ICU · Respiratory / ventilation
Pneumonia — CAP, HAP, VAP & Aspiration
Also known as Pneumonia · Community-acquired pneumonia · CAP · Hospital-acquired pneumonia · HAP · Ventilator-associated pneumonia · VAP · Aspiration pneumonia · CURB-65 · IDSA/ATS criteria
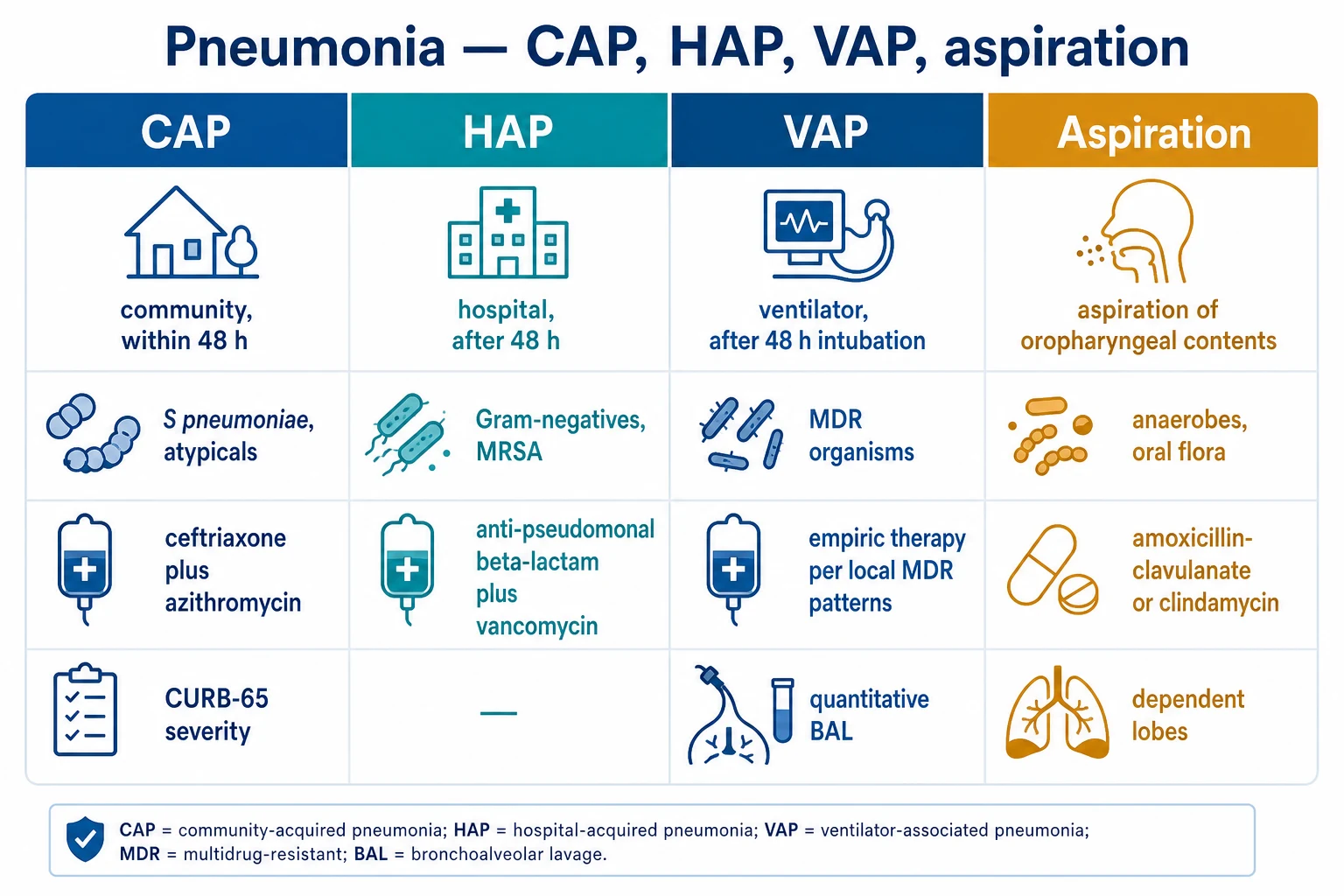
Pneumonia is classified by the setting of acquisition: community-acquired (CAP, outside hospital or within 48 hours of admission), hospital-acquired (HAP, after 48 hours in hospital), ventilator-associated (VAP, after 48 hours of intubation), and aspiration. The severity is graded by CURB-65, PSI, or the IDSA/ATS severe-CAP criteria. The commonest CAP pathogen is Streptococcus pneumoniae; atypicals (Mycoplasma, Legionella, Chlamydia) are also important. Late-onset HAP/VAP introduces multidrug-resistant organisms (Pseudomonas, MRSA, ESBL). The empirical antibiotics are guided by the setting, the severity, and the local antibiogram; de-escalate once the cultures identify the organism. Duration is typically 5-7 days for CAP and 7 days for VAP.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
Pneumonia is an infection of the lung parenchyma (the alveoli), classified by the setting of acquisition, which drives the likely pathogens and the empirical antibiotics:[1][2]
- CAP — community-acquired, outside hospital or within 48 hours of admission.
- HAP — hospital-acquired, 48 hours or more after admission.
- VAP — ventilator-associated, 48 hours or more after intubation.
- Aspiration — from aspiration of oropharyngeal or gastric contents.
The 48-hour cut-off is the examinable boundary between community and nosocomial pathogens. HAP is sub-classified by onset: early (within 4 days of admission — community-type, usually antibiotic-sensitive organisms) versus late (after 4 days — multidrug-resistant organisms). VAP is a subset of HAP occurring 48 hours or more after intubation.[6]
CAP
Community, within 48 h
- Acquired outside hospital or symptoms within 48 h of admission
- S. pneumoniae, H. influenzae, atypicals, respiratory viruses
- Severe ICU: ceftriaxone + azithromycin
- Severity: CURB-65, PSI, IDSA/ATS criteria
- Duration: 5-7 days (stop once stable)
HAP
Hospital, after 48 h
- 48 h or more after admission, not incubating at admission
- Early (<4 d): S. pneumoniae, H. influenzae, MSSA
- Late (>4 d): Pseudomonas, Acinetobacter, ESBL Klebsiella, MRSA
- Empiric: anti-pseudomonal beta-lactam +/- vancomycin
- Duration: 7 days after de-escalation
VAP
Ventilator, after 48 h
- 48 h or more after intubation (subset of HAP)
- Late-onset: MDR Gram-negatives + MRSA dominate
- Empiric: pip-tazo +/- vancomycin; sample BAL/PSB
- Diagnosis: CXR infiltrate + 2 of fever, WBC, purulent sputum
- Prevention bundle is the highest-yield intervention
Aspiration
Oropharyngeal/gastric
- Aspiration of oropharyngeal or gastric contents
- Dependent segments: posterior upper lobe, apical lower lobe
- Anaerobes + oral streptococci + Gram-negatives
- Amoxicillin-clavulanate or clindamycin
- Mendelson pneumonitis (sterile acid) needs no routine antibiotics

CAP — severity and pathogens
Severity scores:[1]
- CURB-65 — Confusion, Urea over 7 mmol/L, Respiratory rate at least 30, Blood pressure (SBP under 90 or DBP 60 or under), age 65 or over. Score 0-1 is outpatient; 2 is ward; 3-5 is ICU.
- PSI/PORT — a more detailed 20-variable score predicting mortality.
- IDSA/ATS severe-CAP criteria — one major (invasive mechanical ventilation, or septic shock needing vasopressors) OR three minor (RR at least 30, PaO2/FiO2 250 or under, multilobar infiltrates, confusion, BUN 20 or over, WBC under 4, hypothermia under 36 degrees Celsius, hypotension needing aggressive fluids). Meets criteria equals ICU admission.[1]
- Typical — Streptococcus pneumoniae (the commonest), Haemophilus influenzae, Moraxella catarrhalis.
- Atypical — Mycoplasma pneumoniae, Chlamydia pneumoniae, Legionella pneumophila.
- Viral — influenza, RSV, SARS-CoV-2.
- Risk factors modify — COPD (Pseudomonas), aspiration (anaerobes, Gram-negatives), immunocompromise (Pneumocystis, fungal).[1]
Pathogens by host profile:[1][2]
- Healthy adult — S. pneumoniae, C. pneumoniae, M. pneumoniae, respiratory viruses.
- COPD / bronchiectasis — add Haemophilus influenzae, Moraxella, and consider Pseudomonas aeruginosa (especially severe COPD on frequent steroids/antibiotics).
- Aspiration risk (stroke, seizure, reduced GCS, dysphagia) — anaerobes plus oral Gram-negatives and streptococci.
- Immunocompromise / HIV — Pneumocystis jirovecii (PJP, if CD4 under 200), fungi (Aspergillus), CMV; plus standard bacterial pathogens which remain commonest.
- Structural lung disease (bronchiectasis, CF) — Pseudomonas aeruginosa (chronic colonisation); Staphylococcus aureus in CF.
Typical bacteria
Covered by beta-lactam
- Streptococcus pneumoniae (commonest overall)
- Haemophilus influenzae
- Moraxella catarrhalis
- Staphylococcus aureus (incl. MRSA post-influenza)
- Gram-negatives (Klebsiella) in alcohol misuse/aspiration
Atypicals
Covered by macrolide/FQ
- Mycoplasma pneumoniae (young adults, cold agglutinins)
- Chlamydia pneumoniae
- Legionella pneumophila (water source, SIADH, GI symptoms)
- Cell-wall-deficient -> not seen on Gram stain, not on blood agar
- Require macrolide, tetracycline, or fluoroquinolone (NOT beta-lactam)
Viruses
Add antiviral
- Influenza A/B (add oseltamivir empirically in season)
- SARS-CoV-2 (COVID-19)
- RSV (elderly, immunocompromised)
- Adenovirus, parainfluenza
- Predispose to secondary Staphylococcal pneumonia (add MRSA cover)
CAP empirical antibiotics
- Outpatient, no comorbidity — amoxicillin, or doxycycline, or a macrolide.[1]
- Outpatient with comorbidity — amoxicillin-clavulanate plus a macrolide, or a respiratory fluoroquinolone.[1]
- Inpatient (non-ICU) — ceftriaxone plus azithromycin, or a respiratory fluoroquinolone.[1]
- ICU — ceftriaxone plus azithromycin (add vancomycin or linezolid if MRSA suspected; add oseltamivir if influenza suspected).[1]
- Duration — 5-7 days (shorter is as effective; guided by clinical stability).[1]
Investigations before antibiotics (do not delay in septic shock):[1]
- Blood cultures x2, sputum for Gram stain and culture, arterial blood gas, full blood count, U&E, LFTs, CRP, lactate.
- Urinary antigens — pneumococcal and Legionella (rapid, high yield in severe CAP).
- Respiratory viral PCR — influenza A/B, SARS-CoV-2, RSV; add oseltamivir empirically if influenza is suspected in season.
- Atypical work-up — Legionella / Mycoplasma serology (paired, fourfold rise) and PCR where available; PJP induced sputum / BAL if immunocompromised.
- Chest X-ray (and CT if complicated: cavitation, effusion, abscess, lymphadenopathy).
Outpatient, no comorbidity
CURB-65 0-1
- Amoxicillin 1 g PO TDS, OR doxycycline 100 mg BD, OR a macrolide
- 5-7 days; stop once afebrile and clinically stable
- Add atypical cover if Legionella suspected
Outpatient with comorbidity
CURB-65 1-2
- Amoxicillin-clavulanate PLUS a macrolide, OR a respiratory fluoroquinolone (moxifloxacin) alone
- Comorbidity: heart, lung, liver, renal disease, diabetes, asplenia
- 5-7 days
Inpatient (non-ICU)
CURB-65 2
- Ceftriaxone 1-2 g IV daily PLUS azithromycin 500 mg IV daily
- Or a respiratory fluoroquinolone (moxifloxacin) alone
- Switch to oral when stable, afebrile, tolerating PO -> early discharge
Severe CAP (ICU)
CURB-65 3-5 / IDSA-ATS
- Ceftriaxone 2 g IV daily PLUS azithromycin 500 mg IV daily
- Add vancomycin/linezolid if MRSA risk (cavitary, post-influenza)
- Add oseltamivir if influenza suspected (do not wait for PCR)
- Add anti-pseudomonal beta-lactam if structural lung disease/Pseudomonas risk
- Minimum 5 days; stop once stable 48-72 h
HAP and VAP
Early-onset (within 4 days) — community-type pathogens (S. pneumoniae, H. influenzae, MSSA). Late-onset (after 4 days) — multidrug-resistant (MDR) organisms: Pseudomonas aeruginosa, Acinetobacter, Klebsiella (ESBL), MRSA.[2]
Empirical antibiotics — guided by the local antibiogram and the risk factors for MDR. An anti-pseudomonal beta-lactam (piperacillin-tazobactam, ceftazidime, cefepime, or meropenem) plus vancomycin or linezolid (if MRSA risk) and consider a second anti-pseudomonal agent (an aminoglycoside or a fluoroquinolone) for high-MDR-risk patients.[2]
De-escalation — narrow once the cultures identify the organism and the sensitivities. Treat for 7 days (shorter if the clinical response is good and the organism is not Pseudomonas or non-fermenting Gram-negative).[2]
VAP diagnosis — new or worsening infiltrate on CXR plus fever, leukocytosis, or purulent secretions; confirmed by quantitative cultures (a BAL with 10 to the 4 CFU/mL or more, or a protected specimen brush with 10 to the 3 or more).[2]
MDR organisms in late VAP — the big four:[6]
- Pseudomonas aeruginosa — the archetypal ICU pathogen; produces biofilm on the tube, inherently resistant to many agents, mutates rapidly to resistance under antibiotic pressure. Cover with an anti-pseudomonal beta-lactam (pip-tazo, cefepime, ceftazidime, meropenem); consider dual therapy in septic shock.
- Acinetobacter baumannii — environmental survivor, often extensively drug-resistant; treat with sulbactam combinations, polymyxin/colistin, or tetracyclines (minocycline, eravacycline). High mortality; involve microbiology.
- Enterobacterales with ESBL or carbapenemases (Klebsiella, E. coli) — ESBL: carbapenem (meropenem). Carbapenem-resistant (CRE): ceftazidime-avibactam, meropenem-vaborbactam, colistin, depending on mechanism.
- MRSA — vancomycin (AUC/MIC-guided) or linezolid (better lung penetration, no nephrotoxicity). Cover empirically if MRSA risk or unit prevalence is high.
- Stenotrophomonas maltophilia — inherently carbapenem-resistant; high-dose TMP-SMX (± ticarcillin-clavulanate or levofloxacin). Classic in patients on prolonged carbapenems.
Anti-pseudomonal beta-lactam
Backbone
- Piperacillin-tazobactam 4.5 g IV q6h (extended infusion)
- Cefepime 2 g IV q8h
- Ceftazidime 2 g IV q8h
- Meropenem 1 g IV q8h (2 g if resistant / ESBL)
- Choose by local antibiogram; extended/continuous infusion improves PK/PD
MRSA cover
Add if MRSA risk
- Vancomycin 15-20 mg/kg q8-12h, AUC/MIC 400-600 guided
- Linezolid 600 mg IV q12h (preferred if AKI, better epithelial lining fluid)
- Risk: prior IV antibiotics, known colonisation, post-influenza, high unit prevalence
- Stop empiric MRSA cover if MRSA not isolated on reliable cultures
Second Gram-negative agent
High MDR risk
- Amikacin / gentamicin (aminoglycoside) — synergistic, nephrotoxic
- Levofloxacin / ciprofloxacin — if susceptible
- Colistin / polymyxin B — if XDR Gram-negative (nephro/neurotoxic)
- Reserve for septic shock, known MDR, or high-prevalence units; stop at 5-7 d
CPIS — Clinical Pulmonary Infection Score
A bedside score (0-2 each across six domains) used to suspect VAP (CPIS >6) and to support stopping antibiotics if it falls by day 3. Domains: temperature (36-38.9 = 0, >=39 or <36 = 1-2), WBC (4-11 = 0), tracheal secretions (none = 0, purulent = 2), PaO2/FiO2 (>240 = 0, <240 = 2), chest X-ray (none/patchy/consolidation), and semi-quantitative BAL culture (0/<1+ / >1+). Moderate accuracy — an adjunct, not a standalone test.[2]
Aspiration pneumonia
From aspiration of oropharyngeal or gastric contents — typically in the dependent segments (the posterior upper lobe and the apical lower lobe in the supine patient; the basal lower lobes if upright). The organisms are anaerobes plus oral Gram-negatives and streptococci. Treat with amoxicillin-clavulanate or clindamycin (covering anaerobes and oral flora). Not every aspiration needs antibiotics (see the aspiration topic — a witnessed aspiration of sterile gastric contents is a chemical pneumonitis, not an infection).[2]
Complications
- Empyema — pus in the pleural space; drain.
- Lung abscess — a cavitating infection; prolonged antibiotics.
- ARDS — from the severe pneumonia (sepsis-induced permeability oedema).
- Septic shock — the commonest cause of ICU admission and death.
- Metastatic infection — endocarditis, meningitis, septic arthritis.[2]
Red flags
VAP prevention bundle
Ventilator-associated pneumonia is the second commonest nosocomial infection in ICU and adds roughly 4-9 extra days of mechanical ventilation. Prevention is a bundle of evidence-based measures applied together — the incremental benefit of each element compounds, and the bundle is the single most examinable and cost-effective intervention in ventilated patients.[6][2]
- Semirecumbent positioning 30-45 degrees — supine positioning is an independent risk factor for VAP; the supine patient aspirates oropharyngeal secretions around the cuff. Drakulovic showed semirecumbent (45 degrees) reduced VAP from 34% (supine) to 8%.[7] Target 30-45 degrees head-up whenever there is no contraindication (spinal instability, severe hypotension, prone).
- Daily spontaneous awakening trials (SAT) + spontaneous breathing trials (SBT) — paired sedation interruption and weaning reduces days of mechanical ventilation (and therefore VAP risk). The ABC trial (Awakening and Breathing Controlled) paired a daily SAT with a daily SBT and increased ventilator-free days.[8]
- Oral hygiene with chlorhexidine 0.12-0.2% — oropharyngeal colonisation with Gram-negatives precedes VAP; chlorhexidine mouthwash reduces this. Note the 2020 IDSA update advised against chlorhexidine in some populations (possible mortality signal in cardiac surgical patients at higher concentration) — routine oral care with tooth brushing plus chlorhexidine remains standard in general ICU.[6]
- Subglottic secretion drainage (SSD) — using an endotracheal tube with a dedicated suction port above the cuff removes the pooled, colonised secretions that leak past the cuff. Use in patients expected to be intubated over 48-72 hours.[2]
- Hand hygiene and strict aseptic suction technique — the foundation of all infection prevention.
- Peptic ulcer prophylaxis and DVT prophylaxis (stress ulcer + VTE prophylaxis) — part of the original "ventilator bundle"; they reduce stress-related mucosal disease and thromboembolism rather than VAP directly, but are bundled with the VAP measures.
- Avoid unnecessary intubation / use NIV where possible; minimise sedation; early mobilisation; tight glucose control — adjuncts that shorten ventilator days.[2][6]
VAP prevention bundle — apply daily to every ventilated patient
Position 30-45 degrees head-up
Maintain semirecumbent position at all times unless contraindicated (spinal shock, haemodynamic instability, proning). Supine position is an independent VAP risk factor (Drakulovic 1999: VAP 34% supine vs 8% semirecumbent).
Daily SAT + SBT
Perform a daily spontaneous awakening trial (stop sedation) paired with a spontaneous breathing trial. The ABC trial showed this increases ventilator-free days and reduces VAP by shortening time on the ventilator.
Oral care with chlorhexidine + tooth brushing
0.12-0.2% chlorhexidine oral rinse every 8-12 hours plus mechanical tooth brushing. Reduces oropharyngeal colonisation that seeds the lower airway.
Subglottic secretion drainage
Use a suction ET tube (HI-LO Evac) and apply continuous or intermittent suction above the cuff. Reserve for patients expected intubated >48-72 h.
Hand hygiene + closed suction + circuit hygiene
5 moments of hand hygiene, change the ventilator circuit only when soiled/malfunctioning (not routinely), use closed-suction catheters, sterile technique for airway manipulation.
Stress ulcer + DVT prophylaxis
PPI or H2 blocker for stress ulcer prophylaxis; LMWH or mechanical for DVT. These complete the "ventilator bundle".
Minimise sedation, mobilise early, control glucose
De-escalate sedation daily, mobilise when stable, target glucose 6-10 mmol/L. Shortens ventilator days and therefore VAP risk.
Diagnosis of VAP — the diagnostic dilemma
VAP is suspected when a ventilated patient develops a new or progressive infiltrate on chest X-ray plus at least two of: fever over 38 degrees Celsius, leukocytosis or leukopenia, purulent tracheal secretions. The diagnosis is, however, notoriously unreliable on imaging alone — atelectasis, pulmonary oedema, ARDS, and contusion all mimic it. Two philosophies exist:[2][6]
- Clinical (non-invasive) — start antibiotics on clinical grounds, sample tracheal aspirate, and re-evaluate at 48-72 hours; stop antibiotics if cultures are unconvincing and the patient improves. Simpler, but over-treats.
- Invasive / quantitative — bronchoalveolar lavage (BAL) or protected specimen brush (PSB) with quantitative culture thresholds: BAL 10^4 CFU/mL or more, PSB 10^3 CFU/mL or more. More specific; reduces antibiotic exposure. Either strategy is acceptable provided there is a consistent local protocol.[6]
Clinical Pulmonary Infection Score (CPIS)
The CPIS combines six domains (temperature, WBC, tracheal secretions, oxygenation PaO2/FiO2, chest X-ray infiltrate, and semi-quantitative BAL culture) scored 0-2 each. A CPIS over 6 supports VAP; it can also be followed over time — a falling CPIS at day 3 supports stopping antibiotics at 5-7 days. CPIS has only moderate accuracy and should not be the sole basis for the decision.[2]
Clinical strategy
Non-invasive
- Diagnosis on CXR + 2 of fever, leukocytosis, purulent secretions
- Send non-directed tracheal aspirate (qualitative)
- Start empirical antibiotics immediately
- Re-assess and stop at 48-72 h if low probability
- Simpler, fewer bronchoscopy risks; tends to over-treat
Invasive strategy
Quantitative BAL / PSB
- Bronchoscopy for BAL or PSB before antibiotics (or within 24 h)
- Positive threshold: BAL >=10^4 CFU/mL, PSB >=10^3 CFU/mL
- More specific — fewer antibiotic days, less resistance pressure
- Risk of bronchoscopy, sampling error, delay if pre-treatment
- Both strategies acceptable if protocol is consistent locally
Antibiotic duration and de-escalation
The modern mantra is shorter is better — once the patient is clinically responding, prolonged courses do not improve outcomes and drive resistance, Clostridioides difficile, and AKI. The pivotal evidence:[1][3][9]
- CAP — 5 days (minimum) and stop once the patient is clinically stable for 48-72 hours and afebrile. Up to 7 days if slower to resolve (typical CAP: 5-7 days). Atypical pathogens (Legionella, mycoplasma) are covered by the macrolide; Legionella may warrant 7-14 days.[1]
- VAP — 7 days for uncomplicated VAP. The PNEUMA trial randomised VAP to 8 vs 15 days and found no difference in mortality, recurrence, or MDR organisms, but 15-day patients had more antibiotic-free days wasted. Exception: if the organism is non-fermenting Gram-negative (Pseudomonas, Acinetobaster, Stenotrophomonas) or there is bacteraemia, extend to 7-8 days and reassess.[3]
- Procalcitonin-guided — the PRORATA trial showed that a procalcitonin algorithm (stop when procalcitonin falls >80% from peak or below 0.5 ng/mL) reduced antibiotic days in ICU without increasing mortality; the Schuetz meta-analysis confirms safety across lower respiratory tract infections. Useful as a decision aid to stop antibiotics, not to start them.[9][10]
PNEUMA (Chastre)
JAMA 2003
401 pts with VAP — 8 vs 15 days of antibiotics
Key finding
No difference in mortality (18.8% vs 17.2%), recurrence, or MDR emergence. 15-day arm had fewer antibiotic-free days (benefit to short course).
Practice change
7-8 days of therapy for uncomplicated VAP became standard; extend only for non-fermenting Gram-negatives
PRORATA (Bouadma)
Lancet 2010
621 ICU patients — procalcitonin-guided stop vs standard duration
Key finding
Reduction in number of antibiotic-free days within 28 days (14.3 vs 8.9, p<0.0001). No excess 28-day or 60-day mortality.
Practice change
Procalcitonin algorithms used as a stop tool to shorten antibiotic courses in ICU and LRTI
Drakulovic (semirecumbent)
Lancet 1999
86 intubated patients — supine vs semirecumbent (45 deg) positioning
Key finding
VAP: 34% supine vs 8% semirecumbent (p=0.003). Supine position an independent risk factor.
Practice change
Head-up 30-45 degrees became a core element of the VAP prevention bundle
ABC trial (Girard)
Lancet 2008
336 mechanically ventilated pts — paired daily SAT+SBT vs usual care + SBT
Key finding
More ventilator-free days (14.7 vs 11.6, p=0.02) and ICU-free days; no increase in self-extubation. Reduced time on ventilator.
Practice change
Pairing daily spontaneous awakening trials with spontaneous breathing trials became standard to accelerate weaning and reduce VAP
Metlay (ATS/IDSA CAP)
Am J Respir Crit Care Med 2019
Joint ATS/IDSA clinical practice guideline for CAP in adults
Key finding
Recommends beta-lactam + macrolide or respiratory fluoroquinolone for inpatient CAP; routine 5-day minimum duration with clinical stability; empiric MRSA/Pseudomonas cover only with risk factors.
Practice change
Standardised empiric CAP regimens, severity-stratified disposition, and de-escalation guidance
Kalil (IDSA/ATS HAP-VAP)
Clin Infect Dis 2016
IDSA/ATS clinical practice guideline for HAP and VAP in adults
Key finding
Recommend empiric cover based on MDR risk factors and local antibiogram; anti-pseudomonal beta-lactam +/- second agent + MRSA cover when indicated; 7-day default duration.
Practice change
Antibiogram-driven, MDR-risk-stratified empiric therapy with 7-day de-escalation for HAP/VAP
Empiric therapy at a glance
Severe CAP (ICU)
No MDR risk
- Ceftriaxone 2 g IV daily PLUS azithromycin 500 mg IV daily
- Alternative: respiratory fluoroquinolone (moxifloxacin) + beta-lactam
- Add vancomycin/linezolid if MRSA suspected (cavitary, post-influenza)
- Add oseltamivir if influenza suspected (do not wait for PCR)
- Duration: 5 days minimum, stop once clinically stable 48-72 h
Late VAP
MDR risk
- Piperacillin-tazobactam 4.5 g IV q6h (or cefepime, ceftazidime, meropenem)
- PLUS vancomycin 15-20 mg/kg q8-12h (AUC-guided) or linezolid for MRSA
- Consider second Gram-negative agent (amikacin/levofloxacin) if high MDR risk
- Sample lower airway (BAL/PSB) before or within 24 h of first dose
- De-escalate at 48-72 h; total 7 days unless non-fermenting GN
MDR risk factors (modify empiric cover)
For VAP, risk factors for multidrug-resistant pathogens that mandate broadened cover are:[6]
- Prior intravenous antibiotics within 90 days.
- Septic shock at VAP onset or ARDS accompanying VAP.
- Five or more days in hospital prior to VAP onset (i.e. late-onset).
- Acute renal replacement therapy prior to VAP onset.
MRSA-specific risk factors (warrant empiric vancomycin/linezolid): prior IV antibiotics, known MRSA colonisation, hospital unit with high MRSA prevalence, and (for CAP) post-influenza or cavitary picture.[7]
Pseudomonas-specific risk factors for CAP (rare — structural lung disease, bronchiectasis, frequent steroids/antibiotics in severe COPD): warrant an anti-pseudomonal beta-lactam in the CAP regimen.[1]
CAP organisms
Community
- Streptococcus pneumoniae (commonest overall)
- Haemophilus influenzae, Moraxella catarrhalis
- Atypicals: Mycoplasma, Chlamydia, Legionella
- Respiratory viruses: influenza, RSV, SARS-CoV-2
- Modifiers: COPD -> Pseudomonas; aspiration -> anaerobes; immunocompromise -> PJP
Early HAP/VAP
Under 4 days
- Streptococcus pneumoniae
- Haemophilus influenzae
- Methicillin-sensitive Staphylococcus aureus (MSSA)
- Usually antibiotic-sensitive; cover as for severe CAP
- Anti-pseudomonal beta-lactam reasonable if ventilated
Late VAP
After 4 days / MDR risk
- Pseudomonas aeruginosa (the key ICU pathogen)
- Acinetobacter baumannii (often extremely drug-resistant)
- Klebsiella / Enterobacter with ESBL or CRE
- MRSA (esp. post-viral, IV drug use)
- Stenotrophomonas maltophilia (inherently resistant, needs TMP-SMX)
CURB-65 and severity — the exam decision tool
CURB-65 (Lim 2003, Thorax) stratifies CAP into mortality risk and disposition:[4]
- Confusion (disorientation in time/place/person).
- Urea > 7 mmol/L.
- Respiratory rate >= 30/min.
- Blood pressure — SBP < 90 or DBP <= 60 mmHg.
- 65 — age 65 years or older.[4]
| Score | Mortality | Disposition |
|---|---|---|
| 0-1 | Low (1.5%) | Outpatient |
| 2 | Moderate (9.2%) | Hospital (ward) |
| 3-5 | High (22-57%) | Consider ICU |
The PSI/PORT (Fine 1997, NEJM) is a more granular 20-variable model that is more sensitive for identifying low-risk patients but is more cumbersome; IDSA/ATS minor criteria (three or more) or one major criterion (need for invasive ventilation or septic shock needing vasopressors) is the trigger for ICU admission.[5][1]
Severe CAP — from presentation to de-escalation
Assess severity
CURB-65 and IDSA/ATS criteria. ICU if CURB-65 >=3 or 1 major (invasive ventilation, septic shock) or >=3 minor (RR >=30, P/F <=250, multilobar, confusion, BUN >=20, WBC <4, T<36, hypotension needing fluids).
Obtain cultures BEFORE antibiotics
Blood cultures x2, sputum/Gram stain, urinary antigens (pneumococcal, Legionella), respiratory viral PCR (influenza/COVID). Do NOT delay antibiotics in septic shock — draw within 1 h.
Start empiric therapy within 1 hour
Ceftriaxone 2 g IV daily + azithromycin 500 mg IV daily. Add vancomycin/linezolid if MRSA risk. Add oseltamivir if influenza. Give the first dose in ED.
Reassess at 48-72 hours
Review cultures, clinical course (fever, WBC, oxygenation, haemodynamics). If stable and afebrile for 48-72 h and organism identified, de-escalate to targeted therapy.
Decide duration
Minimum 5 days, stop once clinically stable for 48-72 h. Use procalcitonin as an aid to stop. Atypicals/Legionella may need 7-14 days. Bacteraemic Staph aureus or Pseudomonas: longer.
Exam practice
SAQ — Severe community-acquired pneumonia with ARDS
10 minutes · 10 marks
A 62-year-old man with type 2 diabetes and a 40 pack-year smoking history presents in mid-winter with a 3-day history of fever, rigors, productive cough, and progressive dyspnoea. He was treated by his GP with oseltamivir for a flu-like illness 5 days ago. On arrival: GCS 14 (E3V4M6), temperature 39.2°C, HR 128, BP 78/46 (MAP 57), RR 38, SpO2 88% on a 15 L non-rebreather mask. Crackles throughout the right lung. Arterial blood gas on 15 L: pH 7.28, PaO2 71 mmHg, PaCO2 34 mmHg, lactate 4.2 mmol/L. WCC 24.6, urea 12, sodium 130. Chest X-ray shows dense right upper and lower lobe consolidation with bilateral patchy change; CURB-65 4.
SAQ — Ventilator-associated pneumonia: diagnosis and management
10 minutes · 10 marks
A 68-year-old man is intubated and ventilated in ICU, day 7 of an admission for a ruptured abdominal aortic aneurysm repair complicated by prolonged intraoperative hypotension and acute kidney injury requiring continuous veno-venous haemofiltration. He received piperacillin-tazobactam for 5 days for a catheter-associated urinary tract infection. He now develops a fever (38.9°C), thick purulent endotracheal secretions needing frequent suctioning, and a rising FiO2 requirement (0.4 to 0.6). WCC 19.2, CRP 180, procalcitonin 3.4. Chest X-ray shows a new right lower lobe infiltrate. He is on noradrenaline 0.15 mcg/kg/min for a MAP of 64.
Clinical pearls — high-yield for the exam
Red flags — don't miss these
References
- [1]Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. American Journal of Respiratory and Critical Care Medicine, 2019.PMID 31573350
- [2]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [3]Chastre J, Wolff M, Fagon JY, Chevret S, et al. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial (PNEUMA). JAMA, 2003.PMID 14625336
- [4]Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study (CURB-65). Thorax, 2003.PMID 12728155
- [5]Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia (Pneumonia Severity Index / PORT). New England Journal of Medicine, 1997.PMID 8995086
- [6]Kalil AC, Metersky ML, Klompas M, et al. Executive Summary: Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the IDSA and ATS. Clinical Infectious Diseases, 2016.PMID 27521441
- [7]Drakulovic MB, Torres A, Bauer TT, et al. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients. Lancet, 1999.PMID 10584721
- [8]Girard TD, Kress JP, Fuchs BD, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial). Lancet, 2008.PMID 18191684
- [9]Bouadma L, Luyt CE, Tubach F, et al. Use of procalcitonin to reduce patients' exposure to antibiotics in intensive care units (PRORATA trial). Lancet, 2010.PMID 20097417
- [10]Schuetz P, Wirz Y, Sager R, et al. Procalcitonin guidance in patients with lower respiratory tract infections: a systematic review and meta-analysis. Clinical Chemistry and Laboratory Medicine, 2018.PMID 29715176