ICU · ECMO
Extracorporeal Membrane Oxygenation (ECMO)
Also known as ECMO · Extracorporeal life support · VV ECMO · VA ECMO · ECLA · Extracorporeal CO2 removal
Extracorporeal membrane oxygenation (ECMO) is the ultimate respiratory and circulatory support — a pump and an oxygenator outside the body that replace the lung (the venovenous, VV ECMO) or the heart and the lung (the venoarterial, VA ECMO). This topic builds the examiner's framework on the circuit and the cannulation, the two modes (VV for the isolated respiratory failure, VA for the cardiogenic shock and the arrest), the evidence (the EOLIA trial for the severe ARDS, the CESAR trial for the conventional-vs-ECMO, and the VA ECMO complications), the anticoagulation and the complications (the bleeding, the thrombosis, the haemolysis, the infection, the limb ischaemia), the weaning and the decannulation, and the ethical and the resource questions of the ECMO.
On this page & tools
Your progress
Saved locally on this device.
Target exams

Overview & definition
Extracorporeal membrane oxygenation (ECMO) is the external pump and oxygenator that takes the venous blood, removes the CO2, adds the oxygen, warms it, and returns it — replacing the function of the lung (the venovenous, VV ECMO), or the heart and the lung (the venoarterial, VA ECMO). It is the ultimate support for the patient in the refractory respiratory or the cardiac failure, and it is a complex, resource-intensive, team-delivered therapy.[4][5]
The two modes serve different purposes. The VV ECMO drains the venous blood, oxygenates it, and returns it to the venous system (the right atrium) — it supports the OXYGENATION but NOT the circulation (the patient's own heart pumps the blood). It is for the isolated, severe, refractory respiratory failure (the severe ARDS). The VA ECMO drains the venous blood and returns it to the arterial system (the femoral artery or the axillary) — it supports BOTH the oxygenation and the circulation (it pumps the blood). It is for the cardiogenic shock, the cardiac arrest and the myocarditis.[4]
The ECMO circuit
The circuit has five components: the cannulae (the drainage and the return), the pump (the centrifugal, the magnetically levitated), the oxygenator (the hollow-fibre membrane that exchanges the O2 and the CO2), the heat exchanger (the warmer), and the monitoring (the flows, the pressures, the pre- and the post-membrane gases).[4]
The cannulation for the VV ECMO is typically the femoral vein (the drainage) to the right internal jugular vein (the return), or a dual-lumen single cannula (the Avalon) in the right internal jugular. For the VA ECMO, it is the femoral vein (the drainage) to the femoral artery (the return). The flows are 3 to 6 L/min for the VV, 3 to 5 L/min for the VA. The sweep gas (the FiO2 of 1.0, the flow titrated to the PaCO2) runs through the oxygenator.[4][5]
VV ECMO: the respiratory support and the evidence
The VV ECMO is for the severe, refractory ARDS — the patient whose lung cannot oxygenate despite the lung-protective ventilation, the proning and the optimisation. The evidence is the EOLIA trial (NEJM 2018) and the CESAR trial (Lancet 2009).[1][2]
The EOLIA trial (NEJM 2018) randomised the patients with the very severe ARDS (the PaO2/FiO2 below 50 for over 3 hours, or below 80 for over 6 hours, or a pH below 7.25 with the PaCO2 above 60) to the early VV ECMO versus the conventional ventilation (with the ECMO rescue if the conventional failed). The trial was stopped early at a prespecified interim analysis for futility, and the 28-day mortality was 35 per cent (ECMO) versus 46 per cent (control, with 28 per cent crossing over to the ECMO) — a reduction that did not reach the statistical significance, but a post-hoc Bayesian reanalysis suggested a high probability of benefit. The controversy persists, but the VV ECMO is used for the very severe ARDS in the experienced centres.[1]
The CESAR trial (Lancet 2009) — the earlier UK trial — showed that the referral to the ECMO centre (the majority of whom received the ECMO) improved the 6-month survival without severe disability compared with the conventional ventilation. It established the principle of the regional ECMO service for the severe ARDS.[2]
VV ECMO in depth: indications, scoring, cannulation and weaning
The indications and the EOLIA criteria. The modern threshold for the VV ECMO in the severe ARDS is built around the EOLIA entry criteria: a PaO2/FiO2 below 50 for over 3 hours, OR a PaO2/FiO2 below 80 for over 6 hours, OR a pH below 7.25 with a PaCO2 above 60 mmHg — all despite the optimised lung-protective ventilation (the tidal volume of 6 mL/kg, the plateau pressure below 30 cmH2O, the PEEP optimisation, the proning, the neuromuscular blockade). The earlier the referral to the ECMO centre — and the earlier the transfer of the patient who meets the criteria — the better the outcome; the transfer of a hypoxic, hypercapnic, acidotic patient on the high airway pressures is high-risk.[1][12]
Beyond ARDS. The VV ECMO is also used for the severe, refractory respiratory failure from other reversible causes: the severe pneumonia (the bacterial, the viral — the H1N1, where the ANZ ECMO experience reported a 71 per cent survival in the 2009 pandemic, and the COVID-19, where the ECMO was used in the most severe cases in the experienced centres), the near-fatal asthma (the CO2 removal and the oxygenation in the patient with the permissive hypercapnia pushed to its limit), the massive pulmonary haemorrhage, and the bridge to the lung transplant in the end-stage lung disease with the acute decompensation. The principle is the same — a reversible (or bridgeable) lung injury in a patient with an otherwise acceptable prognosis.[6][7]
The survival scores. Two bedside scores help the prognostication and the decision: the RESP score (the Respiratory ECMO Survival Prediction, Schmidt 2014 — derived from the ELSO registry, predicting the hospital survival with the variables that include the age, the cause, the pre-ECMO duration of the ventilation, the acute and the chronic comorbidities, and the pre-cannulation gas exchange), and the PRESERVE score (Predicting Death or Severe Lung Injury in Patients Treated with ECMO, Schmidt 2013 — a simpler five-variable score). Neither is perfect — both discriminate modestly — and they are aids to the clinical judgement, not the substitutes. The score is the conversation, the prognosis, the family meeting, the consent.[8][9]
The cannulation. The classic two-site configuration is the femoral vein (the drainage) to the right internal jugular vein (the return) — the femoro-jugular configuration. The drainage cannula is large (23-29 Fr) and multi-side-holed, advanced to the IVC-RA junction; the return cannula is smaller (17-21 Fr) in the right IJ, directed at the tricuspid orifice. The single-cannula alternative is the bicaval dual-lumen cannula (the Avalon ELITE, the ProtekDuo) inserted via the right IJ — the two lumens drain the IVC and the SVC, the reinfusion jet is directed at the tricuspid orifice. The dual-lumen cannula allows the single-site insertion, the patient mobility (the early rehabilitation), and the lower recirculation, but it requires the fluoroscopic and the echocardiographic guidance and the precise tip position — a malposition causes the massive recirculation and the failing oxygenation.[4][13]
The recirculation. In the VV ECMO, some of the oxygenated return blood is drained straight back into the drainage cannula — the recirculation. It is the commonest cause of the inadequate oxygenation on the VV ECMO. The causes are the cannula position (too close, the dual-lumen malposition), the inadequate flow (the hypovolaemia, the kinking), and the excessive flow for the cannula size. The fix is the repositioning, the volume, the flow reduction, and the check of the drainage and the return saturations (the "pre-membrane" and the "post-membrane" gases).[4][12]
The sweep gas. The sweep gas (the oxygen, the FiO2 of 1.0, the flow in L/min) is the gas that runs through the oxygenator. The CO2 removal is flow-dependent — the higher the sweep, the more the CO2 removed — so the sweep gas flow is titrated to the PaCO2 (the permissive hypercapnia for the lung protection). The oxygenation is flow- and haemoglobin-dependent — the higher the ECMO blood flow, the higher the systemic oxygenation, up to the point of the recirculation. The oxygenator is the lung, the sweep gas is its minute ventilation.[4]
The weaning — the sweep-off trial. The VV ECMO is weaned as the native lung recovers. The daily assessment is for the readiness — the improving compliance, the improving gas exchange on the reducing ventilator settings, the resolving infiltrates. The formal trial is the sweep gas off trial: the ECMO blood flow is maintained (to keep the circuit patent), the sweep gas is turned off (so the oxygenator does nothing), and the patient is assessed on the native lung (the FiO2 of 0.4-0.5, the PEEP of 10, the tidal volume of 6 mL/kg) for 30 to 60 minutes. The success is the stable gas exchange (the PaO2 above 60-70, the PaCO2 stable, the saturation above 90 per cent) and the stable mechanics — and the decannulation. The failure is the re-escalation and the continued support.[4][5]
VA ECMO: the circulatory support
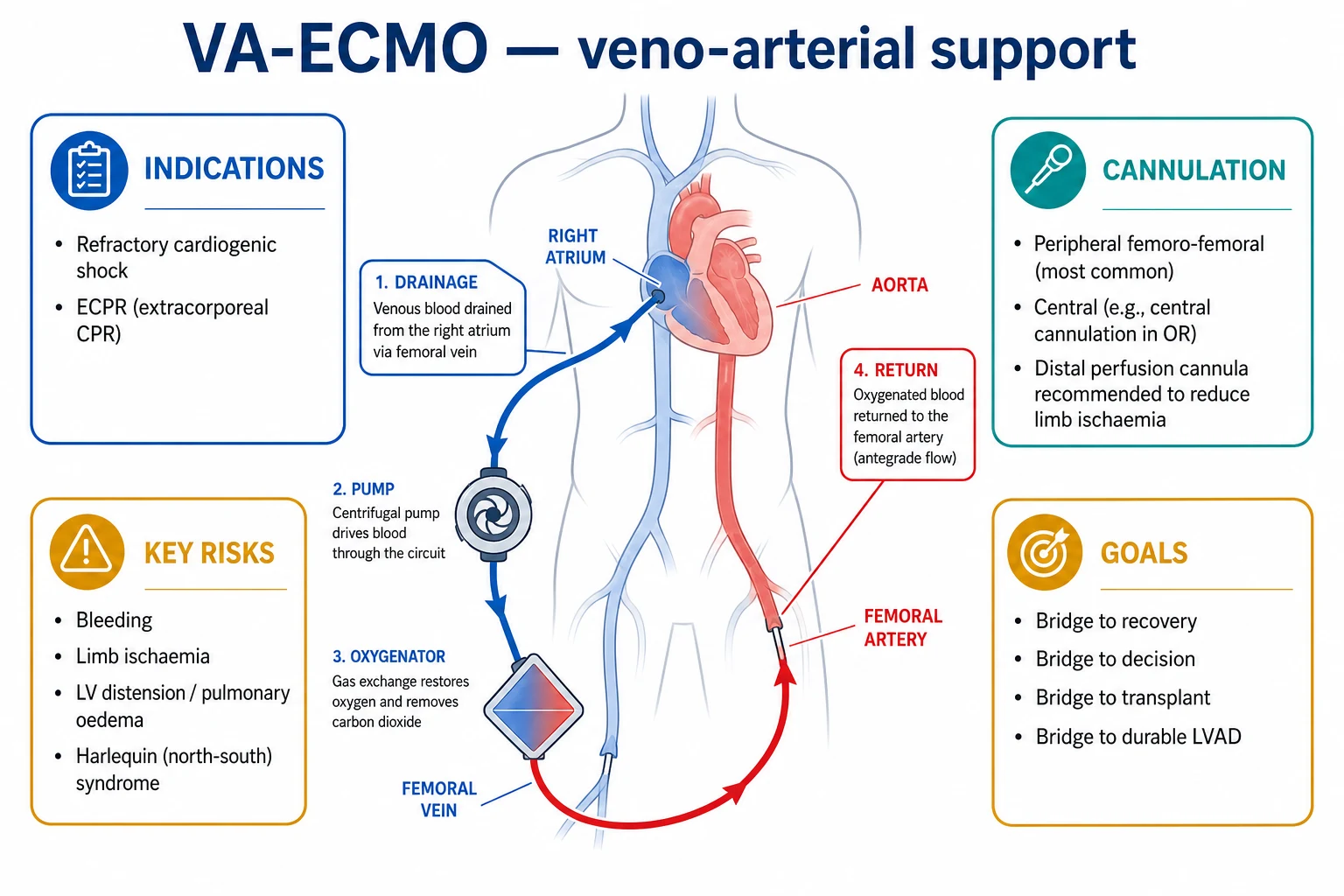
The VA ECMO is for the refractory cardiogenic shock and the cardiac arrest — the failing heart that cannot sustain the circulation. The indications include the fulminant myocarditis (the expected recovery), the massive pulmonary embolism (the right-heart failure), the post-cardiotomy shock, the drug overdose (the reversible cardiotoxicity), and the ECPR (the extracorporeal cardiopulmonary resuscitation for the refractory in-hospital arrest). The principle is the bridge — to the recovery, to the decision, or to the durable therapy (the LVAD, the transplant).[4][5]
The VA ECMO has its own complications — notably the differential hypoxaemia (the upper-body hypoxaemia when the native lung fails in the femoro-femoral VA ECMO, with the deoxygenated blood from the heart perfusing the brain and the coronaries, and the oxygenated ECMO blood perfusing the lower body), the limb ischaemia (from the arterial cannula), and the left-ventricular distension (the afterload rise that impairs the LV emptying, requiring the LV venting or the Impella).[3]
VA ECMO in depth: indications, cannulation, ECPR and the LV distension
The indications. The VA ECMO is for the refractory cardiogenic shock — the circulatory failure despite the optimal medical therapy (the inotropes, the vasopressors, the volume status, the IABP, the rhythm control). The common indications are the fulminant myocarditis (the expected recovery in days to weeks), the massive pulmonary embolism (the right-heart failure, often the bridge to the thrombolysis or the embolectomy), the post-cardiotomy shock (the failure to wean from the cardiopulmonary bypass), the acute myocardial infarction with the cardiogenic shock (the bridge to the revascularisation and the recovery), the drug overdose with the reversible cardiotoxicity (the beta-blocker, the calcium-channel blocker, the bupivacaine), the peri-partum cardiomyopathy, and the refractory malignant arrhythmia (the storm). The principle is the bridge — to the recovery (the myocarditis, the overdose), to the decision (the cardiac arrest, the prognosis uncertain), or to the durable therapy (the LVAD, the heart transplant).[4][5]
ECPR — the extracorporeal cardiopulmonary resuscitation. The ECPR is the rapid deployment of the VA ECMO during the refractory in-hospital or out-of-hospital cardiac arrest — the arrest that has not responded to the conventional CPR. The rationale is to restore the circulation (the brain and the heart perfusion) while the reversible cause is addressed (the coronary occlusion, the pulmonary embolism, the hypothermia, the drug toxicity). The evidence is growing but still selective: the ARREST trial (Yannopoulos 2020, Lancet — a phase-2 single-centre open-label RCT in the refractory VF out-of-hospital arrest) showed a survival-to-discharge benefit (43 per cent vs 7 per cent in the historical control) for the early ECPR. The selection is critical — the witnessed arrest, the bystander CPR, the initial shockable rhythm, the short no-flow and the low-flow time, the age and the comorbidity. The ECPR is a resource-intensive therapy for the highly selected patient.[11]
The SAVE score. The Survival After Veno-arterial ECMO (SAVE) score (Schmidt 2015, derived from a large international cohort) predicts the survival of the VA ECMO for the cardiogenic shock. It uses the age, the weight, the acute and the chronic diagnostics, the pre-ECMO organ failures, the cardiac arrest before the ECMO, the diuresis, the pre-ECMO bicarbonate, the peak inspiratory pressure, and the dlCO2 — and assigns the patients to the survival classes from I (over 75 per cent) to V (below 10 per cent). It is a guide to the prognosis and the family conversation, not the decision rule.[10]
The cannulation. The VA ECMO is most commonly the femoro-femoral — the femoral vein (the drainage, advanced to the right atrium) and the femoral artery (the return). It is rapid, peripheral, and achievable at the bedside or in the arrest. The alternative is the central cannulation (the right atrium to the ascending aorta, at the sternotomy) — used in the post-cardiotomy shock (the chest is already open) and in the cases where the peripheral artery is inadequate or the central flow is preferred (the better upper-body oxygenation). The axillary artery configuration (an end-to-side Dacron graft on the subclavian) is an option for the longer-term support and the better upper-body perfusion, and it allows the patient mobility. The choice is the urgency (the femoro-femoral for the arrest), the expected duration (the central/axillary for the bridge to the LVAD), and the upper-body oxygenation (the central/axillary if the native lung is failing).[4][5]
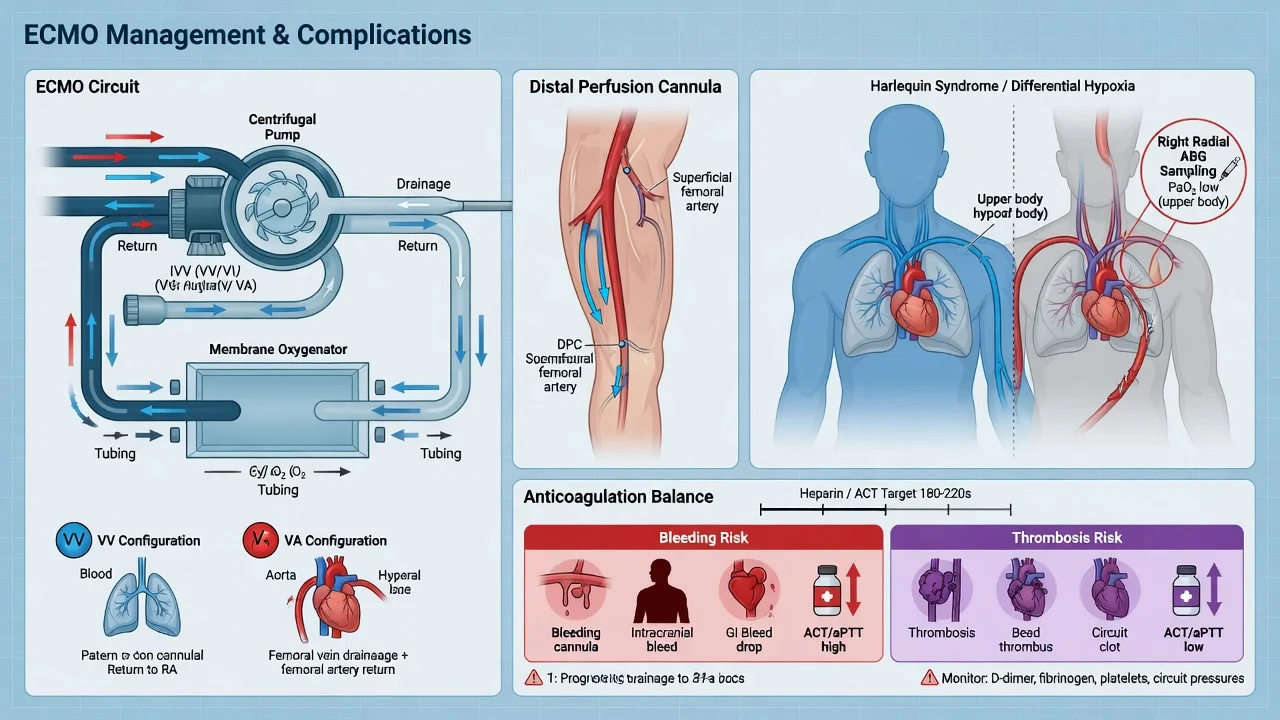
The distal perfusion cannula (DPC). The femoral arterial return cannula (typically 17-21 Fr) can obstruct the ipsilateral limb perfusion — the limb ischaemia, one of the commonest VA ECMO complications (5 to 10 per cent without the prophylaxis). The distal perfusion cannula is a small (6-8 Fr) cannula inserted into the superficial femoral artery (or the posterior tibial, retrograde), connected to a side port of the arterial line, to perfuse the limb. The modern practice is the prophylactic DPC at the time of the cannulation (the ischaemia rate falls to under 1 per cent). The limb is monitored — the pulses, the perfusion, the capillary refill, and the near-infrared spectroscopy (the NIRS) — and any decline prompts the urgent investigation (the angiography, the surgical exploration).[3][4]
The differential hypoxaemia (the North-South / the harlequin syndrome). In the femoro-femoral VA ECMO, the oxygenated ECMO blood is returned to the femoral artery and perfuses the lower body (the abdominal viscera, the legs). The native heart continues to eject — and if the native lung fails (the pulmonary oedema, the pneumonia, the ARDS), the deoxygenated blood from the left heart perfuses the brain and the coronaries (the aortic root, the arch vessels, the upper body). The result is the differential hypoxaemia — the high lower-body saturation with the low upper-body (the right-radial artery) saturation. The recognition is the differential: a low right-radial saturation (below 90 per cent) with the adequate femoral. The fix is the V-AV conversion — adding a venous return (to the right IJ) so the oxygenated blood reaches the right heart and the pulmonary circulation, perfusing the coronaries and the brain. The alternative is the conversion to the central VA (the ascending aorta return) or the optimisation of the native lung.[4][12]
The left-ventricular distension. The VA ECMO returns the blood to the arterial system, raising the afterload against which the failing LV must eject. If the LV cannot eject (the profound LV failure, the aortic stenosis, the severe myocarditis), the LV distends, the mitral regurgitation worsens, the pulmonary oedema worsens, and the coronary and the subendocardial perfusion falls — a vicious cycle that prevents the LV recovery. The recognition is the echo (the dilated LV, the stagnant LV outflow, the spontaneous echo contrast, the aortic valve that does not open) and the rising pulmonary pressures. The fix is the LV venting — the Impella (a percutaneous axial-flow pump across the aortic valve, draining the LV to the aorta), the IABP (the diastolic augmentation and the afterload reduction), the surgical LV vent (the direct drainage via the atrial septostomy or the apex), or the atrial septostomy (the blade balloon, creating an iatrogenic ASD to decompress the left atrium to the right atrium). The unvented, distended LV does not recover, and the pulmonary oedema worsens despite the ECMO.[3][4]
The weaning — the flow-reduction trial. The VA ECMO is weaned as the native heart recovers. The daily assessment is for the readiness — the improving echocardiographic function (the ejection fraction, the aortic-valve opening, the LV contractility), the rising native pulse pressure (the pulsatility on the arterial line — the return of the native cardiac output), the reducing inotropes, the resolving lactate, and the improving end-organ function. The formal trial is the flow-reduction trial: the ECMO flow is reduced stepwise (to 2, then 1.5, then 1 L/min, with the heparin increased to prevent the clotting at the low flow), the haemodynamics and the echo assessed at each step, and the gas exchange maintained by the ventilator. The success is the stable haemodynamics (the MAP above 60, the lactate stable), the stable echo (the EF above 20-25 per cent, the aortic-valve opening, the no LV distension), and the stable gas exchange — and the decannulation. The failure is the re-escalation, the continued support, or the transition to the durable therapy (the LVAD, the transplant).[4][5]
The indications and the contraindications
The indications. For the VV: the severe, refractory ARDS (the PaO2/FiO2 below 80 despite the optimisation, or the EOLIA criteria) with a REVERSIBLE lung injury and no absolute contraindication. For the VA: the refractory cardiogenic shock with a BRIDGE potential (the recovery, the decision, the durable therapy).[4]
The contraindications. The irreversible disease without a bridge (the terminal malignancy, the end-stage fibrotic lung), the severe brain injury (the poor neurological prognosis), the uncontrollable bleeding (the absolute anticoagulation contraindication), the advanced age and the frailty (relative), and the prolonged mechanical ventilation (the concern for the futility, though the threshold varies).[4][5]
Anticoagulation and the complications
The ECMO requires the systemic anticoagulation (the unfractionated heparin, targeting an ACT of about 1.5 times the baseline, or an APTT of 50 to 70 seconds) to prevent the clotting in the circuit. The anticoagulation is a balance — too little and the circuit clots (the oxygenator failure, the embolic stroke); too much and the patient bleeds (the intracranial, the gastrointestinal, the cannula-site).[3][4]
The complications are common and serious: the bleeding (the commonest, at 30 to 50 per cent — the intracranial, the GI, the surgical), the thrombosis (the circuit clotting, the venous, the arterial), the haemolysis (the pump shear, the plasma free haemoglobin), the infection (the cannula-site, the line, the ventilator-associated), the limb ischaemia (the femoral arterial cannula of the VA), the acute kidney injury (common, often requiring the RRT), and the neurological (the stroke, the intracranial haemorrhage).[3]
The weaning and the decannulation
The VV ECMO is weaned as the native lung recovers — the improving lung compliance, the improving gas exchange on the minimal ventilator settings (the FiO2 of 0.4, the PEEP of 10, the tidal volume of 6 mL/kg), and the "sweep gas off trial" (the ECMO flow maintained, the sweep gas turned off, the patient's own lung assessed). The success of the trial is the decannulation.[4][5]
The VA ECMO is weaned as the native heart recovers — the improving echocardiographic function, the rising native pulse pressure, the reducing ECMO flow, and the "flow-reduction trial" (the ECMO flow reduced to 1 to 1.5 L/min, the haemodynamics and the echo assessed). The success is the decannulation; the failure is the re-escalation or the durable therapy.[4]
Management: the ECMO team and the monitoring
The ECMO is managed by a specialised team — the intensivist, the perfusionist (or the ECMO specialist), the nurse, the surgeon. The monitoring is intensive:[4]
- The circuit — the flow, the pre- and the post-membrane pressure (the delta, the clot burden), the sweep gas, the anticoagulation (the ACT, the APTT, the anti-Xa).
- The patient — the haemodynamics (the MAP, the pulsatility in the VA), the gas exchange (the PaO2, the PaCO2, the SvO2), the native-lung mechanics (the compliance, the driving pressure), the haemolysis (the plasma free haemoglobin, the LDH), the renal function, the limb perfusion (the VA).
- The weaning trials — the daily assessment for the readiness, and the formal trial (the sweep-off for the VV, the flow-reduction for the VA).[1]
Prognosis and the outcomes
The survival of the VV ECMO for the severe ARDS is about 60 per cent (the EOLIA and the ELSO data), and the VA ECMO for the cardiogenic shock about 40 to 50 per cent — the survival depends on the reversibility of the cause, the age and the comorbidity, and the timeliness of the initiation. The ECMO is a bridge, not a destination — the patient who cannot be weaned or bridged to a durable therapy has a poor prognosis, and the ethical question of the futility is central.[1][4]
Compare: VV versus VA ECMO at a glance
[10] [9] [1]FlowSteps — the procedural protocols
Key trials and evidence
EOLIA — Combes 2018, NEJM (ECMO for very severe ARDS) — PMID 29791822
CESAR — Peek 2009, Lancet (conventional ventilation vs ECMO referral) — PMID 19762075
ANZ ECMO Influenza — Davies 2009, JAMA (ECMO for H1N1 ARDS) — PMID 19822628
Noah 2013, Am J Respir Crit Care Med (ECMO for H1N1, comparative cohort) — PMID 23155145
ARREST — Yannopoulos 2020, Lancet (ECPR for refractory VF OHCA) — PMID 33197396
Cheng 2014, Ann Thorac Surg (complications of VA ECMO, meta-analysis) — PMID 24210621
Schmidt 2014 — the RESP score (Am J Respir Crit Care Med) — PMID 24693864
Schmidt 2015 — the SAVE score (Eur Heart J) — PMID 26033984
High-yield pearls — the ECMO viva
SAQ — Indications and evidence for VV-ECMO in severe ARDS
10 minutes · 10 marks
A 38-year-old woman (height 165 cm, weight 70 kg) with influenza A pneumonia is intubated and ventilated. Despite lung-protective ventilation (Vt 6 mL/kg PBW), PEEP 14, FiO2 1.0, and 16 hours of prone positioning, her blood gas shows PaO2 56 mmHg, PaCO2 62, pH 7.18. Plateau pressure is 36 cmH2O at Vt 4 mL/kg. The examiners ask you to justify VV-ECMO cannulation, describe the technique, and summarise the evidence.
SAQ — VA-ECMO for refractory cardiogenic shock
10 minutes · 10 marks
A 55-year-old man presents with an extensive anterior STEMI. Despite reperfusion and inotropes (noradrenaline, adrenaline, dobutamine), he remains in cardiogenic shock: BP 70/45, lactate 6.2, cold peripheries, oliguric. Bedside echo shows a severely impaired LV (EF 15%) with no mechanical complication. An IABP has not improved perfusion. The examiners ask you to discuss VA-ECMO as mechanical circulatory support.
Red flags
References
- [1]Combes A, Hajage D, Capellier G, et al.; EOLIA Trial Investigators, REVA, and ECMONet. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome (EOLIA). New England Journal of Medicine, 2018.PMID 29791822
- [2]Peek GJ, Mugford M, Tiruvoipati R, et al.; CESAR trial collaboration. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR). Lancet, 2009.PMID 19762075
- [3]Cheng R, Hachamovitch R, Kittleson M, et al. Complications of extracorporeal membrane oxygenation for treatment of cardiogenic shock and cardiac arrest: a meta-analysis of 1,866 adult patients. Annals of Thoracic Surgery, 2014.PMID 24210621
- [4]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [5]Kazma JM, van den Anker J, Allegaert K, et al. Anatomical and physiological alterations of pregnancy. Journal of pharmacokinetics and pharmacodynamics, 2020.PMID 32026239
- [6]Davies A, Jones D, Bailey M, et al.; Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza Investigators. Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA, 2009.PMID 19822628
- [7]Noah MA, Peek GJ, Finney SJ, et al. Extracorporeal membrane oxygenation for pandemic influenza A(H1N1)-induced acute respiratory distress syndrome: a cohort study. American Journal of Respiratory and Critical Care Medicine, 2013.PMID 23155145
- [8]Schmidt M, Bailey M, Sheldrake J, et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. American Journal of Respiratory and Critical Care Medicine, 2014.PMID 24693864
- [9]Schmidt M, Zogheib E, Rozé H, et al. The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Medicine, 2013.PMID 23907497
- [10]Schmidt M, Burrell A, Roberts L, et al. Predicting survival after ECMO for refractory cardiogenic shock: the Survival After Veno-arterial-ECMO (SAVE) score. European Heart Journal, 2015.PMID 26033984
- [11]Yannopoulos D, Bartos J, Raveendran G, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open label, randomised controlled trial. Lancet, 2020.PMID 33197396
- [12]Brodie D, Bacchetta M. Extracorporeal membrane oxygenation for ARDS in adults. New England Journal of Medicine, 2011.PMID 22087681
- [13]Javidfar J, Brodie D, Wang D, et al. Use of bicaval dual-lumen catheter for adult venovenous extracorporeal membrane oxygenation. Annals of Thoracic Surgery, 2011.PMID 21619973