ICU · GI & nutrition
GI Bleeding, Pancreatitis, Hepatic Failure and Nutrition
Also known as GI bleeding · Acute pancreatitis · Acute liver failure · Nutritional support · Stress ulcer prophylaxis · Enteral nutrition
The GI and the nutritional disorders in the ICU span the upper GI bleeding (the peptic ulcer, the varices), the acute pancreatitis (the severe, the infected necrosis), the acute liver failure (the paracetamol, the encephalopathy), and the nutritional support (the early enteral preferred, the stress ulcer prophylaxis). This topic builds the examiner's framework on each, with the evidence for the stress ulcer prophylaxis (the SUP-ICU trial), the early enteral nutrition (the NUTRIREA-2 trial), the route of feeding (the CALORIES trial), the permissive underfeeding (the Arabi Permissive Underfeeding trial), the caloric and the protein targets (the ESPEN and the SCCM/ASPEN guidelines, the indirect calorimetry), and the acute liver failure (the King's College criteria).
On this page & tools
Your progress
Saved locally on this device.
Target exams

Overview & definition
The GI and the nutritional disorders are the common ICU complications — from the stress ulcer prophylaxis to the acute variceal bleed, from the mild pancreatitis to the severe necrotising, from the early enteral nutrition to the acute liver failure with the encephalopathy. Each has a specific, the evidence-based management, and the intensivist's role is the recognition, the resuscitation, and the targeted therapy.[1][2]
The upper GI bleeding
The upper GI bleeding presents with the haematemesis, the melaena, or the coffee-ground aspirate. The two commonest causes are the peptic ulcer disease (the Helicobacter, the NSAID) and the oesophageal varices (the portal hypertension from the cirrhosis).[1]
The resuscitation. The ABCDE — the airway (the aspiration risk in the massive haematemesis — the early intubation), the breathing (the oxygenation), the circulation (the two large-bore cannulae, the fluid, the blood — the damage-control principles, the restrictive transfusion at the Hb of 70, the correction of the coagulopathy and the platelets).[2]
The peptic ulcer bleed. The proton pump inhibitor infusion (the pantoprazole 80 mg bolus then 8 mg/h), the upper GI endoscopy within 24 hours (the adrenaline injection, the clipping, the thermal coagulation), and the Helicobacter eradication. The risk stratification (the Glasgow-Blatchford score for the admission; the Rockall score for the post-endoscopy risk).[1]
The variceal bleed. The vasoactive drug (the terlipressin or the octreotide — the splanchnic vasoconstriction), the prophylactic antibiotic (the ceftriaxone — the cirrhotic patient is immunocompromised and the infection worsens the outcome), the band ligation (the endoscopic), and the TIPSS (the transjugular intrahepatic portosystemic shunt) for the refractory. The balloon tamponade (the Sengstaken-Blakemore) is the bridge to the definitive therapy.[1][2]
The acute pancreatitis
The acute pancreatitis is the inflammation of the pancreas from the gallstone, the alcohol, the ERCP or the other cause. The severity ranges from the mild (the majority, self-limiting) to the severe (the necrotising, the infected, the multi-organ failure).[1]
The management. The aggressive fluid resuscitation (the lactated Ringer's preferred — the goal-directed), the analgesia (the opiate), the early enteral nutrition (the modern standard — NOT the prolonged fasting; the nasogastric or the nasojejunal if the gastric feeding not tolerated), the ERCP for the gallstone with the cholangitis or the obstruction, and the antibiotics ONLY for the proven or the suspected infected necrosis (NOT the prophylactic — the previous practice of the prophylactic carbapenem is disproven). The necrosectomy (the minimally invasive, the delayed — the 4-week rule for the walling-off) for the infected necrosis.[1][2]
The acute liver failure
The acute liver failure is the severe, the acute hepatocellular injury with the coagulopathy and the encephalopathy — the commonest cause in the developed world is the paracetamol (the acetaminophen) overdose, followed by the drug-induced, the viral and the indeterminate.[1]
The management. The N-acetylcysteine (the NAC — for the paracetamol overdose AND, increasingly, for the non-paracetamol ALF — the antioxidant, the glutathione replenishment), the encephalopathy management (the lactulose, the rifaximin — the ammonia reduction; the intubation for the grade 3 to 4 encephalopathy; the raised ICP management — the mannitol, the hypertonic saline), the coagulopathy (the vitamin K, the fresh frozen plasma only for the bleeding or the procedure — NOT routinely, for the INR is a prognostic marker not a treatment target), and the liver transplant for the poor prognosis (the King's College criteria).[1][2]
The King's College criteria for the paracetamol ALF transplant: the arterial lactate above 3.5 after the early resuscitation, or above 3.0 after the fluid resuscitation; OR the arterial pH below 7.25; OR all three of the INR above 6.5, the creatinine above 300, and the grade 3 to 4 encephalopathy.[1]
The stress ulcer prophylaxis
The stress ulcer bleeding was historically common in the ventilated ICU patient. The modern practice is the selective — the acid suppression (the PPI or the H2 blocker) for the high-risk patient: the mechanical ventilation over 48 hours, the coagulopathy, the shock, the sepsis, the major burns, the traumatic brain injury, the history of the GI bleeding. The routine prophylaxis for the low-risk patient is NOT recommended (the increased pneumonia risk from the gastric alkalinisation).[1][2]
The nutritional support
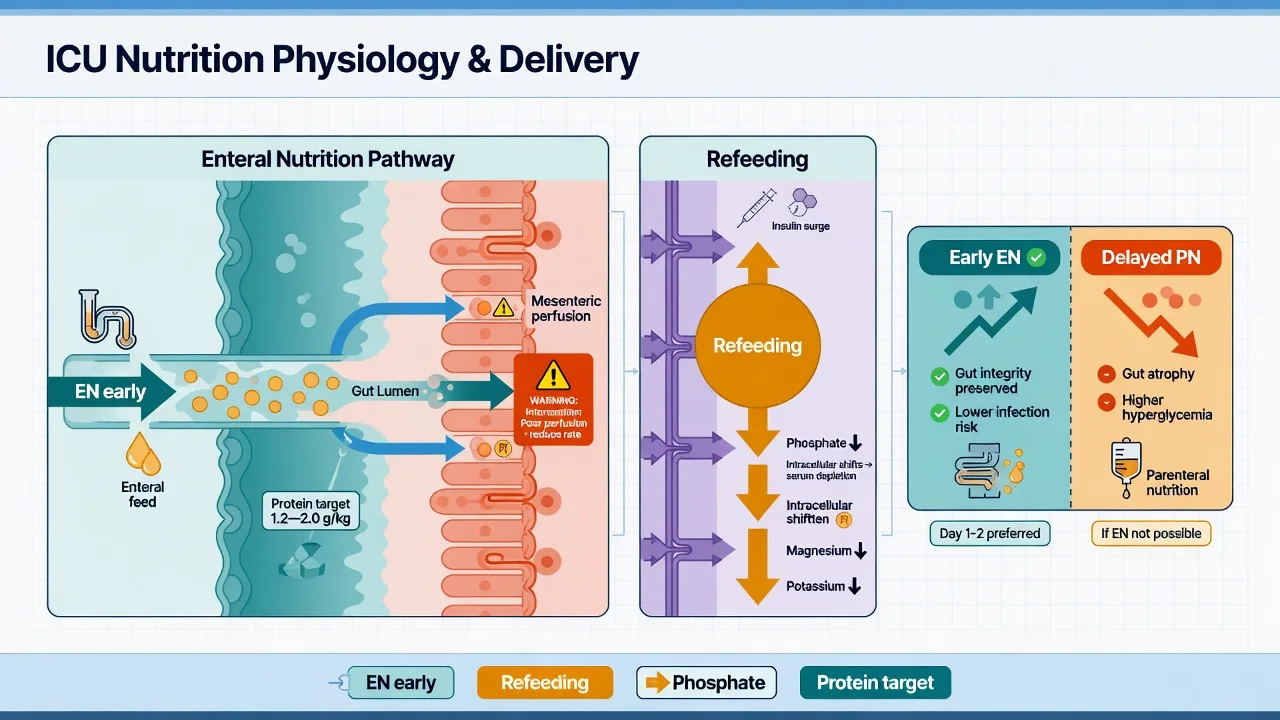
The early enteral nutrition (within 24 to 48 hours) is the standard for the ICU patient — it maintains the gut mucosal integrity, reduces the bacterial translocation, modulates the immune response, and improves the outcome. The parenteral nutrition is reserved for the patient who cannot tolerate the enteral (the prolonged ileus, the high-output fistula, the mesenteric ischaemia) or the malnourished patient whose enteral nutrition is inadequate after 5 to 7 days.[1][2]
The refeeding syndrome. The malnourished patient started on the nutrition is at risk of the refeeding syndrome — the hypophosphataemia, the hypokalaemia, the hypomagnesaemia, the fluid retention, the cardiac arrhythmia. The prevention is the slow escalation (the 10 to 15 kcal/kg/day for the first week in the high-risk), the electrolyte replacement, the thiamine, and the monitoring.[1][2]
Enteral versus parenteral nutrition: the route question
The enteral nutrition (EN) is preferred over the parenteral nutrition (PN) in nearly all critically ill patients who have a functioning gut. The biological rationale is robust: enteral feeding maintains the gut mucosal integrity, supports the gut-associated lymphoid tissue (GALT), preserves the intestinal brush border enzyme activity, attenuates the stress-induced immune response, and reduces the bacterial translocation that drives the nosocomial infection and the multi-organ failure. The enteral route is cheaper, safer (no central line, no catheter-related bloodstream infection, no metabolic derangement), and is associated with fewer infectious complications in the meta-analytic data.[9][10]
The CALORIES trial (Harvey 2014, NEJM) is the landmark randomised study on the route. In 2400 mechanically ventilated ICU patients, early EN was compared with early PN within 36 hours of admission and continued for up to 5 days. There was no difference in the 30-day mortality between the two groups (EN 39% vs PN 40%). However, the EN group had fewer episodes of hypoglycaemia and a lower mean glycaemic load. The trial settled the question: when the gut works, the EN and the PN give equivalent mortality — but the EN is cheaper, safer, and physiologically superior, so it remains the default.[4]
Enteral nutrition (EN) — preferred
The default route
- Maintains the gut mucosal integrity, the villous architecture, the brush border enzymes — prevents the villous atrophy of starvation
- Supports the gut-associated lymphoid tissue (GALT) and the mucosal immunity — reduces the bacterial translocation and the nosocomial infection
- Lower infection rate (catheter-related bloodstream infection, pneumonia, bacteremia) in meta-analyses compared with the PN
- Cheaper, no central venous access required, no PN-associated hepatotoxicity or cholestasis, less hyperglycaemia
- Started early (within 24 to 48 hours) in any patient with a functioning gut — the standard of care in the ICU
- Risks: aspiration (head of bed elevated, prokinetics, post-pyloric if high aspiration risk), diarrhoea (titrate osmolality, treat the cause), distension
Parenteral nutrition (PN) — reserved
When the gut cannot be used
- Reserved for the patient with the genuine GI dysfunction: the prolonged ileus unresponsive to the prokinetic, the high-output fistula, the mesenteric ischaemia, the bowel obstruction, the severe short bowel syndrome
- Indicated in the malnourished patient (NRS-2002 ≥5) who is unable to meet the caloric target via the EN alone within 3 to 5 days — supplemental PN
- NUTRIREA-2: the early PN in shock in place of the EN did NOT improve the outcome and INCREASED the infection and the ICU-acquired weakness — do not start the PN routinely in the shock
- Requires a dedicated central line (or peripherally inserted central catheter), strict asepsis, the pharmacist-compounded all-in-one bag, the careful glucose and triglyceride monitoring
- Complications: the catheter-related bloodstream infection, the hyperglycaemia, the refeeding syndrome, the PN-associated liver disease (cholestasis, steatosis), the metabolic bone disease with the long-term use
Contraindications to enteral nutrition
When NOT to feed enterally
- ABSOLUTE: the mesenteric ischaemia, the complete bowel obstruction, the severe ileus with the abdominal compartment syndrome, the high-output enterocutaneous fistula (relative — the fistuloclysis is possible)
- RELATIVE: the haemodynamic instability on the high-dose vasopressors (do NOT start the EN in unresuscitated shock — the NUTRIREA-2 showed the mesenteric ischaemia risk), the recent major GI surgery (often tolerated within 24 hours in the modern enhanced recovery), the severe acute pancreatitis with the ileus (start the NG, escalate to the NJ if intolerant)
- The "feeding the dead gut" dogma is largely disproven — the ileus often resolves with the feeding, and the prolonged fasting worsens the villous atrophy
- When in doubt, the trial of low-rate trophic EN (10 to 20 mL/h) is preferred over the immediate PN
Timing of nutrition: the early EN question
The early enteral nutrition (within 24 to 48 hours of the ICU admission) is the modern standard for the critically ill patient who is no longer in active unresuscitated shock. The evidence base is now extensive: the early EN reduces the infection, the ICU-acquired weakness, the length of stay, and possibly the mortality (the effect is modest but consistent across the meta-analyses).[9][10]
The NUTRIREA-2 trial (Reignier 2018, Lancet) is the pivotal study on the timing AND the route in shock. It randomised 2410 mechanically ventilated adults with shock (all severities, all causes) to the early EN versus the early PN, both started within 24 hours and isocaloric. The result: there was no difference in the 28-day mortality (EN 37% vs PN 35%) or the infection rate. Crucially, the early PN did NOT improve the outcome — and the EN group had a SIGNIFICANTLY HIGHER rate of the digestive ischemia (1.0% vs 0.0%, p=0.03) and the bowel ischaemia requiring surgery. The takeaway: in the ventilated patient with the shock, the early EN is the standard, but the clinician must be vigilant for the mesenteric ischaemia — and the early PN confers NO benefit.[3]
NUTRIREA-2 — Early EN versus early PN in shock (Reignier, Lancet 2018)
Multicentre randomised controlled open-label parallel-group trial: 2410 adults
Population: Mechanically ventilated adults with circulatory shock (any cause, any severity) within 24 h of intubation
Key finding
No significant difference in 28-day mortality (37% EN vs 35% PN; adjusted HR 1.06, 95% CI 0.88 to 1.27, p=NS). No difference in the cumulative infection rate. EN group had HIGHER digestive ischaemia (1.0% vs 0%, p=0.03) and higher vomiting (notably on day 2 to 3). PN group had more ICU-acquired weakness (7% vs 6%, p=NS) and a higher cumulative proportion of antimicrobial days.
Practice change
In the ventilated patient with the shock, the early EN and the early PN give equivalent mortality and infection outcomes. Early PN provides NO benefit over the EN in shock — the default remains the early EN, with vigilance for the bowel ischaemia (especially with the high-dose noradrenaline). The trial definitively ended the practice of routine early PN in the critically ill shock patient.
Caloric and protein targets in the ICU
The caloric and the protein targets are the two pillars of the ICU nutrition prescription. The cardinal error is the overfeeding — which causes the hyperglycaemia, the hypercapnia (raising the minute ventilation and the work of breathing), the hepatic steatosis, the azotaemia, and the increased infection — and the underfeeding — which causes the loss of the lean body mass, the ICU-acquired weakness, the impaired wound healing, and the prolonged ventilation.[10][11]
The caloric target. The gold standard is the indirect calorimetry (the measurement of the oxygen consumption and the carbon dioxide production to derive the resting energy expenditure, REE). Where it is unavailable, the weight-based predictive equation of 25 to 30 kcal/kg/day is used (the ESPEN and the SCCM/ASPEN guidelines). The older Harris-Benedict equation overestimates the energy expenditure in the critically ill and is NOT recommended. The permissive underfeeding (the 70 to 80% of the target for the first week in the well-nourished patient, then advancing to the full target) is supported by the contemporary trials (see below).[10][11]
The protein target. The critically ill patient is in the catabolic state — the nitrogen losses of 20 to 30 g/day (the equivalent of 0.7 to 1 kg of the lean mass per week) are common. The protein target is 1.2 to 2.0 g/kg/day, with the higher end (1.5 to 2.0 g/kg/day) for the patient with the AKI on the CRRT (the CRRT loses the amino acids), the burns, the trauma, and the prolonged ventilation. The protein is delivered as the whey-based or the casein-based enteral formula, or as the amino-acid solution in the PN.[10][11]
Energy (caloric) target
The fuel
- GOLD STANDARD: indirect calorimetry — measure the REE directly. Recommended by the ESPEN and the SCCM/ASPEN when the equipment is available
- PREDICTIVE EQUATION: 25 to 30 kcal/kg/day (the actual body weight in the normal weight, the ideal body weight in the obese, the adjusted in the morbidly obese)
- TROPHIC feeding for the first week in the well-nourished patient: 10 to 20 kcal/kg/day (≈50 to 70% of the target) — the permissive underfeeding, supported by the EDEN, the Permissive Underfeeding trial, and the NUTRIREA-3 design
- Advance to the full target by day 4 to 7 if tolerated — the goal is to avoid both the underfeeding and the overfeeding
- CONFOUNDERS: the obese patient (use the 11 to 14 kcal/kg actual body weight, the 22 to 25 kcal/kg ideal body weight), the burns (up to 35 to 40 kcal/kg/day), the CRRT patient (add the glucose loss on the dialysate)
Protein target
The nitrogen
- 1.2 to 2.0 g/kg/day in the general ICU patient (the SCCM/ASPEN and the ESPEN)
- 1.5 to 2.5 g/kg/day in the burns, the trauma, the CRRT (the amino-acid loss), the prolonged ventilation, the multi-organ failure
- At least 1.2 g/kg/day in the obese patient (the higher end if catabolic)
- The nitrogen balance (the urinary urea nitrogen) can be measured but is unreliable in the AKI and the catabolic state
- The protein delivery, NOT the caloric delivery, is the more important driver of the survival in the observational data — prioritise the protein
Avoiding overfeeding
The harm of excess
- OVERFEEDING (above 100% of the target): the hyperglycaemia, the hypercapnia (raising the PaCO2 and the minute ventilation), the hepatic steatosis, the azotaemia, the increased infection — the CALORIES and the NUTRIREA-2 trials both reinforce that "more is not better"
- GLUCOSE delivery above 4 mg/kg/min causes the hyperglycaemia and the hepatic lipogenesis — limit the glucose to 70% of the non-protein calories
- LIPID delivery above 1.5 g/kg/day (or 1 g/kg/day in the PN) causes the hypertriglyceridaemia and the reticuloendothelial blockade — monitor the triglycerides
- The refeeding syndrome is the worst form of the overfeeding in the malnourished — start low, escalate slowly
Monitoring the adequacy
The audit
- Calorie count: track the prescribed vs the delivered calories daily — the ICU patient typically receives only 60 to 70% of the prescription (the interruptions for the procedures, the fasting, the GI intolerance)
- Indirect calorimetry: re-measure every 5 to 7 days, or after a major change (the fever, the weaning, the surgery)
- Blood glucose: 6 to 10 mmol/L (the Surviving Sepsis range) — the persistent hyperglycaemia suggests the overfeeding OR the insulin resistance
- Triglycerides: weekly, especially on the PN — keep below 4 mmol/L
- Weight: weekly to monthly — the rapid gain suggests the fluid overload, not the nutritional improvement
Permissive underfeeding: the evidence
The permissive underfeeding (the delivery of approximately 50 to 70% of the caloric target, with the full protein delivery, for the first week of the ICU stay) is the contemporary practice in the well-nourished patient. The rationale: the early full feeding in the catabolic patient does not reverse the catabolism (the catabolism is hormonally driven, not substrate-limited) and may worsen the autophagy (the cell-clearance of the damaged mitochondria and the proteins, which is essential for the recovery). The underfeeding respects the autophagy, avoids the overfeeding harm, and delivers the full protein to mitigate the lean mass loss.[5][12]
Permissive Underfeeding — Arabi, NEJM 2015
Multicentre randomised controlled trial: 894 adults
Population: Medical and surgical ICU patients expected to require at least 3 days of mechanical ventilation and enteral nutrition
Key finding
Permissive underfeeding was NOT inferior to the standard feeding for the 90-day mortality (interquartile difference −1.7%, 95% CI −12.0 to 7.6, p=0.71 for non-inferiority; the permissive underfeeding 27.2% vs the standard 28.9%, p=0.58 for superiority). No difference in the infection, the ICU-acquired weakness, the mechanical ventilation duration, or the length of stay. The food (calorie) delivery was significantly lower in the underfeeding group (mean 59.2% vs 71.3% of target).
Practice change
The permissive underfeeding (delivering 40 to 60% of the caloric target for the first week) is SAFE and does not worsen the outcome compared with the standard feeding. The full protein delivery is maintained. This supports the strategy of starting low and advancing — the early underfeeding respects the autophagy, avoids the overfeeding harm, and the patient tolerates the lower caloric load without consequence. The 2024 meta-analysis confirms the consistent signal of safety and a possible reduction in the infection.
Practical aspects of enteral feeding
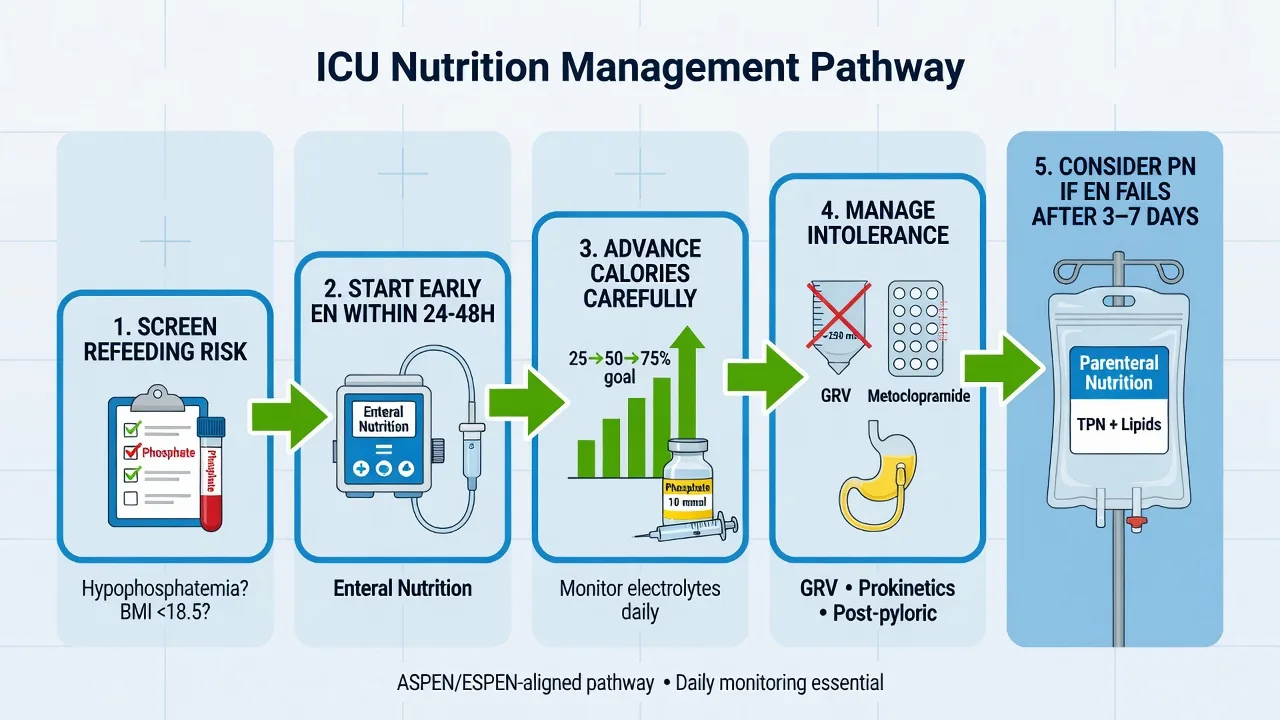
The practical delivery of the enteral nutrition — the route of the tube, the prokinetic, the gastric residual volume (GRV), the position, the monitoring — is the everyday work of the ICU team. The cardinal principle: start the EN early, advance gradually, monitor the tolerance, and use the prokinetics and the post-pyloric route when needed.[9][10]
The tube position — the gastric vs the post-pyloric. The gastric feeding (the nasogastric tube, the NG) is the default — it is easy, the tube is placed at the bedside, and the vast majority tolerate it. The post-pyloric feeding (the nasojejunal tube, the NJ, or the nasoduodenal) is reserved for the patient with the documented gastric intolerance (the high GRV, the vomiting) despite the prokinetic, the severe pancreatitis (the historical, now debated — the NG often works), the severe gastroparesis, the recurrent aspiration. The NJ does NOT reduce the ventilator-associated pneumonia in the meta-analysis — it is not the first choice.[9]
The prokinetics. The metoclopramide (10 mg IV every 8 hours) and the erythromycin (200 mg IV every 12 hours, or 250 mg NG every 8 hours) are the prokinetic agents. The combination (the metoclopramide + the erythromycin) is more effective than either alone for the high GRV. The erythromycin carries the QT-prolongation and the cardiac arrhythmia risk — monitor the ECG, avoid in the long-QT and the concurrent macrolide. The prokinetics are the first-line for the GRV intolerance before the NJ.[9][10]
The gastric residual volume (GRV). The routine GRV monitoring is NO LONGER recommended. The NUTRIREA-2 trial (and the earlier REGANE and the meta-analyses) showed that abandoning the routine GRV monitoring did NOT increase the pneumonia or the outcome harm — and it increased the caloric delivery (fewer interruptions). The current practice: the clinical assessment of the tolerance (the vomiting, the distension, the abdominal examination), the head of bed elevated 30 to 45°, the prokinetic if symptomatic. The GRV is measured only if the patient is symptomatic (the distension, the vomiting, the high aspirate on the suction).[3][9]
Gastric (NG) feeding
The default
- DEFAULT route — the nasogastric tube is placed at the bedside, easy, cheap, fast
- Tolerated by the majority (>80%) of the ICU patients with the head of bed elevated 30 to 45°
- Allows the easy aspiration to check the tolerance if symptomatic
- Suitable for the bolus or the continuous feeding; the bolus is more physiological but the continuous is better tolerated in the early phase
- Does NOT reduce the aspiration risk over the post-pyloric in the meta-analysis (the aspiration is mostly oropharyngeal, not gastric)
Post-pyloric (NJ) feeding
For the intolerant
- INDICATION: the documented gastric intolerance despite the prokinetic, the severe gastroparesis, the severe acute pancreatitis with the ileus, the recurrent aspiration pneumonia
- PLACEMENT: the bedside blind (the Cortrak electromagnetic guidance), the endoscopic, the fluoroscopic — all the techniques require the confirmation of the position (the pH of the aspirate, the X-ray)
- The NJ does NOT reduce the ventilator-associated pneumonia in the meta-analysis (the aspiration is mostly the oropharyngeal secretions, not the gastric contents)
- Reserved for the failure of the NG with the prokinetic — not the first choice
Prokinetic agents
For the intolerance
- METOCLOPRAMIDE 10 mg IV every 8 hours — the dopamine antagonist, the first-line; caution in the Parkinsonism (avoid), the extrapyramidal side effects
- ERYTHROMYCIN 200 mg IV every 12 hours (or 250 mg NG every 8 hours) — the motilin agonist, the second-line or the combination
- COMBINATION (metoclopramide + erythromycin) is more effective than either alone for the refractory high GRV
- CAUTION: the erythromycin prolongs the QT — monitor the ECG, avoid in the long-QT and the concurrent macrolide or the fluoroquinolone
- Use BEFORE the NJ — the prokinetic often restores the tolerance and avoids the NJ placement
Gastric residual volume (GRV)
Largely abandoned
- The routine GRV monitoring is NO LONGER recommended — the NUTRIREA-2 and the REGANE trials showed that abandoning the routine GRV does NOT increase the pneumonia or the harm
- Abandoning the routine GRV INCREASES the caloric delivery (fewer interruptions) — the patient receives more of the prescribed nutrition
- Current practice: the clinical tolerance (the vomiting, the distension, the abdominal examination), the head of bed elevated 30 to 45°, the prokinetic if symptomatic
- If symptomatic (the distension, the vomiting), measure the GRV — the threshold of 500 mL prompts the reassessment, the prokinetic, the slowing of the rate, or the NJ
- The historical threshold of 200 to 250 mL is too low and leads to the unnecessary interruption
Refeeding syndrome: prevention and management
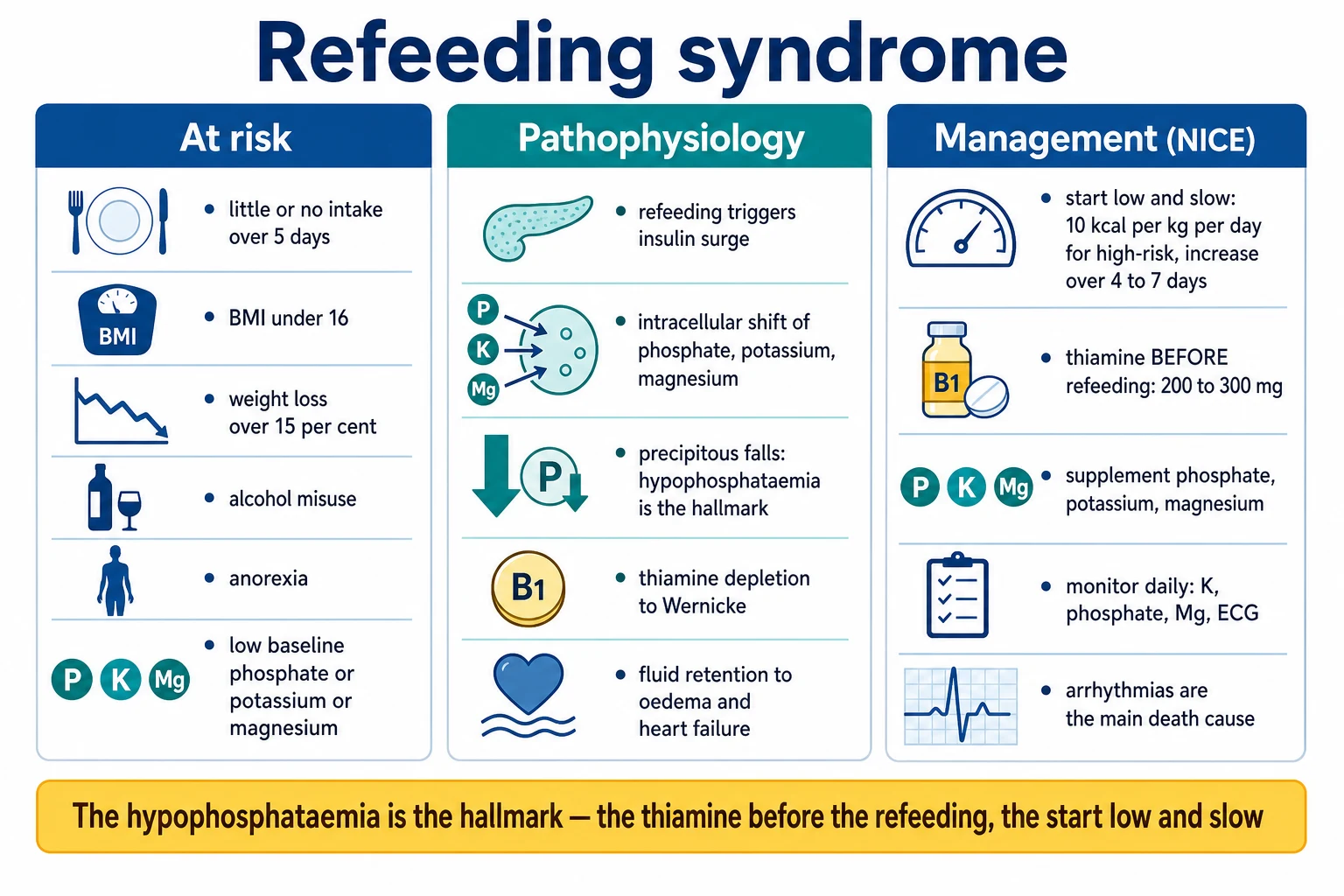
The refeeding syndrome is the potentially fatal metabolic disturbance that occurs when the chronically malnourished or starved patient is fed (the enteral or the parenteral) too rapidly. The mechanism: the refeeding drives the insulin surge, the insulin drives the intracellular shift of the phosphate, the potassium and the magnesium (depleting the serum levels), the glucose becomes the fuel (depleting the thiamine-dependent pathways), and the fluid retention causes the heart failure and the pulmonary oedema. The result: the hypophosphataemia (the weakness, the respiratory failure, the rhabdomyolysis, the haemolysis), the hypokalaemia (the arrhythmia), the hypomagnesaemia (the arrhythmia, the seizures), the thiamine deficiency (the Wernicke, the heart failure), and the fluid overload (the cardiac and the respiratory compromise).[1][10]
The high-risk patient. Anyone with the BMI below 16, the unintentional weight loss over 15% in the 3 to 6 months, the little or no nutritional intake for over 10 days, the low baseline phosphate/potassium/magnesium, the history of the alcohol misuse or the anorexia. These patients need the slow start (10 to 15 kcal/kg/day), the aggressive electrolyte replacement, the thiamine before the feeding, and the daily monitoring.[10]
Refeeding syndrome: the stepwise prevention and management
Step 1 — Identify the high-risk patient
Before the feeding, identify the high-risk: the BMI below 16, the unintentional weight loss over 15% in the 3 to 6 months, the little or no intake for over 10 days, the history of the alcohol misuse or the anorexia, the low baseline phosphate/potassium/magnesium. The NICE criteria stratify the high (BMI <14, the negligible intake over 15 days), the moderate, and the low risk. The high-risk patient needs the slow start and the aggressive monitoring.'
Step 2 — Correct the electrolytes BEFORE the feeding
Check and correct the phosphate, the potassium, the magnesium, and the calcium BEFORE the feeding starts. Do NOT wait for the refeeding to drive them down — pre-emptively replace. The hypophosphataemia (<0.65 mmol/L) is the hallmark — give the IV phosphate (the sodium phosphate 10 to 20 mmol over 4 to 6 hours, repeated as guided). The potassium (keep above 4 mmol/L), the magnesium (keep above 0.75 mmol/L). The calcium often drops as the phosphate is corrected (the 'hungry bone' — monitor).
Step 3 — Give the thiamine BEFORE the first feed
The thiamine is the rate-limiting cofactor of the pyruvate dehydrogenase and the glucose metabolism. The refeeding precipitates the acute thiamine deficiency (the Wernicke encephalopathy, the high-output heart failure). Give the high-dose thiamine (200 to 300 mg PO/NG daily, or the IV 100 to 500 mg daily) BEFORE the first feed and continue for the first 7 to 10 days. The IV route for the alcohol misuse or the severe malnutrition.
Step 4 — Start low and advance slowly
The high-risk patient: start at 10 to 15 kcal/kg/day (the 5 to 10 in the very high risk — the BMI <14, the negligible intake over 15 days). Advance by 100 to 200 kcal/day (or by 5 kcal/kg every 2 to 3 days), monitoring the phosphate, the potassium, the magnesium, the fluid balance. Reach the full target by day 7 to 10. If the electrolytes drop or the arrhythmia occurs, STOP the advance and replete.'
Step 5 — Restrict the fluid and monitor the cardiac
The fluid retention and the heart failure are the feared complications — restrict the total fluid, monitor the daily weights, the JVP, the lung ultrasound (the B-lines). The daily weight gain should be no more than 0.5 to 1 kg/week (the more suggests the fluid). The cardiac monitor (the arrhythmia — the atrial fibrillation, the ventricular ectopy), the ECG daily. The BNP if available.
Step 6 — Daily monitoring for the first week
The phosphate, the potassium, the magnesium, the calcium DAILY for the first 5 to 7 days (then every other day). The clinical: the weakness, the paraesthesia, the oedema, the arrhythmia, the respiratory function. The cardiac monitoring (the telemetry). If the phosphate drops below 0.5 mmol/L or the arrhythmia occurs, SLOW the feeding further or the temporary halt, the aggressive IV replacement.
Step 7 — Supplement the multivitamin and the trace
The refeeding depletes the thiamine, the folate, the vitamin B6, the selenium, the zinc, the copper. The daily multivitamin, the trace-element supplement (the selenium especially — the refeeding cardiomyopathy has been linked to the selenium deficiency). The parenteral preparation if the enteral absorption is uncertain.
Stress ulcer prophylaxis: the SUP-ICU evidence
The SUP-ICU trial (Krag 2018, NEJM) is the contemporary landmark on the stress ulcer prophylaxis. In 3298 ICU patients at risk of the GI bleeding (the mechanical ventilation over 48 hours, the INR over 1.5, the platelet below 50, the renal replacement therapy), the pantoprazole 40 mg IV daily was compared with the placebo. The result: the clinically important GI bleeding was significantly reduced (2.5% pantoprazole vs 4.2% placebo; RR 0.58, 95% CI 0.40 to 0.82), but there was no difference in the 90-day mortality (31% vs 31%), the infection, or the ICU-acquired weakness. The selective prophylaxis in the high-risk patient is confirmed — but the routine prophylaxis in the low-risk patient is NOT recommended (the increased pneumonia from the gastric alkalinisation, the C. difficile risk).[7]
SUP-ICU — Pantoprazole vs placebo for the stress ulcer prophylaxis (Krag, NEJM 2018)
Multicentre randomised double-blind placebo-controlled trial: 3298 ICU adults
Population: ICU patients at risk of the GI bleeding (the mechanical ventilation >48 h, the coagulopathy, the thrombocytopenia, the renal replacement therapy)
Key finding
No significant difference in the 90-day mortality (31.1% pantoprazole vs 30.4% placebo; RR 1.02, 95% CI 0.91 to 1.13). The pantoprazole significantly reduced the clinically important GI bleeding (2.5% vs 4.2%; RR 0.58, 95% CI 0.40 to 0.82; p<0.01). No difference in the infection, the ICU-acquired weakness, the diarrhoea, or the C. difficile.
Practice change
The stress ulcer prophylaxis with the pantoprazole reduces the clinically important GI bleeding in the high-risk ICU patient — but does NOT reduce the mortality. The selective prophylaxis for the high-risk (the ventilated >48 h, the coagulopathic, the shocked, the renal replacement therapy) is confirmed. The routine prophylaxis in the low-risk patient is NOT recommended.
Management: the integrated approach
- The GI bleed — the resuscitation, the endoscopy (the PPI, the band ligation, the terlipressin/antibiotics for the varices), the risk stratification.[1]
- The pancreatitis — the fluid (the lactated Ringer's), the early enteral, the ERCP for the gallstone, the antibiotics only for the infected necrosis.[1]
- The ALF — the NAC, the encephalopathy/ICP, the coagulopathy (selective), the transplant (the King's College).[1]
- The stress ulcer prophylaxis — the selective (the ventilated, the coagulopathic, the shocked).[2]
- The nutrition — the early enteral (within 24 to 48 hours); the parenteral for the intolerant; the refeeding prevention.[1]
Monitoring
- The GI bleed — the haemoglobin, the haemodynamics, the endoscopy findings, the rebleeding.
- The pancreatitis — the CRP (the severity marker at 48 hours — above 150 suggests the severe), the CT severity index (the Balthazar), the organ failure (the Marshall score), the infection markers.
- The ALF — the INR (the prognostic), the ammonia (the encephalopathy), the lactate, the arterial pH, the King's College criteria.
- The nutrition — the electrolytes (the K, the Mg, the phosphate — the refeeding), the gastric residual volumes (the tolerance), the weight, the albumin (the trend, not the single value).[3]
Prognosis
The peptic ulcer bleeding mortality is 5 to 10 per cent. The variceal bleeding mortality is 15 to 20 per cent per the episode (higher with the rebleeding). The severe pancreatitis mortality is 10 to 30 per cent (higher with the infected necrosis and the multi-organ failure). The ALF mortality without the transplant is 50 to 80 per cent (with the transplant, 20 to 30 per cent). The nutritional status is the independent predictor of the ICU outcome.[1][2]
Short-answer questions
SAQ — Early enteral nutrition in a ventilated patient with septic shock
10 minutes · 10 marks
A 68-year-old man (weight 80 kg, BMI 27) is admitted to ICU with community-acquired pneumonia and septic shock. He is intubated and ventilated on noradrenaline 0.25 mcg/kg/min (MAP 68 mmHg after 30 mL/kg of crystalloid), lactate 3.2 mmol/L, creatinine 160 micromol/L, having had minimal oral intake for two days. The registrar proposes starting total parenteral nutrition immediately to 'meet his caloric target without delay'.
SAQ — Stress ulcer prophylaxis in a polytrauma patient on the ICU
10 minutes · 10 marks
A 55-year-old man is admitted after a high-speed motor vehicle crash with a severe traumatic brain injury (GCS 6, intubated), a femoral shaft fracture and a splenic laceration managed non-operatively. He is ventilated and sedated, INR 1.8, platelets 40 x10^9/L from massive transfusion, on noradrenaline for shock, and has been in ICU for 36 hours. The bedside nurse asks whether he should be started on a proton pump inhibitor for stress ulcer prophylaxis.
Red flags
Clinical pearls: the high-yield exam points
Red flags: additional critical points
Compare: the EN vs PN summary at a glance
Enteral (EN)
Preferred
- Route: NG (default), NJ (intolerance), PEG (long-term), surgical jejunostomy
- Start: within 24 to 48 h in the haemodynamically stable patient
- Trophic 10 to 20 mL/h for the first 24 h, advance by 20 to 30 mL/h every 12 to 24 h to the target
- Targets: 25 to 30 kcal/kg/day (or the indirect calorimetry), 1.2 to 2.0 g/kg/day protein
- Tolerated by >80% with the head of bed elevated and the prokinetic
Parenteral (PN)
Reserved
- Route: dedicated central line (or the PICC), the all-in-one pharmacist-compounded bag
- Indication: the genuine GI dysfunction, the malnourished unable to meet the target via the EN in 3 to 5 days
- Composition: the glucose (50 to 70% of the non-protein calories), the lipid (the 30 to 50%), the amino acid (the 1.2 to 2.0 g/kg/day)
- Monitor: the glucose (every 6 h initially), the triglycerides (weekly), the LFTs (weekly), the line (the daily inspection for the infection)
- Avoid the early PN in the shock — the NUTRIREA-2 showed no benefit and possible harm
Combined (EN + supplemental PN)
When the EN is inadequate
- For the malnourished patient unable to meet the target via the EN alone within 3 to 5 days
- Add the supplemental PN to the EN to reach the target — NOT a substitute for the EN
- CALORIES and the NUTRIREA-2 do NOT support the routine early supplemental PN
- Stop the PN when the EN reaches >60 to 80% of the target
References
- [1]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [2]Kazma JM, van den Anker J, Allegaert K, et al. Anatomical and physiological alterations of pregnancy. Journal of pharmacokinetics and pharmacodynamics, 2020.PMID 32026239
- [3]Reignier J, Boisramé-Helms J, Brisard L, et al. (NUTRIREA-2) Enteral versus parenteral early nutrition in ventilated adults with shock: a randomised, controlled, multicentre, open-label, parallel-group study (NUTRIREA-2). Lancet, 2018.PMID 29128300
- [4]Harvey SE, Parrott F, Harrison DA, et al. (CALORIES) Trial of the route of early nutritional support in critically ill adults. New England Journal of Medicine, 2014.PMID 25271389
- [5]Arabi YM, Aldawood AS, Haddad SH, et al. (Permissive Underfeeding) Permissive underfeeding or standard enteral feeding in critically ill adults. New England Journal of Medicine, 2015.PMID 25992505
- [6]Hego A, Boulet M, Lassalle G, et al. (NUTRIREA-3) Impact of early low-calorie low-protein versus standard-calorie standard-protein feeding on outcomes of ventilated adults with shock: design and conduct of a randomised, controlled, multicentre, open-label, parallel-group trial (NUTRIREA-3). BMJ Open, 2021.PMID 33980526
- [7]Krag M, Marker S, Perner A, et al. (SUP-ICU) Pantoprazole in patients at risk for gastrointestinal bleeding in the ICU. New England Journal of Medicine, 2018.PMID 30354950
- [8]Rice TW, Mogan S, Hays MA, et al. (EDEN trial follow-up) One year outcomes in patients with acute lung injury randomised to initial trophic or full enteral feeding: prospective follow-up of EDEN randomised trial. BMJ, 2013.PMID 23512759
- [9]Reintam Blaser A, Starkopf J, Alhazzani W, et al. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intensive care medicine, 2017.PMID 28168570
- [10]Singer P, Blaser AR, Berger MM, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clinical Nutrition, 2019.PMID 30348463
- [11]McClave SA, Taylor BE, Martindale RG, et al. (SCCM/ASPEN) Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN Journal of Parenteral and Enteral Nutrition, 2016.PMID 26773077
- [12]Zhao S, Sun Y, Wang H, et al. Efficacy of permissive underfeeding for critically ill patients: an updated systematic review and trial sequential meta-analysis. Journal of Intensive Care, 2024.PMID 38254228