ICU · Airway management
Tracheostomy — Indications, Types, Percutaneous, Decannulation & Emergencies
Also known as Tracheostomy · Percutaneous dilatational tracheostomy · PDT · Surgical tracheostomy · TracMan trial · Speaking valve · Passy-Muir valve · Decannulation · Tracheostomy emergencies · Tracheo-innominate artery fistula · Ciaglia Blue Rhino · Griggs forceps technique · Fenestrated tracheostomy tube · NTSP algorithm · Tracheo-oesophageal fistula · Tracheal stenosis · Percutaneous tracheostomy
A tracheostomy is a surgical airway through the anterior trachea, placed for prolonged ventilation, upper-airway obstruction, airway protection, or secretion clearance. Percutaneous dilatational tracheostomy (Ciaglia Blue Rhino, bronchoscopic-guided, bedside) is the ICU standard; surgical tracheostomy is reserved for difficult anatomy, children, and emergencies. The TracMan trial (JAMA 2013) found early versus late tracheostomy does not change mortality, so timing is individualised. Complications fall into early (bleeding, displacement, pneumothorax), intermediate (infection, obstruction), and late (tracheal stenosis, tracheo-innominate artery erosion with its sentinel bleed, tracheo-oesophageal fistula). A displaced tube in the first week — before the tract matures — is re-intubated from above, not reinserted blindly.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
A tracheostomy is a surgical airway created through the anterior tracheal wall, bypassing the upper airway. It is placed for prolonged mechanical ventilation, upper-airway obstruction, airway protection in the neurologically impaired, and secretion clearance. Compared with a translaryngeal endotracheal tube it improves comfort, reduces sedation, allows communication (via a speaking valve) and oral intake, eases secretion clearance, and may speed weaning — at the cost of the procedural and stomal complications described below.[2]

The stoma is created between the 2nd and 3rd tracheal rings (occasionally 1st-2nd). Going too high (cricoid/cricothyroid) risks subglottic stenosis; going too low (below the 4th ring) brings the tube tip against the innominate (brachiocephalic) artery and risks catastrophic erosion. The tract takes roughly 7-10 days to mature; before then the stoma collapses if the tube is removed and a blind reinsertion passes into a paratracheal false passage.[2][4]
Indications
- Prolonged mechanical ventilation and weaning — the commonest ICU indication.[2]
- Upper-airway obstruction (tumour, infection, trauma, bilateral vocal-cord palsy).[2]
- Airway protection in the neurologically impaired (TBI, stroke, neurodegenerative disease) and poor bulbar function.
- Secretion clearance when the patient cannot clear their own secretions.[2]
Prolonged ventilation and weaning failure
A patient expected to need mechanical ventilation for more than 10-14 days is the classical trigger: a translaryngeal tube over that duration causes laryngeal injury, glottic oedema, sinusitis, and patient discomfort, and impedes weaning. A tracheostomy converts the airway from a tube traversing the larynx to one that enters the trachea directly — shorter dead space, less work of breathing, no laryngeal trauma, easier weaning to a T-piece/CPAP, and the option to reduce or stop sedation. A systematic review (Griffiths 2007) found tracheostomy was associated with fewer days of mechanical ventilation and shorter ICU stay, but the mortality benefit is uncertain.[7][2]
Weaning failure
Patients who repeatedly fail extubation — typically the elderly, the chronically respiratory-compromised, the neuromuscularly weak (GBS, myasthenia), and those with cardiac failure — benefit from a tracheostomy because the lower resistance, the ability to trial cuff-down and speaking-valve periods, and the protected airway allow graded weaning.[2]
Upper-airway obstruction
A fixed lesion above the tracheostomy site — head-and-neck tumour, supraglottitis/epiglottitis, angioedema, facial/neck burns with inhalation injury, bilateral recurrent laryngeal nerve palsy, or external compression (large retrosternal goitre) — is bypassed by the tracheostomy. In this group the tracheostomy is the primary (sometimes permanent) airway, not a weaning adjunct.[2]
Airway protection and pulmonary toilet
In the neurologically impaired (severe TBI, large stroke, neurodegenerative disease with bulbar failure) the tracheostomy protects the airway from aspiration and allows repetitive suctioning and bronchial toilet that the patient cannot perform themselves. This is a major indication in the neuro-ICU and the rehabilitation setting.[2]
The "what about pneumonia?" question
A common exam misconception is that a tracheostomy reduces ventilator-associated pneumonia. It does not — a tracheostomy is itself a foreign body that bypasses the upper airway defences and colonises the lower airway within days. The TracMan and Cochrane data show no consistent reduction in nosocomial pneumonia with early tracheostomy.[1][5]
Timing — TracMan
The TracMan trial (Young, JAMA 2013) randomised ICU patients to early (within 4 days) versus late (after 10 days) tracheostomy. It found no difference in 30-day mortality (the primary outcome); early tracheostomy reduced days of sedation and ICU stay but did not improve survival.[1] The practical conclusion is that timing is individualised — there is no mandate to place a tracheostomy early purely for a survival benefit, and the decision turns on the expected duration of ventilation and the patient's trajectory.[1][2]
The broader evidence on timing
The Cochrane review (Gomes Silva 2012) pooled the early-vs-late trials and reached the same conclusion as TracMan: no significant mortality difference, though early tracheostomy may shorten mechanical ventilation and ICU stay.[5] A later meta-analysis (Liu 2016) found a modest mortality benefit with early tracheostomy in subgroup analysis, but this was driven by older, smaller, lower-quality trials and is not sufficient to override TracMan.[8] The net exam answer: timing does not change survival; individualise it.[1][5]
The key TracMan insight: of patients randomised to the late arm, about two-thirds never needed a tracheostomy at all — they had recovered or died before day 10. An early-tracheostomy policy therefore commits many patients to a procedure they would never have needed.[1]
Types and technique
Percutaneous dilatational tracheostomy (PDT)
PDT (the Ciaglia technique) is the bedside ICU standard for most patients:[2]
- Bronchoscopic-guided (and increasingly ultrasound-guided) to confirm level and placement.
- Performed at the bedside under sedation; a bronchoscope withdraws the endotracheal tube to just below the cords, the trachea is punctured between the 2nd and 3rd tracheal rings (Seldinger), a single tapered dilator (the Ciaglia Blue Rhino) opens the tract, and the tracheostomy tube is inserted.
- Advantages over surgical tracheostomy: bedside, faster, less scarring, smaller stoma, comparable complications.[2]
The Ciaglia Blue Rhino technique — step by step
The modern Ciaglia technique uses a single tapered hydrophilic dilator (the Blue Rhino) over a guidewire, replacing the older multiple-dilator sequence. It is the dominant PDT method worldwide.[2][6]
Percutaneous dilatational tracheostomy (Ciaglia Blue Rhino) — step by step
Position and prepare
Extend the neck (a shoulder roll), unless c-spine is not cleared. Identify the cricoid and tracheal rings by palpation; mark the 2nd-3rd inter-ring space. Pre-oxygenase with 100% oxygen. The patient is sedated, paralysed and ventilated. Bronchoscopist stands at the head of the bed; operator on the patient's right.
Bronchoscopy and ETT withdrawal
The bronchoscope is passed through the endotracheal tube to the tip. The ETT cuff is deflated and the tube is withdrawn under vision to just below the vocal cords, so the light transilluminates the puncture site from within. The bronchoscope stays in the trachea to visualise needle entry, confirm midline puncture, and watch the tract dilate and the tube pass — guarding against posterior wall injury and paratracheal placement.
Ultrasound (recommended)
Pre-procedural ultrasound identifies the tracheal rings, excludes an overlying vessel (pre-tracheal vein or aberrant branch), and confirms a safe puncture window. Point-of-care ultrasound reduces bleeding and first-attempt failure versus pure landmark technique.<Cite id="9" /><Cite id="10" />
Tracheal puncture (Seldinger)
A small skin incision at the marked space. A needle with cannula is inserted midline between the 2nd and 3rd rings, angled caudally, aspirating for air to confirm intratracheal position (and bronchoscopic confirmation). A J-tipped guidewire is passed through the cannula into the trachea. The cannula is withdrawn, leaving the wire in situ.
Dilate with the Blue Rhino
A short 14 F stiffening dilator is passed over the wire to pre-dilate, then the single tapered Blue Rhino dilator (lubricated, hydrophilic) is advanced over the wire to the skin-level mark, dilating the tract in one smooth motion to ~36-38 F. The wire and stiffener are kept in place throughout (never lose the wire).
Load and insert the tracheostomy tube
The appropriately sized tracheostomy tube (usually size 8 for an adult male, 6-8 for a female) is loaded onto a loading dilator over the wire, and railroaded into the trachea. The wire and loading dilator are removed, leaving the tracheostomy tube.
Confirm and secure
The bronchoscope is passed through the tracheostomy tube to confirm intratracheal position and inspect the posterior wall for injury. The cuff is inflated, the circuit attached, and position confirmed with bilateral chest rise and waveform capnography. The tube is secured with sutures and a tie, and a chest X-ray is obtained to exclude pneumothorax and confirm tip position.
Guidance: bronchoscopy vs ultrasound vs landmark
Bronchoscopic guidance is the established standard — it confirms the puncture level, midline entry, and final tube position, and guards against posterior wall perforation. Ultrasound is increasingly added (or used alone where bronchoscopy is impractical) to map the pre-tracheal vessels, confirm the inter-ring space, and predict the depth. Meta-analyses show ultrasound guidance reduces bleeding, reduces first-attempt failure, and lowers overall complications compared with the pure anatomical-landmark technique.[9][10] A network meta-analysis (Zhang 2019) found that all guided PDT techniques (landmark, bronchoscopic, ultrasound) had comparable overall complication rates to surgical tracheostomy, with bronchoscopic guidance the most widely adopted.[11]
Alternative percutaneous techniques
The Griggs (guidewire dilating forceps) technique uses a pair of curved forceps passed over the wire to spread the tracheal wall, rather than a tapered dilator — faster but with a higher rate of posterior wall injury in some series. The PercuTwist (a single self-rotating screw dilator) and the Fantoni translaryngeal technique (dilated from inside-out, then rotated down) are less commonly used alternatives.[2]
Surgical tracheostomy
An open dissection in theatre, reserved for difficult anatomy, redo tracheostomy, children, an unstable/obese patient unsuited to bedside PDT, or as an emergency (for example a fractured larynx where cricothyroidotomy is contraindicated). It allows direct visualisation and haemostasis.[2]
Percutaneous vs surgical — the comparison
[6]The Diaz-Reganon series of 800 mixed ICU patients undergoing bronchoscopic-guided PDT reported a low serious complication rate (major bleeding <1%, no deaths attributable to the procedure), supporting PDT as a safe bedside standard in experienced hands.[6]
Tracheostomy tubes
- Cuffed (for ventilation/airway protection) versus uncuffed (for weaning/communication).
- Fenestrated tubes (with holes in the shaft to allow airflow through the upper airway when the cuff is down — for speaking).
- Adjustable-flange tubes for deep tracheas or obese necks.
- Double-cannula tubes (a removable inner cannula that can be cleaned or replaced if blocked) — safer for the long-term tracheostomy.[2]
Fenestrated vs non-fenestrated tubes
[7]Complications
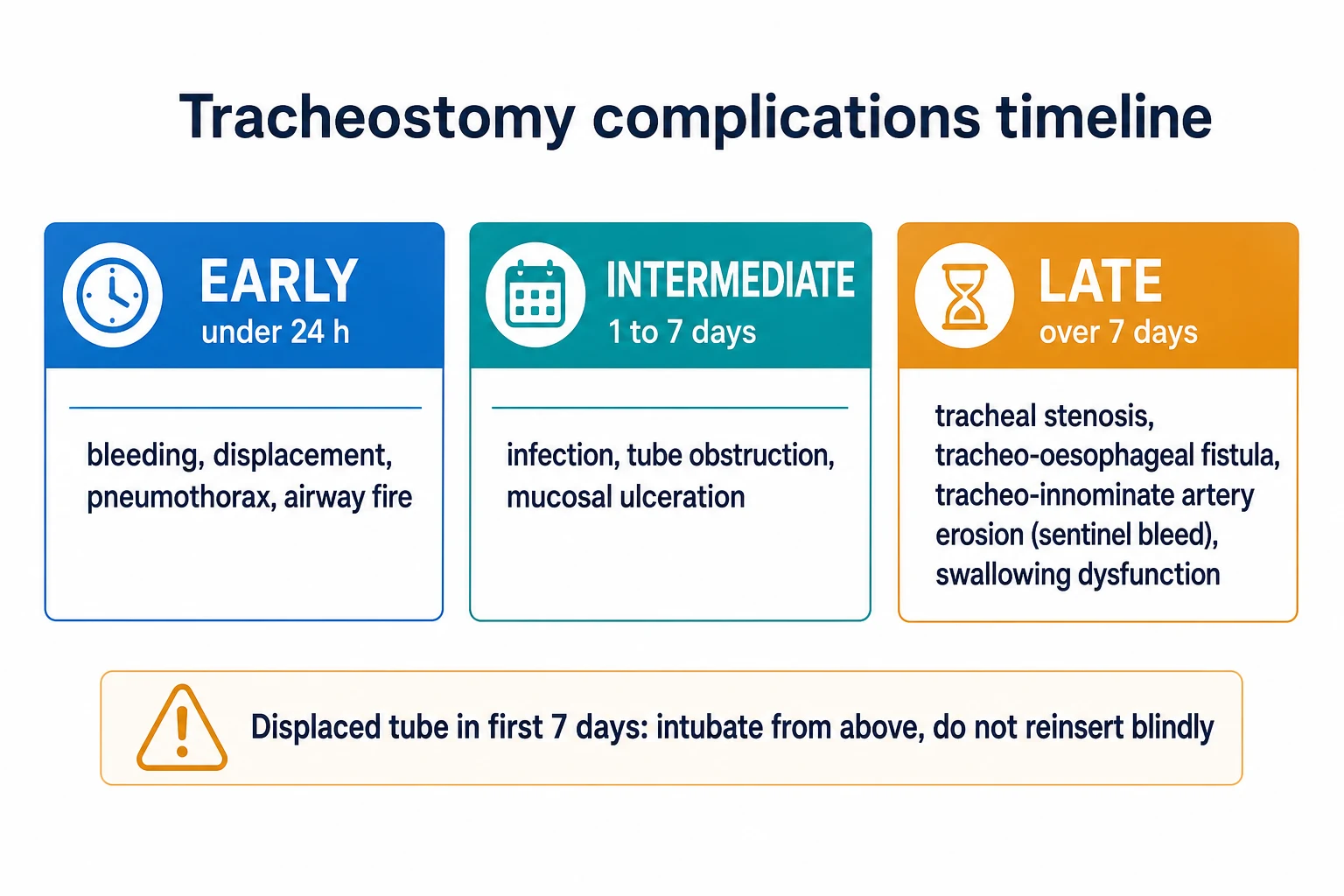
Early (under 24 hours):[2]
- Bleeding (thyroid isthmus, anterior jugular veins, tracheal wall).
- Tube displacement or malposition — the most dangerous early complication.
- Pneumothorax, pneumomediastinum, and subcutaneous emphysema from a posterior tracheal wall injury or a paratracheal pass.
- Airway fire (rare) with electrocautery in a high-oxygen environment — minimise FiO2 and avoid diathermy once the airway is open.[3]
Intermediate (1-7 days):[2]
- Stomal infection, tracheitis.
- Tube obstruction by blood, secretions, or a crust; mucosal ulceration and granuloma.[3]
Late (over 7 days):[2]
- Tracheal stenosis (at the stoma or the cuff site) — the commonest late complication, presenting weeks to months after decannulation with stridor or dyspnoea.
- Tracheo-oesophageal fistula (from cuff or tube pressure against an in-dwelling nasogaugastric tube).
- Tracheo-innominate artery erosion — erosion into the innominate artery (typically around 2-3 weeks), presenting with a small sentinel herald bleed followed within hours by catastrophic haemorrhage. Treat by hyperinflating the cuff, withdrawing the tube, applying direct anterior finger pressure against the sternum (or a cuffed endotracheal tube with the cuff over-extended), and emergency surgery.[2][3]
- Tracheocutaneous fistula (a stoma that will not close) and swallowing dysfunction (the open stoma reduces glottic closure reflex and laryngeal elevation).[3]
Complications in detail — mechanism and prevention
[11]Posterior tracheal wall injury
The posterior membranous wall is the weakest part of the trachea. A needle, dilator, or tube pushed too far — or a needle inserted at too steep an angle — perforates it, producing pneumomediastinum, subcutaneous (surgical) emphysema, pneumothorax, and potentially a tracheo-oesophageal fistula. Bronchoscopic visualisation of the needle tip entering the anterior trachea, a shallow needle angle, and never advancing a dilator without a confirmed intratracheal wire, are the preventive measures.[2][6]
Tracheo-innominate artery fistula (TIF)
The catastrophic late complication. The tube tip (or a low stoma) erodes into the innominate (brachiocephalic) artery as it crosses the trachea anteriorly, typically at the 2nd-3rd week. A small sentinel bleed — a few millilitres of bright blood around or through the tube — is the warning; catastrophic exsanguination follows within hours. The tract must be placed high (2nd-3rd ring), the tube sized correctly, and cuff pressure kept low. Never dismiss a sentinel bleed.[2][4]
Tracheal stenosis
The commonest late complication, occurring at two sites: the stoma (from chondritis and circumferential scarring as the tract heals) and the cuff site (from pressure necrosis). It presents weeks to months after decannulation with exertional dyspnoea, stridor, or failed extubation-like symptoms. Risk factors are high cuff pressure, prolonged cannulation, recurrent infection, and an oversized tube. Prevention centres on cuff pressure <25 cmH2O, humidification, and the smallest effective tube. Management ranges from endoscopic dilution/laser to segmental tracheal resection.[2]
Subcutaneous emphysema
Air tracking into the soft tissues of the neck and chest wall after a posterior wall tear or a paratracheal pass. It signals a procedural injury — obtain a chest X-ray to exclude pneumothorax/pneumomediastinum and bronchoscope to inspect the posterior wall. Usually self-limiting once the airway is secure, but a tension pneumothorax must be excluded.[2]
Tracheostomy emergencies
The two life-threatening emergencies are a blocked or displaced tube and the tracheo-innominate bleed.[3]
A blocked or displaced tube in the first week (before the tract has matured) is a disaster in waiting: a fresh, un-matured tract collapses and a blind reinsertion passes into a false passage (paratracheal), with fatal hypoxia. The safe algorithm (NTSP): call for help; assess and oxygenate; attempt to pass a suction catheter through the tube — if it passes, the tube is in the trachea (deflate the cuff, remove the obstruction, ventilate); if it does not pass, the tube is displaced — deflate the cuff, remove the tube, and re-establish the airway from above by orotracheal intubation (not by blind tracheostomy reinsertion). Once the tract is mature (beyond about a week) a tube can be reinserted more safely.[3]
The tracheo-innominate bleed: a sentinel bleed must never be dismissed — hyperinflate the cuff immediately; if bleeding continues, withdraw the tube, apply anterior digital pressure, intubate from above, and call the surgeon.[3]
The NTSP emergency algorithm — the "Pat-Deflate-Oxygenate" framework
The National Tracheostomy Safety Project provides a structured algorithm for the tracheostomy patient who deteriorates. The core principle is to assess and fix the airway by the safest available route, with orotracheal intubation as the rescue for an un-matured tract.[4]
NTSP algorithm — blocked or displaced tracheostomy tube
Call for help and oxygenate
Call the airway team (anaesthetist/ICU). Apply high-flow oxygen to BOTH the face and the tracheostomy stoma — a patient with a patent upper airway may be oxygenated from above even if the tracheostomy is blocked.
Assess airway patency — the suction-catheter test
Attempt to pass a suction catheter through the tracheostomy tube (remove the inner cannula first, in case it is the obstruction). If the catheter passes easily, the tube is in the trachea and the problem is obstruction — clear it, deflate the cuff, suction, and ventilate.
If the catheter does NOT pass — the tube is displaced
Deflate the cuff, remove the tracheostomy tube entirely, and re-establish the airway from ABOVE by orotracheal intubation. Do NOT attempt blind reinsertion through an un-matured tract — it will pass into a paratracheal false passage.
If the tract is mature (>7-10 days)
A mature tract may allow careful reinsertion with a smaller tube or a bougie, but if there is ANY doubt, intubate from above. Capnography confirms position after any reinsertion.
Confirm with capnography
A persistent CO2 waveform over several breaths is the only acceptable confirmation of tracheal placement after any airway manoeuvre.
The mnemonic "Look, Listen, Feel" at the stoma and mouth, and oxygenate at both sites, captures the NTSP philosophy: a laryngectomy patient can ONLY be oxygenated at the stoma (the upper airway is disconnected), while a tracheostomy patient can usually be oxygenated from above if the upper airway is patent.[4]
Tracheo-innominate bleed — emergency management
Tracheo-innominate artery fistula bleed — emergency sequence
Recognise the sentinel bleed
A small herald bleed of bright red blood around or through a 2-3-week-old tracheostomy is a TIF until proven otherwise. Never attribute it to "just stomal oozing".
Hyperinflate the cuff
Inflate the tracheostomy cuff to maximum volume to tamponade the bleeding against the anterior tracheal wall. This may temporarily arrest the bleed.
If bleeding continues — withdraw and apply anterior pressure
Withdraw the tube slightly. The operator's index finger is passed through the stoma and pressed firmly against the anterior tracheal wall / manubrium, compressing the innominate artery against the sternum. This is the single manoeuvre that buys time for surgery.
Intubate from above and call the surgeon
Orotracheal intubation secures the airway while direct digital pressure is maintained. Emergency surgical exploration (sternotomy/repair or ligation of the innominate) is definitive. Mortality is high even with optimal management.
Decannulation
Decannulation (removing the tracheostomy) follows a structured weaning once the original indication has resolved:[2]
- The patient is off mechanical ventilation and stable.
- Adequate cough, gag, and swallow, and manageable secretions.
- Tolerates cuff deflation and an occlusion/capping trial.
- A one-way speaking valve (Passy-Muir, with the cuff fully deflated) is trialled, then the tube is capped, then removed.
- The stoma is dressed and allowed to close (most close in days to weeks; a persistent tract may need surgical closure).[2]
The decannulation protocol in detail
Structured decannulation protocol
Confirm the indication has resolved
The patient is off the ventilator, neurologically appropriate (or at baseline), with manageable secretions and an effective cough. The original reason for the tracheostomy (ventilation, obstruction, protection) must be gone.
Cuff deflation trial
Deflate the cuff and observe for airway compromise, aspiration, and tolerance of the upper-airway airflow. The patient should be able to manage their secretions and protect their airway.
Speaking valve trial (cuff DOWN)
Place a one-way speaking valve (Passy-Muir) with the cuff fully deflated. The patient inhales through the tracheostomy and exhales through the upper airway. Success confirms upper-airway patency and phonation. NEVER place a speaking valve with the cuff up — the patient cannot exhale and will asphyxiate.
Capping / decannulation cap
The tube is capped (occluded) so all airflow is through the upper airway. The patient tolerates capping for 24-48 h without distress, maintaining oxygenation and clearing secretions. A fenestrated tube or a downsized uncuffed tube eases this stage.
Remove and dress
Once capping is tolerated, the tube is removed, the stoma is dressed with an occlusive dressing, and the patient is observed. The stoma closes by secondary intention over days to weeks.
Persistent stoma
A stoma that has not closed after several months (a tracheocutaneous fistula) may need surgical closure.
The speaking valve (Passy-Muir)
The speaking valve is a one-way valve that fits on the tracheostomy: air is inspired through the tracheostomy and exhaled through the upper airway (past the vocal cords), restoring phonation. The cuff must be fully deflated before a speaking valve is placed, or the patient cannot exhale.[2]
How it works — and why the cuff must be down
Inspiration: the valve opens, air flows through the tracheostomy tube into the lungs. Exhalation: the valve closes, diverting exhaled air up around the tube and through the glottis, where the vocal cords vibrate to produce speech. If the cuff is inflated during exhalation, the air has no route out — the patient cannot exhale, becomes distressed, and will asphyxiate. Hence the non-negotiable rule: cuff fully down before the valve goes on.[2]
Benefits of a speaking valve beyond communication: it restores subglottic pressure (improving cough and swallow), restores upper-airway sensation (reducing aspiration), and aids weaning by reconditioning the upper airway. Contraindications include an unstable airway, severe upper-airway obstruction (air cannot get past the glottis on exhalation), copious secretions, severe anxiety/claustrophobia, and an inflated cuff.[2]
SAQ — Indications, timing, and the TracMan trial
10 minutes · 10 marks
A 68-year-old man is ventilated in ICU on day 6 of a severe Guillain-Barré syndrome with respiratory failure. He is on FiO2 0.4, PEEP 8, and requires prolonged ventilation (anticipated weeks). He is haemodynamically stable, lightly sedated, and tolerating synchronised intermittent mandatory ventilation. The registrar asks whether a tracheostomy should be performed now.
SAQ — Decannulation, speaking valves, and long-term tracheostomy care
10 minutes · 10 marks
A 72-year-old woman has been in ICU for 4 weeks following a severe stroke with aspiration pneumonia. She has had a tracheostomy for 18 days for prolonged ventilation and was successfully weaned to a tracheostomy mask (FiO2 0.3) 3 days ago. She is now neurologically stable, tolerating a speaking valve for 4-hour periods, has an effective cough, and a formal swallow assessment (FEES) showed no aspiration. The team asks about decannulation.
Clinical pearls
Red flags
[11]Key trials and evidence
TracMan — early vs late tracheostomy (PMID 23695482)
Gomes Silva — Cochrane review: early vs late tracheostomy (PMID 22419322)
Griffiths — tracheostomy and outcomes in long-term ventilation (PMID 17255861)
Diaz-Reganon — safety of percutaneous tracheostomy in 800 ICU patients (PMID 18717657)
Wu — ultrasound-guided vs landmark PDT meta-analysis (PMID 34710141)
Zhang — network meta-analysis: PDT guidance vs surgical tracheostomy (PMID 31020401)
Contraindications and relative contraindications
There are no absolute contraindications to a tracheostomy when the airway is needed, but several are relative and shift the balance toward surgical tracheostomy or temporisation:[2][6]
- Coagulopathy (INR >1.5, platelets <50, active bleeding) — correct first if possible; both PDT and surgical trach bleed, but PDT's smaller tract and bronchoscopic tamponade are relatively forgiving once the INR is normalised.[6]
- Children / prepubertal patients — the paediatric trachea is soft, mobile, and hard to fix; PDT is generally avoided in favour of surgical tracheostomy by a paediatric ENT/anaesthetist.
- Difficult anatomy — short/obese neck, overlying thyroid mass, previous neck surgery or radiation, neck infection — favour surgical tracheostomy with direct vision.
- Unstable cervical spine — neck extension is limited; surgical tracheostomy with in-line stabilisation or PDT with bronchoscopic/US guidance.
- High ventilator pressures / high PEEP — the risk of derecruitment and air leak during the procedure (cuff deflation, ETT withdrawal) is significant; plan for rapid tube exchange and minimise the open-airway time.
- Haemodynamic instability — stabilise first; a tracheostomy is rarely the immediate priority in undifferentiated shock.
Humidification and stoma care
The upper airway warms, humidifies, and filters inspired gas — functions lost once the tracheostomy bypasses it. Active humidification (heat-moisture exchanger or heated humidifier) is mandatory from the moment the tracheostomy is placed; without it, secretions dry and crust, obstructing the tube (the commonest cause of late obstruction).[2]
Routine stoma care: daily inspection for infection, skin excoriation, and bleeding; tracheostomy ties secured so one finger fits underneath; sutures retained until the tract is secure; cuff pressure measured daily and kept <25 cmH2O; inner cannula (if double-cannula) cleaned or changed per protocol.[2]
Prognosis and outcomes
The outcome after a tracheostomy is dominated by the underlying illness, not the procedure itself. In TracMan, mortality at 30 days was ~30% in both arms — reflecting the severity of the critically ill population, not the tracheostomy.[1] For patients who survive to decannulation, the late morbidity is driven by tracheal stenosis (the commonest late complication, presenting weeks to months later) and swallowing dysfunction. The tracheo-innominate artery fistula is rare (<1%) but carries a high mortality even with optimal management.[2][6]
The determinants of a good outcome are: (1) correct patient selection — a tracheostomy for a patient who will truly benefit from prolonged ventilation or airway protection; (2) correct timing — individualised, not reflexive; (3) a safe technique — bronchoscopic-guided PDT by an experienced team, with ultrasound where available; (4) meticulous post-procedure care — humidification, cuff pressure, inner-cannula checks, stoma care; and (5) a structured decannulation protocol and rehabilitation.[1][2][4]
References
- [1]Young D, Harrison DA, Cuthbertson BH, Rowan K; TracMan Collaborators. Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: the TracMan randomized trial. JAMA, 2013.PMID 23695482
- [2]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [3]McGrath BA, Bates L, Atkinson D, et al. Multidisciplinary guidelines for the management of tracheostomy and laryngectomy airway emergencies. Anaesthesia, 2012.PMID 22731935
- [4]McGrath BA, Bates L, Atkinson D, et al. Multidisciplinary guidelines for the management of tracheostomy and laryngectomy airway emergencies. Anaesthesia, 2012.PMID 22731935
- [5]Gomes Silva BN, Andriolo RB, Saconato H, Atallah AN, Valente O. Early versus late tracheostomy for critically ill patients. Cochrane Database of Systematic Reviews, 2012.PMID 22419322
- [6]Diaz-Reganon G, Minambres E, Ruiz A, Gonzalez-Herrera S, Holanda-Pena M, Lopez-Espadas F. Safety and complications of percutaneous tracheostomy in a cohort of 800 mixed ICU patients. Anaesthesia, 2008.PMID 18717657
- [7]Combes A, Luyt CE, Nieszkowska A, Trouillet JL, Gibert C, Chastre J. Is tracheostomy associated with better outcomes for patients requiring long-term mechanical ventilation? Critical Care Medicine, 2007.PMID 17255861
- [8]Meng L, Wang C, Li J, Zhang J. Early vs late tracheostomy in critically ill patients: a systematic review and meta-analysis. Clinical Respiratory Journal, 2016.PMID 25763477
- [9]Lin KT, Kao YS, Chiu CW, Lin CH, Chou CC, Hsieh PY. Comparative effectiveness of ultrasound-guided and anatomic landmark percutaneous dilatational tracheostomy: A systematic review and meta-analysis. PLoS One, 2021.PMID 34710141
- [10]Gobatto ALN, Besen BAMP, Cestari M, Pelosi P, Malbouisson LMS. Ultrasound-Guided Percutaneous Dilational Tracheostomy: A Systematic Review of Randomized Controlled Trials and Meta-Analysis. Journal of Intensive Care Medicine, 2020.PMID 29409380
- [11]Iftikhar IH, Teng S, Schimmel M, Duran C, Sardi A, Islam S. A Network Comparative Meta-analysis of Percutaneous Dilatational Tracheostomies Using Anatomic Landmarks, Bronchoscopic, and Ultrasound Guidance Versus Open Surgical Tracheostomy. Lung, 2019.PMID 31020401