ICU · Respiratory
Extracorporeal CO2 removal (ECCO2R) in ICU
Also known as ECCO2R · Extracorporeal carbon dioxide removal · CO2 removal · Low-flow ECMO · Respiratory dialysis
Extracorporeal CO2 removal (ECCO2R): low-flow extracorporeal circuit that removes CO2 WITHOUT providing significant oxygenation (unlike VV-ECMO). Indications: (1) HYPERCAPNIC respiratory failure (COPD exacerbation) where NIV fails — ECCO2R removes CO2 → avoids intubation. (2) FACILITATE ultra-protective ventilation in ARDS (remove CO2 while using very low tidal volumes 3-4 mL/kg → less volutrauma). (3) BRIDGE to lung transplant. ADVANTAGE over VV-ECMO: lower flow (200-500 mL/min vs 2-4 L/min) → smaller cannulae (single venous access — dual-lumen) → less anticoagulation → less complications. LIMITATION: minimal oxygenation (can't treat severe hypoxaemia — need VV-ECMO for that). EVIDENCE: emerging — small RCTs promising but no large definitive trial.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

SAQ — ECCO2R for COPD exacerbation failing NIV
10 minutes · 10 marks
A 68-year-old man with severe COPD (FEV1 35% predicted) is admitted with an infective exacerbation. Despite optimal NIV (IPAP 18, EPAP 6, FiO2 0.4), his ABG shows pH 7.22, PaCO2 78 mmHg, PaO2 64. He is becoming somnolent and tachypnoeic at RR 32. The team is considering intubation. The examiners ask you to discuss the role of ECCO2R as an alternative.
SAQ — ECCO2R to facilitate ultra-protective ventilation in ARDS
10 minutes · 10 marks
A 50-year-old woman with severe ARDS (PaO2/FiO2 95 on FiO2 0.7, PEEP 14) is ventilated with Vt 6 mL/kg predicted body weight; her plateau pressure is 28 cmH2O and driving pressure 16 cmH2O. The examiners ask whether reducing the tidal volume to 3–4 mL/kg ('ultra-protective') — facilitated by ECCO2R — would reduce lung injury, and how you would assess the evidence.
Clinical pearls
Red flags
Prognosis
ECCO2R evidence summary (2023)
Principle and mechanism of action
ECCO2R is an extracorporeal blood-cleansing technique that selectively removes carbon dioxide (CO2) while providing negligible oxygenation. It is conceptually "respiratory dialysis" for CO2. Venous blood is diverted out of the body, passed across a semipermeable membrane lung (hollow-fibre oxygenator) where CO2 diffuses out of the blood and into a ventilating "sweep" gas stream, and then returned to the patient. The fundamental insight that makes low-flow ECCO2R possible is that CO2 is carried in venous blood at a far higher content and diffuses across a membrane far more readily than oxygen, so clinically meaningful CO2 clearance can be achieved at blood flows that are an order of magnitude lower than those needed for ECMO (200–500 mL/min versus 2–4 L/min).[14]
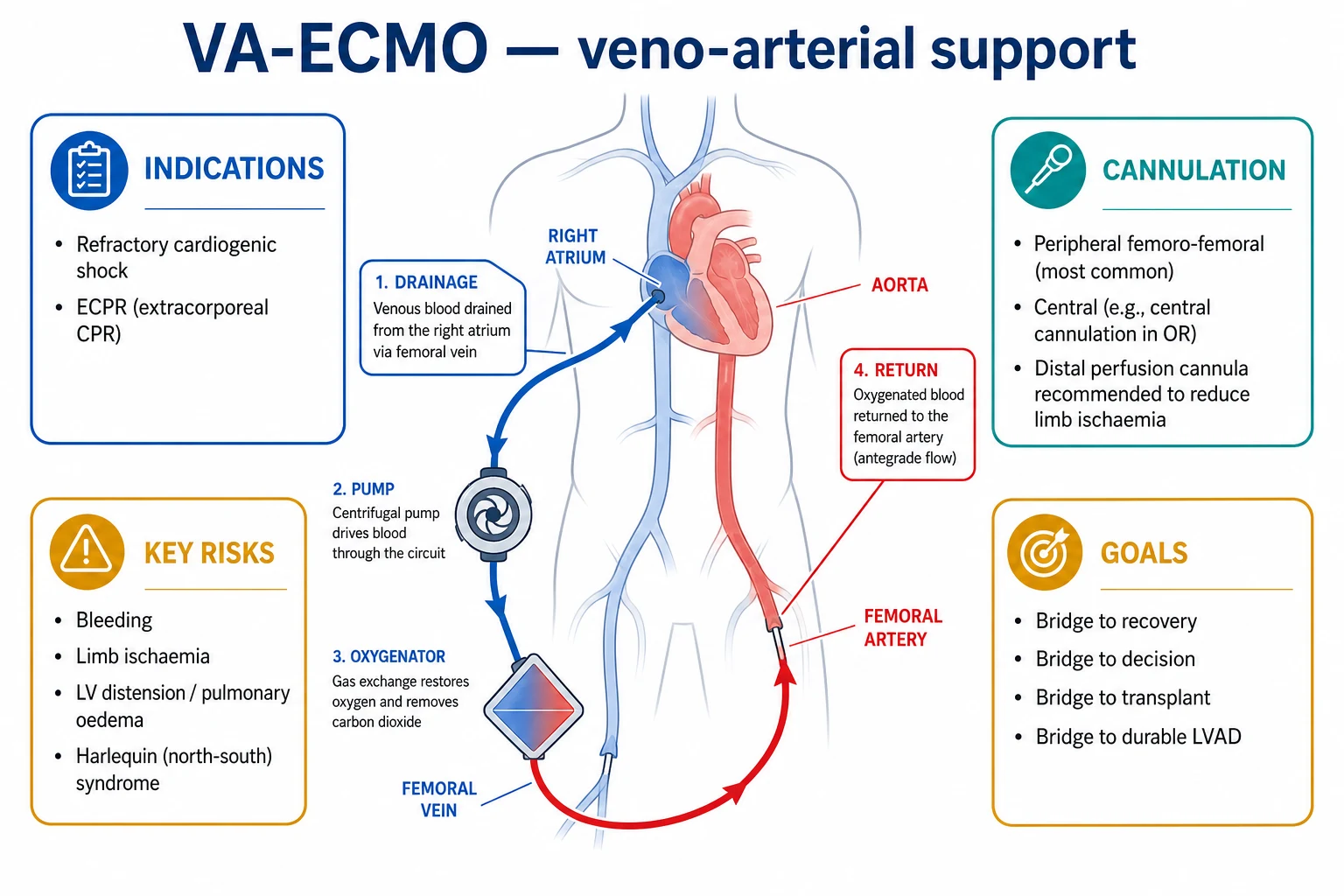
The essential distinction from ECMO is the therapeutic goal, not the hardware. In veno-venous ECMO (VV-ECMO) the objective is to deliver oxygen: the circuit must move enough blood through the oxygenator each minute to supply the body's entire metabolic O2 demand (~250 mL O2/min in a resting adult), which mandates high blood flow. In ECCO2R the objective is to clear a metabolite (CO2): because venous blood is CO2-rich and the membrane is very efficient at stripping CO2, a much smaller fraction of cardiac output (10–15%) needs to be processed. ECCO2R therefore uses the same building blocks — drainage cannula, pump (or arterial driving pressure), membrane lung, sweep gas, return cannula, heat exchanger — but downsized.[12]
[4]Physiology — why low-flow CO2 removal works
Carbon dioxide is the ideal molecule for low-flow extracorporeal clearance, while oxygen is not. Three physiological facts underpin ECCO2R:[14]
1. CO2 content of venous blood is high and the storage capacity is enormous. Mixed venous blood carries ~52 mL CO2/dL (versus ~15 mL O2/dL for arterial blood, of which only ~5 mL/dL is extractible). Most CO2 (~90%) is stored as bicarbonate which, via carbonic anhydrase on the membrane, continuously regenerates diffusible CO2. The body's total CO2 "pool" (120–150 L of CO2 equivalent) dwarfs the O2 pool (~1.5 L). This large, labile reservoir means removing even 50–100 mL/min of CO2 substantially lowers PaCO2 over 30–60 minutes.[7]
2. CO2 diffuses across a membrane ~20× more readily than O2. CO2 is ~20× more soluble in water/blood than O2 (solubility coefficient ~0.03 mmol/L/mmHg vs ~0.0015 for O2). Although the O2 partial-pressure gradient across the lung is larger (~60 mmHg) than the CO2 gradient (~6 mmHg) in vivo, the 20× solubility advantage means CO2 membrane permeability exceeds O2 permeability. In the ECCO2R membrane lung the gradient for CO2 is also large (~50 mmHg, venous PaCO2 ~50 vs sweep gas ~0), so CO2 transfer is highly efficient even at low blood flow.[14]
3. Oxygenation is FLOW-limited, CO2 removal is partly GRADIENT-limited. To deliver the body's ~250 mL O2/min demand, the circuit must extract nearly all O2 from a large blood volume (high flow): delivering 250 mL O2/min from blood donating 5 mL O2/dL requires ~5 L/min of blood flow. By contrast, CO2 removal of 100 mL/min is easily achieved by stripping ~10 mL CO2/dL from just 1 L/min of blood — and because sweep gas flow can be increased independently, CO2 clearance can be boosted without raising blood flow. This asymmetry is the entire physiological justification for ECCO2R.[14]
[14]Clinical consequence: a patient whose problem is pure or predominant hypercapnia (COPD exacerbation, asthma, permissive hypercapnia on protective ventilation) can be supported by ECCO2R. A patient whose problem is predominant hypoxaemia (severe ARDS, pneumonia) cannot — they need the high blood flow of VV-ECMO to deliver oxygen. ECCO2R is a CO2 machine, not an O2 machine.[14]
Techniques and configurations
There are three broad technical approaches to ECCO2R, distinguished by how blood is driven through the membrane lung and by the cannulation strategy. The choice is dictated by the clinical scenario, the amount of CO2 to remove, the desired simplicity, and the patient's haemodynamics.[23]
1. Arterio-venous pumpless — iLA / PECLA
Pumpless Extracorporeal Lung Assist (PECLA), marketed as the iLA (Novalung), uses the patient's own arterial pressure to drive blood from a femoral artery through a low-resistance membrane lung and back into a femoral vein. No pump, no pump-related haemolysis or mechanical failure.
- Driving pressure: mean arterial pressure (requires MAP >70 mmHg and good cardiac function). Flow 1–2 L/min.
- Membrane: very low-resistance biocompatible (heparin-coated) polymethylpentene.
- Cannulae: large-bore femoral arterial (15–17 Fr) and venous (17–19 Fr).
- CO2 removal: very efficient (can remove 100–200 mL/min) — the highest of any ECCO2R configuration.
- Trade-off: places the systemic arterial tree at risk (limb ischaemia from the arterial cannula, distal embolisation) and requires a well-functioning heart. No longer first-line for routine ECCO2R because of lower-flow pump-driven systems, but historically important and still used where pumpless simplicity is desired (e.g., awake bridge-to-transplant).[18][19]
2. Veno-venous pump-driven (modern standard)
A roller or centrifugal pump draws venous blood, pushes it through a small membrane lung, and returns it to the venous system. This is the dominant configuration in modern ECCO2R because it decouples blood flow from the patient's arterial pressure and avoids femoral arterial cannulation.
- Driving mechanism: integrated pump (e.g., Hemolung RAS, iLA activve, PrismaLung on a CRRT platform).
- Blood flow: 200–500 mL/min (up to ~1,000 mL/min on some newer devices).
- Membrane surface: 0.3–0.8 m².
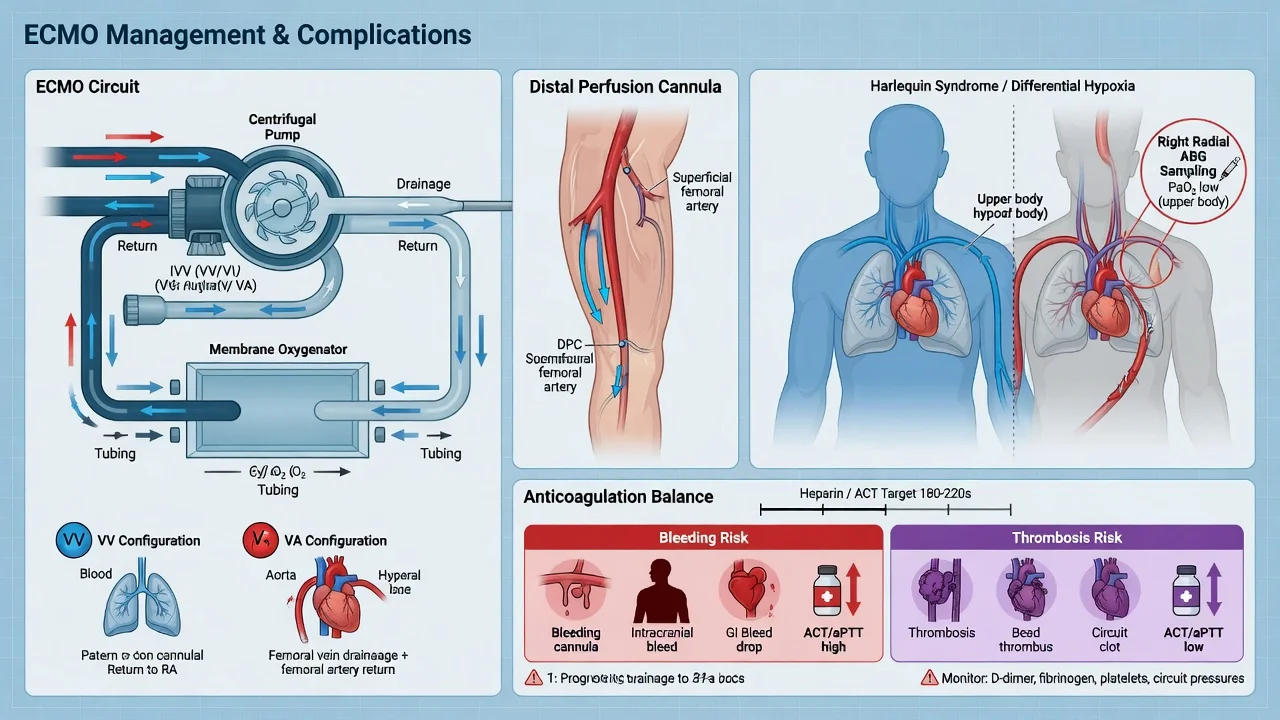
- Anticoagulation: systemic heparin (target ACT 150–180, or aPTT ~1.5×), less than ECMO.[12]
3. Cannulation strategies — single (dual-lumen) vs dual (two-cannula)
- Single dual-lumen cannula (e.g., Avalon Elite / Spectrum): one catheter inserted via the right internal jugular vein has two lumens — one draining blood from the IVC/SVC into the circuit, the other reinfusing oxygenated/decabarboxylated blood directly into the right atrium, oriented toward the tricuspid valve. Advantages: single insertion site, ambulation possible, less recirculation than two-cannula when correctly positioned, suitable for awake patients. Critical caveat: position MUST be confirmed by echocardiography/fluoroscopy — malposition causes recirculation and is the commonest cause of "ECCO2R not working."[12]
- Dual (two-cannula) configuration: drainage cannula (femoral vein) + return cannula (IJ or contralateral femoral). Advantages: simpler to insert, less dependent on precise positioning, less recirculation risk if flow is well directed. Disadvantage: two puncture sites, harder to mobilise the patient.
Devices in current clinical use
- Hemolung RAS (ALung Technologies): integrated pump-oxygenator in one cartridge; single dual-lumen cannula (15 Fr); ~350–450 mL/min flow; most-studied in COPD (the Burki and Del Sorbo cohorts used it).[8][7]
- PrismaLung (Baxter): membrane lung that bolts onto the familiar Prismaflex CRRT platform — leverages ICU staff expertise; 200–450 mL/min.[11]
- iLA activve (Xenios/Novalung): pump-driven, higher flows possible (up to ~1,000 mL/min); also offers the pumpless iLA; widely used in Europe.[18]
- ProLUNG (Estor): similar low-flow pump-driven concept.
- All share: membrane lung + pump + cannula(e) + circuit tubing + sweep-gas source + (optional) heat exchanger.
Indications (in detail)
ECCO2R has three established-or-emerging indications; all rest on the principle that the dominant problem is CO2 retention, not hypoxaemia.[4]
Indication 1 — Hypercapnic respiratory failure (COPD exacerbation) avoiding intubation
The prototypical and best-studied use. A COPD patient with an acute exacerbation develops worsening hypercapnia and acidosis (PaCO2 >70 mmHg, pH <7.25–7.30). NIV (BiPAP) is first-line and succeeds in ~80–90%, but the 10–20% who fail NIV face invasive mechanical ventilation — with its attendant risks (ventilator-associated pneumonia, ICU-acquired weakness, prolonged stay, difficult weaning, mortality). ECCO2R offers a "rescue" to avoid intubation: by removing CO2 extracorporeally, it lowers PaCO2 and corrects pH, reducing the ventilatory load so that the patient can be maintained on (or weaned to) NIV or even HFNC.
- Evidence: Del Sorbo (2015, matched cohort): ECCO2R in hypercapnic patients at risk of NIV failure was feasible; intubation was avoided in a meaningful proportion.[7] Burki (2013, Chest pilot): 20 COPD patients with hypercapnic failure on the Hemolung — most improved their PaCO2 and avoided intubation.[8] Cummins (2018, UK register): real-world ECCO2R outcomes across UK centres.[16]
- Caveat: no definitive large RCT yet; ECLIPSE and similar trials are ongoing/being designed. Current guidance: investigational, specialist centres, carefully selected patients.
Indication 2 — Facilitating ultra-protective ventilation in ARDS
Standard ARDS ventilation (Vt 6 mL/kg PBW, plateau <30) already reduces mortality (ARMA). Ultra-protective ventilation (Vt 3–4 mL/kg PBW) should further reduce volutrauma and strain, but at that Vt minute ventilation is too low and the patient develops permissive hypercapnia and acidosis — which is poorly tolerated (pulmonary hypertension, arrhythmia, raised ICP). ECCO2R removes the excess CO2, allowing the lung to be ventilated at extremely low Vt (or very low driving pressure) without paying the hypercapnia penalty.
- Evidence: Schmidt (2018, Crit Care): low-flow ECCO2R on a CRRT platform enabled reduction of Vt to ~4 mL/kg in mild-moderate ARDS.[11] Combes/SUPERNOVA (2019, ICM): feasibility/safety of ECCO2R to facilitate protective ventilation in moderate ARDS — the device successfully lowered PaCO2 and permitted tidal-volume reduction.[9] Goligher (2019, ICM): SUPERNOVA sub-study showing CO2-removal capacity varied widely between patients and devices — directly informing the design of a definitive trial.[10] Fitzgerald (2014, systematic review): early evidence insufficient for mortality benefit.[17] Worku (2023, meta-analysis): VV-ECCO2R enables ultra-protective ventilation but no proven survival benefit to date.[21]
- Caveat: feasible and safe, but a mortality benefit is unproven; the SUPERNOVA programme is the pivotal trial informing design of larger studies.[13]
Indication 3 — Bridge to lung transplantation
End-stage lung disease (COPD, pulmonary fibrosis, cystic fibrosis) with an acute hypercapnic decompensation can be bridged to transplant with ECCO2R. Because the dominant problem is ventilatory failure (CO2 retention) rather than refractory hypoxaemia, low-flow ECCO2R often suffices and — crucially — can be used in an awake, spontaneously breathing patient via a single dual-lumen cannula, avoiding the deconditioning and complications of intubation while awaiting a donor organ. (When hypoxaemia dominates, VV-ECMO is used instead.)
Emerging / niche indications
- Severe asthma with refractory hypercapnia/acidosis to avoid injurious ventilation (small case series).
- Near-apnoeic oxygenation concept: near-total CO2 removal markedly suppresses respiratory drive, allowing minimal ventilation and "lung rest" (experimental).
- Weaning/liberation from VV-ECMO: step-down from ECMO to ECCO2R before decannulation.
- Peri-operative/peri-procedural support in severe lung disease.
Contraindications
Absolute:
- Severe refractory hypoxaemia as the dominant problem (ECCO2R cannot oxygenate adequately — use VV-ECMO).
- Inability to anticoagulate (active uncontrollable bleeding; absolute heparin contraindication without alternative anticoagulant) — although ECCO2R needs less anticoagulation than ECMO, some anticoagulation is still required.
- No venous access feasible, or uncorrected severe coagulopathy (INR >2.0, platelets <50) not amenable to correction.
- Patient not a candidate for intensive therapy (futility, advance directive declining life support).[20]
Relative:
- Haemodynamic instability / shock for the pumpless AV configuration (needs MAP >70 and good cardiac function — use pump-driven VV instead).
- Severe peripheral vascular disease (femoral cannula risk; favour IJ dual-lumen).
- Severe anaemia (low haemoglobin reduces CO2 carriage and oxygen reserve).
- Morbid obesity or local infection at intended cannulation site.
- Lack of experienced centre/staff — ECCO2R should not be initiated where expertise and circuit-management capability are absent.
- Recovery expected within hours (transient hypercapnia correctable by NIV optimisation).[7]
Complications
ECCO2R complications are fewer and less severe than VV-ECMO (lower flow, smaller cannulae, less anticoagulation) but are not zero.[12][16]
- Bleeding — the commonest significant complication. Sources: cannulation site (jugular is compressible and manageable; femoral arterial worse), heparin anticoagulation, circuit-related consumption of coagulation factors and platelets. Monitor ACT/aPTT, haemoglobin; have low threshold for cannula-site compression and transfusion.
- Haemolysis — mechanical shear on red cells across the pump and membrane. Monitor plasma free haemoglobin, LDH, haemoglobin drop, haptoglobin. Newer centrifugal pumps reduce (but do not eliminate) this; the pumpless iLA has the least haemolysis.
- Circuit clotting / thrombosis — despite anticoagulation, the membrane and tubing can clot, reducing efficiency and requiring circuit exchange. Visible "clot in chamber," rising transmembrane pressure, falling CO2 removal all signal this.
- Access / cannulation complications — pneumothorax (rare with ultrasound guidance), arterial puncture, vessel injury, haematoma, limb ischaemia (especially femoral arterial in pumpless iLA — always use a distal perfusion catheter).
- Recirculation (especially dual-lumen cannula) — reinfused blood is immediately re-drained, halving effective CO2 removal. Suspect when PaCO2 fails to fall; confirm with high pre-/post-membrane CO2 difference; fix by repositioning under imaging.
- Infection — line/catheter-related bloodstream infection; strict asepsis and daily line review.
- Air embolism — risk at any negative-pressure segment of the circuit; modern devices have air detectors and traps.
- Fluid/electrolyte shifts, hypothermia (heat loss across the circuit — use a heat exchanger).
- Device failure (pump stop, membrane rupture) — emergency clamp-and-disconnect protocol must be rehearsed.[4]
Comparison with conventional mechanical ventilation
[7]The fundamental trade-off: conventional ventilation substitutes the lung entirely (oxygenation AND ventilation) at the cost of an artificial airway and positive pressure; ECCO2R substitutes only the ventilatory (CO2-clearance) function, sparing the airway and the lung from pressure, at the cost of an extracorporeal circuit and its bleeding/clotting risks. They are complementary, not interchangeable — ECCO2R fits the gap between failing NIV and intubation.[13]
Additional clinical pearls (advanced)
Evidence summary and ongoing trials
Key ECCO2R studies (verified PMIDs)
Where the evidence is heading
Red flags (consolidated)
Prognosis and current status
ECCO2R sits between NIV/HFNC and invasive ventilation (or between VV-ECMO and liberation) as a CO2-clearance tool. Its physiological rationale is robust and its complication profile is favourable compared with ECMO, but it has not yet been shown in a large RCT to improve survival in any single indication. Current practice: investigational, deployed in specialist ECMO-capable centres for carefully selected patients with predominant hypercapnia — COPD failing NIV, ARDS requiring ultra-protective ventilation, and awake bridge-to-transplant or step-down from VV-ECMO. The trajectory of evidence (SUPERNOVA, ECLIPSE-type trials) will determine whether ECCO2R becomes standard respiratory support or remains a niche rescue.[13][16]
References
- [1]Braune S, Kluge S ECCO(2)R in COPD exacerbation: response to comments by Del Sorbo et al. Intensive care medicine, 2016.PMID 27586995
- [2]Bein T, Aubron C, Papazian L Focus on ECMO and ECCO(2)R in ARDS patients. Intensive care medicine, 2017.PMID 28717835
- [3]Combes A, Fanelli V, Pham T, et al. Feasibility and safety of extracorporeal CO(2) removal to enhance protective ventilation in acute respiratory distress syndrome: the SUPERNOVA study. Intensive care medicine, 2019.PMID 30790030
- [4]Staudinger T Update on extracorporeal carbon dioxide removal: a comprehensive review on principles, indications, efficiency, and complications. Perfusion, 2020.PMID 32156179
- [5]Combes A, Fanelli V, Pham T, et al. Feasibility and safety of extracorporeal CO(2) removal to enhance protective ventilation in acute respiratory distress syndrome: the SUPERNOVA study. Intensive care medicine, 2019.PMID 30790030
- [7]Del Sorbo L, Pisani L, Filippini C, et al. Extracorporeal Co2 removal in hypercapnic patients at risk of noninvasive ventilation failure: a matched cohort study with historical control. Critical care medicine, 2015.PMID 25230375
- [8]Burki NK, Mani RK, Herth FJF, et al. A novel extracorporeal CO(2) removal system: results of a pilot study of hypercapnic respiratory failure in patients with COPD. Chest, 2013.PMID 23460154
- [9]Combes A, Fanelli V, Pham T, Ranieri VM Feasibility and safety of extracorporeal CO(2) removal to enhance protective ventilation in acute respiratory distress syndrome: the SUPERNOVA study. Intensive care medicine, 2019.PMID 30790030
- [10]Goligher EC, Combes A, Brodie D, et al. Determinants of the effect of extracorporeal carbon dioxide removal in the SUPERNOVA trial: implications for trial design. Intensive care medicine, 2019.PMID 31432216
- [11]Schmidt M, Herisse M, Ponthus C, et al. Feasibility and safety of low-flow extracorporeal CO(2) removal managed with a renal replacement platform to enhance lung-protective ventilation of patients with mild-to-moderate ARDS. Critical care, 2018.PMID 29743094
- [12]Morelli A, Del Sorbo L, Pesenti A, Ranieri VM, Fan E Extracorporeal carbon dioxide removal (ECCO(2)R) in patients with acute respiratory failure. Intensive care medicine, 2017.PMID 28132075
- [13]Boyle AJ, Sklar M, McNamee JJ, et al. Extracorporeal carbon dioxide removal for lowering the risk of mechanical ventilation: research questions and clinical potential for the future. Lancet Respiratory Medicine, 2018.PMID 30484429
- [14]Terragni P, Maiolo G, Ranieri VM Role and potentials of low-flow CO(2) removal system in mechanical ventilation. Current opinion in critical care, 2012.PMID 22186219
- [15]Strassmann S, Mertens MC, Bickenbach J, et al. Impact of sweep gas flow on extracorporeal CO(2) removal (ECCO(2)R). Intensive care medicine experimental, 2019.PMID 30911910
- [16]Cummins C, McFadyen A, Rafferty I, Poenaru D, Kinsella J A United Kingdom Register study of in-hospital outcomes of patients receiving extracorporeal carbon dioxide removal. Journal of intensive care society, 2018.PMID 29796067
- [17]Fitzgerald M, Millar J, Blackwood B, et al. Extracorporeal carbon dioxide removal for patients with acute respiratory failure secondary to the acute respiratory distress syndrome: a systematic review. Critical care, 2014.PMID 25033302
- [18]Zimmermann M, Bein T, Arlt M, et al. Pumpless extracorporeal interventional lung assist in patients with acute respiratory distress syndrome: a prospective pilot study. Critical care, 2009.PMID 19183475
- [19]Muller T, Lubnow M, Philipp A, et al. Extracorporeal pumpless interventional lung assist in clinical practice: determinants of efficacy. European respiratory journal, 2009.PMID 19010979
- [20]Bein T, Zimmermann M, Hergeth K, et al. Addition of acetylsalicylic acid to heparin for anticoagulation management during pumpless extracorporeal lung assist. ASAIO journal, 2011.PMID 21427564
- [21]Worku E, Okeke C, Patel R, Goyal R, Henry M Venovenous extracorporeal CO(2) removal to support ultraprotective ventilation in moderate-severe acute respiratory distress syndrome: a systematic review and meta-analysis of the literature. Perfusion, 2023.PMID 35656595
- [22]Karagiannidis C, Brodie D, Strassmann S, et al. Extracorporeal membrane oxygenation: evolving epidemiology and mortality. Intensive care medicine, 2016.PMID 26942446
- [23]Westhoff M, Schonhofer B, Neumann P, et al. Severe hypercapnic respiratory failure in acute exacerbation of COPD: significance of ventilation and extracorporeal CO2 removal. Deutsche medizinische Wochenschrift, 2016.PMID 27903026
- [6]Kryvenko V, Husain-Syed F, Schnell E, et al. Minimally invasive extracorporeal CO(2) removal in hypercapnic respiratory failure: a prospective observational study. Critical care (London, England), 2026.PMID 42057044