ICU · toxicology
Acute Methanol and Ethylene Glycol Poisoning — Comprehensive ICU Management
Also known as Methanol poisoning · Ethylene glycol poisoning · Toxic alcohols · Fomepizole · 4-methylpyrazole · Formic acid toxicity · Calcium oxalate crystals · Osmolar gap · Anion gap acidosis · Wood alcohol · Antifreeze poisoning
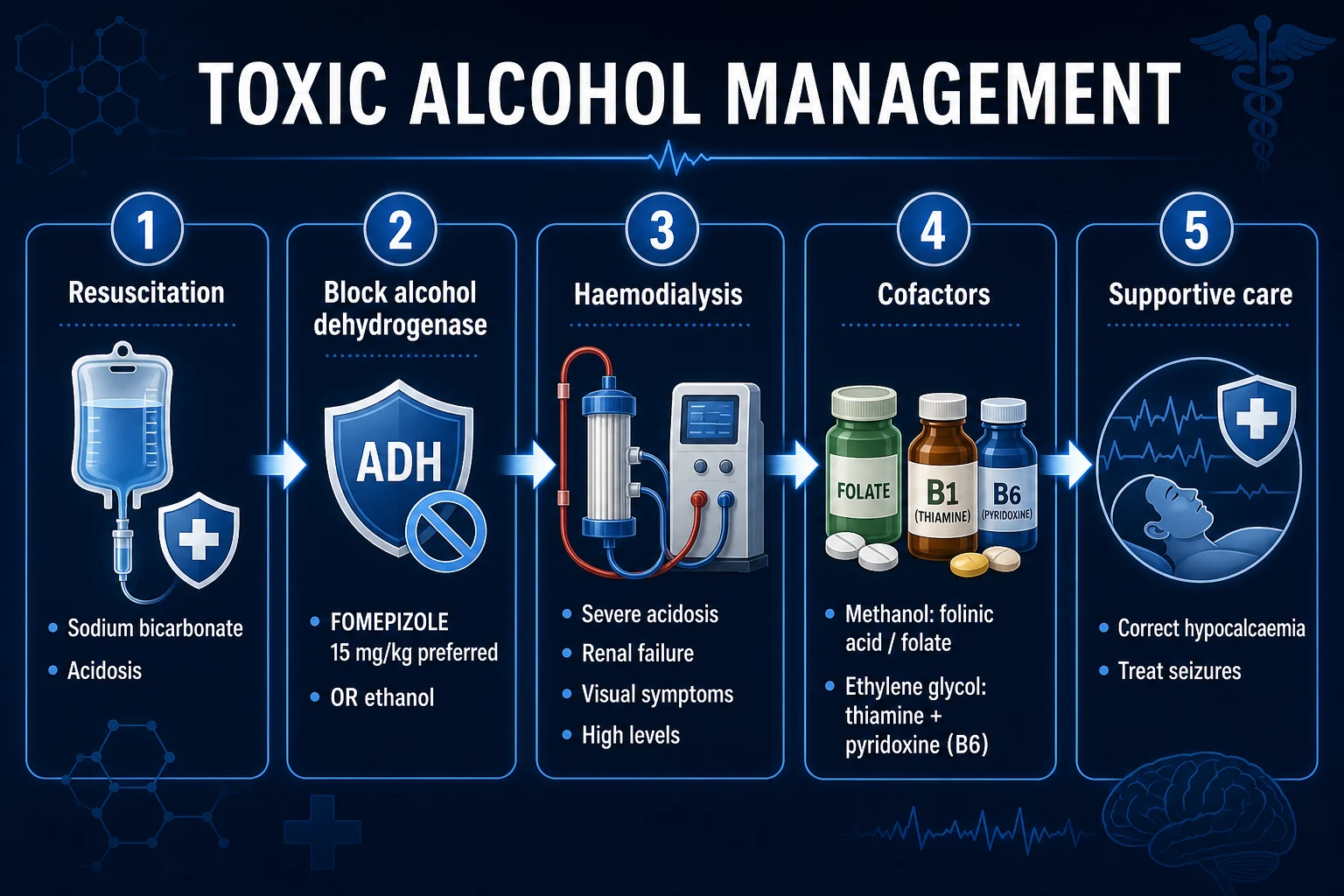
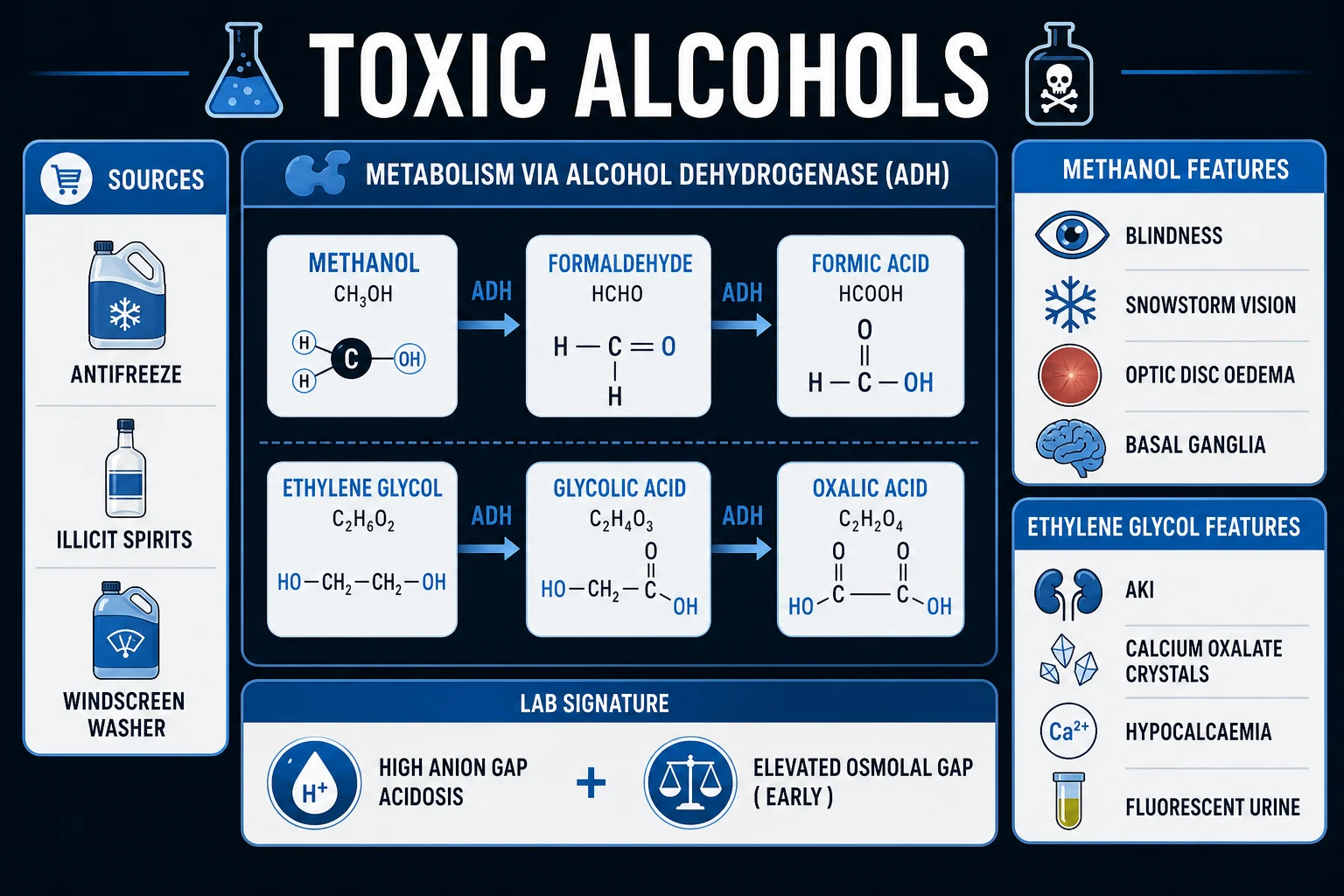
Toxic alcohol poisoning = methanol and ethylene glycol (the 'toxic alcohols') — both are metabolised by ALCOHOL DEHYDROGENASE (ADH) to highly toxic organic acids → SEVERE HIGH ANION GAP METABOLIC ACIDOSIS + end-organ injury. Methanol (CH3OH) → formaldehyde → FORMIC ACID → inhibits mitochondrial cytochrome c oxidase → RETINAL/optic nerve toxicity → BLINDNESS + basal ganglia injury. Ethylene glycol (HOCH2CH2OH) → glycoaldehyde → GLYCOLIC ACID (main acidosis driver) → glyoxylic acid → OXALIC ACID → precipitates with calcium → CALCIUM OXALATE CRYSTALS in renal tubules → ACUTE KIDNEY INJURY + hypocalcaemia. Both cause CNS depression, nausea, abdominal pain. DIAGNOSTIC CLUE: HIGH anion gap metabolic acidosis + HIGH osmolar gap EARLY (parent alcohol present — small osmotically active molecules). The osmolar gap FALLS as the anion gap RISES (parent alcohol is metabolised into organic acids) — so a LATE presenter may have a NORMAL osmolar gap. Latent period 12–24 h (metabolism required) — patient looks 'drunk' then deteriorates. Management PILLARS: (1) FOMEPIZOLE 15 mg/kg IV LOAD (blocks ADH → stops toxic metabolite formation — PREFERRED over ethanol — far safer, no CNS depression/hypoglycaemia) then 10 mg/kg q12h; (2) HAEMODIALYSIS (removes parent alcohol + metabolites — indicated for severe acidosis pH <7.3, AKI, visual symptoms, high levels >50 mg/dL, deterioration); (3) COFACTORS — FOLINIC ACID (methanol — folate-dependent oxidation of formate → CO2 + H2O) + THIAMINE + PYRIDOXINE (ethylene glycol — shunt glyoxylate to non-toxic glycine, AWAY from oxalate); (4) sodium bicarbonate for acidosis (also ion-traps formate/glycolate → enhances elimination). Ethanol is the ALTERNATIVE ADH inhibitor if fomepizole unavailable (target 100–150 mg/dL). Activated charcoal is USELESS (alcohols are small, rapidly absorbed, poorly bound). Outbreaks from illicit/counterfeit alcohol common. Mortality methanol 10–40% (up to 50% in outbreaks); ethylene glycol ~1–2% with early fomepizole + dialysis.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview
Pathophysiology — the two metabolic pathways
The entire toxicity of methanol and ethylene glycol comes from their METABOLITES, not the parent alcohol. The parent compounds are themselves only mildly intoxicating (less potent than ethanol). The lethal injury is generated when alcohol dehydrogenase (ADH) and then aldehyde dehydrogenase (ALDH) oxidise them stepwise into organic acids. This is the single most important concept: block ADH and you stop the poisoning.
[4]Methanol pathway (methyl alcohol, CH3OH — 'wood alcohol', found in windscreen washer fluid, antifreeze, paint thinner, illicit spirits, industrial solvents):
[1]Methanol ──alcohol dehydrogenase──▶ Formaldehyde ──aldehyde dehydrogenase──▶ Formic acid (formate)
(parent) (transient) (THE TOXIN)
Formic acid is the lethal metabolite. It (i) inhibits mitochondrial cytochrome c oxidase (complex IV) → cellular hypoxia (mimics cyanide at the mitochondrial level), and (ii) is a strong organic acid → high anion gap metabolic acidosis. Formate has particular affinity for the retina and optic nerve (retinal ganglion cells, optic disc) → optic disc oedema/hyperaemia → permanent blindness. It also injures the basal ganglia (putaminal necrosis → parkinsonism in survivors). Humans clear formate slowly because they are relatively folate-deficient compared with other primates — this is why folinic acid is a specific cofactor/antidote for methanol (it drives formate → CO2 + H2O via 10-formyl-tetrahydrofolate dehydrogenase).[1]
Ethylene glycol pathway (1,2-ethanediol, HOCH2CH2OH — the main component of automotive antifreeze/coolant, also hydraulic fluids):
[4]Ethylene glycol ──ADH──▶ Glycoaldehyde ──ALDH──▶ Glycolic acid ──▶ Glyoxylic acid ──▶ Oxalic acid
(parent) (acidosis) (shunt point) (renal toxin)
Glycolic acid is the dominant contributor to the metabolic acidosis (a strong organic acid). Oxalic acid is the renal toxin: it irreversibly chelates calcium to form calcium oxalate crystals, which precipitate in and obstruct the renal tubules → acute tubular necrosis → AKI (often oliguric/anuric). The calcium consumption also produces hypocalcaemia (prolonged QT, tetany). Glyoxylic acid sits at a metabolic branch point: with thiamine and pyridoxine it is diverted to the non-toxic amino acid glycine (and α-hydroxy-β-ketoadipate) — away from oxalate. This is why thiamine + pyridoxine are specific cofactors for ethylene glycol.[1][4]
The shared therapeutic target — ADH — is also the key to fomepizole and ethanol: both inhibit ADH competitively and shut down the production of every downstream toxin.
[2]Methanol vs ethylene glycol — the two patterns
[3]Diagnosis — high anion gap + high osmolar gap
The diagnosis is made on blood gas + biochemistry, not on the (often delayed) specific serum methanol/ethylene glycol level. The cardinal combination is a high anion gap metabolic acidosis with a high osmolar gap.[1]
Step 1 — Calculate the anion gap (AG): AG = Na+ − (Cl− + HCO3−). Normal 8–12 mmol/L. In toxic alcohol poisoning the AG is markedly elevated (often >30) from accumulation of formate (methanol) or glycolate/oxalate (ethylene glycol).
[3]Step 2 — Calculate the osmolar gap (OG): OG = measured osmolality − calculated osmolality, where calculated osmolality = 2 × Na+ + glucose + urea (+ 1.25 × ethanol if the patient has also drunk ethanol, + any other measured osmoles). Normal <10 mOsm/kg; a gap >20 mOsm/kg is strongly suggestive of an unmeasured osmotically active solute — the parent toxic alcohol. Methanol (MW 32), ethylene glycol (MW 62) and isopropanol (MW 60) are all small molecules that contribute substantially to serum osmolality but are not included in the calculated figure, generating the gap.[1]
Step 3 — Interpret them TOGETHER, and account for TIME since ingestion:
[1] [1]This timing is the most commonly examined and most commonly missed point: a late or chronically-exposed patient can have a completely normal osmolar gap because the parent alcohol has all been converted to (non-osmotic) organic acids. A normal osmolar gap never excludes toxic alcohol poisoning — if the AG is high and the story fits, treat empirically.[1]
Step 4 — Adjunctive / confirmatory tests:
- Serum methanol / ethylene glycol level (gold standard but often unavailable for hours — never delay treatment). Toxic thresholds commonly cited at >20 mg/dL (fomepizole indication); dialysis threshold >50 mg/dL.
- Urinalysis — calcium oxalate crystals (ethylene glycol): dihydrate = envelope/letterbox shape; monohydrate = needle/prism shape. May also show haematuria/proteinuria from tubular injury.
- Wood's lamp (UV) fluorescence of urine — antifreeze often contains fluorescein; may fluoresce. Unreliable (many preparations lack fluorescein; do not rule out).
- Visual examination (methanol) — optic disc hyperaemia/oedema on fundoscopy; patient describes 'snowstorm', blurred or grey vision.
- Lactate — may be mildly elevated (tissue hypoxia from mitochondrial poisoning; formate/glycolate inhibit cytochrome oxidase). Beware analyser artefact: glycolate can cause spuriously high lactate on some blood gas analysers (the 'lactate gap' — a big difference between lactate measured on two different platforms).
- Calcium — low in ethylene glycol (chelated into oxalate). Prolonged QT, tetany.
- Renal function — rising creatinine / oliguria (ethylene glycol >> methanol).
- CT brain (methanol, severe) — basal ganglia / putaminal hypodensity, haemorrhage; cerebral oedema.
The differential — what else raises BOTH gaps
The combination of high AG + high OG has a focused differential. Always consider:
[6] [4]The standout trap is isopropanol: it produces a high osmolar gap (acetone is osmotically active) but a normal anion gap (acetone is a ketone, not an acid) and no metabolic acidosis — distinguishing it from methanol/ethylene glycol, which always acidify. Isopropanol also causes ketonuria and haemorrhagic gastritis. Treatment is supportive (no fomepizole — isopropanol is metabolised via ADH to acetone, which is non-toxic, so blocking ADH is pointless).[1]
Management protocol
[3]Fomepizole vs ethanol — why fomepizole is preferred
[3]The two landmark trials that established fomepizole — the Methylpyrazole for Toxic Alcohols (MEPO) studies — showed fomepizole halted metabolite accumulation and prevented renal injury / visual loss when given early, with minimal side effects.[2][3]
Clinical pearls
Red flags
Prognosis
[3]Key trials and evidence
Brent et al. 1999 — Fomepizole for ethylene glycol poisoning (NEJM; PMID 10080845)
Brent et al. 2001 — Fomepizole for methanol poisoning (NEJM; PMID 11172179)
Roberts et al. 2015 — EXTRIP: extracorporeal treatment for methanol poisoning (Crit Care Med; PMID 25493973)
Exam SAQ — densified leaf
10 minutes · 10 marks
In structured CICM/FFICM style: (1) define the core entity in one sentence; (2) list three immediate ICU priorities; (3) state two investigations that change management; (4) name one evidence landmark or guideline anchor; (5) give one fatal exam trap.
Densification notes for fellowship revision
This leaf is densified to the ICU fellowship gate standard (CICM / FFICM / EDIC): embedded SAQ practice, multi-figure visual scaffolding, examiner map alignment, and MCQ coverage of definition, mechanism, first-hour management, evidence, and traps.
[4]- Revision checkpoint 1: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 2: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 3: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 4: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 5: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 6: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 7: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 8: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
References
- [1]Kraut JA, et al. Toxic alcohol ingestions: clinical features, diagnosis, and management. Clin J Am Soc Nephrol, 2008.PMID 18045860
- [2]Brent J, et al. Fomepizole for the treatment of methanol poisoning. N Engl J Med, 2001.PMID 11172179
- [3]Brent J, et al. Fomepizole for the treatment of ethylene glycol poisoning. Methylpyrazole for Toxic Alcohols Study Group. N Engl J Med, 1999.PMID 10080845
- [4]Barceloux DG, et al. American Academy of Clinical Toxicology Practice Guidelines on the Treatment of Ethylene Glycol Poisoning. Ad Hoc Committee. J Toxicol Clin Toxicol, 1999.PMID 10497633
- [5]Brent J. Current management of ethylene glycol poisoning. Drugs, 2001.PMID 11434452
- [6]Roberts DM, et al. Recommendations for the role of extracorporeal treatments in the management of acute methanol poisoning: a systematic review and consensus statement. Crit Care Med, 2015.PMID 25493973