ICU · Resuscitation
Hypothermia and environmental emergencies
Also known as Accidental hypothermia · Swiss staging system · ECMO rewarming · Osborn (J) waves · Drowning and near-drowning
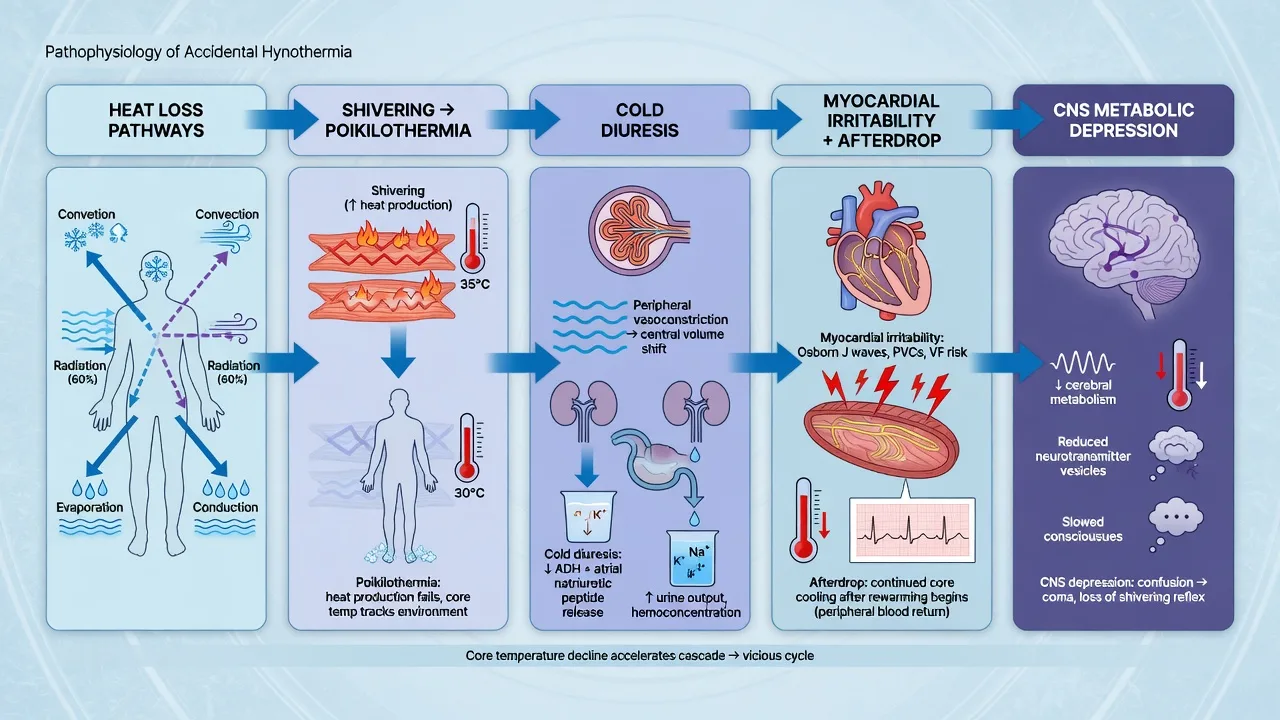
Accidental hypothermia is a core temperature below 35C. Swiss staging: HT I (35-32C, conscious, shivering), HT II (32-28C, altered consciousness, no shivering), HT III (28-24C, unconscious), HT IV (24-13.7C, vital signs present), HT V (<13.7C, cardiac arrest). Management: active rewarming (forced air, warm IV fluids) for HT I-II. HT III-IV: active internal rewarming (warm bladder/colonic lavage, ECMO/extracorporeal). HT V (cardiac arrest): full cardiopulmonary bypass or VA-ECMO — rewarm to 32C before declaring death ('no one is dead until warm and dead'). Key ECG: Osborn (J) waves. Arrhythmias: avoid adrenaline/antiarrhythmics until rewarm to 30C. Near-drowning: lung-protective ventilation, avoid routine steroids/antibiotics, primary lung injury from submersion.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Swiss staging system
Swiss hypothermia staging (click each)
28-24C — Unconscious
Severe hypothermia. Unconscious, may have vital signs. High arrhythmia risk. Active INTERNAL rewarming: warm bladder/colonic/peritoneal lavage, or ECMO/extracorporeal. Handle gently (rough handling can trigger VF).
ECG changes
[8]Rewarming strategy
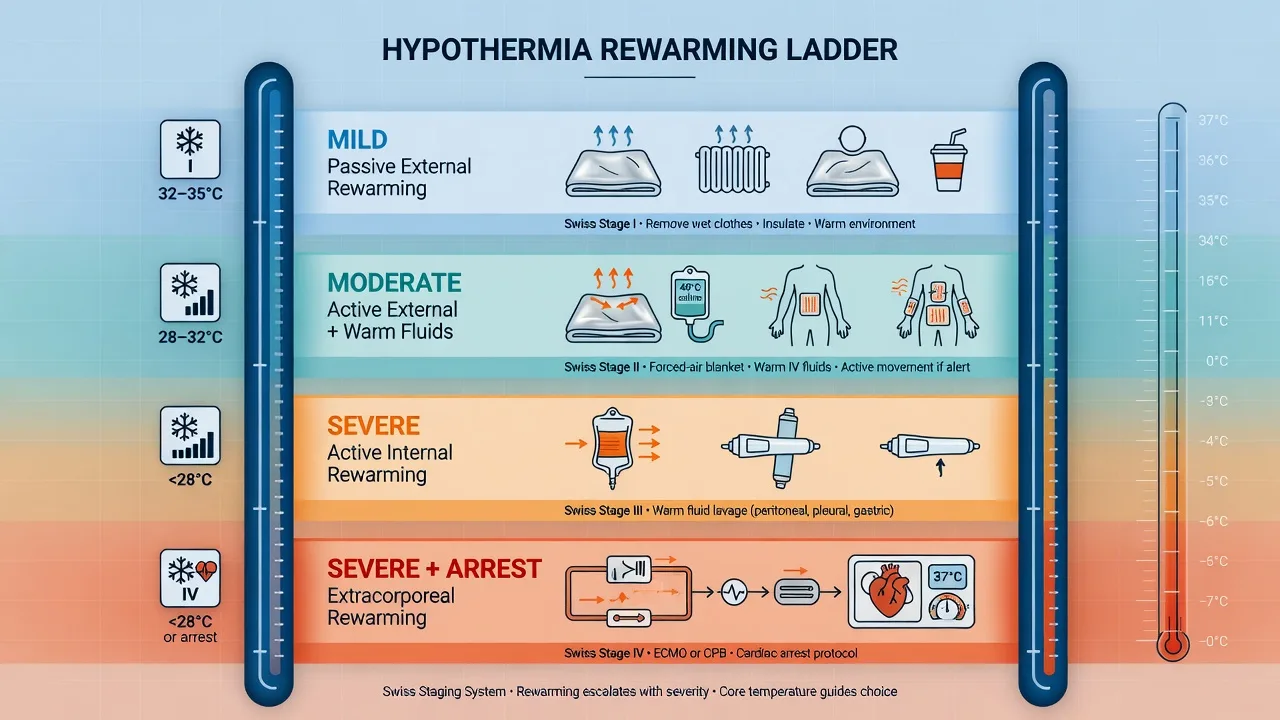
Rewarming protocol by severity
HT I-II (32-35C): Active external rewarming
Forced air warming blanket (Bair Hugger), warm oral/IV fluids (38-42C), remove wet clothing, dry insulation. Rewarm at 0.5-1C/h. Monitor cardiac rhythm. Most patients recover within hours.
HT III-IV (24-32C): Active internal rewarming
All external measures PLUS active internal rewarming: warmed IV fluids (42C), warm bladder lavage (42C saline via 3-way catheter), warm colonic/peritoneal lavage. Consider ECMO/VA-ECMO for HT IV or if not responding. Handle patient gently — rough handling triggers VF.
HT V (cardiac arrest): ECMO/cardiopulmonary bypass
FULL CPR (modified: withhold adrenaline if <30C, give adrenaline at standard intervals if >30C). VA-ECMO or cardiopulmonary bypass is treatment of choice (rapid rewarming + circulatory support). Rewarm to 32C before ceasing resuscitation. "No one is dead until warm and dead." Survivals documented at 13.7C.
Avoid "afterdrop"
Afterdrop = core temperature falls further when peripheral vasodilation returns cold blood to core. Prevent by: rewarming trunk BEFORE extremities, rewarm at 0.5-1C/h (not faster for chronic hypothermia). For acute hypothermia (submersion), faster rewarming is safer.
Medication considerations
Drug metabolism is impaired in hypothermia. AVOID adrenaline/antiarrhythmics if core temp <30C (ineffective, may accumulate). Modified ALS: give adrenaline every other cycle if 30-35C, withhold if <30C. Once rewarm to >30C, resume standard dosing. Rewarm before giving any drugs.
Near-drowning
Near-drowning
Non-fatal submersion
- Primary injury: hypoxic brain injury + acute lung injury (aspiration)
- Secondary: ARDS, pneumonia (especially polluted water), electrolyte disturbance
- Management: lung-protective ventilation, avoid routine steroids/antibiotics/prophylactic barbiturates
- Monitor for ARDS (develops over 4-6h)
- Do NOT use the Heimlich unless airway obstruction
SAQ — Accidental hypothermia: rewarming strategy and arrhythmia management
10 minutes · 10 marks
A 55-year-old homeless man is found unconscious in a park in winter. His core temperature is 27°C, he has an Osborn wave on ECG, a slow junctional rhythm at 30/min, and a palpable faint pulse. He is brought to the ED. Outline the staging, rewarming strategy, and management of arrhythmias.
SAQ — Targeted temperature management after cardiac arrest
10 minutes · 10 marks
A 60-year-old man is admitted to ICU comatose after out-of-hospital VF cardiac arrest with ROSC at 25 minutes. The team asks whether to cool him, to what temperature, and for how long. Outline the evidence and your management.
Clinical pearls
Red flags
ED approach to the hypothermic patient
The first 10 minutes decide survival in severe hypothermia. The single most dangerous moment is movement of the cold, irritable myocardium — every transfer, log-roll, and line insertion is a VF trigger. The ED approach is built around protecting the heart while rewarming.[4]
ED resuscitation of the hypothermic patient (stepwise)
1. Scene and pre-hospital — minimise handling
Rescue gently. Horizontal rescue (sitting a hypothermic patient up causes cold, acidotic blood to return to the core → VF). Remove wet clothing and dry the patient at the scene. Insulate (reflective foil, blanket). Do NOT massage extremities. HT I-II may mobilise; HT III-IV should be kept flat.
2. Airway and breathing
Intubate if GCS <8, unable to protect airway, or hypoxaemic despite oxygen. Intubate GENTLY (pre-oxygenate, avoid rough laryngoscopy — can trigger VF in the cold heart). Use warmed humidified oxygen (42-46C). Ventilate to normocapnia — both hyperventilation (respiratory alkalosis shifts the oxyhaemoglobin curve) and hypoventilation (acidosis lowers fibrillation threshold) increase arrhythmia risk.
3. Circulation and access
Palpate pulse for up to 60 seconds (cold bradycardia is slow). If no definite pulse and <30C: start CPR. Check rhythm — cold VF may look fine-coarse. Insert large-bore IV access. Give warmed crystalloid (40-42C) — cold fluid drops core temp ~0.25C per litre at room temperature. Avoid central lines near the heart if possible (mechanical irritation → VF); femoral or humeral IO preferred.
4. Investigations (do NOT delay rewarming)
Core temperature (rectal/oesophageal/bladder — NOT oral/axilla/tympanic in arrest). ECG (look for Osborn waves, prolonged intervals, AF, VF). Glucose (hypothermia causes hyperglycaemia but coexisting hypoglycaemia is easily missed — cold masks the signs). Troponin (myocardial ischaemia common). ABG (interpret uncorrected — cold reduces PaCO2 and PaO2; do NOT warm-correct). Lactate (clearance is a prognostic marker). Potassium, urea, creatinine, INR, lipase, CK. CXR. Consider alcohol/drug levels, TSH, cortisol.
5. Rewarming matched to severity
HT I: passive rewarming (warm room, blankets). HT II: active external (forced warm air / Bair Hugger, warmed IV fluids). HT III-IV: active internal — warmed humidified O2, gastric/bladder lavage, warmed IVF, and EARLY referral for ECMO/cardiopulmonary bypass (the treatment of choice for the arrested or profoundly cold patient). Set rewarm rate 0.5-1C/h for chronic hypothermia.
6. Cardiac arrest — modified ALS and ECMO referral
Continue CPR. Withhold adrenaline and antiarrhythmics if core <30C (ineffective, accumulates). Give adrenaline every other cycle (alternate cycles) at 30-35C; standard dosing >35C. Defibrillate VF once (max 3 shocks) if <30C; if no response, continue CPR and rewarm before repeating. Call the ECMO/ECPR centre EARLY — the decision to cannulate is time-critical. Rewarm to at least 32C before ceasing resuscitation. "Not dead until warm and dead."
7. Search for and treat the precipitant
Hypothermia is often the visible end of something else: sepsis, hypothyroidism/myxoedema coma, hypoglycaemia, alcohol/sedative/opioid intoxication, adrenal insufficiency, stroke, trauma (especially head and spinal), exhaustion, immersion. Treat each in parallel — rewarming alone will not fix myxoedema coma or septic shock.
Rewarming techniques compared
The choice of rewarming method is dictated by Swiss stage and haemodynamic stability, not by the thermometer alone. A haemodynamically stable HT III patient may be managed with active internal non-extracorporeal techniques; an unstable HT III or any HT IV-V needs extracorporeal support.[6]
Passive external
HT I 35-32C
- Mechanism: endogenous heat production (shivering, metabolism) rewarms the patient. The clinician only stops further heat LOSS.
- Method: remove wet clothing, dry the patient, insulate with blankets/reflective foil, warm room (21-24C), warm oral fluids if alert.
- Rate: ~0.5-2C/h (shivering generates ~5x basal heat).
- Requirement: the patient MUST have intact shivering and metabolism (sepsis, myxoedema, elderly, exhausted cannot passive-rewarm).
- Failure if no rise in 2-4h → escalate to active external.
Active external
HT II 32-28C
- Mechanism: exogenous heat applied to the skin surface.
- Method: forced warm air blanket (Bair Hugger, 43C), radiant heat, warming mattress, warmed IV fluids (38-42C).
- Rate: 1-2C/h.
- Caution in severe hypothermia (<28C): core afterdrop — peripheral vasodilation returns cold, acidotic, potassium-laden blood to the heart → VF ("rewarming shock"). Therefore active external is usually NOT used alone below 28C.
- Apply to trunk FIRST (not extremities) to limit afterdrop.
Active internal (non-extracorporeal)
HT III 28-24C
- Mechanism: heat delivered to body cavities and core fluids.
- Methods: warmed humidified oxygen via ETT (40-45C, 0.5-1C/h), warmed IV fluids 40-42C, gastric lavage (3-way NG, 250 mL aliquots of 42C saline), bladder lavage, rectal/colonic lavage, peritoneal lavage (dialysate 40-45C).
- Combined rate: 1-2C/h.
- Body-cavity lavage has largely been superseded by extracorporeal where available — lavage is slow and labour-intensive. It remains a bridge when ECMO is delayed or unavailable.
- Intrathoracic cavity lavage via chest tubes (warmed saline 40C, closed circuit) is a more potent bridge to ECMO.
Active internal (extracorporeal)
HT IV-V — ECMO / bypass
- Mechanism: blood is withdrawn, warmed in an external heat exchanger, oxygenated (if veno-arterial), and returned.
- VA-ECMO: preferred — provides both rewarming (rate up to 4-8C/h) AND circulatory support. Indicated for HT IV-V, cardiac arrest, or haemodynamic instability.
- Cardiopulmonary bypass (CPB): full circulatory support and rapid rewarm; requires heparinisation and a perfusion team; typically used in arrested patients in cardiac centres.
- Rate: 4-8C/h — the fastest available.
- Survival to discharge in hypothermic arrest with ECLS is 40-60% (HOPE-stratified) — far better than conventional CPR alone. ECLS is the standard of care for HT V.
ECG changes by temperature band
The ECG is a continuous thermometer. Each temperature band has a characteristic electrical signature, and the progression tracks the falling core temperature almost as reliably as a probe.[7]
35-32C (HT I)
Mild
- Sinus bradycardia with prolonged PR.
- Osborn (J) waves appear — positive hump at the J point (QRS-ST junction), best seen in inferior and left precordial leads.
- Inverted T waves, prolonged QT.
- Shivering artefact on the trace.
32-28C (HT II)
Moderate
- Osborn waves enlarge (amplitude inversely proportional to temperature).
- Atrial fibrillation very common — usually slow AF, benign, and self-reverting on rewarm. Do NOT cardiovert.
- Markedly prolonged PR, QRS, QT.
- Heart rate ~50% of baseline.
- Premature ventricular beats; VF threshold falling.
28-24C (HT III)
Severe
- Bradycardia profound (J wave of Osborn now large).
- High risk of spontaneous VF (any stimulus — movement, CVC, rough CPR — can precipitate it).
- PR and QRS markedly widened; the rhythm may look like a slow idioventricular/escape.
- P waves may disappear (sinoatrial node suppressed).
24-20C (HT IV)
Profound
- Ventricular fibrillation — the dominant lethal rhythm. May be fine or coarse and resistant to defibrillation until warmer.
- Asystole and PEA increasingly common as temperature falls further.
- Heart effectively non-reactive to drugs and electricity below ~28-30C.
<20C (HT V)
Irreversible electrical silence
- Asystole predominates.
- Electrical activity of the heart ceases.
- The myocardium is unresponsive to any pharmacological or electrical therapy until rewarmed — hence ECMO/CPB is the only viable resuscitation path.
Arrhythmia management in hypothermia
The cold myocardium is electrically unstable and pharmacologically inert. Standard ALS drugs fail below 30C, and the same energy of defibrillation is far less effective. Management is therefore dominated by rewarming first, with drugs and shocks as adjuncts.[8]
Atrial fibrillation
32-28C — benign
- Almost universal in moderate hypothermia — slow AF.
- Do NOT cardiovert (electrically or chemically) — will not work and may precipitate VF.
- Do NOT give rate-control drugs (beta-blockers, digoxin, CCBs) — ineffective, accumulate, may cause toxicity. Avoid amiodarone for the AF specifically.
- Rewarm — AF reverts spontaneously in almost all cases as the patient warms above 32C.
- Anticoagulate once warm only if persistent or if high CHA2DS2-VASc.
Ventricular fibrillation
<30C — lethal
- If core <30C: deliver ONE shock (biphasic max, e.g. 200 J). If VF persists, do NOT pile on shocks — continue CPR and rewarm. Repeat shock after the patient reaches 30C.
- Amiodarone 300 mg IV once core >30C (earlier it is ineffective and accumulates). A second 150 mg after 3-5 min if VF persists.
- Lidocaine is INEFFECTIVE in hypothermic VF — do not rely on it.
- Magnesium sulphate 2 g IV may help terminate refractory VF (limited evidence; favoured in wilderness protocols).
- Definitive treatment: VA-ECMO/CPB — rewarm and support the circulation; VF usually terminates as the heart rewarms past 30-32C.
- CRITICAL: continue CPR during rewarm — a cold VF that resists everything will often defibrillate easily at 32C.
Bradycardia
All stages
- Bradycardia in hypothermia is appropriate and protective (low O2 demand). Do NOT treat the heart rate.
- Atropine is INEFFECTIVE in hypothermia-induced bradycardia — the cold sinoatrial node does not respond.
- External pacing rarely captures below 30C; if pacing required, the patient needs ECMO, not a wire.
- The bradycardia resolves as the patient rewarms.
Asystole / PEA (arrest)
<28C
- Modified ALS: continue chest compressions, ventilate with warmed humidified O2, give warmed IV fluids.
- Withhold adrenaline if <30C; give every OTHER cycle (alternate) at 30-35C; standard from 35C.
- Withhold antiarrhythmics if <30C.
- ECMO/CPB referral is the priority — this is an ECPR indication if the arrest is hypothermic and reversible.
- CPR may be prolonged (hours) — consider mechanical CPR (LUCAS/AutoPulse) for sustainability and to allow transport to an ECMO centre.
- Check potassium: K+ >=10 mmol/L or K+ >8 with asphyxia/avalanche is a near-absolute poor-prognosis ceiling — discuss before committing to ECLS.
Prognostic factors and the HOPE score
The maxim "not dead until warm and dead" reflects the remarkable capacity of the hypothermic brain to recover from prolonged arrest (low temperature = low metabolic demand). Several factors separate the salvageable patient from the non-survivable case.[4]
Pasquier 2018 — the HOPE score (PMID 29481910)
Brown, Brugger, Boyd & Paal 2012 — Accidental hypothermia, NEJM (PMID 23150960)
Paal, Pasquier, Darocha et al. 2022 — Accidental Hypothermia: 2021 Update (PMID 35010760)
Pasquier, Strapazzon, Kottmann, Paal et al. 2023 — Avalanche victim management, ICAR MEDCOM (PMID 36709825)
Mazur, Kosinski, Podsiadlo et al. 2019 — ECMO for accidental deep hypothermia (PMID 30854323)
Podsiadlo, Darocha et al. 2021 — Unwitnessed hypothermic arrest and ECLS (PMID 32920881)
Special scenarios
Avalanche burial
Asphyxial + hypothermic
- Asphyxia is the dominant injury; hypothermia is secondary.
- Decision to resuscitate: if airway was OBSTRUCTED on extrication AND burial >35 min → asphyxial death → DO NOT START CPR.
- If airway was PATENT → hypothermic arrest possible → start CPR, transport to ECLS centre, check K+ (K+ >8 mmol/L = non-survivable).
- These patients have the worst prognosis of all hypothermia subtypes — the brain has been anoxic far longer than the heart has been cold.
Near-drowning / submersion
Asphyxial + hypothermic
- Submersion causes asphyxial arrest; the concurrent hypothermia may be protective of the brain (the "diving reflex" + cold water).
- Survival with good neurological outcome is documented after very prolonged submersion in ICE water (especially children).
- Manage as hypothermic arrest: CPR, warmed humidified O2, warmed IV fluids, ECLS referral. Do NOT withhold resuscitation based on time alone.
- Beware associated injuries (cervical spine in divers, trauma), aspiration lung injury (ARDS develops over 4-6h), and electrolyte disturbance (fresh vs salt water).
Urban / indoor hypothermia
Elderly, intoxicated, comorbid
- Often a "tip of the iceberg" presentation — the precipitant (sepsis, stroke, myxoedema coma, overdose, urinary sepsis, hip fracture) is the real emergency.
- Commonly chronic/subacute hypothermia → slow rewarm (0.5C/h) to avoid afterdrop and rewarming shock.
- High mortality driven by comorbidity, not by the hypothermia itself.
- ALWAYS search for and treat the precipitant in parallel with rewarming.
Trauma and hypothermia
Lethal triad
- Hypothermia + acidosis + coagulopathy = the lethal triad of trauma. Each worsens the others; hypothermia disables the coagulation cascade.
- Massive transfusion protocols must deliver WARMED fluids and blood (37-40C); cold blood worsens the triad.
- Trauma patients <35C have markedly higher mortality — rewarming is part of damage control resuscitation.
- Avoid over-resuscitation with cold crystalloid — use warmed blood products and rapid transit to definitive surgical/haemorrhage control.
Myxoedema coma
Endocrine precipitant
- Severe hypothyroidism → hypothermia, bradycardia, hyponatraemia, hypoventilation, coma.
- WILL NOT rewarm with passive/active external alone — the hypometabolic state cannot generate or sustain heat.
- Treat with IV levothyroxine (and hydrocortisone, as coexisting adrenal insufficiency is common) + active external rewarming + supportive care.
- A classic exam trap: "the hypothermic patient who is not rewarming" — think myxoedema coma.
Therapeutic vs accidental
TTM context
- Therapeutic hypothermia (TTM) at 32-36C after cardiac arrest is INTENTIONAL and controlled — managed hypothermia, NOT accidental.
- Osborn waves may appear during induction of TTM; they are expected and benign.
- Do NOT confuse TTM with accidental hypothermia — TTM does not need rewarming protocols; it needs controlled maintenance and slow rewarm (0.25-0.5C/h) to avoid rebound hyperthermia.
- TTM-Trial (Nielsen 2013) showed 33C and 36C targets are equivalent for outcome; the key is TTM itself plus the post-arrest bundle.
Pharmacology in hypothermia — what works, what does not
Adrenaline (epinephrine)
Arrest vasopressor
- Withhold if core <30C — does not work in the cold heart, accumulates to toxic levels, and may precipitate arrhythmia on rewarm.
- Give every OTHER ALS cycle (alternate cycles) at 30-35C.
- Resume standard dosing at >35C (or per local protocol >30C with ECLS running).
Amiodarone
Antiarrhythmic
- First-line for VF/pVT in hypothermia ONCE core >30C — 300 mg IV, then 150 mg if recurrent.
- Ineffective and not recommended <30C. Animal data suggest amiodarone may retain some efficacy in hypothermia (more so than lidocaine).
- Use for VF, NOT for slow hypothermic AF (which needs no drug).
Lidocaine
Antiarrhythmic — AVOID
- Ineffective in hypothermic VF — do NOT rely on it.
- Animal and limited human data show lidocaine fails to terminate hypothermic VF and does not raise the fibrillation threshold.
- If only one antiarrhythmic is to be drawn up, it should be amiodarone, not lidocaine.
Magnesium sulphate
Adjunct
- Limited evidence; wilderness and some European protocols favour 2 g IV for refractory hypothermic VF.
- Mechanism: stabilises the myocardial membrane and may terminate VF resistant to amiodarone and shock.
- Safe; consider when VF persists despite one shock and rewarm above 30C.
Atropine
Bradycardia — AVOID
- Ineffective for hypothermia-induced bradycardia — the cold sinoatrial node does not respond to vagal blockade.
- Bradycardia is appropriate and protective (low O2 demand); treat by rewarming, not by speeding the heart.
Defibrillation
Electric therapy
- <30C: deliver ONE biphasic shock (max energy, e.g. 200 J). If VF persists, do NOT pile on shocks — continue CPR + rewarm.
- >30C: standard defibrillation protocol resumes; VF usually responds readily as the heart warms past 30-32C.
- There is no absolute upper limit to shocks, but repeated ineffective shocks below 30C waste time and damage the myocardium — rewarm first.
Additional high-yield clinical pearls
Common exam pitfalls and high-yield questions
References
- [1]Brown DJA, Brugger H, Boyd J, Paal P. Accidental hypothermia. New England Journal of Medicine, 2012.PMID 23150960
- [2]Paal P, Pasquier M, Darocha T, et al. Accidental Hypothermia: 2021 Update. International journal of environmental research and public health, 2022.PMID 35010760
- [3]Mazur P, Kosinski S, Podsiadlo P, et al. Extracorporeal membrane oxygenation for accidental deep hypothermia-current challenges and future perspectives. Annals of cardiothoracic surgery, 2019.PMID 30854323
- [4]Pasquier M, Hugli O, Paal P, Darocha T, et al. Hypothermia outcome prediction after extracorporeal life support for hypothermic cardiac arrest (HOPE score). Resuscitation, 2018.PMID 29481910
- [5]Pasquier M, Strapazzon G, Kottmann A, Paal P, et al. On-site treatment of avalanche victims: scoping review and 2023 recommendations of the International Commission for Mountain Emergency Medicine (ICAR MEDCOM). Resuscitation, 2023.PMID 36709825
- [6]Podsiadlo P, Darocha T, Svendsen OS, Kosinski S, et al. Outcomes of patients suffering unwitnessed hypothermic cardiac arrest rewarmed with extracorporeal life support. Artificial organs, 2021.PMID 32920881
- [7]Sanchez-Inigo L, et al. The Osborn wave: what have we learned? Herz, 2016.PMID 26272271
- [8]Cheng KA, et al. Effect of Amiodarone and Hypothermia on Arrhythmia Substrates During Resuscitation. Journal of the American Heart Association, 2021.PMID 33938226
- [9]Antzelevitch C, Yan GX, et al. J wave syndromes. Heart rhythm, 2010.PMID 20153265