ICU · Resuscitation
Acute upper airway obstruction
Also known as Upper airway obstruction (UAO) · Acute epiglottitis · Supraglottitis · Ludwig's angina · Retropharyngeal abscess · Peritonsillar abscess (quinsy) · Angioedema (hereditary, ACEi-induced, allergic) · Foreign body airway obstruction · Post-extubation stridor · Bilateral vocal cord paralysis · Inhalational thermal injury · Can't intubate, can't oxygenate (CICO) · Heliox · Awake fibre-optic intubation (AFOI)
Acute upper airway obstruction is a life-threatening emergency in which airflow through the nose, mouth, pharynx, or larynx is compromised, leading to hypoxia and death within minutes. Causes: infection (acute epiglottitis/supraglottitis, Ludwig's angina, retropharyngeal/peritonsillar abscess), swelling (hereditary and ACEi-induced angioedema, anaphylaxis), foreign body aspiration, malignancy (laryngeal, pharyngeal, anaplastic thyroid), bilateral vocal cord paralysis, post-extubation laryngeal oedema, and trauma/thermal inhalational injury. Presentation: stridor (inspiratory = extrathoracic/supraglottic, expiratory = intrathoracic, biphasic = glottic/subglottic fixed lesion), drooling, tripod position, distress, muffled or 'hot potato' voice. Stridor at rest = severe, impending obstruction. Management: do NOT agitate the patient (especially children with epiglottitis — can trigger complete laryngeal obstruction and arrest). Call for help early (senior anaesthetist + ENT + difficult airway trolley). Temporise with humidified oxygen, heliox (70:30, low-density gas reduces turbulent-flow work of breathing), nebulised adrenaline 5 mL of 1:1000, dexamethasone 8 mg IV. Secure the airway under controlled conditions — awake fibre-optic intubation preferred, inhalational induction maintaining spontaneous ventilation in children, surgical airway (cricothyroidotomy) as backup. Epiglottitis: do NOT lay flat, do NOT examine the throat. Never attempt blind nasal intubation.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
In one line
[6]Overview & definition
Acute upper airway obstruction is any compromise to the passage of air from the nose and mouth to the carina — encompassing the nasal cavity, oral cavity, pharynx, larynx, and extrathoracic trachea — that threatens gas exchange. Because the upper airway is the narrowest and most readily obstructed segment of the respiratory tract, partial obstruction can progress to complete obstruction over minutes to hours, and complete obstruction causes hypoxaemic cardiac arrest within 5–10 minutes. It is one of the few emergencies where the wrong first action (laying the child flat, poking at the throat, paralysing a partially obstructed patient) can convert a salvageable airway into a fatal one.[1][9]
The unifying principle of management is avoidance of iatrogenic loss of the airway: keep the patient in their preferred posture, do not agitate, do not blind-instrument the airway, and secure the airway in the most controlled way possible — awake fibre-optic intubation (AFOI) in the cooperative adult, inhalational induction maintaining spontaneous ventilation in the child, with a scrubbed surgical team and a front-of-neck access (FONA) kit as the rescue for the can't-intubate, can't-oxygenate (CICO) scenario.[3][5]
Pathophysiology — why upper airway obstruction is uniquely dangerous
The upper airway (pharynx, larynx, extrathoracic trachea) is extrathoracic and therefore subject to dynamic collapse during inspiration: the negative intrathuminal pressure generated by the diaphragm sucks the soft, unsupported walls of the pharynx and supraglottis inward. In a healthy airway this is resisted by pharyngeal dilator muscle tone (genioglossus, tensor palatini). Anything that narrows the lumen — swelling, tumour, foreign body, or loss of tone — converts laminar flow into turbulent flow, and because airway resistance follows Poiseuille's law inversely with the fourth power of the radius (R ∝ 1/r⁴ for laminar flow, and worse for turbulent flow), even a small further reduction in radius produces a dramatic rise in the work of breathing.[9]
The clinical consequences are:[1]
- Increased work of breathing — large negative intrathoracic pressures are generated, pulling on the diaphragm and accessory muscles, producing intercostal and suprasternal recession and paradoxical (see-saw) abdominal breathing.
- Dynamic airway collapse — the more negative the inspiratory pressure, the more the supraglottis and pharynx are sucked inward, so obstruction worsens with effort (a positive-feedback loop). This is why a child with epiglottitis who is agitated cries harder, generates more negative pressure, and obstructs more.
- Fatigue — the upper-airway and accessory muscles tire. The dangerous sign is the tiring child or adult whose work of breathing is decreasing — this is exhaustion and impending arrest, not improvement.
- Hypoxia and hypercapnia — partial obstruction produces rapid shallow breathing and eventually hypoventilation; hypercapnia causes sedation, which worsens airway tone and obstruction (a second positive-feedback loop).
- Negative-pressure pulmonary oedema — the very negative intrathoracic pressure can acutely transude fluid into the alveoli, so the patient may present with frothy pink secretions once the obstruction is relieved (post-obstructive pulmonary oedema).[9]
Causes
Infectious
Common, often dramatic
- ACUTE EPIGLOTTITIS (supraglottitis): Haemophilus influenzae type b (Hib) — Hib vaccination has dramatically reduced paediatric incidence, so adults now predominate. Also S. pneumoniae, S. aureus (incl. MRSA), group A strep. Sudden high fever, toxic, drooling, "hot potato" voice, tripod, NO cough. Cherry-red swollen epiglottis on laryngoscopy. "Thumb sign" on lateral neck X-ray. Do NOT examine throat or lie flat.
- LUDWIG’S ANGINA: bilateral submandibular/sublingual cellulitis, nearly always from a lower second or third molar infection. Woody induration of the floor of mouth, tongue displaced upward and backward, trismus, drooling, neck swelling. Polymicrobial oral flora (streptococci, oral anaerobes, bacteroides). Airway compromise is the killer — sudden death from tongue displacement.
- RETROPHARYNGEAL ABSCESS: pus in the retropharyngeal space (between the pharynx and prevertebral fascia). Children (suppurative retropharyngeal lymph nodes) or adults (trauma — e.g. fish bone; instrumentation; immunocompromise). Neck stiffness, dysphagia, odynophagia, respiratory compromise. "Retropharyngeal widening" on lateral neck X-ray. CT for diagnosis. Risk: DESCENDING NECROTISING MEDIASTINITIS (mortality 25–40%).
- PERITONSELLAR ABSCESS (quinsy): usually unilateral; tonsillar swelling, uvular deviation away from the abscess, trismus, "hot potato" voice. Rarely compromises the airway but can. Drainage + antibiotics.
- PARAPHARYNGEAL / DEEP NECK SPACE ABSCESS: lateral pharyngeal space infection; trismus, neck swelling, sepsis; may involve carotid sheath (vessel erosion, cavernous sinus thrombosis).
Swelling / angioedema
Bradykinin vs histamine
- HEREDITARY ANGIOEDEMA (HAE): C1-esterase-inhibitor deficiency — type 1 (85%, low antigenic and functional levels), type 2 (dysfunctional protein, normal/high levels); autosomal dominant. BRADYKININ-mediated (NOT histamine). Recurrent, non-pitting, non-urticarial, non-pruritic swelling of face/lips/tongue/larynx/bowel (abdominal pain). Triggered by trauma, stress, dental work, oestrogen. Attacks last 2–5 days. Laryngeal oedema is the cause of death. Treatment: C1-INH concentrate (Berinert), icatibant, ecallantide.
- ACQUIRED ANGIOEDEMA: C1-INH depletion from B-cell lymphoproliferative disease or autoantibody; behaves like HAE.
- ACEi-INDUCED ANGIOEDEMA: bradykinin-mediated (ACE degrades bradykinin; inhibition → accumulation). Onset hours–months after starting ACEi. Swelling of lips, tongue, face, larynx, sometimes bowel. NOT histamine → adrenaline, antihistamines and steroids often FAIL. Stop ACEi permanently. Icatibant or C1-INH concentrate (conestat alfa). African ethnicity, age >65, and history of cough with ACEi are risk factors.
- ALLERGIC / HISTAMINE-MEDIATED ANGIOEDEMA: urticaria and pruritus usually accompany it; trigger (food, drug, insect sting, latex). Responds to adrenaline, antihistamines, steroids. Overlaps with ANAPHYLAXIS — see anaphylaxis-icu.
- IDIOPATHIC ANGIOEDEMA: recurrent, no identified mechanism; often histamine-mediated and steroid-responsive.
Foreign body
Sudden onset
- LARYNGEAL FOREIGN BODY: complete obstruction — aphonia, cannot cough or speak, clutching the throat. Immediate death without relief. "Café coronary" — choking at the dinner table.
- BRONCHIAL FOREIGN BODY: partial — unilateral wheeze, decreased breath sounds, persistent pneumonia. Children: peanuts (oil causes lipoid pneumonia), beads, balloons; elderly: dentures, meat.
- OESOPHAGEAL FOREIGN BODY (e.g. coin in child): can compress the trachea and cause secondary UAO.
- Conscious adult/child >1 yr: HEIMLICH (abdominal thrusts). Infants <1 yr: 5 back blows + 5 chest thrusts (NO abdominal thrusts). Unconscious: CPR, direct laryngoscopy + Magill forceps if object visible — NEVER blind finger sweep.
Malignancy & structural
Slower, then acute
- LARYNGEAL CANCER (squamous cell carcinoma): smokers, alcohol; progressive hoarseness. Stridor is a LATE sign = advanced disease, often precipitated by oedema or bleeding.
- ANAPLASTIC THYROID CANCER: rapidly enlarging neck mass in an older patient; invades trachea/larynx; very poor prognosis. Often presents with stridor.
- Pharyngeal / base-of-tongue / hypopharyngeal carcinoma; lymphoma; metastatic nodes.
- BILATERAL VOCAL CORD PARALYSIS: recurrent laryngeal nerve injury (thyroidectomy, thoracic/cardiac surgery, prolonged intubation), tumour, or neurological (stroke, MS). Cords lie in the paramedian position → airway narrowing. Inspiratory stridor; voice may be surprisingly preserved. Treatment: tracheostomy ± later cordotomy/arytenoidectomy.
- EXTERNAL COMPRESSION: large goitre, mediastinal mass, haematoma (post-thyroidectomy, post-CVC, on anticoagulation).
- SUBGLOTTIC STENOSIS: from prolonged intubation/tracheostomy, Wegener’s granulomatosis, relapsing polychondritis, idiopathic.
Post-procedural & traumatic
ICU-specific
- POST-EXTUBATION STRIDOR: laryngeal oedema from endotracheal tube cuff pressure and mucosal trauma. Risk factors: female, large ETT, high cuff pressure, prolonged/repeated intubation, traumatic intubation, active upper-respiratory infection, inadequate sedation. Cuff leak test predicts risk. Prevent with dexamethasone 4 mg Q6H × 48 h (or 8 mg pre-extubation) in high-risk patients. Treat with nebulised adrenaline, dexamethasone, heliox, re-intubate (smaller tube) if severe.
- INHALATIONAL THERMAL INJURY: heat injury to the supraglottic mucosa from hot gases/smoke. Oedema PROGRESSES over 12–48 h. Signs: soot in mouth/sputum, singed nasal hairs, hoarse voice, stridor, facial burns. INTUBATE EARLY before the airway becomes impossible. (See burns topics.)
- LARYNGEAL TRAUMA: blunt (steering-wheel, clothesline) or penetrating; haematoma, fracture, cord injury. Maintain in-line stabilisation; avoid RSI if possible; surgical airway may be needed.
- FACIAL FRACTURES (Le Fort II/III): midface instability, bleeding, posterior displacement of the maxilla obstructing the airway.
- TEMPOROMANDIBULAR JOINT DISLOCATION, retropharyngeal haematoma from anticoagulation or cervical spine injury.
Assessment & clinical features
Stridor — the cardinal sign
Stridor is the audible sound of turbulent airflow through a narrowed airway, and its phase localises the level of obstruction:[1][9]
[1]Stridor at rest = severe (critical) obstruction — an emergency. Stridor only on exertion = moderate. Biphasic stridor = critical fixed narrowing. [2]
Other features
- Drooling — inability to swallow saliva. Pathognomonic for epiglottitis and retropharyngeal abscess (the patient is too obstructed and in too much pain to swallow). Suggests supraglottic obstruction.
- Tripod position — sitting forward, leaning on the hands, neck slightly extended, mouth open. Maximises the diameter of the upper airway (opens the pharyngeal and supraglottic space) and uses accessory muscles. A patient in the tripod position should NOT be made to lie down.
- Voice changes:
- "Hot potato" voice — epiglottitis, peritonsillar abscess (as if speaking with a hot potato in the mouth).
- Muffled voice — supraglottic swelling (angioedema).
- Hoarseness — glottic pathology (vocal cord lesion, tumour, laryngitis).
- Aphonia — complete obstruction, or bilateral vocal cord paralysis.
- Trismus — peritonsillar abscess, Ludwig\u2019s angina, deep neck space infection.
- Neck swelling / woody induration — Ludwig\u2019s angina, deep neck abscess.
- Cyanosis — late, pre-arrest.
- Tachycardia, tachypnoea, accessory muscle use, intercostal/suprasternal recession, paradoxical (see-saw) breathing — increasing work of breathing.
- Agitation, then drowsiness, bradycardia (in children), decreased work of breathing, "silent chest" — EXHAUSTION and impending arrest. Do not be reassured by a quieter child.[2]
Severity grading (after the Westley/other croup scales adapted for adults)
Investigations — only in the stable, and only if they will change management
The unstable patient with severe UAO must not be taken to radiology or subjected to pharyngoscopy — these trigger complete obstruction. Investigations are for the stable patient in whom the result will change management.[1]
- Flexible nasendoscopy (awake, at the bedside) — the single most useful investigation in the cooperative adult. Assesses vocal cord movement, supraglottic swelling, tumour, foreign body with minimal distress. Avoid in the agitated child.
- Soft-tissue lateral neck X-ray — classic signs:
- "Thumb sign" — the swollen epiglottis looks like the thumb (rounded) instead of the usual thin pointed "little finger" — epiglottitis.[1]
- "Vallecula sign" — loss of the vallecular air space — epiglottitis.
- Retropharyngeal soft-tissue widening — >7 mm at C2 or >14 mm at C6 (or >50% of the AP width of the adjacent vertebral body) suggests retropharyngeal abscess.
- Prevertebral soft-tissue swelling, air-fluid level.
- Radio-opaque foreign body.
- AP neck X-ray — "steeple sign" (narrowed subglottic column, like a church steeple) — croup (paediatric subglottic tracheitis).
- CT neck/chest — defines abscess extent, deep neck space infection, mediastinal spread (for retropharyngeal/descending infection), tumour. Only in the stable.
- Laryngoscopy / bronchoscopy — definitive diagnostic and therapeutic; only by an experienced operator in controlled conditions (theatre, with airway equipment).
- Bloods — FBC, CRP, blood cultures (before antibiotics) for infection; tryptase if anaphylaxis suspected (1–2 h, 24 h, baseline); complement (C4, C1-INH antigenic and functional levels) if hereditary angioedema suspected. Do not delay antibiotics for cultures in epiglottitis.
Management
General principles — the non-negotiables
Upper airway obstruction — the first 30 minutes
Call for help EARLY
Call the SENIOR anaesthetist/airway doctor, ENT surgeon, and bring the difficult-airway trolley. This is a can’t-intubate-can’t-oxygenate scenario waiting to happen. Summoning help is the single most important early action — never manage deteriorating UAO alone.<Cite id="3" /><Cite id="4" />
Do NOT agitate the patient
Especially children with epiglottitis: agitation (examination, IV cannulation, lying flat, separation from a parent) generates more negative inspiratory pressure and can trigger complete laryngeal obstruction and cardiac arrest. Keep the child on the parent’s lap in their preferred posture. Do NOT examine the throat with a tongue depressor. Do NOT lay flat for X-ray. Allow the patient to remain upright and as calm as possible.<Cite id="1" />
Position, oxygenate, and prepare temporising treatment
Sit the patient upright in the tripod position. Give humidified oxygen to maintain SpO2 (but do not force a mask onto a distressed child). Consider HELIOX 70:30 (helium:oxygen) — the low density of helium reduces turbulent flow resistance and the work of breathing, buying time (only if the patient needs ≤30% oxygen). NEBULISED ADRENALINE 5 mL of 1:1000 (5 mg) — alpha-1 vasoconstriction rapidly reduces mucosal oedema; onset within 30 min; works for angioedema, post-extubation stridor, infectious oedema; repeat as needed (watch for rebound when it wears off). DEXAMETHASONE 8 mg IV (0.6 mg/kg in children) — long-acting glucocorticoid for oedema; onset over hours.<Cite id="1" /><Cite id="10" />
Treat the specific cause while preparing the airway
Epiglottitis: IV ceftriaxone 2 g (cover Hib, pneumococcus, GAS) — do NOT delay for cultures. Ludwig’s: ampicillin-sulbactam or clindamycin + ceftriaxone or piperacillin-tazobactam (polymicrobial oral flora) + urgent dental/drainage. Retropharyngeal abscess: broad-spectrum + surgical/CT drainage. ACEi angioedema: STOP the ACEi permanently; consider ICATIBANT 30 mg SC or C1-INH concentrate (conestat alfa); adrenaline/antihistamines/steroids often FAIL (bradykinin-mediated). Hereditary angioedema: C1-INH concentrate (Berinert 20 U/kg), icatibant, or ecallantide — NOT adrenaline/antihistamines/steroids. Allergic/anaphylaxis: IM adrenaline per anaphylaxis protocol.<Cite id="6" /><Cite id="7" />
Secure the airway — controlled conditions, surgical backup ready
IDEAL: operating theatre with senior anaesthetist + ENT scrubbed and FONA kit open. Preferred technique: AWAKE FIBRE-OPTIC INTUBATION (AFOI) in the cooperative adult — topicalise the airway with lidocaine, sedate cooperatively (dexmedetomidine), navigate the scope through the cords on inspiration, railroad a SMALLER ETT (1–2 sizes smaller due to swelling). In children/cooperative adults: INHALATIONAL INDUCTION (sevoflurane) MAINTAINING SPONTANEOUS VENTILATION — never paralyse until the airway is confirmed secure. AVOID RSI if at all possible — loss of airway tone on induction can convert a partial obstruction into complete CICO. If RSI is unavoidable (periarrest, uncooperative): have the surgical airway plan open, use a smaller tube, senior operator, videolaryngoscope. NEVER blind nasal intubation (bleeding, dislodges foreign body).<Cite id="3" /><Cite id="5" />
If cannot intubate — SURGICAL AIRWAY (FONA)
CICO rescue: scalpel-bougie CRICOTHYROIDOTOMY — identify the cricothyroid membrane with the laryngeal handshake, transverse stab incision, pass a bougie, railroad a cuffed size 6.0 tube, confirm with capnography. In children under ~8–12 yr the cricothyroid membrane is small and a needle cricothyroidotomy (jet ventilation) or formal tracheostomy may be required. NAP4’s central lesson: the fatal error in airway emergencies is DELAY in performing the surgical airway — decide early.<Cite id="4" /><Cite id="5" />
Heliox — how it works and when to use it
[10]Nebulised adrenaline — the rapid temporising agent
[6]Specific management by cause
Acute epiglottitis
Epiglottitis management:[1]
- Recognise: toxic, febrile, drooling, tripod, "hot potato" voice, no cough; thumb sign on lateral neck (only if it will not destabilise).
- Keep upright, do not agitate, do not examine the throat.
- Call senior anaesthetist + ENT; move to theatre.
- Inhalational induction (sevoflurane) maintaining spontaneous ventilation, or awake fibre-optic intubation; intubate with a tube 1–2 sizes smaller; confirm visually and with capnography.
- Surgical airway (cricothyroidotomy → tracheostomy) if intubation fails.
- IV ceftriaxone 2 g (covers Hib, pneumococcus, GAS) — do not delay for cultures.
- Rifampin prophylaxis (20 mg/kg/day, max 600 mg, for 4 days) for untreated household contacts of Hib epiglottitis.
- Decannulate once swelling resolves (usually 48–72 h).
Ludwig\u2019s angina
Ludwig\u2019s angina — airway first, source control second
Secure the airway
The airway is the immediate threat. Preferred: AWAKE FIBRE-OPTIC INTUBATION (the floor of mouth is swollen and distorted, making direct laryngoscopy difficult; RSI risks loss of the airway). Surgical airway (tracheostomy or cricothyroidotomy) may be the primary airway in severe distortion. NEVER blind nasotracheal intubation (bleeding, displacement). Have a scrubbed ENT surgeon.<Cite id="1" /><Cite id="9" />
Broad-spectrum IV antibiotics
Ampicillin-sulbactam, or clindamycin + ceftriaxone ± metronidazole, or piperacillin-tazobactam — cover streptococci, oral anaerobes, bacteroides, prevotella. Add vancomycin if MRSA suspected or severe.
Source control
Urgent dental extraction of the offending molar and/or surgical drainage of the submandibular/sublingual spaces. CT to define extent once the airway is secure. Do NOT delay antibiotics for imaging.
Monitor for spread
Watch for descending necrotising mediastinitis (CT chest) — mortality 25–40%. ICU admission for airway monitoring and supportive care.
Retropharyngeal abscess
Retropharyngeal abscess
Assess and protect the airway
May cause obstruction from anterior displacement of the posterior pharyngeal wall. Keep upright, nebulised adrenaline/dexamethasone for oedema, controlled airway if obstructed.
IV antibiotics
Broad-spectrum covering oral flora + group A strep + anaerobes (e.g. ampicillin-sulbactam or clindamycin + ceftriaxone). Add MRSA cover (vancomycin) if risk factors.
Imaging
CT neck with contrast (if airway stable) — defines abscess size, extent, mediastinal involvement. Lateral neck X-ray: retropharyngeal soft-tissue widening (>7 mm at C2, >14 mm at C6).
Surgical drainage
Transoral drainage for abscess confined to the retropharyngeal space; transcervical (external) approach if extension into danger space or mediastinum.
Watch for mediastinitis
Descending necrotising mediastinitis is the feared complication — fever, chest pain, sepsis, subcutaneous emphysema. CT chest; aggressive surgical drainage; mortality 25–40%.
Angioedema — three mechanisms, three treatments
[6]Foreign body airway obstruction
Foreign body airway obstruction — the relief algorithm
Conscious adult or child >1 yr
Encourage coughing. If ineffective and obstructed: HEIMLICH MANOEUVRE (abdominal thrusts) — stand behind, fist above the umbilicus, sharp inward and upward thrusts. Repeat. Reassess between thrusts.
Conscious infant <1 yr
5 BACK BLOWS (between the scapulae, heel of hand, infant head-down over the forearm) alternating with 5 CHEST THRUSTS (two fingers on the lower sternum, similar to CPR). NEVER perform abdominal thrusts in infants (risk of visceral injury).
Unconscious patient
Call for help, start CPR. Open the airway and look in the mouth — if the object is visible AND easily removable, use MAGILL FORCEPS under direct laryngoscopy. NEVER perform a BLIND FINGER SWEEP (can push the object deeper or cause trauma). Continue CPR.
Laryngeal foreign body (complete obstruction)
Aphonia, cannot cough/speak, clutching the throat. Heimlich immediately if conscious; CPR/laryngoscopy + Magill forceps if unconscious. If the object cannot be removed and the patient is periarrest, an emergency cricothyroidotomy may be needed to bypass a laryngeal obstruction — though this is rare and difficult.
Bronchial foreign body
Unilateral wheeze, decreased breath sounds, persistent/recurrent pneumonia. Definitive removal by RIGID BRONCHOSCOPY under general anaesthesia in theatre — NOT flexible bronchoscopy (poor control of the airway, cannot remove large objects). Peanuts cause lipoid pneumonia — do not delay.
Bilateral vocal cord paralysis
[5]Post-extubation stridor
Inhalational thermal injury
Evidence — trials, audits and guidelines
NAP4 — 4th National Audit Project (Cook TM, Woodall N, Frerk C; RCoA/DAS 2011) — major complications of airway management in the UK
FAST-3 — icatibant for hereditary angioedema (Cicardi M, NEJM 2010, PMID 21142345)
TOLD — icatibant for ACEi-induced angioedema (Sinert R, Ann Emerg Med 2017, PMID 28461253)
Jaber meta-analysis — corticosteroids to prevent post-extubation laryngeal oedema (JAMA 2009, PMID 19528563)
DAS 2018 — intubation in the critically ill adult (Higgs A, BJA 2018, PMID 29406182) and DAS 2015 CICO algorithm (Frerk C, PMID 26556874)
Exam practice
SAQ — Acute epiglottitis in the adult
10 minutes · 10 marks
A 52-year-old man presents to the emergency department with a 6-hour history of sore throat, fever (39.2°C), drooling, and a muffled voice. He is sitting forward leaning on his hands, in marked respiratory distress with an inspiratory stridor audible at the bedside. SpO2 93% on room air, RR 32, HR 118, BP 142/88. He is toxic in appearance. A junior doctor reaches for a tongue depressor.
SAQ — ACEi-induced angioedema
10 minutes · 10 marks
A 68-year-old man on lisinopril for hypertension presents with progressive swelling of his lips, tongue and floor of mouth over 4 hours. He has no urticaria or pruritus. He is drooling and has mild inspiratory stridor. SpO2 95% on room air. The medical registrar has given IM adrenaline 0.5 mg, IV chlorphenamine 10 mg and IV hydrocortisone 200 mg with no improvement.
SAQ — Heliox and nebulised adrenaline in upper airway obstruction
10 minutes · 10 marks
A 4-year-old child with known severe croup is admitted to the PICU with marked biphasic stridor at rest, sternal recession, and SpO2 94% on room air. The consultant asks you to explain the rationale and limitations of heliox and nebulised adrenaline.
Clinical pearls
Red flags
Key takeaways
[7]References
- [1]Eskander A, de Almeida JR, Irish JC Acute Upper Airway Obstruction. The New England journal of medicine, 2019.PMID 31722154
- [2]Eskander A, de Almeida JR, Irish JC Acute Upper Airway Obstruction. The New England journal of medicine, 2019.PMID 31722154
- [3]Higgs A, McGrath BA, Goddard C, et al.; Difficult Airway Society et al. Guidelines for the management of tracheal intubation in critically ill adults (DAS 2018). British Journal of Anaesthesia, 2018.PMID 29406182
- [4]Cook TM, Woodall N, Harper J, et al. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departments. British journal of anaesthesia, 2011.PMID 21447489
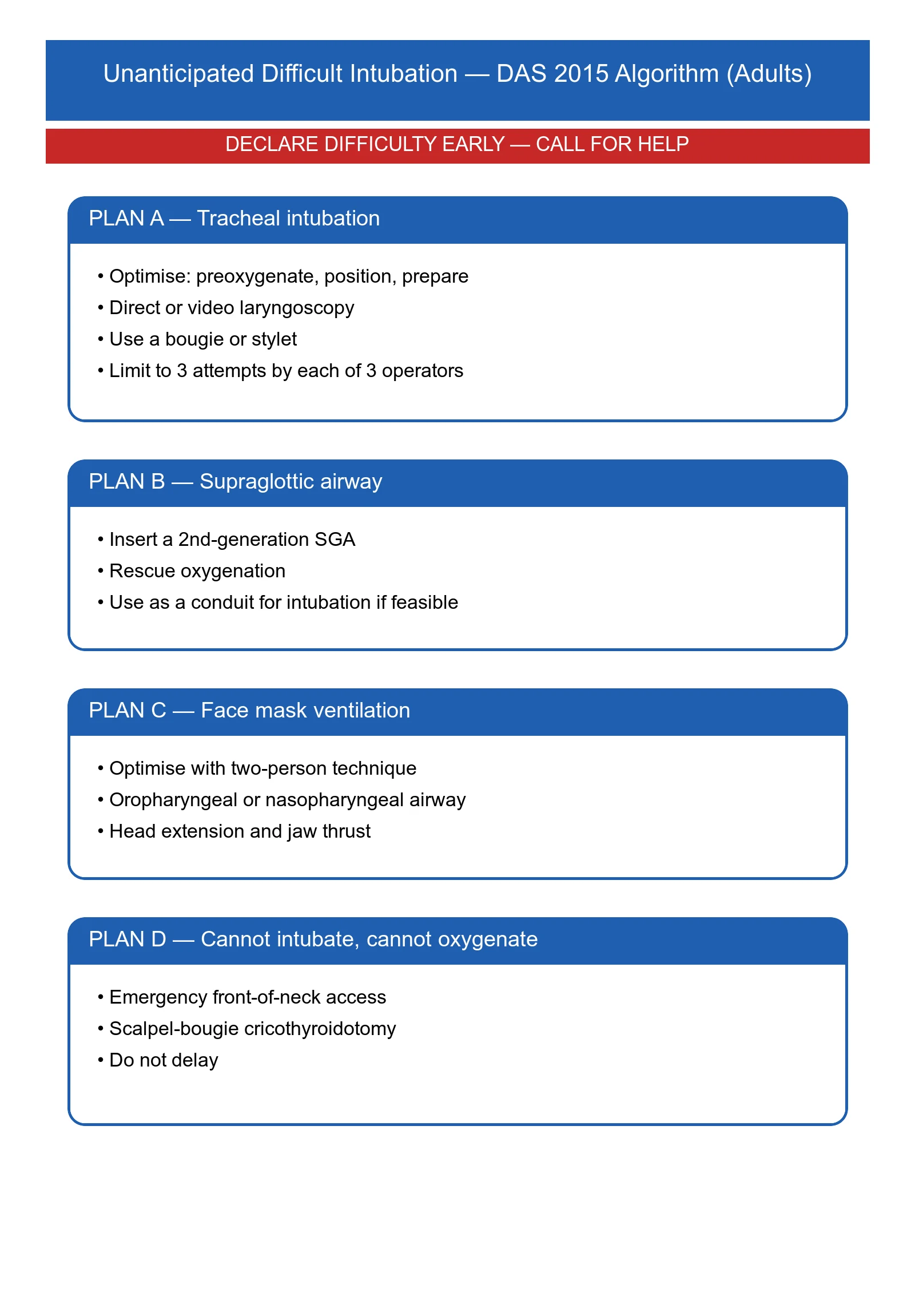
- [5]Frerk C, Mitchell VS, McNarry AF, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. British journal of anaesthesia, 2015.PMID 26556848
- [6]Cicardi M, Banerji A, Bracho F, et al. Icatibant, a new bradykinin-receptor antagonist, in hereditary angioedema. The New England journal of medicine, 2010.PMID 20818888
- [7]Sinert R, Levy P, Bernstein JA, et al. Randomized Trial of Icatibant for Angiotensin-Converting Enzyme Inhibitor-Induced Upper Airway Angioedema. The journal of allergy and clinical immunology. In practice, 2017.PMID 28552382
- [8]Feng IJ, Lin JW, Lai CC, et al. Comparative efficacies of various corticosteroids for preventing postextubation stridor and reintubation: a systematic review and network meta-analysis. Frontiers in medicine, 2023.PMID 37554508
- [9]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [10]Gluck EH, Onorato DJ, Castriotta R Helium-oxygen mixtures in intubated patients with status asthmaticus and respiratory acidosis. Chest, 1990.PMID 2118449