ICU · Airway management
Upper-Airway Obstruction — Epiglottitis, Angioedema & Deep Neck Abscess
Also known as Upper-airway obstruction · Epiglottitis · Supraglottitis · Angioedema · ACE inhibitor angioedema · Hereditary angioedema · Retropharyngeal abscess · Peritonsillar abscess · Quinsy · Ludwig's angina · Stridor
Upper-airway obstruction is an airway emergency. The causes run from the nose and mouth (allergic and ACE-inhibitor angioedema of the lip and tongue), through the supraglottis (epiglottitis, peritonsillar abscess), to the subglottis and retropharyngeal space (retropharyngeal abscess, Ludwig's angina, post-extubation oedema). Stridor at rest, drooling, tripoding, and distress signal severe obstruction. The overarching rule is to do no harm: keep the patient upright and calm, call for senior airway help early, avoid upsetting the airway, and secure it in a controlled setting. Epiglottitis is not examined in the unsecured airway; ACE-inhibitor angioedema is bradykinin-mediated and does not respond to adrenaline, antihistamines, or steroids.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
Upper-airway obstruction is an airway emergency in which airflow through the upper airway is compromised, progressing from noisy breathing to complete obstruction and hypoxic death. The causes run from the nose and mouth (angioedema of the lip and tongue), through the supraglottis (epiglottitis, peritonsillar abscess), to the subglottis and deep neck spaces (retropharyngeal abscess, Ludwig's angina, post-extubation oedema, foreign body).[1]
The overarching rule is to do no harm: keep the patient upright and calm, call for senior airway help early, avoid agitating or instrumenting the airway, and secure it in a controlled setting.[1][2]
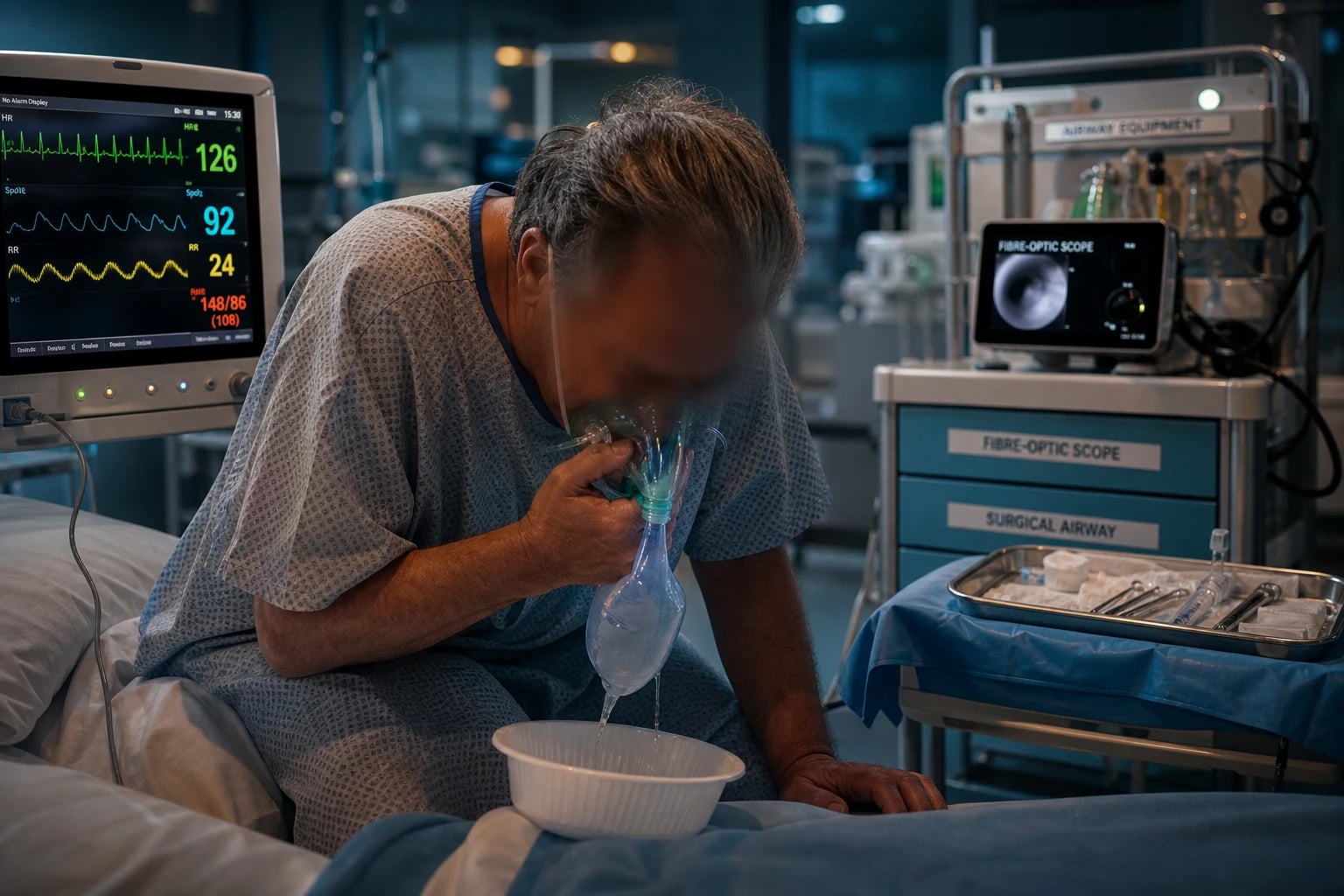
Recognising severity
Severity is judged clinically:[1]
- Stridor at rest (not just on exertion) = severe obstruction.
- Tripoding (sitting forward, arms extended), drooling (cannot swallow secretions), and a muffled 'hot potato' voice.
- Accessory-muscle use, tracheal tug, intercostal recession, agitation, and progressive fatigue.
- Hypoxia and a falling level of consciousness are pre-arrest signs.
A patient who can lie flat and swallow is less acute; one who is drooling, tripoding, and distressed needs an airway secured urgently.[4]
Stridor — the localising sign
The phase of stridor in the respiratory cycle localises the level of obstruction, because extrathoracic obstruction narrows on inspiration (negative intrathoracic pressure collapses the extrathoracic airway inward) and intrathoracic obstruction narrows on expiration (positive intrathoracic pressure collapses the intrathoracic airway).[1]
| [{"header":"Stridor quality"},{"header":"Level"},{"header":"Typical causes"}] |
|---|
- A change in phase is a red flag: a purely inspiratory stridor that becomes biphasic means the obstruction is worsening and approaching the glottis — the airway must be secured now.[1]
- Volume is not severity. A fatiguing patient with a rising PaCO₂ breathes less forcefully, and the stridor quietens just before complete obstruction. A "quieter" stridor with agitation, accessory-muscle use, tracheal tug, or falling SpO₂ is pre-arrest.[1]
- Stertor (snoring) — a coarse, low-pitched sound from the oronasal cavity and pharynx (soft palate, tongue base) — is distinct from stridor (a higher-pitched sound from the larynx or trachea). Stertor localises to the nose, palate, or tongue base and is usually positional; stridor localises to the larynx and below.
- The tripod position (sitting forward, leaning on outstretched arms, jaw thrust forward) is a physiologic rescue, not a comfort choice: the shoulder girdle splints the accessory muscles of respiration, gravity drains secretions, and the position maximises airway patency by preserving muscle tone. Forcing a tripod patient to lie flat for an airway attempt is a classic cause of complete obstruction.[1]
Causes by level
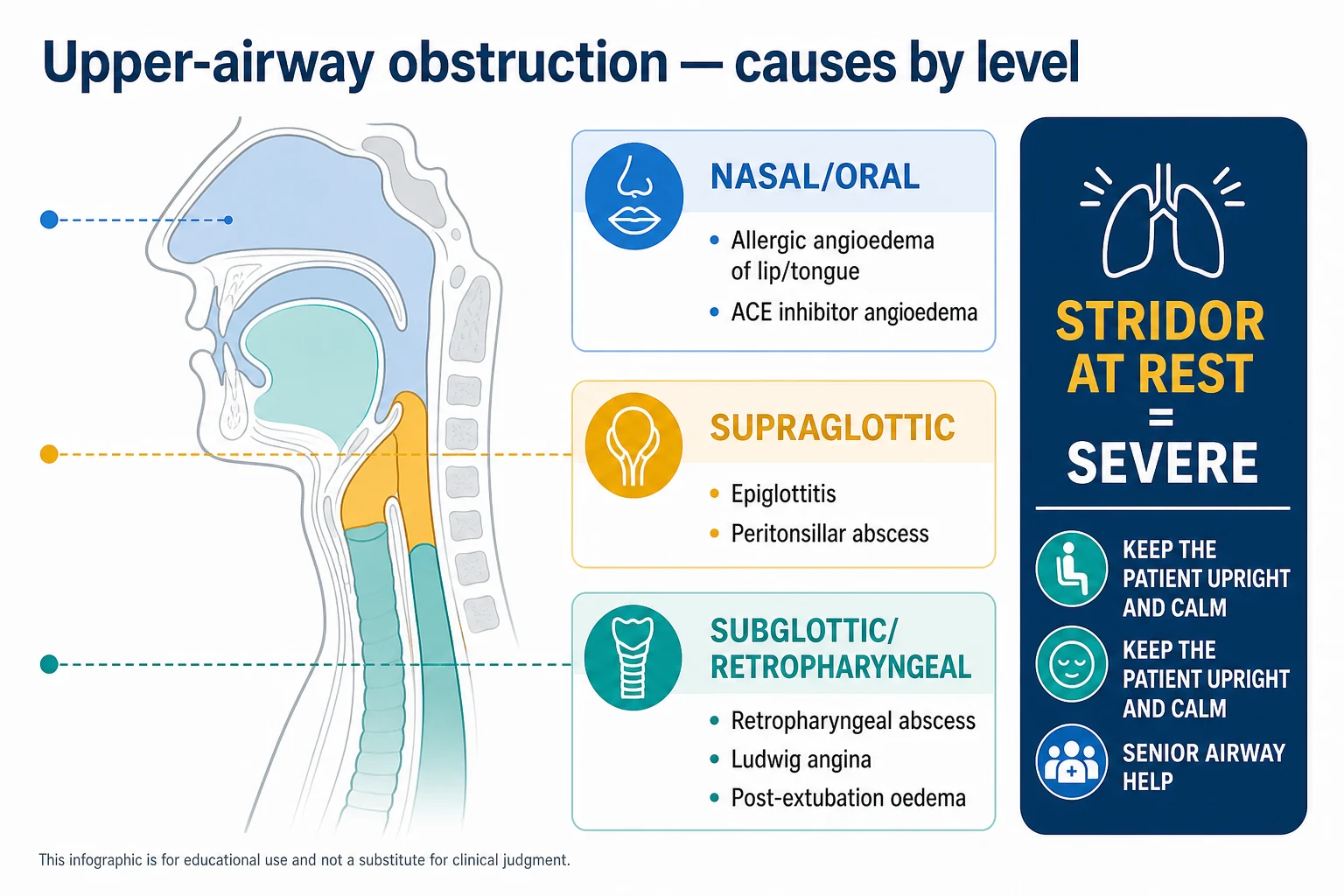
- Oral cavity and tongue — allergic (histamine) angioedema, ACE-inhibitor angioedema (bradykinin), hereditary angioedema.
- Supraglottis — epiglottitis (supraglottitis), peritonsillar abscess (quinsy).
- Subglottis and deep neck spaces — retropharyngeal abscess, Ludwig's angina, post-extubation laryngeal oedema, foreign body.[1]
Pathophysiology — why narrowing collapses the airway
Airflow through the upper airway follows the relationship between driving pressure, airway radius, gas density, and flow regime. The clinical lessons flow from two physical principles:[1]
- Poiseuille's law (laminar flow) — flow is proportional to radius⁴. Halving the radius reduces laminar flow sixteen-fold. Even one millimetre of mucosal oedema on a small child's airway (or on an already narrowed adult airway) is catastrophic.
- The Reynolds number and turbulent flow — as the airway narrows, gas velocity rises and flow becomes turbulent (high Reynolds number). Turbulent flow is far less efficient than laminar flow and is highly density-dependent: a denser gas (air) requires more driving pressure per unit of flow than a less dense gas (a helium–oxygen mixture, Heliox). This single principle is the entire rationale for Heliox.[14]
| [{"header":"Property"},{"header":"Laminar flow"},{"header":"Turbulent flow"}] |
|---|
Clinical consequences:[4]
- Oedema produces a fixed structural narrowing, but the dynamic component (the airway wall collapsing inward on inspiration) makes obstruction worse with effort — agitating the patient, lying them flat, or forcing a child to cry increases turbulent flow and worsens obstruction. Keeping the patient calm and upright is a real treatment, not just a comfort measure.[1]
- A child's airway is small in absolute terms: 1 mm of oedema on a 5 mm-diameter cricoid reduces the cross-sectional area by ~64%. The same oedema on a 15 mm adult trachea reduces it by only ~25%. This is why children decompensate faster and why paediatric epiglottitis/croup were once the leading causes of airway death in young children.
- Heliox (typically 79% helium / 21% oxygen, or 70:30) is a temporising measure only — it buys time by reducing the work of breathing through a narrowed airway. It does NOT treat the underlying cause, and it limits the FiO₂ that can be delivered (a 79:21 mix delivers only 21% oxygen). Heliox is useless in the patient who is already significantly hypoxaemic.[14]
- Hypoxia is a late sign. The upper airway is a high-resistance system; the patient compensates by increasing the work of breathing for a long time before oxygenation fails. A normal SpO₂ does not exclude critical obstruction — exhaustion, hypercapnia, and arrest can occur with a normal oxygen saturation until the very end.[1]
Epiglottitis (supraglottitis)
Acute infection and swelling of the epiglottis and supraglottic structures, historically Haemophilus influenzae type b in children (now rare after Hib vaccination) and in adults caused by streptococci, pneumococci, and other pathogens.[1]
- Clinical: rapid onset, high fever, severe sore throat out of proportion to the visible findings, dysphagia, drooling, a muffled voice, and tripoding. Stridor is a late, ominous sign. The "four Ds" — drooling, dysphagia, dysphonia, distress.[1]
- The critical rule: do not instrument the airway (no tongue depressor, no blind laryngoscopy) in the unsecured airway, because this can precipitate complete obstruction. Keep the patient (especially a child) in the position of comfort; do not force them to lie flat.[1]
- Management: senior airway help early; secure the airway in a controlled setting (theatre, with a surgical airway plan) — intubation is often very difficult. Give intravenous antibiotics (a third-generation cephalosporin such as ceftriaxone, covering H. influenzae); add dexamethasone. Nebulised adrenaline and humidified oxygen may temporise.[1]
- Diagnosis is clinical; a lateral neck X-ray may show the thumb sign (a swollen epiglottis) but only if it does not upset the patient. In the unstable patient, secure the airway first.[1]
| [{"header":"Feature"},{"header":"What to know"}] |
|---|
The Hib vaccine has shifted epiglottitis from a childhood disease to one predominantly of adults. The classic paediatric picture — a toxic, drooling, tripoding child who will not lie flat — is now rare; in adults, comorbidity (diabetes, immunocompromise, alcoholism) and atypical pathogens broaden the differential. The principle that stridor is a late, pre-arrest sign and that the airway must be secured in a controlled setting before decompensation is unchanged.[1]
Angioedema
Angioedema is rapid, deep, non-pitting swelling of the subcutaneous and submucosal tissues. Two mechanisms differ in treatment:[1][2]
Histamine-mediated (allergic)
- Triggered by food, drug, insect sting, or idiopathic; often with urticaria and itching.
- Responds to adrenaline, antihistamines, and corticosteroids — the treatment of anaphylaxis if severe.[1]
Bradykinin-mediated
- Hereditary angioedema (HAE) — deficiency or dysfunction of C1-esterase inhibitor; recurrent attacks of swelling without urticaria or itching. Treated with C1-INH concentrate, the bradykinin-B2 antagonist icatibant, or the kallikrein inhibitor ecallantide.[2]
- ACE-inhibitor angioedema — bradykinin accumulates because ACE (kininase II) normally degrades it. Swelling of the lips, tongue, and face, without urticaria, can occur even years after starting the drug (more common in Black patients). It does not respond to adrenaline, antihistamines, or steroids (it is bradykinin, not histamine). Management: stop the ACE inhibitor, supportive care and airway monitoring (swelling can progress over many hours), and for severe or refractory cases C1-INH concentrate or icatibant. The patient must never take an ACE inhibitor again.[1][2]
| [{"header":"Feature"},{"header":"Histamine (allergic)"},{"header":"Bradykinin (HAE / ACEi / acquired)"}] |
|---|
ACE-inhibitor angioedema — the high-yield detail[10][11][12]
- Up to 40% of all emergency angioedema presentations are ACE-inhibitor related; the lifetime incidence in patients on an ACE inhibitor is 0.1–0.7%, but rises to ~5% in patients of Black African ancestry (lower kininase activity, polymorphisms in the aminopeptidase P pathway).[13]
- Onset can be months to years after starting the drug — a key teaching point. The mechanism is accumulation of bradykinin (ACE = kininase II, the major bradykinin-degrading enzyme). It is NOT histamine, so it does not respond to adrenaline, antihistamines, or steroids.[10]
- The swelling predominantly affects the lips, tongue, and face; laryngeal involvement is less common than in HAE but can be rapidly fatal. The airway can continue to worsen for >24 h despite stopping the drug — observe closely.[12]
- Specific therapy — C1-INH concentrate (20 U/kg IV) or icatibant 30 mg SC — shortens attack duration in case series, randomised trials, and meta-analysis, although high-quality evidence in ACEi disease specifically remains limited and guidelines emphasise that airway protection, not pharmacotherapy, is the priority.[10][11][12]
- The patient must never take an ACE inhibitor again — re-challenge is dangerous. Switch to an alternative (an angiotensin-receptor blocker — though ARBs rarely cause the same — or a calcium-channel blocker).[13]
Hereditary angioedema — the high-yield detail[6][7][9]
- Type I (85%): low C1-INH antigen and function. Type II (15%): normal or high antigen but low function (a dysfunctional protein). Type III (rare, oestrogen-related, normal C1-INH): nearly always women; some have factor XII mutations.[6]
- Diagnosis: low C4 (always, during and between attacks — the screening test), low or dysfunctional C1-INH, normal C1q (which distinguishes acquired from hereditary — C1q is low in acquired).[6][9]
- Triggers: trauma (especially dental work), stress, infection, oestrogen (the oral contraceptive pill, HRT, pregnancy), and ACE inhibitors — a HAE patient on an ACE inhibitor is at very high risk of laryngeal attack.[7]
- Laryngeal attacks are the leading cause of death in HAE — untreated, airway obstruction is fatal in about one-third of laryngeal attacks. All HAE patients should carry home therapy (icatibant SC or self-administered C1-INH) and a medical alert.[7][8][9]
- Long-term prophylaxis: first-line lanadelumab (anti-kallikrein monoclonal, SC every 2 weeks), berotralstat (oral plasma kallikrein inhibitor), or plasma-derived C1-INH. Avoid attenuated androgens (danazol, stanozolol) where possible — they are effective but virilising and hepatotoxic.[7]
Deep neck infections
- Peritonsillar abscess (quinsy) — collection beside the tonsil; severe sore throat, trismus, a muffled voice, uvular deviation away from the abscess, and a bulging tonsil. Treat with needle drainage or incision and drainage plus antibiotics.[1]
- Retropharyngeal abscess — pus in the retropharyngeal space (lymph nodes in children; trauma or foreign body in adults); neck stiffness, dysphagia, stridor, and a widened prevertebral soft-tissue stripe on a lateral neck X-ray. Confirm with CT; treat with surgical drainage and antibiotics.[1]
- Ludwig's angina — a rapidly spreading cellulitis of the submandibular and sublingual spaces, usually of dental origin; the floor of the mouth swells and elevates and displaces the tongue backwards, a direct airway threat. Treat with broad-spectrum antibiotics, airway securing (often very difficult), and surgical drainage of the source.[1]
Ludwig's angina — the high-yield detail[16]
- A bilateral, rapidly spreading cellulitis of the sublingual and submandibular spaces, almost always of dental origin — typically an infected lower second or third molar whose root tracks below the mylohyoid line into the submandibular space.[16]
- The hallmarks: brawny, woody submandibular induration (not fluctuant — it is a cellulitis, not an abscess), trismus, drooling, dysphagia, and a displaced, elevated, protruding tongue that the patient cannot retract — a direct mechanical airway threat.[1][16]
- Microbiology is polymicrobial — oral streptococci, anaerobes (Peptostreptococcus, Prevotella, Fusobacterium), and sometimes Staphylococcus; cover with ampicillin-sulbactam or clindamycin plus a third-generation cephalosporin ± metronidazole. Add vancomycin/linezolid if MRSA is plausible.[16]
- Airway management is the trap. Direct laryngoscopy is often impossible (distorted, bloody field; the tongue cannot be displaced); awake fibre-optic intubation is the usual first choice but may also fail in the distorted, secretions-flooded airway. An awake tracheostomy under local anaesthesia, performed by an experienced surgeon, is frequently the safest definitive airway — and should be planned from the outset.[1][16]
- Treat the source: extract the offending tooth and drain the submandibular space once the airway is secured; a contrast CT neck defines the extent once the airway is safe. Do not send an unstable patient to CT.[16]
Peritonsillar and retropharyngeal abscess — the high-yield detail
- Peritonsillar abscess (quinsy) is the most common deep-neck abscess in adults. The classic findings are trismus, a muffled 'hot potato' voice, uvular deviation away from the abscess, and a bulging, erythematous anterior tonsillar pillar. Drainage (needle aspiration or incision and drainage) plus antibiotics (penicillin + metronidazole or clindamycin) is curative; intubation is rarely needed unless the swelling extends into the parapharyngeal or retropharyngeal space.[1]
- Retropharyngeal abscess sits in the potential space between the buccopharyngeal fascia anteriorly and the alar fascia posteriorly, extending from the skull base to the mediastinum (so it can cause descending necrotising mediastinitis — a surgical emergency). In children it follows suppurative lymphadenitis (the retropharyngeal nodes regress after age 4–5); in adults it follows trauma (fish bone), foreign body, or dental/cervical infection. The lateral neck X-ray shows a widened prevertebral soft-tissue stripe (>7 mm at C2, or >14 mm at C6 in adults, in a true lateral film); confirm with contrast CT.[1]
- The retropharyngeal space communicates with the danger space (between the alar and prevertebral fasciae), which runs the full length of the posterior mediastinum to the diaphragm — the route by which retropharyngeal infection descends to cause mediastinitis and an empyema.[1]
General management of the obstructed upper airway
- Keep the patient upright and calm in the position of comfort; agitation and crying worsen obstruction (especially in children).
- Give humidified oxygen; Heliox (lower-density gas) reduces the work of breathing through a narrowed airway; nebulised adrenaline (racemic adrenaline) reduces inflammatory mucosal oedema; dexamethasone for its delayed anti-oedema effect.
- Call for senior airway help early and prepare for a difficult airway: awake fibre-optic intubation in a controlled setting, or a surgical airway (cricothyroidotomy or tracheostomy) if the upper airway cannot be secured.[1][2]
- Treat the underlying cause (antibiotics for infection, stop the offending drug, specific agents for angioedema).
- Avoid lying the patient flat, agitating them, or instrumenting the airway unnecessarily — the "do no harm" principle.[1]
Temporising agents in detail
| [{"header":"Agent"},{"header":"Mechanism"},{"header":"Dose"},{"header":"Onset / duration"},{"header":"Caveat"}] |
|---|
Securing the airway — the difficult-airway plan
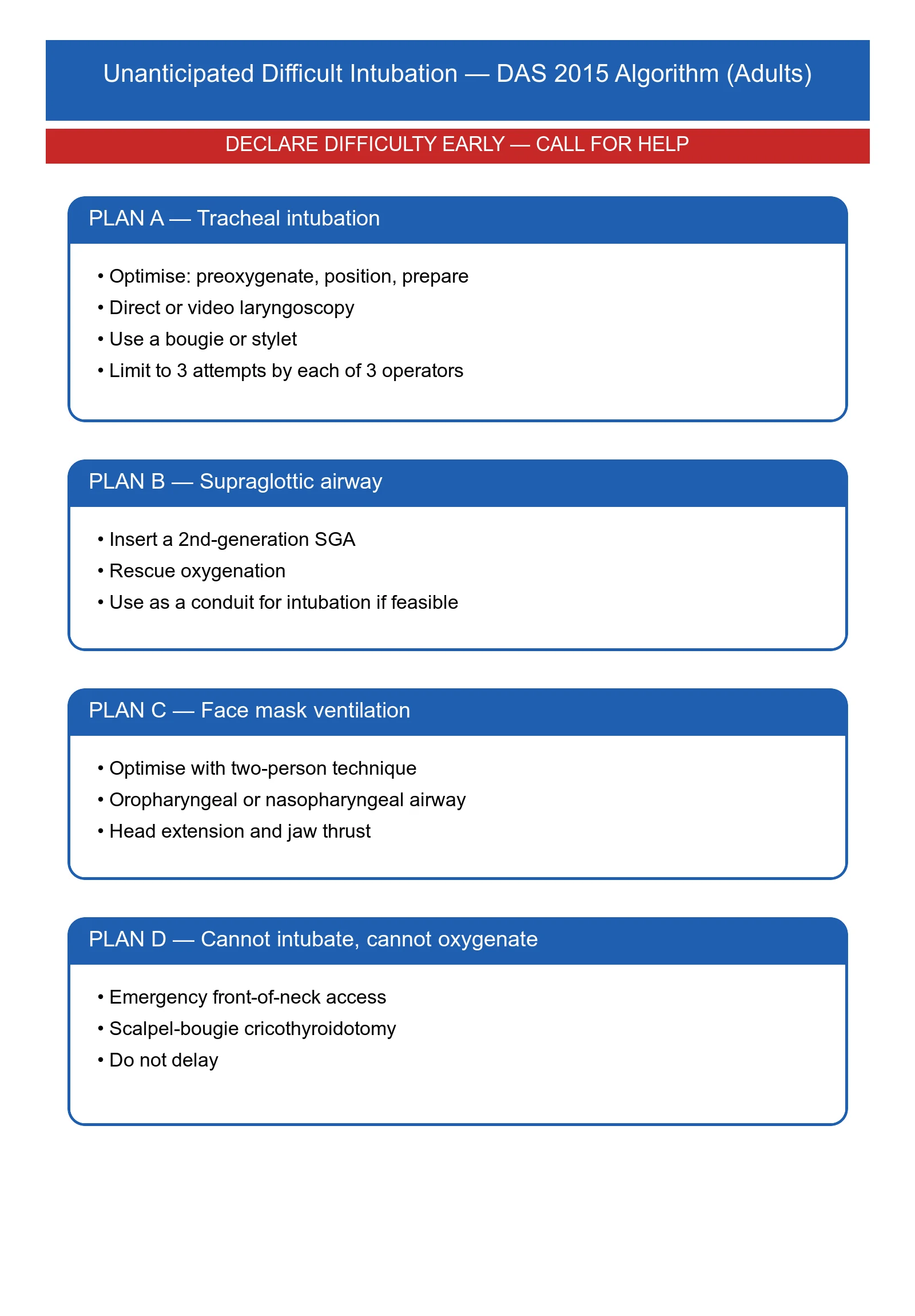
The obstructed upper airway is the canonical 'can't intubate, can't oxygenate' (CICO) scenario. The Difficult Airway Society 2015 and 2018 guidelines, and the lessons of NAP4, converge on a structured plan:[3][4][5]
- Call for senior help early — the most senior airway operator (anaesthetist/ICU), a senior ENT/head-and-neck surgeon, and a second skilled pair of hands. NAP4 showed that delayed senior input is a recurring theme in airway deaths.[4]
- Pre-oxygenase in the sitting position, with full monitoring (ECG, SpO₂, NIBP, capnography once intubated). A cooperative patient breathing spontaneously on humidified oxygen in the position of comfort is the safest state to plan from.
- Primary plan: awake fibre-optic intubation (AFOI) in the cooperative adult, performed in theatre, with the surgical airway kit open and an ENT surgeon scrubbed.[3][5]
- Backup plan: a carefully prepared intravenous induction with a rigid bronchoscope and a senior surgeon standing by — used when the patient cannot cooperate with AFOI (paediatric, agitated, peri-arrest).[3]
- Rescue plan (CICO): scalpel–bougie–tube cricothyroidotomy (the DAS 2015 standard emergency surgical airway).[5]
Emergency surgical airway (eFONA) — the DAS 2015 scalpel–bougie cricothyroidotomy
Identify CICO and call for help
Failure to intubate AND failure to oxygenate (facemask + supraglottic airway). Declare "Can't intubate, can't oxygenate" out loud, call for the surgical airway kit and the most senior surgeon available. Optimise: extend the neck if no c-spine injury, palpate the cricothyroid membrane.
Position and identify the cricothyroid membrane
Extend the neck (shoulder roll). Palpate the laryngeal prominence, slide down to the cricothyroid membrane (the soft dip between the thyroid cartilage above and the cricoid ring below). If the membrane cannot be felt (obese, distorted anatomy), plan a vertical laryngeal-to-suprasternal skin incision to identify landmarks by palpation.
Transverse stab incision
Stab incision through skin and cricothyroid membrane in the midline with a **size 10 or 20 scalpel blade**, transversely, blade pointing towards the feet, until air is aspirated/heard. Keep the blade in situ.
Open the tract and traction
Rotate the blade 90° to open the membrane, or pass a tracheal hook to traction the thyroid cartilage cephalad (Trousseau). The goal is a visible, patent tract into the trachea.
Bougie and railroad the tube
Pass a gum-elastic bougie through the incision angled downwards into the trachea (feel for hold-up or tracheal rings). Railroad a **size 6.0 cuffed ETT** (or a dedicated surgical-airway tube) over the bougie. Remove the bougie.
Confirm and secure
Inflate the cuff, ventilate, confirm with **waveform capnography** (the definitive sign), secure the tube, and arrange formal surgical revision (usually conversion to a formal tracheostomy). Document the indication, time, operator, and complications.
Common technical failures (the viva expects you to know these):[5]
- Inadequate/incision too superficial — the most common failure. The blade must traverse skin, subcutaneous fat, and the membrane in one stab. In the obese, a deliberate vertical (then transverse) "laryngeal palpation" technique is recommended.
- Tube too large for the cricothyroid membrane — use a size 6.0 cuffed tube; a too-large tube will not seat and will leak.
- Bougie kinking or oesophageal placement — keep the bougie angled caudally; if no hold-up or tracheal rings are felt, withdraw and re-pass.
- Late failure — the tube dislodges or the cuff leaks; secure meticulously and arrange formal revision to a tracheostomy.[15]
Other important causes of upper-airway obstruction
Bilateral vocal cord palsy (BVCP)
- Mechanism — bilateral recurrent laryngeal nerve injury causes both cords to lie in the paramedian position (the unopposed action of the cricothyroid muscle), producing a glottic narrowing that presents as biphasic stridor at rest.[1]
- Causes — thyroid surgery (the classic cause; risk after total thyroidectomy, especially with central neck dissection or revision surgery), thyroid malignancy, post-intubation, a prolonged nasogastric/nasotracheal tube, skull-base or mediastinal tumour, and idiopathic (often attributed to viral neuronitis). The left recurrent laryngeal nerve's long intrathoracic course (around the aortic arch) makes it vulnerable to lung-apex tumour, aortic aneurysm, mediastinal nodes, and mitral surgery — the Ortner syndrome (cardiovocal syndrome).[1]
- Clinical — inspiratory stridor (often biphasic), exertional dyspnoea, a weak or breathy voice (the cords cannot fully adduct or abduct), and aspiration. The patient may compensate for months or years and then decompensate with a respiratory infection (added oedema on top of the narrowed glottis).[1]
- Management — secure the airway (AFOI is the primary plan; the distorted glottic anatomy makes a blind RSI dangerous); definitive treatment is surgical — cord lateralisation, arytenoid adduction, posterior cordotomy, or tracheostomy depending on the underlying cause, prognosis, and the prospect of recovery (which is most likely if the nerve is in continuity after thyroid surgery — wait 6–12 months before definitive surgery).[1]
Post-extubation stridor / laryngeal oedema
- Cause — laryngeal oedema (cuff pressure on the glottic/subglottic mucosa) after prolonged intubation, especially in women, with oversized tubes, with high cuff pressures, and after a difficult or traumatic intubation. Up to ~40% of long-stay ICU patients have some laryngeal oedema on endoscopic examination; clinically significant stridor occurs in ~5–16%.[17][18]
- Risk factors — female sex, large tube size (>8.0 in women, >8.5 in men), prolonged intubation (>36–48 h), high cuff pressure (>30 cmH₂O), excessive cuff movement (restlessness, inadequate sedation), traumatic intubation, and concurrent laryngopharyngeal reflux.[18]
- The cuff-leak test — deflate the ETT cuff and listen for an air leak around the tube. No leak (or a leak volume <110–250 mL on a defined volume-controlled breath, depending on protocol) predicts a higher risk of post-extubation stridor. The test has a high false-positive rate and is not used in isolation to delay extubation, but a good audible leak is reassuring.[15]
- Prophylaxis — systemic corticosteroids (e.g. methylprednisolone 20–40 mg IV q6h starting 12–24 h before extubation, or dexamethasone 8 mg IV q8h × 4 doses pre-extubation) reduce the rate of post-extubation stridor and reintubation in high-risk patients (especially adults intubated >36 h); evidence in unselected patients is weaker.[17][18]
- Management of established stridor — sit the patient up, nebulised adrenaline 1:1000 5 mg, dexamethasone 8 mg IV, Heliox if available; and a low threshold for reintubation before the airway is lost — each successive laryngeal-oedema episode is worse, and a patient who was difficult to intubate the first time will be much harder the second time, with distorted anatomy and an oedematous glottis.[17][18]
Foreign-body upper-airway obstruction
- Adults — typically an aspirated food bolus (the "café coronary") — meat, bread, or poorly chewed food, especially in the elderly, the intoxicated, or the denture-wearer. The patient cannot speak, breathe, or cough — sudden silent collapse at the dinner table. Treat with back blows, abdominal thrusts (Heimlich), and chest thrusts; if the patient becomes unconscious, CPR with a look in the mouth before each ventilation. Laryngoscopy with Magill forceps may retrieve a visible supraglottic foreign body; blind finger sweeps are avoided (they may push the object further down).[1]
- Children — small objects (nuts, grapes, balloons, coins, small toys); a partial obstruction presents with cough, stridor, and wheeze; a complete obstruction is silent. Back blows (infant), abdominal/chest thrusts (child). Examine a child with new stridor or persistent unilateral wheeze for an aspirated foreign body, especially if the chest X-ray shows hyperinflation or atelectasis of one lobe.[1]
- ICU/anaesthetic management of a suspected lower-airway foreign body — rigid bronchoscopy under general anaesthesia (a ventilating rigid bronchoscope) by an experienced operator; AFOI is usually inappropriate (the object may be pushed distally or obstruct the working channel).[1]
Tumour and haematoma
- Laryngeal or pharyngeal tumour (squamous cell carcinoma) produces a slowly progressive biphasic stridor with dysphonia, dysphagia, weight loss, and (often) a neck mass. Airway management: AFOI is the primary plan in the cooperative patient — these airways are distorted, and the tumour can fragment and bleed; an RSI in a previously-untreated tumour risks complete loss of the airway. Coordinate with the head-and-neck surgeon for a surgical airway plan.[3]
- Neck haematoma — most commonly post-thyroid or post-carotid surgery, or after central line insertion or cervical spine surgery. A rapidly expanding, tense, painful neck swelling with stridor and a wound under pressure is a surgical emergency. Open the wound at the bedside (remove the sutures, evacuate the clot) to decompress the airway before transfer to theatre — this is a high-yield exam answer. Definitive airway management is then extremely difficult because the anatomy is distorted and the airway compressed; an experienced team is essential.[1]
| [{"header":"Cause"},{"header":"Stridor phase"},{"header":"Key clue"},{"header":"First step"}] |
|---|
Key trials and guidelines
Higgs 2018 — DAS guidelines for intubation in critically ill adults (PMID 29406182)
Cook 2011 — NAP4 (PMID 21447488)
Frerk 2015 — DAS guidelines for unanticipated difficult intubation in adults (PMID 26556848)
Maurer 2018 — WAO/EAACI guideline for the management of hereditary angioedema (PMID 29318628)
Zuraw 2008 — hereditary angioedema (NEJM Clinical Practice) (PMID 18768946)
Cicardi 2010 — icatibant for HAE (FAST-3) (PMID 20818888)
Bas 2010 — icatibant for ACE-inhibitor angioedema (PMID 20447725)
Moraa 2018 — Heliox for croup (Cochrane) (PMID 30371952)
De Bast 2002 — the cuff-leak test (PMID 12209275)
Pluijms 2015 — post-extubation laryngeal oedema (PMID 26395175)
Jeon 2019 — icatibant for ACE-inhibitor angioedema meta-analysis (PMID 31290163)
Iwu 1990 — Ludwig's angina: review of current concepts (PMID 2135660)
SAQ — Acute epiglottitis in the adult
10 minutes · 10 marks
A 52-year-old man presents to the emergency department with a 12-hour history of severe sore throat, fever, drooling, and difficulty swallowing his own saliva. He is sitting forward in a tripod position, with muffled voice, stridor, and a respiratory rate of 28. His SpO2 is 94% on room air. Indirect laryngoscopy by the ENT registrar shows a swollen, cherry-red epiglottis.
SAQ — Hereditary angioedema with laryngeal involvement
10 minutes · 10 marks
A 34-year-old woman presents to the emergency department with progressive lip, tongue, and facial swelling over the past 6 hours, now with muffled voice and difficulty swallowing. She has had similar episodes since childhood, usually triggered by minor trauma or stress. She is not on any regular medication except the oral contraceptive pill. Her father has similar episodes. Her SpO2 is 96% on room air but she has audible stridor.
Red flags
High-yield clinical pearls
Prognosis and follow-up
The outcome of an upper-airway obstruction episode depends almost entirely on whether the airway was secured in a controlled setting before the patient arrested. Adult epiglottitis now has a mortality of ~1–2% (predominantly from airway loss in the unsecured patient); Ludwig's angina mortality has fallen from >50% in the pre-antibiotic era to <5% with modern surgical and antibiotic management; HAE laryngeal attacks were once fatal in ~30% and are now rare causes of death where specific therapy is available.[6][16]
After any upper-airway-obstruction episode: document the airway findings (laryngoscopy findings, technique used, time taken, agents, complications); place an airway alert in the chart and on the patient's electronic record; arrange difficult-airway identification (MedicAlert bracelet, patient-held letter, registry entry); and debrief the team, especially if any step did not go to plan. For patients with structurally difficult airways (radiotherapy, laryngeal tumour, prior difficult intubation, subglottic stenosis, HAE), flag the chart for future AFOI as the default technique and ensure the patient carries the relevant specific therapy (icatibant or C1-INH for HAE).[1][3]
References
- [1]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [2]Wilkerson RG, Moellman JJ Hereditary Angioedema. Emergency medicine clinics of North America, 2022.PMID 34782094
- [3]Higgs A, McGrath BA, Goddard C, et al. Guidelines for the management of tracheal intubation in critically ill adults. British journal of anaesthesia, 2018.PMID 29406182
- [4]Cook TM, Woodall N, Frerk C (eds); Fourth National Audit Project Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society (NAP4). Br J Anaesth 2011; 106(5): 617-631, 2011.PMID 21447488
- [5]Frerk C, Mitchell VS, McNarry AF, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. British journal of anaesthesia, 2015.PMID 26556848
- [6]Zuraw BL Clinical practice. Hereditary angioedema. N Engl J Med 2008; 359(10): 1027-1036, 2008.PMID 18768946
- [7]Maurer M, Magerl M, Anostegui I, et al The international WAO/EAACI guideline for the management of hereditary angioedema - the 2017 revision and update. Allergy 2018; 73(8): 1575-1596, 2018.PMID 29318628
- [8]Cicardi M, Banerji A, Bracho F, et al Icatibant, a new bradykinin-receptor antagonist, in hereditary angioedema. N Engl J Med 2010; 363(6): 532-541 (FAST-3 trial), 2010.PMID 20818888
- [9]Christiansen SC, Zuraw BL Hereditary angioedema: management of laryngeal attacks. Am J Rhinol Allergy 2011; 25(6): 379-382, 2011.PMID 22185739
- [10]Bas M, Greve J, Stelter K, Bier H, Stark T, Hoffmann TK, Kojda G, Strassen U Therapeutic efficacy of icatibant in angioedema induced by angiotensin-converting enzyme inhibitors: a case series. Ann Emerg Med 2010; 56(3): 278-282, 2010.PMID 20447725
- [11]Jeon J, Lintner S, Bensman S, Hatipoglu S Effect of icatibant on angiotensin-converting enzyme inhibitor-induced angioedema: a meta-analysis of randomized controlled trials. J Clin Pharm Ther 2019; 44(5): 701-707, 2019.PMID 31290163
- [12]Riha HM, Matthews JM, Davis GA, Morgan LA, Drew CJ, Cohn E, Bolesta S Novel therapies for angiotensin-converting enzyme inhibitor-induced angioedema: a systematic review of current evidence. J Emerg Med 2017; 53(5): 662-679, 2017.PMID 28939396
- [13]van den Elzen MT, van der Valk ES, Rockmann H, Arendt S, van Hagen PM, van der Zwan A, Rijneveld AW, Dalm VASH Efficacy of treatment of non-hereditary angioedema. Clin Rev Allergy Immunol 2018; 54(3): 402-413, 2018.PMID 27672078
- [14]Moraa I, Sturman N, McGuire TM, van Driel ML Heliox for croup in children. Cochrane Database Syst Rev 2018; 10: CD006822, 2018.PMID 30371952
- [15]De Bast Y, De Backer D, Moraine JJ, Lemaire M, Vandenborght C, Vincent JL The cuff leak test to predict failure of tracheal extubation for laryngeal edema. Intensive Care Med 2002; 28(9): 1267-1272, 2002.PMID 12209275
- [16]Iwu CO Ludwig's angina: report of seven cases and review of current concepts in management. Br J Oral Maxillofac Surg 1990; 28(3): 189-193, 1990.PMID 2135660
- [17]Wittekamp BHJ, van Mook WNKA, Tjan DHT, Zwaveling JH, Bergmans DCJJ Clinical review: post-extubation laryngeal edema and extubation failure in critically ill adult patients. Crit Care 2009; 13(6): 233, 2009.PMID 20017891
- [18]Pluijms WA, van Mook WNKA, Wittekamp BHJ, Bergmans DCJJ Postextubation laryngeal edema and stridor resulting in respiratory failure in critically ill adult patients: updated review. Crit Care 2015; 19: 295, 2015.PMID 26395175