ICU · Airway management
Difficult Airway Algorithms (DAS / ASA / CICO) & Front-of-Neck Access
Also known as Difficult airway · Difficult airway algorithm · DAS guidelines · CICO · Can't intubate can't oxygenate · Front of neck access · FONA · Cricothyroidotomy · MACOCHA score · NAP4 · Physiologically difficult airway
A difficult airway is one where a trained operator struggles with mask ventilation, laryngoscopy, or intubation. In ICU the patient is often both anatomically difficult (LEMON, MACOCHA) and physiologically difficult (shock, hypoxia, acidosis), and cannot simply be woken up. The Difficult Airway Society 2018 ICU intubation guideline structures the response into a sequence of plans (A: laryngoscopy and bougie; B: second-generation supraglottic airway rescue; C: maintain oxygenation and wake if able; CICO: front-of-neck access). CICO — can't intubate, can't oxygenate — is the life-threatening emergency requiring decisive scalpel-bougie cricothyroidotomy. The NAP4 audit showed most major airway events are avoidable: plan, assess, limit attempts, use capnography, and do not delay front-of-neck access.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
A difficult airway is one in which a trained operator experiences difficulty with face-mask ventilation, laryngoscopy and intubation, or both. In the ICU the challenge is greater than in the operating theatre for three reasons: the patient is often physiologically unstable (the "physiologically difficult airway" — shock, hypoxia, acidosis, right-heart failure), may be anatomically difficult, and, unlike the elective anaesthetic patient, cannot simply be woken up when intubation fails. Survival depends on anticipation, a structured algorithm, and a rehearsed plan for the worst case.[1][3]

Two dimensions of difficulty
- Anatomical difficulty — the airway is hard to see or to secure (poor laryngoscopic view, front of neck inaccessible, restricted mouth opening).
- Physiological difficulty — the patient tolerates the apnoea of intubation poorly (hypoxia, hypotension/shock, metabolic acidosis, right-heart failure, raised intracranial pressure). This is the ICU-specific problem, and it kills: cardiovascular collapse and hypoxia at induction are common.
Both must be addressed — resuscitate and preoxygenate before induction where possible, and limit intubation attempts (each deepens hypoxia and trauma).[11]
Predicting the difficult airway
Several bedside tools flag difficulty before the first attempt:[2][3]
- LEMON — for difficult direct laryngoscopy: Look (facial/neck abnormality), Evaluate the 3-3-2 rule (mouth opening, hyoid-chin, thyroid-to-floor of mouth), Mallampati, Obstruction, Neck mobility.
- MACOCHA score (De Jong et al, 2013) — the ICU-specific validated score for difficult intubation. Its seven factors: Mallampati grade III or IV, obstructive sleep apnoea, reduced cervical mobility, mouth opening under 3 cm, coma, severe hypoxia, and a non-anaesthetist operator. A higher score predicts difficult intubation and should trigger senior help and a back-up plan.[2]
- MOANS — difficult bag-valve-mask ventilation: Mask seal, Obesity, Age, No teeth, Stiff (resistant lungs).
- RODS — difficulty placing a supraglottic airway: restricted mouth opening, obstruction, disrupted upper airway, stiff lungs.
Predicted difficulty should change the plan: senior operator, awake intubation if feasible, video laryngoscope, and an explicit back-up.[1]
The ICU difficult-airway algorithm (DAS 2018)
The Difficult Airway Society 2018 guideline for tracheal intubation in critically ill adults (Higgs et al, BJA 2018) structures the response:[1]
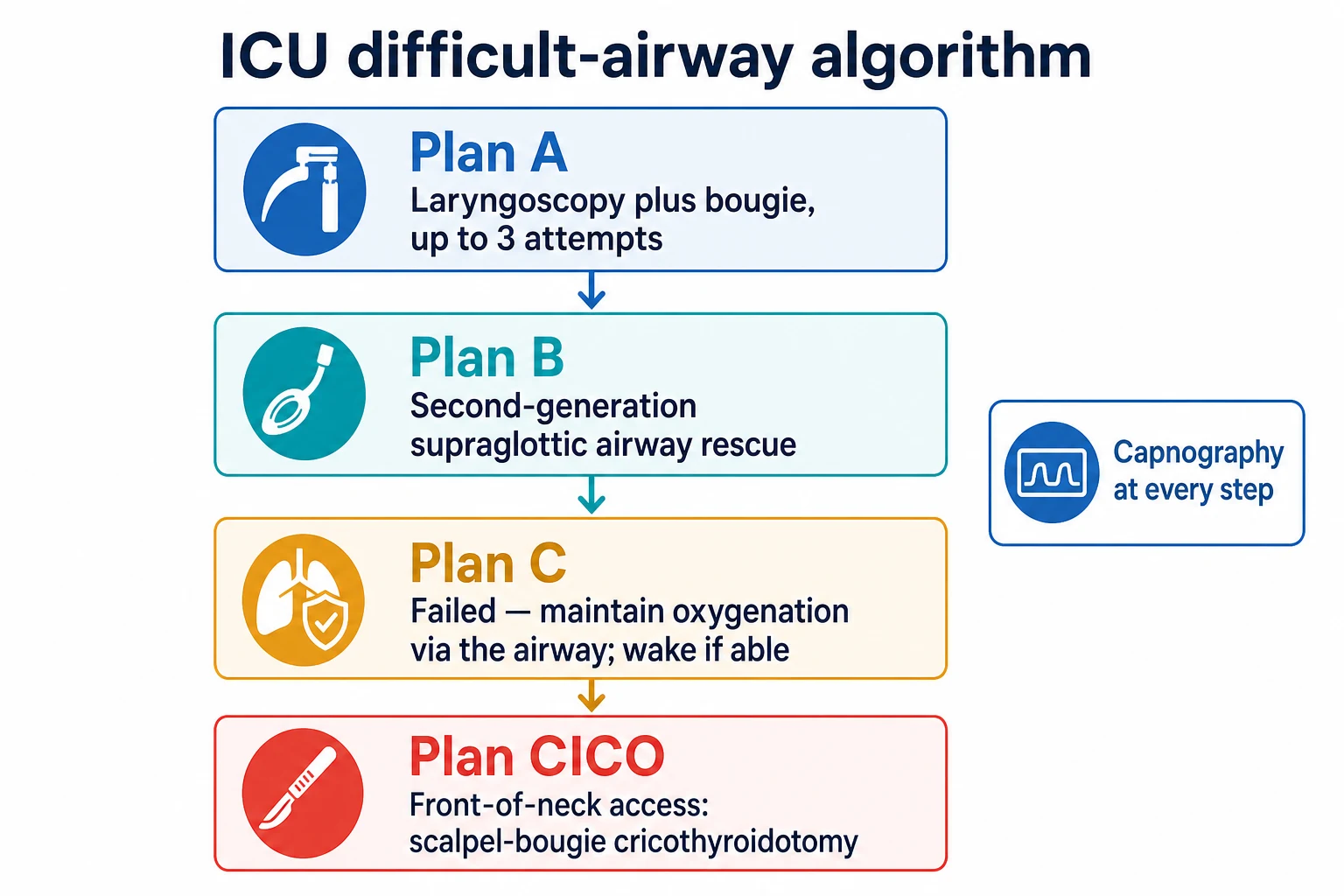
- Prepare — a structured checklist, preoxygenation, ramped position, monitoring (including continuous capnography), drugs, a trained team with defined roles, and a verbalised plan that names the back-up.
- Plan A — direct or video laryngoscopy (first-line in ICU) with a bougie or stylet; a maximum of three attempts, optimising each (position, external laryngeal manipulation, blade change). Persistent failure moves to Plan B.
- Plan B — a second-generation supraglottic airway (e.g. i-gel) as a rescue device. It both oxygenates and provides a conduit for intubation. Avoid first-generation devices (NAP4 showed they failed as rescue).[1][4]
- Plan C — the airway is still failing. If the patient can be woken (the elective option), wake them. In the ICU/emergency patient who cannot be woken, maintain oxygenation through the supraglottic airway and move to the CICO pathway.
- Plan CICO — front-of-neck access.
Waveform capnography is mandatory at every step — a CO2 trace confirms ventilation whether through a tube or a supraglottic airway.[1]
CICO and front-of-neck access (FONA)
CICO — can't intubate, can't oxygenate — is the life-threatening emergency. Death follows within minutes from hypoxia. The definitive rescue is front-of-neck access through the cricothyroid membrane.[1][4]
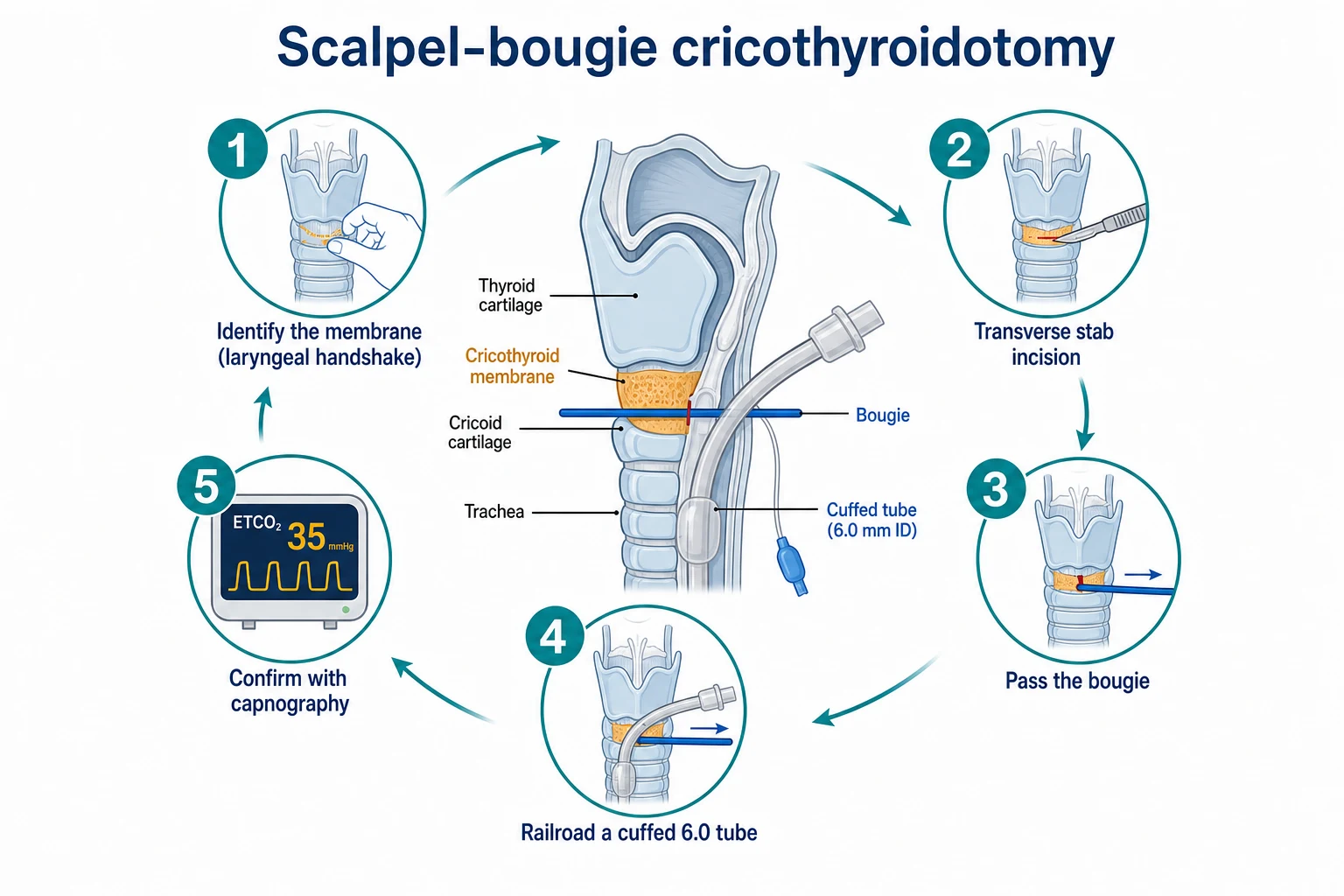
The recommended technique is the scalpel-bougie cricothyroidotomy:[1][3]
- Identify the cricothyroid membrane (between the thyroid and cricoid cartilages); a ultrasound or laryngeal handshake helps in the obese or distorted neck.
- A transverse stab incision through the skin and membrane with a scalpel.
- Pass a bougie through the incision into the trachea.
- Railroad a cuffed tube (commonly a size 6.0 endotracheal tube) over the bougie.
- Confirm with capnography and secure.
Cricothyroidotomy is preferred over formal tracheostomy for the emergency because it is faster, more superficial, and bleeds less; the formal tracheostomy is a later, elective procedure. The common, fatal error is delay — NAP4 found deaths from front-of-neck access performed too late. Decide early; a good rule is to call for FONA before the saturation is catastrophic.[4]
The anticipated difficult airway — awake intubation
When difficulty is predicted and the patient can cooperate and maintain oxygenation, an awake fibre-optic intubation is the safest approach: topicalise the upper airway, sedate lightly (e.g. dexmedetomidine or remifentanil, preserving ventilation and airway reflexes), and intubate awake. This avoids the apnoea and the loss of airway tone of an RSI in a known-difficult airway.[3]
Lessons from NAP4
The 4th National Audit Project (NAP4) of the Royal College of Anaesthetists reviewed major complications of airway management and found most were avoidable. Recurring themes:[4]
- Failure to assess or plan for difficulty.
- Repeated failed attempts deepening hypoxia.
- Absence of capnography (unrecognised oesophageal intubation).
- First-generation supraglottic airways used (and failing) as rescue.
- Delayed front-of-neck access.
- Poor human factors — communication, leadership, and failure to call for help early.
DAS 2015 — the unanticipated difficult intubation algorithm (theatre/perioperative)
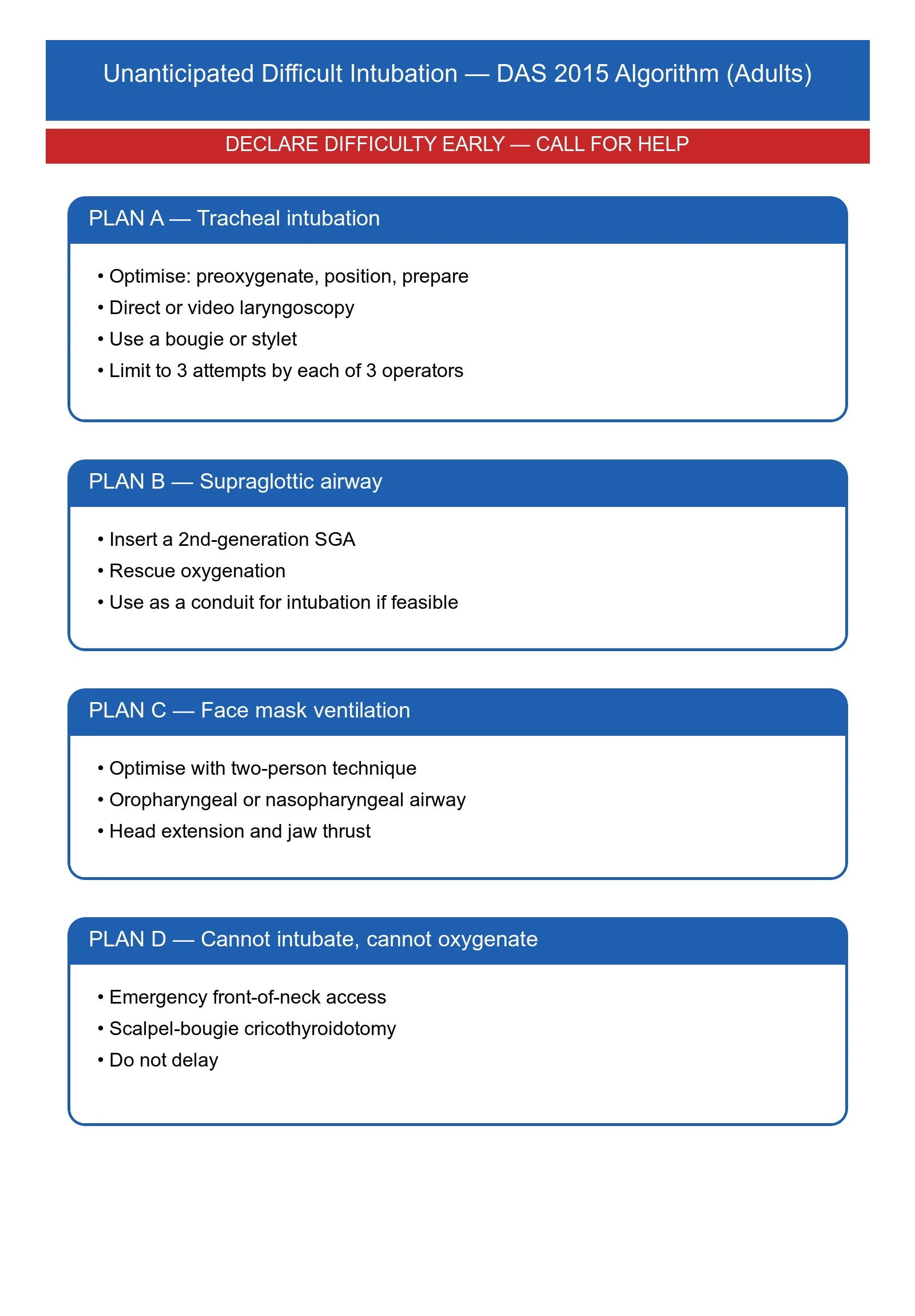
The DAS 2015 guidelines (Frerk et al, BJA 2015) govern the unanticipated difficult intubation in the operating theatre — the elective patient who turns out, after induction, to be difficult.[4] The structure is the familiar four plans, with the elective option of waking the patient preserved at Plan C:
- Plan A — initial tracheal intubation attempt: optimise position, direct/video laryngoscopy, use a bougie or stylet, external laryngeal manipulation. Maximum three best-effort attempts by an experienced operator.
- Plan B — supraglottic airway rescue: insert a second-generation SGA (i-gel or equivalent), oxygenate through it, then intubate via the SGA conduit (fibre-optically, or with a dedicated Aintree intubation catheter exchanged for a tracheal tube).
- Plan C — maintain oxygenation, wake the patient (the elective option). This is the key theatre/ICU divergence: the anaesthetised elective patient can usually be allowed to wake and re-breath, then be managed awake; the ICU/emergency patient often cannot.
- Plan D — "Can't intubate, can't oxygenate": emergency front-of-neck access (eFONA), the scalpel-bougie cricothyroidotomy.[4]
The 2015 guideline explicitly separates the anticipated (manage awake — fibre-optic intubation, regional anaesthesia as an alternative) from the unanticipated difficult airway (the A→B→C→D sequence above).[4]
[4]DAS 2018 — the four plans in detail
The DAS 2018 ICU intubation guideline (Higgs et al) is built on the recognition that the critically ill patient is killed as often by the physiology (cardiovascular collapse, hypoxia) as by the anatomy.[1] The four plans are:
DAS 2018 ICU algorithm — Plan A to Plan CICO (the structured walk-through)
Prepare — the pre-induction checklist
Before induction: complete a structured checklist. Allocate team roles (intensivist, assistant, drugs, cricoid, in-line traction, "float" to fetch equipment). Confirm working suction, ramped position (head-up 25-30°, ear-to-sternum), full monitoring including continuous waveform capnography. Draw up induction agent, paralysing agent AND a vasopressor (metaraminol/phenylephrine/noradrenaline) ready to push. Identify the cricothyroid membrane (ultrasound if obese) and verbalise the back-up: "If we cannot intubate or oxygenate, the plan is a scalpel-bougie cricothyroidotomy; the kit is here; Dr X will perform it."
Plan A — laryngoscopy, up to 3 attempts
Preoxygenase to end-tidal O2 >85% (or as high as physiology allows). Induce and paralyse (RSI). Video laryngoscope is first-line in ICU — it improves the view in anticipated and unanticipated difficulty. Use a bougie (Eschmann/gum-elastic) or stylet; apply external laryngeal manipulation (backwards-upwards-rightwards-pressure, BURP, or bimanual laryngoscopy). Optimise each attempt: change blade (CMAC D-blade, hyperangulated blade), reposition, re-bucket. Maximum three attempts by the most experienced operator. Confirm tracheal placement with waveform capnography.
Plan B — second-generation SGA rescue
On failure of Plan A, do NOT keep laryngoscoping — move to Plan B. Insert a second-generation supraglottic airway (i-gel, ProSeal, LMA Supreme): it seals the oesophagus, oxygenates, and provides a conduit. Confirm ventilation with capnography through the SGA. If oxygenation is restored and the patient stable, intubate via the SGA (Aintree catheter over a scope, exchanged for an ETT). If the SGA also fails, move immediately to Plan C.
Plan C — maintain oxygenation; wake if possible
If SGA rescue fails or is impossible: re-attempt face-mask ventilation with an oral/nasal airway, two-person technique, PEEP valve. If you can oxygenate, consider: (a) waking the patient if they were a stable RSI candidate and the induction agent is short-acting — often NOT feasible in ICU; (b) calling for expert help. If oxygenation CANNOT be maintained, declare CICO.
Plan CICO — declare and perform eFONA
Declare "Can't intubate, can't oxygenate" aloud. This is the cognitive trigger — say it. The most experienced operator performs a scalpel-bougie cricothyroidotomy: laryngeal handshake to fix the larynx, transverse stab through the lower half of the cricothyroid membrane, leave the blade in and twist 90°, slide the bougie alongside, railroad a size 6.0 cuffed ETT, inflate cuff, confirm with waveform capnography. Do NOT delay for equipment, ultrasound, or another laryngoscopy attempt.
Awakening as an option — and why it usually fails in ICU
In the elective theatre patient, waking the patient at Plan C is the safe escape: the propofol or thiopentone wears off, the patient re-breathes, and an awake technique (fibre-optic intubation) is planned for another day.[4] In ICU this option is frequently closed:
- The patient was intubated because they could not maintain their own airway or ventilation — waking them returns them to the respiratory failure that triggered the intubation.
- The induction agent plus a long-acting paralysing agent (rocuronium, suxamethonium) has abolished spontaneous ventilation and airway tone; reversal (sugammadex for rocuronium) is an option but takes time and the patient may remain obtunded from the sedative.
- The patient is shocked or hypoxic — the time to wake is the time to cardiac arrest.[4]
The Fellowship-level teaching is therefore: awakening is the Plan C ideal but rarely the ICU reality; the realistic ICU Plan C is maintaining oxygenation through an SGA or face mask while mobilising expert help and preparing eFONA, with the move to Plan CICO if oxygenation is lost.[1]
ASA 2022 Practice Guidelines for Management of the Difficult Airway
The ASA 2022 guidelines (Apfelbaum et al, Anesthesiology 2022) update the long-standing ASA difficult-airway algorithm and are the North American standard.[5] Key 2022 updates that distinguish them from the 2003 version and from DAS:
- New emphasis on video laryngoscopy as a primary tool — not merely a rescue. Hyperangulated blades and channelscopes (GlideScope, C-MAC D-blade, Airtraq) are first-line options for the anticipated difficult airway.
- Supraglottic airway as a definitive rescue and bridge — second-generation SGAs are endorsed as both ventilation rescue and a conduit for intubation.
- Awake intubation is recommended when difficulty is anticipated AND the patient can cooperate — fibre-optic, video-laryngoscopic, or hybrid awake techniques.
- Explicit incorporation of the difficult extubation — a 2022 addition: plan the exit (extubation) when planning the entry (intubation), with an airway exchange catheter left in situ for the high-risk extubation.
- New attention to human factors, cognitive aids, and team communication — including the recommendation to use a difficult-airway checklist and to document the difficult airway for future encounters (MedicAlert / registry).
- The CICO pathway — the ASA 2022 algorithm retains the emergency invasive airway access (cricothyroidotomy/transtracheal jet ventilation) as the can't-intubate-can't-oxygenate rescue, consistent with DAS.[5]
The Vortex Approach — a unifying cognitive tool
The Vortex Approach (Chrimes) is a cognitive tool designed to collapse the multiple difficult-airway algorithms (DAS, ASA, ANZCA) into a single visual funnel that any team can follow in a crisis.[7] Its genius is that it strips away the branching logic and the setting-specific detail and asks just one question repeatedly: is oxygenation being achieved?
Structure of the Vortex
- Three lifelines, tried once each with best effort: face-mask ventilation → supraglottic airway → endotracheal tube. Each is attempted with optimisation (best position, best device, best operator) — if it works, you are in the green zone (oxygenation achieved) and time is bought.
- The green zone: oxygenation is sustained (SpO2 maintained/rising). The team can regroup, call for help, change operator, prepare the next step. There is no obligation to proceed deeper.
- The blue ring / "best effort": each lifeline is given one genuine best effort, not a token attempt — the operator declares "green" (oxygenated) or moves to the next lifeline.
- The green zone can be re-entered from any depth if oxygenation returns.
- The vortex funnel: if all three lifelines fail and oxygenation is lost, the team is at the bottom of the Vortex — declare CICO and perform eFONA.[7]
Why the Vortex is taught alongside DAS/ASA
Chrimes reframed CICO failure as a "lost in transition" problem: clinicians find it cognitively difficult to abandon the familiar upper airway (where they have rehearsed) and move to the neck (which they have not).[7] The Vortex makes this transition an expected, rehearsed endpoint — the bottom of the funnel — rather than a surprise or a failure. The remediation is:
- Declare the transition aloud — "We are at the bottom of the Vortex, declaring CICO."
- Rehearse eFONA as a distinct cognitive step, not a panic.
- Use a shared visual tool (the Vortex diagram on the wall or trolley) so the whole team sees where they are and what comes next.[7]
Predicting difficulty in depth — LEMON, MOANS, RODS, and 3-3-2
Bedside airway assessment is imperfect — no score reliably predicts every difficult airway, and most "difficult" airways are unanticipated — but a structured assessment forces a plan and is the standard of care.[2][11]
LEMON — for difficult direct laryngoscopy
| Letter | Assesses | Abnormal finding |
|---|---|---|
| L — Look | External features | Facial trauma, large incisors, beard, macroglossia, narrow face, neck mass |
| E — Evaluate 3-3-2 | Mouth/hyoid/neck distances | See below |
| M — Mallampati | Oropharyngeal view | Class III or IV (only soft/hoard palate visible) |
| O — Obstruction | Upper airway pathology | Stridor, muffled voice, trismus, epiglottitis, tumour, infection |
| N — Neck mobility | Cervical movement | Fixed c-spine collar, arthritis, surgical fusion |
The 3-3-2 rule within LEMON: the patient should fit three fingers between the incisors (mouth opening), three fingers from the hyoid bone to the chin (hyomental distance, submandibular space), and two fingers from the thyroid notch to the floor of the mouth (laryngeal position). Failure of any predicts difficulty — a high anterior larynx and a small submandibular space make anterior displacement of the tongue impossible.[11]
MOANS — for difficult mask ventilation
| Letter | Factor | Why |
|---|---|---|
| M — Mask seal | Beard, facial trauma, oedema | No seal, no positive pressure |
| O — Obesity | BMI > 30 | Redundant pharyngeal tissue, low FRC, weight on chest |
| A — Age | Age > 55 | Loss of tissue tone |
| N — No teeth | Edentulous | Cheeks collapse, mask leak (but the SGA fits better!) |
| S — Stiff | Reduced pulmonary compliance | ARDS, bronchospasm, pulmonary oedema |
RODS — for difficult supraglottic airway placement
| Letter | Factor | Why |
|---|---|---|
| R — Restricted mouth opening | < 3 cm | SGA cannot be inserted |
| O — Obstruction | Upper airway | Device cannot seat |
| D — Disrupted upper airway | Trauma, surgery | No anatomy to seal against |
| S — Stiff lungs | High airway pressures | SGA leaks above ~20-25 cm H2O |
MACOCHA — the ICU-specific validated score
The MACOCHA score (De Jong et al, 2013, AzuRea Network) is the only validated bedside score specifically for ICU intubation difficulty.[2] Seven factors:
| Factor | Points |
|---|---|
| Mallampati grade III or IV | 5 |
| Obstructive sleep apnoea syndrome | 2 |
| Reduced cervical mobility | 1 |
| Mouth opening < 3 cm | 1 |
| Coma (GCS < 8) | 1 |
| Severe hypoxia (SpO2 < 80%) | 1 |
| Non-anaesthetist operator | 1 |
Total ≥ 4 (out of 12) predicts difficult intubation with ~73% sensitivity and 86% specificity. A high MACOCHA score should trigger: the most experienced operator present, video laryngoscopy first-line, a second-generation SGA immediately to hand, and a verbalised eFONA plan.[2]
Why no score is perfect — the unanticipated difficult airway
Even with a careful LEMON/MACOCHA assessment, most difficult airways in practice are unanticipated — the scores have low sensitivity, and a "normal" assessment does not exclude difficulty. Reed et al found that the LEMON score only modestly predicted difficulty in the emergency department.[11] The corollary: always have a back-up plan, regardless of the assessment.
The physiologically difficult airway
Mosier introduced the concept of the physiologically difficult airway to capture the fact that, in ICU/ED, the danger is as much the physiology as the anatomy.[12] The four physiological threats at induction are:
- Hypoxaemia — the ICU patient has low FRC, high shunt, and V/Q mismatch; pre-oxygenation may not denitrogenate adequately; desaturation is rapid. Mitigate: ramped position, HFNO/nasal cannulae for apnoeic oxygenation, denitrogenate to EtO2 > 85%.
- Hypotension / cardiovascular collapse — the sedative drops SVR and preload; the loss of sympathetic tone with induction and the positive-pressure ventilation drop venous return. The shocked patient arrests. The INTUBE study found peri-intubation cardiovascular collapse in ~44%** of ICU intubations, and cardiac arrest in ~3-4%**.[13][14] Mitigate: fluid-load if responsive, vasopressor ready (push-dose phenylephrine/metaraminol or noradrenaline infusion), reduced-dose ketamine or etomidate, avoid propofol in the shocked.
- Metabolic acidosis — the patient is compensating with tachypnoea; the induction abolishes it and the acidosis deepens, with cardiovascular collapse. Mitigate: keep the apnoea SHORT, ventilate to maintain the respiratory compensation if possible.
- Right heart failure / cor pulmonale — the positive-pressure ventilation and PEEP increase pulmonary vascular resistance and drop RV preload; the decompensated RV fails. Mitigate: low PEEP, low intrathoracic pressure, vasopressors to maintain coronary perfusion.
The 2024 international Delphi on the physiologically difficult airway (Karamchandani et al) codified strategies: fluid loading, vasopressor infusion, ketamine as induction agent of choice, paralyse to facilitate laryngoscopy, ramped position, and pre-oxygenation with HFNO where feasible.[15]
Supraglottic airway rescue — the Plan B device
A second-generation supraglottic airway is the DAS Plan B rescue device of choice.[1][6] The features that make second-generation superior to first-generation LMAs in the crisis are:
- Oesophageal seal — a drain tube or dual-cuff design that channels regurgitated fluid away from the airway, reducing aspiration.
- Better airway seal pressure — second-generation SGAs seal at 25-30 cm H2O vs ~20 cm H2O for first-generation; they hold during high-pressure ventilation in stiff lungs.
- Intubation conduit — the device accepts an Aintree intubation catheter over a fibre-optic scope, allowing a controlled exchange to a cuffed ETT.
- Bite block built in — protects the device from occlusion.[6]
Intubating via the SGA — the Aintree exchange
When a second-generation SGA has restored oxygenation in Plan B, the next step is to convert to a definitive cuffed ETT. The Aintree intubation catheter technique: load the Aintree over a fibre-optic scope; pass the scope through the SGA into the trachea under direct vision; railroad the Aintree into the trachea; remove the scope and SGA, leaving the Aintree in situ; railroad a size 7.0 ETT over the Aintree; confirm with capnography. This is the controlled, definitive exchange — and is preferable to blind intubation through the SGA.[4]
CICO rescue — declaring and acting
CICO — can't intubate, can't oxygenate — is the trigger for emergency front-of-neck access (eFONA). Note the modern definition: the trigger is failure of oxygenation, not merely failure of intubation or mask ventilation. A patient you can still oxygenate (by mask or SGA) is NOT CICO; they are in the green zone and the algorithm has not failed.[7][8]
Declaring CICO — the cognitive trigger
The single most important cognitive step is declaring CICO aloud:[6]
- Say it: "This is CICO. We are performing a surgical airway." Verbalising breaks the fixation error (the cognitive trap of repeating the same failed laryngoscopy in the hope it will work).
- Name the operator: "Dr X, you are doing the cricothyroidotomy." (the most experienced operator, not the most junior).
- Name the kit location: "The FONA kit is at the head of the bed."
- Set the time pressure: "We need oxygenation in 60 seconds."[6]
The scalpel-bougie cricothyroidotomy — recap
The DAS-recommended adult technique is the scalpel–twist–bougie–tube sequence (detailed in the Front-of-Neck-Access topic): laryngeal handshake → transverse stab through the lower cricothyroid membrane → leave the blade in and twist 90° → slide the bougie alongside the blade caudally → railroad a size 6.0 cuffed ETT → inflate cuff → confirm with waveform capnography.[4][8]
Why not cannula cricothyroidotomy in adults?
NAP4 documented multiple deaths from cannula cricothyroidotomy in adults — from kinking, inadequate driving pressure (wall oxygen is too weak; a proper jet ventilator is needed), and most dangerously failure of exhalation against an obstructed upper airway → barotrauma and tension pneumothorax.[6] The DAS guidance is therefore scalpel-bougie first-line in adults; the cannula technique is reserved for prepubertal children and operators trained exclusively in it.[1][4]
Human factors and crisis resource management (CRM)
The most common root cause of a major airway event is not technical — it is human factors: failure to call for help early, fixation errors, poor communication, and absence of a clear leader.[6] NAP4 and the subsequent Vortex literature converge on the following CRM principles for the difficult airway:[7]
- Call for help early — the moment difficulty is anticipated or the first attempt fails. The senior airway operator, an anaesthetist, ENT, and a second pair of hands should be summoned before the saturation is catastrophic.
- Name a leader and assign roles aloud — intubator, assistant (drugs/cricoid), "float" (fetches equipment), monitor-watcher, timekeeper, scribe. Role ambiguity is a recurring NAP4 theme.
- Use cognitive aids — the difficult-airway algorithm card on the wall, the Vortex diagram on the trolley, the pre-induction checklist. They reduce cognitive load and break fixation.
- Close-loop communication — "Give me the bougie." → "Bougie." → "Bougie in." Not "give me the thing."
- Verbalise the plan and the back-up before induction — "If we cannot intubate, we go to an i-gel; if that fails, Dr X does a cricothyroidotomy; the kit is here."
- Brief for the worst case, not the best — assume the airway will be difficult; pre-position the SGA, the scalpel-bougie kit, and the vasopressor before induction.
- Debrief after every difficult airway event — for the team and for the system; feed back into the difficult-airway registry.[7]
The difficult-airway trolley and institutional preparedness
NAP4's most actionable systems-level recommendation was that every location where airway management occurs (theatre, ICU, ED, ward) must have a standardised difficult-airway trolley with a sealed, dated eFONA kit.[6] The Fellowship-level expectation:
- A standardised trolley with the same layout across the institution — drawer 1: SGA (second-generation) and airways; drawer 2: video laryngoscopes and blades; drawer 3: bougies, stylets, Aintree; drawer 4: sealed scalpel-bougie eFONA kit (size 10 blade, bougie, size 6.0 cuffed ETT, syringe, tie).
- The sealed eFONA kit checked on a schedule (like the crash trolley); every operator knows where it is.
- Annual difficult-airway simulation for all airway operators — the Vortex and the scalpel-bougie technique drilled until they are reflexive.
- A difficult-airway registry / alert — patients with known difficulty flagged in the electronic record and offered a MedicAlert bracelet, so the next encounter is prepared.
- A post-event debrief after every real CICO or major airway event — for clinical, human-factors, and systems learning.[6]
NAP4 — the foundational audit
The 4th National Audit Project (NAP4) of the Royal College of Anaesthetists and the Difficult Airway Society (Cook, Woodall, Frerk, 2011) prospectively audited major complications of airway management across UK NHS hospitals over one year.[6] Its findings reframed airway crises as systems failures, not technical failures, and drove the modern guidelines:
- ICU and ED were over-represented in the major events — despite fewer airway interventions than theatres, ICU and ED contributed a disproportionate number of deaths and brain injuries.
- Capnography was absent or misused in a striking proportion — leading to unrecognised oesophageal intubation and tube dislodgement.
- Repeated failed attempts deepened hypoxia and converted a difficult airway into a CICO.
- First-generation SGAs failed as rescue devices — driving the shift to second-generation devices.
- eFONA was delayed — patients arrested before the surgical airway was established.
- Poor human factors — failure to call for help, lack of leadership, fixation errors.
- Recommendations: dedicated difficult-airway trolleys with sealed eFONA kits; mandatory capnography everywhere; training and simulation; earlier declaration of CICO; and the adoption of second-generation SGAs and scalpel-bougie eFONA.[6]
Prognosis
A structured, rehearsed approach prevents hypoxic brain injury and death. The principles are: assess difficulty, resuscitate and preoxygenate before induction, limit attempts, use video laryngoscopy and a second-generation supraglottic airway, confirm with capnography, call for help early, and perform front-of-neck access decisively when CICO is declared.[1][3][4]
[11]SAQ — The unanticipated difficult airway in ICU (DAS 2018 algorithm)
10 minutes · 10 marks
A 67-year-old man with severe community-acquired pneumonia is admitted to ICU with septic shock and type 1 respiratory failure (SpO2 88% on 15 L/min via non-rebreather, MAP 62 on noradrenaline 0.2 mcg/kg/min, lactate 3.8). You decide to intubate. Pre-oxygenation achieves SpO2 95%. After induction with ketamine 2 mg/kg and rocuronium 1.2 mg/kg, direct laryngoscopy reveals a Cormack-Lehane grade 3 view; video laryngoscopy improves it to grade 2 but you cannot pass the tube. A second-generation i-gel is inserted and provides adequate ventilation with colour-change capnography, but the patient's SpO2 is now drifting and he remains haemodynamically unstable.
SAQ — Anticipated difficult airway and awake fibreoptic intubation
10 minutes · 10 marks
A 54-year-old woman with a retropharyngeal abscess and known laryngeal oedema presents to ICU with worsening stridor, drooling, and trismus. She is maintaining SpO2 94% on 10 L/min, sitting upright and leaning forward, and is cooperative. Laryngoscopy in the emergency department 2 hours earlier was abandoned due to a complete inability to visualise the glottis.
Red flags
Clinical pearls
Key trials and evidence
Higgs et al — DAS 2018 ICU intubation guideline (PMID 29406182)
De Jong et al — MACOCHA score (PMID 23348979)
Frerk et al — DAS 2015 guidelines for unanticipated difficult intubation (PMID 26556848)
Apfelbaum et al — ASA 2022 Practice Guidelines for Management of the Difficult Airway (PMID 34762729)
Cook, Woodall, Frerk — NAP4, Fourth National Audit Project (PMID 21447488)
Chrimes et al — 'Lost in transition' and the Vortex Approach (PMID 32475685)
Heard et al — formulation of the CICO algorithm (PMID 19453312)
Mosier et al — The Physiologically Difficult Airway (PMID 26759664)
Russotto et al — INTUBE Study (PMID 33755076)
Russotto et al — Peri-intubation Cardiovascular Collapse, INTUBE (PMID 35536310)
Karamchandani et al — Physiologically difficult airway Delphi (PMID 39162823)
Aslani et al — cricothyroid membrane palpation accuracy (PMID 22366848)
Rai et al — ultrasound for cricothyroid membrane identification (PMID 32836091)
Reed et al — LEMON score in the emergency department (PMID 15662057)
Prognosis and outcomes
The outcome of the difficult airway is determined less by the technical execution of any single step than by anticipation, a structured algorithm, and the team's human factors. A structured, rehearsed approach prevents hypoxic brain injury and death; the principles are: assess difficulty, resuscitate and preoxygenate before induction, limit attempts, use video laryngoscopy and a second-generation SGA, confirm with capnography, call for help early, declare CICO aloud, and perform eFONA decisively.[1][3][6]
The determinants of outcome are:[6]
- The speed of declaring CICO and acting — the single biggest modifiable factor; NAP4 deaths were from delay.[6]
- The peri-intubation physiology — cardiovascular collapse and hypoxaemia (INTUBE) are as lethal as the airway failure itself.[13][14]
- Operator rehearsal and institutional preparedness — the difficult-airway trolley, sealed eFONA kit, and annual simulation.[6]
- The underlying illness — a difficult airway complicating angioedema or a foreign body has a better prognosis than one in a septic, cardiovascularly collapsed ICU patient.[1]
- Avoidance of the avoidable errors — repeated attempts, first-generation SGA, absent capnography, oversized eFONA tube, lost stoma. LEMON/MACOCHA, the Vortex, second-generation devices, the scalpel-twist-bougie-tube sequence, and a size 6.0 cuffed ETT prevent most of these.[4][8]
References
- [1]Higgs A, McGrath BA, Goddard C, et al. Guidelines for the management of tracheal intubation in critically ill adults. British journal of anaesthesia, 2018.PMID 29406182
- [2]De Jong A, Molinari N, Terzi N, et al. Early identification of patients at risk for difficult intubation in the intensive care unit: development and validation of the MACOCHA score in a multicenter cohort study. American journal of respiratory and critical care medicine, 2013.PMID 23348979
- [3]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [4]Frerk C, Mitchell VS, McNarry AF, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. British journal of anaesthesia, 2015.PMID 26556848
- [5]Apfelbaum JL, Hagberg CA, Connis RT, et al.; American Society of Anesthesiologists Committee on Practice Parameters. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology, 2022.PMID 34762729
- [6]Cook TM, Woodall N, Frerk C; Fourth National Audit Project of the Royal College of Anaesthetists and Difficult Airway Society. Major complications of airway management in the UK: results of the Fourth National Audit Project (NAP4). British Journal of Anaesthesia, 2011.PMID 21447488
- [7]Chrimes N, Higgs A, Rehak A, et al. Lost in transition: the challenges of getting airway clinicians to move from the upper airway to the neck during an airway crisis. British Journal of Anaesthesia, 2020.PMID 32475685
- [8]Heard AMB, Green RJ, Eakins P. The formulation and introduction of a 'can't intubate, can't ventilate' algorithm into clinical practice. Anaesthesia, 2009.PMID 19453312
- [9]Aslani A, Ng SC, Hurley M, McCarthy KF, Ci K, Duggan M. Accuracy of identification of the cricothyroid membrane in female subjects using palpation: an observational study. Anesthesia and Analgesia, 2012.PMID 22366848
- [10]Rai D, Hilton A, Maslovitz S, Bhatia N, Otoupalova E, Smith B, Ramgopal S, Subramaniam K, Mosier JM, Mendonca C. The role of ultrasound in front-of-neck access for cricothyroid membrane identification: a systematic review. Journal of Critical Care, 2020.PMID 32836091
- [11]Reed MJ, Dunn MJ, McKeown DW. Can an airway assessment score predict difficulty at intubation in the emergency department? Emergency Medicine Journal, 2005.PMID 15662057
- [12]Mosier JM, Joshi R, Hypes C, Pacheco G, Valenzuela T, Sakles JC. The Physiologically Difficult Airway. Western Journal of Emergency Medicine, 2015.PMID 26759664
- [13]Russotto V, Myatra SN, Laffey JG, et al.; INTUBE Study Investigators. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA, 2021.PMID 33755076
- [14]Russotto V, Tassistro E, Myatra SN, et al.; INTUBE Study Investigators. Peri-intubation Cardiovascular Collapse in Patients Who Are Critically Ill: Insights from the INTUBE Study. American Journal of Respiratory and Critical Care Medicine, 2022.PMID 35536310
- [15]Karamchandani K, Nasa P, Jarzebowski M, Brewster DJ, De Jong A, et al. Tracheal intubation in critically ill adults with a physiologically difficult airway. An international Delphi study. Intensive Care Medicine, 2024.PMID 39162823