increase resistance by ~5-10% weekly as tolerated; re-measure MIP weekly.
- Continue — through weaning and into the post-discharge pulmonary rehabilitation programme for 6-12 weeks.
The 2018 systematic review and meta-analysis (Vorona et al.) found IMT significantly increases inspiratory muscle strength (MIP) in critically ill adults and may shorten weaning time, though the evidence base is modest and dominated by small trials.[17] It is a low-cost, low-risk intervention worth offering to patients with documented respiratory muscle weakness or difficult weaning.
The structured pulmonary rehabilitation programme
Once through the acute phase, the patient transitions to a formal pulmonary rehabilitation programme — the model proven in COPD (where it is among the most cost-effective interventions in all of medicine) and now extended to post-ICU / post-ARDS recovery.[12][15]
Pulmonary rehabilitation programme — assessment → exercise → wrap-around
- ASSESS at entry (and re-measure at 6-12 wk) — 6MWT (ATS protocol), mMRC dyspnoea, handgrip, MRC sum score if relevant, SGRQ/EQ-5D, spirometry, smoking status, comorbidities, nutrition (MUST), mood (HADS), social/vocational context.[16]
- AEROBIC training — walking, stationary cycling, arm ergometry, treadmill. Target 20-60 min at 60-80% of peak heart rate or Borg dyspnoea 4-6 (moderate-severe); 3-5 sessions/week; interval training if severely deconditioned.
- RESISTANCE training — 8-10 major muscle groups (legs, back, chest, arms, core); 1-3 sets of 8-12 repetitions at 60-80% of 1-repetition maximum; progress weekly. Rebuilds the muscle mass lost to acute wasting.
- INSPIRATORY muscle training — for documented diaphragm weakness or persistent dyspnoea/weaning difficulty (see above).
- EDUCATION — disease understanding, medication adherence, breathing techniques (pursed-lip, diaphragmatic), airway clearance, energy conservation, smoking cessation, vaccination (influenza, pneumococcal, COVID-19, RSV).
- NUTRITIONAL counselling — rebuild muscle mass: protein 1.2-1.5 g/kg/day, energy 25-30 kcal/kg/day; correct malnutrition/sarcopenia; monitor refeeding syndrome (PO4, Mg, K).
- PSYCHOLOGICAL support — screen (HADS, IES-6/PCL-5) and treat anxiety/depression/PTSD; CBT, peer support, ICU diaries; treat the whole PICS, not the legs alone.
- VOCATIONAL & social rehabilitation — phased return to work (50-70% return within 1 year), workplace modifications, driving assessment, home adaptation.
- MAINTENANCE — after the formal 6-12 week programme, ongoing home/community exercise with periodic reassessment to prevent relapse of the deconditioning spiral.
Aerobic vs resistance training in post-ICU rehab
| Feature | Aerobic training | Resistance training |
|---|---|---|
| Primary target | Cardiopulmonary fitness, exercise capacity (peak VO2, 6MWT) | Muscle mass and strength (the deficit from acute wasting) |
| Examples | Walking, cycling, treadmill, arm ergo | Weights, bands, weight-bearing, sit-to-stand, stairs |
| Dose | 20-60 min, 60-80% peak HR, 3-5×/week | 8-10 muscle groups, 1-3 sets × 8-12 reps, 2-3×/week |
| Monitors | Borg dyspnoea 4-6, HR target, SpO2 ≥88% | Load progression, perceived exertion, no substitution |
| Both | Required — combined programmes outperform either alone for functional outcomes after critical illness |
Barriers to mobilisation and rehabilitation
The single most common reason rehabilitation does not happen is the belief that the patient is "too sick to move" — usually wrong, but genuine barriers exist and must be actively managed rather than used as a blanket excuse.[13][14]
Barriers to ICU mobilisation — and how to overcome them
| Barrier | Why it matters | Practical solution |
|---|---|---|
| Lines & tubes (ETT, CVC, arterial line, dialysis line, catheter, chest drains, NG) | Dislodgement risk; staff fear | Secure lines, route them clear of limbs, use a designated "line handler" during moves, prefer femoral→internal jugular access to free arms |
| Delirium | Cannot follow commands; falls/line-pull risk | Screen daily (CAM-ICU/ICDSC); treat cause; mobilise during lucid windows; avoid benzodiazepines |
| Excess sedation | Reduces awake/active time | Daily SAT + SBT (ABCDEF bundle); use dexmedetomidine/propofol over midazolam; keep RASS target −1 to +1 |
| Sleep disruption | Fatigue, poor engagement | Bundle care at night, minimise noise/light, treat pain/agitation, consider earplugs/eye mask |
| Haemodynamic instability | Falls, arrhythmia, desaturation | Respect safety criteria; reduce vasopressors first; escalate rung only when stable for ≥2 h |
| Ventilator dependence | Restricts mobility, fear of disconnection | Portable ventilator, long circuits, dedicated respiratory therapist on the mobilisation team |
| Pain | Guards against movement, fatigue | Assess (CPOT/BPS in non-verbal; NRS in verbal); pre-medicate before sessions |
| Staffing & equipment | Mobilising a ventilated patient is a team sport | Dedicated mobilisation team (physio + nurse + doctor + assistant); hoist, tilt table, portable vent, cycle ergometer |
| Patient fear / low motivation | Kinesiophobia after prolonged illness | Goal-setting, motivational interviewing, peer support, ICU diaries, celebrate small wins |
| Medical instability "blanket excuse" | Default position of "too sick" | Document objective safety criteria; default is to mobilise unless a specific criterion is breached |
The ABCDEF bundle is the organising framework that removes these barriers systematically and is the single most evidence-based approach to preventing the physical (and cognitive/mental) domain of PICS:[13]
- Assess and manage pain
- Both spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT)
- Choice of analgesia and sedation (delirium-friendly — avoid benzodiazepines)
- Delirium — assess, prevent, manage
- Early mobility and exercise
- Family engagement and empowerment
SAQ — Early mobilisation of a ventilated ICU patient
10 minutes · 10 marks
A 58-year-old man is on day 6 of invasive ventilation for severe ARDS caused by pneumococcal pneumonia. Ventilator settings are FiO2 0.45, PEEP 8 cmH2O, assist-control. He is on noradrenaline 0.08 mcg/kg/min, RASS -1, CAM-ICU negative, SpO2 95%. He has an endotracheal tube, a right internal jugular central line, a left radial arterial line and a urinary catheter. The bedside nurse asks whether he can be mobilised today.
SAQ — Pulmonary rehabilitation after ICU discharge
10 minutes · 10 marks
A 62-year-old woman is reviewed in the post-ICU follow-up clinic 6 weeks after an 18-day ICU admission for severe ARDS caused by pandemic influenza (intubated on day 0, extubated on day 14, discharged home on day 22). She has an MRC sum score of 42/60, handgrip dynamometry 12 kg, 6-minute walk test (6MWT) 280 m (40% predicted), mMRC dyspnoea grade 3, and a HADS score of 16 (anxiety 9, depression 7). She asks when she can return to her job as a secondary-school teacher.
Clinical pearls
Red flags
Prognosis and outcomes
Outcomes after ICU — what to tell patients and families
| Outcome | Frequency / magnitude | Note |
|---|---|---|
| Persistent physical weakness at 1 year | 30-40% of ICU-AW patients | Most improve, many never return to baseline |
| Cognitive impairment at 1 year | 30-50% | Resembles mild traumatic brain injury; slowly improves |
| Depression/anxiety/PTSD | ~30/40/20% | Worsens after discharge as memories consolidate |
| Return to work within 1 year | 50-70% (with phased return) | Younger age, fewer comorbidities, lower illness severity predict return |
| 6MWT recovery | Often <70% predicted at 3-6 months | Recovers over 1-2 years; formal rehab accelerates it |
| ICU-AW: CIM recovery | Weeks-months | Muscle protein resynthesis is faster than nerve regrowth |
| ICU-AW: CIP recovery | Months-years | Axonal regrowth ~1 mm/day; some permanent deficit |
| Pulmonary rehab effect (6-12 wk) | ↑ 6MWT, ↓ dyspnoea, ↑ QoL | Among the most cost-effective interventions in medicine (COPD model) |
Key trials and evidence
TEAM Trial — Hodgson et al., NEJM 2022 (PMID 36286256)
Design
Multicentre randomised controlled trial — 750 mechanically ventilated adults (Australia/NZ)
Population
Adults intubated within 5 days, expected to remain ventilated; ICU stay ≥48 h
Intervention
Early, active mobilisation (≥60 min/day active + functional exercises, commenced within 5 days) vs usual care (mobilisation at clinician discretion)
Primary outcome
Days alive and out of hospital at 180 days
Key result
NO significant difference: median 143 days (early active) vs 145 days (usual care); more adverse events (e.g., cardiac arrhythmias) in the active group
Clinical bottom line
Routine aggressive early active mobilisation did NOT improve outcomes and caused more harm than usual care — mobilise selectively and respect safety criteria; 'more is not always better'
Schweickert et al., Lancet 2009 (PMID 19446324) — the landmark positive trial
Design
Single-centre randomised controlled trial — 104 mechanically ventilated patients
Population
Intubated <72 h, expected to ventilate >72 h more
Intervention
Early physical + occupational therapy (within 72 h, daily, progressive) vs usual care (therapy at physician discretion)
Primary outcome
Return to independent functional status at hospital discharge
Key result
59% (early) vs 35% (usual care) returned to independent function; more ventilator-free days (23.5 vs 21.7); shorter delirium duration (2 vs 4 days)
Clinical bottom line
Early, structured mobilisation begun within 72 h of intubation improves functional outcomes, ventilator-free days and delirium — the foundational trial for early ICU mobility
Burtin et al., Critical Care Medicine 2009 (PMID 19623052)
Design
Single-centre randomised controlled trial — 90 long-stay ICU patients
Intervention
Daily 20-minute bedside cycle ergometry (passive → active) vs usual care
Key result
Better functional status at hospital discharge, better 6MWT and quadriceps force at discharge, trend to improved 12-month survival
Clinical bottom line
In-bed cycling is feasible and improves functional recovery in long-stay ICU patients — a practical adjunct to whole-body mobilisation
REVIVE — McWilliams et al., Journal of Critical Care 2018 (PMID 29331668)
Design
Feasibility randomised controlled trial — ~60 mechanically ventilated patients
Intervention
Earlier and enhanced rehabilitation (additional structured physiotherapy sessions) vs standard care
Primary outcome
Feasibility (recruitment, adherence, safety)
Key result
Feasible and safe; improved Manchester Mobility Score at ICU discharge; signal toward better functional outcomes
Clinical bottom line
Earlier, enhanced in-ICU rehab is feasible and promising, but feasibility-grade evidence only — larger definitive trials are needed
Puthucheary et al., JAMA 2013 (PMID 24108501) — the wasting cohort
Design
Prospective observational cohort — 63 ICU patients
Measurements
Serial quadriceps ultrasound + rectus femoris biopsy over 10 days
Key result
~12.7% loss of rectus femoris cross-sectional area over 10 days; wasting occurred early (first week); greatest wasting predicted worse outcomes
Clinical bottom line
Acute skeletal muscle wasting is rapid, early and clinically significant — quantifies why prevention (early mobility, nutrition) cannot wait
Vorona et al., Ann Am Thorac Soc 2018 (PMID 29584447) — IMT meta-analysis
Design
Systematic review and meta-analysis of inspiratory muscle training in critically ill adults
Key result
IMT significantly increased maximal inspiratory pressure (MIP); signal toward shorter weaning duration
Clinical bottom line
IMT is a low-cost, low-risk intervention that improves inspiratory muscle strength in critically ill adults — offer to patients with documented respiratory muscle weakness or difficult weaning
Summary
Post-ICU pulmonary and functional rehabilitation treats the physical domain of the post-intensive care syndrome. It is staged (ICU early mobilisation → ward → formal 6-12 week pulmonary rehabilitation programme) and multidomain (aerobic + resistance exercise, inspiratory muscle training, education, nutrition, psychological support, vocational retraining). The dominant reversible deficit is ICU-acquired weakness (CIP/CIM, 25-50% of long-stay patients), assessed by the MRC sum score, handgrip dynamometry and the 6-minute walk test. Evidence supports early, selective mobilisation (Schweickert, Burtin) but warns against routine aggressive mobilisation (TEAM). The ABCDEF bundle removes mobilisation barriers. Outcomes are hard-won: 30-50% never fully recover, so rehabilitation must begin in the ICU, continue for months, and treat the whole patient — physical, cognitive and mental — not the legs alone.[2][3][4][12][13]
References
- [1]Niederman MS, Torres A. Severe community-acquired pneumonia Eur Respir Rev, 2022.PMID 36517046
- [2]Needham DM, Davidson A, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders' conference Crit Care Med, 2012.PMID 21946660
- [3]Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial Lancet, 2009.PMID 19446324
- [4]Hodgson CL, Capell EAG, Higgins AM, et al. (TEAM Study Investigators and the ANZICS Clinical Trials Group). Early Active Mobilization during Mechanical Ventilation in the ICU N Engl J Med, 2022.PMID 36286256
- [5]McWilliams DJ, Weblin J, Atkins G, et al. Earlier and enhanced rehabilitation of mechanically ventilated patients in critical care: A feasibility randomised controlled trial J Crit Care, 2018.PMID 29331668
- [6]Burtin C, Clerckx B, Robbeets C, et al. Early exercise in critically ill patients enhances short-term functional recovery Crit Care Med, 2009.PMID 19623052
- [7]Puthucheary ZA, Rawal J, McPhail M, et al. Acute skeletal muscle wasting in critical illness JAMA, 2013.PMID 24108501
- [8]Hermans G, Van den Berghe G. Clinical review: intensive care unit acquired weakness Crit Care, 2015.PMID 26242743
- [9]Hermans G, De Jonghe B, Bruyninckx F, Van den Berghe G, et al. Interventions for preventing critical illness polyneuropathy and critical illness myopathy Cochrane Database Syst Rev, 2014.PMID 24477672
- [10]Latronico N, Herridge M, Hopkins RO, et al. The ICM research agenda on intensive care unit-acquired weakness Intensive Care Med, 2017.PMID 28289812
- [11]Fan E, Cheek F, Chlan L, et al. An official American Thoracic Society Clinical Practice guideline: the diagnosis of intensive care unit-acquired weakness in adults Am J Respir Crit Care Med, 2014.PMID 25496103
- [12]Spruit MA, Singh SJ, Garvey C, et al. (ATS/ERS Task Force). An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation Am J Respir Crit Care Med, 2013.PMID 24127811
- [13]Devlin JW, Skrobik Y, Gelinas C, et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU Crit Care Med, 2018.PMID 30113379
- [14]Connolly B, O'Neill B, Salisbury L, McPherson H, et al. Physical rehabilitation interventions for adult patients during critical illness: an overview of systematic reviews Thorax, 2016.PMID 27220357
- [15]Spruit MA, Pitta F, Garvey C, et al. Differences in content and organisational aspects of pulmonary rehabilitation programmes Eur Respir J, 2014.PMID 24337043
- [16]ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test Am J Respir Crit Care Med, 2002.PMID 12091180
- [17]Vorona S, Sabatini U, Al-Maqbali S, et al. Inspiratory Muscle Rehabilitation in Critically Ill Adults. A Systematic Review and Meta-Analysis Ann Am Thorac Soc, 2018.PMID 29584447