Paeds · acute-care-resuscitation-and-toxicology
ABCDE assessment and stabilisation of the acutely ill child
Also known as ABCDE approach · Paediatric primary survey · Systematic assessment of the sick child · Resuscitation of the acutely ill child · Treat-as-found primary survey
A fellowship approach to the systematic ABCDE assessment and immediate stabilisation of the acutely ill child. Treat each life threat as it is found, reassess from A after every action, use age- and weight-appropriate oxygen, ventilation, fluid, glucose and seizure interventions, escalate before local support is exceeded, and hand over safely.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
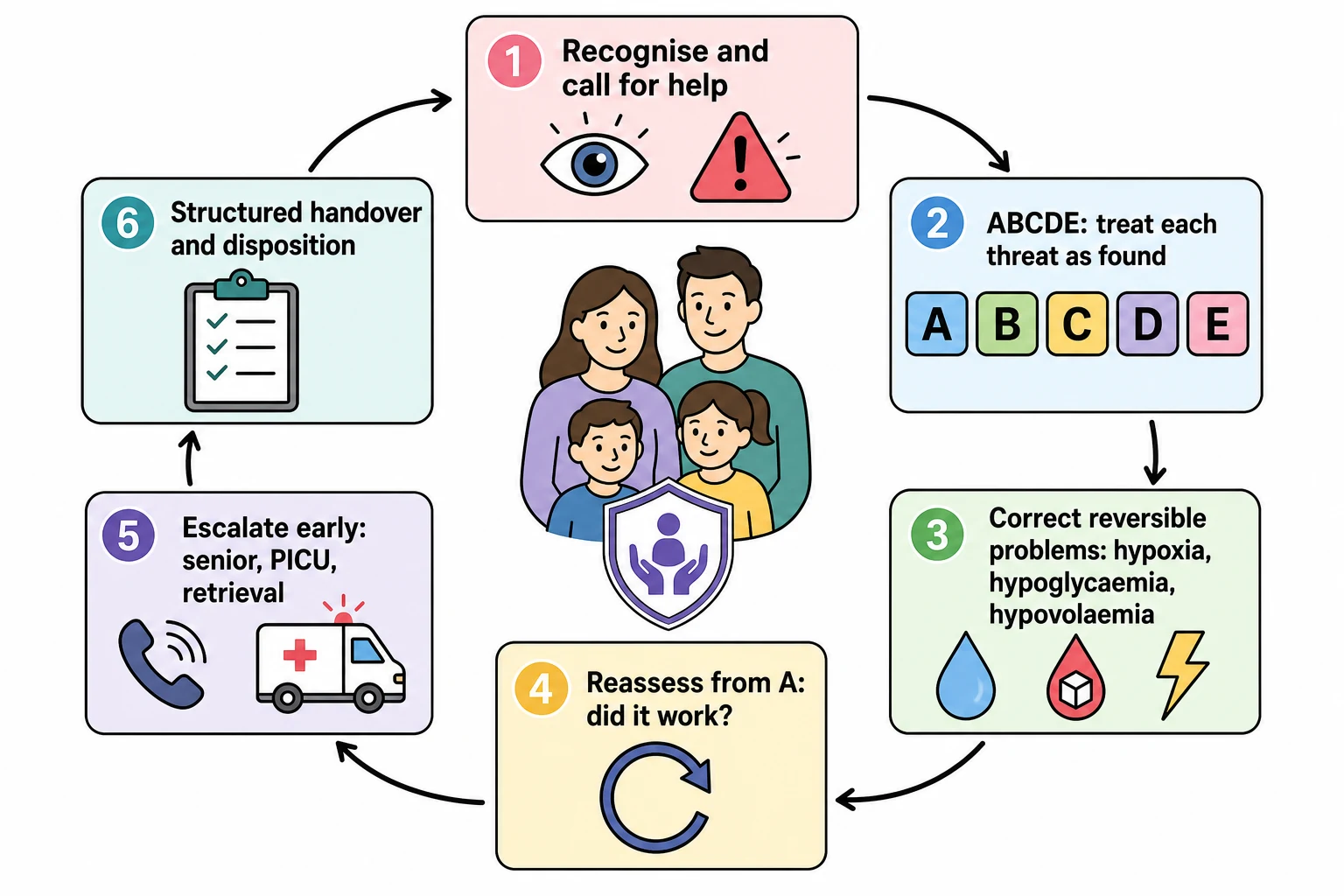
The ABCDE approach is a structured primary survey that finds and fixes life threats in the order they will kill the child: a blocked airway kills before failing breathing, failing breathing kills before shock, shock kills before a falling conscious level. You do not need a diagnosis to start. The moment you find a threat at any step, you treat it, then you return to A and reassess the whole child. This treat-as-found, reassess-from-A discipline is what turns a checklist into resuscitation. [9] [10]
ABCDE is a stabilisation method, not a diagnostic method. It tells you which organ system is failing now and keeps the child alive while you work out why. The cause-specific pathway (sepsis, asthma, anaphylaxis, diabetic ketoacidosis, poisoning, trauma) takes over once the immediate threats are controlled, and reassessment never stops. A child can be perfectly stable on the primary survey and still need urgent work-up because the missed diagnosis is dangerous; equally, an unstable child needs treatment before the diagnosis is certain. [3] [9]
[9] [10]It sits between two other tools. The paediatric assessment triangle is the hands-off first impression from the doorway that tells you to start ABCDE. The focused secondary assessment (full history and head-to-toe examination) comes after the primary survey has made the child safe. ABCDE is the hands-on middle layer where most lives are saved or lost. [9]
The primary survey as a repeating loop
Call for help and prepare
If the child looks unwell from the doorway, call the resuscitation team, name a leader, allocate roles, and bring age- and weight-appropriate equipment and monitoring.
A to E, treat as found
Work through Airway, Breathing, Circulation, Disability and Exposure in order. Treat each threat the moment you find it rather than finishing the survey first.
Reassess from A
After any intervention, return to A and check whether the change you expected actually happened. Compare with the child's baseline and the trend.
Escalate early
Call senior, PICU or retrieval help as soon as the child may need monitoring or treatment your service cannot reliably provide, not after local options fail.
Hand over and dispose
Transfer a structured summary of identity, physiology, timed actions, response, risks and contingency to the team and location that will carry the child forward.
Classification
Each step of the survey answers one question and has one first action. Read the table as the contract for what you do at each letter. [9]
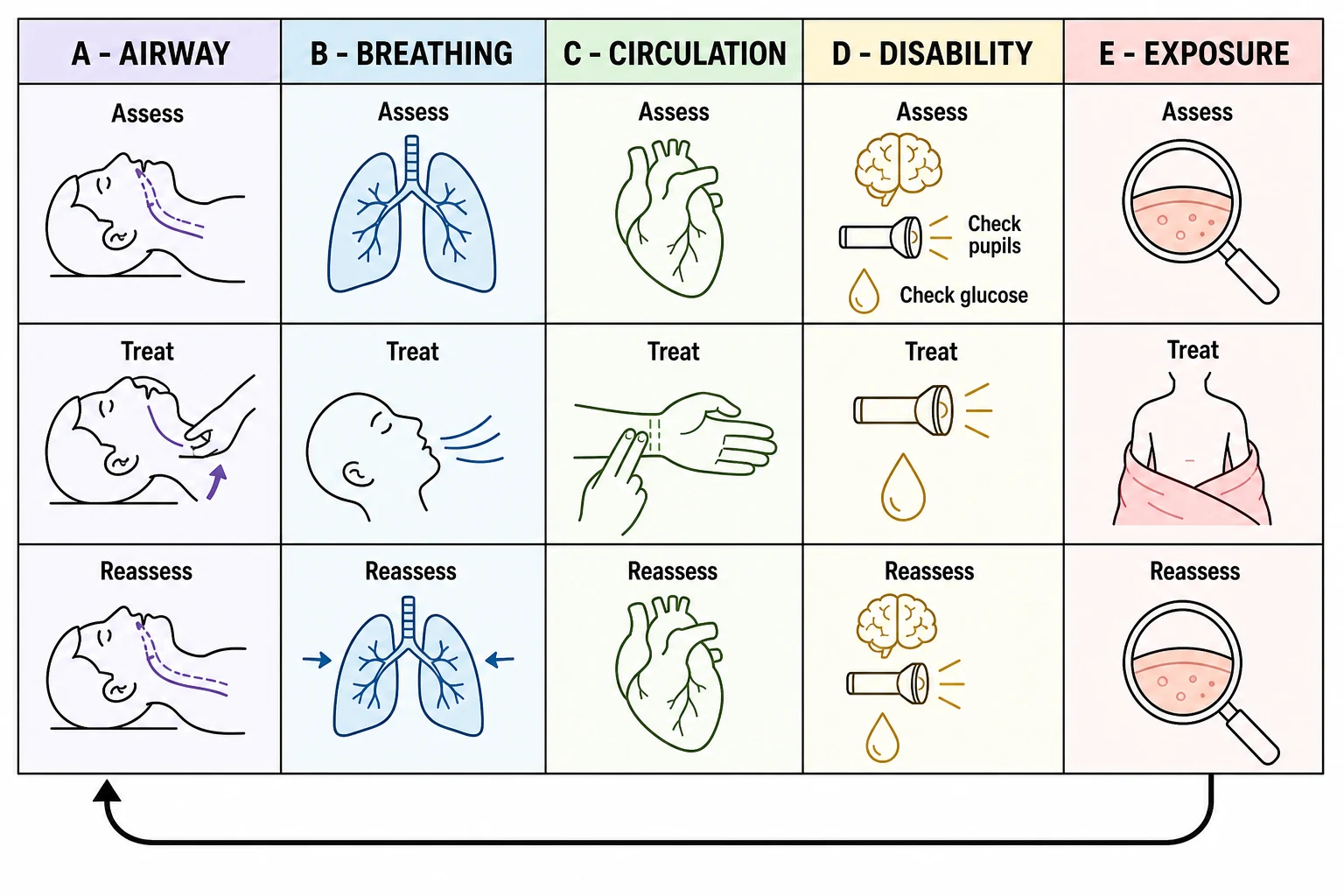
| Step | Question | Find | First action |
|---|---|---|---|
| A - Airway | Is the airway open and protected? | Abnormal sound or silence, obstruction, secretions, blood, inability to vocalise | Position the airway, clear removable obstruction, summon airway expertise before failure |
| B - Breathing | Is breathing effective? | Rate, effort, air entry, symmetry, fatigue, credible oxygen saturation | Give oxygen in failure; support ventilation with bag-mask if ineffective |
| C - Circulation | Is perfusion adequate? | Pulse rate and quality, skin colour and temperature, capillary refill, blood pressure, mental state, urine output | Control loss, gain access, give fluid aliquots for shock with reassessment |
| D - Disability | Is the brain threatened? | AVPU or age-adapted GCS, pupils, posture, tone, seizure, bedside glucose | Protect airway and breathing; correct dangerous low glucose; treat seizure at 5 minutes |
| E - Exposure | Is a cause visible? | Rash, injury, bruising, bleeding, device problem, temperature | Look while preserving warmth and dignity; start safeguarding in parallel |
A useful companion is the staged description of how sick the child is. Respiratory distress means effort is increased but breathing still moves air. Respiratory failure means oxygenation or ventilation is ineffective and appearance is often abnormal. Compensated shock means perfusion is poor but blood pressure is maintained. Decompensated shock adds hypotension and falling consciousness. Cardiorespiratory arrest means unresponsive, no breathing, no pulse. Each stage changes the urgency and the first action, and the boundary is clinical, not a single number. [3] [9]
First impression
Hands-off, seconds
- Paediatric assessment triangle at the doorway
- Decides whether to start ABCDE now
- Does not diagnose
- Never replaces hands-on assessment
ABCDE primary survey
Hands-on, treat as found
- Finds and fixes life threats in order
- Uses measurements, equipment and interventions
- Repeats from A after every action
- Stabilises before diagnosing
Secondary assessment
Once the child is safe
- Full focused history and head-to-toe examination
- Targeted investigations for a named question
- Refines the cause and the pathway
- Never precedes stabilisation of an unstable child
Epidemiology & Risk Factors
Children deteriorate fast because their physiology is built for compensation, and the settings where deterioration is missed share the same features: a young infant, a delayed or repeated presentation, a barrier to communication, and a service with limited monitoring or rescue. The practical point is that risk context changes the tempo of your survey and the threshold for escalation, not the order of the letters. [3] [9]
Young infants deserve particular caution. A neonate or infant under three months can have serious bacterial infection, metabolic disease or a duct-dependent cardiac lesion and present without fever, with only poor feeding, reduced tone or a change in behaviour. Treat these as high-risk presentations: lower your threshold to start ABCDE, check bedside glucose, and seek senior review early. [3] [9]
Child and disease factors
- Young infant or recent neonatal transition
- Prematurity, chronic or multisystem disease
- Immunocompromise or attenuated inflammatory response
- Congenital heart or pulmonary vascular physiology
- Technology dependence with a personal emergency plan
Presentation factors
- Caregiver says the child is different from usual
- Recurrent presentation or recent discharge
- Poor intake, altered behaviour, seizure or collapse
- Known ingestion, medication error, trauma or exposure
- A dangerous diagnosis still possible despite stable physiology
Health-system factors
- Rural distance, weather or delayed transport
- Limited monitoring, airway or critical-care rescue
- Communication or language barriers
- Handover gaps and unclear escalation ownership
- Single-handed or after-hours cover
The limits of individual signs are evidence-based, and examiners test them. Capillary refill time is useful but its sensitivity and specificity for serious illness are modest, and the result depends on technique, site, ambient temperature and the operator. Blood pressure is maintained until late in paediatric shock, so a normal pressure never excludes it. Early-warning scores depend on the chart, complete observations and the response system around them. None of these, used alone, should end your survey. [2] [3]
Pathophysiology
Children compensate well and then collapse. To understand ABCDE you need to know why. A child in early shock or respiratory failure does not look as bad as an adult at the same stage, because heart rate, breathing effort and vascular tone rise to protect blood pressure and cerebral perfusion. This buys time, but it hides the problem and it costs reserve. When reserve runs out, the fall is steep. [3] [9]
Cardiac output in children is heart-rate dependent. Neonates and young infants have a relatively fixed stroke volume, so they maintain output mainly by raising heart rate. Tachycardia and vasoconstriction can preserve blood pressure and wakefulness for a while, but they also raise oxygen demand. In a child who is hypoxic or deteriorating, a falling or abnormally low heart rate is an ominous sign of decompensation, not a sign that the child is calming down. Waiting for hypotension to diagnose circulatory failure is a classic and dangerous error. [1] [3]
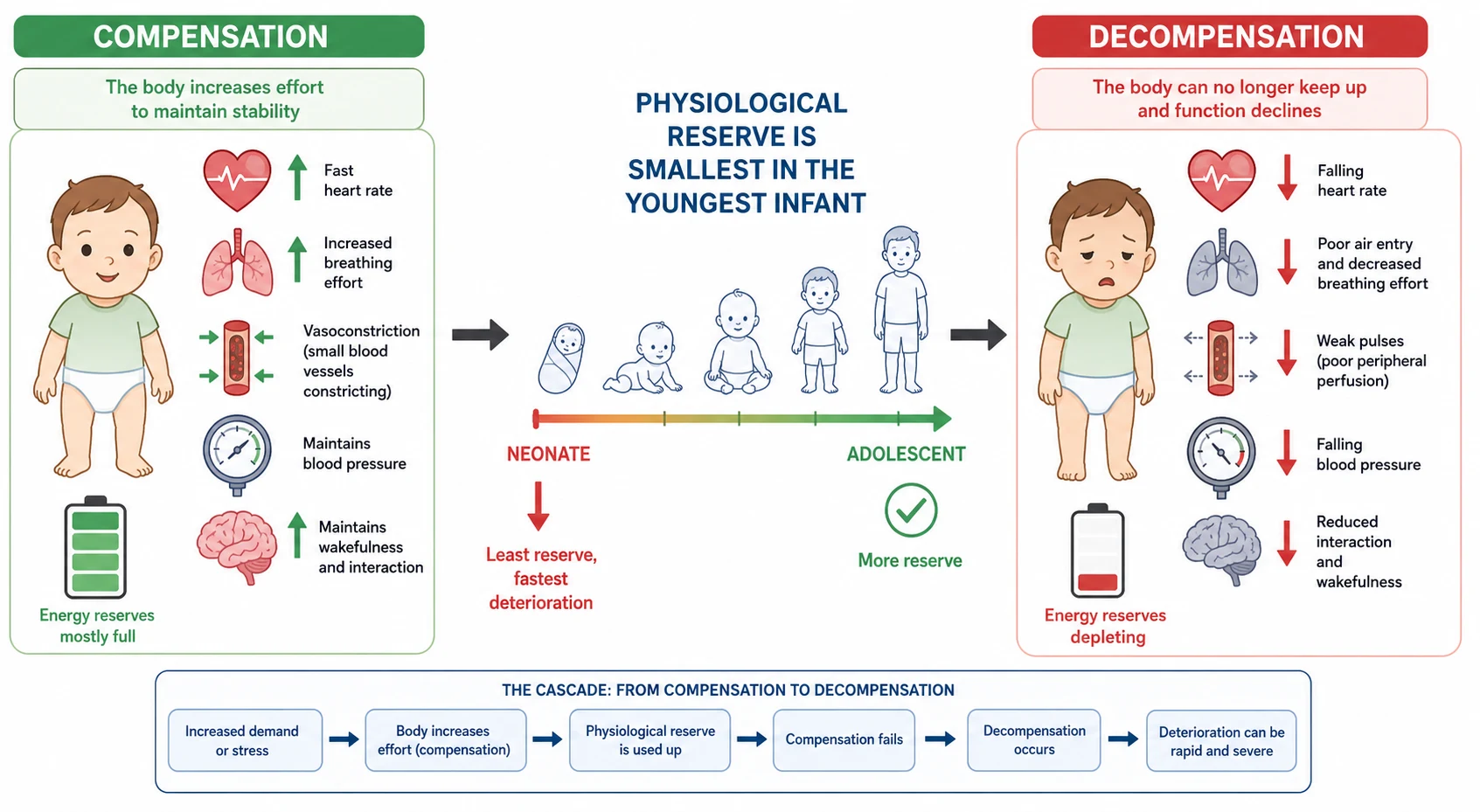
The respiratory system has the same shape. Smaller airways, a compliant chest wall and a higher metabolic rate mean a young child runs out of respiratory reserve quickly. Increasing effort at first moves air and maintains oxygenation; as the muscles fatigue, air entry falls while visible effort may actually lessen. This is the tiring child, and it is one of the most dangerous moments in the survey: a quieter chest after marked effort is failure until you prove otherwise. [1] [9]
Oxygen delivery depends on effective ventilation, arterial oxygen content, cardiac output, tissue perfusion and cellular use. A failure at any of these can make the child acutely ill, which is why the survey moves airway to breathing to circulation to brain in that order: each step protects the next. A child who is blue, mottled and limp is not showing three separate problems but one failing system seen through several signs. [3]
Disability fails because the brain is sensitive to hypoxia, hypercapnia, hypoperfusion, hypoglycaemia, seizures and toxins. A change in appearance or interaction is therefore a late-but-urgent signal that something upstream in A, B or C is failing, or that a metabolic or toxic threat is present. Reading disability as a stand-alone neurological problem, rather than as a window onto the whole child, is a common error. [7] [9]
Clinical Presentation
Begin before you touch. From the doorway, note interaction and arousability, tone and posture, cry or speech, visible and audible breathing effort, colour, and the caregiver's manner. Any of these can trigger ABCDE. The goal is to describe what you see, not to label it. "This child is pale, floppy, grunting and barely responsive" tells the team more than "this child looks septic". [9]
What each step shows when it is failing
At A, a threatened airway may show abnormal sound (stridor, snoring, gurgling, silence), tripoding or a preferred posture, inability to phonise, or obstruction by secretions or blood. A child fighting to keep an airway upright must not be laid flat or agitated; summon airway expertise before the airway is lost. [9]
At B, look for a rate outside the range for age and condition, increased work (recession, nasal flaring, grunting, accessory muscle use), reduced or unequal air entry, and a credible oxygen-saturation trend. Respiratory distress becomes respiratory failure when effort is high but air entry is poor, or when effort falls while the child looks worse. Oxygen saturation is a single input: confirm the signal is reliable and matches the child, because oximetry does not measure ventilation and may overestimate oxygenation in darker skin. [1] [9]
At C, integrate pulse rate and quality, skin colour and temperature, capillary refill measured with the technique stated, blood pressure, mental state and urine output. Warm skin with a bounding pulse does not exclude shock; cold skin with weak pulses does not confirm one type. Hypotension is a late sign. Weigh the whole picture, and treat the direction of change. [2] [3]
At D, use AVPU for speed (Alert, responds to Voice, responds to Pain, Unresponsive) and convert any V, P or U, or a persistently concerning Alert child, to a formal age-adapted Glasgow Coma Scale. Check pupils, posture, tone and movement, time any seizure, and check bedside glucose whenever consciousness is altered, a seizure is present, or shock, poor intake or a toxic or metabolic cause is possible. [7] [9]
At E, look for rash, injury, bruising, bleeding, a device problem or abnormal temperature while keeping the child warm and covered. The skin often holds the diagnosis (purpura, a burn, an injection site, a blocked tracheostomy), and it may hold safeguarding evidence. [9]
| Life stage | High-value change from usual | Adaptation in the survey |
|---|---|---|
| Neonate or young infant | Feeding, behaviour, tone, colour or temperature change; may be afebrile | Clarify perinatal history; check bedside glucose early; seek senior review; use Newborn Life Support at birth |
| Older infant | Reduced interaction, weak cry, poor feeding, fewer wet nappies | Observe on the caregiver first; interpret limited reserve and rapid change |
| Toddler and preschool child | Loss of play, mobility or speech; ingestion or injury possible | Use play, examine least-distressing parts first, ask the child directly |
| School-age child | Reduced exercise tolerance, new pain, behavioural change, hidden exposure | Take the history from the child while retaining the caregiver's account |
| Adolescent | Collapse, chest symptoms, intake restriction, substance or self-harm risk | Create private time when safe; explain confidentiality and its limits |
| Young-adult transition | Change in personal plan, device support or caregiver role | Transfer baseline, emergency plan and decision-making arrangements |
Differential Diagnosis
Build the primary-survey differential in a fixed order: what can kill the child now, what is most likely, what is reversible, and what is most harmful to miss. ABCDE does not name the disease; it names the failing system and the immediately reversible threats. Keep the dangerous causes open until focused history, examination, targeted tests and response narrow them. [3] [9]
REVERSIBLE
A more compact and widely taught frame is the reversible causes to actively seek during the survey: hypoxia, hypovolaemia, hypoglycaemia and hypothermia (the low Hs), and tension pneumothorax, tamponade, toxins and thrombosis (the mechanical and toxic Ts). These are the threats that a single correct action can reverse, so they belong in the front of your mind at every pass. [9] [10]
Airway and breathing
- Upper-airway obstruction: croup, epiglottitis, foreign body, retropharyngeal abscess
- Lower-airway disease: asthma, bronchiolitis
- Parenchymal disease: pneumonia, pulmonary oedema, ARDS
- Impaired drive or neuromuscular weakness
- Tension pneumothorax
Circulation
- Hypovolaemic: haemorrhage, dehydration, DKA
- Distributive: sepsis, anaphylaxis
- Cardiogenic: myocarditis, dysrhythmia, cardiomyopathy
- Obstructive: tamponade, pulmonary embolism, duct-dependent lesion
- Mixed physiology is common
Disability
- Seizure or post-ictal state
- Meningitis or encephalitis
- Dangerous low glucose
- Raised intracranial pressure or head injury
- Toxin or medication effect
Safeguarding
- Non-accidental injury or abusive head trauma
- Neglect or induced illness
- Deliberate or unsupervised poisoning
- Inconsistent or implausible history
- Stabilise first; document objectively; act in parallel
A defensible synthesis sounds like this: "This child has ineffective breathing with falling air entry and reduced interaction, so I am treating respiratory failure with oxygen and ventilation support. My leading threats are severe lower-airway or parenchymal disease with fatigue, but I am keeping sepsis, a cardiac cause, a metabolic problem and a toxin open. I will reassess after ventilation improves, and I will not fix on one diagnosis until the trend supports it." [9]
Clinical & Bedside Assessment
The survey is hands-on but not rough. Keep the child with the caregiver when safe, observe before handling, and examine the least distressing parts first. Distress raises the respiratory rate and heart rate, worsens behaviour, and can destabilise a threatened airway, so a calm sequence is part of the treatment. None of this delays treatment of an unstable child. [9]
A - Airway
Assess whether the airway open and protected. Listen for abnormal sound or an ominous silence. Look for obstruction, secretions, blood or vomit, and assess whether the child can maintain the airway and protect it (can they phonise, swallow, clear secretions?). First actions are airway positioning (head-tilt chin-lift, or jaw thrust if trauma is possible), suction of removable obstruction, and an airway adjunct only if tolerated. Summon definitive airway expertise before the airway fails, not after. [9]
B - Breathing
Count the respiratory rate under stated conditions and compare with the age-appropriate range. Assess effort, effectiveness, symmetry, air entry and fatigue. Attach a credible pulse oximeter and, in serious illness, consider capnography. The first action in respiratory, circulatory or neurological failure is to give high-flow oxygen. If breathing is ineffective, support it with bag-mask ventilation: an open airway, a good seal, an appropriate size, gentle chest rise, and a rate for age. Effective ventilation is judged by chest movement, air entry, improving colour and interaction, not by the monitor alone. [1] [9]
C - Circulation
Assess pulse rate and quality at central and peripheral sites, skin colour and temperature, capillary refill with site, compression time and ambient temperature stated, blood pressure, mental state and urine output. Look for bleeding and check device function. First actions are to control obvious loss, gain vascular access without allowing repeated failed attempts to delay care, and treat shock with fluid aliquots. Diagnose shock from the whole picture, never from blood pressure or capillary refill alone. [2] [3]
D - Disability
Use AVPU for speed. The Royal Children's Hospital Melbourne altered-conscious-state guideline directs any V, P or U response to a formal Glasgow Coma Scale; record AVPU and reassess after immediate care. Perform an age-adapted GCS when concern persists despite an apparently Alert child, and never convert an AVPU letter into an assumed GCS number. Check pupils, posture, tone and movement, time any seizure, and check bedside glucose. Protect the airway and breathing while the local pathway is activated. [7] [9]
E - Exposure
Expose only what you must, look for rash, injury, bruising, bleeding, swelling or a device problem, then cover and warm the child again. Record objective findings and the child's spontaneous words accurately, because exposure often reveals both the diagnosis and safeguarding evidence. [9]
[9]Focused history in parallel
While stabilisation proceeds, take a focused history using a SAMPLE frame: Symptoms, Allergies, Medications, Past history (including baseline and devices), Last meal, Events leading up. Begin with the caregiver: "What is different from usual, and what worries you most?" Add onset, pace, breathing, feeding, urine output, fever, rash, collapse, seizure, exposure, ingestion and trauma. Ask adolescents privately about substances, self-harm and pregnancy when safe. Use a professional interpreter whenever needed. [9]
Synthesis after every pass
After each pass, say and document one sentence: what is failing now, what direction the child is moving, what you expected from the last action and what actually happened, and what you will do next. This spoken synthesis is what examiners listen for, and it is what keeps a team coordinated during rapid change. [8] [9]
Investigations
Stabilise first, then order a test for a named question. A useful test finds an immediately reversible cause, quantifies failing physiology, separates urgent pathways, or changes the destination. A normal panel cannot overrule a child who is worsening. [9]
Immediate and bedside
- Bedside glucose for altered consciousness, seizure, shock, poor intake or toxic or metabolic concern
- Credible oxygen saturation and, in serious illness, capnography
- ECG for any circulatory concern or collapse
- Point-of-care blood gas and lactate to quantify ventilation, perfusion and metabolic state
Conditional on a question
- Blood count, electrolytes, renal and hepatic indices, coagulation and inflammatory markers for a defined branch
- Cultures before antimicrobials when this does not substantially delay time-critical treatment
- Targeted toxicology, endocrine or metabolic sampling when the result changes the plan
- Minimum necessary volume and good pain relief
Targeted imaging
- Chest imaging only if it changes management beyond the clinical assessment
- Echocardiography or point-of-care ultrasound only within operator competence
- Neuroimaging or lumbar puncture only after stability and procedure risk are assessed
- Never move an unstable child to imaging without monitoring, escort and a rescue plan
Interpret urgent tests as physiology and trend, not binary reassurance. A blood gas shows whether ventilation and acid-base state are failing and whether the pattern points to respiratory, circulatory, metabolic or toxic causes; one gas never replaces the child. Lactate reflects perfusion or metabolic stress and should fall with effective resuscitation; a normal lactate does not exclude shock. Blood count and inflammatory markers cannot rule out serious infection in a high-risk child. Confirm an unexpected point-of-care glucose when feasible, but never let confirmation delay treatment of a dangerous low. [7] [9]
[9]Management — Resuscitation
A worrying first impression starts ABCDE immediately. State that you are concerned, call the appropriate team, name a leader, allocate roles, use closed-loop communication, prepare age- and weight-appropriate equipment, and monitor continuously. Treat each problem when found, then reassess from A. History, sampling and cause-specific treatment proceed in parallel only when they do not delay resuscitation. [9]
The first five minutes when the diagnosis is uncertain
Call and organise
State what you see, call senior, resuscitation, airway, critical-care or retrieval help, identify the leader and allocate tasks.
A - Keep the airway open
Position the airway, clear an immediately removable obstruction, avoid agitating a threatened airway, and call airway expertise before failure.
B - Make breathing effective
Give high-flow oxygen in failure; support ventilation with bag-mask if ineffective. Recheck air entry, work, interaction and a credible saturation.
C - Support circulation safely
Control obvious loss, gain access, give fluid aliquots for shock, state the expected response, and reassess after each aliquot.
D - Protect the brain
Assess consciousness, protect airway and breathing, time any seizure, check glucose, correct a dangerous low, escalate non-response.
E - Expose with care
Look for rash, injury and device problems while preventing heat loss and starting safeguarding in parallel.
Reassess from A
Compare the child with the result you expected; record benefit or harm; revise the differential; move to the next pathway.
Oxygen: phase and population matter
The American Heart Association 2020 Paediatric Life Support guideline states that a child in respiratory, circulatory or neurological failure should receive high-flow oxygen initially, followed by titration. For a previously healthy child, target an oxygen saturation of 94 to 98%, using the lowest inspired fraction that achieves at least 94%. These are acute-rescue facts. They are not universal targets for cyanotic congenital heart disease, chronic respiratory support or post-resuscitation care. Confirm a credible oximeter signal before trusting the number. [9]
Circulatory support: a ceiling, not a target
First decide whether the child has shock using the whole circulation assessment. Then consider the likely shock type, whether hypotension is present, and whether ventilation, critical care and vasoactive rescue are available. Decide what improvement you expect before giving fluid, reassess after each aliquot, and stop for overload or no benefit. The Surviving Sepsis Campaign 2026 children's guideline supports up-front fluid boluses in septic shock with careful reassessment, while cautioning against fluid accumulation. The first-hour fluid total is a ceiling, never a target. [3] [11]
The FEAST trial is the cautionary anchor. In African children with severe febrile illness, saline or albumin bolus increased early mortality compared with no bolus. It does not prove that every bolus is harmful everywhere; it proves that a fluid algorithm cannot be transplanted across populations and rescue resources. Apply fluid strategy to the child in front of you, and call for critical-care or retrieval help early if vasoactive support may be needed. [4]
Disability: glucose and seizure
Check bedside glucose whenever altered consciousness, seizure, shock, poor intake or a toxic or metabolic cause is possible. If the point-of-care result is dangerous-low, correct it now through the active age- and context-specific pathway, then recheck and investigate the cause; confirm an unexpected result when feasible, but never delay treatment. Under the AHA 2020 guideline and local pathways, an ongoing convulsive seizure is status epilepticus and activates first-line treatment at five minutes; do not wait for two doses to fail. [6] [7] [9]
Working weight when immediate weighing is unsafe
Use a measured weight if it can be obtained immediately without delaying care. Otherwise announce and document one temporary working weight in kilograms, including its source, method and time. Follow the local protocol: a recent reliable measured weight, a credible caregiver estimate, or the service's trained length-and-habitus method. Published methods vary in accuracy and are not interchangeable, and total body weight is not correct for every drug or device, so always confirm with the local paediatric cognitive aid and re-weigh at the first safe opportunity. [5]
When ABCDE becomes advanced life support
If the child is unresponsive with absent or agonal breathing and no central pulse, move straight into the paediatric arrest algorithm rather than completing the survey. The AHA 2020 and ILCOR 2020 paediatric life support sources anchor the key arrest doses: intravenous or intraosseous adrenaline 10 micrograms per kilogram (0.1 mL/kg of 1:10,000 adrenaline) every three to five minutes, and defibrillation at 4 joules per kilogram for a shockable rhythm. These are anchors for the escalation point, not a full arrest algorithm; the complete pathway lives in the paediatric basic and advanced life support topic. [9] [10]
[9]Management — Definitive & Stepwise
After immediate resuscitation, move into the pathway for the likely cause without stopping reassessment. This hub does not reproduce the full shock, ventilation, status, antimicrobial, toxicology or glucose algorithms; treat the most reversible dangerous problem first while keeping other serious causes open. [3] [9]
From immediate treatment to the right ongoing plan
Name the expected result
Before acting, state the change you expect in airway patency, breathing effectiveness, interaction, perfusion, urine output or device function.
Measure what happened
Repeat the affected ABCDE areas and observations. Distinguish sustained improvement, brief improvement, no response and harm.
Choose the cause-specific pathway
Move to respiratory support, shock, sepsis, status, toxicology, metabolic, trauma, cardiac or safeguarding care as the evidence becomes clearer.
Stop harmful repetition
Do not repeat a treatment because the first label felt right. Reconsider the cause, fluid overload, access problems and whether more support is needed.
Agree monitoring and contingency
Specify the location, staff, observation intensity, response owner, next sign of failure and what to do if transfer is delayed.
Hand over and dispose
Transfer baseline, trend, timed actions, response, unresolved risks, tests, devices, family and safeguarding information, and the next action.
Improvement must make sense across several findings. An open airway must also remain open. Less work of breathing is reassuring only when air entry and interaction improve. Better blood pressure does not prove adequate perfusion. A corrected glucose needs a documented recheck and a plan for the cause. Reassess after each action and meaningful change rather than waiting for a fixed interval. [2] [9]
Early PICU and retrieval consultation
Call PICU or retrieval when the child may need support your service cannot reliably provide, not after every local option has failed. Discuss the likely support, present monitoring and access, equipment and staff limits, transport time and weather, the safest destination, the escort, expected deterioration and what to do if transfer is delayed. Exact referral thresholds, escort arrangements, transport mode and accepting service remain local or regional. [9]
| Domain | Content that must cross the boundary |
|---|---|
| Identity and baseline | Age, measured or estimated weight, development, usual observations, communication, function, devices and emergency plan |
| First impression and physiology | PAT pattern, current ABCDE findings, age-adjusted observations and direction of change |
| Actions and response | Intervention, time, route, expected result, actual response and adverse effect |
| Reasoning | Prioritised threat-based differential, key tests, pending results and unresolved risks |
| Local limits | Access, equipment, staff, airway or critical-care limits, transport constraints and requested destination or support |
| Child and family | Caregiver concern, communication needs, professional interpreter, family understanding and preferences |
| Safety | Safeguarding information, objective documentation, immediate safety plan and the jurisdictional pathway already activated |
| Contingency | Next failure marker, action if deterioration occurs and named ownership until transfer is complete |
A structured handoff program reduced medical errors and preventable adverse events in a multicentre study of resident physicians; the principle generalises to acute handover, where the loss of trend, timed actions and contingency is a recurrent source of harm. Keep the caregiver informed, speak to the child at their developmental level, use a professional interpreter when needed, and check understanding. [8]
Specific Subtypes & Scenarios
The survey stays the same, but age, presentation, baseline and setting change what you look for and how early you escalate. In each scenario: stabilise first, identify what is failing, activate the correct pathway, and state which facts are specific to that source or setting. [9]
Neonate or young infant
- Treat feeding, behaviour, tone or temperature change as significant even without fever
- Clarify perinatal and transition history
- Check bedside glucose early and seek senior review
- Use Newborn Life Support at birth; state the local NLS to PLS boundary
Threatened airway
- Observe sound, position and effort before provoking distress
- Keep the child upright in a position of comfort when safe
- Call airway expertise early, before failure
- Do not delay support for diagnostic examination
Tiring breathless child
- Consider fatigue and falling air entry before assuming improvement
- Reassess effectiveness, not rate alone
- Support breathing and escalate before complete failure
- A quieter child after marked effort is failing until proved otherwise
Anaphylaxis
- Airway and breathing first, then IM adrenaline
- Recognise the continuum: food or sting exposure, rapid onset, skin plus respiratory or circulatory features
- Give fluid for shock and repeat adrenaline as the local pathway allows
- Keep asthma, sepsis and vasovagal causes open
Seizing or post-ictal child
- Protect airway and breathing; time the seizure
- Check glucose and correct a dangerous low now
- Activate status care at 5 minutes of convulsion
- Keep infection, toxin, metabolic and neurological causes open
Technology-dependent child
- Assess the child and the device in parallel
- Ask what normal device function looks and sounds like
- Use the personal emergency plan and the specialty pathway
- Bring caregiver expertise into the escalation and handover
Trauma
- Primary survey first; preserve cervical spine and temperature
- Do not wait for hypotension
- Reassess after handling because movement can change physiology
- Consider non-accidental injury when the history requires it
Adolescent collapse
- Stabilise first, then create private history time when safe
- Ask directly about substance exposure, self-harm, eating restriction and pregnancy
- Explain confidentiality and its safety limits
- Do not use adult assumptions to bypass paediatric services
Congenital heart disease
- Obtain the individual saturation and circulation baseline
- Use the personal emergency plan and early subspecialty input
- Do not apply a universal oxygen or fluid target
- Consider cardiac and obstructive physiology when the presentation looks respiratory
Possible poisoning
- Stabilise physiology while substance, dose and time remain uncertain
- Seek containers, medication lists and collateral
- Use targeted ECG, glucose and toxicology when they change the branch
- Activate the local toxicology pathway
Immunocompromised child
- Absence of fever does not close serious infection
- Compare with baseline and recent treatment
- Sample without delaying treatment for instability
- Escalate on physiology and risk context
Rural or remote setting
- Call retrieval before the child needs support unavailable locally
- State equipment, staff, weather, distance and communication limits
- Agree a delayed-transfer contingency driven by acuity
- Package monitoring, access and handover for transport
Telehealth
- Video cannot replace palpation, air entry or perfusion measurement
- A poor connection or uncertain exam lowers the threshold for in-person review
- Give a specific access route and contingency, not generic reassurance
Complications & Pitfalls
Most harm begins when assessment stops too early. A normal number, a convenient explanation or a brief response is accepted as the answer, so the child is not reassessed. Prevent this by recording the current problem, the serious alternatives, the expected result, the actual response and the next escalation action. [2] [9]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Reassuring single sign ends the survey | Occult or evolving illness is missed | Respond to trend, baseline and concern, not one observation |
| Quieter breathing labelled recovery | Fatigue and falling air entry are misread | Seek concordant improvement in effectiveness and interaction |
| Blood pressure or capillary refill used alone | Compensation creates false reassurance | Integrate multiple perfusion signs and direction of change |
| Abnormal observations blamed on fever, crying or pain | A modifier becomes premature closure | Reassess after comfort; explain persistent abnormalities |
| Adult equipment, drug doses or assumptions | Age, weight and reserve are ignored | Use age and weight, local paediatric charts and the cognitive aid |
| Fluid ceiling turned into a target | Fluid overload and harm | State the expected response; stop for overload or no benefit |
| Imaging or procedure before stability | Transport, sedation or delay destabilises | Ask whether the result changes the immediate branch and whether movement is safe |
| Caregiver or nursing concern discounted | Early deterioration information is lost | Elicit, document and escalate irrespective of score |
| Poor handover | Trend, timed actions and contingency disappear | Use a structured transfer with read-back and named ownership |
| Safeguarding postponed for diagnosis | Immediate safety and evidence are lost | Stabilise first while objective documentation and the pathway proceed in parallel |
Watch for anchoring on the referral diagnosis, ordering tests only to confirm it, and carrying forward a label that silences bedside concern. After stabilisation, look actively for harm from treatment: airway or access complications, fluid overload, heat loss, repeated sampling, medication or device error, and pressure or restraint injury. The fact that the child did not arrest does not prove an intervention was harmless. [4] [9]
[3] [9]Prognosis & Disposition
Disposition follows the trend and response, not one reassuring observation. Consider the child's age and reserve, the duration and severity of organ dysfunction, reversibility, treatment harm, local support, transport risk, and whether the family can carry out the plan. [3] [9]
Critical care or retrieval
- Unresolved or worsening ABCDE threat
- Need for support, monitoring or expertise unavailable locally
- Repeated or transient response with likely further deterioration
- Transport risk that needs early specialist planning
Ward or high-dependency
- Physiology currently supported but trend, age or diagnosis needs close reassessment
- Monitoring and staffing can detect and respond to failure
- Pending tests or treatment response still change disposition
- A named escalation pathway exists
Discharge only when defensible
- Sustained improvement or stability after appropriate reassessment
- No unresolved immediate threat or high-harm diagnostic concern
- Caregiver concern addressed and understanding confirmed
- Specific warning changes, access route, follow-up and pending-result ownership agreed
A useful safety net states what change to watch for, how urgently to act, and exactly where or how to get help. It also states when review will occur, who owns pending results, and what to do if access is difficult. "Return if worried" alone is not enough. Check understanding with teach-back, document it, and connect the family to the medical home, primary care or community team. After a critical event, explain what happened and what remains uncertain, invite questions, and consider debriefing for the child, family and team. [9]
Special Populations
Adapt how you observe, communicate and examine, but never lower the standard for recognising deterioration. Evidence is sparse for recognition tools in disability, neurodiversity, technology dependence and many low-resource settings; present these adaptations as safer practice, not as proven improvements in diagnostic accuracy. [9]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Neonate or young infant | Treat non-specific change as high-risk; check glucose early; use Newborn Life Support at birth | State the local NLS to PLS boundary; do not apply an older-child pathway at birth |
| Complex or technology-dependent child | Establish personal baseline, device function and emergency plan; assess child and device in parallel | A chronically abnormal observation is not automatically safe; compare with the personal baseline |
| Severe neurodisability | Establish usual interaction, tone, movement and pain expression; treat caregiver-described change as evidence | Adaptation improves communication, not proven diagnostic sensitivity |
| Immunocompromised child | Absence of fever does not exclude serious infection; sample and escalate on context | Do not delay time-critical treatment for complete sampling in an unstable child |
| Adolescent | Create private time; ask about substances, self-harm and pregnancy; explain confidentiality limits | Confidentiality has safety limits; safeguarding duties still apply |
| Indigenous, migrant or remote family | Use cultural safety and a professional interpreter; address access and transport barriers | Retrieval and safeguarding routes remain jurisdiction-specific |
Safeguarding runs in parallel with medical care, but immediate stabilisation and safety come first. Ask only necessary open, non-leading questions. Explain confidentiality and information sharing, document objective findings and spontaneous words, preserve evidence when safe, and use the local safeguarding pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [9]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The ABCDE structure itself is consensus: the AHA 2020 Paediatric Basic and Advanced Life Support guideline and the ILCOR 2020 Paediatric Life Support consensus both teach a primary survey that finds and treats life threats in the airway-breathing-circulation order and returns to reassess. The order of the letters is not in dispute; the doses, targets and thresholds attached to each step are source- and population-specific. [9] [10]
FEAST
New England Journal of Medicine
Randomised fluid-bolus trial in African children with severe febrile illness
Key finding
Saline or albumin bolus increased 48-hour mortality compared with no bolus in that population.
Practice change
Fluid strategy must stay specific to the population, shock type and available rescue; do not transplant protocols uncritically.
The Surviving Sepsis Campaign 2026 children's guideline supports early recognition and first-hour fluid resuscitation with vasoactive support for septic shock, with explicit attention to fluid balance. It is a global specialist guideline whose details (crystalloid choice, aliquot size, vasoactive first agent) are read alongside local resources and the child's shock type. [11]
Capillary refill has modest diagnostic value and is highly technique-dependent, early-warning scores depend on the whole response system, and pulse oximetry can overestimate oxygenation in darker skin. There is no universal vital-sign range, oxygen target, fluid volume, glucose threshold or weight-estimation formula that fits every child. Attach each rule to its population, purpose, conditions and jurisdiction. [1] [2]
Jurisdictional implementation
Australia and Aotearoa New Zealand: ANZCOR Guideline 12.2 is the 2026 regional paediatric advanced life support source. The Royal Children's Hospital Melbourne acceptable ranges for physiological variables and the altered-conscious-state and hypoglycaemia guidelines support local implementation. Retrieval systems, observation charts, mandatory reporting and consent remain state-, territory- or service-specific. In Aotearoa New Zealand, verify the active local deterioration, retrieval and safeguarding system rather than borrowing an Australian threshold.
Global and low-resource settings: WHO ETAT adapts emergency triage, assessment and treatment mainly for low-resource hospitals and non-specialists. Its population-specific shock definition and slower fluid approach must stay attached to that context, which is exactly the lesson FEAST reinforces.
Exam Pearls
Doorway
- Recognise the unwell child and call for help
- State the paediatric assessment triangle findings
- Treat life threats before diagnosing
Primary survey
- ABCDE in order; treat each threat as found
- Use age, weight and personal baseline
- Check the reversible threats: hypoxia, hypovolaemia, hypoglycaemia, tension, tamponade, toxins, thrombosis
- Reassess from A after every action
Resuscitation facts
- 100% oxygen in failure, then titrate to 94 to 98%
- Fluid bolus is a ceiling, not a target
- Status pathway at 5 minutes
- Correct dangerous low glucose now
- Adrenaline 10 micrograms/kg IV/IO; defibrillation 4 J/kg at arrest
Escalation
- Call senior, PICU or retrieval before local support is exceeded
- State failure markers and contingency
- Give a structured handover
- Keep family and safeguarding information moving
Pitfalls
- No hypotension-waiting for shock
- No quieter-chest assumption
- No fluid ceiling as target
- No adult doses or equipment
- No retrieval delay
“Recognise and call for help → ABCDE treating each threat as found → check reversible causes → reassess from A → escalate before local support is exceeded → structured handover and safe disposition.”
Viva: the tachypnoeic child becomes quiet
Do not say "improved" until you reassess effectiveness. Recheck air entry, work, respiratory rate, a credible saturation, interaction, perfusion and glucose. Less effort with poorer air entry or reduced interaction means fatigue and impending failure. Support breathing, state the improvement you expect, call airway or critical-care help, and reassess from A.
Viva: when does ABCDE become a cardiac arrest algorithm?
When the child is unresponsive with absent or agonal breathing and no central pulse. Move directly into the paediatric arrest algorithm: high-quality chest compressions, ventilation with oxygen, and the arrest-dose anchors of intravenous or intraosseous adrenaline 10 micrograms per kilogram every three to five minutes and defibrillation at 4 joules per kilogram for a shockable rhythm. Do not finish a survey of an arrested child.
Structured oral: rural retrieval of a deteriorating child
State the current ABCDE problem and the treatment under way. Ask what monitoring, airway, vascular-access, staff and transport resources are available. Call retrieval early, agree the destination, the treatment to continue, the expected response, the deterioration plan and the handover, and explain uncertainty and transport delay to the family. Do not wait until all local options have failed.
References
- [1]Fleming, Susannah Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies Lancet (London, England), 2011.PMID 21411136
- [2]Fleming, Susannah The Diagnostic Value of Capillary Refill Time for Detecting Serious Illness in Children: A Systematic Review and Meta-Analysis PloS one, 2015.PMID 26375953
- [3]Bjorklund, Ashley Pediatric Shock Review Pediatrics in review, 2023.PMID 37777656
- [4]Maitland, Kathryn Mortality after fluid bolus in African children with severe infection The New England journal of medicine, 2011.PMID 21615299
- [5]Young, Kelly D Weight Estimation Methods in Children: A Systematic Review Annals of emergency medicine, 2016.PMID 27105839
- [6]McIntyre, John Safety and efficacy of buccal midazolam versus rectal diazepam for emergency treatment of seizures in children: a randomised controlled trial Lancet (London, England), 2005.PMID 16023510
- [7]Faustino, E Vincent S Hypoglycemia in critically ill children Journal of diabetes science and technology, 2012.PMID 22401322
- [8]Starmer, Amy J Changes in medical errors after implementation of a handoff program The New England journal of medicine, 2014.PMID 25372088
- [9]Topjian, Alexa A Part 4: Pediatric Basic and Advanced Life Support 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Pediatrics, 2021.PMID 33087552
- [10]Maconochie, Ian K Pediatric Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations Circulation, 2020.PMID 33084393
- [11]Weiss, Scott L Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026 Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2026.PMID 41869844