ICU · Airway management
Front-of-Neck Access — Surgical Airway, Cricothyroidotomy & Tracheostomy
Also known as Front of neck access · FONA · Surgical airway · Cricothyroidotomy · Scalpel-bougie cricothyroidotomy · Emergency tracheostomy · Needle cricothyroidotomy · Laryngeal handshake · CICO rescue · Surgical airway · Emergency surgical airway · eFONA · Cricothyrotomy · Trans-tracheal jet ventilation
Front-of-neck access (FONA) is the rescue for can't-intubate-can't-oxygenate (CICO). The emergency standard is the scalpel-bougie cricothyroidotomy: identify the cricothyroid membrane with the laryngeal handshake, a transverse stab incision, pass a bougie, railroad a cuffed size 6.0 tube, and confirm with capnography. Cricothyroidotomy is preferred over tracheostomy for the emergency because it is faster, more superficial, and bleeds less; formal tracheostomy is an elective, lower-neck procedure. The fatal error, highlighted by NAP4, is delay. Children, laryngeal trauma, and tracheal disruption are relative contraindications to cricothyroidotomy.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
Front-of-neck access (FONA) is the surgical rescue for the failed airway — specifically can't-intubate, can't-oxygenate (CICO) — when all other options (laryngoscopy, supraglottic airway) have failed and oxygenation cannot be maintained. Death follows within minutes from hypoxia, so the procedure must be decisive and well rehearsed. The emergency standard is the scalpel-bougie cricothyroidotomy.[1][5]
The language has shifted deliberately. Older literature used "can't intubate, can't ventilate (CICV)"; modern UK and Australasian guidance uses CICO — "can't oxygenate" — to capture the clinically relevant endpoint: it is failure of oxygenation (not just bag-mask ventilation) that mandates FONA. A patient who cannot be intubated but who can still be oxygenated with a bag-mask or supraglottic airway is not CICO, and FONA is not indicated.[1][10]
FONA sits at the bottom of every difficult-airway algorithm — DAS 2015 (Plan C / eFONA), DAS 2018 ICU Plan D, the Vortex Approach (green zone), the ASA difficult airway algorithm, and the CICM/ANZCA airway guidance. Each algorithm differs in its pathway to get there but converges on the same final action: scalpel, bougie, tube.[5][10]
Defining and declaring CICO — when to act
The single most important decision in FONA is declaring CICO. NAP4 found that the commonest failure mode was not a botched incision but a delayed decision — operators persisted with upper-airway rescue while the patient desaturated to arrest.[6]
CICO is declared when:[5]
- Cannot intubate — best laryngoscopy attempt(s) by the most experienced operator present has failed (or a Cormack-Lehane 4 view that cannot be improved), AND
- Cannot oxygenate — face-mask ventilation, a second-generation supraglottic airway, and any combination thereof are failing to maintain oxygenation (typically defined as a falling SpO2 below ~80% despite optimal effort, or an inability to generate chest rise).[5][10]
Practical decision rules:[1]
- Best effort is a maximum of three laryngoscopy attempts by an experienced operator, with the best device and optimal positioning, optimised between attempts. Repeated fruitless attempts worsen trauma, bleeding, and oedema and narrow the time window for FONA.[1]
- A supraglottic airway is a mandatory intermediate step (DAS Plan B). If the SGA fails to oxygenate, declare CICO.[5]
- Call for help at the first hint of difficulty, not at the point of CICO — senior airway operator, surgical colleague, difficult-airway trolley.[1]
- Declare aloud: "This is CICO. We are going to the neck." A clear, verbal declaration cuts the cognitive inertia that kills these patients.[10]
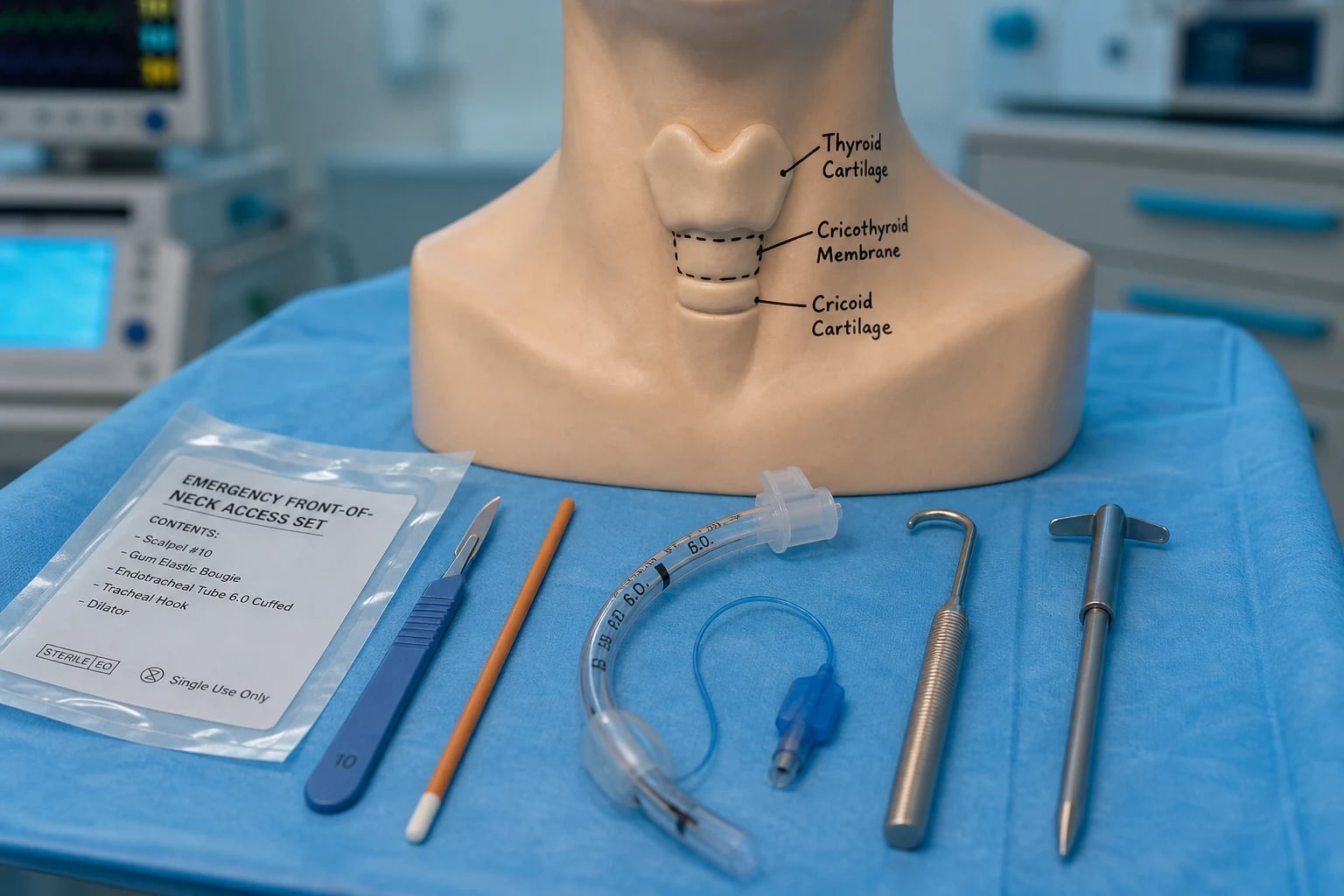
The relevant anatomy
The target is the cricothyroid membrane, the membranous gap between the thyroid cartilage above (with its prominent notch) and the cricoid cartilage below. It is superficial, avascular, and lies below the vocal cords, which makes it the safest and fastest route into the airway in an emergency.[3]
Relations to know:[3]
- The isthmus of the thyroid crosses the trachea lower down (around the 2nd-4th tracheal rings) — a reason the lower tracheostomy bleeds more than cricothyroidotomy.
- The cricothyroid artery branches run across the upper membrane (a small risk of bleeding).
- The recurrent laryngeal nerve lies posteriorly; posterior injury risks vocal-cord paralysis.
- The membrane becomes harder to identify in the obese, oedematous, or distorted neck — use the laryngeal handshake (grasp the larynx: thumb and middle finger on the thyroid cartilage, index finger finds the membrane) and ultrasound if available.[1]
Detailed anatomical landmarks (the Fellowship answer)
flowchart TD
A["Hyoid bone"] --- B["Thyroid notch<br/>(Adam's apple)"]
B --- C["Thyroid cartilage laminae"]
C --- D["Cricothyroid membrane<br/>(the target)"]
D --- E["Cricoid cartilage<br/>(complete ring)"]
E --- F["Tracheal rings 2-4<br/>(isthmus of thyroid crosses here)"]
F --- G["Carina & bronchi"]
style D fill:#ffd966,stroke:#b8860b,stroke-width:2px
style E fill:#cfe2f3,stroke:#1f4e79
The cricothyroid membrane (median cricothyroid ligament) is a fibroelastic membrane ~9-10 mm tall and ~25-30 mm wide in the adult. It is the only part of the laryngeal skeleton not supported by cartilage and is therefore the natural point of entry. Three structural facts shape the technique:[3]
- It is subcutaneous. Skin to membrane is typically 8-12 mm — less than the length of a size 10 scalpel blade. A single deliberate transverse stab traverses both.
- It is avascular centrally. The cricothyroid arteries (a branch of the superior thyroid) anastomose across the upper border, forming the cricothyroid arcade. A lower membrane stab (close to the cricoid) avoids this arcade — the basis for the DAS instruction to incise the lower half of the membrane.[5]
- It is below the vocal cords. Entry here bypasses the glottis entirely — important when the glottis is the source of obstruction (angioedema, tumour, infection). The posterior tracheal wall (membranous, unsupported) is the structure most vulnerable to over-penetration.
Identifying the membrane in the difficult neck. Palpation alone is unreliable, especially in women and the obese (no prominent thyroid notch; submental fat). In a cadaver study by Aslani et al, anaesthetists correctly identified the cricothyroid membrane by palpation in ~30% of female subjects — the rest were misplaced, often over the thyroid or laryngeal cartilage where a stab would fail.[8] Where time permits (the pre-CICO phase), ultrasound identifies the membrane with near-100% accuracy in seconds.[12] The pragmatic answer is: palpate with the laryngeal handshake, and confirm with ultrasound before the patient crashes if you have the seconds.[12]
Equipment — the dedicated FONA kit
NAP4 highlighted that FONA often failed because the right equipment was not immediately to hand: a single, sealed, immediately identifiable kit is now standard.[6] The kit should contain:
- Scalpel — a size 10 or size 20 blade on a size 3 or 4 handle. The size 10 (curved) is preferred by DAS for the transverse stab; the size 20 (broader) is used by some military/prehospital services for the longitudinal "slash and stab" technique. Avoid size 11 (the pointed blade slips and injures the posterior wall).[5]
- Bougie — a 15-French gum-elastic / Eschmann-type bougie, ideally with the angled coudé tip. The bougie is the workhorse: it finds the tracheal lumen, sits reliably in the trachea, and provides a railway for the tube.[7]
- Cuffed tube — a size 6.0 cuffed endotracheal tube is the DAS default for an adult. A tracheostomy tube (size 6.0 or 7.0 cuffed, with an inner cannula) is an alternative used by some ENT-trained operators but is harder to railroad over a bougie and lacks the standard 15 mm connector for the ICU circuit unless a specific tube is used.[5]
- Suction (Yankauer).
- Tracheal hook and Trousseau dilator — used in the classical four-step technique; not required for the scalpel-bougie method but should be in the kit.
- Syringe for the cuff, tape or a tie to secure, and a capnograph connector.
The kit should be sealed, dated, located on every difficult-airway trolley, and checked on the same cycle as the arrest trolley.[1]
The scalpel-bougie cricothyroidotomy (the emergency standard)
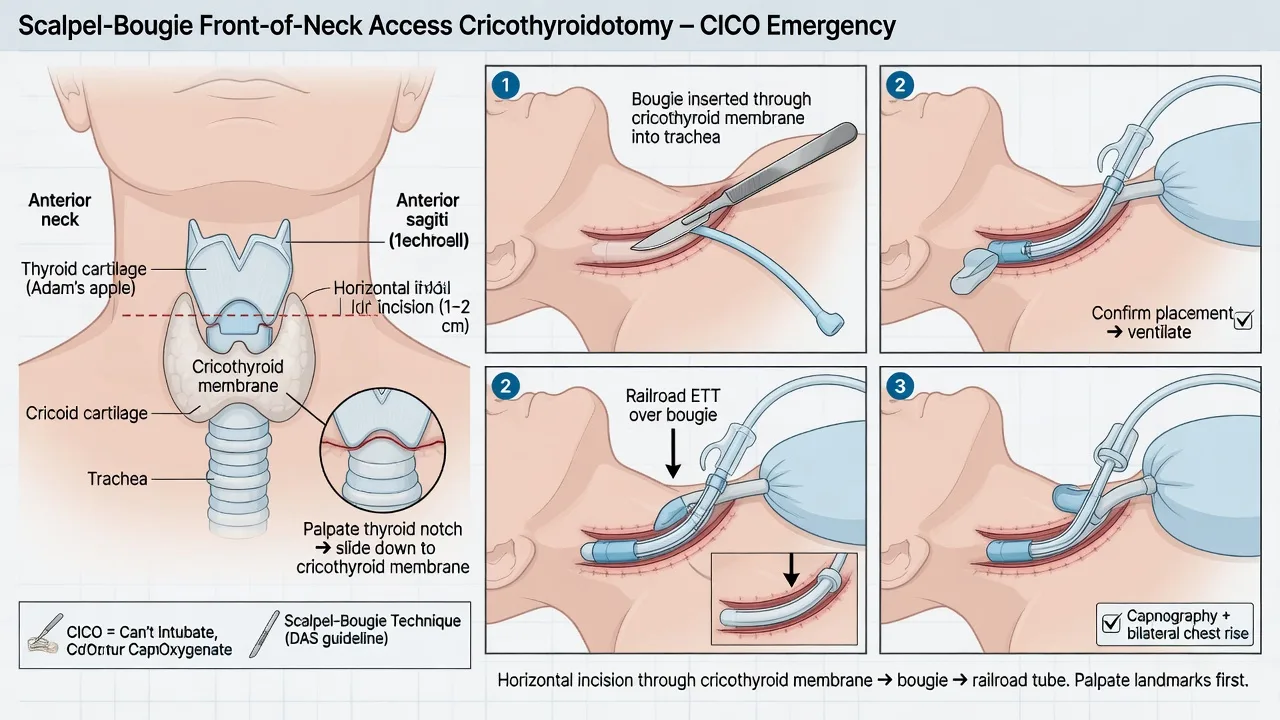
The technique recommended by the Difficult Airway Society:[1][5]
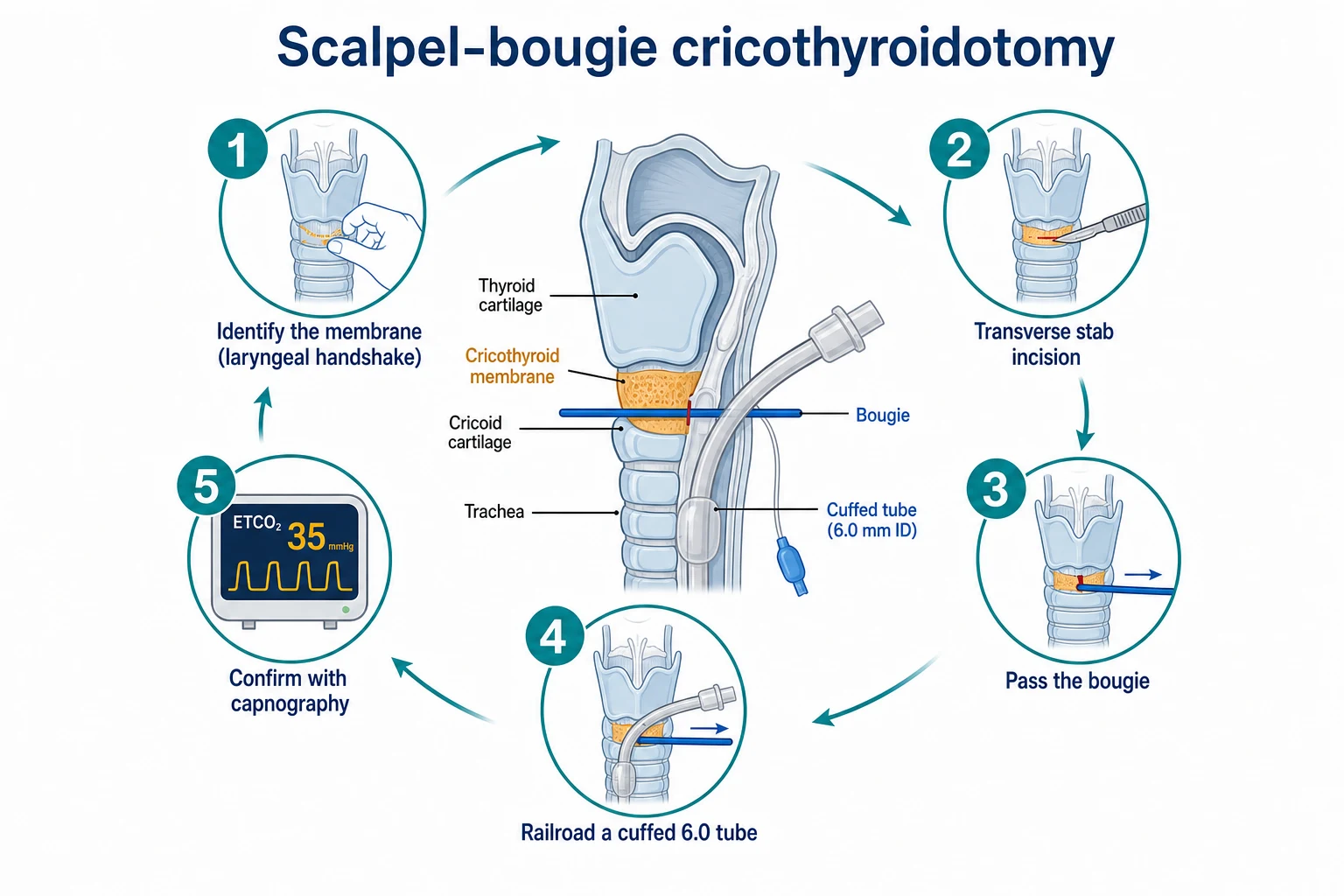
- Position and identify — extend the neck (if not contraindicated); perform the laryngeal handshake to find the cricothyroid membrane between the thyroid and cricoid cartilages. Ultrasound confirms in the difficult neck.
- Stab incision — a transverse skin-and-membrane stab incision with a scalpel (typically a size 10 or 20 blade) through the cricothyroid membrane. In the bloody or obese neck, a vertical skin incision first, then a horizontal membrane stab, helps.
- Pass the bougie — slide a gum-elastic bougie through the incision into the trachea (a "hold-up" and rotation resistance confirms tracheal placement).
- Railroad the tube — pass a cuffed tube (commonly a size 6.0 endotracheal tube, occasionally a tracheostomy tube) over the bougie into the trachea; inflate the cuff.
- Confirm — waveform capnography (a CO2 trace over several breaths), plus bilateral chest rise; then ventilate and secure.[1][3]
The procedure should take under a minute when rehearsed.[1]
The full scalpel–twist–bougie–tube sequence (DAS 2015 technique, step by step)
The DAS 2015 eFONA technique collapses the five classical steps into a scalpel–twist–bougie–tube sequence that is faster and more reliable than older dilator-based methods. Memorise the sequence verbatim — it is the Fellowship oral answer.[5]
Scalpel–twist–bougie–tube — the DAS 2015 eFONA sequence
Stand on the dominant side
Position yourself on the SAME side as your dominant hand (right-hander on the patient's right). You will make the incision with your dominant hand and stabilise the larynx with the other. The assistant stands opposite and retracts. Neck extension if c-spine cleared; otherwise maintain in-line stabilisation but the patient is dying — extend if you must.
Laryngeal handshake
With your NON-DOMINANT hand, grasp the larynx: thumb and middle finger on the thyroid cartilage laminae, index finger palpating down to find the cricothyroid membrane between the thyroid prominence above and the firm cricoid ring below. This hand STAYS in place — it fixes the larynx so it does not roll away during the incision. Keep it there until the tube is in.
Transverse stab incision
With your DOMINANT hand, take a size 10 blade. In the bloody or obese neck, FIRST make a vertical skin incision (~3-4 cm) over the membrane to expose it; then re-palpate with the index finger to confirm the membrane. Then a single firm TRANSVERSE stab through skin and cricothyroid membrane in one movement, in the LOWER half of the membrane (avoids the cricothyroid arcade). You will feel a distinct "give" as the blade enters the trachea.
Twist the blade 90 degrees
LEAVE THE BLADE IN. Rotate it 90 degrees so the flat of the blade opens the hole, edge facing the patient's feet. This holds the stoma open and exposes the tracheal lumen — the "twist" that gives the technique its name.
Slide the bougie alongside the blade
Slide a gum-elastic (Eschmann) bougie through the stoma alongside the blade, angled CAUDALLY (towards the feet) along the posterior tracheal wall. It should pass with minimal resistance. Confirm tracheal position: "hold-up" at the carina (do not force) and the characteristic click of the coudé tip over the tracheal rings. Remove the blade.
Railroad the size 6.0 cuffed ETT
Pass a cuffed SIZE 6.0 ETT over the bougie (the 6.0 slides over the 15 F bougie and through the stab without binding; a 7.0 or 8.0 will jam). Railroad it gently into the trachea to a depth of ~8-10 cm at the lip (or until the cuff is just through the membrane). Inflate the cuff. Remove the bougie.
Confirm with waveform capnography
Attach the circuit and the capnograph. You MUST see a persistent CO2 waveform over several breaths before declaring success — a paratracheal or oesophageal tube will produce no CO2. Bilateral chest rise and auscultation. Then secure the tube, reposition, and ventilate.
Needle cricothyroidotomy (and jet ventilation)
A large-bore cannula through the cricothyroid membrane connected to a high-pressure oxygen source (transtracheal jet ventilation). It is an older technique that only buys time — it oxygenates but does not ventilate (CO2 rises), fails when there is upper-airway obstruction (no gas egress), and risks barotrauma. It is largely superseded by the scalpel-bougie technique in adults, but retains a role in small children (see below).[3]
Why the cannula technique fails in adults (the NAP4 lesson)
NAP4 documented a series of failures and deaths with cannula cricothyroidotomy in adults.[6] The reasons are mechanical:
- Kinking and dislodgement of the cannula — a 14 G/13 G Ravussin-style cannula is fragile; the patient moves, the assistant tugs the tubing, the cannula bends and obstructs.
- Inadequate driving pressure — a standard wall oxygen flowmeter at 15 L/min delivers ~3-4 psi, far below the ~25-30 psi needed to overcome airway resistance in an obstructed, obese, or bronchospastic patient. A proper jet ventilator (Sanders or Manujet, 1-4 bar) is required and is often not immediately available.
- Failure of exhalation — the cannula insufflates oxygen but if the upper airway is obstructed there is no route for gas to escape. Pressure builds, the lung ruptures, and tension pneumothorax / barotrauma supervenes. This is the mechanism of death in the most-cited NAP4 cases.[6]
- No protective cuff — blood and secretions flood the airway.
The DAS 2015 and DAS 2018 guidance therefore places scalpel-bougie as the first-line adult technique, with cannula cricothyroidotomy reserved for paediatric patients and operators trained exclusively in the cannula technique.[1][5]
[6]Surgical tracheostomy as an alternative — and why it is NOT the emergency choice
A formal surgical tracheostomy is a controlled, elective dissection through the lower anterior neck into the trachea (typically between the 2nd and 3rd tracheal rings). It is the definitive airway for prolonged ventilation, weaning, and bronchial toilet — but it is not the CICO rescue.[3]
Why cricothyroidotomy wins in the emergency
- Speed. The cricothyroid membrane is superficial (skin-to-membrane 8-12 mm); a stab takes seconds. The trachea at the 2nd-3rd ring lies behind the thyroid isthmus, strap muscles, pretracheal fascia, and investing deep cervical fascia — a multi-layer dissection that takes minutes even for a trained surgeon.[3]
- Bleeding. The cricothyroid membrane is avascular centrally. The lower tracheostomy crosses the thyroid isthmus (a vascular structure), the inferior thyroid veins, and the anterior jugular veins — bleeding obscures the field, lengthens the procedure, and is dangerous in the anticoagulated or coagulopathic patient.
- Landmarks. The cricothyroid membrane is reliably palpable (with the laryngeal handshake). The lower tracheal rings are harder to identify in the obese, oedematous, or distorted neck and are deeper.
- Rehearsal. Scalpel-bougie can be drilled on a manikin and reproduced under stress. Formal tracheostomy requires surgical training.
When surgical tracheostomy IS the emergency airway
There are a small number of situations where the operator must go to the lower neck (tracheostomy) rather than the cricothyroid membrane:[3]
- Laryngeal trauma or fracture — entering through a fractured larynx fails and worsens the injury; the airway is established below the injury via a tracheostomy.
- Pre-existing laryngeal pathology — tumour, infection (supraglottitis, epiglottitis), prior laryngeal surgery, or known subglottic stenosis.
- Tracheal disruption or transection — a cricothyroidotomy may be ABOVE the injury; the airway is established at the level of the distal trachea (often a field tracheostomy at the wound).
- Children under ~10-12 years — the cricoid is the narrowest part of the paediatric airway and is easily damaged; a paediatric surgical airway is performed lower, by an expert.[14]
Converting the emergency cricothyroidotomy to a tracheostomy
A cricothyroidotomy placed as an emergency is usually converted to a formal tracheostomy within about 24-72 hours if ongoing mechanical ventilation is needed, to reduce subglottic stenosis and long-term airway injury. The cricothyroid membrane is the narrowest part of the adult airway; a tube through it for more than ~7 days risks circumferential scarring and stenosis at the glottic level. The conversion is performed in theatre once the patient is stabilised.[3]
Cricothyroidotomy versus tracheostomy
- Cricothyroidotomy — the emergency airway: through the superficial, avascular cricothyroid membrane; fast, with less bleeding. It is the CICO rescue.[1]
- Tracheostomy — an elective airway: a lower-neck dissection through (or around) the thyroid isthmus into the trachea (typically the 2nd-3rd tracheal ring); slower, more bleeding, more structure to traverse. It is performed for prolonged ventilation, weaning, and airway protection — not for the acute CICO.[3]
A cricothyroidotomy placed as an emergency is usually converted to a formal tracheostomy within about 24-72 hours if ongoing mechanical ventilation is needed, to reduce subglottic stenosis and long-term airway injury.[3]
[14]Contraindications (relative)
- Prepubertal children — the cricoid is the narrowest part of the paediatric airway and is easily damaged; a needle cricothyroidotomy or paediatric surgical airway by an expert is preferred over an adult-style scalpel-bougie.[3]
- Laryngeal trauma or fracture — go lower (a tracheostomy) to avoid the damaged larynx.
- Tracheal disruption or transection — a cricothyroidotomy may be above the injury; a surgical tracheostomy or field tracheostomy at the level of injury may be needed.
- Pre-existing laryngeal pathology (tumour, infection, prior surgery).[3]
- Anticoagulation / coagulopathy — relative; the cricothyroid membrane is avascular so bleeding is usually manageable, but the lower tracheostomy in a coagulopathic patient can be catastrophic. Favour cricothyroidotomy if FONA is unavoidable.
Complications
- Bleeding — from the thyroid isthmus (if too low), cricothyroid vessels, or anterior jugular veins.
- Misplacement — paratracheal, through the posterior tracheal wall, or into the oesophagus (the commonest failure); confirmed and corrected by capnography.[6]
- Posterior tracheal wall perforation (from the bougie or tube) — produces surgical emphysema, loss of the airway, and a tracheo-oesophageal fistula.
- Laryngeal fracture or cricoid damage.
- Barotrauma (cannula technique with jet ventilation, especially with upper-airway obstruction).
- Late: subglottic stenosis, voice change, and tracheo-oesophageal fistula — the reason for elective conversion to tracheostomy.[3]
Human factors — why FONA is delayed
The greatest barrier to a successful emergency surgical airway is not technical but cognitive: the operator delays declaring CICO and starting the incision, hoping the next laryngoscopy attempt will succeed. NAP4 found deaths from front-of-neck access performed too late.[6] A separate review of emergency surgical airways in Australian and New Zealand emergency departments confirmed the procedure is rare, time-critical, and dependent on rehearsal.[2] Mitigation: declare CICO early (before saturations are catastrophic), rehearse the technique and the equipment regularly, and have a dedicated FONA kit immediately available.[1][2]
Chrimes and colleagues reframed this as the "lost in transition" problem: clinicians find it cognitively hard to abandon the familiar upper airway (where they have trained and rehearsed) and move to the neck (which they have not). The remedy is deliberate practice of FONA as a distinct cognitive step — the Vortex Approach's "green zone" is explicitly designed to make this transition explicit and rehearsed.[10]
Surveys repeatedly show that while most anaesthetists and intensivists can describe the technique, far fewer have performed it on a real patient, and skill decays rapidly without rehearsal.[9] Mendonca's survey of anaesthetists and surgeons found wide variation in confidence and in the equipment immediately available — a strong argument for institution-level standardisation.[9]
Paediatric FONA — special considerations
The paediatric airway differs from the adult in ways that change the FONA technique:[3]
- The cricoid ring (not the cricoid cartilage externally) is the narrowest segment of the paediatric airway — a tube placed through the cricothyroid membrane sits at the narrowest point and risks damage.
- The larynx is high and anterior (C3-C4 in the infant vs C6 in the adult), the cartilage is soft, and the membrane is tiny (a few millimetres) — an adult-style scalpel-bougie is often anatomically impossible.
- Children desaturate much faster than adults (low FRC, high oxygen consumption) — the time window from CICO to arrest may be 1-2 minutes.[8]
Recommended approach in prepubertal children: a needle cricothyroidotomy with jet ventilation (oxygenation buys time while CO2 rises — acceptable for a few minutes), or an age-appropriate surgical airway by an expert paediatric anaesthetist/ENT surgeon. An adult-style scalpel-bougie is generally avoided. The APN/APLS paediatric difficult-airway algorithms converge on this.[3]
FONA in special circumstances
Procedural competence and rehearsal
FONA is a low-frequency, high-acuity skill. Real-world incidence is ~1 in 5,000-50,000 general anaesthetics, and ~1 in 200-1,000 ICU intubations in the most difficult patients.[6][13] Without deliberate rehearsal, skill decays within weeks. The fellowship-level expectation is:
- Annual simulation on a task trainer (porcine larynx, manikin, or cadaver) — minimum, ideally quarterly.
- Familiarity with the local FONA kit — every operator must know where it is and what is in it.
- Briefing the team before every difficult intubation — "If we cannot intubate or oxygenate, the plan is a scalpel-bougie cricothyroidotomy; the kit is at the head of the bed; Dr X will perform it."[1]
- Post-event debrief after any real FONA — for the team and for the system.
SAQ — Declaring CICO and performing scalpel-bougie cricothyroidotomy
10 minutes · 10 marks
A 58-year-old obese man is being intubated in the emergency department for severe head injury with aspiration. After induction, three attempts at laryngoscopy (including video laryngoscopy) fail; a second-generation supraglottic airway does not seal and does not ventilate; two-person bag-mask ventilation with oral and nasal airways produces no chest movement. The capnograph is flat. SpO2 has fallen from 92% to 60% and is still falling. He has an anterior neck that is difficult to palpate due to submental fat.
SAQ — Paediatric FONA and the difficult anterior neck
10 minutes · 10 marks
You are the intensivist at a peripheral hospital. A 5-year-old child with severe croup is brought to the emergency department with impending airway obstruction. Despite nebulised adrenaline, helium-oxygen and dexamethasone, she deteriorates; inhalational induction with sevoflurane is attempted but she arrests during laryngoscopy and cannot be intubated or ventilated.
Clinical pearls
Red flags
[12]Key trials and evidence
NAP4 — Fourth National Audit Project of airway management (PMID 21447488)
DAS 2015 guidelines — unanticipated difficult intubation in adults (PMID 26556848)
Chrimes et al — 'Lost in transition' (PMID 32475685)
Heard et al — formulation of the CICO algorithm (PMID 19453312)
Aslani et al — accuracy of cricothyroid membrane palpation (PMID 22366848)
Rai et al — ultrasound for cricothyroid membrane identification (PMID 32836091)
Lockey et al — pre-hospital airway rescue in trauma (PMID 25038154)
Groombridge et al — securing the tube in surgical cricothyroidotomy (PMID 34321049)
Alkhouri et al — emergency FONA in ANZ EDs (PMID 33179449)
Mendonca et al — FONA survey (PMID 29416237)
Prognosis and outcomes
Emergency FONA success — when the operator is rehearsed, the equipment is to hand, and CICO is declared early — is high, with first-pass tracheal placement in >90% of cadaver and simulation studies and a low rate of serious complications in real case series.[2][13] Mortality from CICO itself is dominated by the underlying cause of the airway failure and by delay — patients who arrest before FONA is established do poorly regardless of technique.[6]
The determinants of outcome after emergency FONA are:[2]
- The speed of declaration — the single biggest modifiable factor. Earlier FONA = better survival.[6]
- Operator rehearsal and the immediate availability of a sealed kit — institutional, not individual.[1][9]
- The underlying illness — CICO complicating angioedema or a foreign body has a better prognosis than CICO in a septic, hypoxaemic, cardiovascularly collapsed ICU patient.[2]
- Avoidance of the avoidable technical failures — paratracheal placement, posterior-wall perforation, oversized tube, lost stoma. Capnography, the laryngeal handshake, the scalpel-twist-bougie-tube sequence, and a size 6.0 cuffed ETT prevent most of these.[5]
Late complications — subglottic stenosis, voice change, tracheo-oesophageal fistula — are minimised by converting the emergency cricothyroidotomy to a formal tracheostomy within 24-72 hours.[3]
References
- [1]Higgs A, McGrath BA, Goddard C, et al.; Difficult Airway Society et al. Guidelines for the management of tracheal intubation in critically ill adults (DAS 2018). British Journal of Anaesthesia, 2018.PMID 29406182
- [2]Alkhouri H, Richards C, et al. Case series and review of emergency front-of-neck surgical airways from The Australian and New Zealand Emergency Departments. Emergency Medicine Australasia, 2021.PMID 33179449
- [3]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [5]Frerk C, Mitchell VS, McNarry AF, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. British journal of anaesthesia, 2015.PMID 26556848
- [6]Cook TM, Woodall N, Frerk C; Fourth National Audit Project Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia (NAP4). British Journal of Anaesthesia, 2011.PMID 21447488
- [7]Heard AMB, Green RJ, Eakins P The formulation and introduction of a 'can't intubate, can't ventilate' algorithm into clinical practice. Anaesthesia, 2009.PMID 19453312
- [8]Aslani A, Ng SC, Hurley M, McCarthy KF, Milne AD Accuracy of identification of the cricothyroid membrane in female subjects using palpation: an observational study. Anesthesia and Analgesia, 2012.PMID 22366848
- [9]Mendonca C, Ahmad I, Sajayan A, Wicker J Front of neck access: a survey among anaesthetists and surgeons. Journal of Anaesthesiology Clinical Pharmacology, 2017.PMID 29416237
- [10]Chrimes N, Higgs A, Rehak A, et al. Lost in transition: the challenges of getting airway clinicians to move from the upper airway to the neck during an airway crisis. British Journal of Anaesthesia, 2020.PMID 32475685
- [11]Mabry RL, Nichols MC, Shiner DC, et al. A comparison of two open surgical cricothyroidotomy techniques by military medics using a cadaver model. Annals of Emergency Medicine, 2014.PMID 24094476
- [12]Rai Y, You-Ten E, Zasso F, Chan V, Perlas A The role of ultrasound in front-of-neck access for cricothyroid membrane identification: a systematic review. Journal of Critical Care, 2020.PMID 32836091
- [13]Lockey D, Crewdson K, Weaver A, Davies G Observational study of the success rates of intubation and failed intubation airway rescue techniques in 7256 attempted intubations of trauma patients by pre-hospital physicians. British Journal of Anaesthesia, 2014.PMID 25038154
- [14]Groombridge CJ, Maini A, Mathew J, Kim Y, Singh A, Mitra B, Hsu J Comparing methods to secure a tracheal tube placed via a surgical cricothyroidotomy: a randomised controlled study in cadavers. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 2021.PMID 34321049