ICU · Renal / acid-base
Mixed Acid–Base Disorders & the Delta–Delta — The 5-Step Approach
Also known as Mixed acid-base disorder · Delta-delta · Delta ratio · Anion gap · Winter formula · Compensation · Salicylate toxicity · DKA plus vomiting · Henderson-Hasselbalch · Strong ion difference · Stewart approach · Triple disorder
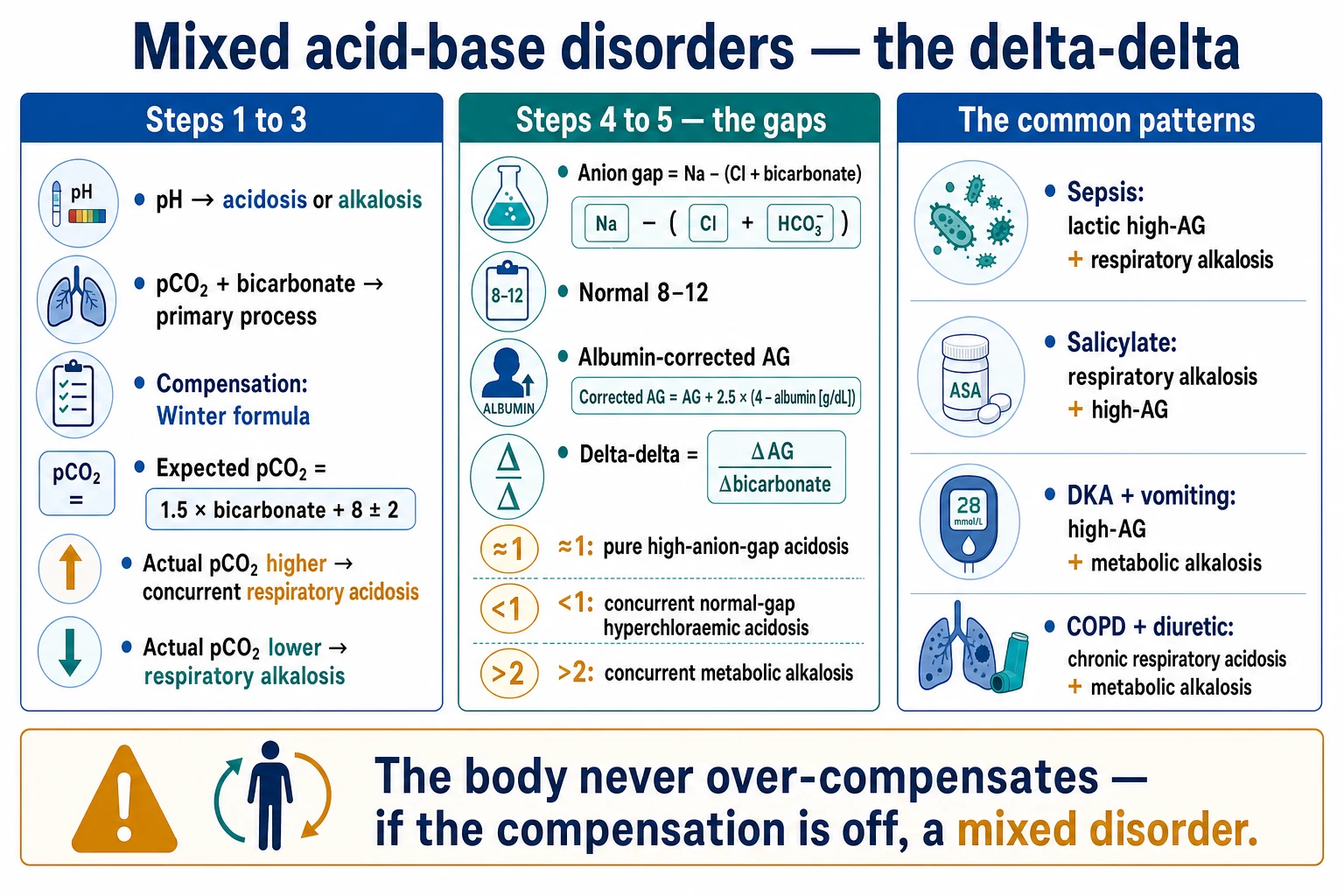
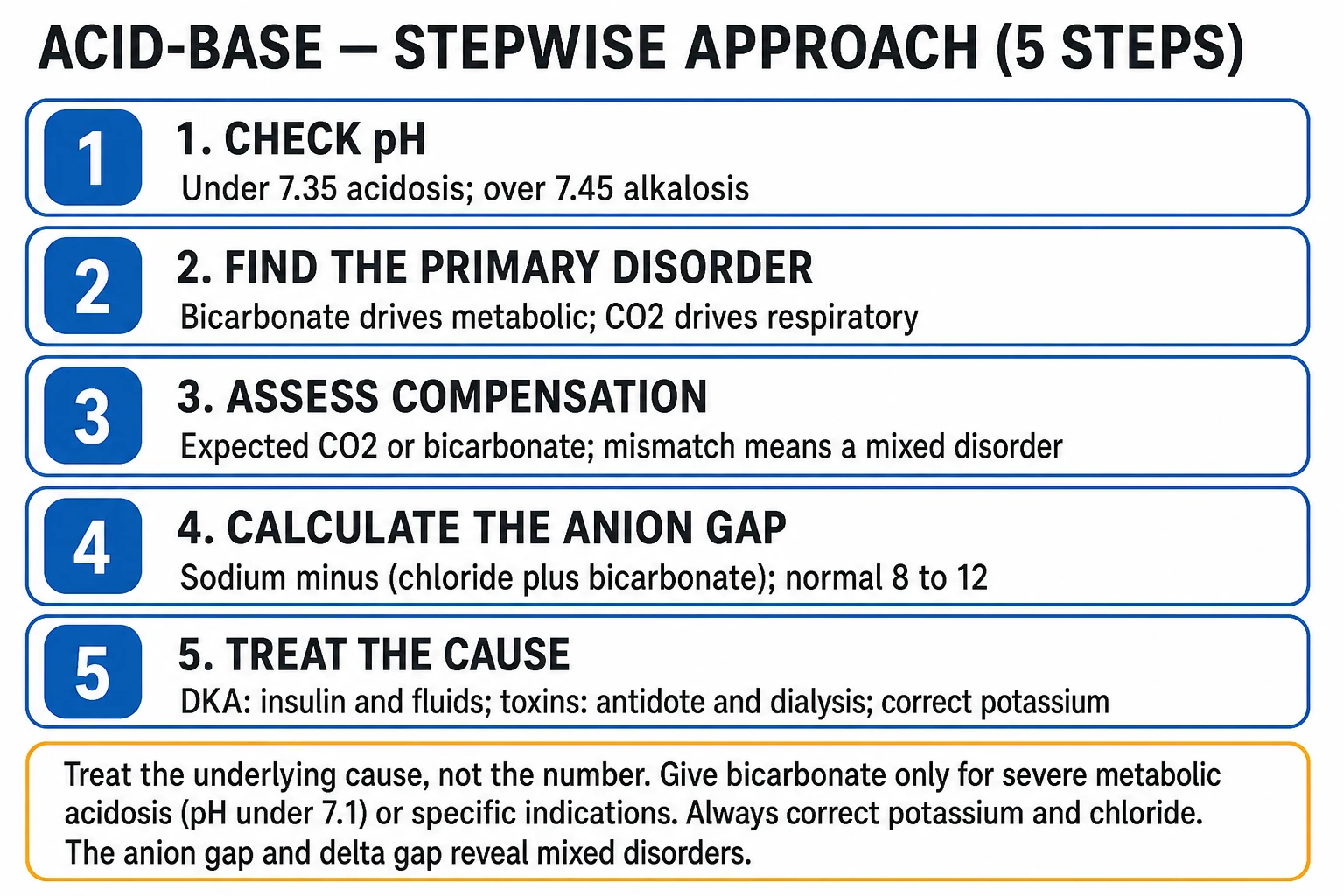
A mixed acid-base disorder is the presence of two or more primary acid-base disturbances simultaneously. The body NEVER over-compensates — if the compensation is more or less than expected, a second primary disorder is present. The systematic approach: (1) the pH to the acidosis or the alkalosis; (2) the pCO2 and the bicarbonate to the primary; (3) the expected compensation (the Winter formula for the metabolic acidosis: the expected pCO2 equals 1.5 times bicarbonate plus 8 plus-or-minus 2; the Henderson-Hasselbalch equation pH equals 6.1 plus log of bicarbonate over 0.03 times pCO2); (4) the anion gap (the Na minus (Cl plus bicarbonate), 8 to 12, the albumin-corrected — the AG rises 2.5 per 10 g/L fall in the albumin); (5) the delta-delta (the delta AG over the delta bicarbonate: about 1 the pure high-AG acidosis, under 1 the concurrent normal-gap hyperchloraemic acidosis, over 2 the concurrent metabolic alkalosis). The Stewart (strong ion difference) approach: pH is set by the PaCO2, the strong ion difference (the Na minus Cl, about 40), and the total weak acids (the albumin). The mixed metabolic acidosis (the combined high-AG and the normal-AG — the delta ratio under 1). The mixed metabolic alkalosis and acidosis (the delta ratio over 2). The triple disorders (the metabolic alkalosis plus the metabolic acidosis plus the respiratory alkalosis — the classic in the sepsis with the vomiting plus the lactic acidosis plus the hyperventilation). The salicylate toxicity (the respiratory alkalosis plus the high-AG acidosis).
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Overview & definition
A mixed acid-base disorder is the presence of two or more primary acid-base disturbances simultaneously. The single most important principle: the body never over-compensates. The physiological compensation is always in the direction of the primary disorder, and it is limited — if the measured compensation is more or less than the expected, a second primary disorder is present. The mixed disorders are common in the ICU (the sepsis, the multi-organ failure, the vomiting, the diarrhoea, the drugs) and the systematic 5-step approach uncovers them.[1]
The 5-step approach
Steps 1 and 2 — the primary disorder
- The pH — the acidosis (under 7.35) or the alkalosis (over 7.45).[1]
- The pCO2 and the bicarbonate — the respiratory (the pCO2 moves opposite to the pH) vs the metabolic (the bicarbonate moves with the pH).[1]
Step 3 — the compensation (is it appropriate?)
- The metabolic acidosis — the Winter formula: the expected pCO2 = (1.5 × HCO3) + 8 (±2). If the actual pCO2 is higher than expected → a concurrent respiratory acidosis (the under-ventilation). If the actual pCO2 is lower → a concurrent respiratory alkalosis (the over-ventilation).[1]
- The metabolic alkalosis — the expected pCO2 rises about 0.7 mmHg per 1 HCO3 (the hypoventilatory compensation, the limited by the hypoxia).[1]
- The respiratory acidosis/alkalosis — the acute: the HCO3 rises 1 per 10 pCO2 in the acidosis (the falls 2 per 10 in the alkalosis); the chronic: the HCO3 rises 4 per 10 pCO2 in the acidosis (the renal compensation over the days).[1]
Step 4 — the anion gap
- The anion gap (AG) = Na − (Cl + HCO3). The normal 8 to 12 (the albumin-corrected: the AG rises 2.5 per 10 g/L fall in the albumin).[1]
- The high AG → the unmeasured anions (the lactate, the ketones, the toxins — the methanol, the ethylene glycol, the salicylate; the renal failure).[1]
- The normal AG → the hyperchloraemic acidosis (the RTA, the diarrhoea, the saline).[1]
Step 5 — the delta-delta (ΔAG/ΔHCO3)
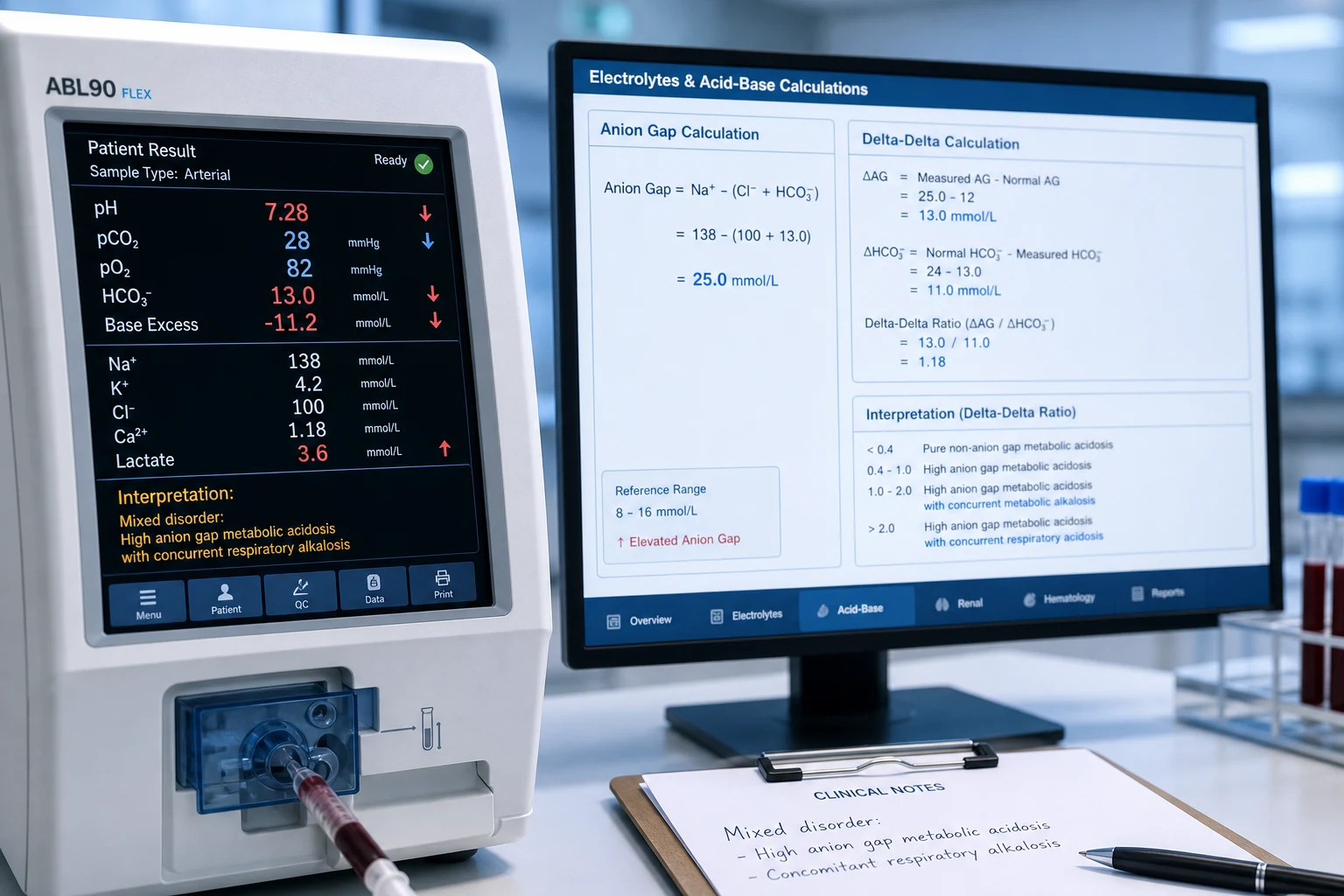
- The ΔAG = (the measured AG) − 12 (the normal). The ΔHCO3 = 24 − (the measured HCO3) (the fall).[1]
- The ratio = ΔAG / ΔHCO3:[1]
- About 1 — the pure high-AG metabolic acidosis (the AG rise matches the HCO3 fall).[1]
- Under 1 (e.g. 0.7) — the AG rise is less than the HCO3 fall → a concurrent normal-gap (hyperchloraemic) metabolic acidosis.[1]
- Over 2 (or over 1.5 to 2) — the AG rise exceeds the HCO3 fall → a concurrent metabolic alkalosis.[1]
- The equivalent: the corrected HCO3 = the measured HCO3 + ΔAG. If over 24 → a concurrent metabolic alkalosis; if under 24 → a concurrent metabolic acidosis.[1]
The Henderson–Hasselbalch equation — the chemistry under the numbers
The bicarbonate buffer system — the dominant extracellular buffer — is governed by the Henderson–Hasselbalch equation: [1]
pH = 6.1 + log₁₀( [HCO₃⁻] / (0.03 × PaCO₂) ) [1]
where 6.1 is the pKa of the carbonic acid system and 0.03 is the solubility coefficient of CO₂ in plasma (the mmol/L per mmHg).[1][8] Three clinically decisive consequences follow:
- The pH is set by the RATIO, not the absolute values. A bicarbonate of 12 with a PaCO₂ of 27 (ratio 12 / 0.81 = 14.8) gives a pH of 7.28; a bicarbonate of 24 with a PaCO₂ of 54 (the same ratio) gives the IDENTICAL pH of 7.28. The first is a metabolic acidosis with appropriate compensation; the second is a respiratory acidosis with appropriate compensation. The number you must hold in your head is the ratio of bicarbonate to (0.03 × PaCO₂).
- The denominator (PaCO₂) is the respiratory variable; the numerator (HCO₃⁻) is the metabolic variable. A primary change in either moves the pH predictably, and the body's compensatory adjustment of the OTHER variable tries to restore the ratio. This is the mathematical heart of "the body never over-compensates" — compensation always pulls the ratio back towards 20:1 (the normal ratio of HCO₃⁻ 24 to dissolved CO₂ 1.2).[8]
- The equation explains why a normal pH in a sick patient is suspicious. In the healthy state the ratio is ~20:1. If a critically ill patient has a PaCO₂ of 30 (low — respiratory alkalosis) and a HCO₃⁻ of 17 (low — metabolic acidosis), the ratio is 17 / 0.9 = 18.9 and the pH is near-normal (~7.40). A near-normal pH in a sick ICU patient almost always means TWO opposing primary disorders, not wellness.[5]
Winter's formula — derivation, application, and the limits of compensation
Winter's formula — the expected PaCO₂ = (1.5 × HCO₃⁻) + 8 (± 2) mmHg — is the bedside tool that tests whether the respiratory compensation for a metabolic acidosis is appropriate. It was derived by Albert, Dell and Winters (1967) from the observed compensatory hyperventilation in patients with a metabolic acidosis, and it is the single calculation that most often unmasks a mixed disorder.[1][1]
The four compensation rules — apply the one that matches the primary disorder
| Primary disorder | Expected compensation | Rule | If the actual is OFF → |
|---|---|---|---|
| Metabolic acidosis | ↓ PaCO₂ | Winter's: PaCO₂ = 1.5 × HCO₃ + 8 ± 2[1] | Higher → concurrent respiratory acidosis; Lower → concurrent respiratory alkalosis |
| Metabolic alkalosis | ↑ PaCO₂ | PaCO₂ rises ~0.7 mmHg per 1 mmol/L rise in HCO₃ (limited by hypoxia) | Higher → concurrent respiratory acidosis; Lower → concurrent respiratory alkalosis |
| Acute respiratory acidosis | ↑ HCO₃ | HCO₃ rises ~1 mmol/L per 10 mmHg rise in PaCO₂ | Higher HCO₃ → concurrent metabolic alkalosis; Lower → concurrent metabolic acidosis |
| Chronic respiratory acidosis (COPD) | ↑ HCO₃ | HCO₃ rises ~4 mmol/L per 10 mmHg rise in PaCO₂ (renal, over days) | Higher HCO₃ → concurrent metabolic alkalosis; Lower → concurrent metabolic acidosis |
| Acute respiratory alkalosis | ↓ HCO₃ | HCO₃ falls ~2 mmol/L per 10 mmHg fall in PaCO₂ | Higher HCO₃ → concurrent metabolic alkalosis; Lower → concurrent metabolic acidosis |
| Chronic respiratory alkalosis | ↓ HCO₃ | HCO₃ falls ~4–5 mmol/L per 10 mmHg fall in PaCO₂ (renal, over days) | Higher HCO₃ → concurrent metabolic alkalosis; Lower → concurrent metabolic acidosis |
The acute-versus-chronic distinction for the respiratory rules is critical: a COPD patient with a chronically elevated PaCO₂ of 70 has a chronically raised HCO₃ (the renal compensation). If that HCO₃ is LOWER than the chronic rule predicts, a concurrent metabolic acidosis is present (a common finding in the COPD exacerbation with a lactic acidosis or a hyperchloraemic acidosis).[2]
The Stewart (strong ion difference) approach — the physical-chemical view
The traditional Henderson–Hasselbalch approach treats the bicarbonate as the metabolic variable. The Stewart approach (Peter Stewart, 1981) re-derives the pH from three independent variables, treating bicarbonate as a dependent (derived) quantity. The two frameworks describe the same chemistry; Stewart simply makes explicit what the traditional model can only describe.[6][7]
- The PaCO₂ — the respiratory variable, identical in both frameworks.
- The strong ion difference (SID) — the difference between the fully dissociated (strong) cations and anions. In practice this is dominated by Na⁺ − Cl⁻, with a normal value of about 40 mmol/L. The strong ions cannot combine with hydrogen, so the SID acts like an electrical charge gap that water dissociation must fill: a small SID (a fall in sodium or, far more commonly, a rise in chloride — as with large-volume 0.9% saline) drives water dissociation towards more free H⁺ and an acidosis; a large SID (chloride loss from vomiting or diuretics) drives an alkalosis.[6][13]
- The total concentration of weak acids (Aₜₒₜ) — predominantly albumin and, to a lesser extent, phosphate. A fall in Aₜₒₜ (hypoalbuminaemia, ubiquitous in critical illness) is itself an alkalinising process, which is why a low albumin masks an underlying high anion-gap acidosis — the basis for the albumin correction of the AG.[7][13]
The Stewart framework earns its place at the bedside by explaining three things the traditional model can only label:[6][16]
- Why large-volume 0.9% saline causes a hyperchloraemic acidosis — it loads chloride without bicarbonate, shrinking the SID. This is the mechanism behind the SMART trial's finding that balanced crystalloids (which preserve the SID) modestly outperform saline.[19][12]
- Why hypoalbuminaemia hides a high anion-gap acidosis — it lowers Aₜₒₜ (alkalinising), offsetting the acid; the albumin-corrected AG restores the diagnostic sensitivity.[7]
- Why a metabolic alkalosis accompanies chloride depletion (vomiting, diuretics) — the chloride loss widens the SID.[13]
In Stewart's terms, the "unmeasured anions" of critical illness (lactate, ketones, toxin metabolites) are quantified as the strong ion gap (SIG) — the difference between the apparent SID (SIDa, calculated from all the measured strong ions) and the effective SID (SIDe, calculated from the buffer bases and the unmeasured anions). A normal SIG is zero; a positive SIG signals unmeasured anions, the Stewart equivalent of a high anion gap, but corrected for albumin and phosphate automatically.[7][12]
The delta-delta in depth — the delta ratio and the corrected bicarbonate
The delta-delta (also called the delta ratio, ΔAG/ΔHCO₃⁻) is the calculation that uncovers a concurrent metabolic disorder hiding inside an apparent single high-anion-gap metabolic acidosis. Wrenn (1990) introduced it as the bedside approach to the mixed metabolic disorders, and it remains the single most reliable screen for a second metabolic process.[4][1]
The principle: in a pure high-AG metabolic acidosis, every molecule of unmeasured anion (lactate, ketone) that accumulates consumes one molecule of bicarbonate — so the rise in the AG (ΔAG) should equal the fall in the HCO₃⁻ (ΔHCO₃⁻), and the ratio is about 1. Any deviation means a second metabolic disorder is pushing the bicarbonate up or down independently.[4]
The delta-delta — what each ratio means
| ΔAG / ΔHCO₃⁻ ratio | Interpretation | Concurrent disorder | Classic clinical setting |
|---|---|---|---|
| ~1 (0.8–2.0) | The AG rise matches the HCO₃⁻ fall | None — a pure high-AG metabolic acidosis | Straightforward lactic acidosis or DKA |
| < 1 (e.g. 0.7) | The HCO₃⁻ has fallen MORE than the AG has risen | Concurrent normal-gap (hyperchloraemic) metabolic acidosis | DKA resuscitated with saline; diarrhoea + lactic acidosis; renal failure |
| > 2 | The AG has risen MORE than the HCO₃⁻ has fallen | Concurrent metabolic alkalosis | DKA + vomiting; lactic acidosis + vomiting/diuretics; uraemia + vomiting |
| < 0.4 | The AG is near-normal but the HCO₃⁻ is very low | Predominant / pure normal-gap acidosis (the high-AG component is minor) | Pure hyperchloraemic acidosis from saline or RTA |
The equivalent and often simpler bedside method is the corrected (or "gap-gap") bicarbonate: [1]
Corrected HCO₃⁻ = measured HCO₃⁻ + ΔAG [1]
If the corrected HCO₃⁻ is greater than 24, a concurrent metabolic alkalosis is present (the bicarbonate has been "pushed up" by the alkalosing process). If it is less than 24, a concurrent metabolic acidosis (additional acid load) is present. The corrected bicarbonate and the delta ratio give the same answer by two routes; many clinicians find the corrected bicarbonate more intuitive at the bedside.[4][5]
Mixed metabolic acidosis — the combined high-AG and normal-AG acidosis
A mixed metabolic acidosis — a high-anion-gap acidosis AND a normal-anion-gap (hyperchloraemic) acidosis occurring together — is one of the commonest mixed disorders in the ICU, and it is the disorder most reliably missed without the delta-delta.[4]
The mixed metabolic acidosis — how the delta-delta catches it
Start with a high-AG metabolic acidosis
The patient has a high AG (e.g. 22, lactate 4) with a low HCO₃⁻ (e.g. 14). Na 140, Cl 104.
Calculate the delta-delta
ΔAG = 22 − 12 = 10. ΔHCO₃⁻ = 24 − 14 = 10. Ratio = 10/10 = 1.0 → a PURE high-AG acidosis. So far, so good.
Now resuscitate with 3 litres of 0.9% saline
Saline loads chloride (Cl rises to 112) without bicarbonate. A hyperchloraemic (normal-AG) acidosis is superimposed. The HCO₃⁻ falls further (to 11) but the AG barely moves (lactate clearing: AG now 16).
Re-check the delta-delta
ΔAG = 16 − 12 = 4. ΔHCO₃⁻ = 24 − 11 = 13. Ratio = 4/13 = 0.3 → a CONCURRENT normal-gap acidosis. The chloride (112) and the falling HCO₃⁻ against a near-normal AG confirm the hyperchloraemic component.
The corrected HCO₃⁻ confirms
Corrected HCO₃⁻ = 11 + 4 = 15 (well under 24) → a concurrent metabolic acidosis. The two methods agree.
The clinical lesson
The delta-delta under 1 (or the corrected HCO₃⁻ under 24) signals the saline-induced hyperchloraemic component. Switch to a balanced crystalloid (Plasma-Lyte, Hartmann) — SMART shows measurable renal and outcome benefit over saline.<Cite id="19" />
The classic settings for a mixed metabolic acidosis are: DKA during recovery (the resolving ketoacidosis + the saline-induced hyperchloraemia from aggressive resuscitation — the AG normalises but the acidosis persists, exactly because the chloride has replaced the ketones); diarrhoea with a lactic acidosis (sepsis, mesenteric ischaemia); renal failure with a superimposed lactic acidosis; and any patient resuscitated with large volumes of 0.9% saline who was already acidaemic.[4][12]
Mixed metabolic alkalosis + metabolic acidosis — the delta ratio over 2
A concurrent metabolic alkalosis and metabolic acidosis is the mirror-image mixed metabolic disorder. The clinical clue is a high-anion-gap metabolic acidosis whose bicarbonate is higher than the AG rise would predict — the alkalosing process (vomiting, diuretics, nasogastric suction) has "rescued" the bicarbonate partially.[4][5]
The DKA-plus-vomiting — the classic metabolic alkalosis + acidosis
The presentation
A young type-1 diabetic with several days of vomiting and polyuria. The vomiting causes a metabolic alkalosis (loss of HCl and volume); the insulin deficiency causes DKA (a high-AG metabolic acidosis from ketoacids). Both are primary.
The blood gas
pH 7.20, HCO₃⁻ 13, PaCO₂ 30. Na 138, Cl 90, K 3.0.
Step 4 — the anion gap
AG = 138 − (90 + 13) = 35 (high-AG acidosis). The delta-delta: ΔAG = 35 − 12 = 23; ΔHCO₃⁻ = 24 − 13 = 11. Ratio = 23/11 = 2.1 → OVER 2.
The corrected HCO₃⁻ confirms
Corrected HCO₃⁻ = 13 + 23 = 36 (well over 24) → a concurrent metabolic alkalosis. The low chloride (90) and low potassium (3.0) point to the vomiting.
Why the pH is "better than expected"
Without the vomiting, the HCO₃⁻ would be much lower (around 11) and the pH correspondingly lower. The alkalosing process partially offsets the acid — the pH 7.20 is "less acidic" than a pure DKA at this AG would produce.
Management implication
Treat the DKA (insulin, fluids) but DO NOT over-correct the potassium — the metabolic alkalosis of vomiting and the impending insulin-driven intracellular K shift conspire to drop the K dangerously. Replete K early. The metabolic alkalosis resolves as the volume is restored and the chloride repleted.
The corrected bicarbonate and the delta ratio over 2 are the two routes to the same diagnosis. The low chloride and the hypokalaemia are the biochemical signatures of the vomiting (or diuretic) alkalosis layered on top of the high-AG acidosis.[2][3]
Triple disorders — the three-way mixed disturbance
A triple disorder is the simultaneous presence of three primary acid-base disturbances. The classic and most examinable is the metabolic alkalosis + metabolic acidosis + respiratory alkalosis — the textbook scenario being the septic patient with vomiting, a lactic acidosis, and hyperventilation.[1]
The classic triple disorder — sepsis + vomiting + lactic acidosis + hyperventilation
The scenario
A 60-year-old with pyelonephritis and septic shock, 2 days of vomiting, now tachypnoeic. Three primary disorders are coexisting.
Disorder 1 — the high-AG metabolic acidosis
The lactic acidosis of septic shock (the lactate 5). A primary metabolic acidosis: the HCO₃⁻ falls.
Disorder 2 — the metabolic alkalosis
The vomiting (the loss of HCl and volume, the chloride depletion). A primary metabolic alkalosis: the HCO₃⁻ rises independently.
Disorder 3 — the respiratory alkalosis
The hyperventilation (septic encephalopathy, fever, the early direct medullary stimulation, hepatic failure). A primary respiratory alkalosis: the PaCO₂ falls.
The blood gas may look deceptively simple
pH 7.39, HCO₃⁻ 16, PaCO₂ 27. The pH is near-normal — three opposing processes nearly cancelling. Na 138, Cl 92.
Step 3 — Winter reveals the respiratory component
Expected PaCO₂ = 1.5 × 16 + 8 = 32 ± 2. The actual PaCO₂ (27) is LOWER than expected → a concurrent respiratory ALKALOSIS.
Step 4 — the anion gap
AG = 138 − (92 + 16) = 30 (high-AG acidosis).
Step 5 — the delta-delta reveals the metabolic alkalosis
ΔAG = 30 − 12 = 18; ΔHCO₃⁻ = 24 − 16 = 8. Ratio = 18/8 = 2.25 → OVER 2 → a concurrent metabolic ALKALOSIS. Corrected HCO₃⁻ = 16 + 18 = 34 (well over 24) — confirms.
The synthesis
Three primary disorders: a high-AG metabolic acidosis (lactate) + a metabolic alkalosis (vomiting) + a respiratory alkalosis (hyperventilation). Each was found by a single calculation — Winter (the respiratory), the delta-delta (the metabolic alkalosis).
The triple disorder is the acid-base diagnosis that most rewards the systematic 5-step approach. A single number (the near-normal pH) conceals three processes; only by working through pH → primary → compensation → anion gap → delta-delta do all three emerge. The salicylate-intoxicated patient who then vomits is another triple-disorder classic (the respiratory alkalosis + the high-AG acidosis of salicylate + the metabolic alkalosis of vomiting).[1][5]
The common ICU mixed patterns
- The high-AG acidosis + the respiratory alkalosis: the sepsis (the lactic acidosis + the hyperventilation), the salicylate toxicity (the early respiratory alkalosis — the direct medullary stimulation + the high-AG acidosis — the salicylate), the hepatorenal syndrome, the severe liver disease.[1]
- The high-AG acidosis + the metabolic alkalosis: the vomiting (the metabolic alkalosis) + the lactic acidosis or the DKA (the "DKA plus the vomiting"). The delta-delta over 2.[1]
- The high-AG + the normal-gap (hyperchloraemic) acidosis: the DKA recovery (the resolving ketoacidosis + the saline-induced hyperchloraemia), the diarrhoea + the lactic acidosis, the renal failure.[1]
- The mixed respiratory + the metabolic: the COPD (the chronic respiratory acidosis) + the metabolic alkalosis (the diuretic); the cardiac arrest (the respiratory + the metabolic acidosis); the respiratory failure + the sepsis.[1]
- The triple disorder: the sepsis + the vomiting + the lactic acidosis + the hyperventilation (the metabolic acidosis + the metabolic alkalosis + the respiratory alkalosis); the salicylate + the vomiting (the respiratory alkalosis + the high-AG acidosis + the metabolic alkalosis).[1]
Worked examples — the 5-step approach applied
Worked example 1 — the septic patient with a near-normal pH (a mixed disorder in disguise)
The gas and the electrolytes
pH 7.38, PaCO₂ 30, HCO₃⁻ 17. Na 140, Cl 105, albumin 30 g/L. Lactate 4.5.
Step 1–2 — the pH and the primary
pH 7.38 is just within normal. The PaCO₂ is low and the HCO₃⁻ is low. Both move in the direction of an acidosis for the HCO₃⁻ and an alkalosis for the PaCO₂ — a near-normal pH from two opposing processes.
Step 3 — the compensation
If the primary is a metabolic acidosis, expected PaCO₂ = 1.5 × 17 + 8 = 33.5 ± 2. The actual (30) is LOWER → a concurrent respiratory ALKALOSIS.
Step 4 — the albumin-corrected anion gap
AG = 140 − (105 + 17) = 18. Corrected for albumin: the albumin is 30 (10 below 40), so add 2.5 → corrected AG ~20.5 (high-AG acidosis). The lactate (4.5) accounts for most of the ΔAG.
Step 5 — the delta-delta
ΔAG = 20 − 12 = 8; ΔHCO₃⁻ = 24 − 17 = 7. Ratio = 8/7 = 1.14 → about 1, a pure high-AG acidosis (no concurrent metabolic disorder).
The diagnosis
A high-AG metabolic acidosis (lactic, from sepsis) + a respiratory alkalosis (hyperventilation). Two primary disorders — the classic septic pattern.
Worked example 2 — DKA that will not clear (the saline-induced hyperchloraemic component)
The setting
12 hours into DKA treatment. The ketones have cleared, the glucose is normalising, but the HCO₃⁻ is still low and the patient was resuscitated with 4 litres of 0.9% saline.
The gas and the electrolytes
pH 7.30, PaCO₂ 28, HCO₃⁻ 14. Na 140, Cl 110, albumin 35.
Step 3 — Winter
Expected PaCO₂ = 1.5 × 14 + 8 = 29 ± 2. Actual 28 → within range. The compensation is appropriate (no concurrent respiratory disorder).
Step 4 — the anion gap
AG = 140 − (110 + 14) = 16 (corrected ~17.5). The AG is only mildly raised — the ketoacidosis has largely resolved.
Step 5 — the delta-delta
ΔAG = 17 − 12 = 5; ΔHCO₃⁻ = 24 − 14 = 10. Ratio = 5/10 = 0.5 → UNDER 1 → a concurrent normal-gap (hyperchloraemic) acidosis. Corrected HCO₃⁻ = 14 + 5 = 19 (under 24) — confirms.
The diagnosis and the lesson
The persistent acidosis is now a hyperchloraemic (normal-AG) acidosis from the saline, NOT ongoing ketoacidosis. The high chloride (110) is the give-away. Stop the saline, switch to a balanced crystalloid, and the HCO₃⁻ will normalise — no bicarbonate, no more insulin beyond maintenance.
The strong ion difference in practice — when Stewart changes management
The Stewart variables — what each does to the pH
| Variable | Normal value | A change towards acidosis | A change towards alkalosis | Clinical correlate |
|---|---|---|---|---|
| PaCO₂ | 40 mmHg | ↑ (hypoventilation) | ↓ (hyperventilation) | The respiratory variable — common to both frameworks |
| Strong ion difference (SID) | ~40 mmol/L (Na⁺ − Cl⁻) | ↓ — chloride rises (saline) or sodium falls | ↑ — chloride falls (vomiting, diuretics) | The dominant metabolic variable in Stewart's terms; explains saline acidosis and vomiting alkalosis |
| Total weak acids (Aₜₒₜ) | albumin ~40 g/L | ↑ (hyperalbuminaemia — rare) or hyperphosphataemia | ↓ — hypoalbuminaemia (very common in ICU) | Hypoalbuminaemia is alkalinising and MASKS a high-AG acidosis; this is why the albumin correction of the AG matters |
| Unmeasured anions (SIG) | ~0 (zero) | ↑ — lactate, ketones, toxins, uraemia | — | The Stewart equivalent of the high anion gap; a positive SIG is the acid load |
The practical use of the Stewart framework at the bedside is not to replace the traditional approach but to explain the cases that the traditional model labels but cannot account for: the hyperchloraemic acidosis of saline (a low SID, not a "bicarbonate loss"), the alkalosis of hypoalbuminaemia (a low Aₜₒₜ), and the unmeasured anions quantified as the SIG rather than the cruder AG.[6][7][16]
The albumin correction of the anion gap — the hidden acid load
The albumin correction is essential in the ICU because hypoalbuminaemia is near-universal in critical illness, and an uncorrected anion gap will MISS a high-AG acidosis in the hypoalbuminaemic patient. The rule: the AG falls by approximately 2.5 mmol/L for every 10 g/L fall in the albumin below 40 g/L.[1][7]
- Corrected AG = measured AG + 2.5 × ( (40 − albumin g/L) / 10 )
- A patient with a measured AG of 14 (apparently normal) and an albumin of 20 g/L has a corrected AG of 14 + 2.5 × 2 = 19 — a high-AG acidosis that the uncorrected gap completely conceals. [1]
This is the single most common reason a high-AG acidosis is missed at the bedside. Always correct the AG for albumin in the ICU patient.[7][20]
Short-answer questions
SAQ — Systematic ABG interpretation in the septic, vomiting patient
10 minutes · 10 marks
A 64-year-old woman is admitted to the ICU with pyelonephritis and septic shock. She has vomited for 48 hours and is tachypnoeic (RR 32). Arterial blood gas on 6 L/min nasal specs: pH 7.39, PaCO₂ 27 mmHg, HCO₃⁻ 16 mmol/L, PaO₂ 94 mmHg. Sodium 138, chloride 92, potassium 3.1, albumin 28 g/L, lactate 5.2 mmol/L. Interpret this blood gas systematically and outline the immediate management.
SAQ — Compensation limits and the body that never over-compensates
10 minutes · 10 marks
A 72-year-old man with severe COPD (baseline PaCO₂ 68 mmHg, HCO₃⁻ 36 mmol/L at last clinic visit) is admitted with a COPD exacerbation and recent frusemide 80 mg daily for cor pulmonale. Arterial blood gas: pH 7.38, PaCO₂ 60 mmHg, HCO₃⁻ 35 mmol/L. Sodium 140, chloride 88, potassium 2.9. Assess the appropriateness of the compensation and explain the principle that governs it.
Clinical pearls
The metabolic alkaloses — chloride-responsive and resistant
A mixed disorder involving a metabolic alkalosis requires the alkalosis itself to be characterised, because the management differs. The first question is whether the alkalosis is chloride-responsive (the urine chloride under 10–20 mmol/L — vomiting, nasogastric suction, diuretics, post-hypercapnia) or chloride-resistant (the urine chloride over 20 — mineralocorticoid excess, severe hypokalaemia).[2][3]
The metabolic alkalosis — chloride-responsive vs resistant
| Feature | Chloride-RESPONSIVE (urine Cl⁻ < 20) | Chloride-RESISTANT (urine Cl⁻ > 20) |
|---|---|---|
| Mechanism | Volume and chloride depletion → the kidney retains bicarbonate | Mineralocorticoid excess or severe K⁺ depletion → bicarbonate generation |
| Common causes | Vomiting, NG suction, diuretics, post-hypercapnia, villous adenoma | Primary hyperaldosteronism, Cushing's, exogenous mineralocorticoids, severe hypokalaemia, Bartter/Gitelman |
| Urine chloride | < 10–20 mmol/L (low) | > 20 mmol/L (high) |
| Blood pressure | Usually normal or low | Usually HIGH (mineralocorticoid) — except Bartter/Gitelman |
| Treatment | Normal saline + KCl repletion (restores volume and chloride) | Treat the cause (spironolactone, remove the adenoma); K⁺ repletion |
| Relevance to the mixed disorder | The common metabolic alkalosis in the ICU mixed picture (vomiting, diuretics) | Rare but consider in the hypertensive ICU patient with an alkalosis |
In the mixed-disorder context, the chloride-responsive alkalosis (vomiting, diuretics) is by far the commonest, and it is the one that elevates the delta-delta above 2 and the corrected HCO₃⁻ above 24. The treatment is chloride and potassium repletion — which also helps resolve the delta-delta towards 1.[2]
Trials and evidence
Albert, Dell & Winters — the origin of Winter's formula (PMID 6016545)
Source
Annals of Internal Medicine, 1967 — the foundational observational study from which Winter's formula is derived
Question
What is the quantitative relationship between the serum bicarbonate and the compensatory PaCO₂ in a metabolic acidosis?
Method
Analysis of patients with metabolic acidosis of varying severity, plotting the observed PaCO₂ against the serum total CO₂ (bicarbonate) content
Key result
The compensatory PaCO₂ fell predictably with the bicarbonate, fitting the regression PaCO₂ = 1.5 × HCO₃⁻ + 8 (± 2). This is the equation every intensivist still uses at the bedside
Enduring legacy
Over 50 years later, Winter's formula remains the standard test of compensation for a metabolic acidosis — the calculation that most often unmasks a concurrent respiratory disorder
Wrenn K — The delta gap: an approach to mixed acid-base disorders (PMID 2240729)
Source
Annals of Emergency Medicine, 1990 — the bedside method that brought the delta-delta into routine clinical use
Concept
In a high-AG metabolic acidosis, the rise in the AG (ΔAG) should match the fall in the bicarbonate (ΔHCO₃⁻). A mismatch reveals a concurrent metabolic disorder
The method
Compare the ΔAG to the ΔHCO₃⁻. A ratio of ~1 = a pure high-AG acidosis; under 1 = a concurrent normal-gap acidosis; over 2 = a concurrent metabolic alkalosis
Clinical impact
Gave clinicians a single calculation that exposes the concurrent metabolic disorder hiding inside an apparent single high-AG acidosis — the cornerstone of the mixed-metabolic-disorder diagnosis
Jaber et al — BICAR-ICU: sodium bicarbonate in severe metabolic acidaemia (PMID 29910040)
Design
Multicentre, open-label, randomised controlled trial — 389 critically ill adults with severe metabolic acidaemia (pH ≤ 7.20, HCO₃⁻ ≤ 20)
Intervention
Sodium bicarbonate 4.2% infusion to maintain pH above 7.30 vs no bicarbonate (standard care)
Primary outcome
Composite of death by day 28 or at least one organ failure at day 7 — NO significant difference in the primary intention-to-treat population
Subgroup signal
In the AKIN stage 2–3 (acute kidney injury) subgroup, bicarbonate REDUCED the primary composite outcome AND the need for renal replacement therapy. This is the modern evidence base for selective bicarbonate use
Bottom line
Bicarbonate is not routinely indicated for severe metabolic acidaemia, but may be considered in the patient with significant acute kidney injury. Treat the cause; do not reflexively give bicarbonate for the number
Semler et al — SMART: balanced crystalloids vs saline in critically ill adults (PMID 29768150)
Design
Pragmatic, cluster-crossover, single-centre randomised trial — 15,802 critically ill adults across 5 ICUs at Vanderbilt
Intervention
Balanced crystalloids (lactated Ringer's or Plasma-Lyte) vs 0.9% saline for all intravenous fluid
Primary outcome
Composite of death, new renal replacement therapy, or persistent renal dysfunction at 30 days
Key result
Balanced crystalloids modestly but significantly REDUCED the composite outcome (14.3% vs 15.4%, p = 0.04). The benefit is attributable to the avoidance of the saline-induced hyperchloraemic (low-SID) acidosis
Acid-base relevance
The trial is the clinical validation of Stewart's prediction: saline lowers the strong ion difference and causes acidosis and renal harm; balanced crystalloids preserve the SID. Prefer balanced crystalloids for resuscitation
Moviat et al — Conventional vs physicochemical (Stewart) approach in ICU metabolic acidosis (PMID 12793889)
Source
Critical Care, 2003 — a head-to-head comparison of the traditional and Stewart approaches in the ICU
Question
Does the Stewart (strong ion difference) method detect mixed disorders the traditional approach misses?
Finding
The Stewart approach detected additional disorders (particularly the hypoalbuminaemia-induced alkalosis and the saline-induced acidosis) that the traditional method under-appreciated. The two methods largely concurred for the high-AG component
Lesson
The Stewart framework adds sensitivity for the SID-driven (saline, chloride) and Aₜₒₜ-driven (albumin) disorders; it complements rather than replaces the traditional approach
Schlichtig, Grogono & Severinghaus — PaCO₂ and standard base excess compensation (PMID 9671365)
Source
Critical Care Medicine, 1998 — the definitive compilation of human acid-base compensation limits
Concept
Defined the EXPECTED compensation for each primary disorder in terms of the standard base excess (SBE), and the limits beyond which a mixed disorder must be present
Key contribution
Established that compensation is predictable and bounded — the basis for the rules (Winter, the acute/chronic respiratory) used at the bedside. When the measured value lies outside the predicted band, a second primary disorder is certain
Rastegar A — Clinical utility of Stewart's method (PMID 19520748)
Source
Clinical Journal of the American Society of Nephrology, 2009 — the accessible review that brought Stewart into mainstream nephrology and critical care teaching
Core teaching
Re-derives the pH from the three independent variables (PaCO₂, SID, Aₜₒₜ) and demonstrates that the traditional and Stewart approaches agree when all variables are accounted for — but Stewart makes the saline acidosis, the albumin effect, and the chloride-depletion alkalosis mechanistically explicit
Bedside relevance
The review clinicians cite when justifying the albumin correction of the AG and the preference for balanced crystalloids over saline
Adrogué & Madias — Management of life-threatening acid-base disorders (PMID 9414329, 9420343)
Source
New England Journal of Medicine, 1998 (two parts) — the authoritative clinical review of acid-base management
Part 1 (9414329)
Covers the metabolic acidoses — the high-AG and normal-AG, the diagnosis by the anion gap and the delta-delta, and the management (treat the cause, dialysis, the role of bicarbonate)
Part 2 (9420343)
Covers the metabolic alkaloses (chloride-responsive and resistant), the respiratory acidoses and alkaloses, and the mixed disorders — with the compensation rules and the delta-delta method
Enduring status
Still the most-cited single reference for the systematic approach to acid-base disorders; the framework the examiners expect you to reproduce
Red flags
References
- [1]Albert MS, Dell RB, Winters RW Quantitative displacement of acid-base equilibrium in metabolic acidosis Ann Intern Med, 1967.PMID 6016545
- [2]Adrogue HJ, Madias NE Management of life-threatening acid-base disorders. First of two parts N Engl J Med, 1998.PMID 9414329
- [3]Adrogue HJ, Madias NE Management of life-threatening acid-base disorders. Second of two parts N Engl J Med, 1998.PMID 9420343
- [4]Wrenn K The delta (delta) gap: an approach to mixed acid-base disorders Ann Emerg Med, 1990.PMID 2240729
- [5]Haber RJ A practical approach to acid-base disorders West J Med, 1991.PMID 1843849
- [6]Emmett M Stewart Versus Traditional Approach to Acid-Base Disorders Anesth Analg, 2016.PMID 27636585
- [7]Rastegar A Clinical utility of Stewart's method in diagnosis and management of acid-base disorders Clin J Am Soc Nephrol, 2009.PMID 19520748
- [8]Kraut JA, Madias NE Approach to patients with acid-base disorders Respir Care, 2001.PMID 11262558
- [9]Kraut JA, Madias NE Treatment of acute metabolic acidosis: a pathophysiologic approach Nat Rev Nephrol, 2012.PMID 22945490
- [10]Gomez H, Kellum JA Understanding Acid Base Disorders Crit Care Clin, 2015.PMID 26410149
- [11]Berend K Diagnostic Use of Base Excess in Acid-Base Disorders N Engl J Med, 2018.PMID 30067929
- [12]Moviat M, van Haren F, van der Hoeven H Conventional or physicochemical approach in intensive care unit patients with metabolic acidosis Crit Care, 2003.PMID 12793889
- [13]Story DA, Kellum JA New aspects of acid-base balance in intensive care Curr Opin Anaesthesiol, 2004.PMID 17021538
- [14]Schlichtig R, Grogono AW, Severinghaus JW Human PaCO2 and standard base excess compensation for acid-base imbalance Crit Care Med, 1998.PMID 9671365
- [15]Moviat M, Terpstra AM, Ruitenbeek W, Kluijtmans LA, Pickkers P, van der Hoeven HG Contribution of various metabolites to the unmeasured anions in critically ill patients with metabolic acidosis Crit Care Med, 2008.PMID 18176310
- [16]Story DA Acid-Base Analysis in the Operating Room: A Bedside Stewart Approach Anesthesiology, 2023.PMID 37934110
- [17]Al-Jaghbeer M, Kellum JA Acid-base disturbances in intensive care patients: etiology, pathophysiology and treatment Nephrol Dial Transplant, 2015.PMID 25213433
- [18]Jaber S, Paugam C, Futier E, et al Sodium bicarbonate therapy for patients with severe metabolic acidaemia in the intensive care unit (BICAR-ICU): a multicentre, open-label, randomised controlled, phase 3 trial Lancet, 2018.PMID 29910040
- [19]Semler MW, Self WH, Wanderer JP, et al Balanced Crystalloids versus Saline in Critically Ill Adults N Engl J Med, 2018.PMID 29768150
- [20]Berend K, Duits AJ The role of the clinical laboratory in diagnosing acid-base disorders Crit Rev Clin Lab Sci, 2019.PMID 30917291