ICU · Resuscitation
Airway management and rapid sequence induction in ICU
Also known as Rapid sequence induction (RSI) · Endotracheal intubation · Difficult airway · Difficult airway society (DAS) guidelines · Can't intubate, can't oxygenate (CICO) · Emergency front of neck access (eFONA) · Video laryngoscopy · Pre-oxygenation and apnoeic oxygenation · Peri-intubation cardiac arrest
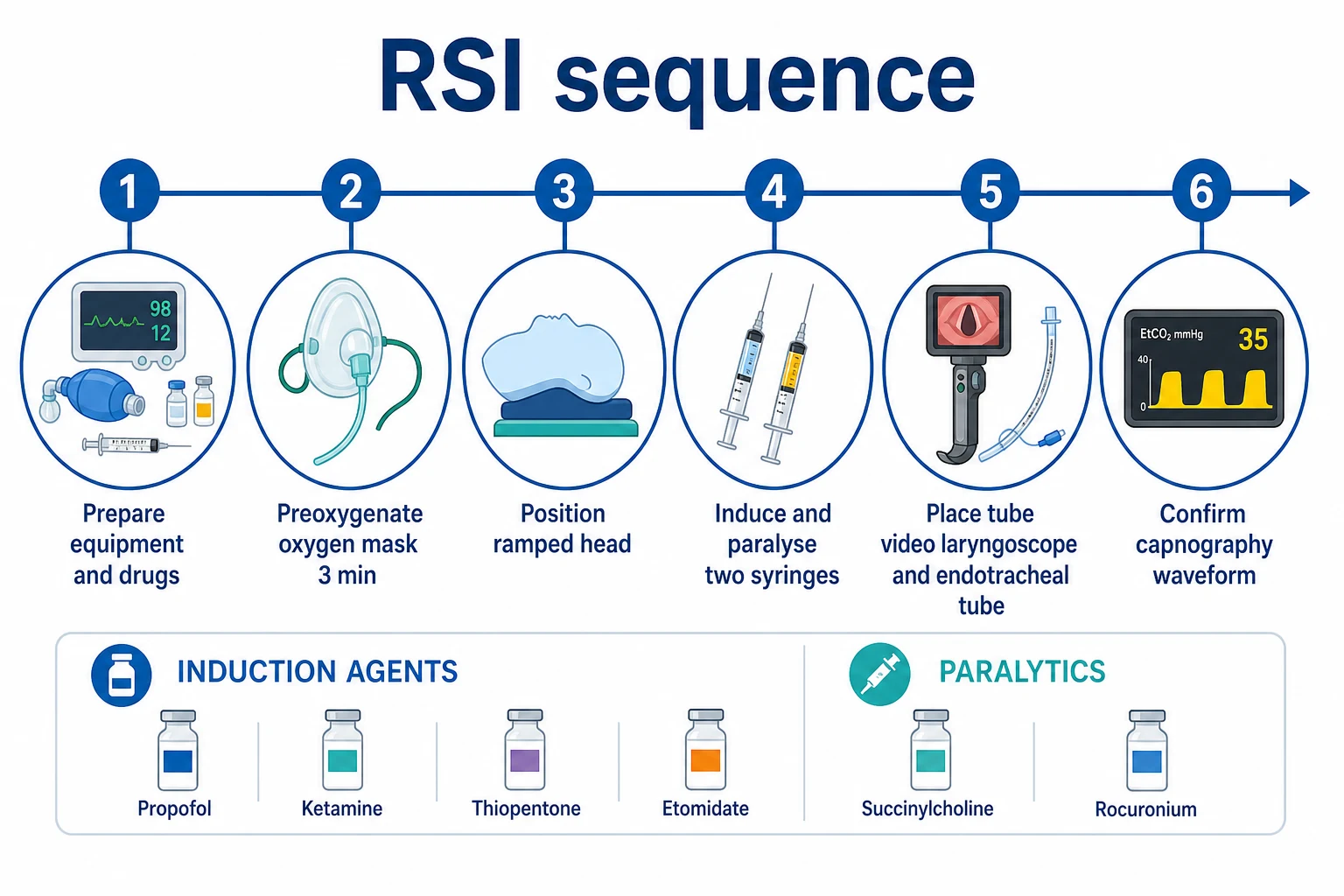
Airway management is a core ICU skill and a high-yield Fellowship exam topic. RSI (rapid sequence induction) is indicated for any critically ill patient requiring intubation who is at risk of aspiration (full stomach, pregnancy, bowel obstruction, sepsis, trauma, obesity) — which in practice is EVERY ICU intubation. Principle: pre-oxygenation (denitrogenation via 100% O2 for 3 min OR 8 vital-capacity breaths of 100% O2, buying 3-5 min of safe apnoeic oxygenation) → induction agent + paralytic given SIMULTANEOUSLY (NO mask ventilation) → laryngoscopy and intubation → confirm with waveform ETCO2. ICU airway is far higher risk than theatre: critically ill patients have profoundly reduced physiological reserve (hypoxaemia, hypotension, acidosis, hypovolaemia) and the 'can't intubate, can't oxygenate' (CICO) scenario is rapidly fatal. Peri-intubation cardiac arrest occurs in ~3% of ICU intubations. Drugs: induction — propofol (avoid in shock), ketamine (preferred for shock/asthma — bronchodilator, sympathomimetic), etomidate (avoid in sepsis — adrenal suppression); paralytic — rocuronium 1.2 mg/kg (preferred — reversible with sugammadex 16 mg/kg) or suxamethonium 1.5 mg/kg (ultra-short but contraindicated in hyperkalaemia, burns 24h, denervation, malignant hyperthermia). Difficult airway prediction: LEMON (Look externally, Evaluate 3-3-2, Mallampati, Obstruction, Neck mobility) plus MACOCHA score for ICU. Video laryngoscopy (GlideScope, C-MAC) preferred — better glottic view, though first-pass success is operator-dependent (MACMAN trial: video = direct laryngoscopy for first-pass success in non-experienced operators). Bougie (esophageal bougie) ROUTINELY for the difficult view — DRIVER trial: bougie first = higher first-pass success than stylet. CICO rescue: emergency front of neck access (eFONA) — scalpel-bougie cricothyroidotomy. Post-intubation: VAP prevention bundle (head of bed 30-45°, oral chlorhexidine, subglottic suction ETT, daily sedation interruption, stress ulcer prophylaxis, DVT prophylaxis — 'bundled care').
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Overview — why ICU airway is different
[7]Airway management in ICU is qualitatively different from the operating theatre. The critically ill patient has profoundly reduced physiological reserve in three domains that conspire against the intubator:[1][2]
- Reduced apnoea tolerance (hypoxaemic reserve). Critically ill patients desaturate to dangerous levels within 30-90 seconds of apnoea — far faster than the healthy, fasted elective patient (who may tolerate 5-10 min). Reasons: low functional residual capacity (FRC) from obesity, pregnancy, splinting, pulmonary oedema, ARDS, pneumonia; increased shunt; increased metabolic rate (sepsis, fever, agitation); reduced cardiac output; reduced haemoglobin (less oxygen storage). When SpO2 falls below ~90% (PaO2 ~60 mmHg), the steep part of the oxyhaemoglobin dissociation curve means SpO2 then plummets to 70% within seconds. Laryngoscopy should be abandoned if SpO2 falls below 90-93% and the patient re-oxygenated before a further attempt.
- Reduced haemodynamic reserve (cardiovascular collapse). Induction agents (propofol, thiopentone) abolish the sympathetic tone that critically ill patients depend on for blood pressure. Combined with loss of venous return from positive-pressure ventilation and the underlying shock state, induction frequently precipitates severe hypotension or cardiac arrest. Peri-intubation cardiac arrest occurs in ~3% of ICU intubations and cardiovascular instability (new vasopressor requirement, significant MAP drop) in 25-40%.[2]
- Difficult airway prevalence. ICU patients are more likely to have a difficult airway — cervical collar in place, in-line stabilisation, blood/vomit/secretions in the airway, distorted anatomy (oedema, tumour, infection), limited mouth opening, pre-existing airway device (LMA, ETT), inability to cooperate with awake techniques.
The INTUBE study (29 countries, 2,964 intubations) found that major adverse events occurred in 45% of ICU intubations — cardiovascular instability 43%, severe hypoxaemia 9%, cardiac arrest 3%, aspiration 2%. The implication: ICU intubation must be approached as a procedure with a checklist, not a bedside reflex.[2]
Preparation — the SOAP-ME checklist
Adequate preparation prevents poor performance. The DAS/ICS 2018 guidelines emphasise a structured pre-intubation checklist; SOAP-ME (or SOAP-2-ME) is the most widely used mnemonic in ICU and ED.[1][8]
RSI preparation checklist (SOAP-2-ME)
Suction
Yankauer sucker switched ON and under the pillow — instant access if regurgitation. Thick secretions, blood, or vomit: wide-bore rigid suction (the flexible suction catheter will block). Test the suction is working BEFORE you need it.
Oxygen
Pre-oxygenate: 100% O2 for 3 minutes of tidal breathing via a well-fitting non-rebreather mask (NRB) with reservoir, OR 8 vital-capacity breaths of 100% O2 (equivalent denitrogenation in ~60 seconds). HFNO (Optiflow/Nasal High Flow, 30-70 L/min) provides continuing apnoeic oxygenation during the apnoeic phase — THRIVE can extend safe apnoea time from minutes to an hour in selected patients. Goal: denitrogenation → FRC filled with O2 → 3-5 (up to 8) min safe apnoea. Monitor: SpO2 continuously. ABANDON laryngoscopy if SpO2 falls below 90-93% — re-oxygenate before next attempt.
Airway equipment
Laryngoscope (video preferred — GlideScope/C-MAC — with a direct Macintosh blade available as backup). ETT: size 8.0 male, 7.0 female (cut to ~23 cm at the teeth for 8.0, ~21 cm for 7.0 — prevents mainstem intubation). Check cuff. Have one size smaller available. Stylet/bougie (elastic bougie is essential — ROUTINELY use for any difficult view; DRIVER trial showed bougie-first improves first-pass success). 10 mL syringe for cuff. Tape/tie/commercial tube holder. ETCO2 detector (waveform capnography — confirm placement). Supraglottic airway — i-gel (preferred — better seal than LMA, no cuff to inflate) size 4 (small female), 5 (large female/small male), 6 (large male). Cricothythyroidotomy kit (scalpel #10 or #20, bougie, size 6.0 ETT) — PLAN C, opened and visible.
Pharmacology
Induction: propofol 1-2 mg/kg (avoid in shock — profound hypotension), ketamine 1-2 mg/kg (preferred for shock, asthma, bronchospasm — maintains BP via sympathetic stimulation, bronchodilator), etomidate 0.3 mg/kg (haemodynamically neutral but causes adrenal suppression — AVOID in sepsis). Reduce ALL induction doses by 30-50% in the critically ill (they are exquisitely sensitive). Paralytic: rocuronium 1.2 mg/kg (reversible with sugammadex 16 mg/kg — preferred for ICU), suxamethonium 1.5 mg/kg (rapid onset 45 s, offset 5-10 min, but risks: hyperkalaemia, malignant hyperthermia, bradycardia). Vasopressor ready: draw up noradrenaline boluses (4-8 mcg) or push-dose adrenaline (10 mcg/mL) — give BEFORE induction if MAP borderline.
Monitoring
ECG, SpO2 (continuous, on a waveform/plethysmograph), NIBP cycling every 3 min (consider arterial line if haemodynamically unstable — beat-to-beat BP), ETCO2 (capnography — confirm intubation AND monitor ventilation). Pre-induction ABG useful (baseline pH, PaO2, PaCO2, K+, lactate).
Team (and briefing)
Most experienced intubator performs laryngoscopy. Airway assistant: applies cricoid pressure (controversial — may improve or worsen view — release or reduce if difficulty). Drug assistant: gives agents as directed. Team leader: stands back, coordinates, watches clock and SpO2/BP, calls out time intervals. Second pair of hands: ready with bougie, suction, suction, second laryngoscope. MANDATORY team brief beforehand — state explicitly Plan A, Plan B, Plan C, and the criteria for moving between them.
Pre-oxygenation — the most important step you can do well
Pre-oxygenation is the single intervention that buys you time to intubate without the patient sustaining hypoxic brain injury. Done well, it converts the urgent into the planned. Done poorly (or skipped), the patient desaturates during laryngoscopy, you panic, and a cascade of errors begins.[1]
Physiology — what pre-oxygenation actually does
The lung is a reservoir holding ~3 L of gas at functional residual capacity (FRC). In a patient breathing room air (21% O2, 79% nitrogen), that reservoir is mostly nitrogen — useless as an oxygen store during apnoea. Pre-oxygenation washes the nitrogen out of the FRC and replaces it with oxygen (denitrogenation). At the end of 3 min of tidal breathing of 100% O2 (or 8 vital-capacity breaths), the FRC holds ~2.5 L of oxygen. Combined with the ~1.5 L normally dissolved in blood bound to haemoglobin (at Hb 150 g/L, fully saturated), this provides a total body oxygen store of ~4 L. At a metabolic consumption of ~250 mL/min, that gives ~16 min of total body oxygen reserve in theory — but in practice the patient desaturates much faster because:[7]
- The FRC mixes with shunted/poorly ventilated alveoli.
- Critically ill patients have reduced FRC (obesity, pregnancy, splinting, ARDS, pulmonary oedema, atelectasis).
- Critically ill patients have increased metabolic demand (sepsis, fever, agitation — Vo2 may be 400-500 mL/min).
- Critically ill patients have increased shunt (pneumonia, ARDS, pulmonary oedema — venous admixture bypasses alveolar gas).[1]
Result: the healthy, fasted patient tolerates ~8-10 min of apnoea before desaturation; the critically ill ICU patient often desaturates in 30-90 seconds. This is why pre-oxygenation alone is often insufficient and why apnoeic oxygenation (continuous oxygen delivery during the apnoeic phase) is so important.[7]
[7] [7]Apnoeic oxygenation — extending the safe window
Apnoeic oxygenation exploits the fact that during apnoea, the alveoli continue to absorb oxygen into the blood (~250 mL/min) faster than CO2 is added back (~10-15 mL/min), creating a sub-atmospheric intrapulmonary pressure that draws gas down the trachea into the alveoli. If you provide a continuous source of 100% O2 at the glottis opening (via nasal cannula or HFNO), oxygen is drawn into the alveoli as fast as it is removed — extending the safe apnoea period by many minutes. Limitation: CO2 continues to rise (~0.4-0.8 kPa/min, ~3-6 mmHg/min) — eventually respiratory acidosis becomes severe (pH <7.0 at ~20 min). So apnoeic oxygenation buys time for intubation; it is NOT a substitute for ventilation.[7]
RSI pharmacology — what to give, when, and to whom
The drug component of RSI is two agents given in rapid sequence (the induction agent followed immediately by the paralytic — through the same IV line, flushed with saline). The choice depends on the patient's physiology.[7]
Induction agents
The induction agent renders the patient unconscious and amnestic. In critically ill patients, the choice of agent and the dose are dominated by haemodynamic considerations: most induction agents cause vasodilation and myocardial depression, which in a shocked patient can precipitate cardiovascular collapse. The general rule in ICU: reduce the induction dose by 30-50% in the critically ill — they are far more sensitive than the healthy elective patient.[1]
[2] [7]Neuromuscular blocking agents (NMBAs / muscle relaxants)
The paralytic agent produces the apnoea and optimal intubating conditions required for RSI. Choice is between rocuronium (the modern default) and suxamethonium (the historical default with a faster offset but a much longer list of contraindications).[7]
[7] [11] [6]Vasopressors and haemodynamic preparation
The peri-induction period is the highest-risk moment for cardiovascular collapse. Every ICU intubation should be preceded by explicit haemodynamic preparation:[1][2]
- IV fluid bolus (250-500 mL crystalloid) — unless clearly volume-overloaded (pulmonary oedema, RV failure). The aim is to improve preload before induction abolishes venous tone.
- Reduce induction dose by 30-50% in any shocked/volume-depleted patient.
- Draw up vasopressor boluses BEFORE induction: noradrenaline 4-8 mcg boluses, or push-dose adrenaline (10 mcg/mL), or phenylephrine 50-100 mcg. Give prophylactically if MAP borderline or reactively to any drop.
- Have an infusion running or ready — start noradrenaline early if shock.
- Peri-intubation arterial line if available — beat-to-beat BP allows immediate detection of and response to hypotension.[6]
Difficult airway prediction — anticipate, do not discover
The DAS/ICS 2018 guidelines stress that the difficult airway should be ANTICIPATED and prepared for, not discovered after induction. Two bedside scores dominate practice: the LEMON law (rapid, originally from emergency medicine) and the MACOCHA score (validated specifically for ICU).[1][6]
LEMON law
[4]MACOCHA score — the ICU-specific prediction score
The MACOCHA score (De Jong 2013) was developed and validated specifically in ICU patients. A score ≥3 predicts a difficult intubation with sensitivity ~73% and specificity ~84%. It is the most validated ICU airway score.[6]
[6]A patient with a high MACOCHA score should be intubated by the most experienced operator available with video laryngoscopy, bougie ready, and plans B and C set up. If the score is very high (≥6) and the patient is sufficiently cooperative, consider awake fibreoptic intubation instead of RSI.[6]
Difficult mask ventilation predictors
Predicting the airway is only half the challenge — predicting difficult mask ventilation is equally important (because mask ventilation is your safety net between induction and intubation). The mnemonic is 'MOANS': Mask seal (beard, obesity, facial trauma), Obstruction, Age >55, No teeth (edentulous — poor mask fit, paradoxically improves once ETT in), Stiff lungs (obesity, ARDS, COPD, asthma). The patient who is BOTH difficult to intubate AND difficult to mask-ventilate is the patient at highest risk of CICO.[3]
Video laryngoscopy vs direct laryngoscopy
Video laryngoscopy (GlideScope hyperangulated blade, C-MAC Macintosh blade with camera) gives a better glottic view than direct laryngoscopy, particularly in patients with predicted difficulty (cervical immobilisation, anterior larynx, blood/secretions, obesity). The view is improved because the camera is at the tip of the blade — the operator does not need a direct line of sight past the tongue.[4]
However, the MACMAN trial (Lascarrou 2020, NEJM) — a multicentre RCT of video vs direct laryngoscopy for non-experienced operators in ICU — found NO difference in first-attempt intubation success (video 99/300 = 33% first-pass failure vs direct 96/300 = 32%, NS). The interpretation: video laryngoscopy improves the VIEW but does not necessarily translate to easier tube PASSAGE — the hyperangulated blade requires a different (and learnable) skill to direct the ETT through the cords (often requiring a rigid stylet or tube-shaping).[4]
[4] [4]The bougie — first-line in any difficult view
The gum-elastic bougie (now usually a single-use polyethylene bougie) is the workhorse rescue device. It is passed (often 'blind') through the cords before the ETT is railroaded over it. The DRIVER trial (Driver 2018, JAMA) randomised 757 critically ill adults to bougie-first vs ETT-with-stylet first. In patients with at least one difficult airway predictor, the bougie-first strategy gave significantly higher first-pass intubation success (96% vs 82%, absolute risk reduction 14%).[5]
Bougie technique — practical points for ICU RSI
When to use
ROUTINELY use the bougie as the first device for ANY predicted difficult airway (LEMON/MACOCHA positive), any grade 2b-3-4 view, or if first direct attempt failed. The bougie is cheap, ubiquitous, and almost always helps — the only situation where it does not is a true grade 4 view (no epiglottis visible — see below).
Passing the bougie
Direct the angled tip of the bougie ANTERIORLY under the posterior aspect of the epiglottis (or under the arytenoids if you cannot see the cords). Look for the "clicks" — the bougie tip clicks over the tracheal rings as it advances (palpable and sometimes audible). Then the "hold-up" sign — the bougie meets resistance at the carina or small bronchus (~30 cm). DO NOT force.
Railroading the ETT
Keep the laryngoscope IN to maintain displacement of the tongue and soft tissues. Have an assistant thread the ETT over the bougie. Rotate the ETT 90° ANTICLOCKWISE as it passes through the cords (the bevel faces posteriorly — reduces arytenoid impingement and vocal cord trauma). Advance to ~23 cm (8.0 ETT) or ~21 cm (7.0 ETT) at the teeth.
Confirm
Remove bougie. Attach ETCO2. Inflate cuff. Confirm continuous waveform capnography. Auscultate both axillae. Secure.
Trap
The ETT may "hang up" on the right arytenoid (the most common railroading failure) — rotate anticlockwise. If repeated failure, withdraw ETT and bougie TOGETHER (do not pull the bougie out of the trachea) and reattempt.
Peri-intubation cardiac arrest — the preventable disaster
Cardiovascular collapse during induction is the most common life-threatening complication of ICU intubation and is largely preventable. The INTUBE study found cardiovascular instability in 43% and cardiac arrest in ~3% of ICU intubations.[2]
Mechanism: induction agents abolish the sympathetic tone that maintains blood pressure in the shocked patient. Combined with loss of venous return from positive-pressure ventilation, hypovolaemia, and the underlying shock state, this precipitates severe hypotension, loss of coronary perfusion, and cardiac arrest. Risk factors: pre-induction hypotension (MAP <65), severe hypoxaemia, shock of any cause (especially distributive and cardiogenic), metabolic acidosis, older age, obesity, hypovolaemia, high induction dose, propofol/thiopentone use in shock.[2]
Prevent peri-intubation cardiac arrest — the haemodynamic bundle
Optimise BEFORE induction
The window between decision-to-intubate and induction is your chance to make the patient safe. Do NOT proceed to induction with MAP <65 or in untreated shock. Resuscitate first: fluid bolus (250-500 mL crystalloid unless clearly overloaded), vasopressor infusion (noradrenaline — start early), transfuse if anaemic (target Hb ≥70 g/L, ≥80 in ischaemic heart disease), correct severe acidosis/metonutrition if feasible.
Reduce induction dose
Halve the dose of propofol/thiopentone in any shocked patient (e.g., propofol 0.5-1 mg/kg instead of 2 mg/kg). Use ketamine as default in shock (1-2 mg/kg, or 0.5-1 mg/kg in profound shock). Consider co-induction (low-dose midazolam 1-2 mg + low-dose ketamine) — synergistic amnesia at lower doses.
Draw up push-dose vasopressors
Have noradrenaline boluses (4-8 mcg) or push-dose adrenaline (10 mcg/mL — dilute 1 mL of 1:1000 adrenaline in 100 mL saline) drawn up and labelled. Give prophylactically if MAP borderline, or reactively at the first sign of BP drop. Phenylephrine (50-100 mcg) is an alternative in tachycardic patients.
Minimise apnoea time
Plan and brief the team so the interval from induction to confirmed intubation is minimised. Pre-oxygenate well. Have all equipment ready. Have a clear Plan A-B-C trajectory. The PrePARE trial (Casey 2019, NEJM) showed that gentle bag-mask ventilation between induction and intubation does NOT increase aspiration in critically ill adults (vs no mask ventilation) and reduces hypoxaemia — so mask ventilation during apnoea (if not contraindicated, e.g., active vomiting) is acceptable and reduces desaturation-related complications.
Arterial line if unstable
Beat-to-beat BP monitoring during induction allows immediate detection of and response to hypotension. Insert BEFORE induction in any unstable patient if feasible.
Difficult airway algorithm — Plans A, B, C, D
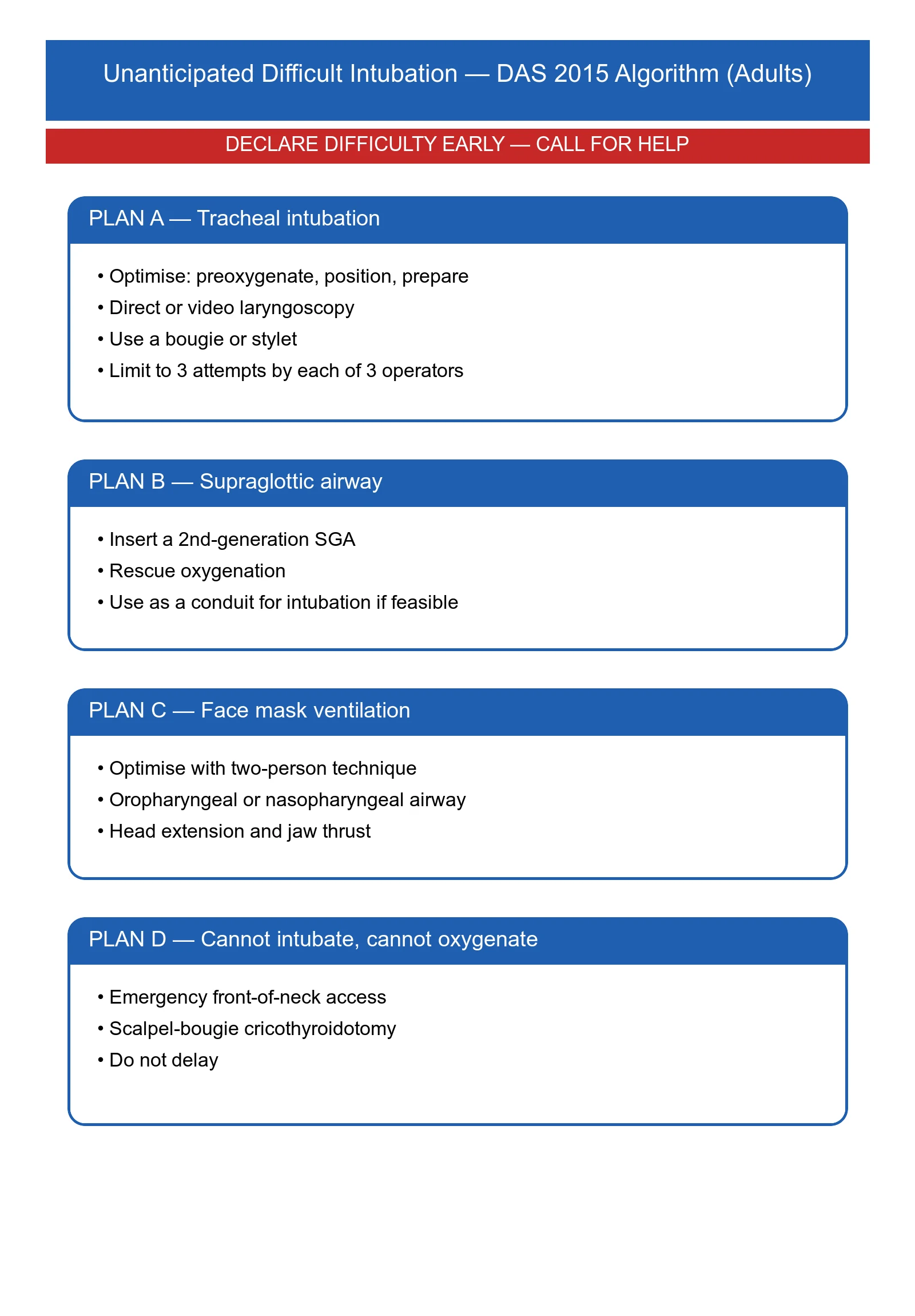
The DAS 2015 guidelines for the unanticipated difficult intubation (the 'intubation has started, you didn't expect difficulty' scenario) and the DAS/ICS 2018 ICU guidelines define a sequential algorithm. The principle: maintain oxygenation at every step, declare failure early, escalate without delay.[1][3]
DAS Plans A-D for the difficult airway in ICU
Plan A — primary laryngoscopy + bougie
Pre-oxygenate → induction + paralytic → direct or video laryngoscopy. Optimise the first attempt: best position (sniffing position unless c-spine), external laryngeal manipulation (BURP — backward-upward-rightward pressure — better than cricoid pressure for view), bougie ready. If first attempt fails, declare failure and call for help EARLY.
Limit attempts
Maximum of 3 attempts by an experienced operator. Each attempt worsens trauma, oedema, bleeding — turning a manageable airway into a surgical airway. Between attempts, mask-ventilate to restore SpO2 (or HFNO/THRIVE).
Plan B — supraglottic airway (i-gel / LMA)
Insert a second-generation supraglottic airway (i-gel preferred — better seal, drain tube, no cuff to inflate). If oxygenation restored through the SGA, you have three options: (a) wake the patient (if reversible anaesthesia); (b) intubate THROUGH the SGA (fibreoptic through i-gel); (c) continue with SGA as definitive airway (suboptimal — proceed to tracheal intubation when feasible).
Plan C — definitive failure to maintain oxygenation → CICO
If you cannot maintain SpO2 >90% with mask ventilation or SGA, you are in CICO (see below). Do NOT delay.
Plan D — emergency front of neck access (eFONA)
Scalpel-bougie cricothyroidotomy — see dedicated section below. This is the final common pathway of the failed airway.
Wake up
If at any point oxygenation is maintained and the patient is sufficiently stable, ABANDON the intubation and wake the patient. Returning to spontaneous ventilation and awake techniques (fibreoptic) is the safest course when the airway is unexpectedly difficult. This is a legitimate and respected decision.
CICO and emergency front of neck access (eFONA)
CICO (can't intubate, can't oxygenate) is the airway emergency to end all airway emergencies. It occurs when (a) you cannot intubate (failed Plan A), (b) you cannot oxygenate via mask or supraglottic airway (failed Plans B), and (c) the patient's SpO2 is falling. From the moment of CICO declaration, the patient has 1-5 minutes before irreversible hypoxic brain injury, then death. There is no time for deliberation or committee.[3]
The DAS 2015 guideline and ANZCA recommend the scalpel-bougie technique for eFONA — it is faster, simpler, and more reliable than the cannula (needle) cricothyroidotomy technique, which has a high failure rate. The technique is performed through the cricothyroid membrane — the easiest and most superficial access point to the trachea.[3]
eFONA — scalpel-bougie cricothyroidotomy (the DAS technique)
Identify the cricothyroid membrane
Palpate the laryngeal landmarks. Find the thyroid notch (Adam's apple) superiorly, the cricoid cartilage inferiorly. The depression BETWEEN them is the cricothyroid membrane. In obese patients or those with distorted anatomy, use ultrasound if immediately available — but do NOT delay for ultrasound if you can palpate the membrane.
Position the patient
Neck extension if c-spine cleared; otherwise maintain in-line stabilisation. The assistant provides jaw thrust and laryngeal manipulation to bring the larynx forward.
Stabilise the larynx
With your NON-DOMINANT hand, grasp the larynx with the thumb and middle finger (laryngeal handshake) — this stabilises the larynx and prevents it from rotating during the incision. Keep this hand in place until the tube is in.
Incise
With the DOMINANT hand, use a scalpel (size 10 or 20 blade) to make a TRANSVERSE incision through the skin AND cricothyroid membrane in one movement, in the lower part of the membrane (to avoid the cricothyroid artery which runs along the upper border). You will feel a "give" as the blade enters the trachea.
Maintain the opening
TURN THE BLADE 90° (so the flat of the blade faces the patient's feet) — this opens the hole in the trachea. Alternatively, slide a bougie alongside the blade into the trachea.
Pass the bougie
Slide an elastic bougie through the incision into the trachea, angled caudally (towards the feet). It should pass easily — if resistance, withdraw slightly and re-angle. Aim down the posterior wall of the trachea.
Railroad the ETT
Pass a size 6.0 cuffed ETT over the bougie and into the trachea. Inflate the cuff. Remove the bougie. Attach the circuit.
Confirm
Waveform capnography — must see a CO2 trace. Bilateral chest rise. Auscultate. Secure the tube. Convert to a formal surgical airway (tracheostomy) when stable.
VAP prevention after intubation — the post-intubation bundle
Once the ETT is secured and the patient is ventilating, attention turns to preventive care. Ventilator-associated pneumonia (VAP) develops in ~10-20% of intubated ICU patients, increases ICU stay by 4-9 days, and is associated with attributable mortality of ~13%. The 'VAP bundle' (or 'ventilator care bundle') is a group of evidence-based interventions that, applied together, reduce VAP rates dramatically. Many components also reduce other ICU complications.[11]
[8] [6]SAQ — Rapid sequence induction in the haemodynamically unstable ICU patient
10 minutes · 10 marks
A 72-year-old man with severe community-acquired pneumonia is in septic shock (MAP 55 on noradrenaline 0.3 mcg/kg/min, lactate 4.2, SpO2 88% on 15 L/min via non-rebreather) and requires intubation for worsening type 1 respiratory failure. He is obese (BMI 36), has a beard, and short neck. He has no allergies and his last meal was 6 hours ago. The team is assembled with a video laryngoscope, a difficult-airway trolley, and a second-generation supraglottic airway.
SAQ — Apnoeic oxygenation, safe apnoea time, and the difficult paediatric airway
10 minutes · 10 marks
A 3-year-old child (weight 14 kg) is admitted to ICU with severe epiglottitis and impending upper-airway obstruction. He is sitting forward, drooling, with stridor and suprasternal recession. He is maintaining SpO2 92% on 10 L/min oxygen. The paediatric anaesthetist is 30 minutes away.
Clinical pearls
Red flags
[5] [5] [11] [6] [4] [5] [5]Key trials and evidence
INTUBE study — peri-intubation adverse events (PMID 32873211)
MACMAN trial — video vs direct laryngoscopy in ICU (PMID 32402170)
DRIVER trial — bougie vs stylet for first attempt (PMID 30407057)
PrePARE trial — bag-mask ventilation during RSI (PMID 30208792)
THRIVE — apnoeic oxygenation with high-flow nasal O2 (PMID 26043238)
MACOCHA — ICU difficult airway prediction score (PMID 23632072)
DAS/ICS 2018 guidelines — intubation in the critically ill (PMID 29102870)
Prognosis and outcomes
[3]The determinants of outcome after ICU intubation are: (1) the underlying illness (the biggest factor — intubation is a marker of severity); (2) the avoidance of preventable complications (peri-intubation cardiac arrest, severe hypoxaemia, oesophageal intubation, aspiration) — these are what the intensivist can influence; (3) the appropriate use of a checklist, team briefing, and pre-prepared rescue plans.[1][2]
References
- [1]Higgs A, McGrath BA, Goddard C, et al. Guidelines for the management of tracheal intubation in critically ill adults. British journal of anaesthesia, 2018.PMID 29406182
- [2]Russotto V, Myatra SN, Laffey JG, et al. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA, 2021.PMID 33755076
- [3]Frerk C, Mitchell VS, McNarry AF, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. British journal of anaesthesia, 2015.PMID 26556848
- [4]Prekker ME, Driver BE, Trent SA, et al. DirEct versus VIdeo LaryngosCopE (DEVICE): protocol and statistical analysis plan for a randomised clinical trial in critically ill adults undergoing emergency tracheal intubation. BMJ open, 2023.PMID 36639210
- [5]Driver BE, Semler MW, Self WH, et al. Effect of Use of a Bougie vs Endotracheal Tube With Stylet on Successful Intubation on the First Attempt Among Critically Ill Patients Undergoing Tracheal Intubation: A Randomized Clinical Trial. JAMA, 2021.PMID 34879143
- [6]De Jong A, Molinari N, Terzi N, et al. Early identification of patients at risk for difficult intubation in the intensive care unit: development and validation of the MACOCHA score in a multicenter cohort study. American journal of respiratory and critical care medicine, 2013.PMID 23348979
- [7]Patel A, Nouraei SA Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia, 2015.PMID 25388828
- [8]Jaber S, Jung B, Corne P, et al. An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive care medicine, 2010.PMID 19921148
- [10]Sklar MC, Lapinsky SE, Parotto M Bag-Mask Ventilation during Tracheal Intubation of Critically Ill Adults. The New England journal of medicine, 2019.PMID 31216409
- [11]Klompas M, Branson R, Eichenwald EC, et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infection control and hospital epidemiology, 2014.PMID 25376073