ICU · Oncology & immunocompromised
The Oncology and Immunocompromised Patient in the ICU
Also known as Immunocompromised host · Neutropenic sepsis · Tumour lysis syndrome · Cancer in the ICU · Opportunistic infection · GvHD
The immunocompromised and the oncology patient in the ICU demands a broad, the early, and the aggressive approach — the febrile neutropenia (the anti-pseudomonal beta-lactam within the hour), the opportunistic infections (the CMV, the PCP, the fungal), the tumour lysis syndrome (the hydration, the rasburicase), and the immune-related toxicity (the GvHD, the ICI toxicity). This topic builds the examiner's framework on each.
On this page & tools
Your progress
Saved locally on this device.
5 MCQs with explanations
Target exams


Overview & definition
The immunocompromised patient in the ICU — whether from the chemotherapy (the neutropenia), the transplantation (the solid organ, the haematopoietic stem cell), the immunosuppressive medication (the steroids, the biologics), or the HIV (the CD4 below 200) — has the BROADENED differential (the opportunistic organisms) and the BLUNTED presentation (the absent fever, the atypical signs). The early, the broad-spectrum, the aggressive management is the principle.[1][1]
The febrile neutropenia
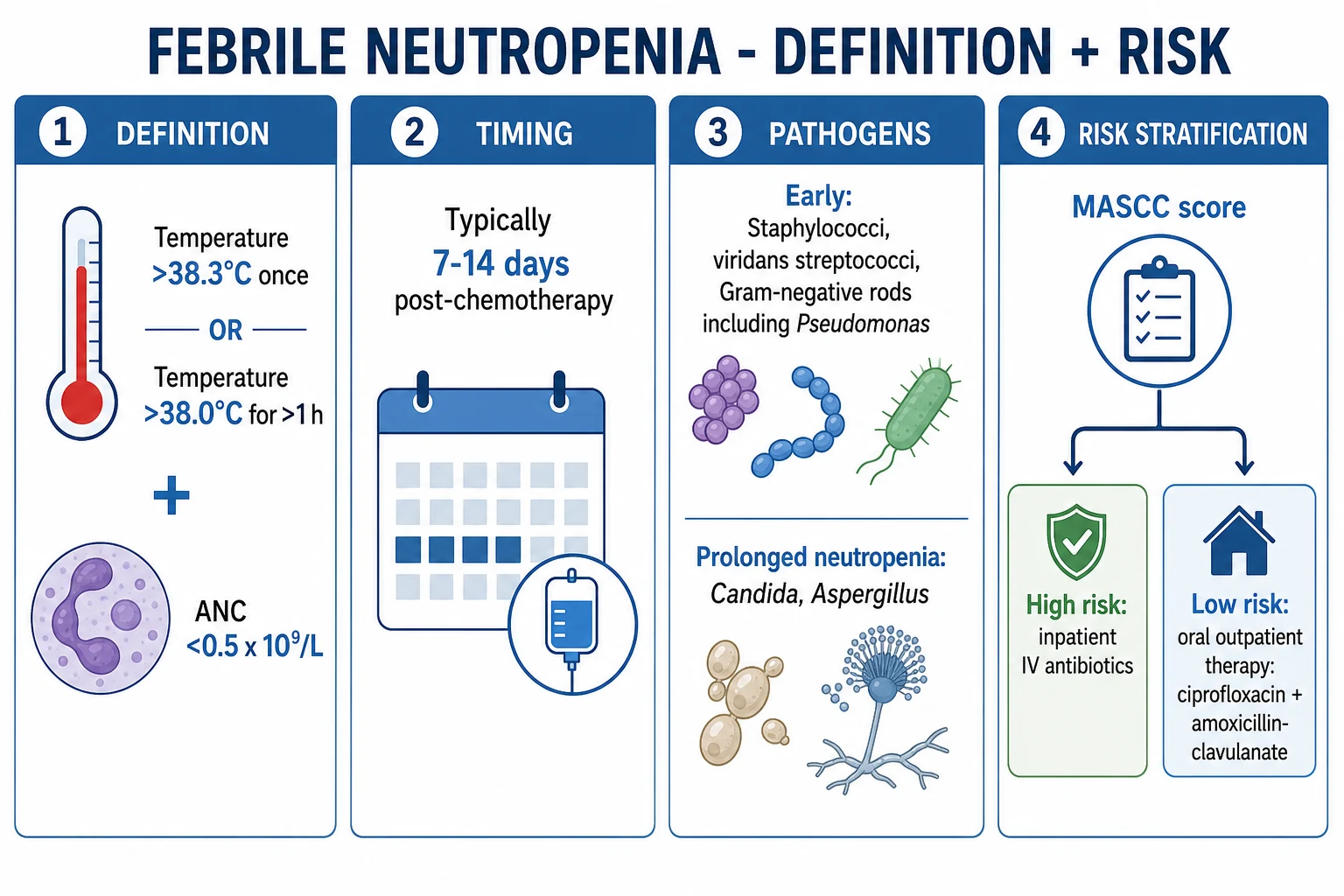
The febrile neutropenia (the ANC below 0.5 x 10^9/L with the fever above 38.3 or the two readings above 38.0) is the MEDICAL EMERGENCY — the empirical antibiotic within the hour (the neutrophil deficiency allows the unchecked bacterial growth).[1]
The empirical antibiotic. The anti-pseudomonal beta-lactam (the piperacillin-tazobactam, the ceftazidime, the cefepime, or the meropenem) as the monotherapy for the stable. The vancomycin added for the line infection, the MRSA risk, the severe mucositis, or the haemodynamic instability. The aminoglycoside added for the septic shock.[1][1]
The antifungal cover. For the persistent fever beyond 4 to 7 days despite the broad-spectrum — the liposomal amphotericin, the caspofungin, or the voriconazole. The galactomannan and the beta-D-glucan screen for the invasive aspergillosis and the candidiasis.[1]
The source search. The line (the CRBSI), the chest (the pneumonia — including the fungal, the PCP), the perianal (the neutropenic enterocolitis — the typhlitis), the abdomen (the neutropenic colitis, the GvHD), the skin (the cellulitis, the zoster), the CNS (the meningitis).[1][1]
The opportunistic infections
The immunocompromised host is susceptible to the organisms that the immunocompetent host resists:[1]
-
The PCP (the Pneumocystis jirovecii pneumonia) — the HIV (the CD4 below 200) or the steroid, the transplant, the chemotherapy. The presentation: the progressive dyspnoea, the dry cough, the hypoxia (often disproportionate to the chest X-ray), the elevated LDH. The CT: the ground-glass opacity. The diagnosis: the induced sputum or the BAL (the stain). The treatment: the high-dose co-trimoxazole (the TMP-SMX 15 to 20 mg/kg/day TMP in divided doses), the steroids if the severe (the PaO2 below 70 — the prevention of the early deterioration from the organism death and the inflammatory response).[1]
-
The CMV — the transplant, the chemotherapy. The CMV syndrome (the fever, the marrow suppression, the hepatitis) or the tissue-invasive (the pneumonitis, the colitis, the retinitis). The diagnosis: the PCR (the quantitative), the tissue biopsy (the inclusion bodies). The treatment: the ganciclovir or the foscarnet.[1]
-
The invasive fungal infection — the aspergillosis (the neutropenia, the transplant — the angioinvasion, the cavitation, the halo sign on the CT; the voriconazole or the isavuconazole), the mucormycosis (the diabetic, the iron overload — the rhinocerebral, the pulmonary; the liposomal amphotericin, the surgery), the candidiasis (the candidoaemia — the echinocandin: the caspofungin or the micafungin; the removal of the lines).[1][1]
The tumour lysis syndrome
The tumour lysis syndrome (the TLS) — the metabolic emergency from the rapid tumour-cell lysis (the chemotherapy initiation, the spontaneous, the steroid). The released intracellular contents cause the hyperkalaemia, the hyperphosphataemia, the hypocalcaemia, and the hyperuricaemia — and the acute kidney injury from the uric acid and the calcium phosphate crystallisation.[1]
The prevention. The hydration (the isotonic saline at 3 L/m2/day — BEFORE the chemotherapy), the allopurinol (for the low-to-moderate risk — the xanthine oxidase inhibition), and the rasburicase (for the high risk — the direct uric acid degradation; the urate oxidase — the rapid, the effective, the contraindicated in the G6PD deficiency).[1]
The management of the established TLS. The aggressive hydration, the rasburicase, the management of the hyperkalaemia (the insulin-dextrose, the calcium for the ECG changes), the renal replacement therapy for the refractory hyperkalaemia, the AKI, or the volume overload.[1][1]
The immune-related adverse events
The graft-versus-host disease (the GvHD) — the donor T-cells attacking the host, post-the HSCT (the acute: the skin rash, the diarrhoea, the cholestatic hepatitis; the chronic: the sclerotic skin, the sicca, the fasciitis). The treatment: the high-dose steroids, the calcineurin inhibitor, the ruxolitinib for the steroid-refractory.[1]
The immune checkpoint inhibitor (the ICI) toxicity — the increasingly common immune-related adverse events from the modern cancer immunotherapy (the CTLA-4, the PD-1/PD-L1 inhibitors). The pneumonitis, the colitis, the hepatitis, the endocrinopathy (the thyroid, the adrenal, the pituitary), and the myocarditis. The management: the STOP the ICI, the high-dose steroids, the infliximab for the severe colitis, the mycophenolate for the severe hepatitis.[1][1]
Management: the integrated approach
- The febrile neutropenia — the anti-pseudomonal beta-lactam within the hour; the vancomycin for the line/MRSA; the antifungal for the persistent fever.[1]
- The opportunistic — the PCP (the co-trimoxazole + the steroid for the severe), the CMV (the ganciclovir), the fungal (the voriconazole or the echinocandin).[1]
- The TLS — the hydration + the rasburicase (prevention); the RRT for the established.[1]
- The immune-related — the GvHD (the steroids), the ICI toxicity (the stop + the steroids).[1][1]
Monitoring
- The temperature, the white count, the CRP — for the infection surveillance.
- The potassium, the phosphate, the calcium, the uric acid, the creatinine — for the TLS.
- The galactomannan, the beta-D-glucan, the CMV PCR — for the opportunistic.
- The chest CT — for the fungal, the PCP. [1]
Prognosis
The mortality of the immunocompromised ICU patient is 30 to 50 per cent (higher than the general ICU), driven by the underlying malignancy, the neutropenia duration, and the organ failure. The early, the aggressive management (the prompt antibiotic, the source control, the organ support) improves the outcome, and the modern oncology (the targeted, the less toxic) brings more patients to the curative ICU pathway.[1][1]
SAQ — Febrile neutropenia: the hour-one antibiotic emergency
10 minutes · 10 marks
A 35-year-old woman with acute myeloid leukaemia, day 12 post-chemotherapy, presents to ED with fever (39.2°C) and rigors. Her full blood count shows ANC 0.2 ×10^9/L, platelets 18 ×10^9/L. Her only source is a peripherally-inserted central line. Outline your immediate management.
SAQ — Tumour lysis syndrome
10 minutes · 10 marks
A 22-year-old man with newly diagnosed Burkitt`s lymphoma and a large abdominal mass begins chemotherapy. Twelve hours later, he develops oliguria and cardiac ectopics. Bloods: K+ 7.1 mmol/L, phosphate 3.2 mmol/L, urate 0.85 mmol/L, calcium 1.7 mmol/L, creatinine 240 µmol/L.
Red flags
The immunocompromised host spectrum — classify the defect first
The single highest-yield cognitive manoeuvre in any immunocompromised ICU admission is to classify the dominant immune defect before choosing empiric therapy. The defect predicts the pathogen, the pathogen predicts the drug, and the drug given inside the first hour predicts survival. There are four canonical defects, often overlapping in the same patient (e.g. a post-allogeneic-HSCT patient on day 12 has neutropenia + mucositis + a T-cell defect from the conditioning + iatrogenic B-cell aplasia). The integrated risk is the 'net state of immunosuppression' (Fishman): the sum of drug intensity, dose, duration, comorbidity, and epidemiological exposure.[1]
The four canonical immune defects — the framework that drives empiric therapy
| Immune defect | Typical setting | Predominant pathogens | Empiric cover implication |
|---|---|---|---|
| Neutropenia (ANC <0.5 x 10^9/L, <0.1 profound) | Cytotoxic chemotherapy (AML/ALL induction, post-autologous HSCT pre-engraftment), ATRA initiation (APL) | Gram-negative bacilli — Pseudomonas aeruginosa (the #1 killer), E. coli, Klebsiella, Stenotrophomonas; gram-positive (Staphylococcus incl. CoNS/MRSA, viridans streptococci from mucositis, enterococci); Candida (mucositis + lines); invasive pulmonary aspergillosis (prolonged neutropenia >10-14 days); Mucorales | Anti-pseudomonal beta-lactam (pip-tazo / cefepime / ceftazidime / meropenem) ± vancomycin (line, MRSA, mucositis, shock); add mould-active coverage (voriconazole/posaconazole/liposomal amphotericin) for persistent fever or CT halo |
| T-cell / cell-mediated defect | Calcineurin inhibitors (tacrolimus/cyclosporine) post-SOT and HSCT, fludarabine, cladribine, alemtuzumab (anti-CD52), anti-thymocyte globulin, prolonged high-dose steroids, HIV with CD4 <200 | Pneumocystis jirovecii (PCP), CMV (and EBV, VZV, HHV-6), Cryptococcus neoformans, Listeria monocytogenes, Nocardia, Legionella, Mycobacterium tuberculosis and NTM, endemic mycoses | Layer co-trimoxazole (PCP/Nocardia), ganciclovir (CMV), and consider anti-mycobacterial cover; Listeria covered by ampicillin ± gentamicin (not by cephalosporins) |
| B-cell / humoral defect | CLL, multiple myeloma, Waldenström's, post-rituximab (B-cell depletion lasts 6-12 months), primary antibody deficiency, protein-losing states | Encapsulated bacteria — Streptococcus pneumoniae, Haemophilus influenzae type b, Neisseria meningitidis; Moraxella, Campylobacter; enteroviruses (chronic); parvovirus B19 | Ceftriaxone ± vancomycin for meningitis; add macrolide/fluoroquinolone; immunoglobulin replacement if hypogammaglobulinaemic |
| Splenectomy / functional hyposplenism (the "overwhelming post-splenectomy infection" — OPSI) | Surgical splenectomy, sickle cell disease (autoinfarction), coeliac disease, post-rituximab, radiation, splenic vein thrombosis | Encapsulated organisms — pneumococcus (#1), meningococcus, H. influenzae b; also Capnocytophaga canimorsus (dog bites), Babesia, malaria (severe) — characteristically pneumococcaemia with Waterhouse-Friderichsen (adrenal haemorrhage) and DIC, mortality 50-70% within 24 h | Ceftriaxone ± vancomycin (meningitis cover) at first fever — do NOT wait for cultures; add doxycycline if Capnocytophaga suspected (dog bite); atovaquone/atovaquone-proguanil for Babesia/malaria |
The 'POST-SPLENECTOMY / OPSI' organisms — CHEPS
The transplant timeline — when each pathogen peaks
In solid organ transplant (SOT) and haematopoietic stem cell transplant (HSCT) recipients the dominant defect, and therefore the dominant pathogen, shifts in a predictable pattern across the post-transplant course. Mapping the patient onto the timeline is the fastest way to generate a focused differential.[1][16]
The transplant timeline — Fishman's 'net state of immunosuppression'
| Period | Dominant defect | Characteristic pathogens |
|---|---|---|
| Month 1 (pre-engraftment, HSCT) / early (SOT) | Neutropenia + mucositis + central lines + surgical wounds | Hospital-acquired: gram-negative bacilli (incl. Pseudomonas), staphylococci (CoNS, S. aureus), Candida (lines), early invasive aspergillosis, HSV reactivation from mucositis; Clostridioides difficile |
| Months 1-6 (post-engraftment, HSCT) / early cellular (SOT) | Cellular immunodeficiency peak (calcineurin inhibitors, T-cell depletion) | PCP (if no co-trimoxazole prophylaxis), CMV (the most important), invasive aspergillosis, Nocardia, Cryptococcus, Listeria, EBV/PTLD, adenovirus, HHV-6, community respiratory viruses (RSV, influenza, parainfluenza, metapneumovirus) |
| Beyond 6 months | Partial immune reconstitution; risk concentrated in those with chronic GVHD or chronic rejection needing intensified immunosuppression | Community-acquired (encapsulated bacteria — S. pneumoniae, H. influenzae) + recurrent opportunists (Cryptococcus, late CMV, P. jirovecii, NTM); varicella-zoster reactivation |
Tumour lysis syndrome — risk stratification, rasburicase, and dialysis
The tumour lysis syndrome (TLS) is an oncologic emergency from massive, rapid release of intracellular contents when tumour cells lyse — either spontaneously (high-grade lymphomas, Burkitt, ALL with high white count) or, more dangerously, after the first cytotoxic or steroid exposure. The metabolic signature — hyperkalaemia, hyperphosphataemia, hypocalcaemia (driven by the phosphate), hyperuricaemia, and acute kidney injury — develops over hours to days. The kidney is the victim on two fronts: uric acid nephropathy (urate crystals in the distal tubules) and calcium phosphate nephropathy (nephrocalcinosis from the hyperphosphataemia-driven Ca x P product > 55-70).[6][7]
Risk stratification (the Cairo-Bishop framework)
The empiric approach to TLS is risk-stratified. Stratify BEFORE chemotherapy and choose prophylaxis accordingly — getting this right at the bedside prevents the emergency.[7]
TLS risk stratification and prophylaxis (Cairo-Bishop international consensus)
| Risk | Typical diseases | Prophylaxis | Monitoring |
|---|---|---|---|
| High | Burkitt lymphoma / ALL-lymphoma (LDH >2x ULN, high tumour burden); ALL with WBC >100 x 10^9/L or WBC >50 + LDH high; AML with WBC >100; high-grade lymphoma with bulky disease; tumour burden >10 cm; high cell-turnover and chemo-sensitive (small-cell lung cancer with bulky disease, germ cell tumour) | Hydration (isotonic saline 3 L/m2/day, BEFORE and during chemo) + rasburicase (0.15-0.2 mg/kg, repeat to keep uric acid low; or single fixed 3 mg or 6 mg dose in adults). Do NOT use allopurinol alone — it does not degrade existing uric acid. Avoid urinary alkalinisation (raises calcium phosphate precipitation) | q4-6 h electrolytes, uric acid, creatinine, Ca x P product, ECG for hyperkalaemia — for the first 24-72 h |
| Intermediate | AML (most), ALL with WBC 50-100, intermediate-grade lymphoma (LDH elevated but not extreme), CLL on venetoclax (especially with 11q/17p deletion), multiple myeloma with high tumour burden | Hydration + rasburicase (if any feature pushes toward high) OR allopurinol 300 mg/day (start 24 h before chemo) | q6-8 h electrolytes and uric acid |
| Low | Indolent lymphomas, CLL (standard), most solid tumours, AML with WBC <25 and no other risk | Hydration ± allopurinol | q24 h or per clinical course |
Established tumour lysis syndrome — first six hours
- RECOGNISE — confirm the metabolic triad (K+ >6.0, phosphate >1.5 mmol/L or rising, uric acid >475 micromol/L) ± AKI (creatinine rise, oliguria) ± symptomatic hypocalcaemia (perioral tingling, Chvostek/Trousseau, seizures, ECG QT prolongation). The K+ can be the immediate threat
- CARDIAC MONITOR + 12-LEAD ECG — peaked T waves, PR widening, QRS widening — the patient can arrest from hyperkalaemia before the TLS is fully treated
- AGGRESSIVE HYDRATION — isotonic saline 3 L/m2/day (or 200 mL/h boluses reassessed); maintain urine output >100 mL/m2/h. Furosemide ONLY if euvolaemic/overloaded with good output — do not diurese a hypovolaemic TLS patient
- GIVE RASBURICASE (0.15-0.2 mg/kg IV, repeat in 24 h if uric acid still high) — single most effective intervention for the hyperuricaemia. Confirm G6PD status first if feasible but do not delay the first dose if unobtainable and the patient is not in a high-prevalence ancestry group
- TREAT THE HYPERKALAEMIA — calcium gluconate 10% 10 mL IV for ECG changes (stabilises myocardium, NOT for the TLS); insulin-dextrose (10 U actrapid + 25 g dextrose) + salbutamol 10-20 mg nebulised for transcellular shift; bicarbonate only if acidotic
- RENAL REPLACEMENT THERAPY — indicated for: refractory hyperkalaemia, refractory acidosis, refractory volume overload, symptomatic uraemia, Ca x P product > 70 with rising phosphate (calcium phosphate deposition), or oligoanuric AKI. CVVH/CVVHDF preferred in the haemodynamically unstable; the effluent clears uric acid and phosphate effectively
- AVOID THE PITFALLS — do NOT alkalinise the urine (raises calcium phosphate precipitation); do NOT give IV calcium unless the patient is symptomatic or has ECG changes (you will precipitate metastatic calcification by driving the Ca x P product higher); do NOT stop the chemotherapy — TLS means the chemo is working (consult the haematology/oncology team about continuing or modifying)
Graft-versus-host disease — acute, chronic, and steroid-refractory
Graft-versus-host disease (GvHD) is the donor T-cell attack on host tissues after allogeneic HSCT (and rarely after solid organ transplant or transfusion in the severely immunocompromised). It is the leading cause of late non-relapse mortality after allogeneic HSCT and the single biggest driver of the 'net state of immunosuppression' that predisposes to the opportunistic infections discussed above. The two forms are distinguished primarily by timing and clinical pattern, not by mechanism.[9][10]
Acute GvHD — the classic triad
Acute GvHD occurs in the first 100 days (classic) or beyond (late/chronic overlap), grading by the Glucksberg / MAGIC criteria across three target organs: skin (maculopapular rash → bullae/desquamation), gastrointestinal tract (anorexia, nausea, secretory watery diarrhoea up to litres/day, abdominal pain, ileus), and liver (conjugated hyperbilirubinaemia — cholestatic). Grade II-IV acute GvHD affects ~30-50% of allogeneic HSCT recipients and is the major determinant of ICU need (volume depletion from GI loss, sepsis from broken skin/bowel, transaminitis). [1]
Acute GvHD — the Glucksberg organ-staging framework (examiner favourite)
| Stage | Skin (rash %BSA) | Liver (bilirubin micromol/L) | Gut (stool volume/day) | Overall grade (composite) |
|---|---|---|---|---|
| 1 | <25% | 34-50 | 500-1000 mL (or persistent nausea on endoscopy) | Grade I: stage 1-2 in one organ, no dysfunction |
| 2 | 25-50% | 51-100 | 1000-1500 mL | Grade II: stage 1 + one organ stage 1-2, OR stage 2 in any |
| 3 | >50% (erythroderma) | 101-255 | 1500-2000 mL | Grade III: stage 3 in any organ; significant dysfunction |
| 4 | Bullae + desquamation | >255 | >2000 mL or severe pain/ileus/bleeding | Grade IV: stage 4 in any organ; life-threatening |
Chronic GvHD — the sclerotic, sicca, multi-organ syndrome
Chronic GvHD (after day 100, often overlapping with late acute) is a sclerotic, immune-dysregulation syndrome with skin (lichenoid then sclerotic — "hidebound" skin, restriction), sicca (dry eyes, dry mouth — destroys salivary glands), oral ulceration, fasciitis (limitation of range of motion), bronchiolitis obliterans (the lethal pulmonary form — progressive obstructive lung disease), oesophageal web/stricture, vaginal stenosis, and antibody deficiency. It is the leading cause of late non-relapse mortality and drives lifelong immunosuppression and infection risk. [1]
Steroid-refractory GvHD and ruxolitinib
~40-50% of acute GvHD and ~70% of chronic GvHD are steroid-refractory (no improvement after 5-7 days of methylprednisolone 1-2 mg/kg/day), at which point the historic mortality was >70%. The REACH1 (acute, NEJM 2020) and REACH2 (chronic, NEJM 2021) trials established ruxolitinib (a JAK1/2 inhibitor that blocks the donor-T-cell inflammatory signalling) as the standard for steroid-refractory disease, with overall response rates around 55-62% at day 28.[9][10]
Steroid-refractory GvHD — the workup and escalation
- CONFIRM STEROID-REFRACTORINESS — no improvement after 5-7 days of methylprednisolone 1-2 mg/kg/day (or progression on steroids). Re-stage by Glucksberg
- EXCLUDE MIMICS — the diarrhoea might be C. difficile, CMV colitis, or mycophenolate enteritis (not GvHD — biopsy before escalating); the rash might be drug eruption, viral exanthem, or engraftment syndrome; the jaundice might be SOS/VOD, drug hepatotoxicity, or biliary obstruction. Endoscopy/skin/liver biopsy is mandatory before adding immunosuppression
- START RUXOLITINIB (5-10 mg BD, titrate by response and cytopenias) — the JAK1/2 inhibitor with the strongest evidence base (REACH1/REACH2). Cautions: cytopenias (worsen the existing thrombocytopenia/neutropenia), infection risk (reactivation of HBV, CMV, BK; cover with PCP prophylaxis), withdrawal syndrome if stopped abruptly (flare + cytokine rebound — taper over 4-8 weeks)
- EXTRA-CORPOREAL OPTIONS — extracorporeal photopheresis (ECP) for skin and chronic GvHD; mesenchymal stromal cells; anti-TNF (infliximab, etanercept); tocilizumab; methotrexate; MMF; sirolimus. These are second/third-line in most units
- MAINTAIN INFECTION PROPHYLAXESIS — co-trimoxazole (PCP), mould-active azole (Aspergillus — but ruxolitinib interacts with azoles, halve the ruxolitinib dose), aciclovir (HSV/VZV), consider CMV pre-emptive monitoring
Engraftment syndrome — the auto-inflammatory fever around neutrophil recovery
Engraftment syndrome (also called autologous GvHD, cytokine release of engraftment, or peri-engraftment respiratory distress syndrome — PERDS when pulmonary) is a self-limiting inflammatory syndrome at the moment of neutrophil recovery (ANC rising through 0.5 x 10^9/L), driven by the abrupt release of pro-inflammatory cytokines (TNF-alpha, IL-1, IL-6, IFN-gamma) as neutrophils re-enter the circulation and home to damaged tissue. It is seen after autologous HSCT (in ~7-20% of patients, especially after peripheral blood stem cells and growth-factor mobilisation) and, less commonly, after allogeneic HSCT and after induction chemotherapy for AML.[1][1]
The clinical picture is a non-infectious fever around the time of neutrophil recovery, accompanied by: a localised or diffuse erythematous skin rash (often capillary-leak oedema), weight gain and fluid overload, non-cardiogenic pulmonary oedema / ARDS (PERDS — the most dangerous manifestation, presenting as hypoxaemia and bilateral infiltrates at engraftment), hepatic/renal dysfunction, and sometimes encephalopathy. It is a diagnosis of exclusion — neutropenic fever, occult infection (PCP, CMV, fungal), allergic drug reaction, transfusion reaction, and hyperacute GvHD (allogeneic setting) must be ruled out by cultures, CT, and biomarkers first. [1]
[1] [1]Immune checkpoint inhibitor toxicity — the modern organ-by-organ syndrome
Immune checkpoint inhibitors (ICIs — the anti-CTLA-4 ipilimumab; the anti-PD-1 nivolumab, pembrolizumab; the anti-PD-L1 atezolizumab, durvalumab) release the brakes on T-cells to attack the tumour — but also generate a spectrum of immune-related adverse events (irAEs) that can affect any organ, can present weeks to months after the last dose (the half-life of these antibodies is 12-25 days), and are the modern ICU referral in oncology. ICI myocarditis is the highest-mortality form (mortality 25-50% in severe cases).[11][12]
Immune checkpoint inhibitor toxicity — organ-specific recognition and treatment
| Organ / syndrome | Incidence | Presentation | Diagnosis | Management |
|---|---|---|---|---|
| Pneumonitis | 2-5% (10% with combination) | Cough, dyspnoea, hypoxia; CT ground-glass/patchy opacities | CT chest; bronchoscopy to exclude infection; grade by symptoms (G1 asymptomatic radiology → G4 life-threatening) | STOP ICI; G2-G4 = prednisone 1-2 mg/kg/day (methylprednisolone 2-4 mg/kg/day for G3-4), taper over 6 weeks; infliximab/MMF/mycophenolate if refractory |
| Colitis | 5-35% (ipilimumab >> PD-1) | Diarrhoea (often >6/day), abdominal pain, bleeding, perforation | Stool exclude C. difficile, CMV; flexible sigmoidoscopy/colonoscopy biopsy | STOP ICI; loperamide for G1; prednisone 1-2 mg/kg for G2+; infliximab 5 mg/kg or vedolizumab 300 mg for refractory (avoid anti-TNF if perforation risk) |
| Hepatitis | 5-10% | Asymptomatic transaminase rise; jaundice when severe | Exclude viral/drug hepatitis; liver biopsy if severe | STOP ICI; prednisone 0.5-1 mg/kg (start at <5x ULN); methylprednisolone 1-2 mg/kg + mycophenolate 500-1000 mg BD if >8x ULN; avoid infliximab (hepatotoxic) |
| Endocrinopathy | 10-20% (combination) | Thyroid (hyper then hypo); adrenal insufficiency (fatigue, hypotension, hyponatraemia); hypophysitis (headache, visual field defect, panhypopituitarism); T1DM (DKA) | TSH, free T4, morning cortisol, ACTH, FSH/LH/prolactin, pituitary MRI; do not stop ICI for most endocrinopathies | Hormone replacement is the mainstay: levothyroxine; hydrocortisone 100 mg IV stat then 50 mg q6h for adrenal crisis; testosterone/oestrogen; insulin for new T1DM. Steroids for hypophysitis (prednisone 0.5-1 mg/kg) |
| Myocarditis | 0.1-1% (highest with combination) | Chest pain, dyspnoea, arrhythmia, cardiogenic shock, complete heart block, sudden death | Troponin + ECG + echocardiogram + cardiac MRI (the diagnostic test — late gadolinium enhancement + oedema); endomyocardial biopsy if doubt | STOP ICI PERMANENTLY; high-dose methylprednisolone 1 g/day x3-5 then taper; add MMF; supportive — pacemaker for heart block, VA-ECMO/mcn for shock; mortality 25-50% in severe |
| Nephritis | 2-5% | Rising creatinine, oliguria | Urine MCP, renal biopsy (interstitial nephritis); exclude pre/post-renal | STOP ICI; prednisone 0.5-1 mg/kg; dialysis if severe |
ICU outcomes in the cancer patient — improving and no longer a terminal referral
For decades a cancer diagnosis was considered a near-contraindication to ICU admission, and the saying "cancer patients don't survive the ICU" drove late, conservative referrals with predictably poor outcomes. That has changed: modern critical care (lung-protective ventilation, early NIV, prompt source control, rasburicase, ruxolitinib, less toxic cancer therapy) and earlier ICU referral have brought ICU mortality in haematological malignancy down from >80% in the 1990s to ~30-50% today, with hospital mortality for those admitted to ICU within 24 h of organ failure around 35-45%. The single biggest modifiable factor is timing: ICU admission once the patient has three or more organ failures carries mortality >80-90%, while admission for one organ failure carries mortality <25%.[13][14]
ICU mortality in cancer — the changing landscape
| Population / era | ICU mortality | Key modifier |
|---|---|---|
| Haematological malignancy, 1990s | 70-85% | Late referral, no lung-protective ventilation, no rasburicase, no NIV evidence |
| Haematological malignancy, contemporary (2010s-2020s) | 30-50% | Early NIV (Antonelli, Azoulay), prompt rasburicase, ruxolitinib for steroid-refractory GvHD, less toxic regimens, early ICU referral (within 24 h of organ failure) |
| Solid tumour, contemporary | 25-40% | Generally better than haematological; septic shock the leading cause |
| Need for invasive mechanical ventilation | 40-60% | The strongest single marker of poor outcome across the board |
| Three or more organ failures at ICU admission | 80-95% | Drives the case for early referral — once multi-organ failure is established, mortality approaches 100% |
| Allogeneic HSCT recipient in ICU, mechanically ventilated | 60-85% | Highest-risk subgroup; reflects both the underlying malignancy and the cumulative 'net state of immunosuppression' |
| Steroid-refractory acute GvHD requiring ICU (post-ruxolitinib era) | 30-45% (improved from >70%) | REACH1/REACH2 have shifted outcomes meaningfully |
Prognostic markers at ICU admission in the immunocompromised oncology patient
high
The most powerful adverse markers are: (1) three or more organ failures (SOFA >11), (2) need for invasive mechanical ventilation within 24 h, (3) refractory septic shock at admission, (4) allogeneic HSCT with steroid-refractory GvHD, (5) prolonged (>14 day) profound neutropenia, (6) invasive aspergillosis or mucormycosis with dissemination. Favourable markers: single organ failure, early (<24 h) ICU referral, reversible cause (PCP, TLS, drug toxicity), good performance status before the acute illness.
Clinical pearls
Additional red flags
Key trials and evidence
Antonelli 2000 (JAMA) — NIV for acute respiratory failure in solid-organ transplant recipients (PMID 11094492)
Source
Antonelli M, Conti G, Bufi M, et al. Noninvasive ventilation for treatment of acute respiratory failure in patients undergoing solid organ transplantation: a randomized trial. JAMA 2000;283(2):235-241
Design
RCT, 40 immunospromised (SOT) patients with hypoxaemic respiratory failure and pulmonary infiltrates; NIV vs standard oxygen (with intubation if needed)
Key result 1
NIV reduced the intubation rate (20% vs 70%, p=0.001), and reduced serious complications (including septic shock and fatal complications)
Key result 2
NIV reduced ICU mortality (20% vs 50%, p=0.05) and the number of patients with fatal complications
Clinical bottom line
Established NIV as first-line respiratory support in the immunocompromised hypoxaemic patient — 'reach for the BiPAP mask before the laryngoscope'. Subsequent Azoulay-era data extended this to HSCT and haematological malignancy
Herbrecht 2002 (NEJM) — voriconazole vs amphotericin B for invasive aspergillosis (PMID 12167683)
Source
Herbrecht R, Denning DW, Patterson TF, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med 2002;347(6):408-415
Design
Randomised open-label multicentre trial, 277 patients with proven/probable invasive aspergillosis; voriconazole vs amphotericin B deoxycholate
Key result 1
Voriconazole had a higher initial response rate (52.8% vs 31.6%, p<0.001) at 12 weeks
Key result 2
Voriconazole improved survival (70.8% vs 57.9%, p=0.05) at 12 weeks
Clinical bottom line
Established voriconazole as first-line therapy for invasive pulmonary aspergillosis — the foundation of modern mould-active therapy. Isavuconazole is an alternative (better tolerability, covers Mucorales); therapeutic drug monitoring (trough 1-5.5 mg/L) is essential
Zeiser REACH1 (NEJM 2020) — ruxolitinib for steroid-refractory acute GvHD (PMID 32320566)
Source
Zeiser R, von Bubnoff N, Butler J, et al. Ruxolitinib for glucocorticoid-refractory acute graft-versus-host disease. N Engl J Med 2020;382(19):1800-1810
Design
REACH1, single-arm phase 2, 71 patients with steroid-refractory acute GvHD grade II-IV after allogeneic HSCT; ruxolitinib 10 mg BD
Key result 1
Overall response rate at day 28 was 62% (95% CI 49-74); 34% achieved a complete response
Key result 2
Durable response at day 56 was 40%; the response was greatest in lower-grade GvHD and across skin/GI/liver
Clinical bottom line
Established ruxolitinib as the standard for steroid-refractory acute GvHD, transforming a historically near-fatal condition (mortality >70%) into a treatable one (30-45% ICU mortality in the post-ruxolitinib era)
Zeiser REACH2 (NEJM 2021) — ruxolitinib for steroid-refractory chronic GvHD (PMID 34260836)
Source
Zeiser R, Polverelli N, Ram R, et al. Ruxolitinib for glucocorticoid-refractory chronic graft-versus-host disease. N Engl J Med 2021;385(3):228-238
Design
REACH2, randomised phase 3, 329 patients with steroid-refractory chronic GvHD; ruxolitinib vs best available therapy
Key result 1
Overall response rate at week 24 was 49.7% with ruxolitinib vs 25.6% with best available therapy (p<0.001)
Key result 2
Improved failure-free survival and patient-reported symptom scores; main adverse events were thrombocytopenia and anaemia
Clinical bottom line
Established ruxolitinib as the standard for steroid-refractory chronic GvHD — the leading cause of late non-relapse mortality after allogeneic HSCT
Freifeld 2011 (Clin Infect Dis) — IDSA febrile neutropenia guideline (PMID 21205990)
Source
Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: update by the IDSA. Clin Infect Dis 2011;52(4):e56-93
Key principle 1
Empiric high-risk febrile neutropenia (ANC <0.5 expected >7 days): anti-pseudomonal beta-lactam (cefepime, ceftazidime, piperacillin-tazobactam, or carbapenem) within 60 minutes of fever
Key principle 2
Add vancomycin (or linezolid) for suspected line infection, severe mucositis, MRSA risk, or haemodynamic instability; do NOT add routinely
Key principle 3
Persistent fever >4-7 days despite broad-spectrum — add empiric antifungal (liposomal amphotericin B, caspofungin, or mould-active azole); screen with galactomannan and beta-D-glucan
Clinical bottom line
The foundational empiric therapy framework for febrile neutropenia — the door-to-needle antibiotic is the survival-defining intervention
Brahmer 2018 (JCO) — ASCO/SITC immune-related adverse events guideline (PMID 29517954)
Source
Brahmer JR, Lacchetti C, Thompson JA, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO clinical practice guideline. J Clin Oncol 2018;36(17):1714-1768
Key principle 1
STOP the ICI for grade 2+ toxicity; permanently discontinue for severe pneumonitis, myocarditis, or neurological toxicity
Key principle 2
Corticosteroid 1-2 mg/kg/day (methylprednisolone IV equivalent for grade 3-4) is first-line; taper over at least 4-6 weeks to avoid rebound
Key principle 3
Steroid-refractory cases need a second-line immunomodulator (infliximab for colitis, mycophenolate for hepatitis/pneumonitis, vedolizumab for colitis); ICI myocarditis is the highest-mortality irAE
Clinical bottom line
The defining management framework for ICI toxicity in the ICU — the modern cancer immunotherapy emergency
Haanen 2017 (Ann Oncol) — ESMO immunotherapy toxicity guideline (PMID 28881921)
Source
Haanen JBAG, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2017;28(suppl 4):iv119-iv142
Key principle 1
Toxicities can occur weeks to months after the LAST dose (antibody half-life 12-25 days) — ask about ICI history on every cancer admission
Key principle 2
Endocrinopathies (thyroid, adrenal, pituitary, T1DM) are treated primarily with hormone replacement — do NOT stop ICI for most endocrinopathies; steroids reserved for hypophysitis and severe adrenal crisis
Clinical bottom line
The European companion to the ASCO/SITC guideline — together they define the standard of care for irAE recognition and management
Azoulay 2017 (Intensive Care Med) — outcomes in critically ill haematology patients (PMID 27661125)
Source
Azoulay E, Pickkers P, Soares M, et al. Outcomes in critically ill patients with hematological malignancies: a systematic review and meta-analysis. Intensive Care Med 2017;43(8):1109-1122 (and update)
Key result 1
ICU mortality in haematological malignancy has fallen to 30-50% in the contemporary era (from >80% in the 1990s)
Key result 2
The single strongest marker of poor outcome is the need for invasive mechanical ventilation; three or more organ failures at admission carries mortality >80-90%
Clinical bottom line
Cancer is no longer a near-contraindication to ICU care — early referral (within 24 h of organ failure) and a time-limited trial of intensive care are the standard. The prognosis is made on organ failures, not the cancer diagnosis
Cairo-Bishop 2010 (Br J Haematol) — TLS risk stratification and prophylaxis (PMID 20331465)
Source
Cairo MS, Coiffier B, Reiter A, Younes A, on behalf of the TLS Expert Panel. Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases. Br J Haematol 2010;149(4):578-586
Key principle 1
TLS risk is stratified as low / intermediate / high based on disease histology, tumour burden, white cell count, LDH, cell turnover, and chemo-sensitivity
Key principle 2
High-risk: hydration + rasburicase (urate oxidase); intermediate: hydration + rasburicase or allopurinol; low: hydration ± allopurinol
Key principle 3
Rasburicase is contraindicated in G6PD deficiency (haemolysis + methaemoglobinaemia); avoid urinary alkalinisation (raises calcium phosphate precipitation)
Clinical bottom line
The international consensus framework that drives TLS prophylaxis — getting the risk stratification right before chemotherapy prevents the emergency
References
- [1]Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 Update by the Infectious Diseases Society of America Clin Infect Dis, 2011.PMID 21205990
- [2]Herbrecht R, Denning DW, Patterson TF, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med, 2002.PMID 12167683
- [3]Patterson TF, Thompson GR 3rd, Denning DW, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America Clin Infect Dis, 2016.PMID 27365388
- [4]Pappas PG, Kauffman CA, Andes DR, et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America Clin Infect Dis, 2016.PMID 26679628
- [5]Antonelli M, Conti G, Bufi M, et al. Noninvasive positive pressure ventilation as treatment for acute respiratory failure in critically ill patients Crit Care, 2000.PMID 11094492
- [6]Howard SC, Jones DP, Pui CH. The tumor lysis syndrome N Engl J Med, 2011.PMID 21561350
- [7]Cairo MS, Coiffier B, Reiter A, Younes A. Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: an expert TLS panel consensus Br J Haematol, 2010.PMID 20331465
- [8]Pui CH, Relling MV, Lascombes F, et al. Urate oxidase in the prophylaxis or treatment of hyperuricemia: the United States experience Semin Hematol, 2001.PMID 11694947
- [9]Zeiser R, von Bubnoff N, Butler J, et al. (REACH1). Ruxolitinib for Glucocorticoid-Refractory Acute Graft-versus-Host Disease N Engl J Med, 2020.PMID 32320566
- [10]Zeiser R, Polverelli N, Ram R, et al. (REACH2). Ruxolitinib for Glucocorticoid-Refractory Chronic Graft-versus-Host Disease N Engl J Med, 2021.PMID 34260836
- [11]Brahmer JR, Lacchetti C, Thompson JA, et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline Summary J Oncol Pract, 2018.PMID 29517954
- [12]Haanen JBAG, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol, 2017.PMID 28881921
- [13]Azoulay E, Pickkers P, Soares M, et al. Outcomes in adult critically ill cancer patients with and without neutropenia: a systematic review and meta-analysis of the Groupe de Recherche en Réanimation Respiratoire du patient d'Onco-Hématologie (GRRR-OH) Oncotarget, 2017.PMID 27661125
- [14]Nates JL, Pène F, Darmon M. Septic shock in the immunocompromised cancer patient: a narrative review Crit Care, 2024.PMID 39215292
- [15]Mokart D, Saillard C, Zemmour C, et al. Early prognostic factors in septic shock cancer patients: a prospective study with a proteomic approach Acta Anaesthesiol Scand, 2018.PMID 29315472
- [16]Maschmeyer G, Donnelly JP. How to manage lung infiltrates in adults suffering from haematological malignancies outside allogeneic haematopoietic stem cell transplantation Br J Haematol, 2016.PMID 26729577