Paeds · acute-care-resuscitation-and-toxicology
Airway assessment and basic airway management
Also known as Paediatric airway management · Basic airway management in children · Bag-valve-mask ventilation in children · Airway opening manoeuvres · Airway adjuncts in children
Fellowship guide to paediatric airway assessment and basic airway management: how the child's airway differs from the adult's, recognising the threatened and the failing airway at the bedside, head tilt-chin lift and jaw thrust, sizing and selecting oropharyngeal and nasopharyngeal airways, and effective two-person bag-valve-mask ventilation, with escalation triggers to a definitive airway.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who is unconscious, obstructing, or not breathing will die of a blocked airway long before any other problem is addressed, which makes opening and ventilating that airway the single most decisive thing a clinician can do in the first minute of paediatric resuscitation. Basic airway management is the set of immediately available, non-invasive techniques that achieve this before any tracheal tube or supraglottic device is placed. It rests on three skills: opening the airway with a manoeuvre, keeping it open with an adjunct, and ventilating it with a bag-valve-mask. [1]
Because most paediatric cardiopulmonary arrests are respiratory rather than primary cardiac, competent basic airway management is the skill most likely to prevent the arrest altogether. A child whose airway is opened and ventilated early often recovers dramatically, and the airway and breathing that follow it determine whether circulation ever has a chance. [3]
Classification
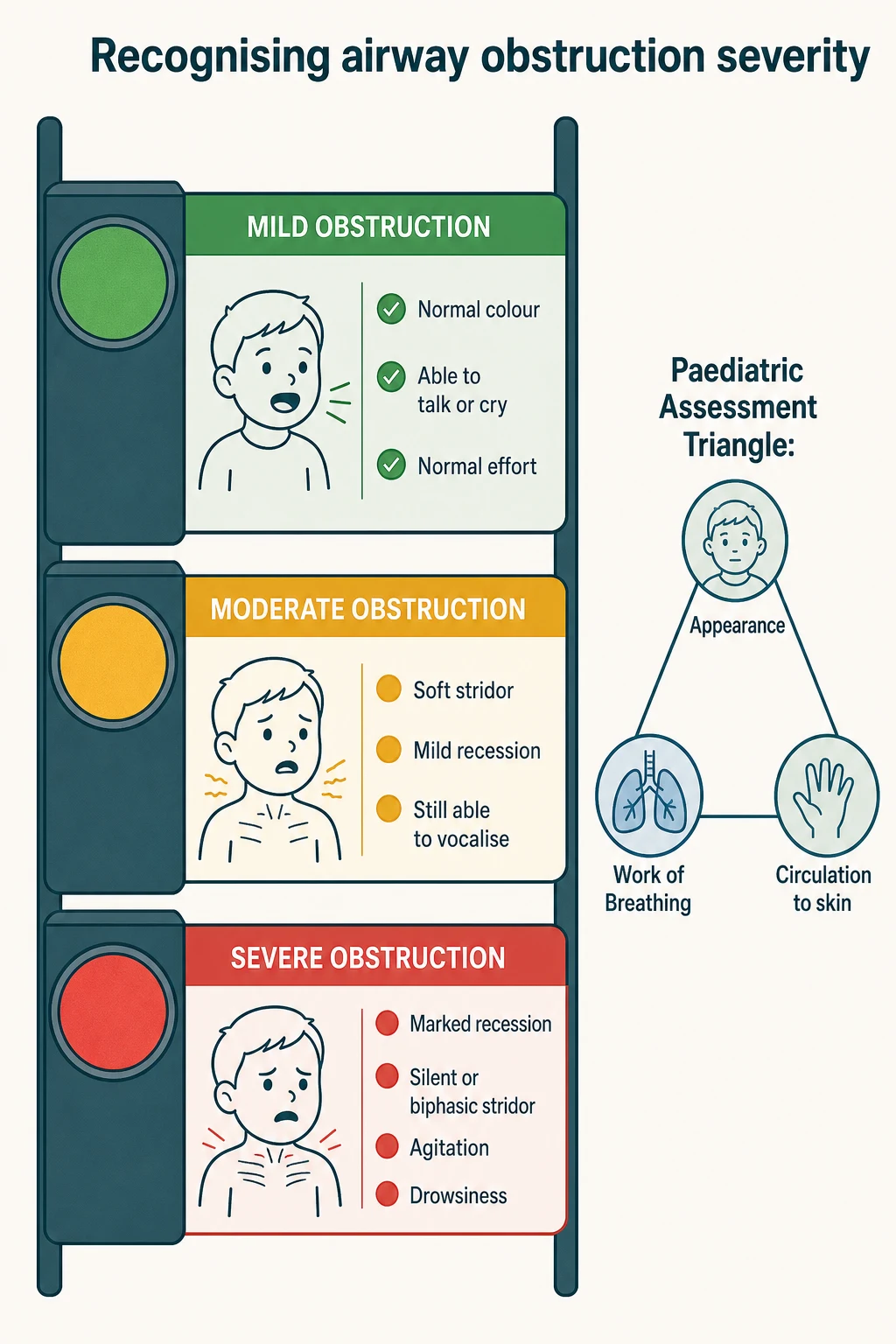
The practical classification is by how badly the airway is threatened, because that determines what you do next. A safe airway is open, the child is pink and alert, and breathing is easy and silent. A threatened airway is noisy and working: there is stridor, recession, or nasal flaring, but air is still moving and the child is compensating. A lost or failing airway is quiet against a background of exhaustion: the effort falls, the noise softens, and the child becomes drowsy or bradycardic. [1]
[2]It helps to classify the noise itself by where it points. Snoring points to the tongue and soft palate and responds to a manoeuvre or adjunct. Gurgling points to liquid in the airway and responds to suction. Stridor points to extrathoracic narrowing such as croup or epiglottitis, wheeze points to intrathoracic narrowing, and silence is either a clear airway or complete obstruction, which you tell apart by feeling for air at the mouth. [8]
Epidemiology & Risk Factors
Most paediatric arrests are asphyxial: hypoxia from airway obstruction, hypoventilation, or apnoea is the proximate cause, and the heart stops only after the oxygen has run out. This is the central reason that basic airway management, done early and well, prevents death in the sick child. [3]
Some children are harder to manage than others, and recognising them in advance prevents panic. Infants under one year carry the most adverse airway anatomy and the least tolerance of hypoxia. Obesity, micrognathia, and craniofacial syndromes make mask ventilation and airway maintenance harder, and Down syndrome combines a large tongue, a small midface, and hypotonia. A reduced conscious level, copious secretions, and upper airway infection all raise the chance that the airway will obstruct. [4]
The PeDI registry, a large multicentre dataset, has shown that difficult or impossible mask ventilation in children is closely linked to difficult tracheal intubation, and that the two problems tend to travel together in the same child. This is why the responder who struggles to mask-ventilate should summon senior help immediately rather than persist alone. [5]
Pathophysiology
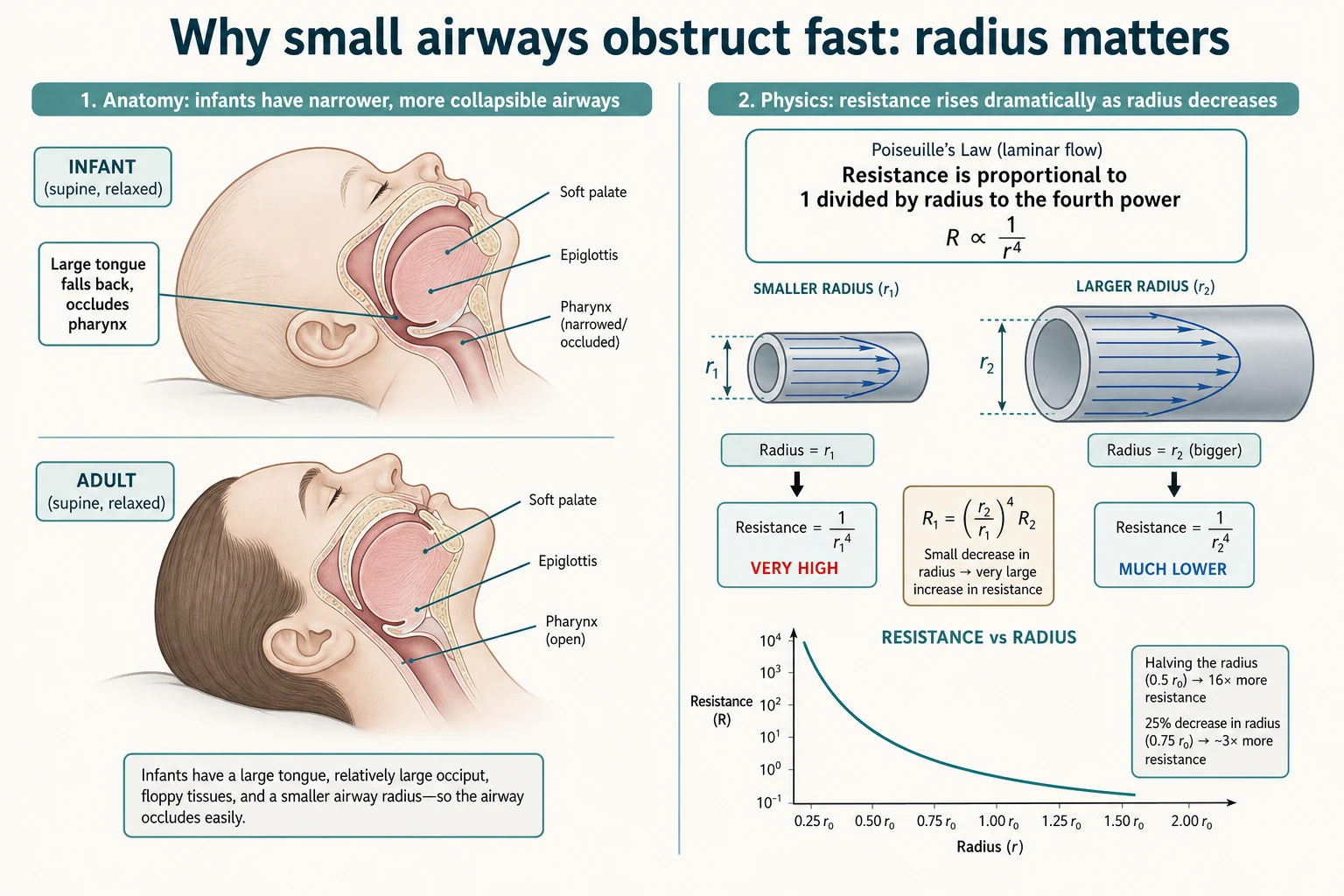
A child's airway is not a small adult airway, and the differences explain both why children obstruct so readily and why the techniques of basic management work the way they do. The infant has a large occiput that flexes the neck when supine, a tongue that is large relative to the oral cavity and falls back against the posterior pharynx when tone is lost, and a larynx that sits high and anterior, around the level of the third and fourth cervical vertebrae rather than the fifth and sixth. [4]
Two more features complete the picture. The infant epiglottis is long, stiff, and U-shaped, and it angles down over the laryngeal inlet, which matters when a tongue depressor or an airway adjunct is mis-sized. Most importantly, the narrowest point of the child's airway is the cricoid cartilage, a fixed ring below the vocal cords, whereas in the adult the narrowest point is the vocal cords themselves. [4]
The physics of airflow is what turns these anatomy differences into clinical danger. Because airway resistance is proportional to the inverse of the radius raised to the fourth power, a fixed millimetre of circumferential narrowing or tongue displacement narrows a child's small airway far more, in relative terms, than the same narrowing in an adult. A small child can therefore move from partial to complete obstruction within minutes. [3]
Clinical Presentation
Assess the airway and breathing together, and begin from across the room. The paediatric assessment triangle reads appearance, work of breathing, and circulation to skin without touching the child, and it tells you instantly whether the child is sick and whether the threat is respiratory. A child who is alert and pink with easy breathing has time; a child who is still, recessed, and pale does not. [1]
At the airway itself, use look, listen, and feel over about five seconds. Look for chest and abdominal movement and for colour. Listen at the nose and mouth for noise: snoring, gurgling, stridor, or wheeze each localises the problem. Feel for air movement at the mouth, because silence is ambiguous until you confirm whether air is moving. [2]
Look-listen-feel at the airway
Look for chest rise, abdominal movement, and colour from across the room
Listen at the nose and mouth for snoring, gurgling, stridor, or wheeze
Feel for expired air at the mouth for about five seconds
Classify the noise to localise the obstruction
Judge effort: tracheal tug, subcostal and intercostal recession, nasal flaring
Watch for the pre-terminal quiet phase of softening noise and falling effort
Increasing work of breathing shows that the child is compensating, and it is reassuring while it lasts: tracheal tug, subcostal and intercostal recession, and nasal flaring all mean the child is still trying. The danger comes when the effort falls, because a tiring child generates less noise and less movement while the obstruction worsens. Cyanosis is a late and unreliable sign in children, so do not wait for it. [2]
Differential Diagnosis
The responder's differential at the bedside is simpler than the anatomical list, and it is the one that drives action. First decide whether the obstruction can be opened by basic technique or whether it needs a definitive airway and expert help. If the problem is the tongue and soft tissues, a manoeuvre and an adjunct will open it. If it is liquid, suction will clear it. If it is a fixed pathological narrowing, such as epiglottitis or a foreign body, basic technique buys time but the child needs escalation. [8]
By level, the causes run from nose to alveolus. Nasal obstruction matters most in the newborn obligate nose-breather with choanal atresia. Oropharyngeal obstruction by the tongue is the commonest problem in the unconscious child. Supraglottic causes include epiglottitis and angio-oedema, glottic and subglottic causes include croup and a laryngeal foreign body, and intrathoracic causes include asthma, bronchiolitis, and an inhaled foreign body. [12]
A witnessed choking event with sudden stridor or cough, without fever, points to an inhaled foreign body and demands a different response: back blows and chest thrusts in the conscious infant, and basic life support if the child collapses. This is one obstruction that basic airway adjuncts will not relieve, and recognising it changes the immediate action. [1]
Clinical & Bedside Assessment
Bedside assessment is fast and decisive. After the look-listen-feel sweep, classify the airway as safe, threatened, or failing, and act on that classification rather than waiting for investigations. Reassess constantly, because a threatened airway can become a failing one within minutes. [2]
Adjunct sizing is a bedside skill the responder must master, because a mis-sized device worsens the obstruction. An oropharyngeal airway is sized from the corner of the mouth to the angle of the jaw or the earlobe, and the GUEDEL-I study, which used magnetic resonance imaging in children, confirmed that this facial-landmark method estimates the correct size more reliably than guessing. [6]
A nasopharyngeal airway is sized from the tip of the nose to the tragus of the ear, and it is the adjunct of choice when the child still has airway reflexes, because an oropharyngeal airway would provoke gagging and vomiting. The oropharyngeal airway is reserved for the deeply unconscious child with no gag reflex. Choosing the wrong adjunct for the level of consciousness is a common and avoidable error. [9]
Investigations
No investigation precedes opening and ventilating an obstructed airway. Basic airway management is a clinical, bedside act, and the first test is whether the chest rises with the mask. Sending an unstable child to radiology before the airway is controlled is a classic and dangerous error, because moving or lying the child flat can precipitate complete obstruction. [2]
Once the airway is open and the child is stabilised, the directed workup follows the cause. A lateral neck radiograph may show the thumbprint of epiglottitis or the widened retropharyngeal space of an abscess, but only in a stable child and never as a condition for acting on the airway. Endoscopy confirms and treats bacterial tracheitis and an inhaled foreign body. [12]
Continuous monitoring is part of safe airway care. Apply pulse oximetry from the outset, remembering that it lags behind the failing airway, and add end-tidal carbon dioxide monitoring once the child is ventilated or intubated to confirm and track ventilation. These monitors support but never replace the clinical look-listen-feel. [1]
Management — Resuscitation
The resuscitation sequence is airway then ventilation, performed in the first minute. Open the airway with a head tilt and chin lift in the unconscious child, or a jaw thrust without head tilt if cervical spine injury is possible. Suction any liquid. Insert an oropharyngeal airway in the deeply unconscious child with no gag, or a nasopharyngeal airway if reflexes are present. Give high-flow oxygen, and ventilate with a bag-valve-mask if breathing is inadequate. [1]
Position the head correctly for the age. The infant's large occiput flexes the neck when supine, so a neutral position, not the sniffing position used in older children, opens the infant airway. Over-flexion or over-extension of the neck obstructs the infant airway, which is why a small towel under the shoulders can help align the airway in a young infant. [2]
The first-minute airway sequence
Open the airway: head tilt and chin lift, or jaw thrust if trauma is possible
Suction liquid obstruction from the mouth and oropharynx
Insert an adjunct: oropharyngeal if unconscious, nasopharyngeal if reflexes present
Apply high-flow oxygen by mask
Ventilate with bag-valve-mask if breathing is inadequate
Call for senior anaesthetic and intensive care help early
If the airway cannot be maintained by basic technique, escalate at once. Summon the most senior anaesthetist available, prepare a supraglottic airway and tracheal intubation equipment, and have a smaller and larger tube ready. Effective bag-valve-mask ventilation is the bridge that keeps the child alive while the definitive airway is assembled. [5]
Management — Definitive & Stepwise
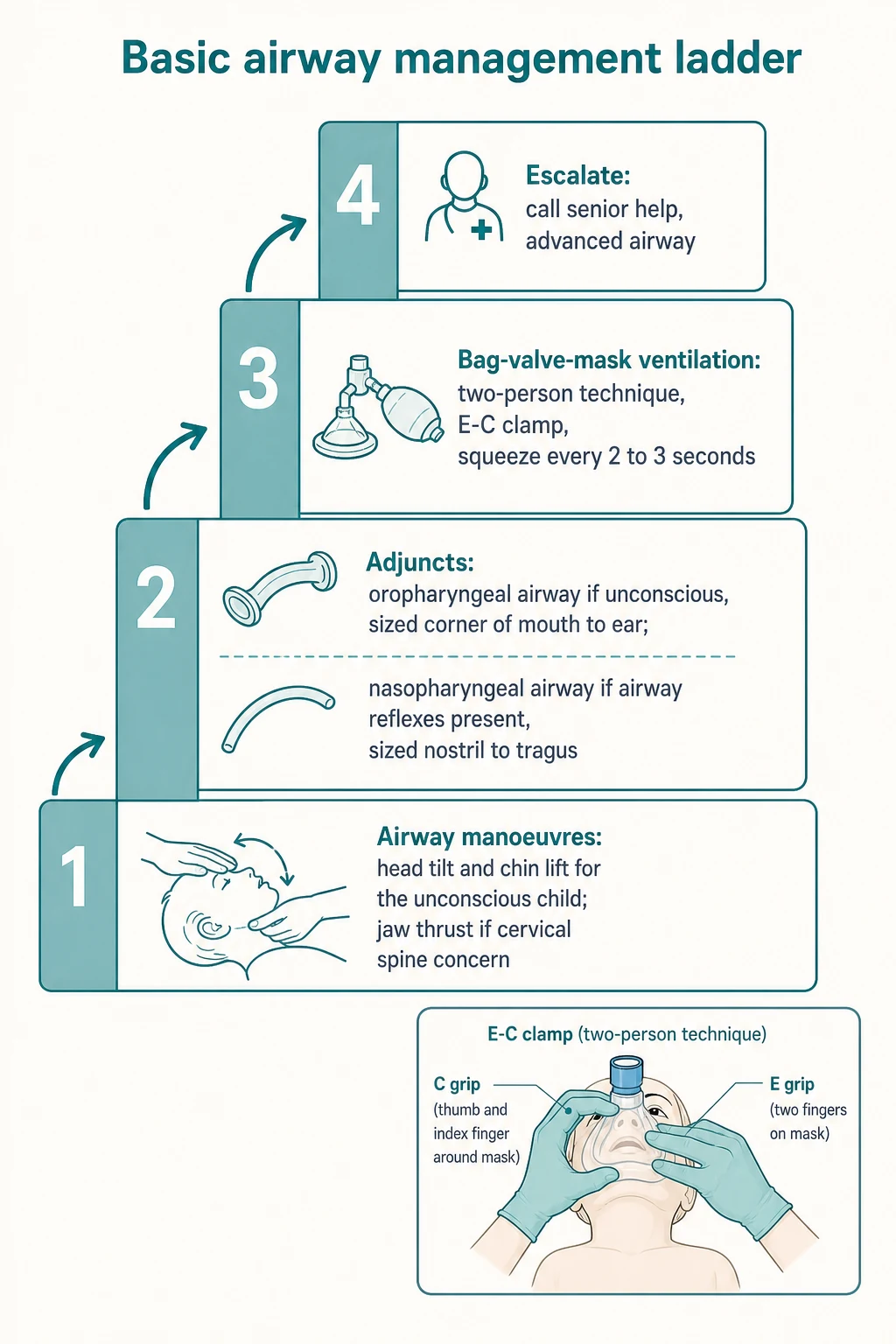
The ladder runs from manoeuvre to adjunct to ventilation to escalation. Step one is the airway manoeuvre: head tilt and chin lift for the unconscious child, or jaw thrust with manual in-line stabilisation when cervical spine injury is suspected, never hyperextending the neck. [1]
Step two is suction and adjunct placement. Suction visible fluid under direct vision, then place an oropharyngeal airway in the unconscious child without a gag reflex, inserting it carefully to avoid pushing the tongue back, or a nasopharyngeal airway in the child with preserved reflexes. An oropharyngeal airway is inserted in the older child with the curve following the roof of the mouth and then rotated, but in the infant it is inserted directly under direct vision to avoid trauma, because rotation can injure the mouth. [8]
Bag-valve-mask ventilation (basic airway)
Dose
One breath every 2 to 3 seconds, about 20 to 30 breaths per minute, using just enough volume for normal chest rise
Step three is oxygen and bag-valve-mask ventilation. Use a two-person technique whenever a second rescuer is available: one rescuer holds the mask to the face with a two-hand E-C or thenar eminence grip while the other squeezes the bag. Ventilate with one breath every two to three seconds, about twenty to thirty per minute, using only enough volume to produce normal chest rise. [10]
The basic airway ladder
The two-person technique matters because it produces a better seal and better ventilation than one-person bag-valve-mask. Studies comparing hand grips have found that the thenar eminence and two-hand E-C grips both give superior mask seal and ventilation compared with the one-hand technique, which is why the second rescuer is so valuable when available. [7]
Step four is escalation. Call for senior help early, prepare a supraglottic airway and tracheal intubation, and move to a definitive airway if basic techniques fail. For the unconscious child who is breathing adequately once the airway is open, place them in the recovery position while help is summoned, provided the airway is protected and monitored. [12]
Specific Subtypes & Scenarios
The neonate and young infant need special positioning. The large occiput flexes the neck when the baby is supine, so the airway opens best in a neutral position, and over-flexion or over-extension obstructs it. A small towel under the shoulders can align the head and neck in a small infant, and the newborn obligate nose-breather obstructs with nasal blockage, so keeping the nose clear matters. [2]
The child with suspected cervical spine injury is managed with a jaw thrust and manual in-line stabilisation, never head tilt. The airway still comes first, and the small risk of worsening a spinal injury is never a reason to leave an airway obstructed; the principle is to open the airway while minimising neck movement. [1]
The syndromic child, such as one with Down syndrome, Pierre Robin sequence, or Treacher Collins syndrome, should be anticipated as a difficult airway. Position early, have senior help present from the start, and in the micrognathic infant whose tongue obstructs, a nasopharyngeal airway or prone positioning can relieve obstruction while help arrives. [11]
[3]The child with copious vomit or blood needs aggressive suction, a head-down lateral position, and readiness to intubate to protect the lungs, because aspiration compounds the airway problem. The seizing or post-ictal child loses tone and obstructs, so positioning and an adjunct come first while the seizure is treated. [8]
Complications & Pitfalls
The gravest error is failing to recognise the quietly failing airway. A child whose stridor softens, whose effort falls, or who becomes drowsy and bradycardic is obstructing, not improving, and the responder who reads this as recovery loses the window to act. Every reassessment must look for the pre-terminal quiet phase. [2]
Technical pitfalls cluster around the adjuncts and the mask. An oropharyngeal airway placed in a child with a gag reflex provokes vomiting and aspiration; one that is too long pushes the epiglottis down and worsens obstruction; one inserted with the rotation technique in an infant can injure the mouth. A nasopharyngeal airway that is too long, or one forced into a child with a basilar skull fracture or coagulopathy, can cause harm. [8]
Bag-valve-mask errors cause real harm. A one-person technique with a poor seal leads to gastric insufflation, regurgitation, and aspiration, and ventilation that is too forceful or too fast causes gastric distension, pneumothorax, and reduced cardiac output. The remedy is the two-person technique, an appropriate rate, and enough volume only for normal chest rise. [10]
Prognosis & Disposition
When the airway is opened and ventilation restored promptly, the child often recovers dramatically, and the outlook is then that of the underlying illness rather than the airway event itself. Because most paediatric arrests are respiratory, effective basic airway management can prevent progression to cardiac arrest entirely, which is why it is the most life-saving skill in paediatric resuscitation. [3]
Children who remain dependent on basic airway techniques, or in whom those techniques falter, need prompt escalation to a definitive airway by experienced staff. The responder's job is to keep the child oxygenated and ventilated until that help arrives, and to recognise early when basic measures are not enough. [5]
Any child who has required airway manoeuvres, adjuncts, or bag-valve-mask ventilation belongs in a resuscitation area with continuous monitoring and early anaesthetic or intensive care involvement. Children retrieved between hospitals need airway-capable staff in transit, because the safest place for an airway to fail is not the back of an ambulance. [2]
Special Populations
Neonates and infants carry the most adverse airway anatomy, the smallest faces and most difficult masks, and the lowest tolerance of hypoxia, and they are the group in whom bag-valve-mask ventilation is both hardest and most often needed. Neutral head positioning, correctly sized masks, and a low threshold for senior help define good care in this group. [2]
Children with neurodisability often have chronic hypotonia, copious secretions, and scoliosis, all of which make obstruction recurrent. Families usually know the child's usual airway and the position that opens it best, and listening to them is both safer and faster than starting from scratch in a crisis. [12]
Technology-dependent children with a tracheostomy or home ventilation follow their own airway plan. Carry the spare tracheostomy tube, know how to change it, and involve the family, who are often the most expert people at the bedside. Basic principles still apply: open, oxygenate, ventilate, and escalate. [12]
[3]Indigenous and remote communities across Australia and New Zealand carry a higher burden of acute respiratory illness combined with distance from tertiary services, so culturally safe care, interpreter access, reliable retrieval pathways, and clear family safety-netting are part of equitable airway management. Early escalation matters most where the definitive airway is furthest away. [2]
Evidence, Guidelines & Regional Differences
The international guidance converges on the same core. The 2025 American Heart Association and American Academy of Pediatrics Pediatric Basic Life Support guidance, the 2021 European Resuscitation Council Paediatric Life Support guideline, and the 2020 International Liaison Committee on Resuscitation consensus all teach head tilt-chin lift with jaw thrust in trauma, adjunct use, and two-person bag-valve-mask ventilation as the cornerstones of paediatric basic airway care. [1]
[7]Large registries have strengthened the evidence base. The PeDI registry has quantified how often difficult mask ventilation accompanies difficult intubation in children, making a case for early escalation, and the GUEDEL-I magnetic resonance imaging study has validated the facial-landmark method for sizing the Guedel oropharyngeal airway, replacing guesswork with an evidence-based estimate. [5]
Controversies persist. The optimal one-hand versus two-hand grip for the single rescuer, the routine use of cricoid pressure during bag-valve-mask ventilation, which is not recommended in children, and the place of apnoeic oxygenation and high-flow nasal cannula during basic airway care remain active areas of study, with emerging equipment and techniques continually reshaping paediatric airway management. [12]
Exam Pearls
Why the child's airway is dangerous — FLARED
References
- [1]Joyner BL Jr Part 6: Pediatric Basic Life Support: 2025 American Heart Association and American Academy of Pediatrics Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2025.PMID 41122891
- [2]Van de Voorde P European Resuscitation Council Guidelines 2021: Paediatric Life Support. Resuscitation, 2021.PMID 33773830
- [3]Maconochie IK Pediatric Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation, 2020.PMID 33084393
- [4]Holzki J The anatomy of the pediatric airway: Has our knowledge changed in 120 years? A review of historic and recent investigations of the anatomy of the pediatric larynx. Paediatr Anaesth, 2018.PMID 29148119
- [5]Garcia-Marcinkiewicz AG Difficult or impossible facemask ventilation in children with difficult tracheal intubation: a retrospective analysis of the PeDI registry. Br J Anaesth, 2023.PMID 37076335
- [6]Nemeth M Guedel oropharyngeal airway: The validation of facial landmark-distances to estimate sizing in children - Visualisation by magnetic resonance imaging (GUEDEL-I): A prospective observational study. Resuscitation, 2023.PMID 36702339
- [7]Soleimanpour M Comparison of four techniques on facility of two-hand Bag-valve-mask (BVM) ventilation: E-C, Thenar Eminence, Thenar Eminence (Dominant hand)-E-C (non-dominant hand) and Thenar Eminence (non-dominant hand) - E-C (dominant hand). J Cardiovasc Thorac Res, 2016.PMID 28210469
- [8]Castro D Oropharyngeal Airway. StatPearls [Internet], 2026.PMID 29261912
- [9]Atanelov Z Nasopharyngeal Airway. StatPearls [Internet], 2026.PMID 30020592
- [10]Bucher JT Bag-Valve-Mask Ventilation. StatPearls [Internet], 2026.PMID 28722953
- [11]Fiadjoe J Pediatric difficult airway management: current devices and techniques. Anesthesiol Clin, 2009.PMID 19703672
- [12]Stein ML Emerging trends, techniques, and equipment for airway management in pediatric patients. Paediatr Anaesth, 2020.PMID 32022437