ICU · Respiratory / ventilation
Auto-PEEP & Ventilation in Obstruction (Asthma & COPD)
Also known as Auto-PEEP · Intrinsic PEEP · Dynamic hyperinflation · Permissive hypercapnia · Ventilation in asthma · Ventilation in COPD · Status asthmaticus ventilation · Inspiratory threshold load · Breath stacking
In severe airflow obstruction (asthma, COPD), incomplete expiration traps gas and generates intrinsic (auto-) PEEP and dynamic hyperinflation, which raise the work of breathing, drop venous return and cardiac output, and risk barotrauma. Ventilation must prioritise emptying over ventilation: permissive hypercapnia (accept a PaCO2 up to 60-80 mmHg with a pH at least 7.15), a low tidal volume (6-8 mL/kg ideal body weight), a low respiratory rate (10-12) for a long expiratory time, a high inspiratory flow with an I:E ratio of 1:3 to 1:4, and a low external PEEP set at about 75-80 per cent of the auto-PEEP. If the blood pressure crashes after intubation, disconnect the circuit to let the lung deflate.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
In severe airflow obstruction — asthma and COPD — narrowed airways and (in emphysema) lost elastic recoil slow expiration, so the patient cannot fully exhale before the next breath begins. Gas traps, the lungs hyperinflate, and a positive alveolar pressure builds at end-expiration: intrinsic (auto-) PEEP. The central goal of mechanical ventilation here is not to normalise the CO2 but to limit dynamic hyperinflation — by deliberate under-ventilation (permissive hypercapnia), a long expiratory time, and low external PEEP.[1][1]

Why hyperinflation is dangerous
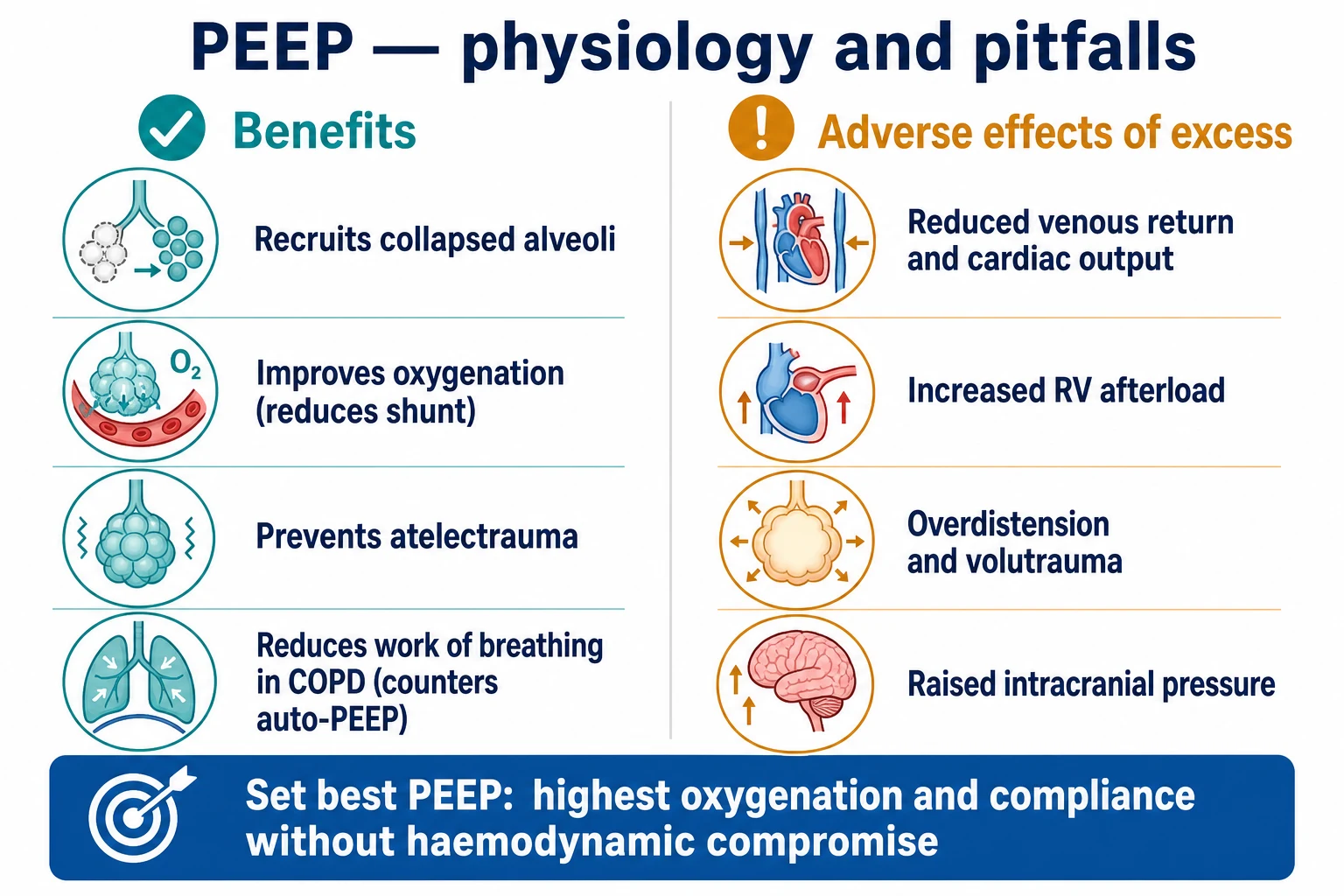
Trapped gas raises the end-expiratory lung volume and the intrathoracic pressure, with several consequences:[1]
- Increased work of breathing — the patient must first overcome the auto-PEEP (the inspiratory threshold load) before generating flow, which is exhausting.
- Haemodynamic compromise — raised intrathoracic pressure reduces venous return and cardiac output; in the extreme, the patient loses their pulse on intubation (the "auto-PEEP arrest"), with pulseless electrical activity that recovers when the circuit is disconnected and the lung deflates.
- Barotrauma — a pneumothorax from the high alveolar pressures.
- Volutrauma — overdistension injures the lung.[1][1]
The pathophysiology — the cascade from obstruction to circulatory arrest
Auto-PEEP is the visible tip of a mechanical and then haemodynamic cascade. Understanding the chain is the difference between treating a number on the ventilator and treating a dying lung: [1]
The dynamic hyperinflation cascade — from bronchospasm to a flat blood-pressure trace
- Airflow obstruction raises expiratory resistance. In asthma, bronchospasm, mucosal oedema and mucus plugs narrow the airway lumen; in COPD, lost elastic recoil destroys the radial traction that holds airways open and flow limitation appears at low lung volumes. Expiration becomes a high-resistance, low-flow event.[2]
- The expiratory time constant (τ = resistance × compliance) lengthens. Each lung unit empties exponentially, with a time constant equal to airway resistance × compliance. In obstructed, compliant emphysematous units τ is several-fold longer than normal, so at the next machine breath the unit is still exhaling and gas is trapped.[7]
- Incomplete expiration traps gas. If the available expiratory time is less than three to five time constants, end-expiratory volume rises above the passive functional residual capacity. This is dynamic hyperinflation — the lung is being filled faster than it can empty.[7]
- Trapped gas generates positive end-expiratory alveolar pressure — intrinsic or auto-PEEP. Because the airway is collapsed or obstructed, this positive pressure is not transmitted to the airway opening, so it is "occult." Pepe and Marini first described this hidden pressure in 1982.[2]
- End-expiratory lung volume and intrathoracic pressure rise. The hyperinflated chest squashes the heart and great vessels, raises mean pleural pressure, and flattens the diaphragm.
- Venous return and right-heart filling fall. Raised intrathoracic pressure lowers the gradient for systemic venous return, and the hyperinflated lung raises pulmonary vascular resistance against the right ventricle — producing acute cor pulmonale.[6]
- Stroke volume falls → hypotension. Left ventricular preload drops; in the extreme, cardiac output collapses and the patient develops pulseless electrical activity — the auto-PEEP arrest. This is reversible within seconds of disconnecting the circuit.[2][8]
The key insight for the exam: auto-PEEP is not just a respiratory problem — it is a circulatory problem mediated by intrathoracic pressure. Anything that lowers mean intrathoracic pressure (a longer expiration, a lower rate, a lower tidal volume, or circuit disconnection) restores venous return and cardiac output.[6]
| Tier | Mechanism | Bedside sign | Reversibility |
|---|
| Tier | Mechanism | Bedside sign | Reversibility |
|---|---|---|---|
| 1. Mechanical / ventilatory | The inspiratory threshold load — the patient must first "climb" the auto-PEEP before generating flow; wasted triggering | Failed or ineffective triggers, missed breaths, increased work of breathing | Set external PEEP at ~80% of auto-PEEP; bronchodilate |
| 2. Haemodynamic | Raised intrathoracic pressure reduces venous return and increases right-ventricular afterload | Hypotension, narrow pulse pressure, a raised JVP/CVP that paradoxically falls with fluid, oliguria | Drop the rate and tidal volume; give fluid; disconnect the circuit |
| 3. Barotrauma / volutrauma | Alveolar overdistension; high plateau pressure | Sudden desaturation with raised airway pressures → pneumothorax; subcutaneous emphysema | Chest drain; lower the tidal volume; allow permissive hypercapnia |
Detecting auto-PEEP
- The flow-time scalar — the expiratory flow does not return to baseline (zero) before the next breath begins.
- The end-expiratory hold — occluding the expiratory port at end-expiration lets the pressure equilibrate, and the ventilator reads the trapped alveolar pressure.
- Difficulty triggering — in the spontaneously triggering patient, the auto-PEEP makes each triggered breath hard work (the inspiratory threshold load).[1]
How to measure auto-PEEP at the bedside
There are three bedside methods, in increasing order of accuracy and effort. Blanch's review sets out the technique and the pitfalls of each.[7]
Performing an end-expiratory hold to measure intrinsic PEEP
- Make the patient passive. Any active respiratory effort corrupts the reading — active expiration raises it, active inspiration lowers it. Deepen sedation; paralyse if there is any doubt or triggering continues.[7]
- Confirm a stable baseline. On the flow-time scalar, ensure the expiratory limb is the familiar "not returning to zero" shape — that is the problem you are about to quantify.
- Activate the expiratory-hold (end-expiratory occlusion) manoeuvre on the ventilator. The machine occludes the circuit at the very end of expiration, before the next inspiration.
- Hold for 1–2 seconds. Pressure equilibrates between alveoli and the airway opening across the still-open expiratory valve. The ventilator displays the difference between this occlusion pressure and the set external PEEP — that difference is the intrinsic (auto-) PEEP.[2][7]
- Read the value, then repeat. The first reading is often spurious (timing, residual effort). Take two or three and use the highest consistent value, because regional time-constant heterogeneity means only the slowest units reflect the true end-expiratory pressure.[7]
- Interpret it. A measured auto-PEEP above 5 cmH2O is significant; above 10–15 cmH2O warrants active reduction. Remember the number is an average — some units have far more, some far less, so it always under-estimates the worst-affected regions.[7]
Why the displayed value underestimates the regional burden
Auto-PEEP is heterogeneous: fast units (short time constant) empty fully and contribute little; slow units (long time constant, e.g. emphysematous or mucus-plugged regions) trap most of the gas. The single airway-opening pressure measured by an expiratory hold is dominated by the fast units that equilibrate quickly, so it under-reads the pressure in the slow, most-dangerous units. The flow-time scalar (does expiration reach baseline?) is therefore the more sensitive screen, even though the hold gives the number.[7]
The passive vs actively breathing patient
In the passive, controlled-ventilation patient the expiratory hold is reliable and the auto-PEEP is read directly. In the actively triggering patient (pressure-support or spontaneous modes) the hold still works but the value reflects only the static intrinsic PEEP — the dynamic intrinsic PEEP that the patient actually works against can be higher, because triggering clips expiration short. Failed or ineffective triggers are the practical clue that occult dynamic auto-PEEP is loading the patient even when the measured value looks modest.[5][7]
The ventilation strategy
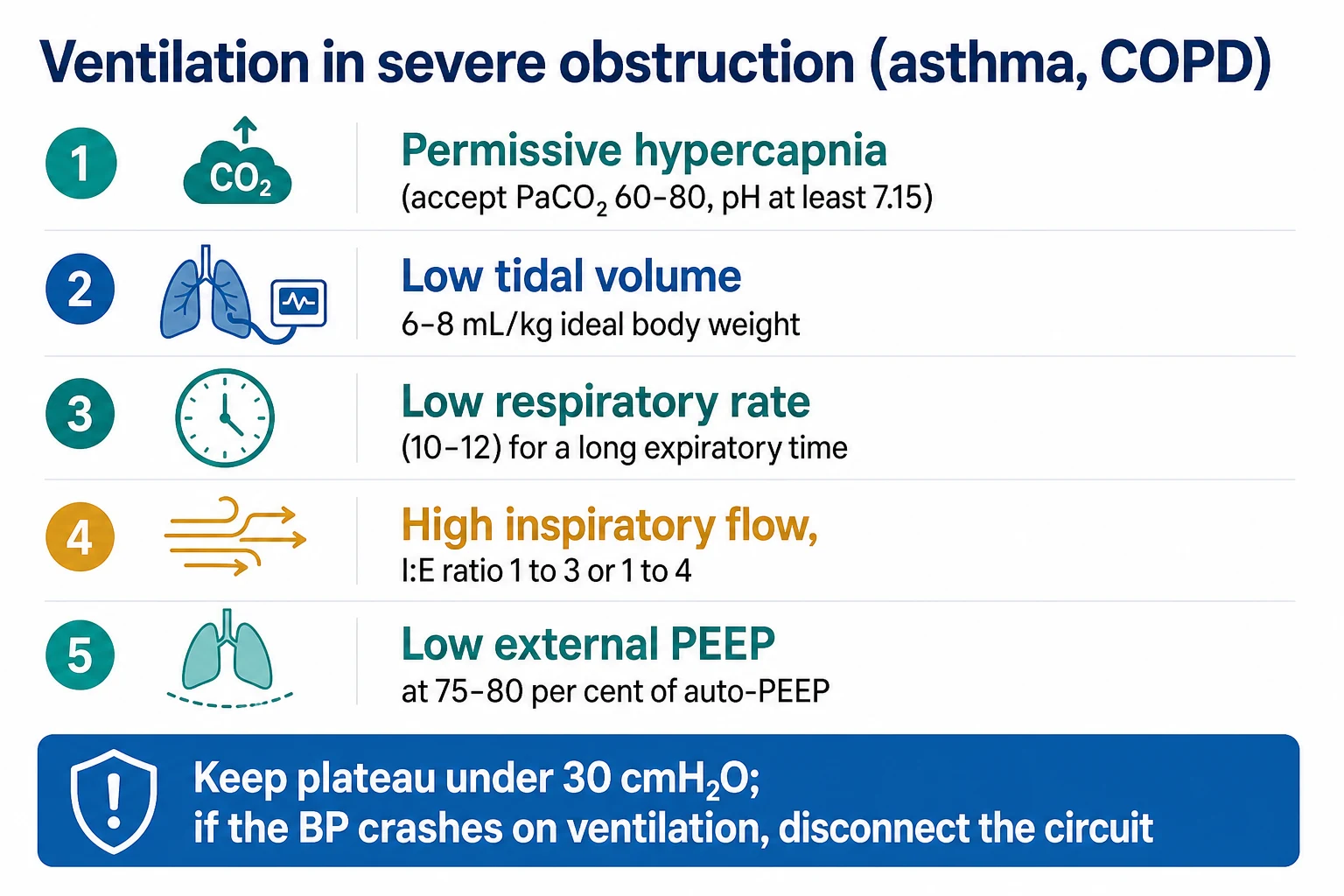
- Permissive hypercapnia — accept a high PaCO2 (up to 60-80 mmHg) provided the pH is tolerated (about 7.15-7.20, even lower with bicarbonate retention). The goal is oxygenation and avoiding hyperinflation, not a normal CO2.[1]
- A low tidal volume — 6-8 mL/kg of ideal body weight, to limit overdistension.
- A low respiratory rate — 10-12 (sometimes lower), to allow a long expiratory time.
- A long expiratory time (a high I:E ratio, 1:3 to 1:4 or more) — set a high inspiratory flow (60-80 L/min) so inspiration is short and expiration is maximised.
- Low external PEEP — set external PEEP at about 75-80 per cent of the auto-PEEP; this counteracts the inspiratory threshold load (easier triggering) and, in flow-limited COPD, splints open collapsing airways, without worsening hyperinflation. (External PEEP set higher than the auto-PEEP adds to the hyperinflation.)[1]
- Keep the plateau pressure under about 30 cmH2O — a marker of the degree of hyperinflation.[1]
Medical and adjunct therapy
- Bronchodilation — nebulised salbutamol and ipratropium, systemic corticosteroids; intravenous magnesium sulphate and parenteral salbutamol in severe asthma.
- Ketamine for sedation (a bronchodilator) and, for refractory bronchospasm, inhalational volatile anaesthetics (isoflurane, sevoflurane) which bronchodilate.[1]
- Deep sedation and paralysis to eliminate patient-ventilator asynchrony and breath-stacking in severe status asthmaticus (short course, watch for critical-illness myopathy).[1]
- Heliox (helium-oxygen) reduces the work of breathing through narrowed airways by its lower density (in the unintubated or near-extubation patient).[1]
- ECMO for refractory cases (the recruitable gas exchange fails).[1]
Causes of auto-PEEP — patient, ventilator, and circuit factors
Auto-PEEP arises whenever the expiratory time available is too short for the (long) expiratory time constant of the lung, or whenever the delivered volume exceeds what can be exhaled in the time given. The factors divide into three buckets — the patient, the ventilator, and the circuit: [1]
| Bucket | Factor | Why it traps gas | The fix |
|---|
| Bucket | Factor | Why it traps gas | The fix |
|---|---|---|---|
| Patient — high resistance | Asthma (bronchospasm, mucus, mucosal oedema) | High airway resistance lengthens the time constant | Bronchodilators, steroids, magnesium |
| Patient — lost recoil | COPD / emphysema | Flow limitation; small airways collapse at low lung volume | External PEEP ≈ 80% auto-PEEP; treat the exacerbation |
| Patient — high compliance | Emphysema, ARDS-recovery lung | Large compliant units empty slowly | Lengthen expiration; reduce Vt |
| Patient — small airway / ETT | Paediatric, obesity, an undersized or kinked ETT | Added tube resistance stacks onto Raw | Upsize the ETT; use a larger-bore circuit |
| Ventilator — high RR | Tachypnoea, or a set RR that is too high | Steals expiratory time per breath; breaths stack | Drop the set RR to 10–12; sedate/paralyse to stop tachypnoea |
| Ventilator — high Vt | Vt above 8 mL/kg ideal body weight | More volume must be exhaled each breath | Reduce to 6–8 mL/kg IBW |
| Ventilator — short expiratory time | Inverse or near-equal I:E, low inspiratory flow | Inspiration occupies most of the cycle | High inspiratory flow (60–80 L/min); I:E 1:3 to 1:4 |
| Circuit — high resistance | HME, blocked filter, water in the limb, kinked tube | Adds resistance to the expiratory limb | Change the HME/filter; drain water; check patency |
| Asynchrony | Reverse triggering, double triggering, breath-stacking | Extra breaths land within expiration | Deep sedation ± paralysis; adjust trigger and cycle |
The bedside shorthand: auto-PEEP = high RR + high Vt + short expiratory time + an obstructed or flow-limited lung. Change any of the first three to relieve it.[8]
Bedside ventilator optimisation — the structured response
When you see expiratory flow failing to return to baseline, or a rising plateau pressure in an obstructed patient, work through the ventilator in this order: [1]
The structured ventilator response to auto-PEEP
- Confirm and quantify — perform an expiratory hold (occlude at end-expiration, with the patient passive and sedated) and read the pressure above the set PEEP. This is the total intrinsic (auto-) PEEP.[7]
- Reduce the respiratory rate — usually the single most effective change. Drop to 10–12, sometimes as low as 8, and accept permissive hypercapnia (PaCO2 60–80 mmHg, pH ≥ 7.15).[1]
- Reduce the tidal volume to 6–8 mL/kg ideal body weight to lower the volume that must be exhaled each breath.[1]
- Lengthen expiratory time — raise the inspiratory flow to 60–80 L/min (which shortens inspiration) and target an I:E ratio of 1:3 to 1:4, or even 1:5 in severe asthma.[8]
- Set external PEEP at roughly 80 per cent of the measured auto-PEEP to offset the inspiratory threshold load and splint open flow-limited airways, without worsening hyperinflation.[1][5]
- Treat the bronchospasm — salbutamol 5 mg plus ipratropium 500 µg nebulised (repeat or run continuously), intravenous hydrocortisone 100 mg, and intravenous magnesium sulphate 2 g over 20 minutes.[1]
- Deepen sedation ± a short-acting paralysing agent to eliminate breath-stacking and reverse triggering; ketamine or propofol infusions are typical.[1]
- Confirm resolution on the flow scalar — expiratory flow now returns to baseline before the next breath — and re-check the plateau pressure is below 30 cmH2O.[1]
- Escalate if refractory — inhaled volatile anaesthetic (isoflurane or sevoflurane via an anaesthetic machine), Heliox, or veno-venous ECMO for the lung that cannot be safely ventilated.[1]
| Obstruction type | Mechanism | Effect of external PEEP | Setting |
|---|
| Obstruction type | Mechanism | Effect of external PEEP | Setting |
|---|---|---|---|
| COPD — flow-limited (dynamic airway collapse) | Starling resistor at the small airways; a choke point downstream | Reduces the threshold load WITHOUT raising lung volume, up to the choke-point pressure | External PEEP ≈ 80% of measured auto-PEEP |
| Asthma — predominantly high-resistance | Diffuse bronchoconstriction and mucus plugging | Benefit less clear-cut; risk of adding volume if there is no flow limitation | Cautious; titrate to triggering and plateau, often ~5 cmH2O |
| Fixed upper-airway (tight ETT, stridor, post-extubation oedema) | No choke point downstream | ADDS to hyperinflation — harmful | Do not apply; treat the cause (change ETT, racemic adrenaline) |
The intubation hazard — the auto-PEEP arrest
The dangerous moment is the intubation and the first ventilated breaths: aggressive ventilation of a hyperinflated obstructed lung can drop the venous return so far that the blood pressure collapses and the patient loses their pulse (pulseless electrical activity). The immediate treatment is to disconnect the ventilator circuit (let the trapped gas escape and the lung deflate), then reduce the rate and tidal volume, give fluid, and recommence ventilation gently.[1][1]
Recognising and reversing the auto-PEEP arrest
The just-intubated obstructed chest behaves like a tamponade: intrathoracic pressure is so high that venous return is abolished and the right heart empties against a hyperinflated, high-resistance pulmonary circulation. Ranieri showed that intrinsic PEEP directly depresses cardiac output in COPD, and that lowering it restores stroke volume.[6]
Immediate management of a suspected auto-PEEP arrest
- Recognise the pattern. Hypotension or pulseless electrical activity developing within minutes of commencing ventilation in an asthmatic or COPD patient; high airway pressures; quiet breath sounds (little gas exchange despite high pressures); a raised CVP that does not improve with fluid.[4]
- Disconnect the ventilator circuit at the Y-piece and let the trapped gas escape. You will hear and feel a prolonged expiratory wheeze lasting 10–30 seconds. The blood pressure and pulse usually recover within seconds as venous return is restored.[8]
- Confirm lung deflation (breath sounds return, the chest looks less hyperinflated), then reconnect at much lower settings: RR 8–10, Vt 6 mL/kg IBW, high inspiratory flow, I:E 1:4, FiO2 1.0.[1]
- Give a fluid bolus (250–500 mL crystalloid) to rebuild the venous-return reserve.
- Treat the bronchospasm aggressively — nebulised salbutamol 5 mg and ipratropium 500 µg, intravenous hydrocortisone 100 mg, and consider intravenous magnesium 2 g and intravenous salbutamol; use ketamine for induction or sedation (it bronchodilates).[1]
- Exclude a tension pneumothorax. Auto-PEEP and tension pneumothorax are clinically indistinguishable at the bedside (high pressure, low BP, PEA). If disconnection does NOT restore the blood pressure within 30–60 seconds, ultrasound the chest and decompress.[8]
- Reassess the plateau pressure (inspiratory hold) — target below 30 cmH2O — and re-check the flow scalar to confirm expiration now reaches baseline.[1]
SAQ — Auto-PEEP arrest at intubation in severe asthma
10 minutes · 10 marks
A 28-year-old woman with acute severe asthma is intubated on the ward for exhaustion, a silent chest and drowsiness. Immediately after transfer to the ventilator (RR 16, Vt 500 mL, I:E 1:2) her blood pressure falls from 132/80 to 64/undetectable, her heart rate slows, and she develops pulseless electrical activity at 40 bpm. The peak airway pressure is 52 cmH₂O and breath sounds are barely audible despite the high pressures.
SAQ — Detecting and quantifying auto-PEEP in a ventilated COPD patient
10 minutes · 10 marks
A 68-year-old man with an acute exacerbation of COPD is intubated and ventilated in pressure support. He is tachypnoeic at 30, appears to be 'fighting the ventilator,' and several of his inspiratory efforts fail to trigger a breath. The ventilator displays a peak pressure of 28 cmH₂O. The nurse reports he failed a spontaneous breathing trial because he 'got tired.'
Clinical pearls
Landmark trials and papers
Pepe & Marini 1982 — the original description of auto-PEEP (PMID 7046541)
Source
Am Rev Respir Dis — case series of mechanically ventilated patients with airflow obstruction
Key finding
Demonstrated 'occult' positive end-expiratory pressure: alveolar pressure trapped behind obstructed airways, not displayed by the ventilator
Clinical bottom line
Named the entity (the 'auto-PEEP effect') and established the need for an expiratory-hold manoeuvre to detect it
Darioli & Perret 1984 — controlled hypoventilation in status asthmaticus (PMID 6703497)
Source
Am Rev Respir Dis — case series of 34 episodes of mechanically ventilated status asthmaticus
Key finding
Zero mortality using deliberate controlled hypoventilation, accepting PaCO2 values often above 90 mmHg
Clinical bottom line
Established permissive hypercapnia as the ventilation paradigm in severe asthma — ventilate to empty the lung, not to normalise the gas
Williams 1992 — risk factors for morbidity in ventilated severe asthma (PMID 1519836)
Source
Am Rev Respir Dis — prospective observational study of mechanically ventilated acute severe asthma
Key finding
Dynamic hyperinflation (reflected in plateau pressure) was the dominant predictor of morbidity; circulatory arrest at intubation was the leading preventable death
Clinical bottom line
Plateau pressure became the titration target, and the 'ventilate to empty the lung' principle was enshrined
Appendini 1996 — external PEEP unloads the COPD patient (PMID 8912740)
Source
Am J Respir Crit Care Med — physiological study in ventilator-dependent COPD patients
Key finding
External PEEP set below the intrinsic PEEP offset the inspiratory threshold load and reduced the work of breathing without worsening hyperinflation
Clinical bottom line
Provided the physiological rationale for the rule 'external PEEP at roughly 80 per cent of intrinsic PEEP'
Blanch 2005 — measurement of air trapping and intrinsic PEEP (PMID 15636649)
Source
Respir Care — narrative review of measurement techniques
Key finding
Compared the expiratory hold, the flow-time scalar, and the occlusion methods, and defined the pitfalls (active effort, heterogeneous time constants) that distort each
Clinical bottom line
The bedside reference for how (and when) to measure auto-PEEP reliably in the ventilated patient
Red flags
Additional red flags
Putting it together — the structured daily review
The daily ventilator review in the obstructed patient
- Look at the flow scalar. Does expiratory flow reach baseline before the next breath? If not — auto-PEEP is present. Quantify with an expiratory hold (patient passive).[7]
- Read the plateau pressure (inspiratory hold). Target < 30 cmH₂O. If raised, the lung is over-inflated regardless of the CO₂.[1]
- Confirm the strategy is in place: low Vt (6–8 mL/kg IBW), low RR (10–12), high inspiratory flow (60–80 L/min), I:E 1:3 to 1:4.[8]
- Check the blood gas. Is the pH ≥ 7.15? If yes, do not escalate ventilation — treat the bronchospasm and the hyperinflation instead.[1]
- Reassess the haemodynamics. Is the BP stable off or on minimal vasopressors? A rising vasopressor requirement in the obstructed patient is dynamic hyperinflation until proven otherwise.[6]
- Set external PEEP at about 80 per cent of the measured auto-PEEP (if flow-limited) and confirm triggering is now easy.[5]
- Plan the bronchodilator and steroid wean, the sedation/paralysis holiday (avoid critical-illness myopathy), and the day of extubation.[1]
| Question | The answer an examiner wants |
|---|
| Question | The answer an examiner wants |
|---|---|
| What is auto-PEEP? | Positive alveolar pressure at end-expiration that is not displayed by the ventilator because it is trapped behind obstructed/collapsed airways — first described by Pepe and Marini in 1982.[2] |
| How do you detect it? | Two ways: qualitatively on the flow-time scalar (expiratory flow fails to return to baseline), and quantitatively by an end-expiratory hold manoeuvre in a passive patient.[7] |
| Why is it dangerous? | Three reasons: increased work of breathing (inspiratory threshold load), haemodynamic compromise (reduced venous return, RV afterload, the "auto-PEEP arrest"), and barotrauma/volutrauma from overdistension.[1][6] |
| How do you ventilate the obstructed patient? | Permissive hypercapnia (PaCO₂ up to 60–80, pH ≥ 7.15), low Vt 6–8 mL/kg IBW, low RR 10–12, high inspiratory flow with I:E 1:3 to 1:4, external PEEP at ~80% of auto-PEEP, plateau < 30 cmH₂O.[1][8] |
| What do you do if the BP crashes after intubation? | Disconnect the circuit at the Y-piece and let the trapped gas escape (the lung deflates over 10–30 s); the BP usually recovers in seconds. Then ventilate gently, give fluid, treat the bronchospasm, and exclude a tension pneumothorax if there is no recovery.[4] |
References
- [1]Laher AE, Buchanan SK. Mechanically Ventilating the Severe Asthmatic J Intensive Care Med, 2018.PMID 29105540
- [2]Pepe PE, Marini JJ. Occult positive end-expiratory pressure in mechanically ventilated patients with airflow obstruction: the auto-PEEP effect Am Rev Respir Dis, 1982.PMID 7046541
- [3]Darioli R, Perret C. Mechanical controlled hypoventilation in status asthmaticus Am Rev Respir Dis, 1984.PMID 6703497
- [4]Williams TJ, Tuxen DV, Scheinkestel CD, et al. Risk factors for morbidity in mechanically ventilated patients with acute severe asthma Am Rev Respir Dis, 1992.PMID 1519836
- [5]Appendini L, Purro A, Patessio A, et al. Partitioning of inspiratory muscle workload and pressure assistance in ventilator-dependent COPD patients Am J Respir Crit Care Med, 1996.PMID 8912740
- [6]Ranieri VM, Giuliani R, Cinnella G, et al. Intrinsic PEEP and cardiopulmonary interaction in patients with COPD and acute ventilatory failure Eur Respir J, 1996.PMID 8804950
- [7]Blanch L, Bernabe F, Lucangelo U. Measurement of air trapping, intrinsic positive end-expiratory pressure, and dynamic hyperinflation in mechanically ventilated patients Respir Care, 2005.PMID 15636649
- [8]Mosier JM, Sakles JC, Stevens AC, et al. Mechanical Ventilation Strategies for the Patient with Severe Obstructive Lung Disease Emerg Med Clin North Am, 2019.PMID 31262414