ICU · Airway management
Aspiration — Prevention & Management (Pneumonitis vs Pneumonia)
Also known as Aspiration · Aspiration pneumonitis · Mendelson syndrome · Aspiration pneumonia · Ventilator-associated pneumonia · VAP prevention · Subglottic suction · Semi-recumbent position · Post-extubation dysphagia · Chemical pneumonitis · Cuff pressure monitoring · Silent aspiration
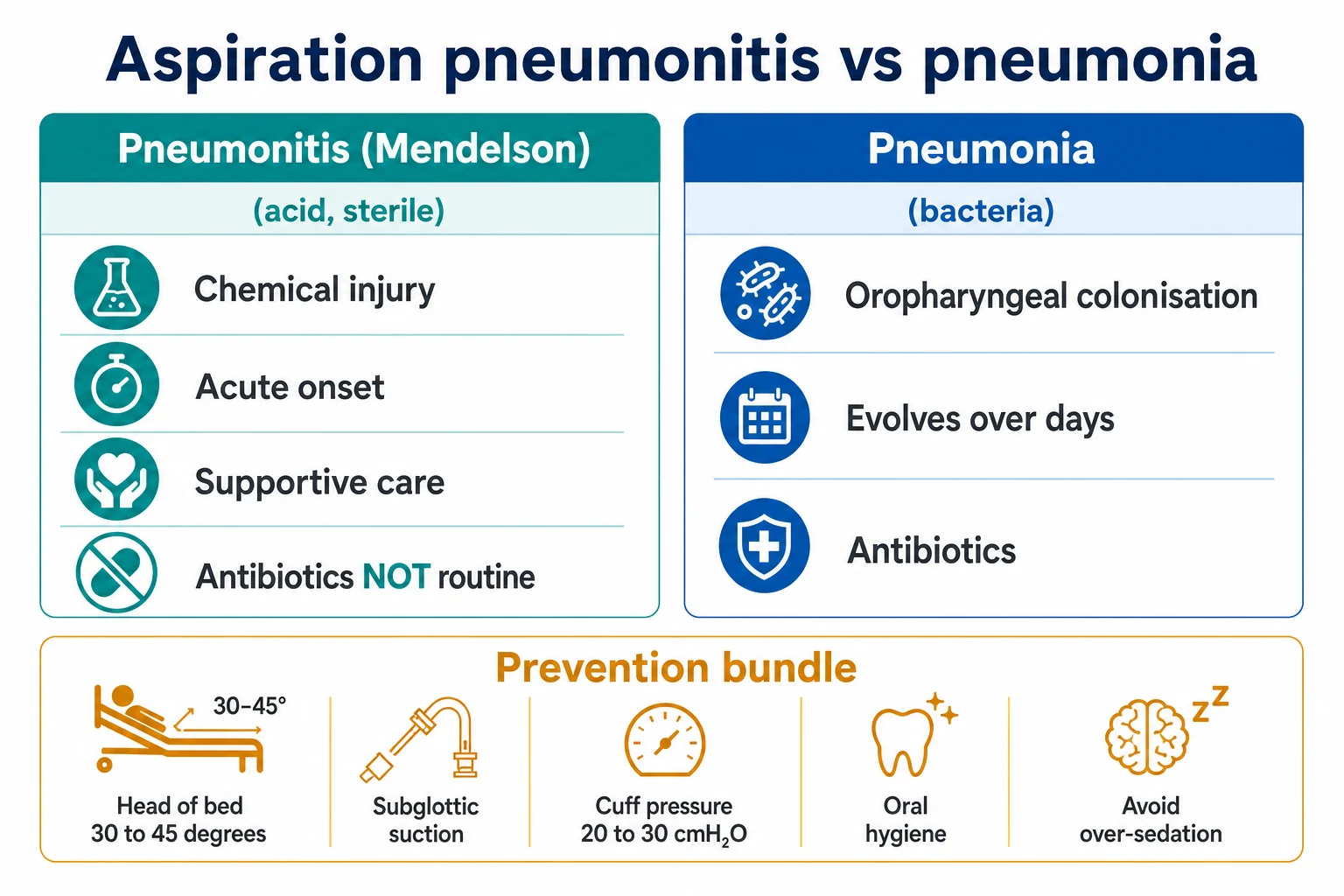
Aspiration causes two distinct syndromes. Aspiration pneumonitis (Mendelson syndrome) is a sterile chemical injury from acidic gastric contents — treated with supportive care (oxygen, positive pressure, bronchodilators), with antibiotics and corticosteroids NOT given routinely. Aspiration pneumonia is an infection from aspiration of colonised oropharyngeal secretions (the elderly, dysphagia, poor dentition, reduced consciousness) — treated with antibiotics. The distinction drives treatment. Prevention is the VAP bundle: head of bed 30-45 degrees (Drakulovic, Lancet 1999), subglottic suction, cuff pressure 20-30 cmH2O, oral hygiene, minimal sedation, and post-pyloric feeding for the high-risk patient. Proton pump inhibitors for stress ulcer prophylaxis have NO mortality benefit (SUP-ICU, Krag NEJM 2018).
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
Aspiration is the entry of material into the airway below the vocal cords. It causes two distinct syndromes that share a name but differ fundamentally in treatment:[2]
- Aspiration pneumonitis (Mendelson syndrome) — a sterile chemical lung injury from aspiration of sterile, acidic gastric contents.
- Aspiration pneumonia — an infective pneumonia from aspiration of colonised oropharyngeal secretions.
The distinction drives treatment: the first is managed supportively without routine antibiotics or steroids; the second needs antibiotics.[2][4]
Micro-aspiration is the term used for the small-volume, often clinically silent leakage of oropharyngeal or gastric secretions past the endotracheal tube cuff in the intubated patient. It is the proximate mechanism for most ventilator-associated pneumonia (VAP), and the entire VAP-prevention bundle is fundamentally a micro-aspiration prevention bundle.[3][9] Macro-aspiration is a witnessed or large-volume event — vomiting, regurgitation, or a contents seen in the airway — and is the classical setting for Mendelson syndrome.

Pathophysiology — the shared mechanism
All aspiration syndromes begin with failure of the airway protective reflexes — the gag reflex, the cough reflex, glottic closure, and the swallow-breathe coordination of the larynx. In the healthy awake adult these reflexes prevent any significant volume from crossing the vocal cords. Aspiration occurs when one or more of these is impaired (depressed consciousness, neuromuscular disease, prolonged intubation), or when a volume overwhelms a competent reflex (massive vomiting during a rapid sequence induction).[4][5]
What happens next depends almost entirely on what is aspirated:[4]
- Sterile, acidic gastric contents (pH less than 2.5) — the acid burns the bronchial and alveolar epithelium directly, within seconds producing epithelial denudation, capillary leak, surfactant inactivation, and a non-cardiogenic pulmonary oedema / ARDS picture. This is chemical pneumonitis — initially sterile; infection is a later, secondary, and not inevitable, event.[2][4]
- Colonised oropharyngeal secretions — the inoculum is the bacterial load of the mouth (anaerobes, streptococci) rather than the pH of the material. The insult is infective from the outset, and the injury evolves over days as a pneumonia rather than within hours as a chemical burn.[4][5]
- Particulate matter — a food particle, a fragment of a tablet, a tooth, or a piece of a dental appliance obstructs a bronchus, producing atelectasis and a post-obstructive pneumonia that will not resolve until the particle is removed by bronchoscopy.[2]
- Neutral / non-acidic gastric contents (the patient on a proton pump inhibitor, or with food in the stomach) — produce a less dramatic chemical injury but a heavier bacterial inoculum, blurring the pneumonitis/pneumonia distinction.[4]
The dependent segments are preferentially affected because aspirated liquid flows to gravity-dependent lung: in the supine patient these are the posterior segments of the upper lobes and the apical segments of the lower lobes; in the upright patient the basal segments of the lower lobes.[2]
Risk factors for aspiration
Aspiration risk is the product of impaired airway protection multiplied by the likelihood of having material in the pharynx or stomach to aspirate. The classic Fellowship viva expects you to list risk factors under these two headings, and then to map each to a specific prevention measure.[4][5]
Impaired airway protection (impaired consciousness or impaired laryngeal / swallow function)
- Decreased Glasgow Coma Scale (GCS) — the single most powerful risk factor. The cough and gag reflexes are progressively lost as GCS falls; clinically, a GCS of 8 or below is the threshold at which the airway is considered unprotected and intubation is offered. The overdose patient, the post-ictal patient, the post-cardiac-arrest patient, and the intoxicated patient all aspirate through this mechanism.[2][4]
- Stroke and neurodegenerative disease — dysphagia is the mechanism. Up to 50-80% of stroke patients have some aspiration on instrumental assessment, and aspiration pneumonia is the leading cause of death after stroke. Brainstem strokes (lateral medullary syndrome) and bilateral hemisphere strokes are the highest risk.[4][11]
- Neuromuscular disease — myasthenia gravis, Guillain-Barre syndrome, amyotrophic lateral sclerosis (ALS), and muscular dystrophy weaken the muscles of mastication, swallow, and cough; the bulbar variants are particularly dangerous.[5]
- Dementia, frailty, and old age — sarcopenia of the swallowing muscles, poor dentition, reduced cough force, and institutionalisation combine; aspiration pneumonia is the most common cause of death in advanced dementia.[4][11]
- Anaesthesia and sedation — the induction agent abolishes consciousness and the muscle relaxant abolishes laryngeal closure; this is exactly the window during which the protective laryngeal reflexes are lost and the reason a rapid sequence induction (RSI) with cricoid pressure and pre-oxygenation exists.[2][4]
- Prolonged intubation / tracheostomy — the tube splints the glottis open, the cuff prevents glottic closure, and prolonged intubation produces laryngeal oedema and sensory neuropathy that persist after extubation (post-extubation dysphagia).[2]
- Critical illness per se — even without sedation, the critically ill patient has blunted cough, reduced mucociliary clearance, recumbency, gastric and bowel dysmotility, and an oropharynx that becomes colonised with Gram-negatives within days of admission.[3][9]
Increased likelihood of material in the pharynx or stomach
- Gastro-oesophageal reflux disease (GORD/GERD) and hiatus hernia — a competent lower oesophageal sphincter is the backstop against regurgitation; an incompetent one allows gastric contents into the pharynx, especially when supine.[4]
- Gastric over-distension / high gastric volume — ileus, bowel obstruction, delayed gastric emptying (opioids, diabetes, critical illness), and over-aggressive gastric feeding all raise the volume available to be aspirated and the pressure driving it proximally.[2]
- Obesity and pregnancy — both raise intra-abdominal pressure, both delay gastric emptying, and pregnancy additionally raises progesterone-mediated sphincter tone reduction; the parturient is the classical high-risk aspiration patient (Mendelson's original 1946 case series was of obstetric anaesthesia).[4]
- Bowel obstruction and upper GI bleeding — a stomach full of blood or faeculent material is a particularly dangerous aspirate, both for volume and for bacterial load.[2]
- Feeding tubes — a misplaced (intrathoracic/intrabronchial) nasogastric tube delivers feed directly into the lung; even a correctly sited gastric tube can cause reflux and micro-aspiration, particularly if the patient is supine and over-fed.[14]
- Poor oral hygiene and poor dentition — raise the bacterial inoculum of any aspirated material and shift the oropharyngeal flora toward anaerobes and Gram-negatives, converting a chemical pneumonitis into a bacterial pneumonia.[5][11]
Aspiration pneumonitis (Mendelson syndrome)
Aspiration of sterile, acidic gastric contents (pH below about 2.5, a large volume) causes an acute chemical burn of the bronchial and alveolar epithelium, with capillary leak, surfactant disruption, and an ARDS-like picture.[2][4] The injury is biphasic: an immediate chemical burn (the first 1-2 hours) followed by a neutrophil-driven inflammatory cascade (12-24 hours) that produces the capillary leak and hypoxaemia. Curtis Mendelson described the syndrome in 1946 in an obstetric anaesthesia case series; the pH threshold of 2.5 and the volume threshold of about 0.3-0.4 mL/kg of body weight are the classical (Robert & Shirley) experimental benchmarks, though both have been challenged — neutralisation of gastric pH by a proton pump inhibitor converts a chemical pneumonitis into a heavier bacterial pneumonia without abolishing the aspiration risk.[4]
- Clinical: acute onset, within hours, of dyspnoea, cough, wheeze, bronchospasm, and hypoxaemia, often a low-grade fever; a witnessed regurgitation or vomiting event in an obtunded patient (overdose, post-ictal, post-cardiac arrest, anaesthetic aspiration).[2][4]
- Imaging: pulmonary infiltrates, typically in the dependent segments — in the supine patient, the posterior segments of the upper lobes and the apical segments of the lower lobes.[2]
- Treatment: supportive — oxygen, lung-protective ventilation with PEEP for the severe case, bronchodilators for bronchospasm, and fluid management. Antibiotics are not given routinely (the insult is initially sterile); they are added only if infection develops or is strongly suspected. Corticosteroids are not recommended (no benefit, possible harm — Wolfe 1977 and multiple subsequent studies). Bronchoscopy is reserved for suspected particulate obstruction, not for simple liquid acid aspiration.[2][4][10]
The natural history is rapid — within 6-12 hours the patient has either stabilised on supportive care or progressed to frank ARDS needing lung-protective ventilation. A patient who is deteriorating after 48 hours is no longer having a pure chemical pneumonitis; this is the signal to revisit the diagnosis, add antibiotics, and look for a superimposed infection or a missed particulate obstruction.[4][5]
Aspiration pneumonia
Aspiration of colonised oropharyngeal contents causes a bacterial pneumonia. Risk factors: reduced consciousness, dysphagia (stroke, neurodegenerative disease), poor dentition, alcoholism, and prolonged intubation.[2][5] The inoculum is the oropharyngeal flora, so the microbiology is that of the mouth, not of the lung or the stomach.
- Clinical: a more gradual onset over days, with fever, purulent sputum, and infiltrates in dependent segments; often a putrid sputum odour (anaerobes).[2][4]
- Imaging: patchy or confluent infiltrates in dependent segments; necrotising infection may cavitate (classically with anaerobes), producing a lung abscess or an empyema if the pleura is breached.[5]
- Treatment: antibiotics directed at the oral flora (see Antibiotic strategy, below), plus supportive care.[4][5]
Microbiology of aspiration pneumonia
Aspiration pneumonia is a mixed infection of the oral flora — polymicrobial, with anaerobes and streptococci dominating. The microbiology differs from that of a typical community-acquired pneumonia (pneumococcus, Haemophilus) and from a hospital-acquired pneumonia (Gram-negatives, MRSA), and this drives the antibiotic choice.[4][5][11]
[1]A pure Mendelson syndrome is sterile; a patient who has been in hospital for days, has poor dentition, or has had repeated aspiration episodes is aspirating a heavily colonised inoculum and should be treated for aspiration pneumonia from the outset rather than observed.[4][5]
The key distinction
| Feature | Aspiration pneumonitis (Mendelson) | Aspiration pneumonia |
|---|---|---|
| Mechanism | Sterile acidic gastric contents — chemical burn | Colonised oropharyngeal secretions — bacterial infection |
| Onset | Acute, within hours of the event | Gradual, over days |
| Setting | Witnessed vomiting/regurgitation in an obtunded patient (anaesthesia, overdose, post-arrest, post-ictal) | Dysphagia, stroke, dementia, poor dentition, alcoholism, prolonged intubation |
| Fever | Low-grade, early | High, with rigors |
| Sputum | Scant; not purulent | Purulent; classically putrid (anaerobes) |
| CXR pattern | Dependent-lobe infiltrates, bilateral, within hours | Dependent-lobe infiltrates; may cavitate or form abscess/empyema |
| Initial treatment | Supportive (oxygen, PEEP, bronchodilators); no routine antibiotics, no steroids | Antibiotics (cover oral anaerobes and streptococci) + supportive care |
| Course | Often resolves in 24-48 h on supportive care; progression after 48 h suggests superimposed infection | Responds over days to antibiotics; abscess/empyema are complications |
The common error is giving antibiotics to every aspiration — for a pure chemical pneumonitis they are not needed initially, and over-use drives resistance. Reserve them for signs of infection (progressive infiltrates, purulent sputum, rising inflammatory markers, risk factors for bacterial colonisation).[2][4]
In practice the distinction is often blurred: the patient who aspirates in the ICU has often been colonised, is intubated, and has poor dentition, so a pragmatic approach is to withhold antibiotics initially for a witnessed, clearly chemical aspiration in a previously well patient, observe closely, and start antibiotics at 48 hours if there is no improvement or sooner if infection declares itself.[4][5]
Antibiotic strategy — when, what, and for how long
When to start
- Do NOT start antibiotics routinely for a witnessed aspiration of clear acidic gastric contents in a previously well patient with a clean chest — this is a chemical pneumonitis and will resolve with supportive care.[2][4]
- Do start antibiotics immediately if there is any of: purulent sputum, progressive infiltrates at 48 hours, a small inoculum in a colonised patient (ICU, nursing home, prolonged intubation, poor dentition), abscess or empyema on imaging, or a febrile, septic presentation.[4][5]
- A useful pragmatic rule: re-assess at 48 hours — if the patient has not improved on supportive care alone, start antibiotics for presumed superimposed infection.[4]
What to give
[5]Duration
- 5-7 days for uncomplicated aspiration pneumonia that responds promptly.[5]
- Longer (2-6 weeks) for necrotising infection, lung abscess, or empyema — these need source control (drainage) and prolonged anaerobic cover.[5]
- De-escalate to oral amoxicillin-clavulanate or clindamycin once the patient is afebrile, clinically improving, and able to take oral intake.
Particulate aspiration
Aspiration of particulate matter (food debris, a foreign body, a tooth) can obstruct a bronchus, causing atelectasis and a post-obstructive pneumonia, and is not cleared by coughing or supportive care alone. Suspect it with a localised wheeze, segmental collapse, or failure to improve, and remove it with bronchoscopy.[2] Bronchoscopy is also indicated to clear retained secretions if aspiration of thick particulate material is witnessed, even if a foreign body is not seen — the goal is to physically remove the particulate matter that the mucociliary escalator cannot. Lavage with large volumes of saline is not recommended for acid aspiration as it simply pushes the injurious material distally; suction the visible material and stop.[2][4]
Prevention — the VAP/aspiration bundle
Prevention is the mainstay, because treatment of established aspiration is limited. The bundle reduces both aspiration and ventilator-associated pneumonia:[1][3][9]
- Head of bed elevated 30-45 degrees (semi-recumbent) — the landmark randomised trial (Drakulovic, Lancet 1999) showed that supine positioning is a risk factor for nosocomial pneumonia in mechanically ventilated patients, and semi-recumbency reduces it.[1]
- Subglottic suction — an endotracheal tube with a subglottic drainage port removes the secretions that pool above the cuff and would otherwise be aspirated.[3][8]
- Cuff pressure 20-30 cmH2O — high enough to prevent leak of secretions past the cuff, low enough to avoid mucosal ischaemia. Measure and document regularly (every 8-12 hours), because cuff pressure drifts down with time, with nitrous oxide diffusion, and with patient movement.[3][9]
- Oral hygiene (with chlorhexidine in selected populations) and good dental care to reduce oropharyngeal bacterial load.[3][7]
- Minimise sedation and daily sedation interruption; maintain a good cough and airway-reflex tone.[3]
- Enteral feeding: avoid gastric over-distension; use a post-pyloric (jejunal) tube for the patient at very high aspiration risk.[2][14]
- Rapid sequence induction for intubation (to prevent aspiration during the intubation itself) and suction above the cuff before extubation.[2]
- A swallow assessment before resuming oral intake after prolonged intubation or tracheostomy (post-extubation dysphagia is common).[2]
- Stress ulcer prophylaxis is NOT a prevention measure for aspiration — keep the gastric pH acidic to suppress bacterial overgrowth; pantoprazole has no mortality benefit in the general ICU population (SUP-ICU, Krag NEJM 2018).[12][13]
Prevention deep-dive — the evidence, and where it cuts against intuition
Head of bed elevation. Drakulovic (Lancet 1999) randomised 86 mechanically ventilated patients to semi-recumbent (45 degrees) versus supine positioning; suspected VAP was 8% versus 34% and confirmed VAP 5% versus 23%, with the supine position and enteral nutrition as independent risk factors.[1] This is the single most cited prevention paper in ICU. The intervention is free, immediate, and reversible — the only contraindication is hypotension/shock, spinal precautions, or a specific procedural need.
Subglottic secretion drainage. A specialised endotracheal tube with a dorsal suction port above the cuff continuously removes the pooled secretions that would otherwise leak past the cuff in the folds of the inflated cuff. Bouza (Chest 2008) in a randomised trial of 690 cardiac-surgery patients showed a roughly halved incidence of VAP with continuous aspiration of subglottic secretions (CASS).[8] Meta-analyses confirm a VAP reduction and a shorter time to first extubation; cost-effectiveness is best when the expected duration of ventilation is more than 48-72 hours.[3]
Cuff pressure monitoring. Secretions leak past the cuff through longitudinal folds that form in even a correctly inflated cuff, and the leak is proportional to cuff pressure being too low. Target 20-30 cmH2O: below 20 cmH2O the leak of pooled secretions rises sharply; above 30 cmH2O the risk of tracheal mucosal ischaemia, ulceration, and later stenosis rises. Check with a handheld manometer every 8-12 hours and after any position change or nitrous oxide exposure.[3][9]
Oral hygiene — the chlorhexidine controversy. The intuition that an antiseptic mouthwash should reduce VAP by reducing oropharyngeal bacterial load is only partly borne out. Labeau (Lancet Infect Dis 2011) showed oral antiseptics reduce VAP in observational and trial data, but Klompas (JAMA Intern Med 2014) reappraised routine chlorhexidine and found no mortality benefit and a possible signal toward increased mortality in some subgroups — leading several guidelines to retreat from universal chlorhexidine to a selective (cardiac surgery, selected ICU) recommendation.[6][7] The current consensus is mechanical oral care (toothbrushing) for all, plus chlorhexidine in selected populations (post-cardiac-surgery), and not routine chlorhexidine for all ICU patients.
Proton pump inhibitors — no mortality benefit, and a risk. The SUP-ICU trial (Krag, NEJM 2018) randomised 3298 ICU patients with one or more risk factors for GI bleeding to pantoprazole versus placebo and found no difference in 90-day mortality (31% vs 32%); the only signal was a reduction in clinically important bleeding (2.5% vs 4.2%) in the highest-risk subgroup, at the cost of more C. difficile infection. The Alhazzani network meta-analysis confirms that stress-ulcer prophylaxis reduces bleeding but does not reduce mortality.[12][13] Furthermore, raising gastric pH promotes gastric bacterial overgrowth, which paradoxically increases the bacterial inoculum if the patient does aspirate — converting a sterile chemical pneumonitis into a bacterial pneumonia. The lesson for the viva: PPIs do not prevent aspiration, they do not improve survival, and they may worsen the aspirate — reserve them for patients with a genuine indication (active ulcer, upper GI bleed, dual anti-platelet therapy with a proven ulcer).[12]
[3]Special populations
The obstetric / anaesthetic patient
Mendelson's original 1946 case series was of obstetric anaesthesia, and the parturient remains the prototype high-risk aspiration patient: raised intra-abdominal pressure, delayed gastric emptying, progesterone-mediated lower oesophageal sphincter relaxation, and an often-difficult airway.[4] Prevention is the rapid sequence induction with pre-oxygenation and cricoid pressure (its evidence base is contested, but it remains standard where aspiration risk is high), a cuffed endotracheal tube, and a careful extubation once fully awake with reflexes returned. The pharmacological adjuncts (H2-blocker, sodium citrate, metoclopramide) reduce gastric volume and raise gastric pH but do not abolish the risk and are secondary to airway protection.
The stroke patient
Stroke is one of the commonest causes of aspiration pneumonia in any ICU or stroke unit. Dysphagia screening (a bedside swallow screen, then formal assessment by speech-language pathology with videofluoroscopy or fibre-optic endoscopic evaluation of swallow, FEES) is mandatory in the first few hours.[11] NPO until the screen is passed; a texture-modified diet and fluid thickeners for those who fail; and a high index of suspicion for silent aspiration. Pharmacological prevention (ACE-inhibitors, amantadine, cilostazol) has been studied but the evidence is weak and inconsistent.[11]
The intubated / tracheostomised patient
The endotracheal tube cuff is the principal barrier but it is imperfect: it leaks via longitudinal folds, and it splints the glottis open and abolishes the cough and glottic-closure reflexes. This is the population in whom the VAP bundle in its entirety (HOB elevation, subglottic suction, cuff pressure, oral care, sedation interruption, SAT/SBT) earns its keep.[3][9] For the tracheostomised patient the same applies, with the added caveat that the tracheostomy cuff, when deflated for speech or swallowing, is itself a window for aspiration — assess swallow with the cuff deflated (often with a speaking valve/Passy-Muir) before resuming oral intake.
The critically ill patient on enteral feeding
Feed-related aspiration is reduced by: gastric rather than bolus feeding where possible, checking gastric residual volumes (though the value of this is debated), prokinetics (metoclopramide, erythromycin) for gastroparesis, and a post-pyloric (jejunal) tube for the patient with proven reflux, gastroparesis, or recurrent aspiration despite gastric feeding and HOB elevation.[2][14] Always radiologically confirm nasogastric tube position before the first feed — intrabronchic placement is a preventable and occasionally fatal error.[14]
Diagnosis and investigation
The diagnosis of an aspiration event is usually clinical and contextual: an obtunded patient with witnessed vomiting or regurgitation who then develops hypoxaemia and dependent-lobe infiltrates. There is no single confirmatory test, but a structured workup clarifies the syndrome and rules out mimics.[4][5]
- Arterial blood gas — hypoxaemia is the cardinal finding; type 1 respiratory failure, often with a widened A-a gradient. A respiratory or mixed acidosis suggests severe disease or fatigue.
- Chest X-ray — dependent-lobe infiltrates within hours (pneumonitis) or evolving over days (pneumonia); look for cavitation (anaerobes), pleural effusion/empyema, or segmental collapse (particulate obstruction).
- Bloods — FBC (leucocytosis), CRP and procalcitonin (rising inflammatory markers at 48 hours favour infection and antibiotics), electrolytes, and a lactate (sepsis).
- Sputum and blood cultures — before antibiotics if possible, but do not delay antibiotics in the septic patient. In the intubated patient, a tracheal aspirate or bronchoalveolar lavage samples the lower respiratory tract.
- Bronchoscopy — for suspected particulate obstruction, for retained secretions, or to obtain BAL for microbiology; NOT a routine diagnostic test for simple liquid aspiration.[2][4]
- CT chest — if cavitation, abscess, empyema, or an underlying lesion is suspected, or if the CXR is inconclusive.
Differential diagnosis includes cardiogenic pulmonary oedema, ARDS from another cause, atelectasis, pulmonary embolism, and a primary bacterial pneumonia — and several can coexist in the critically ill patient.[5]
Management of an acute aspiration event
Acute macro-aspiration event — the first 30 minutes
1. Position and suction
Head down (Trendelenburg), turn the patient onto their side (recovery position if not intubated), and suction the oropharynx and upper airway under direct vision. The aim is to physically remove the aspirated material from the airway before it reaches the distal bronchi.
2. Intubate and ventilate if the airway is unprotected
If GCS is 8 or below, or the patient cannot protect their airway or is failing ventilation, perform a rapid sequence induction and intubate with a cuffed tube. Use lung-protective ventilation (tidal volume 6 mL/kg ideal body weight, plateau pressure under 30 cmH2O) with PEEP titrated to oxygenation for the chemical lung injury.
3. Bronchoscopy ONLY for particulate obstruction
Suction the visible material, but do not lavage with large volumes of saline — this pushes the injurious liquid distally. Reserve bronchoscopy for suspected particulate matter, a localised wheeze or segmental collapse, or failure to clear secretions.<Cite id="2" />
4. Supportive care — oxygen, bronchodilators, fluids
High-flow oxygen to target SpO2 92-96% (88-92% in COPD). Salbutamol for bronchospasm. Cautious IV fluids — the chemical injury causes capillary leak, so a positive fluid balance worsens pulmonary oedema; titrate to perfusion.
5. Do NOT give antibiotics or corticosteroids routinely
For a pure chemical pneumonitis (Mendelson), antibiotics do not alter the early course and drive resistance, and corticosteroids have shown no benefit and possible harm (Wolfe 1977 and subsequent). Add antibiotics only if infection develops or is strongly suspected (purulent sputum, progressive infiltrates at 48 hours, colonised patient).<Cite id="4" /><Cite id="10" />
6. Re-assess at 48 hours
If the patient has not improved on supportive care alone, start antibiotics for presumed superimposed infection, repeat the CXR, and look for a missed particulate obstruction, abscess, or empyema. The 48-hour checkpoint is the single most important decision point in managing a chemical pneumonitis.<Cite id="4" />
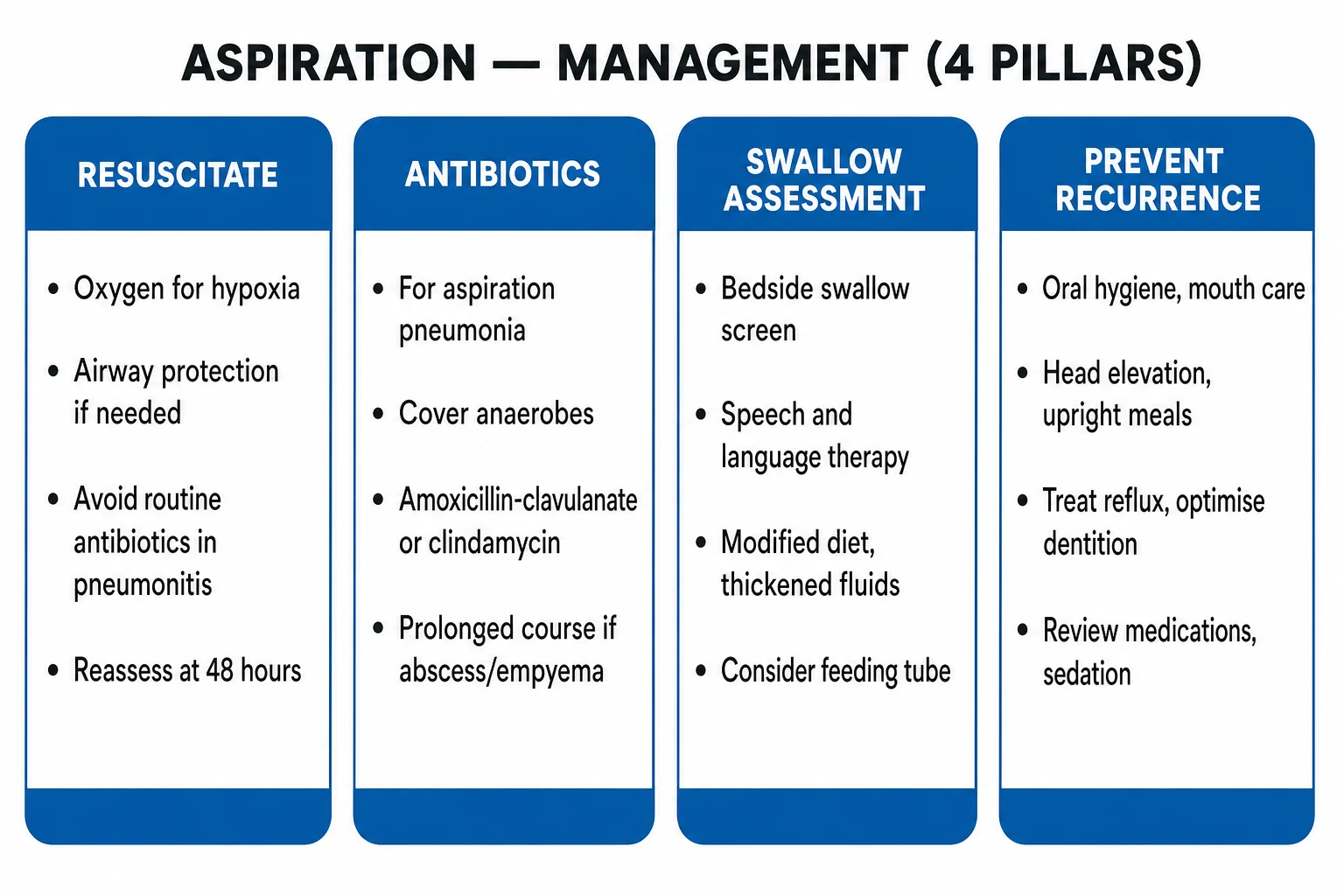
- Position and suction — head down, turn the patient onto their side, and suction the oropharynx and upper airway.
- Intubate and ventilate if the airway is unprotected or ventilation is failing (lung-protective ventilation with PEEP for the chemical lung injury).
- Bronchoscopy only if particulate obstruction is suspected — not for simple liquid acid aspiration.[2]
- Supportive care — oxygen, bronchodilators, fluids.
- Antibiotics only if pneumonia is present or develops, not routinely for a pure chemical pneumonitis.[2]
Post-extubation dysphagia
Post-extubation dysphagia is common, under-recognised, and a leading cause of aspiration pneumonia after ICU discharge. The mechanism is laryngeal injury (oedema, granuloma, arytenoid dislocation) and sensory change (the cuff abolishes laryngeal sensation, and the tube splints the glottis), which persist for days after extubation; risk factors are prolonged intubation (more than 48-72 hours), repeated intubation, large tube size, older age, and a tracheostomy.[2] It is frequently silent — the patient does not cough when aspirating. Perform a swallow assessment (bedside screen, then formal speech-language pathology assessment with FEES or videofluoroscopy if the screen fails) before resuming oral intake after prolonged intubation, and keep the patient NPO with enteral feeding until it is passed.[2][11]
Landmark trials
Drakulovic et al — supine vs semi-recumbent position (PMID 10584721)
Bouza et al (CIVAP) — continuous aspiration of subglottic secretions (PMID 18641114)
Klompas et al — reappraisal of routine chlorhexidine (PMID 24663255)
Krag et al (SUP-ICU) — pantoprazole for stress ulcer prophylaxis (PMID 30354950)
Marik — aspiration pneumonitis and aspiration pneumonia review (PMID 11228282)
Wolfe et al — corticosteroids for gastric aspiration (PMID 930946)
The one-paragraph exam answer
[8]SAQ — Witnessed aspiration under anaesthesia (Mendelson syndrome)
10 minutes · 10 marks
A 28-year-old woman for emergency caesarean section regurgitates gastric contents during a rapid sequence induction; particulate-free acidic fluid is seen in the oropharynx and suctioned, she is intubated, and within 4 hours she develops hypoxaemia (SpO2 88% on FiO2 0.5), bronchospasm, and bilateral dependent infiltrates. Outline your management and justify the use (or non-use) of antibiotics, corticosteroids, and bronchoscopy.
SAQ — Aspiration pneumonia in an elderly stroke patient
10 minutes · 10 marks
An 82-year-old nursing-home resident is admitted 5 days after a left hemisphere stroke with fever (38.9°C), purulent sputum with a putrid odour, and a right lower-lobe consolidation. She has poor dentition and was fed orally on the ward. Outline the antibiotic strategy and the VAP/aspiration prevention bundle for the unit.
Red flags
Clinical pearls
Quick-revision summary
- Mendelson syndrome = sterile acidic gastric contents, hours, supportive care, no routine antibiotics or steroids.
- Aspiration pneumonia = oral flora (anaerobes + streptococci), days, antibiotics.
- Prevention bundle = HOB 30-45 degrees, subglottic suction, cuff pressure 20-30 cmH2O, oral care (toothbrushing all, chlorhexidine selective), minimal sedation, RSI, suction above cuff pre-extubation, swallow assessment, post-pyloric feeding if high risk.
- PPIs do not prevent aspiration and do not reduce mortality.
- 48-hour checkpoint for chemical pneumonitis; bronchoscopy only for particulate matter.[14]
References
- [1]Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet, 1999.PMID 10584721
- [2]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [3]Prevention of Aspiration in Adults. Critical care nurse, 2017.PMID 28572110
- [4]Marik PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med, 2001.PMID 11228282
- [5]DiBardino DM, Wunderink RG. Aspiration pneumonia: a review of modern trends. J Crit Care, 2015.PMID 25129577
- [6]Klompas M, Speck K, Howell MD, Greene LR. Reappraisal of routine oral care with chlorhexidine gluconate for patients receiving mechanical ventilation: systematic review and meta-analysis. JAMA Intern Med, 2014.PMID 24663255
- [7]Labeau SO, Van de Vyver K, Brusselaers N, Vogelaers D, Blot SI. Prevention of ventilator-associated pneumonia with oral antiseptics in critically ill patients: systematic review and meta-analysis. Lancet Infect Dis, 2011.PMID 21798809
- [8]Bouza E, Perez MJ, Munoz P, Rincon C, Barrio JM, Hortal J, Sanchez-Petruzza P, Rivas D, Burillo A, Pelaez T, et al. (CIVAP Study Group). Continuous aspiration of subglottic secretions in the prevention of ventilator-associated pneumonia in the postoperative period of major heart surgery. Chest, 2008.PMID 18641114
- [9]Rello J, Afonso E, Lisboa T, Ricart P, Melnychuk P, Perez B, Campogayar L, Diaz E, (COMBACMed Group). A care bundle approach for prevention of ventilator-associated pneumonia. Clin Microbiol Infect, 2013.PMID 22439889
- [10]Wolfe JE, Bone RC, Ruth WE. Effects of corticosteroids in the treatment of patients with gastric aspiration. Am J Med, 1977.PMID 930946
- [11]El Solh AA. Pharmacologic prevention of aspiration pneumonia: a systematic review. Am J Geriatr Pharmacother, 2007.PMID 18179994
- [12]Krag M, Marker S, Perner A, Wetterslev J, Wise MP, Schefold JC, Kesecioglu J, Borthwick M, Bendel S, McAuley DF, et al. (SUP-ICU Trial Group). Pantoprazole in patients at risk for gastrointestinal bleeding in the ICU. N Engl J Med, 2018.PMID 30354950
- [13]Alhazzani W, Alshahrani M, Multz A, Seet E, Smith O, Muscedere J, Lopes R, Guyatt G, Meade MO, Cook D. Efficacy and safety of stress ulcer prophylaxis in critically ill patients: a network meta-analysis. Intensive Care Med, 2018.PMID 29199388
- [14]Metheny NA, Clouse RE, Chang YH, et al. Tracheobronchial aspiration of gastric contents in critically ill tube-fed patients: frequency, outcomes, and risk factors. Critical care medicine, 2006.PMID 16484901