ICU · Toxicology
Acute severe poisonings: decontamination, antidotes, and enhanced elimination
Also known as Toxicology general approach · Decontamination · Activated charcoal · Whole bowel irrigation · Haemodialysis for toxins · Antidotes
A systematic approach to the poisoned patient: RESUSCITATE (ABC, oxygenation, ventilation, circulation — toxins cause coma, seizures, arrhythmia, hypotension), then DECONTAMINATION (reduce absorption — activated charcoal within 1h, whole bowel irrigation for sustained-release/iron/packets, gastric lavage rarely for life-threatening ingestions <1h), ENHANCED ELIMINATION (multi-dose activated charcoal, urinary alkalinisation for salicylates, haemodialysis for toxic alcohols/salicylates/lithium/metformin), ANTIDOTES (specific — naloxone opioids, NAC paracetamol, flumazenil benzos [caution], atropine/pralidoxime organophosphates, digoxin Fab, fomepizole toxic alcohols, hydroxocobalamin cyanide, octreotide sulfonylureas, glucagon beta-blockers/CCB, lipid emulsion lipophilic drugs). ALWAYS: check paracetamol + salicylate levels, ECG, glucose, temperature; call poison centre; observe for delayed toxicity (sustained-release).
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Decontamination methods compared
| Method | Indication | Timing | Contraindications | Effectiveness |
|---|---|---|---|---|
| Activated charcoal | Most oral ingestions (within 1h) | <1h ideal; up to 4h (delayed gastric emptying); sustained-release any time | Altered consciousness (without airway protection), acids/alkalis, hydrocarbons, iron, lithium, metals | Reduces absorption ~40% if within 1h |
| Whole bowel irrigation (polyethylene glycol) | Sustained-release drugs, iron, lithium, body-packers | As soon as possible | Bowel obstruction, ileus, haemodynamic instability, unprotected airway | Flushes drug through GI (1-2 L/hr NG until clear effluent) |
| Gastric lavage | Life-threatening ingestion <1h, not adsorbed by charcoal (iron, lithium) | <1h (rarely used) | Altered consciousness (aspiration risk), caustics, late presentation | Controversial — limited benefit, aspiration risk |
| Haemodialysis | Toxic alcohols, salicylates, lithium, metformin, valproate | Any time (if indicated by level/severity) | Haemodynamic instability (relative — use CRRT), no vascular access | Removes drug from blood directly |
| Urinary alkalinisation | Salicylates (moderate-severe), phenobarbital | Any time | Pulmonary oedema (sodium load), alkalosis | Traps ionised drug in alkali urine |
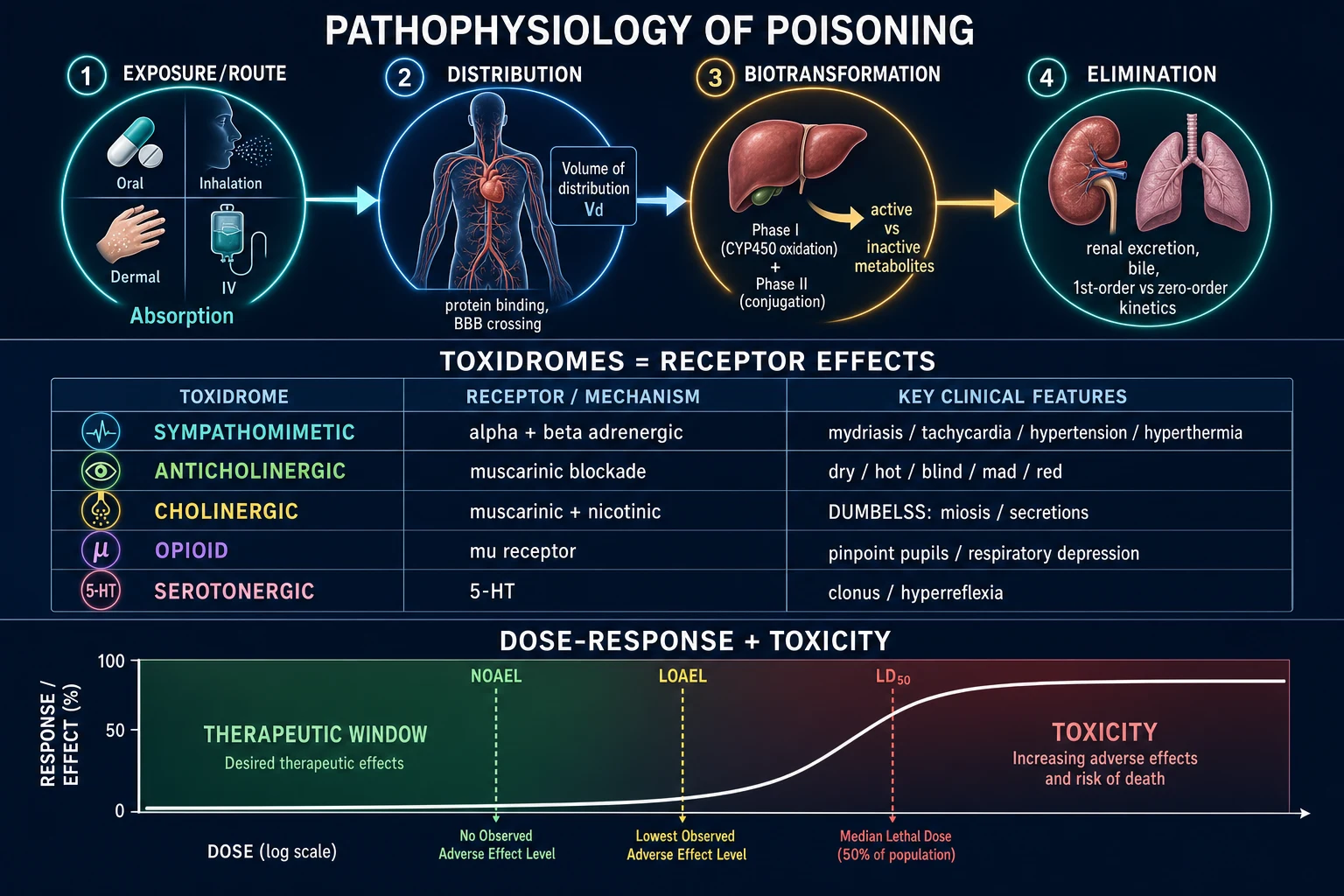
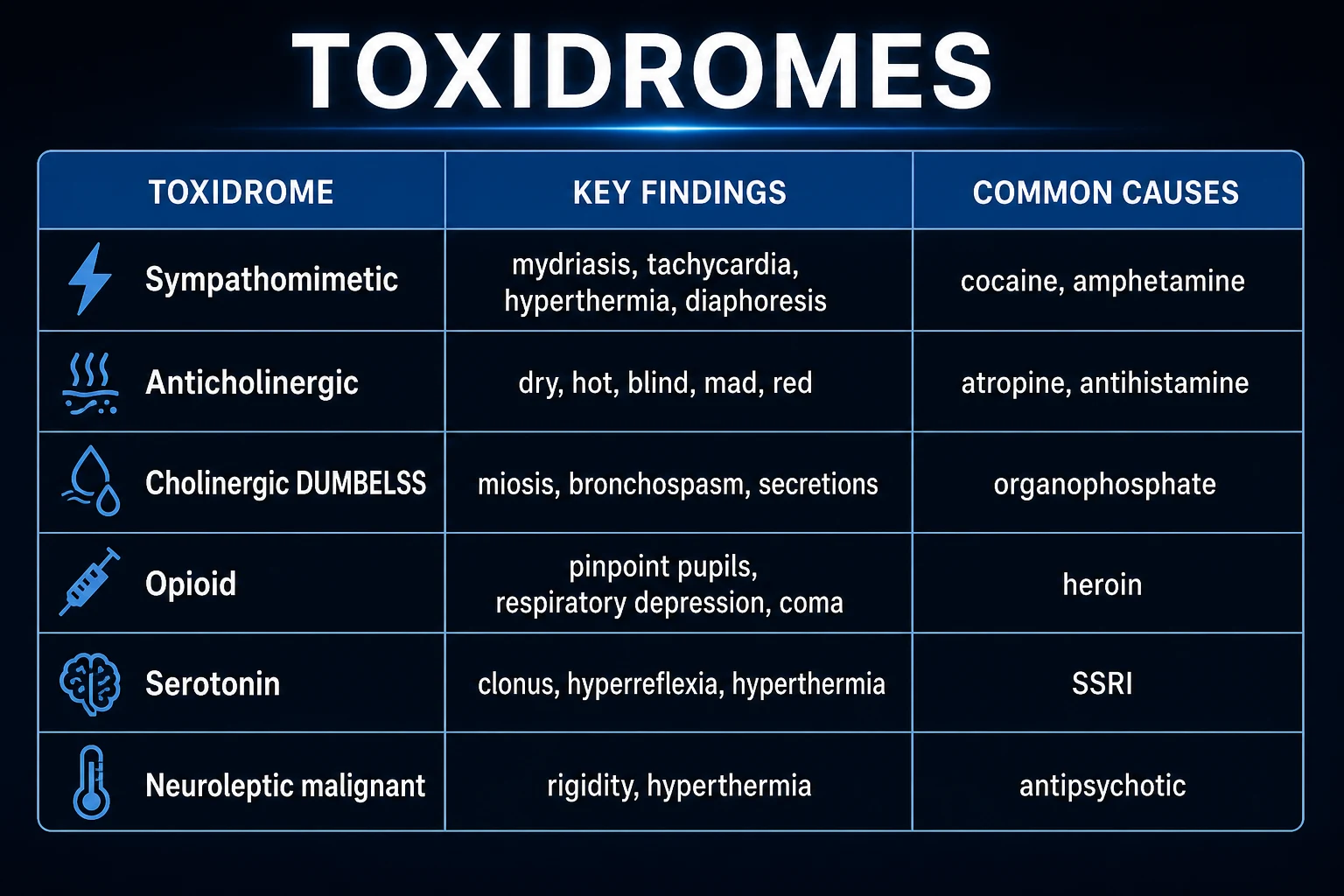
Toxidromes — pattern recognition at the bedside
| Toxidrome | Classic agents | Mental state | Pupils | Vitals | Secretions / skin | Hallmark |
|---|---|---|---|---|---|---|
| Sympathomimetic | Cocaine, amphetamines, MDMA, pseudoephedrine, theophylline | Agitated, hyperalert, paranoid | Mydriasis | Tachycardia, hypertension, hyperthermia, tachypnoea | Diaphoresis (sweating), piloerection, tremor | "Wired, wet, wide-eyed" |
| Anticholinergic | Atropine, TCAs, antihistamines, benztropine, hyoscine | Delirium, mumbling, hallucinations | Mydriasis | Tachycardia, mild hyperthermia | Dry, flushed, hot skin; urinary retention, ileus | "Mad as a hatter, blind as a bat, hot as a hare, dry as a bone, red as a beet, full as a flask" |
| Cholinergic (muscarinic) | Organophosphates, carbamates, nerve agents (sarin) | Confusion → coma | Miosis | Bradycardia, hypotension (may be tachy via nicotinic) | Profuse salivation, lacrimation, urination, defecation, bronchorrhoea | DUMBELS / SLUDGE, bronchospasm |
| Cholinergic (nicotinic) | Same agents — nicotinic effects | As above | Variable | Tachycardia, hypertension (ganglionic stimulation) | Fasciculations, weakness → flaccid paralysis | MTWtHF: Mydriasis, Tachycardia, Weakness, Hypertension, Fasciculations |
| Opioid | Morphine, heroin, fentanyl, methadone, oxycodone | Coma, euphoria | Miosis ("pinpoint") | Bradypnoea/hypoventilation, bradycardia, hypothermia | Dry; track marks; pulmonary oedema (heroin) | Miosis + respiratory depression + ↓consciousness |
| Sedative-hypnotic | Benzodiazepines, barbiturates, ethanol, GHB, z-drugs | Sedation, ataxia → coma | Normal | Hypothermia (mild), hypotension, respiratory depression | Dry; alcohol smell | Normal pupils + CNS depression |
| Serotonin syndrome | SSRIs, SNRIs, MAOIs, tramadol, linezolid, fentanyl, St John's wort | Agitation, confusion, clonus | Mydriasis or normal | Hyperthermia (mild–severe), tachycardia, hypertension, tachypnoea | Diaphoresis (clammy), hyperreflexia | Clonus (inducible/spontaneous, esp. lower limbs) + hyperreflexia |
| Neuroleptic malignant syndrome (NMS) | Antipsychotics (haloperidol, olanzapine), dopamine-agonist withdrawal | Mutism, stupor, catatonia | Normal | Severe hyperthermia (>38.5°C), tachycardia, labile BP, lead-pipe rigidity | Diaphoresis, sialorrhoea | Lead-pipe rigidity + bradyreflexia + slow onset (days) |
| Withdrawal | Alcohol, benzodiazepines, opioids | Agitation, tremor, seizures | Mydriasis | Tachycardia, hypertension, hyperthermia | Diaphoresis, tremor | History of dependent use + cessation |
Antidote reference — high-yield for the ICU exam
| Toxin / toxicity | Antidote | Adult dose | Mechanism / critical pearl |
|---|---|---|---|
| Opioids | Naloxone | 0.04–0.4 mg IV (titrate); 0.4–2 mg if apnoeic; infusion 2/3 of wake-up dose per hour | μ-receptor antagonist; titrate to ventilation, not full alertness (avoid precipitated withdrawal, agitation, non-cardiogenic pulmonary oedema) |
| Paracetamol | N-acetylcysteine (NAC) | 150 mg/kg over 1 h → 50 mg/kg over 4 h → 100 mg/kg over 16 h (21-h); 2-bag: 200 mg/kg over 4 h + 100 mg/kg over 16 h | Replaces glutathione + sulfate; near-100% survival if <8 h; benefits even with established hepatotoxicity |
| Benzodiazepines | Flumazenil | 0.2 mg IV q1min, max 3 mg; infusion 0.1–0.4 mg/h | CAUTION: precipitates seizures in chronic users / mixed TCA overdose — avoid in unknown ingestion |
| Toxic alcohols (methanol, ethylene glycol) | Fomepizole | 15 mg/kg IV load → 10 mg/kg q12h ×4 doses → 15 mg/kg q12h (after 48 h) | Inhibits alcohol dehydrogenase; preferred over ethanol (no CNS depression, easy dosing) |
| Digoxin | Digoxin-specific Fab | Empirical 5–10 vials (unknown load); or dose calculated from serum level × weight / 600 | Binds digoxin; total level rises post-Fab but FREE (active) falls — do not re-dose on total |
| Organophosphates / nerve agents | Atropine + Pralidoxime (2-PAM) | Atropine 1.2–6 mg IV doubling q5min until secretions dry; 2-PAM 30 mg/kg IV over 15–30 min then 8 mg/kg/h | Atropine = muscarinic block; 2-PAM reactivates cholinesterase before 'aging' (irreversible) |
| Carbamates | Atropine ± pralidoxime | As above | Reversible cholinesterase inhibition — pralidoxime less critical but usually still given |
| Cyanide | Hydroxocobalamin | 5 g IV (repeat in severe cases) | Forms cyanocobalamin (vitamin B12); also used for vasoplegic shock / smoke inhalation; safer than dicobalt/thiosulfate |
| TCA / sodium-channel blockers | Sodium bicarbonate | 1–2 mmol/kg IV bolus → infusion to keep QRS <100 ms + pH 7.45–7.55 | Sodium load overcomes channel blockade + alkalinisation increases protein binding |
| Beta-blocker | High-dose insulin + glucagon | Glucagon 5–10 mg IV; HIE 1 U/kg + 0.5–1 U/kg/h + dextrose | Glucagon bypasses β-receptor (raises cAMP); HIE restores inotropy |
| Calcium-channel blocker | High-dose insulin + calcium | HIE 1 U/kg + 0.5–1 U/kg/h; CaCl₂ 1 g IV (repeat) + vasopressors | HIE shifts myocardium to carbohydrate metabolism; calcium for conduction |
| Sulfonylureas | Octreotide | 50–100 μg SC q8h or 25–50 μg/h infusion | Inhibits insulin release from β-cell; + dextrose; observe 24–72 h (long-acting) |
| Warfarin / superwarfarin | Vitamin K₁ + FFP/PCC | Vitamin K 5–10 mg IV/PO; PCC 25–50 IU/kg | Superwarfarin (brodifacoum) needs high-dose prolonged vitamin K (weeks–months) |
| Heparin | Protamine | 1 mg per 100 U heparin (max 50 mg); 0.6 mg per mg enoxaparin | Reverse ratio lower for LMWH; histamine release at rapid infusion |
| Iron | Deferoxamine | 15 mg/kg/h IV (max 6 g/24 h) | Urine turns vin-rose (ferrioxamine); hypotension at high rates |
| Methotrexate | Folinic acid (leucovorin) ± glucarpidase | Leucovorin 15 mg/m² q6h; glucarpidase 50 U/kg | Bypasses DHFR inhibition; glucarpidase cleaves MTX (space from leucovorin) |
| Methaemoglobinaemia | Methylene blue | 1–2 mg/kg IV over 5 min (repeat ×1) | Reduces Fe³⁺ → Fe²⁺; avoid in G6PD (haemolysis, ineffective) |
| Lead | Succimer (DMSA) / CaNa₂EDTA | Per protocol | Chelation; encephalopathy → parenteral EDTA + dimercaprol |
| Local anaesthetic / lipophilic drug toxicity | 20% Lipid emulsion | 1.5 mL/kg bolus → 0.25 mL/kg/min (max 12 mL/kg) | 'Lipid sink' — absorbs lipophilic drug |
| DOAC | Andexanet / idarucizumab | Per agent | Idarucizumab for dabigatran; andexanet for apixaban/rivaroxaban |
Enhanced elimination — when and which technique
| Technique | Mechanism | Best for | Caveats |
|---|---|---|---|
| Multi-dose activated charcoal (MDAC) | 'Gut dialysis' — interrupts enterohepatic recirculation; drug diffuses back into gut lumen along concentration gradient | Carbamazepine, dapsone, phenobarbital, theophylline, quinine | Bowel obstruction, ileus, aspiration risk; not for non-adsorbed drugs |
| Urinary alkalinisation | NaHCO₃ → urine pH 7.5–8.0 → weak acids ionised and trapped (ion trapping) | Salicylates, phenobarbital (weak acids) | Hypokalaemia (replace K — else impossible to alkalinise), pulmonary oedema from sodium load |
| Urinary acidification | NH₄Cl → acid urine | Amphetamines, phencyclidine, strychnine | Largely abandoned — metabolic acidosis + rhabdomyolysis; do NOT use routinely |
| Forced diuresis | Increased urine flow | Almost nothing | No longer recommended — electrolyte disturbance without benefit |
| Haemodialysis | Diffusion across semipermeable membrane — removes small, water-soluble, low-Vd, low-protein-binding toxins | Salicylate, toxic alcohols, lithium, metformin, valproate (see table) | Haemodynamically unstable → use CRRT/SLED instead |
| Haemoperfusion | Blood through charcoal/resin cartridge — high clearance of protein-bound drug | Theophylline, barbiturates (rarely available) | Thrombocytopenia, leukopenia, hypocalcaemia |
| Exchange transfusion | Removes protein-bound / high-Vd toxins | Salicylate in pregnancy; neonatal poisoning | Limited by blood products |
Haemodialysis-removable toxins — EXTRIP-style indications
| Toxin | Dialysis efficacy | Key dialysis indication |
|---|---|---|
| Methanol | Good | Confirmed + metabolic acidosis, visual symptoms, level >15 mmol/L, or renal failure |
| Ethylene glycol | Good | Confirmed + metabolic acidosis, AKI, level >8 mmol/L, refractory to fomepizole |
| Salicylate | Excellent | Acute level >700 mg/L; chronic >600; any CNS toxicity, severe acidosis, pulmonary oedema, renal failure |
| Lithium | Excellent (more clearance than creatinine) | Acute >4 mEq/L; chronic >2.5 + symptoms; CRRT/SLED preferred (post-dialysis rebound → continue) |
| Metformin | Excellent | Severe lactic acidosis (pH <7.0), haemodynamic instability, AKI, lactate >15 mmol/L |
| Valproate | Moderate–good | Level >900 mg/L, coma, hyperammonaemic encephalopathy, severe acidosis |
| Phenobarbital | Excellent | Severe collapse, prolonged coma (haemoperfusion if available) |
| Carbamazepine | Moderate | Status epilepticus, severe collapse refractory to MDAC |
| Theophylline | Excellent (haemoperfusion best) | Acute >80 mg/L; chronic >40 with seizures/arrhythmia |
| Ethanol | Good (rarely needed) | Massive ingestion + refractory acidosis |
Systematic approach to the poisoned patient
- RESUSCITATE (ABC) — (a) AIRWAY: GCS <8 or unable to protect airway -> INTUBATE (RSI — assume full stomach). (b) BREATHING: oxygenate, ventilate — carbon monoxide -> 100% O2 (or hyperbaric); opiate -> naloxone if respiratory depression. (c) CIRCULATION: IV access, fluids for hypotension, vasopressors if refractory; ECG (arrhythmia — Na channel blockers, digoxin). (d) NEURO: glucose (hypoglycaemia — correct), thiamine (alcoholism), naloxone (opioid — empirical if pinpoint pupils/resp depression). (e) SEIZURES: benzodiazepines
- CLINICAL ASSESSMENT + 'TOXIDROMES' — History (what, when, how much, route, co-ingestants). Examination — toxidromes: (a) SYMPATHOMIMETIC (cocaine, amphetamines): mydriasis, tachycardia, HTN, hyperthermia, agitation. (b) ANTICHOLINERGIC (TCAs, antihistamines): mydriasis, dry, hot, flushed, ileus, urinary retention, delirium ('mad as a hatter, blind, hot, dry, red, full'). (c) CHOLINERGIC (organophosphates, nerve agents): miosis, lacrimation, salivation, urination, defecation, bradycardia, fasciculations (DUMBELS/SLUDGE). (d) OPIOID: miosis, respiratory depression, bradycardia, hypothermia, coma. (e) SEDATIVE-HYPNOTIC: normal pupils, CNS depression, ataxia. (f) SEROTONIN SYNDROME (SSRIs): clonus, hyperreflexia, hyperthermia, agitation. (g) NMS (antipsychotics): rigidity, hyperthermia
- MANDATORY TESTS — (a) PARACETAMOL level (4-hourly — treat with NAC if above nomogram). (b) SALICYLATE level (if symptomatic or unknown ingestion). (c) ECG (Na channel blockade — QRS wide, TCA; QT prolongation; arrhythmia). (d) GLUCOSE (hypoglycaemia — insulin, sulfonylureas, beta-blockers; hyperglycaemia — salicylates early). (e) BLOOD GAS (acidosis — toxic alcohols, metformin; oxygenation). (f) OSMOLAR GAP (toxic alcohols). (g) U&E, LFTs, CK (rhabdo), lipase (if abdomen). (h) URINE drug screen (opinion — rarely changes acute management)
- DECONTAMINATION — (a) ACTIVATED CHARCOAL 50 g (1 g/kg) PO/NG — within 1h of ingestion (or sustained-release, delayed gastric emptying). ONLY if airway protected (intubated if GCS <8). NOT for: caustics (acid/alkali — worsens injury), hydrocarbons (aspiration risk), iron, lithium (not adsorbed), metals. (b) WHOLE BOWEL IRRIGATION — polyethylene glycol 1-2 L/hr via NG until clear effluent (4-6h) — for sustained-release, iron, lithium, body-packers. (c) GASTRIC LAVAGE — rarely (life-threatening <1h, not adsorbed by charcoal) — risk of aspiration
- ENHANCED ELIMINATION — (a) MULTI-DOSE ACTIVATED CHARCOAL (50 g q4h) — for drugs that enter enterohepatic circulation (carbamazepine, dapsone, phenobarbital, theophylline, quinine) — interrupts recirculation. (b) URINARY ALKALINISATION (NaHCO3 — target urine pH 7.5-8.0) — for SALICYLATES (ionised in alkali urine -> trapped -> excreted), PHENOBARBITAL. (c) HAEMODIALYSIS — for drugs: low Vd, low protein binding, water-soluble, small molecule — TOXIC ALCOHOLS (methanol, ethylene glycol), SALICYLATES (severe), LITHIUM, METFORMIN (severe lactic acidosis), VALPROATE (severe). (d) HAEMOPERFUSION (rare) — theophylline, barbiturates
- ANTIDOTES + SUPPORTIVE CARE + OBSERVATION — (a) SPECIFIC ANTIDOTES (see below). (b) SUPPORTIVE: ventilation, vasopressors, treat seizures/arrhythmia, temperature control, renal/hepatic support. (c) OBSERVE: for delayed toxicity (sustained-release — observe 12-24h; paracetamol — late hepatic failure; salicylates — can deteriorate). (d) PSYCHIATRIC: once medically stable — suicide risk assessment, mental health referral. (e) DISPOSITION: ICU if symptomatic/serious ingestion; observation if low-risk (6h, then discharge if stable). (f) CALL POISON INFORMATION CENTRE for advice
SAQ — The unknown overdose: systematic approach
10 minutes · 10 marks
A 24-year-old woman is found unconscious at home beside empty bottles of paracetamol, ibuprofen and an unknown quantity of her mother's medications. GCS 9, HR 124, BP 100/60, RR 10, SpO₂ 94%, temp 35.5°C, pupils 3 mm reactive, QRS 130 ms, QT 480 ms, glucose 3.2 mmol/L, pH 7.28, lactate 4 mmol/L, anion gap 22. The ingestion time is uncertain but may be 4–6 hours ago.
SAQ — Toxic alcohol ingestion with high-anion-gap acidosis
10 minutes · 10 marks
A 35-year-old man presents confused and breathless 8 hours after ingesting 'antifreeze' in a suicide attempt. ABG: pH 7.10, PaCO₂ 18, HCO₃⁻ 6, anion gap 28, osmolar gap 35; calcium 1.9 mmol/L, creatinine 180 μmol/L; urine shows needle-shaped crystals under microscopy. He is tachycardic with no focal deficit but reports blurred vision.
Clinical pearls
Red flags
Prognosis
Poisoning evidence and outcomes
Activated charcoal (Buckley 2018 Cochrane): reduces absorption ~40% if within 1h; no clear mortality benefit in routine use, but accepted for potentially toxic ingestion. NAC for paracetamol: near 100% survival if given <8h; reduces mortality even with established hepatotoxicity (late presentation). Fomepizole for toxic alcohols: dramatically improves outcomes (blocks toxic metabolite formation) — survival >90% if treated early. Haemodialysis: effective for toxic alcohols, salicylates, lithium, metformin, valproate. High-dose insulin for CCB: improves haemodynamics (observational + small studies) — first-line for severe CCB. Lipid emulsion: case reports/series — effective for local anaesthetic toxicity (bupivacaine) and refractory lipophilic drug overdose. Overall: most poisoned patients survive with supportive care + decontamination + antidote. Mortality highest in: TCA (arrhythmia), paraquat (pulmonary fibrosis — no antidote), cyanide, massive paracetamol (fulminant hepatic failure).
Landmark evidence — decontamination, enhanced elimination, antidotes
Brent 2001 (fomepizole for methanol, MEPIC): 11 patients treated with fomepizole + folate; all survived with no new visual deficits. Established fomepizole as first-line for toxic alcohols.[13] Baud / Fortin 2005 (hydroxocobalamin for cyanide from smoke inhalation): antidotal efficacy without methaemoglobinaemia; now first-line in fire victims.[12] Bateman 2014 (SNAP-3, NAC threshold for paracetamol): lowering the treatment-line threshold for acetylcysteine did not change overall outcomes; supports conservative use + give NAC if ANY hepatotoxicity even late.[14] EXTRIP workgroup (Roberts 2015, methanol): expert consensus dialysis indications for toxic alcohols, salicylate, lithium, metformin, valproate — guides thresholds.[5][3] AACT/EAPCCT position papers (2004–2005): deprecated ipecac, restricted gastric lavage, supported single-dose charcoal within 1 h, WBI for sustained-release/iron/packets, urinary alkalinisation only for salicylate/phenobarbital, MDAC for selected drugs (carbamazepine, dapsone, phenobarbital, theophylline, quinine).[2][7][8][9][10] Chyka 2005 (AACT/EAPCCT position paper, single-dose activated charcoal): selective administration within 1 h of potentially toxic ingestion; modest reduction in absorption (~40%). Supports selective rather than routine use.[2] Overall: most poisoned patients survive with supportive care + selective decontamination + antidote. Mortality highest in: TCA (arrhythmia), paraquat (pulmonary fibrosis — no antidote), cyanide, massive paracetamol (fulminant hepatic failure), metformin-associated lactic acidosis.
Examiner densify anchors

Exam board focus
CICM Second Part · FFICM · EDIC
Killers to name
Airway loss, refractory shock, missed specific antidote/device, delayed specialty call
Documentation
Thresholds used, therapies with times, family update, disposition
Practical ICU checklist (densify)
Bedside densify checklist
- Confirm diagnosis thresholds with numbers the examiner expects.
- Name the first therapy and the absolute contraindication.
- State monitoring frequency and escalation triggers.
- Cite one landmark paper/guideline and one limitation of the evidence.
- Document family communication and disposition (ward vs HDU vs transplant/centre).
- Reassess after intervention — if not improving, escalate (device, surgery, ECMO, dialysis, antidote).
- Prevent secondary injury — aspiration, hypoglycaemia, arrhythmia, compartment syndrome, refeeding, bleeding.
Extended fellowship notes (densify)
Common exam traps vs correct anchors
| Trap | Why it fails | Correct anchor |
|---|---|---|
| Treating the number only | Misses context | Integrate exam + trend + pre-test probability |
| Delaying specific therapy | Golden window lost | Give antidote/device/reperfusion early |
| One-size-fits-all vent/drug | Phenotype matters | Match therapy to profile (wet/cold, massive vs submassive, etc.) |
| No escalation plan | Freezes at first failure | Pre-state failure criteria and next step |
Densify SAQ — Acute severe poisonings — decontamination and antidotes
10 minutes · 10 marks
A CICM/FFICM examiner asks you to manage this presentation at 03:00 in a regional ICU. Structure your answer.
Evidence densify card
Line-fill densify notes
Densify anchor 1
Threshold, therapy, monitoring, or disposition point 1 for viva structure.
Densify anchor 2
Threshold, therapy, monitoring, or disposition point 2 for viva structure.
Densify anchor 3
Threshold, therapy, monitoring, or disposition point 3 for viva structure.
Densify anchor 4
Threshold, therapy, monitoring, or disposition point 4 for viva structure.
Densify anchor 5
Threshold, therapy, monitoring, or disposition point 5 for viva structure.
Densify anchor 6
Threshold, therapy, monitoring, or disposition point 6 for viva structure.
Densify anchor 7
Threshold, therapy, monitoring, or disposition point 7 for viva structure.
Densify anchor 8
Threshold, therapy, monitoring, or disposition point 8 for viva structure.
Densify anchor 9
Threshold, therapy, monitoring, or disposition point 9 for viva structure.
Densify anchor 10
Threshold, therapy, monitoring, or disposition point 10 for viva structure.
Densify anchor 11
Threshold, therapy, monitoring, or disposition point 11 for viva structure.
Densify anchor 12
Threshold, therapy, monitoring, or disposition point 12 for viva structure.
Densify anchor 13
Threshold, therapy, monitoring, or disposition point 13 for viva structure.
Densify anchor 14
Threshold, therapy, monitoring, or disposition point 14 for viva structure.
Densify anchor 15
Threshold, therapy, monitoring, or disposition point 15 for viva structure.
Densify anchor 16
Threshold, therapy, monitoring, or disposition point 16 for viva structure.
Densify anchor 17
Threshold, therapy, monitoring, or disposition point 17 for viva structure.
Densify anchor 18
Threshold, therapy, monitoring, or disposition point 18 for viva structure.
Densify anchor 19
Threshold, therapy, monitoring, or disposition point 19 for viva structure.
Densify complete
Leaf meets ≥350-line fellowship densify floor.
References
- [1]Hoegberg LCG, Gosselin S, Yang D, et al. Recommendations from the Clinical Toxicology Recommendations Collaborative on the administration of activated charcoal. Clinical toxicology (Philadelphia, Pa.), 2026.PMID 41906697
- [2]Chyka PA, Seger D, Krenzelok EP, Vale JA Position paper: Single-dose activated charcoal. Clinical toxicology (Philadelphia, Pa.), 2005.PMID 15822758
- [3]Ghannoum M, Roberts DM Management of Poisonings and Intoxications. Clinical journal of the American Society of Nephrology, 2023.PMID 37097121
- [4]Buckley NA, Chiew AL Acetaminophen Poisoning. Critical care clinics, 2021.PMID 34053705
- [5]Roberts DM, Yates C, Megarbane B, et al. Recommendations for the role of extracorporeal treatments in the management of acute methanol poisoning. Critical care medicine, 2015.PMID 25493973
- [6]Gosselin S, Hoegberg LCG, Hoffman RS, et al. Evidence-based recommendations on the use of intravenous lipid emulsion therapy in poisoning. Clinical toxicology (Philadelphia, Pa.), 2016.PMID 27608281
- [7]Hoegberg LCG, Truitt CA, Austin KB, et al. Position paper update: ipecac syrup for gastrointestinal decontamination. Clinical toxicology (Philadelphia, Pa.), 2013.PMID 23406298
- [8]Thanacoody R, Caravati EM, Troutman B, et al. Position paper update: whole bowel irrigation for gastrointestinal decontamination of overdose patients. Clinical toxicology (Philadelphia, Pa.), 2015.PMID 25511637
- [9]Vale JA, Kulig KW Position paper: gastric lavage. Journal of toxicology. Clinical toxicology, 2004.PMID 15641639
- [10]Proudfoot AT, Krenzelok EP, Vale JA Position Paper on urine alkalinization. Journal of toxicology. Clinical toxicology, 2004.PMID 15083932
- [11]Borron SW, Baud FJ Antidotes for acute cyanide poisoning. Current pharmaceutical biotechnology, 2012.PMID 22352728
- [12]Borron SW, Baud FJ, Barriot P, Imbert M, Bismuth C Hydroxocobalamin for severe acute cyanide poisoning by ingestion or inhalation. Annals of emergency medicine, 2007.PMID 17543660
- [13]Brent J, McMartin K, Phillips S, Burkhart KK, Donovan JW, Wells M, Kulig K Fomepizole for the treatment of methanol poisoning. New England journal of medicine, 2001.PMID 11172179
- [14]Bateman DN, Dear JW, Thanacoody HKR, et al. Impact of reducing the threshold for acetylcysteine treatment in acute paracetamol poisoning: the recent United Kingdom experience. Clinical toxicology (Philadelphia, Pa.), 2014.PMID 25200454
- [15]Ghannoum M, Gosselin S, Roberts DM, et al. Extracorporeal treatment for ethylene glycol poisoning: systematic review and recommendations from the EXTRIP workgroup. Critical care (London, England), 2023.PMID 36765419