ICU · toxicology
Acute Lithium Toxicity — Comprehensive ICU Management
Also known as Lithium poisoning · Lithium toxicity · Lithium intoxication · SILENT · Syndrome of irreversible lithium-effectuated neurotoxicity · Narrow therapeutic index · Whole bowel irrigation lithium · Lithium haemodialysis
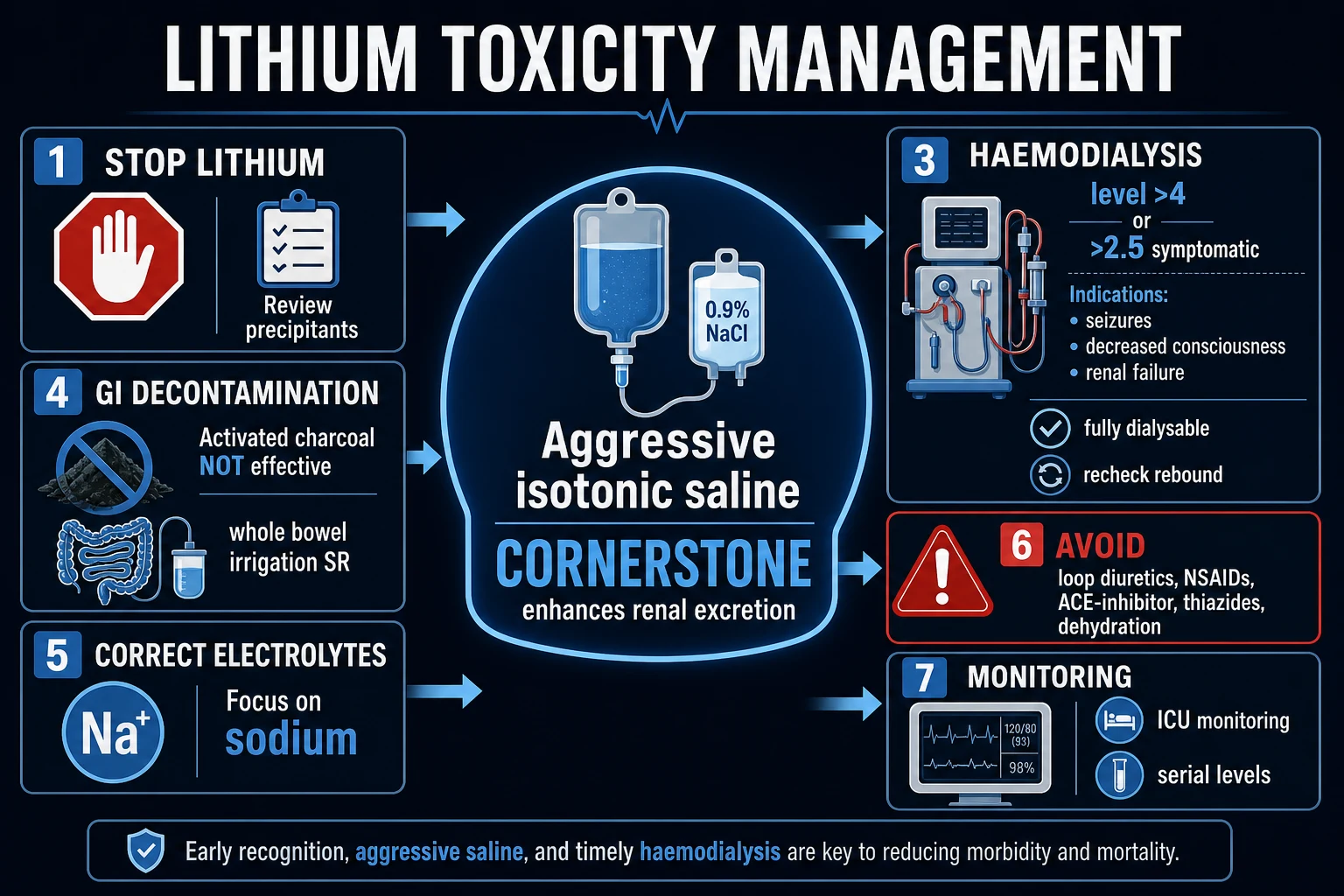
Acute and chronic lithium toxicity — the narrowest therapeutic index in psychiatry (therapeutic 0.6-1.2 mmol/L; toxicity 1.5; severe 2.5). Lithium is freely filtered at the glomerulus and reabsorbed in the PROXIMAL tubule via the SAME pathway as sodium — so dehydration, salt depletion, renal failure, thiazides, NSAIDs and ACE inhibitors all increase proximal Li reabsorption → toxicity. ACUTE overdose: primarily GI (nausea, vomiting, diarrhoea) with delayed neurological features as Li distributes into the CNS. CHRONIC toxicity: NEUROLOGICAL — coarse tremor, hyperreflexia, ataxia, nystagmus, fasciculations, seizures, coma, and the syndrome of irreversible lithium-effectuated neurotoxicity (SILENT). Management: STOP lithium + aggressive IV 0.9% normal saline (enhances Li excretion by increasing proximal tubule Na delivery → reduces Li reabsorption) + haemodialysis for level 4 acute or 2.5 chronic with severe neurology/renal failure (Li is small, water-soluble, no protein binding → easily dialysed BUT rebound occurs). AVOID thiazides and NSAIDs. Monitor Li level q4-6h.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview

Pharmacology — why lithium is so dangerous
Lithium (Li⁺, atomic weight 7) is the lightest alkali metal and a monovalent cation. As a mood stabiliser it remains first-line for bipolar affective disorder (prophylaxis of mania and depression, augmentation in refractory depression, reduction of suicide risk). Three pharmacological properties make it uniquely dangerous in the ICU:[3][6]
-
The narrowest therapeutic index in psychiatry. The therapeutic window is 0.6-1.2 mmol/L (some units target 0.6-0.8 for maintenance, 0.8-1.0 for acute mania). Toxicity appears above 1.5 mmol/L and is severe above 2.5 mmol/L. A patient can sit at 0.8 (therapeutic) and be pushed to 2.0 (toxic) by an intercurrent illness or a single interacting drug — there is almost no margin for error.[1]
-
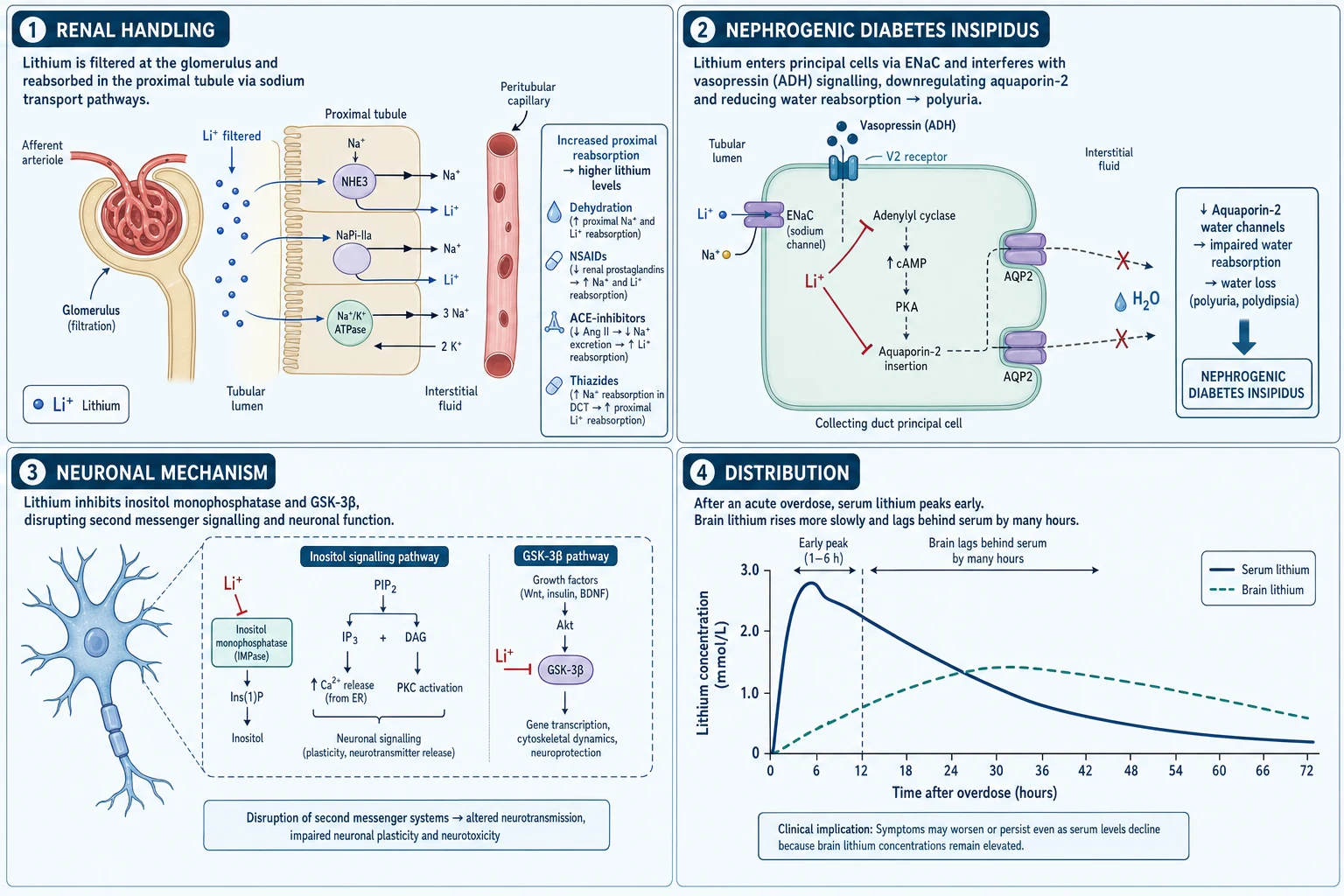
It is handled by the kidney exactly like sodium. Lithium is freely filtered at the glomerulus. Approximately 80% of the filtered load is then reabsorbed in the proximal tubule through the same transport pathways that handle sodium (the proximal tubule Na⁺/H⁺ exchanger, and paracellular reabsorption driven by the electrochemical gradient established by basolateral Na⁺/K⁺-ATPase). The critical implication: any state that increases proximal sodium reabsorption also increases lithium reabsorption. Volume depletion, dehydration, sodium restriction, renal hypoperfusion, heart failure, diuretic-induced natriuresis (with downstream sodium avidity), and NSAID/ACE-inhibitor effects on renal haemodynamics all preferentially retain lithium and precipitate toxicity.[2][3]
-
It distributes widely and is eliminated slowly. Lithium has a large volume of distribution (Vd ≈ 0.6-0.9 L/kg) — it distributes into total body water and is taken up slowly into cells, especially in the brain (intracellular accumulation underlies its neurotoxicity and the delayed onset of chronic toxicity). It has zero protein binding and is eliminated almost entirely by the kidney (renal clearance ≈ GFR of lithium). The elimination half-life is long — 18-24 h in normal renal function, and up to 40-50 h in renal failure or the elderly. This slow elimination means that even after haemodialysis acutely lowers the serum level, tissue stores (especially the brain) leach lithium back into the blood → the rebound phenomenon.[2][5]
The downstream toxicity of intracellular lithium is pleiotropic: it substitutes for sodium in voltage-sensitive ion channels and the Na⁺/K⁺-ATPase, inhibits inositol monophosphatase (depleting intracellular inositol and disrupting phospholipase-C second-messenger signalling), interferes with GSK-3β and cyclic AMP signalling, and at toxic concentrations disrupts cellular energy metabolism. Clinically this translates into neurological, gastrointestinal, renal, endocrine and cardiovascular effects.[1][6]
Acute overdose versus chronic toxicity — the critical distinction
The single most important clinical judgement in suspected lithium toxicity is distinguishing acute overdose from chronic (acute-on-chronic) accumulation. They differ in onset, organ dominance, severity, and the meaning of the serum level.[2][4]
Acute overdose — a single large ingestion (typically deliberate self-harm, or accidental in a child). Lithium is still predominantly in the vascular and interstitial compartment early. The dominant early features are gastrointestinal: nausea, vomiting, diarrhoea (lithium irritates the gastric mucosa and is a cholinergic stimulus). Neurological features are initially mild or absent because the serum lithium has not yet distributed into the brain — they appear 6-12 h later as distribution proceeds. The serum level rises early and peaks late. Prognosis is relatively favourable because the brain concentration rises slowly and dialysis can intercept it.[2]
Chronic toxicity (and acute-on-chronic) — gradual accumulation from reduced renal clearance. The precipitants are anything that increases proximal lithium reabsorption or reduces GFR: dehydration (gastroenteritis, hot weather, fever, inadequate intake), renal failure, sodium restriction, thiazide diuretics (increase proximal Na reabsorption by blocking distal Na reabsorption → volume depletion → proximal Na/Li avidity), loop diuretics (similar, but less potent), NSAIDs (reduce renal prostaglandins → afferent arteriolar vasoconstriction → reduced GFR and increased Li reabsorption), ACE inhibitors/ARBs (efferent arteriolar dilatation → reduced GFR), and drug interactions raising lithium levels. The clinical picture is neurologically dominant and far more dangerous because the brain concentration is already high. The serum level correlates POORLY with the severity of chronic neurotoxicity — a patient with a "moderate" level of 2.0 mmol/L may be in coma from chronic tissue saturation. Chronic toxicity carries the risk of SILENT (see below).[1][4]
[3]Clinical features
The clinical features of lithium toxicity span multiple systems, but the neurological manifestations dominate and determine prognosis.[1][4]
- Central nervous system (the dominant system): fine tremor progressing to coarse tremor, hyperreflexia, ataxia, nystagmus, muscle fasciculations, myoclonus, dysarthria, confusion/delirium, seizures, coma. The tremor is action/postural. The progression fine → coarse tremor → fasciculations/myoclonus → seizures → coma is the classic sequence of worsening. Upper motor neuron signs (extensor plantar responses) may appear. A parkinsonian or extrapyramidal picture can occur, and is a clue to SILENT.
- Gastrointestinal (dominant in acute overdose early): nausea, vomiting, diarrhoea, abdominal pain. May be the first sign.
- Renal: nephrogenic diabetes insipidus (lithium down-regulates aquaporin-2 → resistance to ADH → polyuria/polydipsia), sodium-losing nephropathy, chronic interstitial nephritis (with long-term therapy). The polyuria worsens dehydration → worsens toxicity — a vicious cycle.
- Endocrine: hypothyroidism (lithium inhibits thyroid hormone release), hypercalcaemia (lithium raises parathyroid hormone and serum calcium).
- Cardiovascular: ECG changes (T-wave flattening/inversion, QT prolongation), bradycardia, hypotension (in severe toxicity). Less prominent than neurological features.
- Metabolic: hyperthermia (uncommon — distinguish from NMS/serotonin syndrome), leukocytosis.
SILENT — Syndrome of Irreversible Lithium-Effectuated Neurotoxicity. The most feared complication: irreversible cerebellar and brainstem dysfunction (ataxia, dysarthria, nystagmus, extrapyramidal/parkinsonian features, dementia, cognitive impairment) that persists or worsens despite normalisation of the serum lithium level. It arises after severe or prolonged toxicity, typically chronic, and reflects structural neuronal damage from prolonged intracellular lithium. There is no specific treatment beyond prevention — early, aggressive clearance (fluids, dialysis) before irreversible neuronal injury is the only defence.[1][2]
Investigations and monitoring
- Serum lithium level: the cornerstone. Draw a level on presentation and repeat serially every 4-6 h until the level is falling and the patient is neurologically stable. In acute overdose, the level is misleading early (Li still distributing) — always repeat. Therapeutic 0.6-1.2; toxic >1.5; severe >2.5; very severe >3.5-4.0. Use a TEDTA (lithium-heparin) tube is NOT acceptable — use a plain/serum tube; check local lab policy. Crucially, in chronic toxicity the level does not correlate well with severity — treat the patient, not the number.[2]
- Renal function (urea, creatinine, eGFR): lithium is renally cleared and renal impairment both causes and results from toxicity. AKI is a strong indication for dialysis.
- Electrolytes: sodium (hyponatraemia worsens Li retention), potassium, magnesium, calcium (lithium can cause hypercalcaemia), glucose.
- Thyroid function: lithium causes hypothyroidism — check TSH.
- ECG: QT prolongation, T-wave changes, bradyarrhythmias.
- Venous gas / lactate: assess for acidosis (worsens Li distribution to brain).
- Serum osmolality and urine osmolality: assess for nephrogenic diabetes insipidus (inappropriately dilute urine despite high osmolality / dehydration).
- Paracetamol and salicylate levels: rule out co-ingestion in deliberate self-harm.
- CT brain: if there is altered consciousness, seizures, or focal signs — to exclude alternative diagnoses (lithium itself does not have a specific CT signature, though chronic toxicity may show cerebellar atrophy).
Management
SAQ — Chronic lithium toxicity requiring haemodialysis
10 minutes · 10 marks
A 62-year-old woman on long-term lithium carbonate for bipolar affective disorder is brought to the emergency department after four days of gastroenteritis and poor oral intake. She is confused, with a coarse action tremor, ataxia and widespread muscle fasciculations; GCS 12. Serum lithium 3.2 mmol/L, creatinine 190 micromol/L, sodium 128 mmol/L. Her regular medications include a thiazide diuretic.
Clinical pearls
Red flags
Prognosis
[5]The strongest predictors of a poor outcome are chronic (rather than acute) toxicity, delayed clearance/dialysis, renal failure, old age, and severe neurological involvement (seizures, coma) — all of which increase the risk of SILENT. The single most important determinant of recovery is how quickly the serum and brain lithium concentrations are reduced below the toxic threshold: aggressive fluids and early, adequate (and continuous/repeated) dialysis are protective.[1][2][4]
Key trials and evidence
Baird-Gunning 2017 — Lithium Poisoning (PMID 27516079)
McKnight 2012 — Lithium toxicity profile: systematic review and meta-analysis (PMID 22265699)
Beckmann/Oakley 2001 — Continuous venovenous haemodialysis in severe lithium toxicity (PMID 11527234)
Densification notes for fellowship revision
This leaf is densified to the ICU fellowship gate standard (CICM / FFICM / EDIC): embedded SAQ practice, multi-figure visual scaffolding, examiner map alignment, and MCQ coverage of definition, mechanism, first-hour management, evidence, and traps.
[1]- Revision checkpoint 1: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 2: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 3: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 4: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 5: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 6: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 7: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 8: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
References
- [1]Gitlin M Lithium side effects and toxicity: prevalence and management strategies. Int J Bipolar Disord, 2016.PMID 27900734
- [2]Baird-Gunning J, et al. Lithium Poisoning. J Intensive Care Med, 2017.PMID 27516079
- [3]Amdisen A Serum level monitoring and clinical pharmacokinetics of lithium. Clin Pharmacokinet, 1977.PMID 324690
- [4]Hansen HE, Amdisen A Lithium intoxication. (Report of 23 cases and review of 100 cases from the literature). Q J Med, 1978.PMID 356084
- [5]Beckmann U, et al. Efficacy of continuous venovenous hemodialysis in the treatment of severe lithium toxicity. J Toxicol Clin Toxicol, 2001.PMID 11527234
- [6]McKnight RF, et al. Lithium toxicity profile: a systematic review and meta-analysis. Lancet, 2012.PMID 22265699