ICU · Trauma
Chest Trauma — Blunt, Penetrating, Flail Chest & Cardiac Tamponade
Also known as Chest trauma · Flail chest · Pulmonary contusion · Cardiac tamponade · Beck triad · Tension pneumothorax · Massive haemothorax · Traumatic aortic injury · Traumatic diaphragmatic injury · Resuscitative thoracotomy
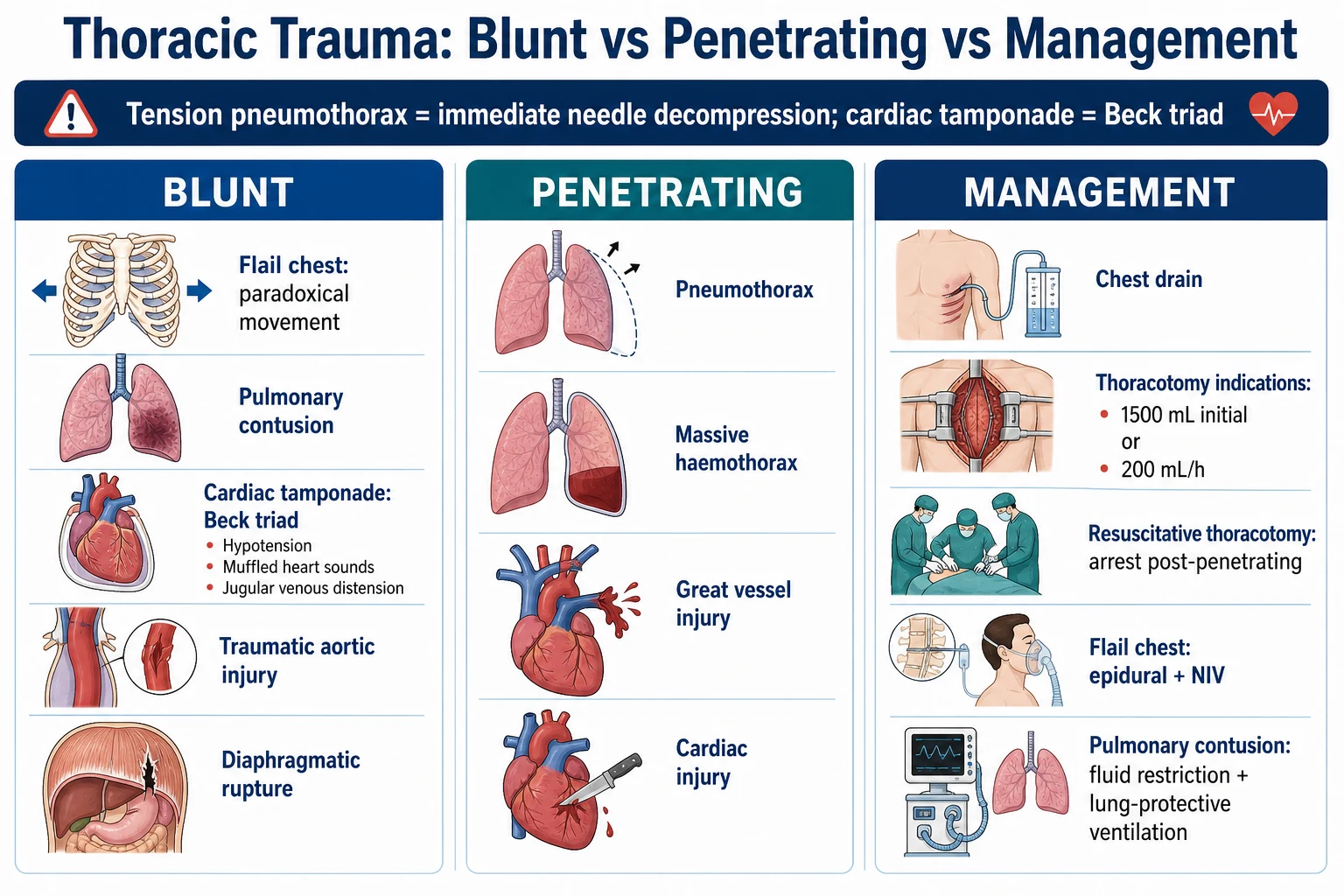
The chest trauma in the ICU: the blunt (the flail chest — the paradoxical movement; the pulmonary contusion; the cardiac tamponade — the Beck triad; the traumatic aortic injury; the diaphragmatic rupture) and the penetrating (the pneumothorax, the haemothorax, the great vessel, the cardiac). The immediately life-threatening (the ATLS): the tension pneumothorax, the massive haemothorax, the flail chest, the open pneumothorax, the cardiac tamponade. The management: the chest drain (the pneumothorax and the haemothorax), the thoracotomy (the massive haemothorax over 1500 mL or over 200 mL per h, the cardiac tamponade, the great vessel), the resuscitative thoracotomy (the arrest post-penetrating). The flail chest — the analgesia (the epidural), the ventilation (the NIV or the invasive for the respiratory failure), the pulmonary contusion — the fluid restriction, the lung-protective.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
The chest trauma is the common and the potentially the life-threatening. The two mechanisms: the blunt (the motor vehicle, the fall, the crush — the flail chest, the pulmonary contusion, the cardiac, the aortic) and the penetrating (the stab, the gunshot — the pneumothorax, the haemothorax, the cardiac, the great vessel). The ATLS identifies the immediately life-threatening (the tension pneumothorax, the massive haemothorax, the flail chest, the open pneumothorax, the cardiac tamponade) — the recognise and the treat in the primary survey.[1]
The immediately life-threatening (ATLS)
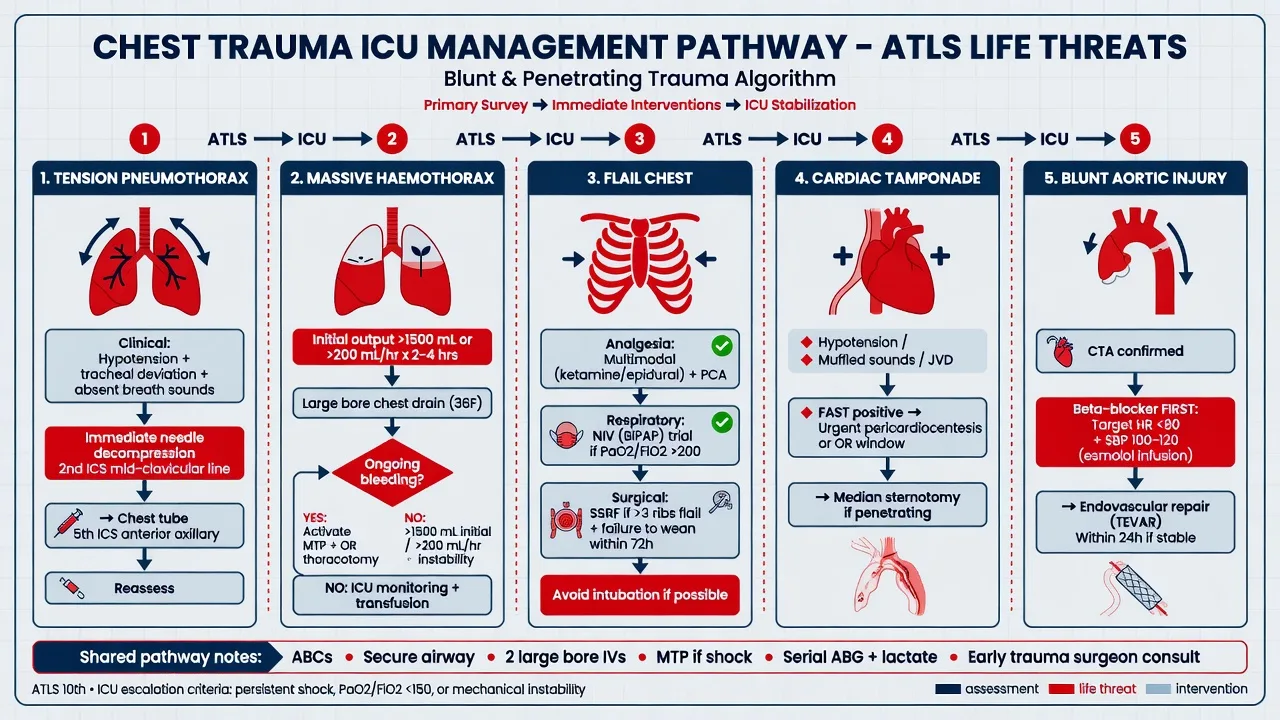
Tension pneumothorax
- The air enters the pleural space but cannot escape → the mediastinal shift → the obstructive shock (the hypotension, the distended neck veins, the tracheal deviation, the absent breath sounds one side).[1]
- The immediate needle decompression (the 14G cannula in the 2nd intercostal space mid-clavicular line — or the 5th intercostal mid-axillary; the finger thoracostomy if the ventilated). Then the chest drain.[1]
Massive haemothorax
- The over 1500 mL on the initial drainage, or the over 200 mL per hour for 2 to 4 hours → the thoracotomy.[1]
- The chest drain (the large-bore 28 to 36 Fr; the 5th ICS mid-axillary). The resuscitation (the blood, the MTP).[1]
Flail chest
- The 3 or more ribs fractured in 2 or more places → the free-floating segment → the paradoxical movement (the in on inspiration, the out on expiration).[1]
- The underlying pulmonary contusion (the main the cause of the respiratory failure).[1]
- The management: the analgesia (the epidural — the preferred), the ventilation (the NIV for the mild; the invasive for the severe respiratory failure), the fluid restriction (the contused lung the prone to the pulmonary oedema), the lung-protective ventilation.[1]
- The surgical fixation (the controversial; the select the cases).[1]
Cardiac tamponade
- The blood in the pericardial sac → the obstructive shock (the Beck triad — the hypotension, the distended neck veins, the muffled heart sounds).[1]
- The pulsus paradoxus (the BP drop over 10 mmHg on inspiration).[1]
- The echocardiogram (the diagnostic — the pericardial fluid, the right atrial/ventricular collapse, the RA pressure equal to the pericardial).[1]
- The management: the pericardiocentesis (the temporising), the thoracotomy / sternotomy (the definitive — the repair the cardiac laceration).[1]
Open pneumothorax
- The open wound (the "sucking chest wound"). The 3-sided occlusive dressing (the flutter valve — the air escapes but not enters). Then the chest drain.[1]
The other injuries
Traumatic aortic injury
- The rapid deceleration (the motor vehicle — the aortic isthmus). The CXR (the widened mediastinum, the apical cap, the NG tube deviation). The CT angiography (the diagnostic). The TEE (the intraoperative).[1]
- The management: the BP control (the SBP under 120 — the beta-blocker; the avoid the hypertension), the surgical or the endovascular repair.[1]
Diaphragmatic injury
- The blunt (the left — the liver protects the right) or the penetrating. The CXR (the herniated stomach/abdominal contents in the chest). The CT. The surgical repair.[1]
Pulmonary contusion
- The blunt force → the alveolar haemorrhage and the oedema. The develops over the 24 to 48 hours (the CXR the lags the clinical).[1]
- The management: the fluid restriction, the oxygen, the lung-protective ventilation (the if the severe). The avoid the over-resuscitation (the worsens the contusion).[1]
Red flags
Rib fractures — patterns, severity and surgical stabilisation (SSRF)
Rib fractures are the most common blunt thoracic injury and the single strongest predictor of morbidity and mortality after chest trauma. The severity is driven by (1) the number of ribs fractured, (2) the patient's age and respiratory reserve, and (3) the presence of an underlying pulmonary contusion. Three or more rib fractures in a patient over 65 carry a 10–20% mortality — Battle's meta-analysis (2019) confirmed a near-linear rise in death with each additional rib fractured.[24] The first rib, scapula and sternum are protected bones — fracture of any of them implies very high-energy transfer and should trigger a search for great-vessel, spinal and cardiac injury.
[3]Analgesia — the cornerstone
Adequate analgesia is the single most important intervention in rib fractures. Pain → splinting → atelectasis → retained secretions → pneumonia → respiratory failure. A stepwise, multimodal ladder is used: paracetamol ± NSAID as baseline, with a regional technique layered on top. Systemic opioids alone are inadequate (they suppress cough drive and cloud consciousness) and should be adjuncts, not the primary tool.[6]
[6]Gamberini's 2025 network meta-analysis ranked epidural first for analgesic efficacy and pneumonia reduction, with continuous ESP catheter a close second — and preferred when epidural is contraindicated (anticoagulated trauma patient, spinal concern).[5] ESP block has rapidly displaced paravertebral in many units because it is forgiving of coagulopathy and avoids the neuraxis.
Surgical stabilisation of rib fractures (SSRF)
SSRF — plating the fractured ribs to restore chest-wall integrity — has moved from controversial to a guideline-supported intervention for selected patients. The Hisamune 2024 meta-analysis of RCTs (and Sharma 2024 meta-analysis) showed reduced ICU stay, fewer ventilation days, lower pneumonia rate, and improved quality of life versus non-operative management in flail chest.[3][4]
[3]Flail chest — physiology and respiratory support
A flail segment generates paradoxical (inward) movement on inspiration because the negative intrathoracic pressure pulls the free-floating segment inwards. This wastes ventilatory work, causes pain, and — critically — almost always overlies a pulmonary contusion that independently causes hypoxia. It is the contusion, not the paradoxical movement, that dominates outcome.[15]
Pulmonary contusion — the delayed killer
A pulmonary contusion is a parenchymal lung injury (alveolar-capillary disruption → haemorrhage and oedema) that evolves over 24–48 h. The CXR characteristically lags the clinical picture by a day or two: a near-normal admission film does not exclude a contusion, and CT (much more sensitive) detects the non-aerated parenchyma immediately. Hypoxia is the dominant clinical feature and worsens over the first 48 h, peaking at 48–72 h.[16]
The EAST 2012 practice guideline and multiple cohort studies converge on three principles: (1) restrictive fluid strategy, (2) lung-protective ventilation when intubated, and (3) no routine steroids, diuretics or antibiotics.[16]
[16] [15]Pneumothorax and haemothorax — tube thoracostomy in detail
Chest-tube size — does it matter?
Traditional trauma teaching favoured large-bore (28–36 Fr) tubes for all traumatic haemothoraces because viscous blood clots in small tubes. However, contemporary evidence (randomised trials and large cohort studies in trauma) shows that small-bore (14–20 Fr) pigtail catheters are non-inferior for most pneumothoraces and many haemothoraces, with less pain, smaller scars and equivalent drainage. The pragmatic compromise: small-bore for isolated pneumothorax; large-bore for known/suspected haemothorax, massive air leak, or mechanically ventilated patients (where a clotted haemothorax must not be missed).[20]
[20]Massive haemothorax — thoracotomy thresholds
[2]Retained haemothorax — the preventable complication
A retained haemothorax is undrained blood in the pleural space after initial tube thoracostomy (typically diagnosed on follow-up CT). It is a high-risk state: empyema develops in ~25%, fibrothorax in up to 10% if left untreated. The duBose WTA multicentre trial (2012) and Chou review (2015) established the modern management: early VATS within 7 days (ideally 3–5 days) of admission reduces both empyema and length of stay.[9][20]
[20]Rahman NEJM 2011 — MIST2: tPA + DNase for pleural infection
Blunt thoracic aortic injury (BTAI) — TEVAR era
Blunt thoracic aortic injury is the second leading cause of trauma death after head injury; 80–90% die at the scene. Survivors reach hospital with a contained (pseudoaneurysm) tear — almost always at the aortic isthmus (just distal to the left subclavian, where the mobile arch meets the fixed descending aorta). The CXR is the screening test (widened mediastinum, apical cap, depressed left main bronchus, deviated NG tube), but CT angiography is definitive.[2]
The Society for Vascular Surgery 2021 guideline (Upchurch) stratifies BTAI by grade and recommends endovascular repair (TEVAR) for grade II–IV injuries, reserving non-operative (strict BP control) management for grade I (intimal tear) with repeat imaging.[2]
[2] [2] [2]Tracheobronchial injury
Blunt tracheobronchial injury is rare (1–3% of blunt chest trauma) but lethal. The classic mechanism is deceleration or crush — the airway tears within 2.5 cm of the carina (the rigid cricoid and carina anchor the airway; the mobile trachea is torn between them). Penetrating tracheal injury presents more overtly (bubbling wound, haemoptysis, stridor).[14]
[14] [14]Traumatic diaphragmatic rupture
Diaphragmatic rupture is easily missed in the acute phase (the CXR is abnormal in only ~50% of cases) and presents late with herniation and strangulation of abdominal viscera. Blunt rupture (from a sudden rise in intra-abdominal pressure) usually affects the left diaphragm (75% — the liver buttresses the right); ruptures are typically 10–15 cm posterolateral tears. Penetrating injuries produce smaller defects that may not herniate for years.[18]
[18] [18]Commotio cordis — sudden cardiac arrest in the structurally normal heart
Commotio cordis is instantaneous ventricular fibrillation triggered by a relatively low-energy, non-penetrating blow directly over the precordium in a person with a structurally normal heart. The mechanism is exquisitely timing-dependent: the impact must strike the chest during a narrow 10–30 ms window on the upstroke of the T wave (the vulnerable repolarisation window), mechanically activating K-ATP channels and triggering an R-on-T phenomenon. The classic victim is a young male athlete struck by a projectile (baseball, hockey puck, lacrosse ball); non-sports cases (assault, airbag, handlebar) are increasingly recognised.[12]
[12] [12]Maron JAMA 2002 — the commotio cordis registry
Resuscitative thoracotomy (RT / EDT)
Resuscitative thoracotomy — the left anterolateral thoracotomy performed in the emergency department on a patient in extremis or arrest from trauma — is one of the most dramatic interventions in medicine. Its purpose is four-fold: (1) release cardiac tamponade, (2) cross-clamp the descending aorta to preserve coronary/cerebral perfusion, (3) control intrathoracic haemorrhage, (4) open cardiac massage. Outcome is dictated almost entirely by the mechanism (penetrating >> blunt) and the presence of signs of life.[7]
[7] [7]Joseph TSACO 2018 — TQIP review of resuscitative thoracotomy outcomes
Blunt cardiac injury (BCI) — screening and the ECG / troponin rule
BCI covers a spectrum from subclinical troponin rise to cardiac rupture. The EAST 2012 practice guideline (Clancy) simplified screening: an admission ECG and troponin are the foundation; a normal ECG and troponin (at 6–8 h) reliably excludes clinically significant BCI and obviates the need for echocardiography or prolonged monitoring.[17]
[17] [17]SAQ — Flail chest with pulmonary contusion and respiratory failure
10 minutes · 10 marks
A 68-year-old man is admitted after a high-speed motor vehicle crash with left-sided rib fractures 3–8 in two places each, paradoxical chest wall movement, and a pulmonary contusion on CT. Initial GCS 15, SpO₂ 92% on 15 L O₂, RR 32. After 6 h of high-flow nasal cannula at 60 L/min / FiO₂ 0.9, his RR is 34, SpO₂ 88%, he is using accessory muscles and his ABG shows pH 7.28, PaCO₂ 62, PaO₂ 56.
SAQ — Penetrating cardiac injury with tamponade
10 minutes · 10 marks
A 24-year-old man is brought to ED by ambulance after a single stab wound to the precordium. He is agitated, dyspnoeic, distended neck veins, muffled heart sounds, HR 130, BP 70 systolic, SpO₂ 92%. There is a 1 cm laceration just left of the sternum at the 4th intercostal space. FAST shows pericardial fluid. He is rapidly becoming unconscious.
Clinical pearls — chest trauma in the ICU
Prognosis
Chest trauma outcomes (Battle 2019; Joseph 2018; SVS 2021)
Differential diagnosis — by presenting sign
[20]ICU bundle — the daily checklist
[15]Key points — the one-minute exam revision
[6]References
- [1]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [2]Lee WA, Matsumura JS, Mitchell RS, et al. Endovascular repair of traumatic thoracic aortic injury: clinical practice guidelines of the Society for Vascular Surgery. Journal of vascular surgery, 2011.PMID 20974523
- [3]Sharma VJ, et al. Surgical stabilisation of rib fractures: a meta-analysis of randomised controlled trials. Injury, 2024.PMID 38945079
- [4]Hisamune R, Kobayashi M, Nakasato K, et al. A meta-analysis and trial sequential analysis of randomised controlled trials comparing nonoperative and operative management of chest trauma with multiple rib fractures. World journal of emergency surgery : WJES, 2024.PMID 38504282
- [5]Gamberini L, et al. Regional anaesthesia modalities in blunt thoracic trauma: a systematic review and Bayesian network meta-analysis. American Journal of Emergency Medicine, 2025.PMID 39740311
- [6]Hewson DW, Nightingale J, Ogollah R, et al. Erector Spinae Plane block with fascial plane catheter for the Early Analgesia of Rib fractures in trauma (ESPEAR): a multicentre feasibility randomised trial. BJA open, 2025.PMID 41142587
- [7]Joseph B, et al. Improving survival after an emergency resuscitative thoracotomy: a 5-year review of the Trauma Quality Improvement Program. Trauma Surgery and Acute Care Open, 2018.PMID 30402559
- [8]Tesoriero R, Coimbra R, Biffl WL, et al. Adult emergency resuscitative thoracotomy: A Western Trauma Association clinical decisions algorithm. The journal of trauma and acute care surgery, 2024.PMID 39451159
- [9]Patel NJ, Dultz L, Ladhani HA, et al. Management of simple and retained hemothorax: A practice management guideline from the Eastern Association for the Surgery of Trauma. American journal of surgery, 2021.PMID 33487403
- [10]Broderick SR, et al. Hemothorax: etiology, diagnosis, and management. Thoracic Surgery Clinics, 2013.PMID 23206720
- [11]Rahman NM, Maskell NA, West A, et al. Intrapleural use of tissue plasminogen activator and DNase in pleural infection. The New England journal of medicine, 2011.PMID 21830966
- [12]Maron BJ, et al. Clinical profile and spectrum of commotio cordis. JAMA, 2002.PMID 11879111
- [13]Shemmeri E, et al. Blunt tracheobronchial trauma. Thoracic Surgery Clinics, 2018.PMID 30054080
- [14]Grewal HS, et al. Treatment of tracheobronchial injuries: a contemporary review. Chest, 2019.PMID 30059680
- [15]Walkey AJ, et al. Use of airway pressure release ventilation is associated with a reduced incidence of VAP in patients with pulmonary contusion. Journal of Trauma, 2011.PMID 20526208
- [16]Simon B, Ebert J, Bokhari F, et al. Management of pulmonary contusion and flail chest: an Eastern Association for the Surgery of Trauma practice management guideline. The journal of trauma and acute care surgery, 2012.PMID 23114493
- [17]Clancy K, et al. Screening for blunt cardiac injury: an EAST practice management guideline. Journal of Trauma and Acute Care Surgery, 2012.PMID 23114485
- [18]Thiam O, Konate I, Gueye ML, et al. Traumatic diaphragmatic injuries: epidemiological, diagnostic and therapeutic aspects. SpringerPlus, 2016.PMID 27652187
- [19]Beks RB, et al. Fixation of flail chest or multiple rib fractures: current evidence and how to proceed — a systematic review. European Journal of Trauma and Emergency Surgery, 2019.PMID 30276722
- [20]Chou YP, et al. Video-assisted thoracoscopic surgery for retained haemothorax in blunt chest trauma. Current Opinion in Pulmonary Medicine, 2015.PMID 25978625
- [21]Wallen TE, et al. Intercostal liposomal bupivacaine injection for rib fractures: a prospective randomised controlled trial. Journal of Trauma and Acute Care Surgery, 2022.PMID 34789700
- [23]Rhee PM, et al. Survival after emergency department thoracotomy: review of published data from the past 25 years. Journal of the American College of Surgeons, 2000.PMID 10703853
- [24]Battle CE, Hutchings H, Evans PA Risk factors that predict mortality in patients with blunt chest wall trauma: a systematic review and meta-analysis. Injury, 2012.PMID 21256488