ICU · Renal / RRT
Renal Replacement Therapy Modalities — IHD vs CVVH vs CVVHDF vs SLED
Also known as Renal replacement therapy · RRT · Haemodialysis · IHD · Continuous renal replacement therapy · CRRT · CVVH · CVVHDF · SLED · Diffusion · Convection · Ultrafiltration · Citrate anticoagulation · AEIOU
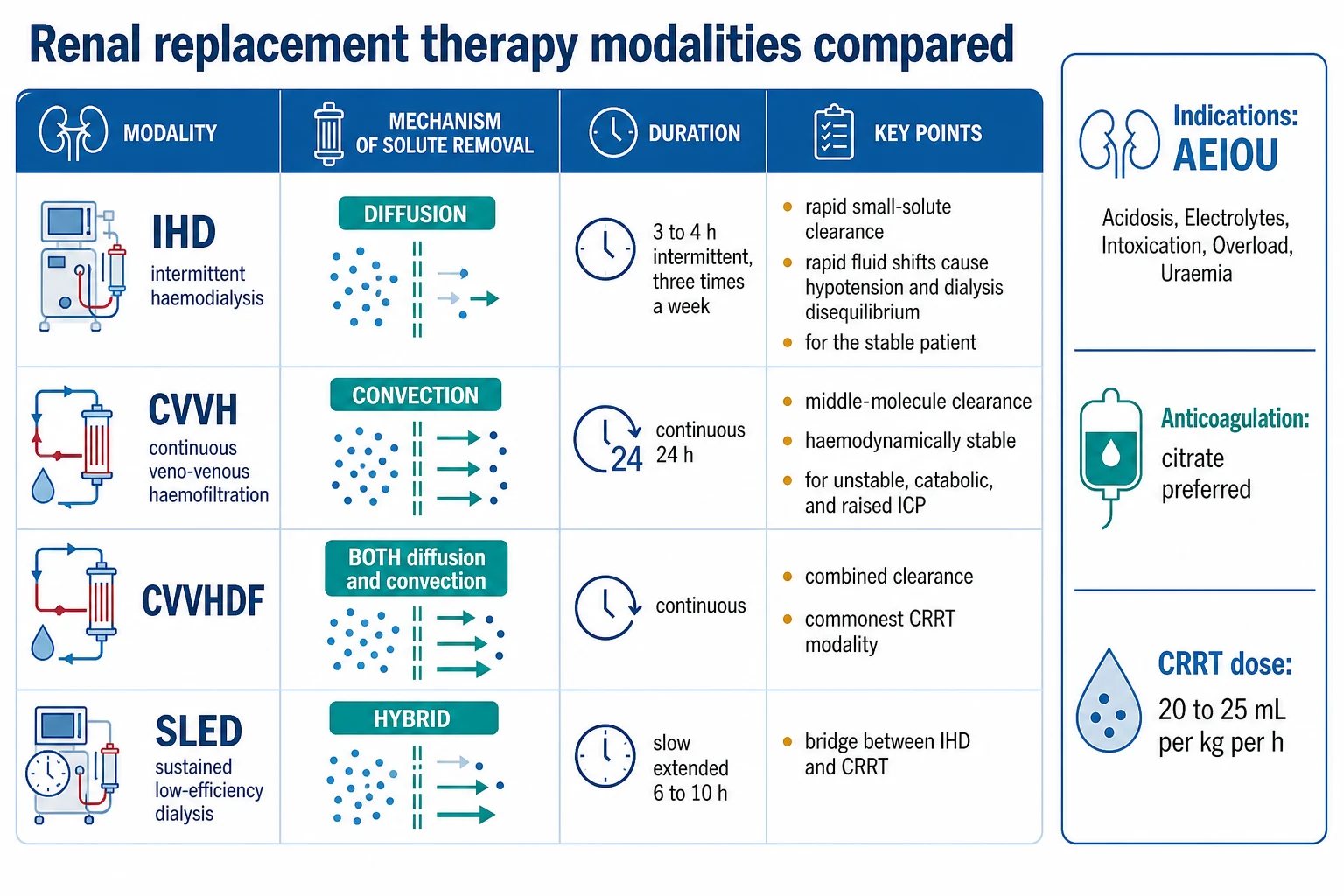
The renal replacement therapy (RRT) removes the solutes and the fluid when the kidneys fail. The four modalities — the intermittent haemodialysis (IHD), the continuous veno-venous haemofiltration (CVVH), the continuous veno-venous haemodiafiltration (CVVHDF), and the sustained low-efficiency dialysis (SLED) — differ in the solute-transport mechanism (the diffusion vs the convection), the duration and the intermittency, and the haemodynamic tolerance. The IHD is diffusion-based, intermittent, rapid, and for the stable patient (the rapid solute and fluid shifts cause the hypotension and the dialysis disequilibrium). The CVVH is convection-based, continuous, gentle, and for the haemodynamically unstable and the catabolic patient (the middle-molecule clearance). The CVVHDF combines both and is the commonest CRRT modality. The SLED is the hybrid bridge. The indications follow the AEIOU (the Acidosis, the Electrolytes, the Intoxication, the Overload, the Uraemia). The anticoagulation is the regional citrate (preferred) or the heparin. The CRRT dose is 20 to 25 mL/kg/h (the ATN and the RENAL trials — the higher dose offered no benefit). The early vs the late RRT (the AKIKI, the STARRT-AKIN, the ELAIN) — no clear benefit of the early in the moderate AKI.
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Overview & definition
The renal replacement therapy (RRT) removes the solutes (the urea, the creatinine, the potassium, the toxins) and the fluid (the ultrafiltration) when the kidneys fail. The four modalities differ in the solute-transport mechanism (the diffusion vs the convection), the duration and the intermittency, and the haemodynamic tolerance. The choice depends on the haemodynamic stability, the solute-removal goal, the fluid-balance need, and the bleeding risk.[1]

The solute-transport mechanisms
- The diffusion — the solute moves down its concentration gradient across the semipermeable membrane (the dialysate flows counter-current to the blood). Efficient for the small solutes (the urea, the creatinine, the potassium). The basis of the haemodialysis (the IHD).[1]
- The convection — the solute is dragged with the water across the membrane (the solvent drag) by the hydrostatic pressure; the bulk flow removes the small AND the middle molecules. The basis of the haemofiltration (the CVVH).[1]
- The ultrafiltration — the fluid (water) removal by the hydrostatic pressure (the plasma water dragged across the membrane). The fluid-balance control.[1]
The modalities
Intermittent haemodialysis (IHD)
- The diffusion-based, the intermittent, the 3 to 4 hours a session, three times a week (or daily in the AKI). The high blood and the dialysate flows.[1]
- The rapid solute clearance — the efficient small-solute removal.[1]
- The rapid fluid and solute shifts — the hypotension (the risk for the haemodynamically unstable), the dialysis disequilibrium (the rapid solute shifts → the cerebral oedema, the risk in the uraemia and the raised ICP).[1]
- For the stable patient (the stable AKI, the CKD, the end-stage).[1]
Continuous veno-venous haemofiltration (CVVH)
- The convection-based, the continuous (the 24 hours), the pumped veno-venous access (a dual-lumen central catheter).[1]
- The middle-molecule clearance (the larger solutes, the inflammatory mediators).[1]
- The gentle, the haemodynamically tolerated — the slow, the continuous fluid removal avoids the rapid shifts. The good for the haemodynamically unstable, the catabolic, and the raised ICP.[1]
- Needs the anticoagulation (the regional citrate or the heparin).[1]
Continuous veno-venous haemodiafiltration (CVVHDF)
- The combined diffusion and convection — the dialysate (the diffusion) plus the replacement fluid (the convection).[1]
- The combined clearance — better than the CVVH alone. The commonest CRRT modality.[1]
- The continuous, the gentle, the haemodynamically tolerated.[1]
Sustained low-efficiency dialysis (SLED)
- The hybrid — a slow, the extended (the 6 to 10 hours) intermittent haemodialysis, the daily.[1]
- A bridge between the IHD and the CRRT — the better haemodynamic tolerance than the IHD, the less anticoagulation than the CRRT.[1]
- Useful when the CRRT is unavailable or for the transitional phase.[1]
The indications — the AEIOU
The RRT is indicated for:[1]
- A — the acidosis refractory to the bicarbonate.[1]
- E — the electrolyte disorders refractory to the medical therapy (the severe or the refractory hyperkalaemia).[1]
- I — the intoxications with the dialysable toxins (the lithium, the salicylate, the metformin, the methanol, the ethylene glycol).[1]
- O — the overload — the refractory fluid overload (the pulmonary oedema).[1]
- U — the uraemia — the complications (the uraemic pericarditis, the uraemic encephalopathy, the uraemic bleeding).[1]
Plus the oliguria with the inability to meet the fluid and the nutritional needs.[1]
The timing — the early vs the late
The AKIKI, the STARRT-AKIN, and the ELAIN trials addressed the early vs the late RRT in the moderate-to-severe AKI. The consensus: no clear benefit of the early RRT in the moderate AKI without the absolute indication — the standard is to wait for the absolute indication (the refractory K, the acidosis, the overload, the uraemia) unless the uraemic complications or the fluid overload develop. The early RRT increases the exposure to the dialysis (the catheter, the anticoagulation) without the outcome benefit. The ELAIN trial suggested a benefit of the earlier (the furosemide-staged) RRT, but this is controversial and not the standard.[1]
The anticoagulation
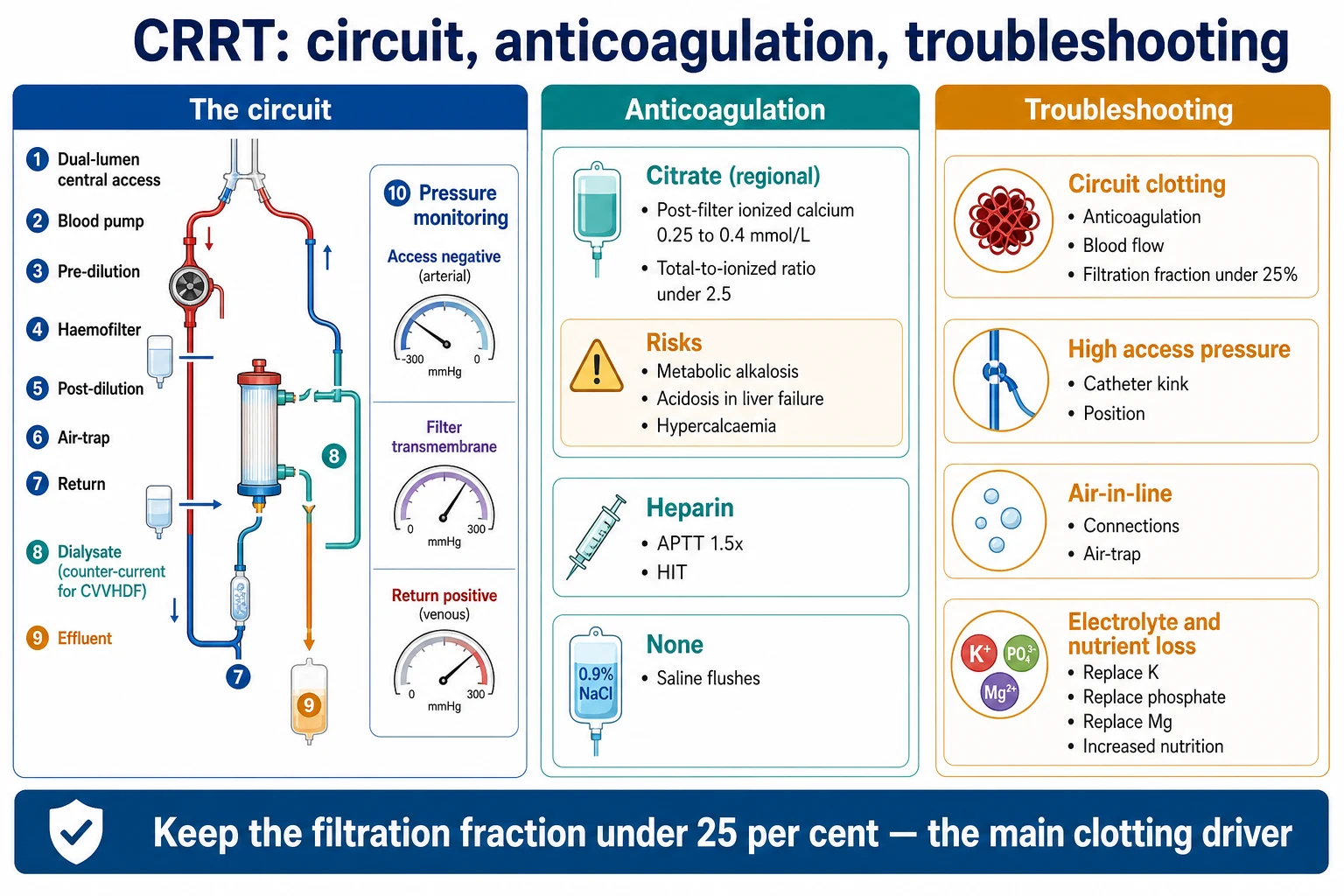
- The regional citrate — the preferred. The citrate chelates the calcium in the circuit (the local anticoagulation) and is metabolized in the liver (the systemic anticoagulation avoided). The monitoring: the post-filter ionized calcium (low), the systemic ionized calcium (normal), the total calcium rising. The risks: the metabolic alkalosis (the citrate metabolized to the bicarbonate), the hypercalcaemia, and the citrate accumulation (the total-to-ionized calcium ratio over 2.5) in the severe liver failure.[1]
- The unfractionated heparin — the effective, the cheap; the bleeding risk and the heparin-induced thrombocytopenia (the HIT).[1]
- The low-molecular-weight heparin, the prostacyclin.[1]
- The no anticoagulation — for the high-bleeding-risk patient; the saline flushes; the shorter circuit life.[1]
The dose
The CRRT dose (the effluent rate) is the 20 to 25 mL/kg/h. The ATN and the RENAL trials showed that the higher dose (the 35 mL/kg/h) offered no benefit over the 20 to 25 mL/kg/h. The delivered dose is less than the prescribed (the downtime for the filter change, the investigations, the clotting).[1]
[1]SAQ — Choosing the RRT modality and dose in vasopressor-dependent septic AKI
10 minutes · 10 marks
A 62-year-old man with septic shock from a perforated viscus is on noradrenaline 0.4 µg/kg/min and vasopressin 0.03 U/min, intubated for type 1 respiratory failure. He develops oliguric KDIGO stage 3 acute kidney injury (creatinine 390 µmol/L, K⁺ 6.7 mmol/L with peaked T waves, pH 7.18, lactate 3.2). The team asks whether to start intermittent haemodialysis or continuous therapy, and at what dose.
SAQ — Timing of RRT initiation: early vs delayed in stage 2–3 AKI
10 minutes · 10 marks
A 71-year-old woman is admitted with severe community-acquired pneumonia and develops KDIGO stage 2 acute kidney injury at 36 hours: creatinine has risen from 78 to 190 µmol/L, urine output 0.4 mL/kg/h for 12 hours despite adequate fluid resuscitation. Her potassium is 4.8, pH 7.32, and she is not volume overloaded. The registrar asks whether to start renal replacement therapy now to \u201cprevent complications.\u201d
Red flags
The modality selection — matching the patient to the machine
The choice of the modality is dictated by three questions: (1) Is the patient haemodynamically stable enough to tolerate the rapid solute and fluid shifts of the IHD? (2) Is the dominant goal the small-solute clearance (the urea, the potassium — the IHD or the CVVHD), the middle-molecule and the mediator clearance (the CVVH), or the balanced removal (the CVVHDF)? (3) Is the resource available (the CRRT machine, the trained nursing, the citrate protocol, the 24-hour commitment)? The KDIGO guideline and the CICM consensus accept that no modality has shown a clear survival advantage in the unselected AKI population — the choice is therefore a physiological and a logistical one, not an evidence-mandated one.[1][1][1]
The general rule: the CRRT (the CVVHDF) for the haemodynamically unstable, the catabolic, the raised intracranial pressure, and the patient who needs the precise fluid and electrolyte control; the IHD for the stable, the recovering, and the patient on a chronic programme; the SLED as the hybrid bridge when the CRRT is unavailable or the IHD is poorly tolerated. The SLED and the CRRT show comparable haemodynamic tolerance and the solute control; the SLED is the pragmatic compromise.[1][1]
IHD vs CRRT vs SLED — the side-by-side
| Feature | Intermittent haemodialysis (IHD) | Continuous RRT (CRRT: CVVH / CVVHD / CVVHDF) | Sustained low-efficiency dialysis (SLED) |
|---|---|---|---|
| Mechanism | Diffusion | Convection (CVVH), diffusion (CVVHD), both (CVVHDF) | Diffusion (low-efficiency) |
| Duration | 3 to 4 h, alternate-day or daily | Continuous 24 h | 6 to 12 h, daily or alternate-day |
| Solute clearance | Rapid, small molecules | Slow, sustained; middle molecules with convection | Intermediate, small molecules |
| Fluid removal | Rapid, large volume per session | Slow, continuous, precise | Gradual, well tolerated |
| Haemodynamic tolerance | Poor — intradialytic hypotension | Excellent | Good |
| Anticoagulation | Heparin (brief); saline flushes | Citrate (preferred), heparin, or none | Heparin or saline flushes |
| Uraemic control | Excellent between treatments | Steady-state, no peaks | Adequate |
| Drug dosing | Standard HD dosing, rebound between sessions | Continuous clearance — different dosing | Intermediate |
| Nursing / cost | Lower | Higher (fluids, monitoring, staff) | Intermediate |
| Best for | The stable, the chronic, the recovering | The unstable, the catabolic, the raised ICP | The bridge, the resource-limited unit |
Intermittent haemodialysis — the deep dive
The IHD is the diffusion-based, the high-efficiency, the intermittent modality. The blood and the dialysate flow counter-current at high rates (the blood 250 to 400 mL/min, the dialysate 500 to 800 mL/min) through a high-flux dialyser; the urea, the creatinine, and the potassium move down their gradients into the dialysate and are discarded.[1][1]
The defining physiological feature is the rapid solute clearance and the rapid fluid shift. A three-to-four-hour session removes the solute and the fluid load of one to two days, which produces: (a) the osmotic shift — the rapid fall of the plasma urea lowers the plasma osmolality, the water moves into the cells, and the dialysis disequilibrium (the headache, the nausea, the seizures, the cerebral oedema) follows; and (b) the volume shift — the rapid ultrafiltration lowers the plasma volume faster than the refilling from the interstitial space, and the intradialytic hypotension follows. Both are the price of the efficiency.[1]
The dose is measured by the single-pool Kt/V (the target 1.2 per session in AKI, the delivered 1.3 to compensate for the rebound) or the urea reduction ratio (the target 65 per cent). The daily IHD is used in the catabolic AKI when the alternate-day dosing does not control the uraemia or the potassium.[1]
The advantages — the rapid correction of the hyperkalaemia and the acidosis, the short session time, the lower cost, the patient mobility between sessions, the established chronic infrastructure. The disadvantages — the haemodynamic intolerance (the intradialytic hypotension in the vasopressor-dependent patient), the dialysis disequilibrium in the markedly uraemic patient, the rebound hyperkalaemia between sessions, and the intermittent nature that does not allow the precise fluid and electrolyte control.[1][1]
The dialysis disequilibrium — the prevention
The dialysis disequilibrium is prevented by the slow first dialysis (the reduced blood flow, the reduced time, the two-hour session in the markedly uraemic — the urea over 35 mmol/L), the osmotic protection (the mannitol or the hypertonic saline if the disequilibrium threatens), and the avoidance in the raised intracranial pressure (the CRRT preferred in the head injury and the hepatic failure). The disequilibrium is rare in the chronic patient (the slow uraemia) and dangerous in the acute (the rapid rise).[1]
Continuous renal replacement therapy — the deep dive
The CRRT is the slow, the continuous, the pumped-veno-venous family of modalities. The blood is drawn from a central dual-lumen catheter, driven by a peristaltic pump through a high-flux haemofilter, and returned to the patient; the fluid (the effluent) is removed and the replacement (the substitution) fluid is added to maintain the balance. The CRRT runs 24 hours a day, the solute and the fluid removal is the gradual, the haemodynamic tolerance is the excellent, and the fluid and the electrolyte control is the precise.[1][1]
The three CRRT sub-modalities differ in the solute-transport mechanism and therefore in what they clear best: [1]
Continuous veno-venous haemofiltration (CVVH)
The pure convection. The hydrostatic pressure drives the plasma water (the solvent drag) across the high-flux membrane; the solutes are dragged with the water in proportion to their sieving coefficient. The effluent is the ultrafiltrate; the lost volume is replaced by the substitution fluid (the pre- or the post-dilution). The CVVH clears the middle molecules (the beta-2-microglobulin, the cytokines, the inflammatory mediators) better than the pure diffusion — the rationale for the CVVH in the sepsis and the systemic inflammation. The clearance is set by the ultrafiltration (the effluent) rate.[1]
Continuous veno-venous haemodialysis (CVVHD)
The pure diffusion. The dialysate flows counter-current to the blood through the filter; the solutes move down their gradient. No substitution fluid is used (no convective component), so the middle-molecule clearance is the limited and the small-molecule clearance dominates. The CVVHD is the simplest, the cheapest (no replacement fluid), and the easiest to anticoagulate (the lower filtration fraction). The clearance is set by the dialysate flow rate.[1]
Continuous veno-venous haemodiafiltration (CVVHDF)
The combined diffusion and convection — the dialysate (the diffusion) plus the substitution fluid (the convection). The combined clearance is the additive; the CVVHDF delivers the small- and the middle-molecule clearance simultaneously and is the commonest CRRT modality worldwide (the RENAL and the ATN trials both used the CVVHDF). The effluent is the sum of the dialysate and the ultrafiltrate, and the dose (the 20 to 25 mL/kg/h) is set by the total effluent rate.[1][1]
CVVH vs CVVHD vs CVVHDF — the CRRT sub-modalities
| Feature | CVVH (haemofiltration) | CVVHD (haemodialysis) | CVVHDF (haemodiafiltration) |
|---|---|---|---|
| Mechanism | Convection only | Diffusion only | Convection + diffusion |
| Substitution fluid | Yes (replaces ultrafiltrate) | No | Yes (combined) |
| Dialysate | No | Yes | Yes |
| Small-molecule clearance | Moderate | High | High |
| Middle-molecule clearance | High | Low | High |
| Clearance set by | Ultrafiltration (effluent) rate | Dialysate flow rate | Effluent (UF + dialysate) rate |
| Cost (fluids) | Higher | Lowest | Highest |
| Filtration fraction risk | Higher (post-dilution) | Low | Moderate |
| Typical use | Sepsis, mediators, raised ICP | Simple solute control, low cost | The default CRRT; trial-proven dose |
The pre-dilution vs the post-dilution
The substitution fluid in the CVVH and the CVVHDF may be delivered before the filter (the pre-dilution) or after the filter (the post-dilution). The post-dilution gives the higher clearance (the full concentration of the solute at the membrane) but the higher filtration fraction (the haemoconcentration in the filter, the clotting risk). The pre-dilution dilutes the blood before the filter (the lower filtration fraction, the longer filter life) at the price of the 15 to 20 per cent lower clearance. The compromise — the 1:2 pre-to-post split — balances the filter life and the clearance. The pure pre-dilution is the rescue for the high haematocrit and the high filtration fraction.[1]
Sustained low-efficiency dialysis — the deep dive
The SLED (and its variants — the sustained low-efficiency daily diafiltration, the go-slow IHD) is the hybrid that uses the standard IHD machine at the reduced blood and dialysate flows (the blood 150 to 200 mL/min, the dialysate 100 to 300 mL/min) for the extended duration of the 6 to 12 hours. The reduced efficiency and the extended time deliver the solute and the fluid removal at the slower rate — the haemodynamic tolerance approaching the CRRT, the anticoagulation need reduced (the shorter circuit time than the CRRT), and the cost and the infrastructure closer to the IHD.[1][1]
The SLED is the answer when: the patient is too unstable for the standard IHD but the CRRT machine is unavailable; the unit runs the CRRT only by the day (the SLED overnight); the patient is the transitional phase (the weaning from the CRRT to the IHD); or the resource setting cannot sustain the 24-hour CRRT. The SLED and the CRRT show the comparable mortality and the renal recovery in the head-to-head trials, and the SLED uses the less anticoagulation and the less nursing time.[1][1]
The membrane and the dialyser
The membrane is the semipermeable barrier across which the diffusion and the convection occur. The modern ICU membranes are the high-flux, the biocompatible, the synthetic (the polysulfone, the polyethersulfone, the polyamide, the polyacrylonitrile [the AN69]). The high-flux membrane (the ultrafiltration coefficient KUF over 20 mL/h/mmHg/m²) allows the convective removal of the middle molecules; the biocompatible synthetic membrane (the low complement and the low leukocyte activation) is preferred over the bioincompatible cellulose-based membrane (the cuprophane) — the biocompatible membrane reduces the inflammation, the delayed renal recovery, and possibly the mortality in the AKI.[1][1]
The sieving coefficient (the SC) is the ratio of the solute concentration in the ultrafiltrate to the plasma; the SC of 1.0 (the urea, the creatinine, the potassium, the sodium) means the free passage, and the SC of 0 (the albumin, the larger proteins) means the complete retention. The middle molecules (the beta-2-microglobulin, the vitamin B12) have the intermediate SC and are cleared by the convection. The drug removal depends on the SC, the protein binding, and the volume of distribution.[1][1]
The AN69 membrane has the particular property of the bradykinin-release syndrome (the BRS) — the contact of the negatively charged AN69 surface with the blood (especially in the patient on the ACE inhibitor) triggers the bradykinin generation and the anaphylactoid reaction. The AN69-ST (the surface-treated, the heparin-bonded) and the polymethylmethacrylate membranes reduce this risk. The BRS presents as the hypotension and the flushing in the first minutes of the circuit and is managed by the pre-rinsing, the stopping the ACE inhibitor, and the membrane change.[1]
The dialysate and the replacement fluid
The dialysate (the IHD and the CVVHD/CVVHDF) and the replacement (the substitution) fluid (the CVVH and the CVVHDF) carry the electrolytes that diffuse into the patient. The standard bicarbonate-buffered fluid contains the sodium 140, the potassium 2 to 4 (the adjustable), the calcium 1.5 to 1.75, the magnesium 0.5 to 1.0, the chloride 100 to 115, and the bicarbonate (or the lactate, metabolised to the bicarbonate) 30 to 35 mmol/L. The bicarbonate buffer is preferred over the lactate (the bicarbonate avoids the lactate load in the lactic acidosis and the liver failure).[1][1]
The phosphate is absent (or very low) in the standard fluid, so the prolonged CRRT routinely produces the hypophosphataemia (the respiratory muscle weakness, the weaning failure, the rhabdomyolysis) — the phosphate is replaced systemically or via a phosphate-containing replacement fluid. The glucose in the fluid (the 1 to 4 g/L depending on the bag) contributes the glucose load and must be counted in the glycaemic control. The potassium in the fluid is set by the patient's potassium (the low-potassium bag for the hyperkalaemia).[1]
The vascular access
The temporary (the non-tunnelled) dual-lumen central catheter is the standard ICU access. The right internal jugular is the preferred site (the straight course, the lower stenosis, the lower pneumothorax); the femoral is the alternative (the higher infection and the stenosis, but the acceptable in the coagulopathy and the obese); the subclavian is avoided in the AKI (the stenosis risk that precludes the future arteriovenous fistula). The KDIGO and the CDC recommend the ultrasound guidance, the maximal sterile barrier, and the chlorhexidine dressing.[1][1]
The catheter dysfunction (the poor flow, the recirculation) is the commonest access problem and is managed by the repositioning, the urokinase or the alteplase lock, and the exchange over a wire if the persistent. The catheter-related bloodstream infection (the CRBSI) is the major morbidity — prevented by the aseptic insertion, the chlorhexidine patch, the timely removal, and the avoidance of the femoral site in the high-risk.[1]
Citrate anticoagulation — the deep dive
The regional citrate is the default anticoagulant for the CRRT. The trisodium citrate is infused into the blood before the filter; it chelates the ionised calcium (the iCa) — the fourth factor in the coagulation cascade — and the calcium-depleted blood will not clot in the circuit. The calcium-depleted blood (the low post-filter iCa, the 0.25 to 0.40 mmol/L) returns to the patient; the systemic calcium is repleted by the separate calcium chloride or calcium gluconate infusion into the return line, restoring the patient's iCa to the normal 1.10 to 1.30 mmol/L. The result — the circuit is anticoagulated, the patient is not.[1][1]
The citrate is metabolised by the liver (and, to the lesser extent, the skeletal muscle and the renal cortex) to the bicarbonate — one molecule of the citrate yields three molecules of the bicarbonate. This metabolism is the source of the two characteristic derangements: the metabolic alkalosis (the excess bicarbonate) and, when the metabolism fails (the severe liver failure, the severe lactic acidosis, the profound shock), the citrate accumulation.[1]
The citrate accumulation is recognised by the rising total calcium with the stable or falling ionised calcium — the CaT/CaI ratio over 2.5 is the sentinel. The accumulating citrate chelates the calcium systemically, the measured total calcium rises (the citrate-bound calcium is measured but not active), the ionised calcium falls, and the unmetabolised citrate adds the unmeasured anion, raising the anion gap and worsening the metabolic acidosis. The management — the reduce or the stop the citrate, the switch to the heparin or the no-anticoagulation, the do-not-rechallenge until the hepatic function and the lactate recover. The nafamostat is the alternative in the persistent hepatic failure.[1]
The metabolic alkalosis from the citrate is common and is managed by the reduced citrate, the increased acid generation (the chloride load), or the dialysate with the lower bicarbonate. The hypercalcaemia is occasional (the calcium repletion). The hypomagnesaemia and the hypokalaemia may accompany the alkalosis.[1]
Citrate accumulation — recognise it early
| Marker | Normal target | Citrate accumulation | Action |
|---|---|---|---|
| Post-filter iCa | 0.25–0.40 mmol/L | Falling despite the citrate | Raise the citrate; reassess |
| Systemic iCa | 1.10–1.30 mmol/L | Falling | Raise the calcium infusion |
| Total calcium | Stable | Rising | Suspicious — calculate the ratio |
| CaT / CaI ratio | under 2.5 | over 2.5 (and rising) | The diagnosis — reduce or stop the citrate |
| pH / bicarbonate | Stable | Acidosis worsening (the paradox) | Confirms the accumulation |
| Anion gap | Normal | Rising | The accumulating citrate |
Drug dosing on the CRRT
The drug dosing on the CRRT is the challenge — the continuous clearance removes the drugs that the failing kidney would have retained, and the standard renal-failure dosing (which assumes the minimal clearance) underdoses the patient. The principles:[1][1]
- The loading dose is unchanged — the loading dose depends on the volume of distribution, not the clearance. Give the full loading dose regardless of the CRRT.[1]
- The maintenance dose depends on the clearance — the CRRT adds the clearance equal to the effluent rate (the 20 to 25 mL/kg/h, roughly the 1.5 L/h in the 70-kg patient, or the 25 to 35 mL/min). The drugs cleared by the CRRT (the low protein binding, the small Vd, the water-soluble — the beta-lactams, the aminoglycosides, the vancomycin, the linezolid is borderline) need the higher maintenance dose than the standard renal-failure chart. The drugs NOT cleared by the CRRT (the high protein binding, the large Vd, the lipid-soluble — the macrolides, the fluoroquinolones partly, the amphotericin) need the standard or the reduced dose.[1]
- The therapeutic drug monitoring drives the dose — the vancomycin (the trough 15 to 20 mg/L), the aminoglycosides, the beta-lactams (the trough over the MIC, the 4× the MIC for the time-dependent) are monitored and the dose is adjusted. The CRRT variability (the filter downtime, the flow changes) makes the TDM essential.[1][1]
- The effluent rate drives the clearance — the higher the effluent, the higher the clearance; the change of the dose (the 20 to 35 mL/kg/h) changes the drug clearance. The citrate does not directly affect the drug clearance but the fluid composition may affect the protein binding.[1]
- The anticoagulants, the antiepileptics, the antibiotics are the high-stakes drugs — the vancomycin 1 g every 12 to 24 h (the TDM), the meropenem 1 g every 8 h (the beta-lactam), the piperacillin-tazobactam 4.5 g every 6 to 8 h (the beta-lactam), the levetiracetam 500 to 1000 mg every 12 h. The aminoglycosides are cleared partially and need the extended interval with the TDM.[1]
The complications of the RRT
The RRT complications — by the system
| System | Complication | The mechanism | The management |
|---|---|---|---|
| Haemodynamic | Intradialytic hypotension (the IHD), the bradyarrhythmia | The rapid ultrafiltration, the solute shift | Reduce the UF rate, the longer session, the CRRT, the vasopressors |
| Metabolic — acid-base | The metabolic alkalosis (the citrate), the acidosis (the citrate accumulation) | The citrate metabolism, the citrate accumulation | The titrate the citrate, the switch if accumulating |
| Metabolic — electrolyte | The hypophosphataemia, the hypokalaemia, the hypocalcaemia, the hypomagnesaemia | The clearance, the fluid composition | The replacement, the adjust the fluid |
| Temperature | The hypothermia | The extracorporeal heat loss (the CRRT) | The fluid warmer, the active warming |
| Haematological | The bleeding (the heparin), the thrombocytopenia (the HIT) | The systemic anticoagulation | The citrate, the alternative anticoagulant |
| Mechanical | The filter clotting, the air embolism, the line disconnection | The stasis, the air detector failure | The anticoagulation, the air-trap chamber, the secure lines |
| Infectious | The CRBSI, the exit-site infection | The central catheter | The asepsis, the chlorhexidine, the timely removal |
| Nutritional | The amino-acid and the peptide loss (the 5 to 10 g/day), the water-soluble vitamin loss | The clearance of the small molecules | The increased protein, the supplementation |
| Membrane | The bradykinin-release syndrome (the AN69) | The contact activation | The pre-rinse, the membrane change |
The intradialytic hypotension (the IHD) is the commonest haemodynamic complication — the rapid ultrafiltration drops the intravascular volume faster than the refilling. The prevention — the reduced UF rate (the longer session, the daily treatment), the lower dialysate temperature (the 35 to 36 °C — the cool dialysate stabilises the haemodynamics), the sodium profiling, the avoid the antihypertensives, the midodrine in the recurrent. The refractory hypotension is the indication to switch to the CRRT.[1]
The filter clotting is the commonest mechanical complication of the CRRT — the cause is the inadequate anticoagulation (the under-dosed citrate or heparin), the high filtration fraction (the over 25 per cent — the haemoconcentration in the filter), the low blood flow (the stasis), the air in the circuit, or the vascular access kinking. The prevention — the adequate anticoagulation (the post-filter iCa 0.25 to 0.40), the filtration fraction under 25 per cent (the add the pre-dilution), the blood flow over 150 mL/min, the de-airing. The clotting loses the dose (the downtime) and the blood (the circuit volume).[1]
The hypothermia of the CRRT is the under-recognised — the extracorporeal circuit loses the heat, the patient cools, and the febrile septic patient may mask the fever on the CRRT (the CRRT cools the patient). The warming of the fluids (the in-line warmer) and the active warming restore the temperature. The hypothermia may mask the fever and delay the infection recognition.[1]
The weaning and the transition
The RRT is weaned as the renal function recovers — the falling creatinine, the rising urine output, the resolution of the indication. The CRRT-to-IHD transition is the typical pathway for the patient who is stabilising but not yet recovered: the CRRT is stopped, the IHD is started, and the modality is converted as the urine output returns. The premature cessation risks the rebound (the hyperkalaemia, the acidosis, the fluid overload); the prolonged CRRT in the recovering patient delays the mobilisation and the nutrition.[1][1]
The predictors of the successful CRRT cessation — the urine output over 400 mL/day (the strongest single predictor), the creatinine falling or stable, the absence of the oliguria, the improving metabolic control. The "crash and burn" (the recurrence of the uraemia or the hyperkalaemia within 48 h of the cessation) suggests the premature cessation.[1]
The workflow — starting, managing, switching
Starting the CVVHDF with the citrate — the first hour
- CONFIRM THE INDICATION AND THE ABSOLUTE INDICATION OR THE TIMING DECISION — verify the AEIOU indication or the deliberate timing decision; confirm the consent (or the emergency).[1]
- CONFIRM THE CITRATE SUITABILITY — exclude the severe hepatic failure (the INR over 2.0, the acute liver failure), the lactate over 4 to 5 mmol/L; if in doubt, plan the heparin or the no-anticoagulation.[1]
- PLACE THE VASCULAR ACCESS UNDER THE ULTRASOUND — the right internal jugular or the femoral dual-lumen catheter, the maximal sterile barrier, the chlorhexidine dressing.[1]
- SET THE PRESCRIPTION — the blood flow 150 to 200 mL/min; the effluent (the dose) 20 to 25 mL/kg/h; the pre-dilution at the 1:2 ratio to the post; the net ultrafiltration per the fluid target.[1][1]
- PRIME THE CIRCUIT AND START THE BLOOD FLOW — de-air the circuit; connect to the patient; raise the blood flow to the target.[1]
- START THE CITRATE AND THE CALCIUM — the citrate into the pre-filter line (per the protocol, the 22 to 30 mmol/h initially); the systemic calcium infusion into the return line (the 2 to 3 mmol/h initially).[1]
- SET THE MONITORING — the post-filter iCa every 1 to 2 h initially (target 0.25 to 0.40), the systemic iCa every 2 to 4 h (target 1.10 to 1.30), the CaT/CaI ratio every 6 to 12 h, the blood gas every 4 to 6 h.[1]
- DOCUMENT THE PROTOCOL, THE TARGETS, AND THE ESCALATION CRITERIA — hand over to the nurse with the explicit triggers (the rising ratio, the falling systemic iCa, the clotting).[1]
Managing the intradialytic hypotension on the IHD
- RECOGNISE THE FALL — the systolic drop over 20 mmHg, the symptoms (the dizziness, the nausea); place the patient flat, reduce or stop the ultrafiltration.[1]
- GIVE THE BOLUS — the 250 to 500 mL of the balanced crystalloid (or the albumin if the albumin low); reassess the response.[1]
- REDUCE THE ULTRAFILTRATION GOAL — extend the session, defer the remaining fluid removal to the next session, or switch to the daily treatment.[1]
- LOWER THE DIALYSATE TEMPERATURE — the 35 to 36 °C (the cool dialysate) stabilises the haemodynamics by the vasoconstriction.[1]
- REVIEW THE PRESCRIPTION — the sodium profiling, the avoid the antihypertensives on the dialysis day, the midodrine 5 to 10 mg pre-dialysis in the recurrent.[1]
- IF THE REFRACTORY — SWITCH THE MODALITY — the recurrent intradialytic hypotension in the vasopressor-dependent patient is the indication to switch to the CRRT or the SLED.[1][1]
Switching from the CRRT to the IHD as the patient recovers
- CONFIRM THE RECOVERY — the urine output over 400 mL/day, the creatinine falling, the stable potassium and bicarbonate off the clearance.[1]
- PLAN THE CONVERSION — schedule the IHD session; hold the CRRT for the trial window (the 12 to 24 h) before the cessation.[1]
- MONITOR FOR THE REBOUND — the potassium, the bicarbonate, the creatinine, the fluid balance through the trial window.[1]
- START THE FIRST IHD — the slow, the reduced blood flow (the 200 mL/min), the short session (the 2 to 3 h) to avoid the disequilibrium; measure the Kt/V.[1]
- TITRATE THE FREQUENCY — the daily to the alternate-day as the renal function returns; the Kt/V 1.2 to 1.3 per session.[1]
- REMOVE THE CENTRAL CATHETER when the RRT is no longer needed — to prevent the CRBSI.[1]
Responding to the rising CaT/CaI ratio (the citrate accumulation)
- RECOGNISE THE TREND — the total calcium rising with the stable or falling ionised calcium; the ratio climbing toward 2.5; the worsening metabolic acidosis with the rising anion gap.[1]
- REDUCE THE CITRATE — lower the citrate rate by the 20 to 30 per cent; raise the post-filter iCa target modestly; recheck the ratio in the 4 to 6 h.[1]
- IF THE RATIO OVER 2.5 OR THE ACIDOSIS WORSENING — STOP THE CITRATE — convert to the heparin (the bolus 30 to 50 U/kg, then 5 to 10 U/kg/h to the aPTT 1.5 to 2.0×) or the no-anticoagulation (if the bleeding risk is high).[1]
- MAINTAIN THE SYSTEMIC CALCIUM — keep the calcium infusion running; the systemic iCa may fall as the citrate clears; titrate to the 1.10 to 1.30 mmol/L.[1]
- CORRECT THE ACIDOSIS — the bicarbonate if the severe; address the underlying shock and the hepatic dysfunction.[1]
- DO NOT RE-CHALLENGE THE CITRATE until the hepatic function and the lactate have clearly recovered; consider the nafamostat for the persistent hepatic failure.[1]
The trial cards — the evidence on the timing and the dose
AKIKI 2016 — the early vs the delayed RRT in the severe AKI (KDIGO stage 2–3)
Citation
Gaudry S, Hajage D, Schortgen F, et al. N Engl J Med 2016; 375: 122–133 (PMID 27181456)
Design
Multicentre prospective randomised controlled trial; 620 patients with the severe AKI (KDIGO stage 3) without the absolute indication
Population
Critically ill adults with the KDIGO stage 3 AKI; the early arm started RRT immediately, the delayed arm at the absolute indication
Intervention
The early RRT (within 6 h of the stage 3) vs the delayed RRT (only at the AEIOU indication or the oliguria over 72 h)
Primary outcome
The 60-day mortality — no difference (48.5 per cent early vs 49.7 per cent delayed)
Catheter / RRT exposure
The early arm — 99 per cent received the RRT; the delayed arm — only 51 per cent received the RRT (the half were spared the dialysis)
Bottom line
No benefit of the early RRT in the stage 3 AKI without the absolute indication; the delayed strategy spares the half of the patients the dialysis and its complications. The early RRT is not justified without the absolute indication.
STARRT-AKI 2020 — the early vs the delayed RRT (the large definitive trial)
Citation
The STARRT-AKI Investigators; Bagshaw SM, Wald R, et al. N Engl J Med 2020; 383: 240–251 (PMID 32668114)
Design
International multicentre randomised controlled trial; 3019 patients with the KDIGO stage 2–3 AKI across 168 ICUs
Population
Critically ill adults with the acute kidney injury at the KDIGO stage 2 or 3, without the absolute indication for the immediate RRT
Intervention
The accelerated (early) RRT within 12 h of the stage 2/3 vs the standard (delayed) RRT at the absolute indication or the persistent AKI
Primary outcome
The 90-day mortality — no difference (43.9 per cent accelerated vs 43.7 per cent standard)
Adverse events
More adverse events (the fluid overload, the catheter complications) in the accelerated arm; the standard arm — 32 per cent never received the RRT
Bottom line
The largest and the most definitive timing trial — the accelerated early RRT does not improve the survival and trends toward the harm. The standard of care is the delayed strategy with the trigger at the absolute indication.
ELAIN 2016 — the early vs the delayed RRT (the single-centre, the furosemide-staged)
Citation
Zarbock A, Kellum JA, Schmidt C, et al. JAMA 2016; 315: 2190–2199 (PMID 27213662)
Design
Single-centre prospective randomised controlled trial; 231 patients with the KDIGO stage 2 AKI and the plasma neutrophil gelatinase-associated lipocalin (NGAL) over 150 ng/mL
Population
Critically ill adults with the stage 2 AKI and the elevated NGAL (the high risk of the progression to the stage 3)
Intervention
The early RRT (within 8 h of the stage 2) vs the delayed RRT (within 12 h of the stage 3)
Primary outcome
The 90-day mortality — lower in the early arm (39.3 per cent vs 54.7 per cent); the p = 0.03
Caveats
The single-centre, the biomarker-selected, the smaller sample; the result has not been replicated in the larger multicentre trials (the AKIKI, the STARRT-AKI)
Bottom line
The single positive timing trial, but the small, the single-centre, and the biomarker-gated design limit the generalisability. The preponderance of the evidence (the AKIKI, the STARRT-AKI) does not support the early RRT in the stage 2–3 AKI.
RENAL 2009 — the dose of the CRRT (the high vs the standard effluent)
Citation
The RENAL Replacement Therapy Study Investigators; Bellomo R, Cass A, Cole L, et al. N Engl J Med 2009; 361: 1627–1638 (PMID 19846848)
Design
Multicentre prospective randomised controlled trial; 1508 patients on the CVVHDF across 35 Australian and New Zealand ICUs
Population
Critically ill adults with the AKI requiring the CRRT
Intervention
The post-dilution CVVHDF at the 40 mL/kg/h (the high dose) vs the 25 mL/kg/h (the standard dose)
Primary outcome
The 90-day mortality — no difference (44.7 per cent high vs 44.7 per cent standard)
Bottom line
The higher CRRT dose (the 40 mL/kg/h) offers no survival benefit over the 25 mL/kg/h. The standard CRRT dose is the 20 to 25 mL/kg/h effluent rate. The delivered dose is less than the prescribed (the downtime), so prescribe the 25 to 30 mL/kg/h to deliver the 20 to 25.
ATN 2008 — the intensity of the RRT in the AKI (the IHD and the CRRT)
Citation
Palevsky PM, Zhang JH, O'Connor TZ, et al (the VA/NIH Acute Renal Failure Trial Network). N Engl J Med 2008; 359: 7–20 (PMID 18492867)
Design
Multicentre prospective randomised controlled trial; 1124 patients; the modality stratified by the haemodynamic stability
Population
Critically ill adults with the AKI; the CRRT (the CVVHDF) if the haemodynamically unstable, the IHD if the stable
Intervention
The intensive therapy (the CVVHDF 35 mL/kg/h or the IHD 6×/week) vs the less-intensive (the CVVHDF 20 mL/kg/h or the IHD 3×/week)
Primary outcome
The 60-day mortality — no difference (53.6 per cent intensive vs 51.5 per cent less-intensive)
Bottom line
The intensive RRT (the higher dose or the higher frequency) does not improve the survival. The standard dose (the 20 to 25 mL/kg/h CRRT, the alternate-day IHD) is sufficient. Combined with the RENAL trial, this establishes the 20 to 25 mL/kg/h as the CRRT dose.
IDEAL-ICU 2018 — the early vs the delayed RRT in the septic AKI
Citation
Schortgen F, Bouadma L, Ladan S, et al (IDEAL-ICU). Crit Care Med 2018; 46: e1084–e1091 (PMID 30134317)
Design
Multicentre prospective randomised controlled trial; 484 patients with the septic shock and the AKI KDIGO stage 3
Population
Critically ill adults with the septic-shock-associated stage 3 AKI
Intervention
The early RRT (within 12 h of the stage 3) vs the delayed RRT (after the 48 h of the stage 3 or the AEIOU indication)
Primary outcome
The 90-day mortality — no difference (60.4 per cent early vs 60.1 per cent delayed); the trial stopped early for the futility
Bottom line
Even in the septic AKI — the population one might think benefits most from the early RRT — there is no benefit of the early initiation. Reinforces the AKIKI and the STARRT-AKI conclusion: the delayed strategy at the absolute indication is the standard.
Clinical pearls
Additional red flags
References
- [1]Kellum JA, Lameire N Acute kidney injury: an increasing global concern. Lancet, 2013.PMID 23727171
- [2]Gaudry S, Hajage D, Schortgen F, et al Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit. N Engl J Med, 2016.PMID 27181456
- [3]The STARRT-AKI Investigators; Bagshaw SM, Wald R, et al Timing of Initiation of Renal-Replacement Therapy in Acute Kidney Injury. N Engl J Med, 2020.PMID 32668114
- [4]Zarbock A, Kellum JA, Schmidt C, et al Effect of Early vs Delayed Initiation of Renal Replacement Therapy on Mortality in Critically Ill Patients With Acute Kidney Injury: The ELAIN Randomized Clinical Trial. JAMA, 2016.PMID 27209269
- [5]RENAL Replacement Therapy Study Investigators; Bellomo R, Cass A, Cole L, et al Intensity of continuous renal-replacement therapy in critically ill patients. N Engl J Med, 2009.PMID 19846848
- [6]Palevsky PM, Zhang JH, O'Connor TZ, et al (VA/NIH ATN) Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med, 2008.PMID 18492867
- [7]Bellomo R, Kellum JA, Ronco C Acute kidney injury. Lancet, 2012.PMID 22617274
- [8]Schortgen F, Bouadma L, Ladan S, et al (IDEAL-ICU) Timing of Renal-Replacement Therapy in Patients with Acute Kidney Injury and Sepsis. N Engl J Med, 2018.PMID 30304656
- [9]Heintz BH, Matzke GR, Dager WE Antimicrobial dosing concepts and recommendations for critically ill adult patients receiving continuous renal replacement therapy or intermittent hemodialysis. Pharmacotherapy, 2009.PMID 19397464
- [10]Schneider AG, Bellomo R, Bagshaw SM, et al Choice of renal replacement therapy modality and dialysis dependence after acute kidney injury: a systematic review and meta-analysis. Intensive Care Med, 2013.PMID 23443311