ICU · Airway management
Rapid Sequence Intubation (RSI) & Its Drugs
Also known as Rapid sequence intubation · RSI · RSI drugs · Rapid sequence induction · Succinylcholine · Rocuronium · Sugammadex · Etomidate · Cricoid pressure · Sellick manoeuvre · First-pass success · Preoxygenation · Apnoeic oxygenation · THRIVE · HFNC · KETASED · Video laryngoscopy · Peri-intubation cardiac arrest · Sugammadex · INTUBE study · Peri-intubation hypotension
Rapid sequence intubation (RSI) is the standard for emergency airway control in the non-fasted, critically ill patient: preoxygenation, then an induction agent and a neuromuscular blocker in rapid succession with no mask ventilation, to secure the airway swiftly and minimise aspiration. Induction agents are chosen to the haemodynamics (propofol/thiopentone in the stable; ketamine in shock/asthma; etomidate for neutrality, with the sepsis-adrenal controversy). Succinylcholine (fast, short, but hyperkalaemia and malignant hyperthermia) versus rocuronium (reversible with sugammadex). Confirm with waveform capnography. Cricoid pressure is no longer routine.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
Rapid sequence intubation (RSI) is the standard technique for emergency endotracheal intubation in the critically ill, non-fasted patient. The principle is to render the patient unconscious and paralysed as swiftly as possible — minimising the window of risk — by giving an induction agent and a neuromuscular blocker in rapid succession, after thorough preoxygenation and with no mask ventilation between, so that the airway is secured before regurgitation and aspiration can occur.[3][4]
The goal is first-pass success: the tube through the cords, cuff inflated, and ventilation confirmed on the first attempt. Repeated attempts cause hypoxia, airway trauma, regurgitation, and cardiovascular collapse.[3]

The RSI sequence
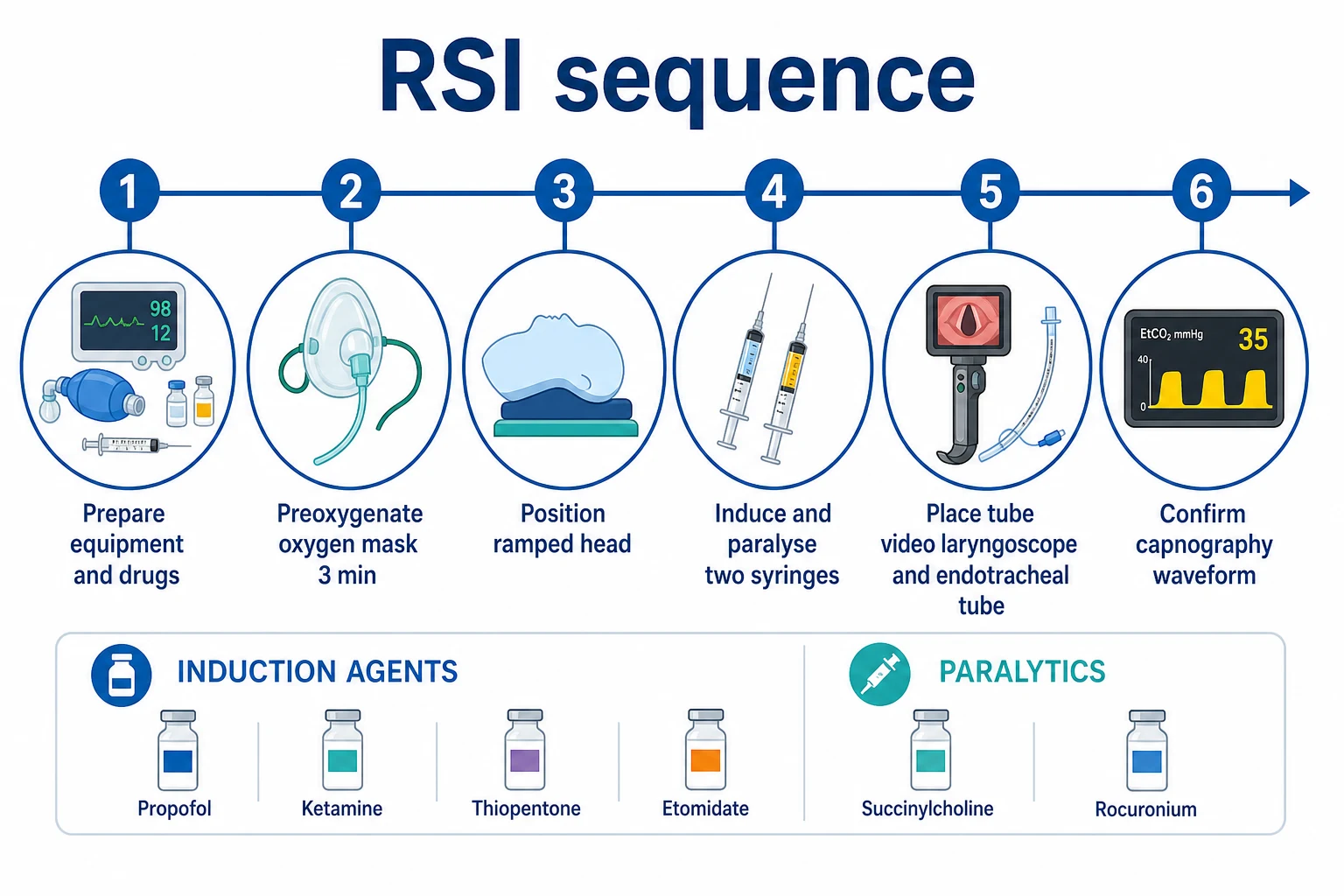
The sequence is taught as a series of structured steps:[3][4]
- Prepare — equipment checked (working suction, endotracheal tube with a tested cuff, syringe, bougie, video laryngoscope with a charged blade, supraglottic airway as rescue, tube tie), drugs drawn up and labelled, monitoring attached (ECG, SpO2, non-invasive blood pressure cycling every 2-3 min, capnography), intravenous access, and a clear back-up plan for failed intubation.
- Preoxygenate — denitrogenate the functional residual capacity with 100 per cent oxygen for about 3 minutes of tight-mask breathing, or 8 vital-capacity breaths. In the hypoxaemic patient, preoxygenate with non-invasive ventilation (or continuous positive airway pressure) and apply nasal apnoeic oxygen (high-flow nasal cannula) during the apnoeic period. This builds the apnoea reserve that buys time.
- Position — ramp the patient so the external auditory meatus is level with the sternal notch (the "sniffing" position), with the head elevated in the obese. Good position is a major determinant of laryngoscopic view.
- Induce and paralyse — give the induction agent, immediately followed by the neuromuscular blocker, in rapid succession. Do not ventilate by mask between (the crux of "rapid sequence"). Wait for the onset of paralysis (about 45-60 seconds).
- Place the tube — laryngoscopy (video laryngoscope first-line in many ICU patients), pass the tube through the cords, inflate the cuff.
- Confirm and secure — waveform capnography is the gold standard for confirming tracheal placement (a persistent CO2 trace over several breaths); also confirm with bilateral chest rise and auscultation. Then secure the tube, note the depth at the teeth, and check a chest X-ray.[4]
Induction agents
Choose the agent to the haemodynamics and the underlying state.[3]
- Propofol — smooth, fast onset; a potent negative inotrope and vasodilator, so it causes hypotension — reduce the dose or avoid in cardiovascular instability.
- Thiopentone (thiopental) — the classic RSI barbiturate; fast and smooth, but also causes hypotension and is a negative inotrope; reduces cerebral metabolic rate and intracranial pressure (useful in raised ICP).
- Ketamine — a dissociative anaesthetic that preserves blood pressure through sympathetic stimulation (a catecholamine-sparing agent), and is a bronchodilator. It is the agent of choice in shock and in asthma. It transiently raises heart rate and blood pressure; the traditional concern about raising intracranial pressure is now thought to be clinically modest, and ketamine should not be withheld in TBI if it is the best haemodynamic choice.
- Etomidate — haemodynamically neutral, which makes it attractive in the unstable patient, but it inhibits 11-beta-hydroxylase and causes adrenal suppression. This is the sepsis controversy (see below).
- Fentanyl / midazolam — used as adjuncts or in reduced doses, less reliably a rapid induction on their own.[2]
The etomidate–sepsis controversy
Etomidate suppresses the adrenal axis even after a single dose, and because adrenal insufficiency is harmful in septic shock, whether etomidate increases mortality in sepsis has been debated for two decades:[1][2]
- One meta-analysis found etomidate is associated with mortality and adrenal insufficiency in sepsis (Chan, Critical Care Medicine 2012).[2]
- A later, larger meta-analysis found that a single dose does not increase mortality in patients with sepsis (Gu and Wang, Chest 2015).[1]
Current practice varies: many intensivists still use etomidate for its haemodynamic stability, while others prefer ketamine in septic shock and reserve etomidate. The pragmatic position is that the single-dose mortality signal is weak and inconclusive, but the adrenal effect is real — weigh it against the greater harm of induction-induced hypotension.[1][2][3]
Neuromuscular blockers
- Succinylcholine (suxamethonium) — a depolarising blocker; rapid onset (30-60 seconds) and short duration (5-10 minutes), which makes it ideal for RSI: if intubation fails, the patient resumes breathing quickly. Contraindications: the hyperkalaemic states (burns beyond 24 hours, crush injury, renal failure with hyperkalaemia, denervating states, prolonged immobility), malignant hyperthermia, pseudocholinesterase deficiency (prolonged paralysis), and bradyarrhythmias (especially in children). It briefly raises serum potassium by about 0.5 mmol/L.[3]
- Rocuronium — a non-depolarising blocker; at RSI doses (about 1.0-1.2 mg/kg) it has an onset close to succinylcholine (around 60 seconds) but a much longer duration (40-60 minutes). It carries no hyperkalaemia or malignant-hyperthermia risk and is the alternative when succinylcholine is contraindicated. Crucially, rocuronium is fully reversible with sugammadex (16 mg/kg for immediate reversal), which is the pharmacological rescue in a failed RSI that cannot be intubated or oxygenated — a major reason rocuronium is now the default paralytic in many ICUs.[3][4]
A key principle: paralyse the patient fully for RSI. Intubating a partially relaxed, gagging patient causes worse views, more trauma, and failed first attempts.[3]
Cricoid pressure (Sellick)
Cricoid pressure — downward force on the cricoid cartilage to occlude the oesophagus and prevent regurgitation — was once routine. Current evidence shows no benefit and possible harm (difficulty with laryngoscopy, worsened view), and recent large trials and guideline updates recommend it not be used routinely. If applied, release it if it impairs the view.[4]
Special situations
- The shocked patient — reduce the induction dose (e.g. ketamine, or a reduced dose of propofol/thiopentone); have a vasopressor drawn up and ready; preoxygenate aggressively. Cardiovascular collapse at induction is common and dangerous.[3]
- Asthma — ketamine (bronchodilator); avoid a tube that is too small; beware breath-stacking and auto-PEEP.[3]
- Raised intracranial pressure — thiopentone or propofol (reduce cerebral metabolic rate); avoid hypotension and hypoxia (both worsen secondary brain injury); rocuronium is often preferred over succinylcholine to avoid the transient ICP rise and coughing.[3]
- Cardiac arrest — this is a "crash" airway, not an RSI: intubate without induction drugs.[3]
Complications
The common and dangerous complications are cardiovascular collapse (from the induction agent in a vasodilated, hypovolaemic patient), hypoxia (from inadequate preoxygenation or prolonged attempts), aspiration, oesophageal intubation (caught by capnography), multiple failed attempts, and cardiac arrest. Most are preventable with preparation, preoxygenation, correct dosing, and limiting to a planned number of attempts before escalating to a supraglottic airway or front-of-neck access.[3][4]
[1]Red flags
Preoxygenation in depth — the physiological foundation of safe apnoea
Preoxygenation is the single most important step that determines how long the patient can tolerate apnoea before desaturation. Done well it buys minutes; done poorly the patient desaturates within 30-90 seconds, forcing a rushed, dangerous intubation. The physiological goal is to denitrogenate the functional residual capacity (FRC) — the ~2.5-3 L of gas left in the lungs at end-expiration — replacing the 79 per cent nitrogen with oxygen, creating a reservoir that diffuses into the pulmonary capillary blood as oxygen is consumed.[11][3]
In a healthy 70 kg adult breathing room air, the FRC holds about 1.5 L of oxygen (FRC × 21 per cent). After thorough preoxygenation with 100 per cent oxygen, the FRC holds nearly 3 L of pure oxygen. At a resting oxygen consumption of ~250 mL/min, this reservoir supports 8-10 minutes of safe apnoea in the ideal patient. The critically ill patient, however, has a far smaller reserve — a reduced FRC (recumbency, atelectasis, obesity, pregnancy, splinting), increased oxygen consumption (sepsis, fever, agitation, shivering), shunt physiology (pneumonia, pulmonary oedema, ARDS), and anaemia (less oxygen carried per decilitre). In these patients desaturation below 90 per cent can occur in under a minute.[13][3]
Methods of preoxygenation
Two techniques achieve near-complete denitrogenation and are considered equivalent:[11][3]
- 3 minutes of tidal-volume breathing (TVB) of 100 per cent oxygen through a tight-fitting mask with a reservoir bag, the circuit flushed at high flow (≥10-15 L/min). This is the conventional, reliable method and reaches an end-tidal oxygen (ETO2) of 80-90 per cent.
- 8 vital-capacity breaths of 100 per cent oxygen over about 60 seconds. Vital-capacity breathing denitrogenates faster because each large breath turns over a greater fraction of the FRC; eight such breaths produce equivalent denitrogenation to three minutes of tidal breathing. This is useful when the patient cannot cooperate with three minutes of breathing or when time is short, but it requires a cooperative patient who can take deep breaths.[10]
An end-tidal oxygen concentration above 80-90 per cent is the objective marker of adequate denitrogenation where capnography also reads ETO2; if available, it confirms readiness. In practice, most ICUs rely on time (3 minutes) and clinical observation (the reservoir bag does not collapse, the mask seals well, the patient is calm).[7]
Special populations where standard preoxygenation is inadequate
Several patient groups desaturate quickly and need augmented preoxygenation:[11][13]
- The hypoxaemic patient (SpO2 < 92-93 per cent on a high-FIO2 mask) cannot be denitrogenated effectively with a simple mask — the underlying shunt continues to admix deoxygenated blood. Use non-invasive ventilation (NIV) or continuous positive airway pressure (CPAP) for preoxygenation. NIV at IPAP 10-15 / EPAP 5-8 cmH2O, FIO2 1.0, recruits collapsed alveoli and improves oxygenation during the preoxygenation period. Several randomised trials (Baillard, De Jong) show NIV preoxygenation markedly reduces desaturation compared with a reservoir mask in hypoxaemic patients.
- The obese patient — the FRC is markedly reduced by the weight of the abdominal contents against the diaphragm in recumbency. Ramp the patient (pillows/trochanter roll to elevate the head and shoulders so the external auditory meatus is level with the sternal notch), and consider 25-30° reverse Trendelenburg. Apply PEEP via mask (CPAP 7-10 cmH2O) during preoxygenation. The combination of ramping and positive pressure restores FRC and doubles safe apnoea time.
- The pregnant patient — FRC is reduced (the gravid uterus elevates the diaphragm) and oxygen consumption is increased (20 per cent above baseline). Desaturation is rapid — within 60 seconds of apnoea. Preoxygenate to an ETO2 above 90 per cent, position with left lateral tilt or manual uterine displacement, and have a difficult-airway plan in place. Pregnancy is a difficult airway by default: oedema, friable mucosa, and reduced mobility of the larynx.
- The septic patient — high oxygen consumption, often anaemic, shunt from pulmonary involvement, and vasoplegia. Preoxygenate with 100 per cent oxygen via NIV/CPAP rather than a mask, optimise haemoglobin and haemodynamics before induction if possible, and apply apnoeic oxygenation throughout.
- Children — a proportionally smaller FRC and a higher metabolic rate mean desaturation is faster still. Preoxygenate meticulously and have a lower threshold to mask-ventilate between attempts.[10]
Apnoeic oxygenation and THRIVE
Apnoeic oxygenation exploits the fact that alveolar gas is continuously removed into the blood (oxygen consumption ~250 mL/min) faster than it is replaced (CO2 production ~200 mL/min), generating a net sub-atmospheric alveolar pressure that draws gas down the trachea. If a high flow of oxygen is provided at the airway opening — typically via high-flow nasal cannula (HFNC) at 30-70 L/min, fully humidified, FIO2 1.0 — oxygen is drawn into the alveoli as it is consumed, prolonging safe apnoea time substantially. This is the principle behind THRIVE (Transnasal Humidified Rapid-insufflation Ventilatory Exchange).[10][7]
THRIVE extends safe apnoea time from the conventional 3-8 minutes to over 30-60 minutes in selected patients (Patel 2015 — median apnoea time 14 minutes in difficult-airway patients with no desaturation). Carbon dioxide continues to rise (~3-6 mmHg per 10 minutes) — apnoeic oxygenation does not ventilate, and respiratory acidosis eventually becomes problematic — but the oxygenation benefit is real and large.[10]
Important caveats and contraindications to apnoeic nasal oxygenation:[11]
- Apnoeic oxygenation fails where there is significant shunt or low V/Q — the oxygen reaching the alveoli does not reach the blood. In severe pneumonia, ARDS, or pulmonary oedema, THRIVE does not reliably prevent desaturation, and the patient may still crash. Do not trust THRIVE alone in a hypoxaemic patient.
- HFNC is best used as an adjunct, not a substitute for mask preoxygenation or ventilation. The recommended combination is mask preoxygenation with HFNC running underneath (nasal prongs at 30-70 L/min under the mask), continued through induction and the apnoeic period.
- In patients with high airway obstruction or risk of gastric insufflation (bowel obstruction, recent meal), high-flow nasal oxygen is theoretically safe (it escapes around the catheter), but be cautious.
- THRIVE can mask the urgency of re-oxygenation: SpO2 stays high while CO2 climbs, so the team can be lulled into prolonged apnoea. Set a hard time limit (the team calls out time from induction) and ventilate (mask or tube) by 5-10 minutes regardless of SpO2.
- Standard low-flow nasal cannula at 2-6 L/min does not deliver meaningful apnoeic oxygenation in adults and should not be relied upon; the flow is too low to overcome the resistance of the nasal cavity and pharynx. The benefit is achieved at flows of 30-70 L/min (HFNC/Optiflow/Nasal High Flow).[10]
Induction agents — pharmacology in detail
The induction agent is chosen to the haemodynamic state and the underlying condition. There is no perfect agent; each has trade-offs. The cardinal rule is that all induction agents cause some cardiovascular depression, and the critically ill patient — vasodilated, hypovolaemic, with exhausted sympathetic reserve — tolerates that depression far worse than the elective patient. Reduce the dose in any unstable patient.[3][15]
| Agent | Typical RSI dose | Onset | Duration | Haemodynamic effect | Best use |
|---|---|---|---|---|---|
| Propofol | 1-2 mg/kg (0.5-1 mg/kg in shock) | 30-60 s | 5-10 min | Marked vasodilation and negative inotropy — hypotension | Stable, normotensive patient; seize/status; reduce ICP |
| Thiopentone | 3-5 mg/kg (1-2 mg/kg in shock) | 30-60 s | 5-10 min | Negative inotropy, venodilation — hypotension; reduces CMR/ICP | Raised ICP, status epilepticus; avoid in shock |
| Ketamine | 1-2 mg/kg (0.5-1 mg/kg in profound shock) | 45-60 s | 10-20 min | Sympathetic stimulation — preserves BP (caution: direct negative inotrope in catecholamine-depleted patient) | Shock, asthma, bronchospasm; safe in TBI |
| Etomidate | 0.2-0.3 mg/kg | 30-60 s | 5-15 min | Haemodynamically neutral — minimal BP change | Haemodynamic instability where adrenal effect acceptable |
| Midazolam | 0.05-0.1 mg/kg (rarely used alone) | 1-2 min | 20-30 min | Mild depression; unreliable as sole agent | Adjunct/co-induction only |
Ketamine — the critical-care induction agent of choice in shock
Ketamine is a phencyclidine derivative producing a dissociative anaesthetic state. It stimulates the sympathetic nervous system (central release of catecholamines), which preserves blood pressure and heart rate — the property that makes it the preferred agent in shock, sepsis, trauma, and bronchospasm. It is also a bronchodilator, useful in asthma and COPD. It does not abolish the airway reflexes as completely as other agents, and salivation and secretions increase (give an anti-sialogogue if awake-fibreoptic).[3][6]
Three historical concerns about ketamine have been largely refuted:[3]
- Emergence phenomena (nightmares, hallucinations on recovery) — uncommon in the critically ill, less so than in the elective population; benzodiazepines reduce them but are not routinely needed in the intubated ICU patient.
- Raised intracranial pressure — ketamine does modestly raise ICP, but it also raises MAP, so cerebral perfusion pressure (CPP = MAP − ICP) is preserved or improved. Modern neuroanaesthesia and neurocritical care have reversed the historical prohibition: ketamine is acceptable in traumatic brain injury when the haemodynamic benefit outweighs the small ICP effect. Do not withhold ketamine in a shocked patient with TBI.
- Direct negative inotropy — in a patient who is catecholamine-depleted (maximal sympathetic drive already), ketamine's indirect sympathomimetic effect is exhausted and the direct depressant effect dominates; profound hypotension can still occur. Give a reduced dose (0.5-1 mg/kg) and have vasopressors ready.[3]
KETASED — ketamine versus etomidate in sepsis
The KETASED trial (Jabre, Lancet 2009) is the landmark study on induction agent choice in septic shock. It randomised 469 critically ill patients with sepsis to ketamine (2 mg/kg) versus etomidate (0.3 mg/kg) for RSI and followed them for 28 days.[6]
KETASED — ketamine vs etomidate for RSI in septic shock (PMID 19589851)
The KETASED result is the pragmatic underpinning of modern practice: a single dose of etomidate, despite measurable adrenal suppression, has not been shown to increase mortality. Ketamine remains a sound default in shock and is increasingly preferred because it preserves blood pressure — the haemodynamic benefit is more reliably useful than the theoretical adrenal harm of etomidate.[6]
Fentanyl as a haemodynamic adjunct
Fentanyl is not an induction agent in its own right, but a small dose (1-3 mcg/kg, or 50-150 mcg in a typical adult) given 1-3 minutes before induction blunts the sympathetic surge of laryngoscopy (rise in blood pressure, heart rate, and ICP) and reduces the dose of induction agent needed. This is useful in:[3][15]
- Aortic stenosis, hypertrophic cardiomyopathy, severe coronary disease, raised ICP — where a sudden hypertensive surge is dangerous.
- The "tight" cardiovascular patient — to avoid tachycardia and hypertension from laryngoscopy.[8]
Fentanyl causes dose-dependent respiratory depression and bradycardia; in the shocked patient a small dose can precipitate hypotension (vagally mediated). Do not rely on fentanyl alone for unconsciousness — it is an analgesic adjunct, not a hypnotic. A common regimen in the haemodynamically stable patient is fentanyl 100 mcg, then propofol 1-2 mg/kg, then the paralytic. In the shocked patient, omit the fentanyl or use a tiny dose, and use ketamine.[6]
Co-induction
Co-induction — combining two or more agents at lower doses — exploits synergy and reduces the dose of each. A typical combination is midazolam 1-2 mg + ketamine 0.5-1 mg/kg + fentanyl 50-100 mcg, providing reliable hypnosis with reduced haemodynamic effect. This is most useful in the elderly or the vasodilated patient where a single full-dose agent would cause dangerous hypotension. The drawback is a slower onset (1-2 minutes) and less reliable timing for the rapid sequence.[6]
Neuromuscular blockers — doses and sugammadex reversal
The paralytic is what makes intubation possible. Paralyse fully — a partially paralysed patient who gags, coughs, or splints makes laryngoscopy harder, not easier, and increases the risk of trauma and failed attempts. The two agents in routine use are succinylcholine (suxamethonium) and rocuronium.[3][4]
| Agent | Class | RSI dose | Onset | Duration | Reversal |
|---|---|---|---|---|---|
| Suxamethonium | Depolarising | 1.5 mg/kg (1.0-2.0 range) | 30-60 s | 5-10 min | None — spontaneous hydrolysis by pseudocholinesterase |
| Rocuronium | Non-depolarising (steroid) | 1.2 mg/kg (1.0-1.2; some use 1.0 mg/kg) | 60-90 s | 40-60 min | Sugammadex 16 mg/kg for immediate reversal |
Succinylcholine — fast and short, but with a long list of contraindications
Suxamethonium is a depolarising blocker (a bis-quaternary ammonium compound structurally similar to acetylcholine) that binds and persistently activates the nicotinic receptor, producing an initial fasciculation followed by flaccid paralysis. It has the fastest onset (30-60 seconds) and shortest duration (5-10 minutes) of any NMBA, which makes it the historical RSI standard: if intubation fails, the patient resumes breathing quickly.[3]
It transiently raises serum potassium by ~0.5 mmol/L (clinically irrelevant in health) and intracranial, intraocular, and intragastric pressure by small amounts. The dangers are:[3]
- Hyperkalaemic response — in the denervated/upregulated states, suxamethonium releases large amounts of potassium (5-10 mmol/L) and can precipitate cardiac arrest. The classic states are: burns beyond 24 hours (peak risk 7-30 days, persists for up to 2 years), crush injury and major trauma, denervating syndromes (spinal cord injury, stroke, Guillain-Barré, MS, MND) after 72 hours to 6 months, prolonged immobility, severe intra-abdominal sepsis, renal failure with existing hyperkalaemia, and rhabdomyolysis. The risk window opens 24-72 hours after the insult and persists for many months.
- Malignant hyperthermia — suxamethonium is a potent trigger. Suspect in any post-induction hypermetabolic crisis (rising ETCO2, hyperkalaemia, rigidity, fever); treat with dantrolene 2.5-10 mg/kg and active cooling. Rocuronium does not trigger MH.
- Pseudocholinesterase (plasma cholinesterase) deficiency — a genetic variant (1 in 2,500 homozygous) leads to prolonged paralysis lasting 4-8 hours rather than 5-10 minutes. There is no reversal; supportive ventilation until recovery.
- Bradycardia — repeated doses cause vagal bradycardia; an anticholinergic (atropine) is given for repeat dosing in children.
- Anaphylaxis — NMBAs are the leading cause of anaesthetic anaphylaxis, and suxamethonium is the most implicated.[1]
Rocuronium — the modern default, fully reversible
Rocuronium is a non-depolarising (steroid) NMBA. At the high RSI dose of 1.2 mg/kg it has an onset approaching suxamethonium (60-90 seconds) and a duration of 40-60 minutes. It carries no hyperkalaemia risk and does not trigger malignant hyperthermia, and it does not raise ICP/ICP/IOP. The decisive advantage is that rocuronium is fully and rapidly reversed by sugammadex, a modified gamma-cyclodextrin that encapsulates and inactivates the rocuronium molecule.[3][4]
[8]Sugammadex — the failed-RSI rescue
Sugammadex 16 mg/kg encapsulates rocuronium and reverses profound paralysis within 1-3 minutes — the pharmacological rescue in a "can't intubate, can't oxygenate" (CICO) situation where rocuronium was used. This has transformed the calculus of RSI: with sugammadex available, rocuronium can be used as the default paralytic, and the historical advantage of suxamethonium's short duration is offset by chemical reversal. Where sugammadex is not available, suxamethonium retains the advantage of spontaneous recovery if intubation fails — but suxamethonium's contraindications remain. The choice often comes down to local availability and the patient profile: rocuronium if the patient is at risk of hyperkalaemia or MH, suxamethonium if sugammadex is unavailable and the airway is predicted difficult (so that the patient wakes quickly if intubation fails).[3][11]
Video laryngoscopy
Video laryngoscopy (VL) uses a camera at the tip of the blade (GlideScope, C-MAC, McGrath, Pentax-AWS) to give an enlarged, magnified view of the glottis that does not require alignment of the oral, pharyngeal, and laryngeal axes — the chief difficulty of direct laryngoscopy. VL improves the Cormack-Lehane view, especially in predicted difficult airways (obesity, anterior larynx, limited neck movement, blood/secretions, pregnancy), and is first-line in many ICUs for the critically ill.[4][8]
Two blade geometries exist:[8]
- Hyperangulated blade (GlideScope) — extreme angle; gives an excellent view of the anterior larynx but the tube must be directed around a tight curve (often requires a pre-shaped stylet; bougie is harder to use). Tube delivery to the glottis can be the difficult part even when the view is good.
- Macintosh-style channelled/standard blade (C-MAC Mac) — can be used as direct or video; familiar geometry; bougie works well. Often preferred for the ICU where operators are most familiar with the Macintosh shape.[8]
The MACMAN trial (Lascarrou, JAMA 2020) randomised 600 non-expert operators in French ICUs and found no difference in first-pass success between video and direct laryngoscopy, but the population was non-expert operators and the direct-laryngoscopy arm may have benefited from the operator's training. The DTI-2 and Prekker trials and a large meta-analysis suggest VL improves the view and reduces difficult intubations in the predicted-difficult and critically ill groups, where it is now the default.[8]
MACMAN — video vs direct laryngoscopy in ICU (PMID 32402170)
Practical video laryngoscopy points
- Use a pre-shaped stylet matching the blade's curve for hyperangulated devices — the tube will not follow the curve without it.
- Do not blind-insert — bring the blade in slowly, identify the epiglottis, lift it. The view is on the screen; the tube is in the mouth; coordinate the two.
- Watch for soft-tissue injury — the operator cannot see the tube tip directly, and posterior pharyngeal/tonsillar-pillar injury is more common than with direct laryngoscopy.
- Have a Macintosh blade available — VL can fail (fogging, blood, secretions, light failure), and the operator must be able to revert to direct laryngoscopy.
- Combine VL with the bougie where the view is good but tube delivery is hard — pass the bougie through the cords under vision, then railroad the tube.[8]
Cricoid pressure (Sellick manoeuvre) — the controversy
Cricoid pressure — the application of downward force (the original Sellick description used 20-30 N, ~2-3 kg) on the cricoid cartilage to compress the oesophagus against the vertebral body and occlude it, preventing passive regurgitation of gastric contents — was taught as a mandatory component of RSI from the 1960s until the 2010s. The theory was elegant; the evidence has not borne it out.[4][11]
The problems are several:[11]
- The cricoid does not reliably occlude the oesophagus — MRI and ultrasound studies show the oesophagus is frequently displaced laterally by the pressure rather than compressed, and may not be in apposition to the cricoid in the first place.
- It worsens the laryngoscopic view — downward force on the cricoid distorts the larynx, narrows the laryngeal inlet, and can convert an easy view into a difficult one; it is associated with failed intubation in observational data.
- It does not reduce aspiration — the large-population observational studies (including the INTUBE cohort) found no difference in aspiration rates whether cricoid pressure was used or not.
- It can cause regurgitation — if the pressure is applied while the patient is awake or only lightly sedated, it can trigger gagging and active vomiting — which is far more dangerous than passive regurgitation.[12]
The DAS/ICS/FICM/RCA 2018 guideline and the subsequent ANZICS guidance recommend cricoid pressure not be used routinely. If it is applied and the view is impaired, release it (or reduce the force); the view almost always improves. Many units have abandoned it entirely. The historical justification was the prevention of aspiration in the non-fasted patient, but aspiration has not been shown to fall with cricoid pressure, and the harm to the view is well documented.[3]
What replaced cricoid pressure
Aspiration prophylaxis in the modern RSI rests on:[11]
- Avoiding mask ventilation (the rapid-sequence principle) — though the PrePARE trial showed gentle bag-mask ventilation does not increase aspiration in critically ill adults (Casey, NEJM 2019), the default remains no mask ventilation in the patient at high aspiration risk.
- Head-up position (25-30° reverse Trendelenburg) wherever haemodynamically tolerated — reduces regurgitation by gravity.
- A working suction under the pillow, instantly available.
- A second-generation supraglottic airway (i-gel) with an oesophageal drain tube as the rescue device.
- Rapid, expert intubation with first-pass success.[7]
PrePARE — bag-mask ventilation during RSI (PMID 30208792)
Peri-intubation cardiac arrest and post-intubation hypotension
The most feared complication of ICU intubation is cardiovascular collapse: the patient arrests during or immediately after the intubation, often from the combination of induction-induced vasodilation, hypovolaemia, the loss of sympathetic tone from the induction agent, positive-pressure ventilation reducing venous return, and the underlying critical illness. The INTUBE study (Caprini, JAMA 2021) — a prospective international cohort of 2,964 ICU intubations — quantified the scale of the problem.[5]
INTUBE — international prospective cohort of ICU intubation (PMID 32873211)
Mechanisms of peri-intubation cardiovascular collapse
The arrest is multifactorial. The induction agent removes whatever sympathetic tone the critically ill patient was using to maintain their blood pressure; venodilation reduces preload; positive-pressure ventilation after intubation further reduces venous return; hypoxia from prolonged apnoea causes bradycardia and contractile failure; and the underlying shock (septic, hypovolaemic, cardiogenic, obstructive) has no reserve. Each factor compounds the others, and the patient can arrest within 60 seconds of induction.[5][14]
The keys to prevention are summarised in the haemodynamic bundle below.[5]
Prevent peri-intubation cardiac arrest — the haemodynamic bundle
Resuscitate BEFORE induction
Do not induce in untreated shock. Give a fluid bolus (250-500 mL crystalloid if not volume-overloaded), start a vasopressor infusion (noradrenaline) early, transfuse if anaemic (target Hb ≥70 g/L, ≥80 in ischaemic heart disease). Aim for MAP ≥65 mmHg before induction.
Reduce the induction dose
Halve the dose in any shocked patient: propofol 0.5-1 mg/kg instead of 1-2; thiopentone 1-2 mg/kg instead of 3-5. Default to ketamine (0.5-1 mg/kg in profound shock) because it preserves blood pressure.
Draw up push-dose vasopressors
Have noradrenaline boluses (4-8 mcg) or push-dose adrenaline (10 mcg/mL — 1 mL of 1:1000 in 100 mL saline) drawn up and labelled. Give prophylactically if MAP is borderline, or reactively at the first sign of BP drop. Phenylephrine (50-100 mcg) is an alternative in tachycardic patients.
Arterial line if unstable
Beat-to-beat blood pressure during induction allows immediate detection of and response to hypotension. Insert before induction in any unstable patient if feasible; otherwise cycle NIBP every 1-2 minutes through the procedure.
Minimise apnoea time
Plan and brief the team so the interval from induction to confirmed intubation is minimised. Pre-oxygenate meticulously. Use the bougie or video laryngoscope to maximise first-pass success. The PrePARE trial showed gentle bag-mask ventilation during apnoea is acceptable and reduces desaturation in adults without active vomiting.
Use a checklist
A pre-induction intubation checklist (SOAP-2-ME or equivalent) reduces complications — the Jaber intervention study (Crit Care Med 2010) showed a 50% reduction in life-threatening events with a standardised bundle. Checklist use is associated with fewer adverse events in the INTUBE data.
Management of post-intubation hypotension
When the blood pressure falls after intubation, act immediately — do not wait:[3][14]
- Reduce or stop the sedative infusion — propofol or midazolam infusions started at full theatre doses will continue to depress the circulation. Titrate to the lowest effective dose; many shocked patients need only a fraction of the standard sedation dose. Ketamine is the sedative of choice in the shocked patient post-intubation (preserves BP).
- Give a fluid bolus — 250-500 mL crystalloid rapidly (or albumin) if there is any element of hypovolaemia; reassess (capillary refill, pulse pressure variation, point-of-care ultrasound) for fluid responsiveness.
- Start or up-titrate a vasopressor — noradrenaline is the default first-line vasopressor for vasodilatory shock (septic, neurogenic, post-induction vasoplegia). If the patient is bradycardic or profoundly unstable, adrenaline is preferred (inotrope and vasoconstrictor). Vasopressin is a useful adjunct in vasodilatory shock resistant to noradrenaline.
- Address mechanical causes — excessive PEEP (reduces venous return), too high a tidal volume (the recently intubated patient with sepsis or ARDS needs lung-protective ventilation: tidal volume 6 mL/kg ideal body weight, plateau pressure < 30 cmH2O), breath-stacking/auto-PEEP in COPD/asthma (disconnect the circuit and squeeze the chest to release trapped gas).
- Consider specific causes — tension pneumothorax (especially post-positive-pressure ventilation; examine for asymmetry, tracheal deviation, use POCUS), anaphylaxis to the induction agent or antibiotic (urticaria, bronchospasm; give adrenaline), hypoxaemia (check the tube, the circuit, the oxygen supply), and ongoing haemorrhage.
- Reassess the sedation and analgesia plan daily — the patient who was intubated for hypoxaemic respiratory failure may need only light sedation; the deeply shocked patient may need vasopressors first and sedation titrated down.[14]
Rescue ventilation and oxygenation for the failed RSI — APRV and ECMO
When the RSI succeeds but the patient cannot be oxygenated despite protective mechanical ventilation — profound ARDS, refractory hypoxaemia from pneumonia or aspiration, severe asthma with breath-stacking — escalating the ventilator strategy is the next step before considering extracorporeal support.[3][16]
Airway pressure release ventilation (APRV) as a rescue mode
APRV is a pressure-controlled, time-cycled mode that maintains a continuous high level of positive pressure (P-high, typically 25-35 cmH2O) for most of the respiratory cycle (T-high), with brief release phases (T-low, 0.4-0.8 s) to a low pressure (P-low, usually 0) that allow ventilation. The sustained high pressure recruits and holds open collapsed alveoli (improving oxygenation), spontaneous breathing is permitted throughout (improving V/Q matching, venous return, and reducing sedation needs), and the brief release clears CO2.[3]
APRV is a recognised rescue mode for refractory hypoxaemia in ARDS where conventional lung-protective ventilation has failed. It is not without controversy (the Baird and RAIN trials did not show survival benefit, and it carries a risk of overdistension and haemodynamic compromise), but as a temporising measure to improve oxygenation in a crashing patient it has a place. Set P-high based on the upper inflection point of the pressure-volume curve or 25-30 cmH2O; T-high 4-6 s; T-low set to terminate at 50-75 per cent of peak expiratory flow (prevents alveolar derecruitment and air-trapping).[10]
Veno-venous ECMO for refractory hypoxaemic respiratory failure
When maximal mechanical ventilation (including APRV, prone positioning, inhaled pulmonary vasodilators, and neuromuscular blockade) fails to oxygenate the patient, veno-venous ECMO is the rescue therapy of last resort. It drains venous blood from a large central vein (femoral), oxygenates and decarboxylates it through a membrane lung, and returns it to the right atrium (via the internal jugular), providing full gas exchange independent of the native lungs. The lungs are rested on minimal ventilator settings ("lung rest": tidal volume 4-6 mL/kg, plateau pressure < 25 cmH2O, FIO2 0.3, RR 6-10) while the ECMO circuit does the work.[3][16]
V-V ECMO is indicated in severe but potentially reversible respiratory failure (the EOLIA criteria: PaO2/FIO2 < 50 for > 3 h, or PaO2/FIO2 < 80 for > 6 h, with optimized conventional ventilation, or pH < 7.25 with PaCO2 ≥ 60 for > 6 h). Contraindications include irreversible lung disease without a transplant pathway, fatal comorbidity, advanced age with poor functional status, and inability to anticoagulate (relative). The decision to cannulate is a multidisciplinary one and is made in a centre with an ECMO service; mortality in V-V ECMO for severe ARDS is ~40 per cent (EOLIA, CESAR).[16]
When RSI itself fails — the cannot-intubate-cannot-oxygenate (CICO) pathway
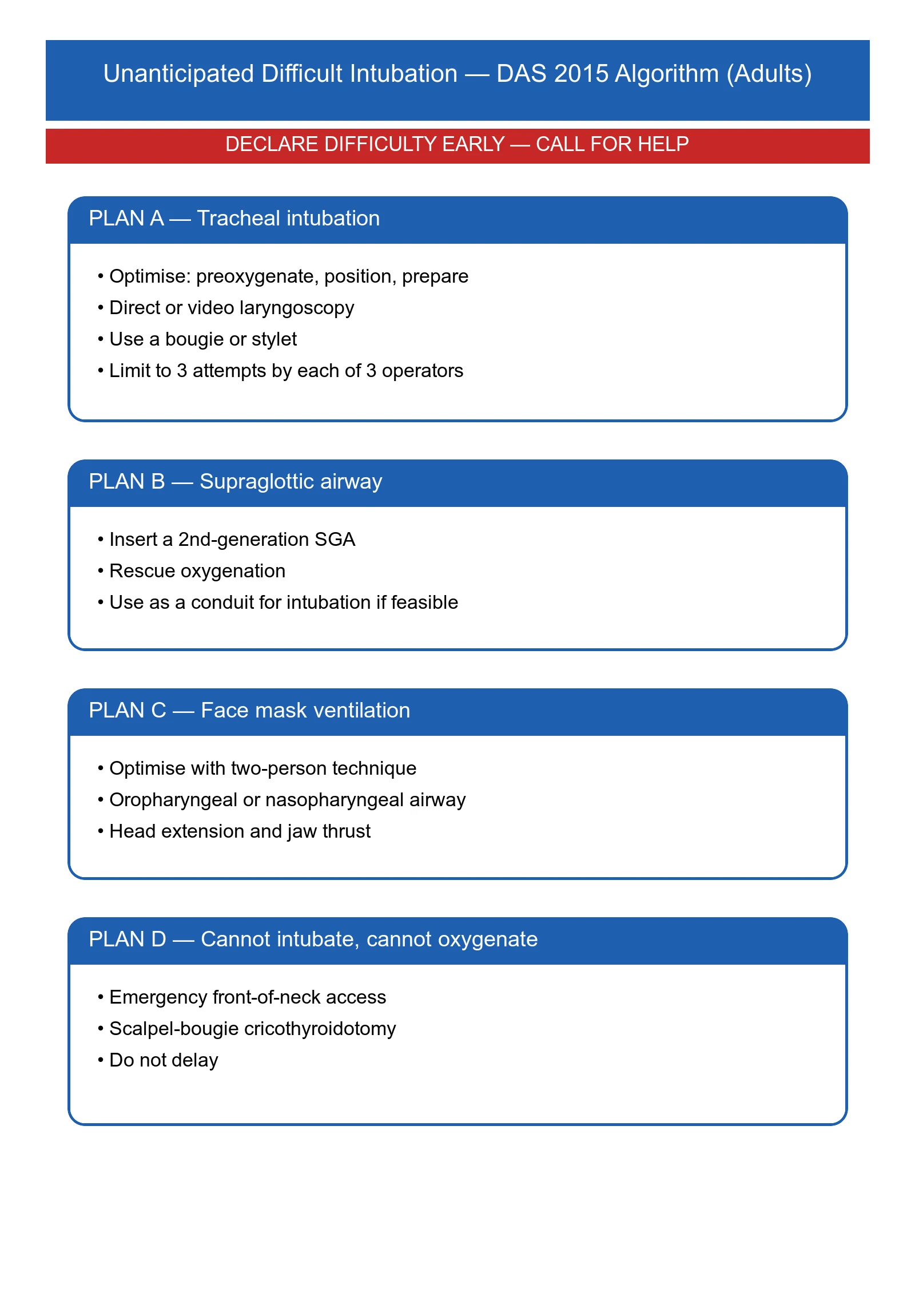
If intubation fails and mask/SGA ventilation fails to maintain SpO2, the patient is in CICO and emergency front-of-neck access (eFONA) is the rescue — a scalpel-bougie cricothyroidotomy. Delay is the enemy: each minute of CICO worsens outcome. Declare CICO out loud, call for the scalpel, and proceed without waiting for senior help if it is not immediately available. The DAS technique (scalpel-bougie, transverse incision through the cricothyroid membrane, turn the blade 90°, railroad a size 6.0 cuffed tube over a bougie) is the standard. See the dedicated difficult-airway topic for the full technique.[4][11]
Difficult airway prediction — LEMON and MACOCHA
Predicting the difficult airway before induction allows planning and avoids the surprise of CICO. Two bedside tools are in common use.[4][11]
LEMON law (a quick mnemonic):[10]
- Look externally — small chin, large incisors, beard, facial trauma, obesity.
- Evaluate 3-3-2 — mouth opening (3 finger-breadths), hyoid-to-chin distance (3), thyroid-to-floor-of-mouth (2).
- Mallampati — class III-IV predicts difficulty (limited validity in isolation).
- Obstruction — stridor, muffled voice, retropharyngeal mass.
- Neck mobility — arthritis, c-spine immobilisation, burns contracture.[10]
MACOCHA score (a validated ICU score, De Larminat 2012): six factors (Mallampati III-IV, Apnoea/Obstructive sleep apnoea, Cervical mobility reduced, Opening < 3 cm, Coma, Hypoxaemia) and non-anaesthetist operator. A score ≥ 3 predicts a difficult airway with high sensitivity.[10]
A predicted difficult airway is not a contraindication to RSI, but it mandates a different plan: have a video laryngoscope ready, a second-generation SGA and a bougie immediately available, an experienced operator and assistant, a low threshold to wake the patient if intubation fails, and consideration of an awake-fibreoptic technique where feasible (the upper-airway-obstructed, "can-intubate-cannot-wait" patient is the exception).[10]
[10]SAQ — Pharmacology and physiological optimisation of RSI
10 minutes · 10 marks
A 70-year-old man with severe ARDS from influenza pneumonitis requires intubation. He is ventilated on CPAP 12 cmH2O, FiO2 0.9, with SpO2 90%, MAP 60 on noradrenaline 0.4 mcg/kg/min, lactate 3.5, and a known difficult airway (previous surgery for oral cancer, limited mouth opening, receding mandible). He has chronic kidney disease (eGFR 35). He weighs 80 kg.
SAQ — Pre-oxygenation, safe apnoea time, and rescue oxygenation strategies
10 minutes · 10 marks
A 28-year-old woman who is 32 weeks pregnant is admitted to ICU with severe pneumonia. She requires intubation for type 1 respiratory failure (SpO2 88% on 15 L/min, RR 32). Her BMI is 38. The registrar asks why pre-oxygenation is so critical and what technique is best.
Clinical pearls — high-yield Fellowship points
[10] [2]The standard ICU RSI sequence — step by step
Pre-oxygenate
Tight-fitting mask, 100% O2, 3 min tidal-volume breathing OR 8 vital-capacity breaths. In the hypoxaemic patient use NIV/CPAP at FIO2 1.0. In the obese/pregnant/rapid-desaturator, add HFNC (THRIVE) at 30-70 L/min under the mask and continue through induction. Goal: ETO2 above 80-90%, or 3 min.
Position
Ramp the patient — external auditory meatus level with the sternal notch (sniffing position); head elevated 25-30° in the obese. Reverse Trendelenburg where tolerated. C-spine precautions if trauma.
Prepare drugs and team
Induction agent chosen to haemodynamics (ketamine default in shock; propofol in stable; etomidate acceptable). Paralytic: rocuronium 1.2 mg/kg (default) or suxamethonium 1.5 mg/kg (if sugammadex unavailable and predicted difficult airway). Draw up push-dose vasopressor (noradrenaline boluses or push-dose adrenaline). Run the SOAP-2-ME checklist. Brief the team: Plan A, B, C, D and the criteria for moving between them.
Induce and paralyse
Give the induction agent, immediately followed by the paralytic, in rapid succession. Do NOT ventilate by mask between (unless adopting the PrePARE approach in the hypoxaemic, non-vomiting patient). Wait for paralysis — about 45-90 s depending on the agent.
Laryngoscopy and tube placement
Video laryngoscope first-line in the predicted difficult airway; Macintosh otherwise. Pass the tube through the cords under vision. Use a bougie for any grade 2b-3-4 view (DRIVER trial — bougie-first improves first-pass success). Inflate the cuff.
Confirm
Waveform capnography — persistent CO2 trace over several breaths is the gold standard. Bilateral chest rise, auscultation. Note depth at the teeth (~23 cm for 8.0 ETT, ~21 cm for 7.0). Secure the tube. Chest X-ray to confirm position.
Post-intubation
Tie and secure the tube. Start sedation (propofol + fentanyl; ketamine if shocked) and analgesia. Commence lung-protective ventilation (Vt 6 mL/kg IBW, plateau pressure < 30, PEEP titrated). Treat post-intubation hypotension immediately: reduce sedation, fluid bolus, vasopressor.
Intubation checklist — SOAP-2-ME adapted for ICU
Suction
Yankauer under the pillow, switched on, tested. Thick secretions/vomit/blood need wide-bore rigid suction — the flexible catheter will block.
Oxygen
Pre-oxygenate to ETO2 above 80-90%. HFNC running if used. Confirm a tight mask seal; flush the circuit at 10-15 L/min.
Airway equipment
Video or direct laryngoscope (tested, charged blade). ETT size 8.0 male / 7.0 female with cuff tested; one size smaller available. Bougie (use routinely for difficult views — DRIVER). Stylet for hyperangulated VL. 10 mL syringe. Tube tie/holder. ETCO2 detector.
Pharmacology
Induction (ketamine/propofol/etomidate) at reduced dose if shocked. Paralytic (rocuronium 1.2 mg/kg or suxamethonium 1.5 mg/kg). Push-dose vasopressor drawn up. Sedation plan for after intubation.
Rescue airway
Second-generation supraglottic airway (i-gel) — sizes 4/5/6 available. Scalpel-bougie cricothyroidotomy kit immediately accessible.
Monitoring and access
ECG, SpO2 continuous, NIBP cycling every 1-2 min (arterial line if unstable), ETCO2. Two large-bore IV cannulae or a central line. Baseline ABG.
Team brief
Most experienced operator does laryngoscopy. Drug assistant, airway assistant, team leader watching clock and SpO2/BP. State Plan A-B-C-D out loud and the criteria for moving between them.
Additional red flags
[9]References
- [1]Gu WJ, Wang F. Single-dose etomidate does not increase mortality in patients with sepsis: a systematic review and meta-analysis. Chest, 2015.PMID 25255427
- [2]Chan CM, Mitchell AL, Shorr AF. Etomidate is associated with mortality and adrenal insufficiency in sepsis: a meta-analysis. Critical Care Medicine, 2012.PMID 22971586
- [3]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [4]Acquisto NM, Mosier JM, Bittner EA, et al. Society of Critical Care Medicine Clinical Practice Guidelines for Rapid Sequence Intubation in the Critically Ill Adult Patient. Critical care medicine, 2023.PMID 37707379
- [5]Russotto V, Myatra SN, Laffey JG, et al. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA, 2021.PMID 33755076
- [6]Jabre P, Combes X, Lapostolle F, et al. Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial. Lancet (London, England), 2009.PMID 19573904
- [7]Casey JD, Janz DR, Russell DW, et al. Bag-Mask Ventilation during Tracheal Intubation of Critically Ill Adults. The New England journal of medicine, 2019.PMID 30779528
- [8]Lascarrou JB, Boisrame-Helms J, Bailly A, et al. Video Laryngoscopy vs Direct Laryngoscopy on Successful First-Pass Orotracheal Intubation Among ICU Patients: A Randomized Clinical Trial. JAMA, 2017.PMID 28118659
- [9]Brenner MJ, McGrath BA, Cook TM Use of a Bougie vs Endotracheal Tube With Stylet and Successful Intubation on the First Attempt Among Critically Ill Patients Undergoing Tracheal Intubation. JAMA, 2022.PMID 35438736
- [10]Patel A, Nouraei SA Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia, 2015.PMID 25388828
- [11]Higgs A, McGrath BA, Goddard C, et al. Guidelines for the management of tracheal intubation in critically ill adults. British journal of anaesthesia, 2018.PMID 29406182
- [12]Mort TC Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts. Anesthesia and analgesia, 2004.PMID 15271750
- [13]Russotto V, Cortegiani A, Raineri SM, et al. Respiratory support techniques to avoid desaturation in critically ill patients requiring endotracheal intubation: A systematic review and meta-analysis. Journal of critical care, 2017.PMID 28505486
- [14]Green RS, Turgeon AF, McIntyre LA, et al. Postintubation hypotension in intensive care unit patients: A multicenter cohort study. Journal of critical care, 2015.PMID 26117220
- [15]Jaber S, Jung B, Corne P, et al. An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive care medicine, 2010.PMID 19921148
- [16]Combes A, Hajage D, Capellier G, et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. The New England journal of medicine, 2018.PMID 29791822