ICU · Resuscitation
Acute limb compartment syndrome
Also known as Compartment syndrome · Fasciotomy · The 6 Ps · Delta pressure · Volkmann contracture · Two-incision fasciotomy · Crush syndrome · Perfusion pressure
Acute limb compartment syndrome is elevated pressure within a fascial compartment causing ischaemia and necrosis of muscles and nerves. Causes: fracture (1 — tibial shaft, forearm), crush injury, burns (circumferential), prolonged immobility, reperfusion injury (post-vascular repair), tight casts/dressings, bleeding into compartment (anticoagulated). The 6 Ps: Pain (disproportionate, worse on passive stretch — the EARLIEST and most sensitive sign), Pallor, Paraesthesia, Paralysis, Pulselessness (LATE — absence of pulse means it's too late), Poikilothermia. Diagnosis: clinical + compartment pressure measurement (delta pressure = diastolic BP - compartment pressure <30 mmHg = positive). Treatment: EMERGENT FASCIOTOMY (within 6 hours to prevent irreversible necrosis). Untreated → Volkmann ischaemic contracture, amputation, rhabdomyolysis, renal failure.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Pathophysiology — the pressure-perfusion cascade
[8]Pathophysiological sequence — from raised pressure to permanent damage
Trigger: volume increase or decreased compliance
Blood (fracture haematoma, anticoagulant-related bleed), oedema (crush, reperfusion, burn resuscitation), or external compression (cast, tight dressing, circumferential burn eschar) increases compartment content or reduces its ability to expand. The fascial boundary is unyielding — volume increase becomes pressure increase.<Cite id="8" />
Venous outflow obstruction
As tissue pressure rises, thin-walled venules are compressed first (they have the lowest transmural pressure). Venous pressure rises to equal tissue pressure. This increases post-capillary resistance, reducing capillary perfusion gradient even before arterioles are affected. Venous congestion causes further swelling — vicious cycle.<Cite id="8" />
Capillary flow ceases — delta pressure <30 mmHg
Capillary perfusion requires: arterial pressure > venous pressure > tissue pressure. When tissue pressure approaches diastolic BP (delta pressure <30 mmHg), capillary blood flow stops. This occurs at a tissue pressure far BELOW systolic or even mean arterial pressure — which is why pulses are maintained until very late (arterial inflow has the highest pressure).<Cite id="7" /><Cite id="3" />
Tissue ischaemia and necrosis
Muscle tolerates ischaemia for approximately 4 hours before irreversible changes begin; peripheral nerves for ~2-4 hours. After 6-8 hours, muscle necrosis is irreversible. Necrotic muscle releases myoglobin (rhabdomyolysis), potassium, and inflammatory mediators. The limb becomes gangrenous; systemic effects (AKI from myoglobinuria, hyperkalaemia, acidosis) may be fatal.<Cite id="1" />
Fibrosis and contracture — Volkmann ischaemic contracture
Necrotic muscle is phagocytosed and replaced by dense fibrous scar tissue that contracts over weeks-months. In the forearm, this produces the classic Volkmann contracture: elbow flexion, forearm pronation, wrist flexion, and clawing of the fingers (flexor muscle fibrosis). In the leg: equinovarus or claw toes. This is a permanent, devastating disability from delayed or missed compartment syndrome.<Cite id="2" />
Early (0-2h)
Reversible — pain only
- Tissue pressure rising but capillary flow intermittently maintained
- Only symptom: pain out of proportion, pain on passive stretch
- Tissue ischaemic but NOT YET necrotic — fully reversible with fasciotomy
- NO neurological deficit yet
Intermediate (2-6h)
At-risk — paraesthesia, weakness
- Sustained ischaemia — nerve dysfunction begins (paraesthesia, subjective weakness)
- Skin appears tense, shiny, swollen
- Muscle damage is developing but largely reversible if decompressed promptly
- Fasciotomy within this window offers the best outcomes
Late (6-8h+)
Irreversible — necrosis
- Irreversible muscle necrosis and nerve damage
- Paralysis, pulselessness, poikilothermia
- Fasciotomy may still be needed (to prevent further damage, treat rhabdomyolysis) but limb salvage is in doubt
- Risk of amputation, Volkmann contracture, permanent disability
Causes and risk factors
Fractures (MOST COMMON)
~70% of cases
- **Tibial shaft fracture** — #1 cause (especially high-energy, comminuted, open)
- Forearm fracture (especially supracondylar humerus in children)
- Higher risk: younger patients (tighter fascia), high-energy mechanism, open vs closed (open fracture does NOT exclude compartment syndrome)
Crush injury
Direct muscle damage
- Building collapse, entrapment, heavy object impact
- Massive muscle injury + oedema + haemorrhage into compartments
- Associated with rhabdomyolysis, hyperkalaemia, AKI (crush syndrome)
- Risk of reperfusion injury after extrication
Vascular injury / reperfusion
Post-repair swelling
- Reperfusion after vascular repair (femoral/popliteal/brachial artery)
- Ischaemic tissue releases inflammatory mediators → massive oedema on reperfusion
- Prophylactic fasciotomy indicated if ischaemia time >6 hours
Circumferential burns
Eschar constriction
- Full-thickness burn eschar is inelastic — acts like a tourniquet as swelling progresses
- **Escharotomy** (incision through eschar to fat) releases the constriction
- May still develop compartment syndrome requiring formal fasciotomy
Drug / immobility
Prolonged compression
- Unconscious patient lying on limb ("Saturday night palsy" → compartment syndrome)
- Drug overdose, prolonged surgery (lithotomy position), tight cast/splint
- Anticoagulant therapy — bleeding into compartment with minimal trauma
The 6 Ps — in order of appearance
Compartment syndrome clinical signs (click each)
LATE — irreversible damage
Paralysis: loss of motor function in muscles of affected compartment. Pulselessness: ABSENT distal pulses. This is the LATEST sign — by the time pulse is absent, irreversible necrosis has occurred. Do NOT wait for pulselessness to diagnose compartment syndrome.
Diagnosis
Compartment syndrome diagnostic approach
Clinical diagnosis — the foundation
High-risk injury (tibial fracture, forearm fracture, crush, circumferential burn, reperfusion after vascular repair) + pain out of proportion + pain on passive stretch + increasing analgesia requirement = compartment syndrome until proven otherwise. Do NOT wait for all 6 Ps — early diagnosis saves the limb. In the awake cooperative patient, clinical diagnosis alone is sufficient to proceed to fasciotomy.
Compartment pressure measurement (if clinical diagnosis uncertain)
Insert needle manometer (Whitesides technique, Stryker intracompartmental pressure monitor) into each compartment. Normal: 0-10 mmHg. Abnormal: absolute pressure >30 mmHg, OR delta pressure (diastolic BP - compartment pressure) <30 mmHg. **Delta pressure is more accurate** than absolute pressure (accounts for variations in blood pressure — a hypotensive patient develops compartment syndrome at lower tissue pressures). Measure ALL compartments in the limb (leg has 4: anterior, lateral, superficial posterior, deep posterior).<Cite id="7" /><Cite id="3" />
Do NOT delay fasciotomy for tests
If clinical diagnosis is clear, do NOT delay fasciotomy for pressure measurements, blood tests, or imaging. Time is tissue — irreversible necrosis occurs after 6-8 hours of ischaemia. Measure pressure ONLY if clinical diagnosis is uncertain or patient is unconscious/unreliable (intubated, intoxicated, head injury, spinal cord injury).<Cite id="1" />
Near-infrared spectroscopy (NIRS) — emerging tool
Non-invasive tissue oxygenation monitoring (similar to cerebral NIRS). Sustained tissue oxygenation < preserved in a limb at risk may detect compartment syndrome earlier. Not yet standard of care but promising for continuous monitoring in high-risk patients (e.g., tibial fractures, post-vascular repair).<Cite id="2" />
Absolute pressure threshold
Older criteria
- Tissue pressure >30 mmHg absolute = concerning
- Simple but does NOT account for patient blood pressure
- May miss compartment syndrome in hypotensive patients (who develop ischaemia at lower tissue pressures)
- May lead to unnecessary fasciotomy in hypertensive patients
Delta pressure threshold
Current standard
- Delta pressure (DBP - tissue pressure) <30 mmHg = positive
- Accounts for individual blood pressure variations
- Validated by McQueen & Court-Brown in prospective tibial fracture monitoring study
- Higher sensitivity, lower unnecessary fasciotomy rate
- **This is the Fellowship exam answer**
Differential diagnosis — compartment syndrome vs arterial occlusion vs DVT
Compartment syndrome
Elevated tissue pressure
- Onset: hours (typically 6-24h after injury)
- **Pain OUT OF PROPORTION** — the hallmark, earliest sign
- **Pain on passive stretch** of affected compartment muscles
- Pulses: PRESENT until very late (pulselessness = irreversible damage)
- Limb: swollen, tense, shiny skin over affected compartment
- Paraesthesia: in nerve distribution within the compartment
- Cause: fracture (#1), crush, burns, reperfusion, tight dressings
- Pressure measurement: delta pressure <30 mmHg
- Treatment: **EMERGENT FASCIOTOMY**
Acute arterial occlusion
Embolic or thrombotic
- Onset: sudden (minutes to hours) — embolic events are abrupt
- Pain: present but proportionate to ischaemia; painless in severe cases (nerve death)
- **Pulses: ABSENT** (this is the hallmark, not a late sign)
- Limb: pale, cold, mottled, no swelling (limb is shrunken)
- Paraesthesia/paralysis: early and progressive
- Cause: cardiac embolus (AF), in-situ thrombosis (atherosclerosis), graft occlusion
- Pressure measurement: normal compartment pressure
- Treatment: **EMERGENT EMBOLECTOMY / THROMBOLYSIS**
- Rutherford classification guides urgency
Deep vein thrombosis (DVT)
Venous obstruction
- Onset: gradual (days)
- Pain: dull ache, calf tenderness — NOT severe or disproportionate
- **Pulses: PRESENT** (venous obstruction does not affect arterial inflow until very late)
- Limb: swollen, warm, erythematous (phlegmasia alba dolens → phlegmasia cerulea dolens if severe)
- Paraesthesia: absent or minimal
- Cause: venous stasis, hypercoagulability, endothelial injury (Virchow triad)
- Wells score, D-dimer, compression ultrasonography (non-compressible vein)
- Pressure measurement: normal or mildly elevated compartment pressure
- Treatment: **ANTICOAGULATION** (LMWH → DOAC/warfarin); phlegmasia cerulea dolens → venous thrombectomy/thrombolysis
Management — fasciotomy
Fasciotomy decision and preparation
Recognise and act immediately
Compartment syndrome is a **surgical emergency**. Time is tissue. Once the diagnosis is made (clinically or by delta pressure <30 mmHg), proceed to fasciotomy WITHOUT delay. Do NOT wait for theatre if the limb is threatened — fasciotomy can be performed at the bedside in extremis. Inform theatre, anaesthetist, and orthopaedic/vascular surgeon simultaneously.<Cite id="1" />
Remove constrictive agents
Split/remove ALL dressings, casts, splints to skin. Cut circumferential bandages. If circumferential burn eschar, perform escharotomy. Elevate the limb to heart level (not above — elevation above heart reduces arterial inflow and worsens ischaemia). These manoeuvres alone may reduce pressure and buy time.
Optimise the patient
Ensure adequate analgesia, fluid resuscitation, correction of coagulopathy. Treat hyperkalaemia (calcium gluconate, insulin-dextrose). Prepare for anaesthesia. Check bloods: CK, renal function, potassium, coagulation, FBC, group and save. Monitor for rhabdomyolysis (dark urine, rising CK, falling urine output).
Perform fasciotomy — release ALL compartments
Longitudinal incisions through skin, subcutaneous tissue, and fascia over each affected compartment. Release ALL compartments in the limb (4 in the leg, 3-4 in the forearm). Leave wounds OPEN (vacuum dressing or saline-soaked gauze). Do NOT close primarily — closure re-creates the compartment syndrome.<Cite id="1" /><Cite id="9" />
Two-incision fasciotomy technique (leg)
[9]Fasciotomy technique and aftercare
Perform fasciotomy — release all compartments
Using the 2-incision technique (lateral + posteromedial), release all 4 leg compartments. Make incisions full length of the compartment. Incise skin, subcutaneous tissue, and fascia. Ensure complete release — incomplete fasciotomy is a common cause of treatment failure. Leave wounds OPEN.<Cite id="9" />
Wound management — leave open
Do NOT close primarily. Cover with vacuum-assisted closure (VAC) dressing or saline-soaked gauze. The VAC dressing reduces oedema, promotes granulation, and facilitates delayed closure. Elevate limb to heart level (reduces swelling, but not above heart — would reduce arterial inflow). Re-examine all compartments for viability — dead muscle is debrided.
Delayed closure (5-7 days)
Once swelling resolves (typically 5-7 days), attempt delayed primary closure or skin grafting. If closure tension is too high, split-thickness skin graft is applied. Premature closure risks re-elevation of compartment pressures — re-measure if unsure.
Manage complications
**Rhabdomyolysis**: IV fluids to maintain urine output 1-2 mL/kg/h, check CK, treat hyperkalaemia, alkalinise urine if severe (sodium bicarbonate). **Infection**: prophylactic antibiotics, wound surveillance. **Renal failure**: from myoglobinuria — may need RRT. **Nerve damage**: may be permanent (especially if delayed fasciotomy). **Amputation**: if irreversible necrosis (muscle non-viable at fasciotomy — dead, dusky, non-contractile muscle).<Cite id="1" />
Leg (4 compartments)
Most common site
- Compartments: anterior, lateral, superficial posterior, deep posterior
- **2-incision technique** (Mubarak): lateral + posteromedial
- Tibial shaft fracture = #1 cause
- Nerves at risk: superficial peroneal (lateral incision), saphenous (medial), posterior tibial (deep posterior)
- Incomplete release of the deep posterior compartment is the most common technical error
Forearm (3-4 compartments)
#2 site (children)
- Compartments: superficial flexor (flexor carpi radialis/palmaris/flexor digitorum superficialis), deep flexor (flexor digitorum profundus, flexor pollicis longus, pronator quadratus), mobile wad (brachioradialis, ECRL/ECRB), extensor (dorsal)
- Supracondylar humerus fracture in children = classic cause
- Volkmann contracture is the feared complication — claw hand
- Henry volar approach (curvilinear incision) releases flexor compartments; dorsal incision for extensor
- Carpal tunnel release may be needed if median nerve compromised
Thigh (3 compartments)
Less common
- Compartments: anterior (quadriceps, sartorius), posterior (hamstrings), medial (adductors)
- Cause: femur fracture, quadriceps haematoma (anticoagulants), trauma
- Large compartment volume — typically requires significant injury
- Lateral incision releases anterior + posterior; separate medial incision for adductor compartment
Foot (9 compartments)
Rare, difficult
- Calcaneal fracture, crush injury to foot
- Multiple small compartments — technically challenging
- Pain on passive toe extension — key clinical sign
- Two dorsal incisions + one medial incision to release all compartments
Key evidence and landmark studies
McQueen & Court-Brown 1996 — Delta pressure threshold (PMID 8898137)
McQueen et al 2013 — Sensitivity and specificity of pressure monitoring (PMID 23595064)
McQueen et al 2015 — Predictors of compartment syndrome after tibial fracture (PMID 25882967)
Whitesides et al 1975 — Tissue pressure and fasciotomy threshold (PMID 1192674)
Mubarak & Owen 1977 — Double-incision fasciotomy technique (PMID 15455478)
von Keudell et al 2015 — Lancet review (PMID 33529977)
Complications
Local (limb)
From the syndrome itself or from fasciotomy
- **Volkmann ischaemic contracture** — fibrosis and contracture of necrotic muscle; forearm: claw hand; leg: equinovarus/claw toes
- **Amputation** — if muscle is non-viable (dead, dusky, non-contractile at fasciotomy) or infection/gangrene supervenes
- **Nerve damage** — permanent paraesthesia, motor deficit (especially if delayed fasciotomy)
- **Infection** — wound infection, osteomyelitis (if fracture communicated)
- **Chronic pain / CRPS** — complex regional pain syndrome after severe limb injury
- **Cosmetic deformity** — large fasciotomy scars, skin grafts
Systemic
From rhabdomyolysis / reperfusion
- **Rhabdomyolysis** — myoglobinuria (dark/tea-coloured urine), CK often >10,000, myoglobin casts
- **Acute kidney injury** — myoglobin-induced ATN (pigmented casts, positive blood on dipstick but no RBCs on microscopy); may require RRT
- **Hyperkalaemia** — release of intracellular potassium from necrotic muscle; can cause fatal arrhythmia
- **Metabolic acidosis** — release of organic acids and phosphate from necrotic muscle
- **Reperfusion syndrome** — after fasciotomy or vascular repair, release of potassium, myoglobin, acid, and inflammatory mediators into the systemic circulation; monitor closely
- **Crush syndrome** — the systemic manifestation of massive rhabdomyolysis (seen with building collapse, prolonged entrapment)
From delayed closure
After fasciotomy
- **Re-elevation of compartment pressure** — if closed too early before swelling resolves
- **Skin graft failure** — if the wound bed is poor or infected
- **Tethering of tendons/muscles** — if skin graft adheres to underlying structures, limiting gliding
Management of rhabdomyolysis after compartment syndrome
Recognise rhabdomyolysis
Dark/tea-coloured urine, rising CK (often >5,000-10,000 U/L), myoglobinuria (urine dipstick positive for blood but NO red cells on microscopy — myoglobin cross-reacts with the blood reagent), rising potassium, falling calcium, metabolic acidosis, rising creatinine.
Aggressive IV fluid resuscitation
Goal: urine output 1-2 mL/kg/h (HIGHER than usual — to flush myoglobin through the tubules). Use isotonic crystalloid (Hartmann preferred — avoids hyperchloraemic acidosis). Monitor urine output hourly. The volume needed is often large (up to 6-12 L in 24h in severe crush syndrome).
Treat hyperkalaemia
Calcium gluconate (stabilise myocardium), insulin-dextrose (shift K+ into cells), salbutamol, sodium bicarbonate (especially if acidotic). Treat BEFORE it causes arrhythmia. Continuous ECG monitoring.
Consider urine alkalinisation
Sodium bicarbonate (150 mmol in 1L 5% dextrose) to raise urine pH >6.5 — makes myoglobin more soluble, reduces tubular precipitation. Controversial — some evidence of benefit in severe cases but not definitive. Avoid if causes hypernatraemia or hypokalaemia.
Renal replacement therapy if needed
If AKI develops despite fluids (oliguria, rising creatinine, refractory hyperkalaemia/acidosis), initiate RRT. Continuous renal replacement therapy (CRRT) preferred in haemodynamically unstable ICU patients.
Special scenarios
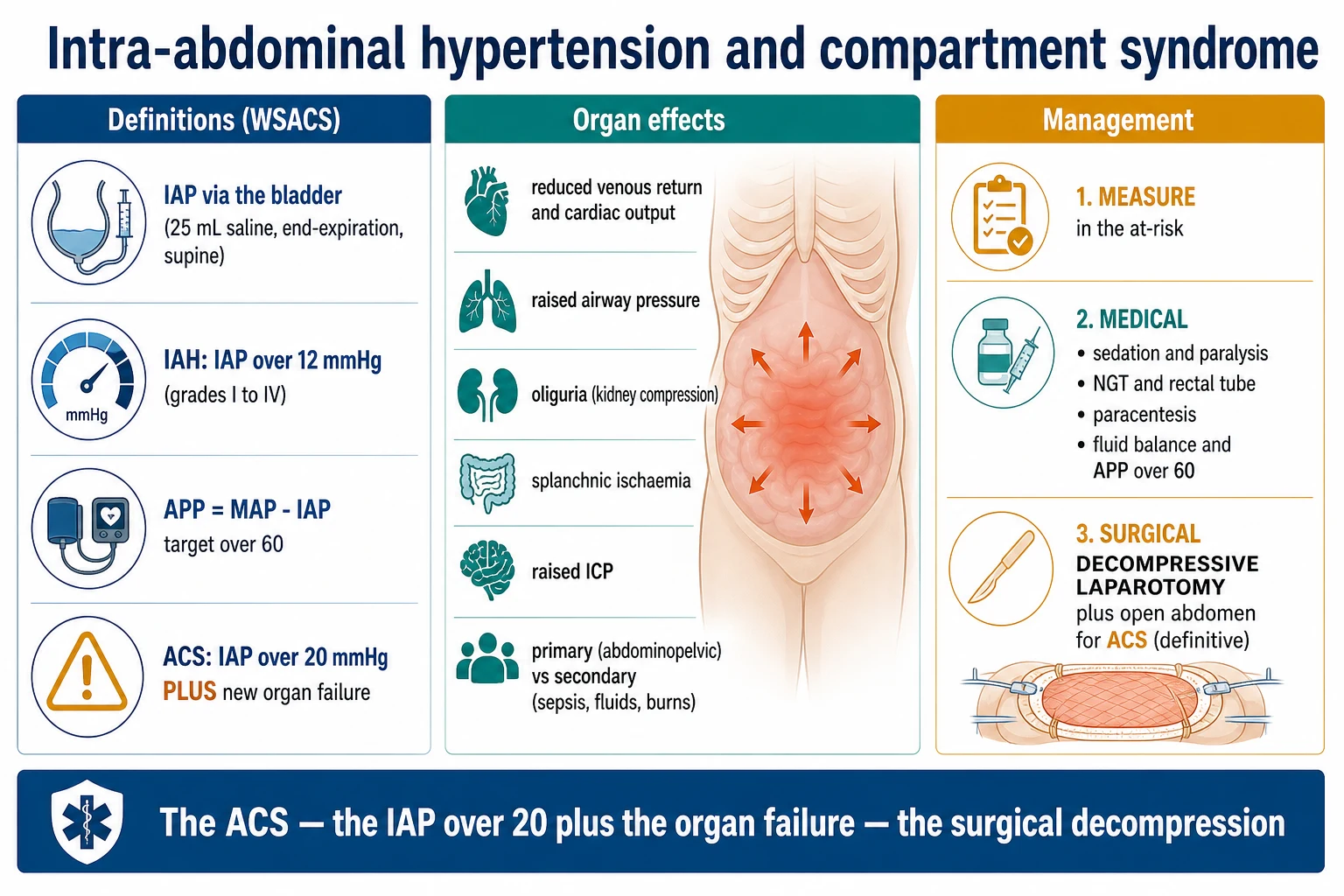
Abdominal compartment syndrome
Intra-abdominal hypertension
- Intra-abdominal pressure (IAP) >20 mmHg with new organ dysfunction (kidney: oliguria; lung: high ventilatory pressures; heart: reduced cardiac output; brain: raised ICP)
- Causes: massive fluid resuscitation, trauma, pancreatitis, burns, post-laparotomy
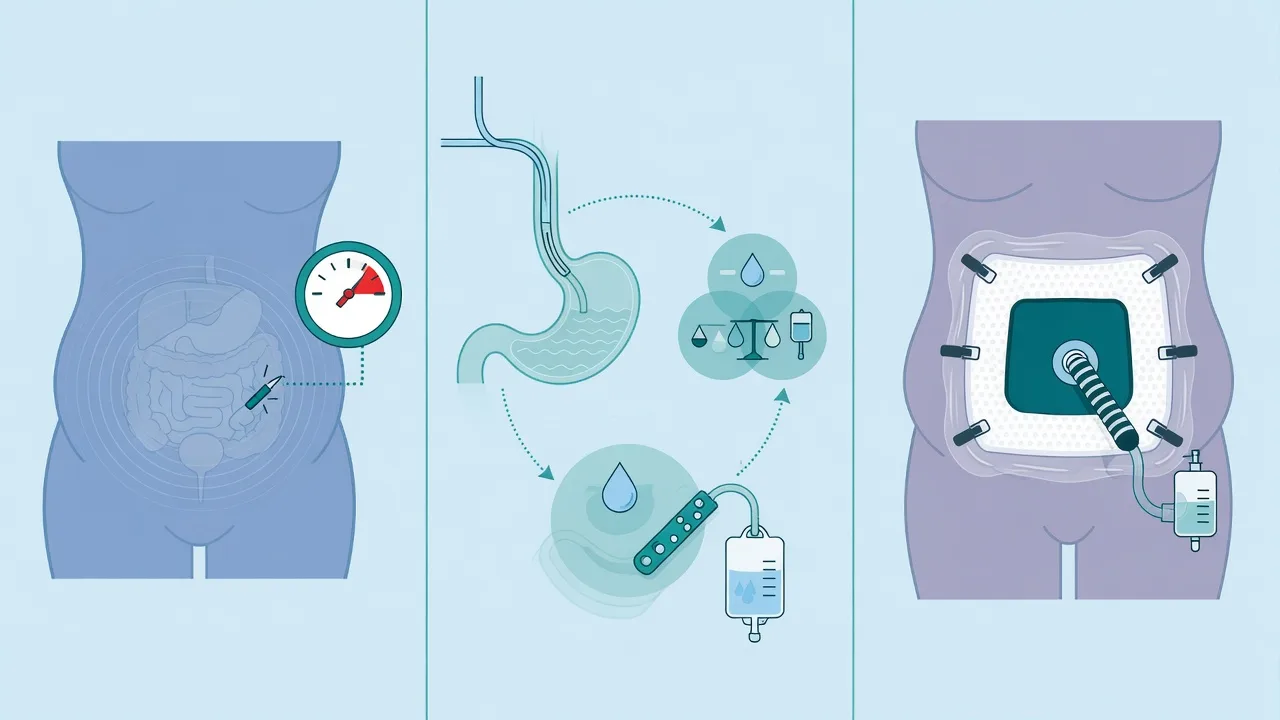
- Measured via bladder pressure (Foley catheter transduction)
- Treatment: decompressive laparotomy (open abdomen), fluid balance optimisation, percutaneous drainage
- **A limb compartment syndrome patient receiving massive fluids for rhabdomyolysis can develop abdominal compartment syndrome — monitor bladder pressure**
Chronic exertional compartment syndrome (CECS)
Recurrent exercise-induced
- Recurrent exercise-induced limb pain (usually leg, in athletes/runners)
- Pressure rises during exercise, resolves with rest
- Diagnosis: pressure measurement before and after exercise (peak post-exercise pressure >30 mmHg)
- Treatment: activity modification, gait retraining; elective fasciotomy if refractory
- NOT an emergency — but important differential for recurrent exercise-induced leg pain
Compartment syndrome in children
Special considerations
- Supracondylar humerus fracture is the classic cause (forearm compartment syndrome → Volkmann contracture)
- Children may not articulate pain well — rely on anxiety, increasing analgesia need, and "the 3 As" (Anxiety, Agitation, Analgesia increasing)
- Pain on passive finger extension is the key sign in forearm compartment syndrome
- Lower threshold for pressure monitoring if the child is unable to cooperate with serial exams
Reperfusion / post-vascular repair
Prophylactic fasciotomy
- Reperfusion after prolonged ischaemia causes massive oedema
- Prophylactic fasciotomy at the time of vascular repair if: ischaemia time >6h, combined arterial + venous injury, significant soft tissue injury, prolonged hypotension
- Do NOT wait for compartment syndrome to develop in these high-risk patients — prophylactic fasciotomy prevents it
- Monitor for reperfusion syndrome (hyperkalaemia, acidosis, myoglobinuria) after reperfusion
Unconscious / intubated patient
Cannot assess clinically
- Cannot report pain — the most sensitive clinical sign is LOST
- Rely on: compartment pressure monitoring (delta pressure <30 mmHg), NIRS, serial clinical exams (limb firmness, capillary refill), high index of suspicion
- Common in ICU: post-cardiac arrest, trauma with TBI, overdose, post-prolonged surgery
- **Have a LOW threshold for pressure monitoring or prophylactic fasciotomy in the unconscious patient with a high-risk limb injury**
SAQ — Acute limb compartment syndrome: diagnosis and the threshold for fasciotomy
10 minutes · 10 marks
A 25-year-old man is admitted to ICU after a high-energy tibial fracture with a below-knee cast. He is now complaining of severe, increasing pain in his leg, requiring escalating morphine. The leg feels tense. Pulses are present. The foundation doctor asks if this is compartment syndrome.
SAQ — Abdominal compartment syndrome in the ICU
10 minutes · 10 marks
A 60-year-old woman is admitted to ICU after emergency laparotomy for a ruptured abdominal aortic aneurysm. She has received 8 L of crystalloid and 6 units of blood. Her ventilator peak airway pressures have risen to 45 cmH2O, her urine output is 10 mL/h, and her bladder pressure is 32 mmHg.
Clinical pearls
Red flags
References
- [1]von Keudell AG, Weaver MJ, Appleton PT, et al. Diagnosis and treatment of acute extremity compartment syndrome. Lancet (London, England), 2015.PMID 26460664
- [2]Schmidt AH Acute compartment syndrome. Injury, 2017.PMID 28449851
- [3]McQueen MM, Court-Brown CM. Compartment monitoring in tibial fractures. The pressure threshold for decompression. Journal of Bone and Joint Surgery (British), 1996.PMID 8898137
- [4]McQueen MM, Duckworth AD, Aitken SA, Court-Brown CM. The estimated sensitivity and specificity of compartment pressure monitoring for acute compartment syndrome. Journal of Bone and Joint Surgery (American), 2013.PMID 23595064
- [5]McQueen MM, Duckworth AD, Aitken SA, Sharma RA, Court-Brown CM. Predictors of compartment syndrome after tibial fracture. Journal of Orthopaedic Trauma, 2015.PMID 25882967
- [6]McQueen MM, Christie J, Court-Brown CM. Acute compartment syndrome in tibial diaphyseal fractures. Journal of Bone and Joint Surgery (British), 1996.PMID 8898136
- [7]Whitesides TE, Haney TC, Morimoto K, Harada H. Tissue pressure measurements as a determinant for the need of fasciotomy. Clinical Orthopaedics and Related Research, 1975.PMID 1192674
- [8]Owen CA, Mubarak SJ, Hargens AR, et al. Intramuscular pressures with limb compression. Clarification of the pathogenesis of the drug-induced muscle-compartment syndrome. New England Journal of Medicine, 1979.PMID 431646
- [9]Mubarak SJ, Owen CA. Double-incision fasciotomy of the leg for decompression in compartment syndromes. Journal of Bone and Joint Surgery (American), 1977.PMID 15455478