ICU · Resuscitation
Trauma resuscitation and primary survey (ATLS)
Also known as ATLS primary survey · ABCDE approach to trauma · Damage control resuscitation (DCR) · Traumatic cardiac arrest
The ATLS primary survey is a systematic approach to the trauma patient: Airway (with cervical spine control), Breathing (with ventilation), Circulation (with haemorrhage control), Disability (neurological assessment), Exposure (with temperature control). The goal is to identify and treat immediately life-threatening injuries in order of priority. Key principles: treat as you find, do not delay life-saving interventions for investigations, minimise time to definitive haemorrhage control (damage control surgery). Traumatic cardiac arrest: reversible causes (hypoxia, hypovolaemia, tension pneumothorax, cardiac tamponade) — focus on treating these, not standard ALS.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Primary survey — ABCDE
ATLS primary survey — step by step
`<C>` Catastrophic haemorrhage control (BEFORE airway)
External massive bleeding → direct pressure, tourniquet (limbs), pelvic binder (pelvic fracture — reduces volume), wound packing with haemagogel. The revised ATLS (military) puts catastrophic haemorrhage control as `<C>` before A — exsanguination kills faster than airway obstruction. Activate massive transfusion protocol early.
A — Airway with CERVICAL SPINE control
Assess: can the patient speak? (patent airway). If compromised: jaw thrust (NOT head tilt — C-spine may be injured). Consider: oropharyngeal airway (GCS <8), endotracheal intubation (RSI — assume difficult airway, full stomach). Maintain in-line C-spine immobilisation throughout. Surgical airway (cricothyroidotomy) if failed intubation.
B — Breathing and ventilation
Assess: RR, SpO2, chest movement, air entry, tracheal position. LIFE-THREATENING B problems: (1) TENSION PNEUMOTHORAX — needle decompression IMMEDIATELY (2nd ICS MCL or 5th ICS MAL, then chest drain). Do NOT wait for CXR. (2) Massive haemothorax (>1.5L) — chest drain + IV fluids + thoracotomy if >1.5L initial or >200 mL/h. (3) Flail chest — paradoxical movement, underlying contusion. Analgesia, consider intubation. (4) Open pneumothorax — 3-sided dressing, then chest drain.
C — Circulation with haemorrhage control
Assess: HR, BP, capillary refill, skin colour, urine output. Identify SOURCE of bleeding: external (visible), chest (haemothorax), abdomen (FAST scan — free fluid), pelvis (fracture — apply binder), long bones (femur fracture — traction splint). TWO large-bore IV cannulae. Blood: O-negative uncrossmatched, then type-specific, then crossmatched. Activate MTP if massive bleeding. Permissive hypotension SBP 80-90 (NOT in TBI — need MAP >80).
D — Disability (neurological assessment)
AVPU (Alert, Voice, Pain, Unresponsive) initially. GCS (Eye, Verbal, Motor) when stable. PUPILS: size, symmetry, reactivity (unilateral dilated = raised ICP/uncal herniation). Check glucose (hypoglycaemia mimics head injury). GCS <8 = intubate for airway protection and CT brain. Trend GCS — deterioration = urgent CT and neurosurgical review.
E — Exposure and temperature control
Fully expose the patient (remove all clothes — log roll for back examination). BUT keep WARM — hypothermia worsens coagulopathy (lethal triad). Use forced air blanket, warm fluids. Rectal temperature. Prevent the lethal triad: hypothermia + acidosis + coagulopathy.
MARCH and CABCDE — the military / pre-hospital variants
CABCDE (cABCDE)
Military-revised ATLS order
- `
` Catastrophic haemorrhage control first — exsanguination kills in 3-5 min, airway obstruction in 10 min - A — Airway (with C-spine)
- B — Breathing
- C — Circulation (other haemorrhage)
- D — Disability
- E — Exposure / Environment
MARCH (TCCC)
US Tactical Combat Casualty Care
- M — Massive haemorrhage control (tourniquets, wound packing with haemostatic agents)
- A — Airway (surgical airway favoured early in maxillofacial blast injury)
- R — Respiration (decompress tension pneumothorax, chest seal for sucking wound)
- C — Circulation (catastrophic — IV access, blood products, TXA, permissive hypotension)
- H — Hypothermia prevention (space blanket, ready-heat — cold + coagulopathy = death)
<XABCDE>
Civilian pre-hospital
- X — Exsanguinating haemorrhage first
- Then standard ABCDE sequence
- Adopted by many UK/Aus/NZ ambulance services (e.g., MIST handover aligns)
- Reflects the civilian translation of battlefield lessons (Iraq/Afghanistan)
Tension pneumothorax — immediate recognition
[3]Traumatic cardiac arrest
Survivable causes (4 Ts)
Potentially reversible
- Tension pneumothorax — bilateral needle decompression immediately
- Tamponade (cardiac) — resuscitative thoracotomy, pericardiocentesis
- Thromboembolism (massive PE) — rare in trauma
- Traumatic asphyxia — remove crushing force
Survivable causes (4 Hs)
Potentially reversible
- Hypoxia — intubate, 100% O2
- Hypovolaemia — massive transfusion, control bleeding
- Hypokalaemia/hyperkalaemia — check electrolytes
- Hypothermia — rewarm (see hypothermia topic)
Resuscitative thoracotomy (ED thoracotomy)
[4]Damage control resuscitation
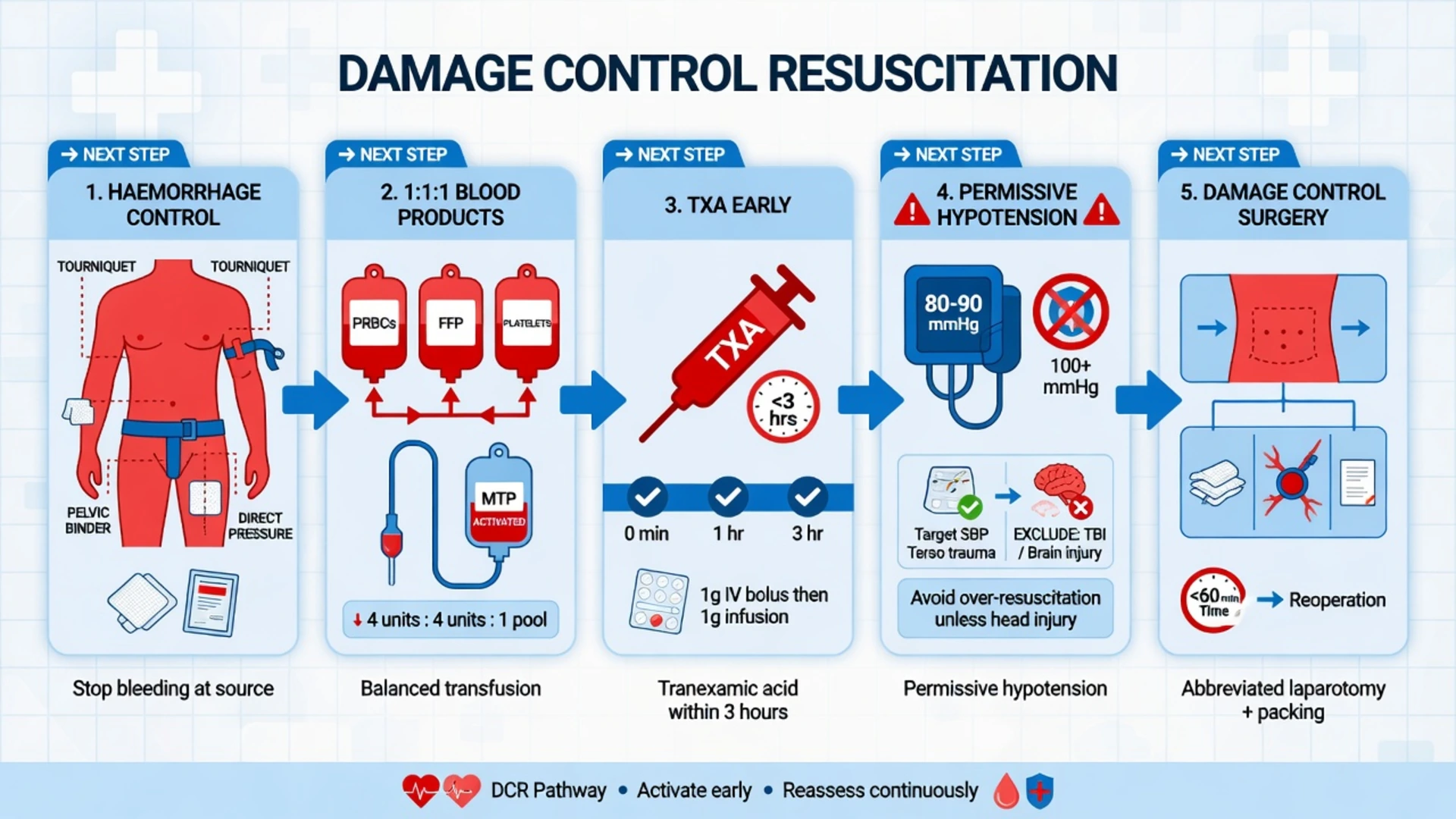
Damage control resuscitation (DCR) is the systematic, integrated package of interventions aimed at treating the lethal triad of trauma (hypothermia, acidosis, coagulopathy) while minimising time to definitive haemorrhage control. It links three domains: permissive hypotension, haemostatic (ratio-based) resuscitation, and damage control surgery. The central principle — give blood, not saline — arose from the observation that aggressive crystalloid resuscitation dilutes clotting factors, worsens acidosis, ruptures clots (pops the clot), and causes the lethal triad.[4][8]
The lethal triad / diamond of death
Hypothermia
Core temp <35°C
- Slows enzymatic clotting cascade (functionally halts at <33°C)
- Causes platelet sequestration and dysfunction
- Common in trauma — exposure, cold fluids, blood transfusion, alcohol
- Prevent: forced-air warmer (Bair Hugger), warm IV fluids (39°C), warm ventilator circuit, blanket — "keep them warm from the start"
Acidosis
pH <7.2
- Impairs clotting factor function (each 0.1 pH drop reduces factor activity ~30%)
- Caused by shock (lactic acidosis) and hyperchloraemia from saline
- Treat the cause — restore perfusion; consider balanced isotonic solutions
- Bicarbonate does NOT fix coagulopathy (and worsens tissue CO2)
Coagulopathy
Trauma-induced (TIC)
- Endogenous (acute traumatic coagulopathy — see below) + iatrogenic (dilution from crystalloid)
- Best monitored with viscoelastic testing (TEG/ROTEM), not just INR/PTT
- Treat with balanced blood products (1:1:1), cryoprecipitate (fibrinogen), and TXA
Permissive hypotension
[7]Haemostatic resuscitation — 1:1:1 ratio
Give plasma : platelets : red blood cells in a 1:1:1 ratio (sometimes called "whole blood equivalents"), aiming to replicate the constituents of whole blood. The PROPPR trial established the safety and possible benefit of the 1:1:1 strategy.[6]
PROPPR (Holcomb, JAMA 2015)
Multicentre RCT: 680 severely injured patients predicted to need massive transfusion
Population: Adult trauma patients at 12 US level-1 trauma centres
Key finding
No significant difference in 24-hour mortality (12.7% vs 17.0%, p=0.09) or 30-day mortality (relative risk 0.92, 95% CI 0.76–1.12). BUT 1:1:1 achieved earlier haemostasis and fewer exsanguination deaths at 24h. No significant difference in complications.
Practice change
1:1:1 is safe, achieves earlier haemostasis, and reduces death from exsanguination — use empirically during active massive bleeding while awaiting definitive control.
Tranexamic acid (TXA)
CRASH-2 (Lancet 2010)
Multicentre placebo-controlled RCT: 20,211 trauma patients with significant bleeding
Population: Adult trauma patients with or at risk of major bleeding, within 8h of injury
Key finding
TXA reduced all-cause mortality (14.5% vs 16.0%, p=0.0035) and bleeding death (4.9% vs 5.7%, p=0.0077). Benefit GREATEST when given within 1 hour. Given >3 hours after injury, TXA INCREASED bleeding death.
Practice change
Give TXA 1 g IV ASAP in trauma bleeding — ideally within 1 hour, MUST be within 3 hours. Do NOT give if >3 hours since injury. Cheap, safe, simple — the single most cost-effective intervention in trauma.
Prehospital plasma and blood products
PAMPer (Sperry, NEJM 2018)
Multicentre cluster-randomised trial: 501 trauma patients transported by helicopter
Population: Adult trauma patients at risk of haemorrhagic shock (SBP <90 or HR >108)
Key finding
Plasma reduced 30-day mortality (23% vs 33%, p=0.03). Benefit greatest in those with longer transport times and more severe shock.
Practice change
Prehospital plasma in patients at risk of haemorrhagic shock improves survival — supports early blood-product (not crystalloid) resuscitation from first contact.
Damage control surgery (DCS)
Damage control surgery vs definitive surgery
Phase 1 — Abbreviated/index operation (0.5–1 h)
Aim: control bleeding + contamination, NOT definitive repair. Techniques: packs (liver/pelvis), ligation, balloon tamponade, simple closure/skin-only closure (laparostomy), temporary vascular shunt (not definitive graft). Rapid — get off the table, get to ICU to correct physiology. Re-warm, correct coagulopathy, normalise acidosis.
Phase 2 — ICU resuscitation (24–48 h)
Correct the lethal triad: warm to ≥36°C, give blood products to INR <1.5 / fibrinogen >2 g/L, ventilate to normocapnia, vasopressors/inotropes as needed, plan re-look. The "physiological" resuscitation phase — the patient is too sick for definitive surgery.
Phase 3 — Definitive reconstruction (24–72 h)
Return to theatre once physiology restored (warm, coagulopathy corrected, lactate <2, not acidotic). Remove packs, definitive bowel anastomosis, vascular repair, abdominal closure. May need multiple re-looks.
Trauma-induced coagulopathy (TIC)
TIC is an endogenous, early (within 30 min of injury) coagulopathy that occurs in ~25% of severely injured trauma patients and is independent of dilution from fluid. It is one of the strongest predictors of mortality (4× increase) and massive transfusion. TIC is now understood to have two intertwined mechanisms — acute traumatic coagulopathy (ATC) and iatrogenic dilutional coagulopathy — plus the modifying effects of acidosis and hypothermia.[9][8]
Pathophysiology — the three pillars
Activation of protein C
Brohi hypothesis
- Tissue hypoperfusion → endothelial glycocalyx shedding + thrombin-thrombomodulin complex
- Thrombomodulin activates protein C → auto-anticoagulation
- Activated protein C consumes factor Va, VIIIa, and PAI-1 → both anticoagulation AND hyperfibrinolysis
- Explains why TIC occurs WITHOUT fluid resuscitation
Hyperfibrinolysis
Clot breakdown
- Increased tPA release from injured endothelium + reduced PAI-1
- Visible on TEG/ROTEM as rapid clot lysis (LY30 >3%)
- Rationale for TXA — antifibrinolytic
- Both DIC-like consumption AND pathological breakdown contribute
Endothelial activation
Systemic endotheliopathy
- Sympathetic surge → endothelial glycocalyx degradation → leak
- von Willebrand factor surge + platelet activation early (prothrombotic in microvasculature) + consumption
- Catecholamine-driven — explains why shocked, agitated patients clot worst
Diagnosis — viscoelastic testing
TEG (Kaolin)
Whole blood, 30 min
- R-time (reaction) → clotting factor function (prolonged → give FFP)
- K-time + α-angle → fibrinogen and platelets (low α → give cryoprecipitate)
- MA (max amplitude) → platelet function (low → give platelets)
- LY30 → fibrinolysis (>3% → give TXA)
ROTEM
European equivalent
- EXTEM (extrinsic) and INTEM (intrinsic) — analogous to PT and aPTT
- FIBTEM (with platelet inhibitor) → fibrinogen level (MCF <10 mm → cryoprecipitate)
- APTEM → distinguishes hyperfibrinolysis (compare to EXTEM)
- Better than standard coagulation tests (INR/PTT) which take >45 min and miss the dynamic picture
Management framework — "minimise dilution, give what is missing"
Treating TIC stepwise
1. Stop dilution
NO crystalloid boluses beyond 1 L. Avoid 0.9% saline (hyperchloraemic acidosis). Use balanced crystalloid (PlasmaLyte, Hartmann) only as carrier. Blood, not saline.
2. Give blood products in 1:1:1 ratio
During active bleeding, target RBC:plasma:platelets 1:1:1 empirically (PROPPR). Use uncrossmatched O-negative first, then type-specific, then fully crossmatched.
3. Give TXA 1 g IV within 3 h
CRASH-2 — give ASAP. Do NOT give if >3 h since injury (increases mortality). Then 1 g infusion over 8 h.
4. Correct fibrinogen FIRST
Fibrinogen is the FIRST clotting factor to fall in trauma (target >2 g/L, >2.5 in pregnancy). Give cryoprecipitate (2 pools = 10 units) or fibrinogen concentrate (5–7 g). TEG/ROTEM (FIBTEM <10 mm) guides this.
5. Prevent and treat the lethal triad
Warm the patient (forced-air blanket, warm fluids & blood, ambient temp). Treat acidosis by restoring perfusion (not bicarbonate). Correct coagulopathy with blood products.
6. Calcium replacement
Citrate in stored blood chelates calcium → hypocalcaemia causes hypotension and coagulopathy. Give calcium chloride 1 g per 4 units RBC/FFP. Maintain ionised Ca²⁺ >1.0 mmol/L.
7. Definitive haemorrhage control
All of the above is futile without surgical or angioembolisation control of bleeding. Time to theatre/angio is the single most important factor.
Traumatic brain injury (TBI) in trauma resuscitation
TBI is the leading cause of trauma death in patients who reach hospital alive. The anaesthesia/ICU principles revolve around preventing secondary brain injury from hypoxia, hypotension, and raised intracranial pressure (ICP) — because the primary injury (the mechanical damage at the moment of impact) cannot be undone.[7]
Cerebral perfusion pressure (CPP) — the master variable
[6]Intracranial hypertension — emergency management
Raised ICP / impending herniation — escalating ladder
Tier 0 — Resuscitation
Airway, oxygenation (SpO₂ ≥94%, PaO₂ ≥11), ventilation (PaCO₂ 4.5–5.0 kPa — prophylactic hyperventilation is HARMFUL). Maintain SBP ≥110 (MAP ≥80). Normothermia (36–37°C), normoglycaemia. Head-up 30°, head neutral (no neck ties).
Tier 1 — First-line therapy
Sedation + analgesia (propofol infusion, fentanyl — reduces cerebral metabolic rate for O₂ → reduces cerebral blood flow → reduces ICP). Normotonic saline bolus (3% hypertonic saline 250 mL for acute rise, or mannitol 0.5 g/kg if serum Na >160 / osmolality >320). EVD if hydrocephalus / ICP monitoring if GCS ≤8 with abnormal CT.
Tier 2 — Second-line
Hyperosmolar therapy (3% saline infusion to Na 150–155 mmol/L, OR mannitol 1 g/kg alternating). Normobaric hyperoxia may be considered. Maintain CPP 60–70 with noradrenaline if needed. Pupil check — unilateral dilation = herniation.
Tier 3 — Rescue / refractory
Decompressive craniectomy (RESCUEicp — improves mortality but many survivors in vegetative or severe disability state). Barbiturate coma (pentobarbital) to burst suppression on EEG. Hypothermia 33–35°C (controversial). Consider PARAGON / neuromonitoring. Definitive surgical evacuation of mass lesion.
Trauma airway in suspected TBI
Goals of RSI in TBI
Prevent secondary injury
- Avoid hypoxia (preoxygenate, apnoeic oxygenation with nasal spec)
- Avoid hypotension (avoid propofol / thiopentone as sole agent; use ketamine 1–2 mg/kg)
- Avoid coughing/bucking (cough → ICP spike → herniation)
- Avoid hypercarbia (rapid sequence — do not delay ventilation)
Drug choices
TBI-friendly
- Induction: ketamine 1–2 mg/kg (maintains BP, traditionally thought to raise ICP but actually safe with controlled ventilation); or etomidate 0.3 mg/kg
- Avoid propofol in shocked patients (hypotension)
- Paralytic: rocuronium 1.2 mg/kg (sugammadex reversal) or suxamethonium 1.5 mg/kg
- Pre-treatment with fentanyl 2–3 mcg/kg blunts sympathetic response
TXA in TBI — CRASH-3
CRASH-3 (Lancet 2019)
Multicentre placebo-controlled RCT: 12,737 trauma patients with TBI
Population: Adults with isolated TBI (no major extracranial bleeding), within 3h of injury
Key finding
No overall significant reduction in head-injury death (8.9% vs 9.6%). BUT clear benefit in patients with **mild-to-moderate TBI** (GCS 9–15) treated **within 3 hours** (RR 0.78). No increase in complications, no excess vascular occlusion. Benefit disappears >3h.
Practice change
Give TXA 1 g IV ASAP in suspected TBI within 3h of injury — particularly benefit in mild-moderate TBI. Safe, simple, cheap. No role if >3h.
Pelvic fractures — haemorrhage control
Pelvic ring fractures can cause massive retroperitoneal haemorrhage (up to 4 L into the retroperitoneum before tamponade) — the volume is fixed by the broken ring, so the bleeding doesn't stop until you close the ring. Mechanism: high-energy blunt trauma (fall from height, motor vehicle crash, crush). The pelvis is a "bucket" — break the bucket and the volume increases uncontrollably.[12]
Management ladder
Unstable pelvic fracture — control bleeding stepwise
1. Pelvic binder IMMEDIATELY
Apply a **circumferential pelvic binder** (T-POD, SAM Pelvic Sling) at the level of the **greater trochanters** (NOT the iliac crests) — this closes the open book / vertical shear fracture, reduces pelvic volume, and tamponades venous/arterial bleeding. Apply early — in the resus bay, on suspicion. Do NOT spring the pelvis (exacerbates bleeding). Leave binder in place until skeletal stabilisation (external fixator or ORIF).
2. Volume resuscitation + MTP
Damage control resuscitation: blood not saline, 1:1:1 ratio, TXA within 3h. Permissive hypotension (SBP 80–90) UNLESS TBI. Aim for definitive haemorrhage control within 60–90 min.
3. Angiography + embolisation
If persistent haemodynamic instability after binder + resuscitation, OR if CT shows contrast blush (active arterial bleeding) → interventional radiology for **pelvic angioembolisation** (gelatin sponge, coils). Targets internal iliac artery branches. Necessary in ~10–20% of unstable pelvic fractures.
4. Pre-peritoneal pelvic packing (PPP)
If haemodynamically unstable AND no IR available within 60 min → PPP at the bedside or theatre. Pack 3 rolled swabs each side of bladder via suprapubic incision → tamponades venous bleeding. Temporary, then external fixator, then angiography.
5. External fixation
Definitive early skeletal stabilisation — anterior external fixator (OR C-clamp for posterior ring). Reduces fracture, controls bleeding, allows nursing. Definitive ORIF later once stabilised.
LC (lateral compression)
Most common, most stable
- Side-impact (e.g., T-bone crash)
- Posterior force → internal rotation of hemipelvis
- Often low-energy, internal bleeding usually minimal
- Binder less critical (already closed); treat associated injuries
APC (anteroposterior compression) — "open book"
Highest bleeding risk
- AP compression (head-on crash, crush between vehicles)
- Symphysis pubis + sacroiliac joints disrupted → external rotation
- Pelvic volume massively increased → massive retroperitoneal bleeding
- **PELVIC BINDER MANDATORY** — may be life-saving
VS (vertical shear) — Malgaigne
High-energy, unstable
- Fall from height onto one leg, or motorcyclist
- Vertical displacement of hemipelvis through sacroiliac complex
- Risk of internal iliac arterial bleeding AND lumbosacral plexus injury
- Binder + skeletal traction (femoral pin) to reduce vertical migration
Blunt thoracic aortic injury (BTAI)
The second leading cause of trauma death at scene (after head injury). Deceleration injury (motor vehicle crash, fall from height) tears the aorta — typically at the isthmus (just distal to the left subclavian artery, where the mobile arch meets the fixed descending aorta). Most die at scene (80%). Survivors who reach hospital have a partial transection contained by the adventitia — a time bomb that can rupture hours to days later.[7]
[7]BTAI management — graded by grade
Grade I (intimal tear)
Small intimal flap <10 mm, no haematoma. Conservative management — strict BP control (SBP <120), serial imaging. Many resolve spontaneously.
Grade II (intramural haematoma)
Larger intimal injury, intramural haematoma. Strict BP control, repeat CTA at 24–48h, delayed repair if progressing.
Grade III (pseudoaneurysm)
Pseudoaneurysm — contained rupture by adventitia. **Urgent endovascular repair (TEVAR)** — thoracic endovascular aortic repair. Stent graft across the injury.
Grade IV (rupture)
Free rupture — almost always fatal. Emergent TEVAR if any signs of life. Open repair if no IR available.
TEVAR (endovascular)
Modern standard
- Preferred for grade III/IV in 2020s — covered stent across isthmus
- Lower mortality (5–9%) and paraplegia risk than open
- Access via femoral artery cut-down
- Risk: stroke (~5%), access vessel injury, endoleak, late stent migration
Open repair
Historical standard
- Left thoracotomy, clamp-and-sew with interposition graft
- Higher mortality (15–25%) and paraplegia (~5–10%) from spinal cord ischaemia
- Reserved for patients with rupture not amenable to TEVAR or no IR
Fat embolism syndrome (FES)
FES is a clinical triad occurring 24–72 h after major trauma (classically isolated femoral or tibial shaft fracture), OR after orthopaedic (joint replacement) surgery. It arises from fat globules entering the venous circulation from the marrow of fractured long bones, causing both mechanical obstruction (pulmonary capillary) and a biochemical inflammatory response (free fatty acids → capillary leak → ARDS). Cerebral involvement causes the characteristic neurological picture.[12]
Gurd's diagnostic triad
Respiratory
Nearly universal (95%)
- Hypoxaemia (SpO₂ drop, tachypnoea) — first sign
- Bilateral diffuse alveolar infiltrates on CXR (snowstorm)
- Can progress to ARDS
- May precede neurological signs
Neurological
Highly variable
- Confusion, agitation, altered mental status
- Can progress to seizures, coma, focal deficits
- Microvascular fat emboli — diffuse, non-focal
- Differs from TBI (no history of impact) — FES appears 24–72h after fracture
Petechial rash
Pathognomonic (~60%)
- On **chest, axillae, conjunctivae, palate** (not on limbs)
- Transient (12–24 h)
- Pathognomonic when present — but absence does not exclude FES
FES management — supportive
1. Stabilise + oxygenation
High-flow oxygen (target SpO₂ ≥94%). Progression to ARDS mandates lung-protective ventilation (Vt 6 mL/kg, plateau pressure <30, PEEP titrated). Consider HFNO early.
2. Early fracture fixation
EARLY (within 24 h) surgical fixation of long bone fractures **reduces** FES incidence (reduces ongoing marrow fat embolisation). This is the strongest preventive evidence. Avoid prolonged traction of femoral shaft fractures.
3. Supportive ICU care
No specific antidote. Corticosteroids controversial (prophylactic methylprednisolone has mixed evidence — NOT routinely recommended). Fluid restriction, haemodynamic support (noradrenaline for shock).
4. Manage cerebral oedema
Mild head elevation, normocapnia, hyperosmolar therapy if raised ICP. Most neurological deficits resolve over days.
5. Prevent
Early fixation of long bone fractures is THE most effective prevention. Avoid multiple relocations of un-united fractures.
Crush syndrome and rhabdomyolysis
Crush syndrome is the systemic manifestation of prolonged muscle compression (classically building collapse — earthquake, bombing, trench collapse) leading to muscle necrosis (rhabdomyolysis) and release of intracellular contents (potassium, myoglobin, creatine kinase, phosphate, lactic acid). The patient looks fine while trapped; decompensation occurs on extrication and reperfusion.[5]
[3]Management priorities
Crush injury — the crush rescue protocol
1. Pre-extrication
IV access while still trapped. Begin isotonic saline 1–1.5 L/h during extrication, then 500 mL/h thereafter. Aim for urine 300 mL/h, 200–300 mL/h once stable. Do NOT use potassium-containing fluids.
2. Treat hyperkalaemia
Calcium gluconate 10% (10 mL IV) for cardioprotection. Insulin 10 units + 25 g dextrose. Salbutamol nebs. Sodium bicarbonate if severe acidosis (also helps myoglobin solubility). Sodium zirconium cyclosilicate or patiromer for slow removal. Consider haemodialysis if refractory or AKI.
3. Forced alkaline diuresis
Sodium bicarbonate 1.26% in dextrose-water to keep urine pH >6.5 — alkalinising urine prevents myoglobin precipitation in tubules. Mannitol 1–2 g/kg if NOT hypovolaemic (osmotic diuresis, free radical scavenger). Monitor CK and urine myoglobin.
4. Manage compartment syndrome
Crushed limbs frequently develop compartment syndrome — measure compartment pressures, fasciotomy if delta pressure (diastolic − compartment) <30 mmHg. Prophylactic fasciotomy in severe crush is contentious.
5. Treat AKI and DIC
Renal replacement therapy for hyperkalaemia, acidosis, fluid overload. DIC from released tissue factor — treat with blood products, FFP.
6. Prevent infection
Wounds are heavily contaminated — broad-spectrum antibiotics (ampicillin + metronidazole + aminoglycoside) + tetanus prophylaxis.
Abdominal compartment syndrome (ACS)
ACS is sustained intra-abdominal pressure (IAP) >20 mmHg with new-onset organ failure. It occurs after major trauma (especially requiring massive fluid resuscitation), ruptured AAA, severe pancreatitis, burns, or post-laparotomy. Untreated, mortality exceeds 70%. The key is recognition — it is missed because it presents as multi-organ failure with a non-specific picture.[6]
[1]Effects of raised intra-abdominal pressure
Cardiovascular
Reduced preload
- Compressed IVC and portal vein → reduced venous return
- Increased intrathoracic pressure → reduced cardiac output
- Tachycardia, hypotension, mottled peripheries
- Raised CVP and PA pressures (misleadingly high — NOT a sign of fluid overload)
Respiratory
Compressed diaphragm
- Elevated hemidiaphragms, reduced functional residual capacity
- High peak airway pressures on the ventilator
- Basal atelectasis, hypoxia, ARDS
- A "tight" abdomen with rising peak pressure = suspect ACS
Renal
Pre-renal + ATN
- Compressed renal veins + reduced cardiac output → oliguria/anuria
- Direct compression of renal parenchyma → renal dysfunction
- May mimic "shocked kidney" or ATN — but treat the cause (decompress)
Cerebral / GI
Multi-organ
- Raised ICP (transmitted intrathoracic pressure → impaired venous return)
- Intestinal ischaemia, bacterial translocation, liver dysfunction
- Mesenteric hypoperfusion — lactate rises
Management ladder
ACS — escalation from medical to surgical decompression
1. Medical management (for IAH and grade I–II ACS)
Decompress the bowel — nasogastric tube, rectal tube, prokinetics (metoclopramide, neostigmine). Reduce fluid load (diuretics, RRT if needed). Position: head of bed <30°. Avoid Trendelenburg. Optimise analgesia/sedation, consider neuromuscular blockade. Correct electrolytes (esp. K⁺ which worsens ileus).
2. Surgical decompression (for grade III–IV ACS, organ failure)
**Decompressive laparotomy** — open the abdomen, leave open (laparostomy with negative pressure wound therapy, e.g., ABThera). IAP drops immediately; cardiac output, ventilation, urine output improve within minutes. Definitive closure days later once oedema resolves.
3. Damage control — do NOT close a tight abdomen
After trauma laparotomy or massive resuscitation, **leave the abdomen open** (laparostomy) if there is any concern about IAH/ACS — primary closure under tension causes ACS. Use Bogota bag or NPWT. Plan delayed closure.
4. Resuscitation — fine balance
After decompression there may be reperfusion (sudden lactate/acid release, hyperkalaemia). Continue resuscitation, watch for reperfusion syndrome. Avoid re-tightening.
Secondary survey
Secondary survey — after primary survey complete and patient stabilised
AMPLE history
A: Allergies. M: Medications. P: Past medical history/Pregnancy. L: Last meal. E: Events/Environment (mechanism of injury — high vs low energy, blunt vs penetrating).
Head-to-toe examination
Head: scalp lacerations, racoon eyes (base of skull), Battle sign (base of skull), CSF rhinorrhoea/otorrhoea. Face: midface fractures, dental trauma. Neck: penetrating injury, expanding haematoma, subcutaneous emphysema. Chest: fractures, flail segment, auscultation. Abdomen: tenderness, guarding, FAST scan. Pelvis: stability (do NOT spring — can worsen bleeding). Perineum: lacerations, blood at urethral meatus. Extremities: fractures, pulses, compartments. Back: log roll — spinal tenderness, step-off, lacerations.
Investigations
Trauma series: CXR, pelvis X-ray, FAST scan (or CT if stable). Blood: FBC, U&E, coagulation, crossmatch, lactate, blood gas, beta-HCG (all females of childbearing age). CT: whole-body CT (pan-scan) in stable patients — head, C-spine, chest, abdomen, pelvis. FAST is for the UNSTABLE patient (identifies free fluid → operating theatre).
Definitive management
Based on injuries found. Prioritise: (1) life-threatening (haemorrhage, raised ICP, tension pneumothorax). (2) Limb-threatening (compartment syndrome, vascular injury). (3) Other injuries (fractures, facial injuries). Multidisciplinary approach: trauma surgery, orthopaedics, neurosurgery, radiology.
SAQ — Damage control resuscitation in haemorrhagic shock
10 minutes · 10 marks
A 35-year-old man is brought to the ED after a high-speed motorcycle crash. He is agitated, pale, cold and clammy. HR 132, BP 70/45 (MAP 53), RR 30, SpO2 95% on 15 L O2. There is an externally bleeding open femur fracture, a tender distended abdomen, and a systolic blood pressure that does not improve after 1 L of warmed crystalloid. A pelvic X-ray shows an unstable pelvic fracture. Lactate 6.8 mmol/L, pH 7.15, INR 1.7, temp 34.5°C. The trauma team is preparing for massive transfusion and transfer to theatre.
SAQ — Traumatic brain injury: secondary injury prevention and ICP management
10 minutes · 10 marks
A 42-year-old cyclist without a helmet is struck by a car at 60 km/h. He has a GCS of 7 (E1 V2 M4), pupils 3 mm and reactive, and is intubated in the ED for airway protection. CT brain shows a large right acute subdural haematoma with 8 mm midline shift. BP 110/70, SpO2 99% on the ventilator. The neurosurgeon is en route for a decompressive craniectomy. Outline your ICU management to prevent secondary brain injury and the ICP-targeted therapy while awaiting surgery.
Clinical pearls
Red flags
[12]References
- [1]Galvagno SM Jr, Nahmias JT, Young DA Advanced Trauma Life Support(®) Update 2019: Management and Applications for Adults and Special Populations. Anesthesiology clinics, 2019.PMID 30711226
- [2]Bhattacharya S, et al. Massive transfusion protocol in adult trauma population. Transfusion and apheresis science, 2020.PMID 33071074
- [3]Smith J, et al. Traumatic cardiac arrest: a narrative review. Resuscitation, 2024.PMID 39327636
- [4]Briggs A, Askari R Damage control resuscitation. International journal of surgery (London, England), 2016.PMID 27107662
- [5]CRASH-2 collaborators. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2). Lancet, 2010.PMID 20554319
- [6]Holcomb JB, Tilman BC, Dobson ME, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma (PROPPR). JAMA, 2015.PMID 25647203
- [7]CRASH-3 trial collaborators. Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3). Lancet, 2019.PMID 31623894
- [8]Rossaint R, Bouillon B, Cerny V, et al. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Critical care, 2019.PMID 30917843
- [9]Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. Journal of trauma, 2003.PMID 12813333
- [10]Sperry JL, Guyette FX, Brown JB, et al. Prehospital Plasma during Air Medical Transport in Trauma Patients at Risk for Hemorrhagic Shock. The New England journal of medicine, 2018.PMID 30044935
- [11]Akhtar S. Fat embolism. Anesthesiology clinics, 2009.PMID 19825491
- [12]Costantini TW, Coimbra R, Holcomb JB, et al. Current management of hemorrhage from severe pelvic fractures: Results of an American Association for the Surgery of Trauma multi-institutional trial. The journal of trauma and acute care surgery, 2016.PMID 26958799