ICU · resuscitation
Post-Cardiac Arrest Syndrome (PCAS) — Comprehensive ICU Management
Also known as Post-cardiac arrest syndrome · PCAS · Post-ROSC syndrome · Post-arrest brain injury · Post-arrest myocardial dysfunction · Post-resuscitation care · Post-arrest care bundle · Post-arrest multi-organ failure
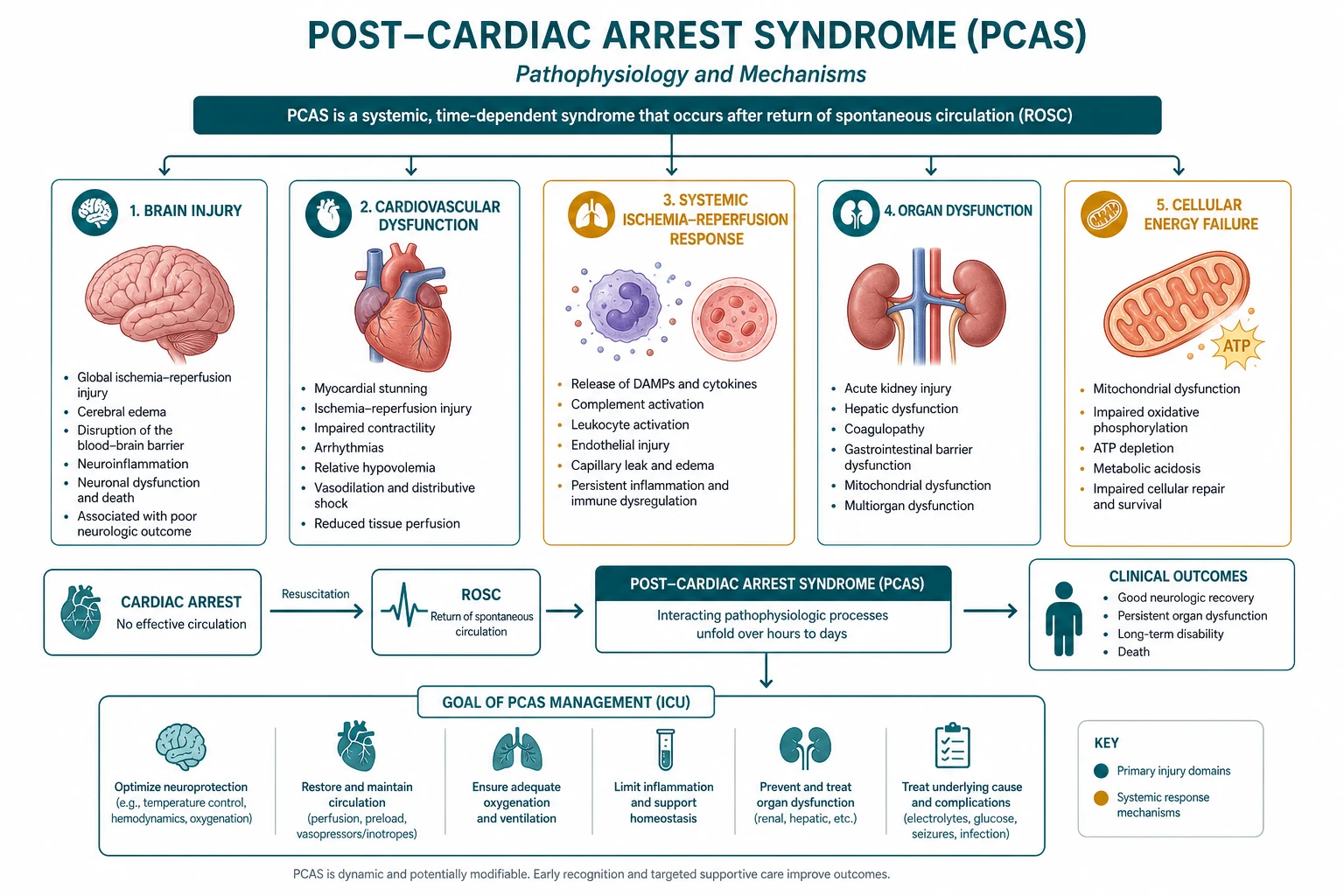
Post-cardiac arrest syndrome (PCAS) — the pathophysiological sequela of whole-body ischaemia/reperfusion injury following return of spontaneous circulation (ROSC), comprising four interconnected components: (1) post-arrest brain injury (PABI — the leading cause of death, from excitotoxicity, apoptosis, blood-brain barrier disruption, seizures), (2) post-arrest myocardial dysfunction (myocardial stunning — reversible global LV systolic dysfunction, onset hours, nadir 24-48h, recovery 72h+), (3) systemic ischaemia/reperfusion response (SIRS-like vasoplegia, coagulopathy, adrenal suppression, immunosuppression, MODS), (4) persistent precipitating pathology (ACS in 50-70% — must be identified and treated). ICU management bundle: (1) targeted temperature management (32-36C x 24h), (2) haemodynamic optimisation (MAP 65 mmHg, avoid hypotension — each episode MAP <65 = worse neurological outcome, SBP <90 = 80% mortality), (3) oxygen titration (target SpO2 94-98% — avoid both hypoxia AND hyperoxia — hyperoxia worsens oxidative stress after reperfusion), (4) ventilation (normocapnia PaCO2 35-45 mmHg — both hypocapnia [cerebral vasoconstriction] and hypercapnia [intracranial hypertension] worsen outcome), (5) seizure detection and treatment (continuous EEG — non-convulsive status in 10-30%), (6) glucose control (8-10 mmol/L — avoid hypoglycaemia), (7) identify and treat the cause (urgent coronary angiography if ACS suspected), (8) prognostication (delay 72h post-rewarming — multimodal approach).
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Overview
PCAS is not a single disease — it is a syndrome of interconnected injuries that feed back on each other: brain injury causes catecholamine surge → myocardial stress → arrhythmia → re-arrest; myocardial dysfunction → hypotension → cerebral hypoperfusion → worsened brain injury; systemic inflammation → vasoplegia → hypotension → worsened brain injury. The intensivist must manage ALL four components simultaneously — focusing on only one (e.g., TTM alone) misses the systemic nature of the injury.[1][2]
Component 1: Post-Arrest Brain Injury (PABI) — the #1 killer
Brain injury is the leading cause of death in patients admitted to ICU after cardiac arrest (responsible for ~68% of deaths). The injury occurs in FOUR phases:[1]
Four phases of post-arrest brain injury
| Phase | Timing | Mechanism | Intervention |
|---|---|---|---|
| 1. No-flow (ischaemic insult) | During arrest (before CPR) | Cerebral blood flow = 0 → ATP depletion → failure of Na+/K+ ATPase → intracellular Na+ accumulation → cytotoxic oedema → cell death. Calcium influx → activation of proteases/lipases → membrane damage | Reduce no-flow time (bystander CPR, rapid EMS) |
| 2. Low-flow (CPR) | During CPR | Cerebral blood flow = 15-30% of normal (marginal) → ongoing ischaemia → energy failure | High-quality CPR (rate 100-120, depth 5-6 cm, minimise interruptions) |
| 3. Reperfusion injury | First minutes-hours after ROSC | Reperfusion → massive oxidative stress (ROS generation) → lipid peroxidation, mitochondrial damage → apoptosis + necrosis. Glutamate excitotoxicity (NMDA receptor activation → calcium overload). Blood-brain barrier disruption → vasogenic oedema. Inflammatory cascade (cytokines, complement, neutrophil infiltration) | TTM (neuroprotection — reduces metabolic demand, suppresses apoptosis/inflammation). Avoidance of secondary insults (hypotension, hypoxia, hyperoxia, hypercapnia, fever, hyperglycaemia, seizures) |
| 4. Secondary injury | Hours-days after ROSC | Ongoing cerebral hypoperfusion (from systemic hypotension), recurrent seizures (non-convulsive status), fever, hyperglycaemia, metabolic derangement | ICU bundle: MAP >65, SpO2 94-98%, PaCO2 35-45, normothermia (post-TTM), glucose 8-10, continuous EEG, treat seizures |
Component 2: Post-Arrest Myocardial Dysfunction — the stunning
Post-arrest myocardial dysfunction ("myocardial stunning") is a REVERSIBLE global LV (and sometimes RV) systolic dysfunction that occurs after ROSC, unrelated to structural heart disease. The clinical hallmark: a patient who arrests from VF, is defibrillated to ROSC, then develops cardiogenic shock with LVEF 20-30% — despite having had a normal EF before arrest.[1]
Pathophysiology: reperfusion injury to myocardium → generation of reactive oxygen species → mitochondrial dysfunction → calcium overload → myofilament desensitisation to calcium → reduced contractility. The stunning is REVERSIBLE because the myocytes are ALIVE (not necrotic) — they are just stunned (hypocontractile). Recovery occurs as mitochondrial function and calcium handling normalize. [1]
Time course:
- Onset: within hours of ROSC
- Nadir: 24-48 hours post-ROSC (maximum LV dysfunction)
- Recovery: begins at 72 hours, complete recovery within 1-2 weeks (in survivors) [1]
Clinical significance:
- LVEF at 24h post-ROSC does NOT predict final cardiac function or outcome (stunning will recover)
- Post-arrest hypotension may be from myocardial stunning (NOT just vasoplegia)
- May require temporary inotrope/mechanical support (IABP, Impella, VA-ECMO) to bridge to recovery
- Do NOT list for transplant or place durable LVAD in the first 72h (stunning may fully recover) [1]
Management:
- Echocardiography at 6-24h post-ROSC (assess LVEF, RV function, wall motion abnormalities)
- If LVEF <30% or cardiogenic shock: inotrope (dobutamine 2.5-10 mcg/kg/min, milrinone 0.125-0.5 mcg/kg/min) — promote contractility while stunning recovers
- If refractory shock: mechanical support (IABP, Impella, VA-ECMO) — bridge to myocardial recovery
- Serial echocardiography (every 24-48h) — track recovery of LVEF [1]
Component 3: Systemic Ischaemia/Reperfusion Response — SIRS after ROSC
Whole-body ischaemia/reperfusion triggers a systemic inflammatory response that resembles sepsis (SIRS). The syndrome includes vasoplegia, coagulopathy, adrenal suppression, and immunosuppression.[1]
Systemic ischaemia/reperfusion response — organ-specific effects
| System | Mechanism | Clinical manifestation | ICU management |
|---|---|---|---|
| Vasculature | NO-mediated vasoplegia + endothelial dysfunction → loss of vascular tone | Distributive shock (high cardiac output, low SVR) — may coexist with cardiogenic shock (from stunning) → combined shock physiology | Noradrenaline (alpha-agonist — restores SVR). Add vasopressin if refractory. Target MAP >65 |
| Coagulation | Ischaemia-reperfusion activates coagulation cascade → microvascular thrombosis + fibrinolysis → DIC-like syndrome | Elevated D-dimer, prolonged APTT, thrombocytopenia, bleeding (from fibrinolysis) | Supportive — blood products if bleeding. LMWH prophylaxis (avoid therapeutic anticoagulation unless ACS/PE) |
| Adrenal | Ischaemia of adrenal cortex + cytokine-mediated suppression → relative adrenal insufficiency | Refractory vasopressor-dependent shock (steroid-responsive). Cortisol low/normal but inadequate for stress | Consider hydrocortisone 200 mg/day if refractory shock (CORTICUS-type approach — controversial). Check morning cortisol if possible |
| Immune | Gut ischaemia → bacterial translocation → endotoxaemia → immunosuppression | Fever (from SIRS, not infection), leucocytosis, positive blood cultures (from translocation). Secondary infections common (VAP, CRBSI) | Blood cultures. Empiric antibiotics if infection suspected (but don't treat SIRS fever with antibiotics). Prophylaxis: head-of-bed 30 degrees, oral care, VAP bundle |
| Kidney | Renal ischaemia (ATN) + nephrotoxic contrast (PCI) + rhabdomyolysis (from CPR) | AKI (creatinine rising, oliguria) — 40-50% of post-arrest patients | CRRT if severe. Avoid nephrotoxins. Monitor creatinine, urine output |
| Liver | Hepatic ischaemia ("shock liver") → transaminitis | ALT/AST 5-20x ULN (peak at 24-48h), coagulopathy (synthetic dysfunction) | Supportive. N-acetylcysteine (controversial — may help). Monitor LFTs + INR |
| GI | Splanchnic ischaemia → mucosal damage → bacterial translocation → ileus | Ileus, feeding intolerance, stress ulceration, acalculous cholecystitis, mesenteric ischaemia | Early enteral nutrition (within 48h). PPI prophylaxis. Monitor for abdominal compartment syndrome |
Component 4: Persistent Precipitating Pathology — find and treat the cause
The cause of the arrest MUST be identified and treated — untreated, the patient will re-arrest. In 50-70% of cardiac arrests, the cause is acute coronary syndrome (ACS).[1][2]
Common causes of cardiac arrest — identification and management
| Cause | Frequency | How to identify | Management |
|---|---|---|---|
| ACS (STEMI/NSTEMI) | 50-70% | ECG (ST elevation, new LBBB), troponin (elevated — may be elevated from CPR itself, so trend is more useful than single value), echo (regional wall motion abnormality), history (chest pain before arrest) | Urgent coronary angiography within 2h of ROSC (if STEMI on ECG or high suspicion). PCI + DAPT + anticoagulation. Even if ECG non-diagnostic (post-arrest ECG can be misleading — ST changes from CPR) → consider angiography if cardiac cause suspected |
| Pulmonary embolism | 5-10% | History (DVT risk, immobilisation, recent surgery), ECG (S1Q3T3 — non-specific), echo (RV dilation, McConnell sign), D-dimer (elevated), CT pulmonary angiogram | Thrombolysis (alteplase 50-100 mg IV) or surgical/embolectomy. Anticoagulation. Consider ECPR if cardiac arrest from massive PE |
| Hypoxia (asphyxial arrest) | 5-10% | History (drowning, hanging, choking, opiate overdose), ABG (hypoxia + hypercapnia), CXR (aspiration, oedema) | Treat underlying cause (reversal agents, bronchoscopy). Lung-protective ventilation for ARDS/aspiration |
| Electrolyte derangement | 5-10% | U&E (severe hyperkalaemia K >6.5, hypokalaemia K <2.5, hypermagnesaemia, hypomagnesaemia, hypocalcaemia), toxicology screen | Correct electrolyte (calcium gluconate + insulin/dextrose for hyperkalaemia, etc.) |
| Drug toxicity / overdose | 5-10% | History (access to medications, intentional overdose), toxicology screen (TCA, opioid, beta-blocker, CCB, digoxin) | Antidotes (naloxone, glucagon, digoxin Fab, lipid emulsion), decontamination (charcoal — if airway protected), enhanced elimination |
| Arrhythmia (primary) | 5-10% | ECG (long QT, Brugada pattern, ARVC, WPW), echo (structural heart disease), electrophysiology study | Antiarrhythmics, ICD (secondary prevention), ablation |
| Haemorrhage (hypovolaemic arrest) | 2-5% | History (GI bleed, trauma, aortic aneurysm rupture), exam (pale, hypotensive, abdominal distension), CT | Massive transfusion protocol, surgical/radiological control of bleeding source |
| Unknown | 5-10% | Extensive workup (cardiac MRI, tox screen, genetic testing, EP study) | Treat empirically (antiarrhythmics, ICD) while investigating |
The ICU management bundle — evidence-based targets

Post-cardiac arrest syndrome ICU bundle — first 24 hours
-
TARGETED TEMPERATURE MANAGEMENT (TTM):
- Cool to 32-36C for 24 hours (TTM trial: 33C = 36C — both equally effective for shockable rhythm — HYPERION: 33C beneficial for non-shockable rhythm/comatose)
- Method: surface cooling (Arctic Sun, Bard), intravascular cooling, or simple (ice packs, cold IV fluids). ECMO heat exchanger if on ECPR
- Rewarm at 0.25-0.5C/hr (avoid rapid rewarming — causes seizures, electrolyte shifts, vasodilation → hypotension)
- After rewarming: maintain normothermia (36.5-37.5C) — treat ANY fever aggressively (paracetamol, cooling) — fever in first 72h = worse outcome
- Sedation: propofol + fentanyl/morphine (prevent shivering during cooling — shivering increases metabolic demand + temperature). Bispectral index (BIS) or continuous EEG to monitor depth [1]
-
HAEMODYNAMIC OPTIMISATION:
- Target: MAP >65 mmHg (avoid any hypotension — SBP <90 in first 6h = 80% mortality)
- Noradrenaline first-line (restores SVR in vasoplegia) — titrate to MAP >65
- Add dobutamine/milrinone if cardiogenic component (post-arrest myocardial stunning — LVEF <30% on echo)
- Consider hydrocortisone 200 mg/day if refractory vasopressor-dependent shock (relative adrenal insufficiency)
- Avoid fluid overload (worsens pulmonary oedema) — use fluid responsiveness assessment (passive leg raise, pulse pressure variation) before boluses
- Arterial line (continuous BP monitoring) + central venous line (vasopressor access) [1]
-
OXYGEN TITRATION:
- Target: SpO2 94-98% (PaO2 80-120 mmHg)
- AVOID hyperoxia (PaO2 >300 mmHg in first hour = independent predictor of mortality — oxidative stress worsens reperfusion injury)
- Start on FiO2 100% (during resuscitation) but TITRATE DOWN within minutes of ROSC to lowest FiO2 maintaining SpO2 94-98%
- ABG within 30 min of ROSC (verify PaO2, PaCO2, pH, lactate) [1]
-
VENTILATION:
- Target: PaCO2 35-45 mmHg (normocapnia)
- AVOID hypocapnia (PaCO2 <35 — cerebral vasoconstriction → cerebral ischaemia — 2-4% reduction in CBF per mmHg drop in PaCO2)
- AVOID hypercapnia (PaCO2 >45 — cerebral vasodilation → increased cerebral blood volume → raised ICP)
- Lung-protective ventilation: Vt 6-8 mL/kg IBW, PEEP 5-8, plateau pressure <30
- Head-of-bed 30 degrees (reduce ICP + reduce VAP) [1]
-
SEIZURE DETECTION AND TREATMENT:
- Continuous EEG within 24h of ROSC (non-convulsive status epilepticus in 10-30% of comatose post-arrest patients — ONLY detectable with cEEG)
- If EEG unavailable: at minimum, 30-min routine EEG at 24h
- Treat seizures: levetiracetam 1 g IV (first-line — minimal interactions, no respiratory depression), valproate 20 mg/kg IV (second-line), benzodiazepines (midazolam — for status), propofol (for refractory status)
- Do NOT give prophylactic anticonvulsants (no evidence of benefit — treat only if seizures occur) [1]
-
CORONARY ANGIOGRAPHY:
- Within 2h of ROSC if STEMI on ECG, or if cardiac cause suspected (even without STEMI — post-arrest ECG is unreliable)
- PCI if occlusion found — improves survival
- If no PCI capability: thrombolysis (alteplase) — less evidence post-arrest but may be considered if no other option [1]
-
GLUCOSE CONTROL:
- Target: 8-10 mmol/L (moderate control — NICE-SUGAR: tight control 4-6 increased hypoglycaemia and mortality)
- AVOID hypoglycaemia (<4 mmol/L — worsens brain injury — check glucose every 1-2h initially)
- Insulin infusion if glucose >10 mmol/L [1]
-
OTHER MEASURES:
- VTE prophylaxis (LMWH — but balance with bleeding risk, especially if anticoagulated for ACS)
- Stress ulcer prophylaxis (PPI — if mechanically ventilated >48h or coagulopathy)
- Early enteral nutrition (within 48h — trophic feeding, advance as tolerated)
- Antibiotics only if infection suspected (do NOT treat post-arrest SIRS fever with antibiotics — cultures first)
- Family communication + discussion of goals of care + organ donation consideration
Targeted temperature management — the evidence
TTM evidence — the landmark trials
| Trial | Year | Comparison | Key finding | Clinical implication |
|---|---|---|---|---|
| HACA (Bernard) | 2002 | Hypothermia 32-34C vs normothermia (comatose post-VF arrest) | Hypothermia: 55% good outcome vs 39% normothermia (NNT=6) | Established TTM as standard of care for VF arrest |
| TTM (Nielsen) | 2013 | 33C vs 36C for 24h (comatose post-arrest, all rhythms) | NO difference in mortality or neurological outcome (both ~50% good outcome) | 33C = 36C — both acceptable. Centres can choose either target. Many centres moved to 36C (fewer side effects — shivering, arrhythmia, bleeding, infection) |
| HYPERION (Lascarrou) | 2019 | 33C vs 37C for non-shockable rhythm (PEA/asystole) arrest | 33C: 10.2% good CPC vs 5.7% normothermia (p=0.04) | TTM at 33C BENEFICIAL for non-shockable rhythm arrest (previously unclear — TTM trial included mostly shockable) |
| TTM-2 (Dankiewicz) | 2021 | 33C vs normothermia (~37.5C with active treatment of fever) | NO difference in mortality or outcome (both ~50%) | 33C = normothermia (if fever actively treated). Suggests the key intervention may be FEVER PREVENTION rather than hypothermia per se |
| Current practice | 2024 | Individualised — 32-36C for 24h + normothermia thereafter | TTM recommended for ALL comatose post-arrest patients. 33C preferred for non-shockable. Normothermia with fever avoidance is minimum standard | The field is moving towards: (1) individualised TTM (lower for worse injuries). (2) Aggressive fever avoidance after rewarming. (3) Recognition that TTM is just ONE part of the post-arrest bundle |
Prognostication — the multimodal approach
Prognostication after cardiac arrest is the MOST DIFFICULT decision in ICU. Withdraw life-supporting therapy (WLST) too early = lose a potentially recoverable patient. WLST too late = prolonged futile suffering. The principle: use MULTIPLE modalities at >72 hours post-rewarming and NEVER rely on a single test.[5]
Prognostication timeline — the 72-hour rule
- DAYS 0-2 (TTM period): DO NOT PROGNOSTICATE. The patient is sedated, cooled, and possibly paralysed. Clinical examination is unreliable. Biomarkers (NSE, S100B) may be falsely elevated. EEG may show burst suppression from TTM/sedation
- DAY 2-3: Rewarm to normothermia (0.25-0.5C/hr). STOP sedatives (allow washout — propofol: 30-60 min; midazolam: 6-12h; fentanyl: 3-6h; if renal/hepatic dysfunction: longer)
- DAY 3+ (72h post-rewarming, fully normothermic, sedation-free): Begin MULTIMODAL prognostication:
- Clinical exam: (a) Brainstem reflexes (pupillary light reflex — ABSENT at 72h = strong predictor of poor outcome). (b) Motor response to pain — extensor or absent = poor. (c) Glasgow Coma Scale. (d) Myoclonus (not myoclonic status — which is different): continuous myoclonus <24h = historically poor but not absolute
- EEG: (a) Continuous EEG for 24h. (b) Background reactivity (present = good prognosis). (c) Malignant patterns (suppression, burst-suppression, status epilepticus) = poor. (d) Somatosensory evoked potentials (SSEP): bilateral absent N20 cortical response at 72h = most reliable predictor of poor outcome (positive predictive value >95%)
- Biomarkers: (a) Neuron-specific enolase (NSE) — serum — elevated >60 ng/mL at 48-72h = poor. (b) S100B — elevated >0.4 ug/L = poor. (c) Trends more useful than single values
- Neuroimaging: (a) CT brain: diffuse cerebral oedema (loss of grey-white differentiation, sulcal effacement) = poor. (b) MRI brain: diffuse cortical restricted diffusion (DWI) = poor (but MRI is difficult in ICU patients — lines, monitors)
- DECISION: combine ALL modalities. If MULTIPLE modalities concordantly predict poor outcome (e.g., absent brainstem reflexes + absent N20 on SSEP + malignant EEG + elevated NSE + diffuse oedema on CT) → discuss WLST with family. If ANY modality is indeterminate → continue observation. If modalities are discordant → continue observation + repeat at 5-7 days. NEVER WLST based on a single modality
- FAMILY DISCUSSION: explain the findings, the uncertainty, the timeline. Use clear language. Involve palliative care. Respect cultural/religious beliefs. Consider organ donation (if WLST decided)
SAQ — Post-cardiac arrest syndrome: the ICU management bundle
10 minutes · 10 marks
A 60-year-old man achieves ROSC after out-of-hospital VF arrest, with a down-time of 25 minutes. He is intubated, sedated, and admitted to ICU. Outline the integrated ICU management bundle and the evidence for each component.
SAQ — Neuroprognostication after cardiac arrest
10 minutes · 10 marks
A 65-year-old woman is 72 hours post-ROSC after a witnessed VF arrest with a down-time of 18 minutes. She is now normothermic and off sedation, but remains unresponsive (GCS 4) with absent brainstem reflexes. The family asks about prognosis.
Clinical pearls
Red flags
Prognosis
Post-cardiac arrest outcomes — what determines survival
| Factor | Survival with good neurological outcome | Notes |
|---|---|---|
| Witnessed VF arrest, bystander CPR, ROSC <20 min | 50-60% | The ideal candidate — TTM + bundle gives best outcomes |
| Witnessed VF arrest, delayed CPR (>5 min no-flow) | 25-35% | Brain injury from no-flow period limits outcome |
| Non-shockable rhythm (PEA/asystole) | 10-20% | HYPERION: TTM at 33C improves outcome vs normothermia |
| Unwitnessed arrest | 5-15% | Unknown no-flow time → worse outcome |
| Profound acidosis (pH <7.0) at ROSC | 10-20% | Marker of severity of ischaemia |
| Lactate >10 mmol/L at ROSC | 15-25% | Marker of severity — falling lactate over 24h = better prognosis |
| Anoxic brain injury (CT: diffuse oedema, loss of grey-white) | <5% | Severe brain injury — poor prognosis regardless of other factors |
| Overall (all comatose post-arrest ICU admissions) | 30-50% | Has improved dramatically with TTM + post-arrest bundle |
Key trials and evidence
TTM trial — 33C vs 36C after cardiac arrest (PMID 24637031)
Study design
Randomised, international, multicentre — 950 patients
Population
Comatose adults after out-of-hospital cardiac arrest (all rhythms)
Intervention
TTM at 33C vs 36C for 28 hours, then normothermia
Primary outcome
All-cause mortality at end of trial: 50% (33C) vs 48% (36C) — NO significant difference
Neurological outcome
Good (CPC 1-2): 46% (33C) vs 48% (36C) — NO significant difference
Adverse events
Hypokalaemia more common at 33C. No difference in bleeding, infection, arrhythmia
Clinical bottom line
33C and 36C are EQUIVALENT for outcome. Centres can choose either target. The key is TTM itself (not the specific temperature) plus the entire post-arrest bundle (MAP, oxygen, ventilation, seizure control, PCI)
HYPERION trial — TTM for non-shockable rhythm arrest (PMID 30870392)
Study design
Randomised, multicentre — 581 patients
Population
Comatose adults after in-hospital or out-of-hospital cardiac arrest with NON-SHOCKABLE rhythm (asystole/PEA)
Intervention
TTM at 33C vs normothermia (37C) for 24 hours
Primary outcome
Good neurological outcome (CPC 1-2) at 90 days: 10.2% (33C) vs 5.7% (37C) — statistically significant (p=0.04)
Key finding
TTM at 33C IS beneficial for non-shockable rhythm arrest — previously unclear (TTM trial was mostly shockable)
Clinical bottom line
ALL comatose post-arrest patients should receive TTM — including non-shockable rhythm (asystole/PEA). 33C is preferred for non-shockable
Kilgannon 2010 — Hyperoxia after cardiac arrest (PMID 22517881)
Study design
Multicentre cohort — 6,326 patients (PROTECT trial database)
Population
Adults after cardiac arrest with ROSC admitted to ICU
Exposure
Arterial PaO2 in first 24h post-arrest
Key finding
Hyperoxia (PaO2 >300 mmHg) — independent predictor of in-hospital mortality (OR 1.8 vs normoxia)
Key finding
Hypoxia (PaO2 <60 mmHg) — also predictor of mortality
Clinical bottom line
AVOID hyperoxia after cardiac arrest — titrate FiO2 to SpO2 94-98% — the optimal PaO2 is 80-120 mmHg. Both hyperoxia and hypoxia are harmful
References
- [1]Nolan JP, et al. Evaluation of the cytotoxicity, genotoxicity and mutagenicity of diphenyl ditelluride in several biological models Mutagenesis, 2010.PMID 20123696
- [2]Callaway CW, et al. Reduction of hexavalent chromium using Aerva lanata L.: elucidation of reduction mechanism and identification of active principles J Hazard Mater, 2014.PMID 24681590
- [3]Kilgannon JH, et al. The power of one Sci Transl Med, 2012.PMID 22517881
- [4]Nielsen N, et al. [Aneurysmal rupture complicating aortitis: a case report] J Mal Vasc, 2014.PMID 24637031
- [5]Sandroni C, et al. A study of association between cervical cytology and period of co-habitation with husbands in the wives of serving soldiers Med J Armed Forces India, 2019.PMID 31388232
- [6]Lascarrou JB, et al. The Association of Nurse Practitioner Scope-of-Practice Laws With Emergency Department Use: Evidence From Medicaid Expansion Med Care, 2019.PMID 30870392