Paeds · acute-care-resuscitation-and-toxicology
Altered conscious state in children
Also known as Altered mental status in children · Decreased conscious level in children · Paediatric coma assessment · AVPU and paediatric GCS · DEFG don't ever forget glucose
A fellowship approach to the child with an altered conscious state. Secure the airway with oxygen and ventilation, screen level of consciousness with AVPU and convert any response below Alert to an age-adapted Glasgow Coma Scale, check a bedside glucose immediately and correct a dangerous low now, treat an ongoing convulsion at five minutes, and keep infection, raised intracranial pressure, toxin, metabolic and safeguarding causes open while you escalate.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Altered conscious state means any fall from the child's usual awareness of, and response to, their environment. It spans the wide gap between a child who is merely sleepy and a child who is deeply comatose, and it carries the same message in every case: the brain is failing, and the cause may kill or maim within minutes to hours. The job at the bedside is not to name the disease first; it is to protect the brain while you find out why. [1] [2]
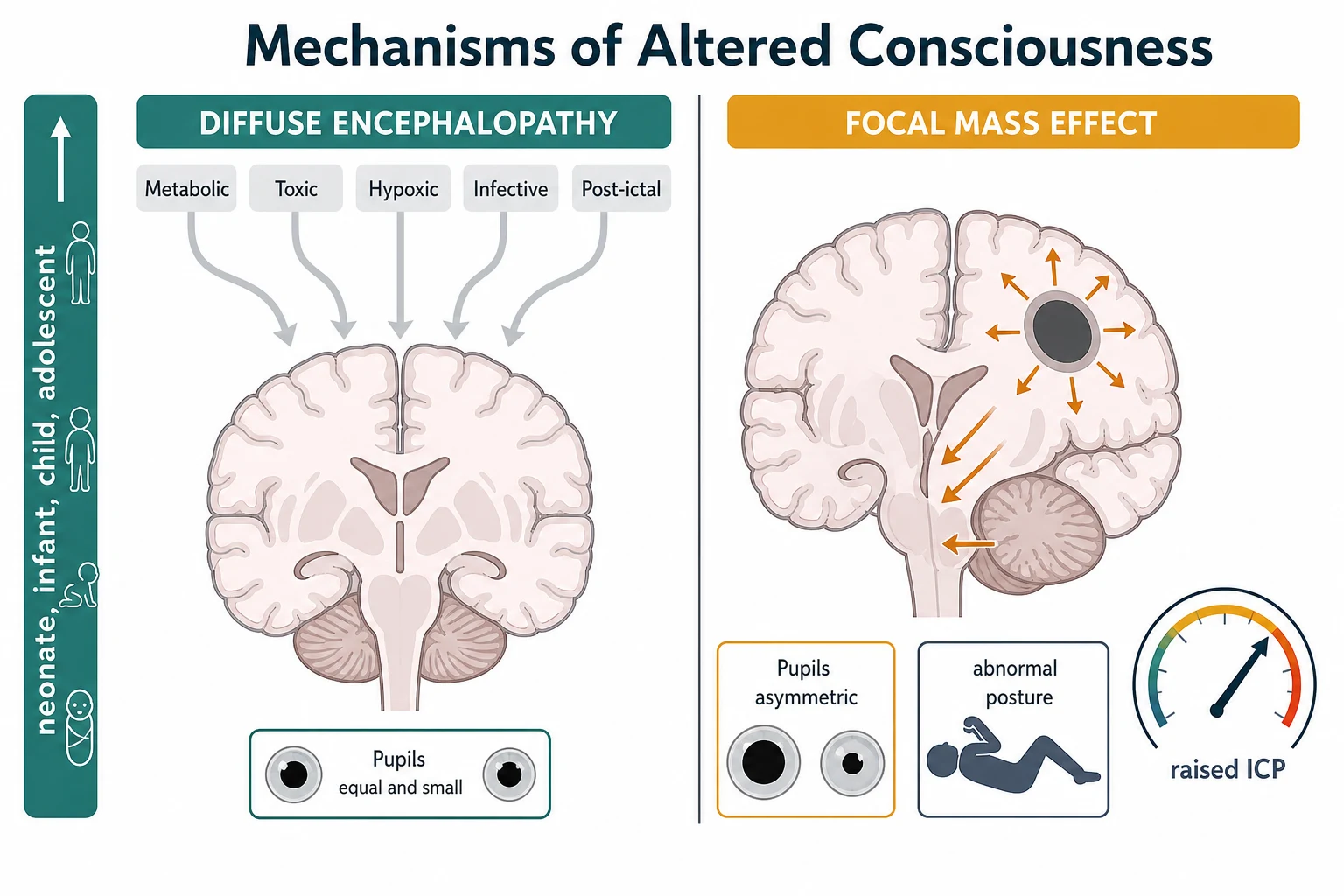
Consciousness is the product of arousal, generated by the brainstem reticular activating system, and awareness, generated by the cerebral hemispheres. A fall in conscious level therefore points to one of two broad mechanisms: a diffuse disturbance of both hemispheres (metabolic, toxic, hypoxic, infective, post-ictal) or a focal lesion pressing on the brainstem (mass, haemorrhage, oedema, herniation). This single distinction drives almost every decision that follows, because a diffusely impaired brain is usually reversible, while a brain under pressure from a focal lesion can herniate and die. [2] [8]
[4] [5]The assessment runs inside the broader primary survey. Airway, breathing and circulation are assessed and supported first, because the most common cause of a falling conscious level in a sick child is upstream failure: hypoxia, hypercapnia or shock. Disability is then assessed with AVPU, an age-adapted Glasgow Coma Scale, the pupils, posture and tone, a timed seizure check, and the bedside glucose. A child with a reduced conscious level cannot protect their airway, so disability and airway protection advance together. [1] [2]
The disability assessment as a repeating loop
Secure A, B, C first
Protect and open the airway, give oxygen, support ventilation if breathing is ineffective, and treat shock, because upstream failure is the commonest cause of a falling conscious level.
Screen with AVPU
Record Alert, responds to Voice, responds to Pain or Unresponsive. Any response below Alert triggers a formal age-adapted Glasgow Coma Scale.
Examine the brain
Check pupil size and reactivity, posture and tone, movement, and time any seizure. Look for lateralising signs and for Cushing physiology.
Check glucose now
Measure a point-of-care glucose in every child with altered consciousness and correct a dangerous low immediately through the local age-specific pathway.
Reassess and escalate
Repeat the disability assessment after each action, watch the trend, and call senior, PICU or retrieval help before local support is exceeded.
Classification
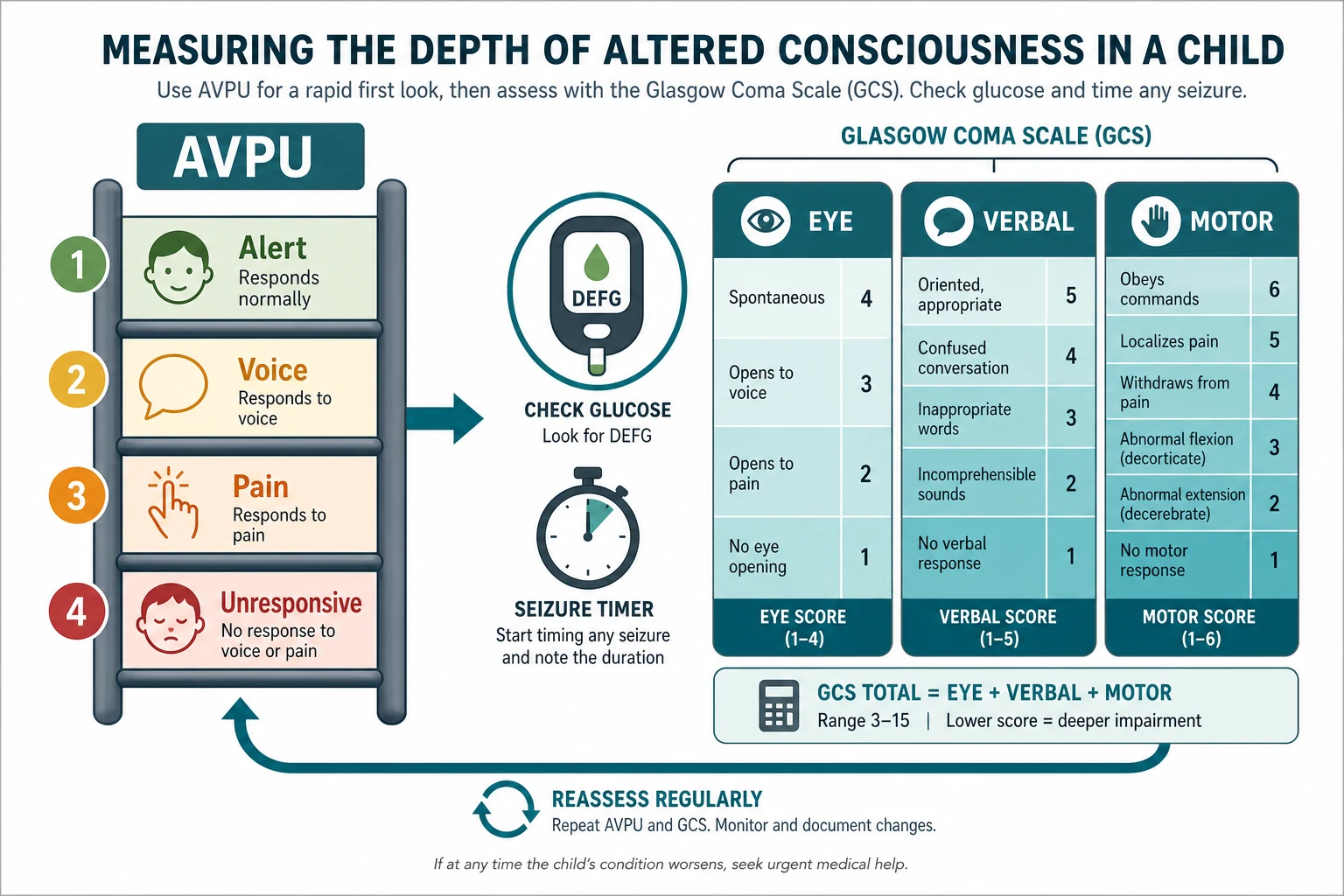
Classify altered consciousness on two axes at once: how deeply impaired the child is, and which mechanism is causing it. The depth axis is measured, not guessed. AVPU is the rapid screen used from the doorway and during resuscitation; the Glasgow Coma Scale is the formal, repeatable measure that documents severity and trends. [1] [2]
| Tool | What it measures | When to use it | Boundary and cautions |
|---|---|---|---|
| AVPU | A rapid four-level screen of responsiveness | Doorway impression, resuscitation, serial reassessment | Any V, P or U must be converted to a formal GCS; never treat an AVPU letter as a number |
| Glasgow Coma Scale | Best eye opening, best verbal response and best motor response, total 3 to 15 | Any child whose responsiveness is below Alert, or whose Alert state remains concerning | Use the age-adapted verbal component for preverbal children; a GCS of 8 or below flags a threatened airway |
| Pediatric FOUR score | Eye, motor, brainstem reflexes and respiration | Where intubation or sedation limits verbal scoring | Useful in intensive care; complements rather than replaces the GCS |
| Bedside glucose | A reversible cause of coma, not a level of consciousness | Every child with altered consciousness, without exception | Confirm an unexpected result when feasible, but never delay treatment of a dangerous low |
The AVPU screen maps roughly onto Glasgow Coma Scale bands. A child who is Alert is near the top of the scale; a child who responds only to Voice sits around the low teens; a child who responds only to Pain is near a score of eight; an Unresponsive child is at the bottom. This mapping is a clinical anchor, not a calculation: never convert one AVPU letter into a single assumed GCS number, because the components that matter most for airway protection are hidden inside the scale. [1]
The mechanism axis separates diffuse encephalopathy from a focal mass effect. A diffuse process tends to produce a symmetrical, flaccid, poorly responsive child with preserved or equal pupils and a normal or rapid respiratory pattern, until late. A focal lesion under pressure tends to produce lateralising signs, abnormal posture, pupillary asymmetry, and the Cushing pattern of a rising blood pressure with a falling heart rate and irregular breathing. Recognising the second pattern is an emergency, because it signals impending herniation and changes the destination from investigation to urgent neuroimaging and neurosurgical input. [2] [9]
Epidemiology & Risk Factors
The causes of altered consciousness change with age, and the high-risk groups are predictable. In young infants, serious bacterial infection, inborn errors of metabolism, hypoglycaemia and abusive head trauma dominate, and the presentation is often non-specific: poor feeding, altered tone, irritability or a change in cry. In preschool and school-age children, febrile illness with meningitis or encephalitis, seizure and post-ictal states, accidental and non-accidental head injury, and intentional or accidental poisoning become more common. In adolescents, self-harm and substance exposure join the differential. [10] [12]
Young infant
- Serious bacterial infection and sepsis may present without fever
- Inborn errors of metabolism and hypoglycaemia with poor intake
- Abusive head trauma with an inconsistent story
- A normal behavioural baseline is hard to establish; caregiver concern is key
Preschool and school-age
- Meningitis, encephalitis and post-infective demyelination
- Seizure, convulsive status epilepticus and post-ictal states
- Accidental and non-accidental head injury
- Intentional and accidental poisoning become accessible
Adolescent
- Intentional self-poisoning and substance exposure
- New or undiagnosed seizure, and eating-restriction electrolyte disturbance
- Create private history time and ask about self-harm
- Confidentiality has safety limits; safeguarding duties still apply
System and context
- Immunocompromise and complex chronic disease lower the threshold
- Rural distance and limited rescue change escalation timing
- Communication barriers delay recognition
- Caregiver-reported change from usual is high-value information
Recurrent or unexplained presentations carry particular weight. A child brought back repeatedly with altered behaviour, tone or responsiveness, or an infant whose story does not fit the injury or the developmental stage, must keep non-accidental injury and safeguarding open while medical stabilisation proceeds. Document objective findings and the child's spontaneous words, ask only necessary non-leading questions, and activate the local safeguarding pathway. [11]
Pathophysiology
Consciousness fails when the reticular activating system cannot sustain arousal or when both cerebral hemispheres cannot sustain awareness. The reticular activating system sits in the brainstem, so any lesion large enough to compress it, or any rise in intracranial pressure enough to displace it, can abolish arousal rapidly and irreversibly. The hemispheres tolerate diffuse insults better, because they have more reserve, but they fail together when metabolic, toxic, hypoxic, infective or post-ictal depression lowers global function below the threshold for wakefulness. [2] [8]
Intracranial pressure matters because the skull is a rigid box holding brain, blood and cerebrospinal fluid. In a child, an expanding lesion first displaces fluid and is partly compensated, so consciousness may be preserved until late. Once compensation is exhausted, small volume increases produce large pressure rises, perfusion falls, the brain shifts, and herniation follows. Cerebral oedema during diabetic ketoacidosis is the classic paediatric example of a rapid, life-threatening rise in intracranial pressure, and it illustrates why fluid and insulin strategy in such children is cautious and monitored. [9]
Hypoglycaemia injures the brain because glucose is the obligate cerebral fuel in young children. A dangerous low activates counter-regulatory stress, depresses cortical function, and can present as irritability, confusion, seizure or coma, and it can coexist with any of the other causes. Metabolic and electrolyte disturbances share the same pathway: hyponatraemia, hypernatraemia, hypocalcaemia, hepatic failure with hyperammonaemia, and inborn errors of metabolism all lower global hemisphere function below the threshold for wakefulness. [4] [5]
Seizures alter consciousness both during the ictal phase and after it. An ongoing convulsion that persists beyond five minutes is convulsive status epilepticus, a state in which the seizure self-perpetuates, becomes harder to terminate, and carries a rising risk of secondary brain injury. Even after a seizure stops, a post-ictal child may be obtunded for a prolonged period, and non-convulsive status must be considered when a child fails to recover as expected. [6] [7]
Hypoxia and hypercapnia depress consciousness directly and rapidly. A rising carbon dioxide level causes cerebral vasodilation, increases cerebral blood volume, and can worsen any rise in intracranial pressure, which is why effective ventilation is both a treatment for the brain and a protection against it. Toxins act through receptor, channel and metabolic effects that produce the same end result: diffuse, usually reversible, depression of consciousness. [2] [12]
Clinical Presentation
The presentation is rarely "coma" as the chief complaint. More often the child is brought in drowsy, floppy, irritable, not feeding, not responding normally, or found unresponsive, and the caregiver reports a change from usual. Begin with the first impression and the primary survey before detailed examination, and describe what you see objectively rather than labelling it. "This three-year-old is drowsy, responds to voice only, has a stiff neck and a purpuric rash" tells the team far more than "this child is encephalopathic". [1] [10]
Measuring the level of consciousness
Use AVPU first for speed. A is Alert, opens eyes spontaneously and fixes and follows; V responds to Voice; P responds only to Pain; U is Unresponsive to pain. Any response below Alert, or an Alert child who remains concerning, must be measured with a formal age-adapted Glasgow Coma Scale. Record the best eye, verbal and motor response separately, because the trend in the components, especially the motor response, is what predicts the threat to the airway. [1] [2]
The Glasgow Coma Scale scores best eye opening (1 to 4), best verbal response (1 to 5) and best motor response (1 to 6), for a total from 3 to 15. For preverbal infants, the verbal component is adapted to crying, babbling and interaction, and the motor response is scored to the best response to stimulation. A total of 8 or below is the traditional threshold at which the airway is considered threatened and intubation should be anticipated, but the decision is clinical, made from the components and the trend, never from the number alone. [2]
The rest of the disability examination
After the score, examine the pupils, posture and tone. Document pupil size and reactivity to light for each eye; new inequality, dilation or unresponsiveness suggests a focal lesion with raised intracranial pressure. Look for abnormal posture: decorticate flexion of the arms and extension of the legs, or decerebrate extension throughout, signals deep hemisphere or brainstem dysfunction. Assess tone and movement for asymmetry that points to a focal lesion, and time any ongoing seizure precisely. [2] [9]
| Finding | What it suggests | First response |
|---|---|---|
| Symmetrical, flaccid, equal reactive pupils | Diffuse encephalopathy (metabolic, toxic, hypoxic, infective, post-ictal) | Secure airway, oxygen, glucose, treat the cause |
| Unilateral dilated unresponsive pupil with posture | Focal mass effect with raised intracranial pressure and impending herniation | Urgent neuroimaging, raise head of bed, neurosurgical input, treat raised pressure |
| Rising blood pressure, falling heart rate, irregular breathing | Cushing response to raised intracranial pressure | Treat as impending herniation; escalate immediately |
| Ongoing convulsion beyond five minutes | Convulsive status epilepticus | First-line benzodiazepine now, then second-line as planned |
| Dangerous low bedside glucose | Hypoglycaemic encephalopathy | Correct immediately; do not wait for the laboratory |
| Fever with neck stiffness or purpuric rash | Meningitis, meningococcaemia or encephalitis | Time-critical antimicrobials and dexamethasone per local pathway |
Differential Diagnosis
Build the disability differential in a fixed order: what can kill or injure the brain now, what is most likely, what is reversible, and what is most harmful to miss. The mnemonic AEIOU-TIPS is one way to keep the reversible causes open at the bedside. [2] [4]
AEIOU-TIPS
A more compact frame separates the reversible threats a single correct action can fix. These are the low Hs and the structural or toxic threats that must be sought actively during the survey: hypoxia, hypoglycaemia, hypo- and hyperthermia, and the threats of raised intracranial pressure, ongoing seizure, and toxin exposure. Holding these open in parallel is the point of the disability assessment. [2] [6]
Metabolic and endocrine
- Hypoglycaemia is the must-not-miss reversible cause
- Hyponatraemia, hypernatraemia and hypocalcaemia
- Inborn errors of metabolism with hyperammonaemia
- Adrenal crisis and hypothyroid decompensation
Infective
- Bacterial meningitis and meningococcaemia
- Viral and autoimmune encephalitis
- Cerebral abscess and empyema
- Systemic sepsis with encephalopathy
Neurological and structural
- Seizure, convulsive and non-convulsive status, post-ictal state
- Traumatic brain injury and abusive head trauma
- Tumour, hydrocephalus and vascular events
- Cerebral oedema of diabetic ketoacidosis
Toxic and environmental
- Accidental and intentional poisoning
- Opioids, sedatives, anticonvulsants and recreational substances
- Carbon monoxide and envenomation
- Heat illness and hypothermia
Safeguarding
- Non-accidental injury and abusive head trauma
- Neglect and induced or fabricated illness
- Inconsistent history for the injury or developmental stage
- Stabilise first, document objectively, act in parallel
A defensible synthesis sounds like this: "This child has a reduced conscious level with a GCS motor response of localising pain, unequal pupils and a falling heart rate, so I am treating impending herniation from raised intracranial pressure by raising the head of bed, optimising ventilation, and arranging urgent neuroimaging and neurosurgical input. I have checked and corrected the glucose, and I am keeping infection, toxin and metabolic causes open while I escalate." [2] [9]
Clinical & Bedside Assessment
Assess and support airway, breathing and circulation before detailed disability examination. A reduced conscious level impairs airway protection, so position the airway, clear secretions, give oxygen, and support ventilation if breathing is ineffective. Treat shock, because a hypoperfused brain cannot stay awake. Only then measure the disability in detail. [1] [2]
AVPU and the Glasgow Coma Scale
Record AVPU as the first disability measure. Alert means eyes open spontaneously and the child fixes and follows; Voice means eyes or a purposeful response to speech; Pain means a response only to a painful stimulus; Unresponsive means no response. Apply the stimulus to a central site such as supraorbital pressure or trapezius squeeze, and record the best response. Any result below Alert prompts a full age-adapted Glasgow Coma Scale. [1] [2]
[2]For the verbal component, adapt to development. The preverbal infant cannot orient, so score the equivalent of cooing and babbling, irritable cry, or grunt, reserving the oriented score for a child who can speak. Avoid inserting an oral airway or suctioning purely to test the verbal response, because agitation can destabilise a threatened airway. Reassess and document the components and the total after every intervention. [2] [3]
Pupils, posture, tone and glucose
Examine the pupils for size, equality and reactivity, and document the time. New pupillary asymmetry, dilation or loss of reactivity is a lateralising sign that points to a focal lesion under pressure. Assess posture and tone for decorticate or decerebrate patterns and for asymmetry of movement. Check the bedside glucose in every child, regardless of the apparent cause, and repeat it if the child does not recover as expected or after treatment. [2] [9]
A focused history runs in parallel using a SAMPLE frame: Symptoms and onset, Allergies, Medications and access to toxins, Past history including seizures, metabolic disease and baseline, Last meal and intake, and Events leading up. Begin with the caregiver: "What is different from usual, and when did it start?" Add fever, rash, seizure, trauma, ingestion, vomiting, diarrhoea, and any change in medication. Ask adolescents privately about substances, self-harm and pregnancy when it is safe to do so. Use a professional interpreter whenever needed. [10] [12]
After each pass, state and document one sentence: what the level of consciousness is, which mechanism the findings point to, what you expected from the last action and what actually happened, and what you will do next. This spoken synthesis keeps the team coordinated during rapid change and is exactly what examiners listen for. [1] [2]
Investigations
Stabilise first, then order a test for a named question. A useful test in altered consciousness finds an immediately reversible cause, confirms or excludes raised intracranial pressure, separates urgent pathways, or changes the destination. A normal panel never overrules a child who is worsening. [2] [4]
Immediate and bedside
- Point-of-care glucose in every child, without exception
- Credible oxygen saturation and, in serious illness, capnography to control carbon dioxide
- Blood gas to quantify ventilation, perfusion and acid-base state
- ECG for any circulatory concern or collapse
Conditional on a question
- Electrolytes, renal and liver function, calcium, ammonia and blood gas for metabolic and electrolyte causes
- Blood count, coagulation and inflammatory markers for an infective or metabolic branch
- Cultures and viral studies before time-critical antimicrobials when this does not delay them
- Targeted toxicology and drug levels when the result changes the plan
Targeted imaging and neurophysiology
- Urgent neuroimaging when a focal lesion, raised pressure or herniation is suspected, only after stability and airway safety
- Lumbar puncture only after raised intracranial pressure is excluded and the child is stable
- Electroencephalography when non-convulsive status is suspected or recovery is delayed
- Never move an unstable child to imaging without monitoring, escort and a rescue plan
Interpret the results as physiology and mechanism, not as binary reassurance. A point-of-care glucose must be acted on immediately when dangerous-low, and confirmed when feasible without delaying treatment. A blood gas shows whether ventilation and acid-base state are contributing to the encephalopathy. Ammonia and metabolic studies separate a reversible metabolic cause from a structural one. Neuroimaging answers the question of a focal lesion; the lumbar puncture answers the question of infection, but only when it is safe to perform. [4] [5] [10]
[2] [4]Management — Resuscitation
A reduced conscious level triggers the resuscitation team. State your concern, call for help, name a leader, allocate roles, use closed-loop communication, and prepare age- and weight-appropriate equipment and monitoring. Assess and support airway, breathing and circulation first, then run the disability assessment, treat each reversible cause as it is found, and reassess after every action. [1] [2]
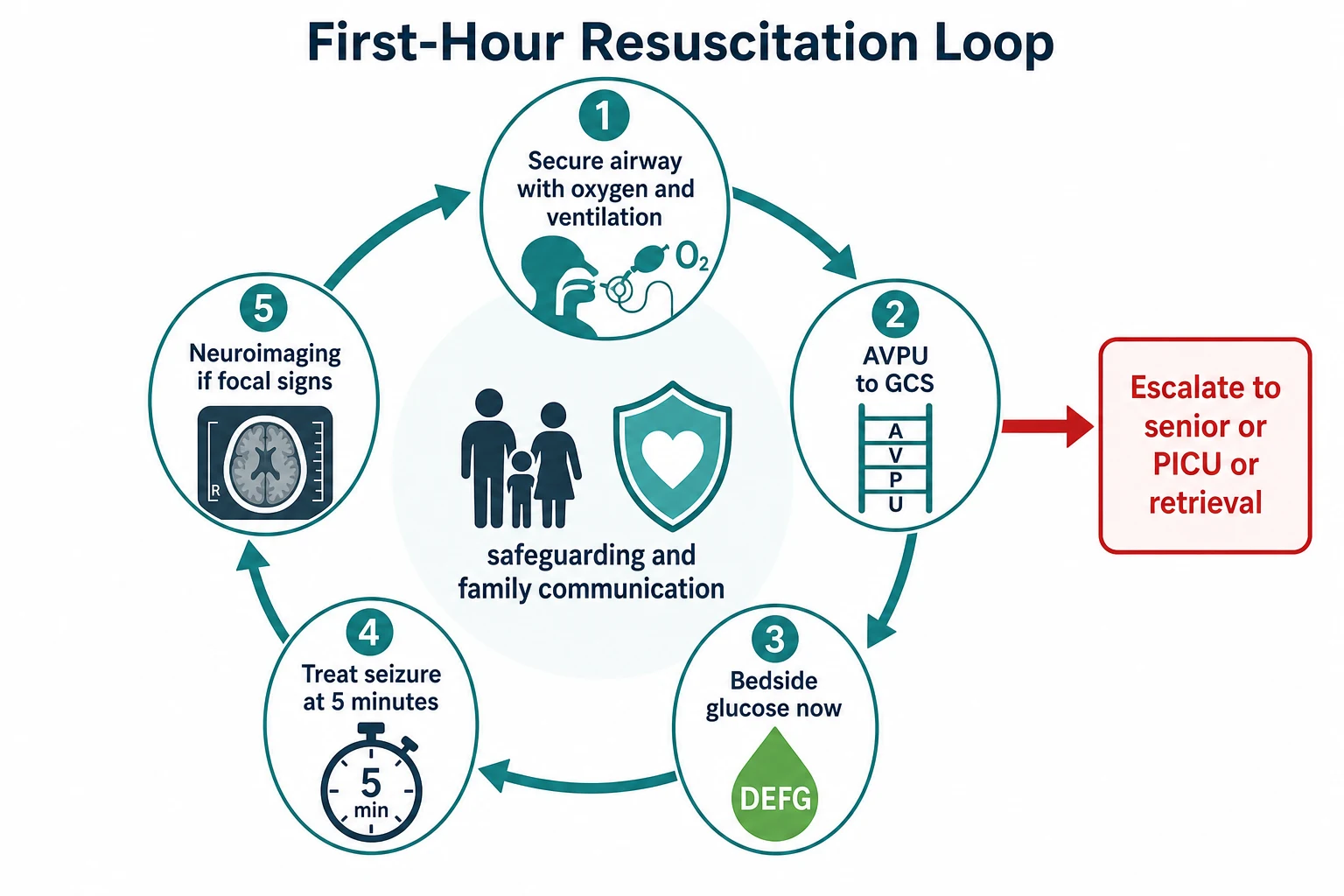
The first minutes when the cause is uncertain
Call and organise
Declare concern, call senior, resuscitation, airway, critical-care or retrieval help, identify the leader and allocate tasks.
A and B
Position and protect the airway, give high-flow oxygen, and support ventilation if breathing is ineffective, controlling carbon dioxide because hypercapnia raises intracranial pressure.
C
Treat shock and control obvious loss, because a hypoperfused brain cannot stay awake.
D
Record AVPU and a formal GCS, examine pupils and posture, time any seizure, and check the bedside glucose now.
Treat reversible causes
Correct a dangerous low glucose immediately, give a first-line benzodiazepine for an ongoing convulsion at five minutes, and recognise and treat raised intracranial pressure.
Reassess and escalate
Repeat the disability assessment, watch the trend, arrange urgent neuroimaging if a focal lesion is suspected, and escalate before local support is exceeded.
Glucose: the must-not-miss reversible cause
Check a bedside glucose in every child with altered consciousness and correct a dangerous low immediately. In most children a dangerous low is around or below 3 mmol per litre (about 54 mg per decilitre), but the threshold is age-specific, particularly in neonates and young infants, so apply the local age-specific value and do not let uncertainty delay treatment. Treat through the active age- and context-specific pathway, recheck after treatment, and then investigate the cause. Confirm an unexpected result when feasible, but never let confirmation delay correction of a dangerous low. [4] [5]
Seizure and status epilepticus
Time the seizure from onset. An ongoing convulsive seizure at five minutes is convulsive status epilepticus and activates first-line treatment; do not wait for two doses to fail. Give a first-line benzodiazepine by the available route, such as intravenous lorazepam or diazepam, or buccal or intranasal midazolam when intravenous access is delayed. If the seizure continues, give a second-line agent. The ESETT trial and the paediatric EcLiPSE trial found levetiracetam, fosphenytoin and valproate broadly comparable for established status in children, and levetiracetam was favoured over phenytoin for safety; follow the local status pathway and the weight-appropriate doses. [6] [7]
Raised intracranial pressure and impending herniation
When pupillary asymmetry, abnormal posture, or a Cushing pattern of rising blood pressure with falling heart rate and irregular breathing suggests raised intracranial pressure, act immediately. Raise the head of the bed, keep the midline position, avoid hip flexion that impedes venous return, optimise oxygenation and ventilation to control carbon dioxide, and arrange urgent neuroimaging and neurosurgical input. Osmotic therapy and other pressure-lowering measures follow the local neurocritical-care pathway. This is the moment to escalate, because herniation is rapid and may be irreversible. [9]
Airway protection
A child with a Glasgow Coma Scale of 8 or below, or with a motor response of withdrawal or worse that is falling, is approaching or past the threshold for airway threat and should be assessed for intubation by an experienced clinician. Secure the airway before aspiration, obstruction or respiratory arrest occurs, using the rapid sequence approach and weight-appropriate equipment and drug doses. Never sedate or paralyse a threatened airway without a plan and the people to execute it. [2]
[9]Management — Definitive & Stepwise
After resuscitation, move into the pathway for the likely cause without stopping reassessment. This hub does not reproduce the full meningitis, status, metabolic, toxicology or neurocritical-care algorithms; treat the most reversible dangerous problem first while keeping the other serious causes open. [6] [10]
From resuscitation to the right ongoing plan
Name the expected result
Before acting, state the change you expect in level of consciousness, airway safety, glucose, seizure control, or intracranial pressure.
Measure what happened
Repeat the disability assessment and the key investigations. Distinguish sustained improvement, brief improvement, no response, and harm.
Choose the cause-specific pathway
Move to infection, status, metabolic, toxicology, raised pressure, trauma, or safeguarding care as the evidence becomes clearer.
Agree monitoring and contingency
Specify the location, staff, observation intensity, response owner, next sign of failure and the plan if transfer is delayed.
Hand over and dispose
Transfer baseline, trend, timed actions, response, unresolved risks, imaging, family and safeguarding information, and the next action.
Improvement must make sense across several findings. A rising Glasgow Coma Scale must be matched by better interaction and a protected airway. A corrected glucose needs a documented recheck and a plan for the cause. A controlled seizure must be confirmed clinically, with non-convulsive status considered if recovery stalls. Reassess after each action and meaningful change, not on a fixed schedule. [2] [6]
Call PICU or retrieval when the child may need support your service cannot reliably provide, such as intubation, neurocritical care, osmotic therapy or neurosurgery, not after every local option has failed. Discuss the likely support, present monitoring and access, equipment and staff limits, transport time and weather, the safest destination, the escort, expected deterioration, and the plan if transfer is delayed. Exact referral thresholds and transport arrangements remain local or regional. [2]
Specific Subtypes & Scenarios
The disability assessment stays the same, but age, presentation and baseline change what you look for and how early you escalate. In each scenario: stabilise first, identify the failing mechanism, activate the correct pathway, and state which facts are specific to that source or setting. [1]
Young infant
- Treat altered feeding, behaviour, tone or temperature as significant even without fever
- Check bedside glucose early; consider inborn errors of metabolism
- Keep serious bacterial infection and abusive head trauma open
- Seek senior review and use the Newborn Life Support to Paediatric Life Support boundary at birth
Meningitis and encephalitis
- Fever with altered consciousness, neck stiffness, seizure or purpuric rash
- Give time-critical antimicrobials and dexamethasone per local pathway
- Lumbar puncture only after raised pressure is excluded and the child is stable
- Keep autoimmune encephalitis open when infection is not found
Convulsive status epilepticus
- Time from onset; first-line benzodiazepine at five minutes
- Second-line levetiracetam or fosphenytoin per local pathway
- Check glucose and treat; consider non-convulsive status if recovery stalls
- Reassess airway and breathing between doses
Diabetic ketoacidosis with cerebral oedema
- Altered consciousness in DKA may signal cerebral oedema
- Cautious fluid and insulin strategy with close neurological monitoring
- Treat rising pressure immediately; raise head and control ventilation
- Avoid rapid biochemical correction
Poisoning
- Stabilise physiology while substance, dose and time remain uncertain
- Seek containers, medication lists and collateral
- Use targeted ECG, glucose and toxicology when they change the branch
- Activate the local toxicology pathway and consider antidotes
Raised intracranial pressure
- Pupillary asymmetry, abnormal posture, Cushing pattern
- Raise head, control carbon dioxide, urgent neuroimaging
- Neurosurgical input and neurocritical-care pathway
- No lumbar puncture until pressure is excluded
Adolescent collapse
- Stabilise first, then create private history time when safe
- Ask directly about substance exposure, self-harm and eating restriction
- Explain confidentiality and its safety limits
- Intentional self-poisoning is common; use the toxicology pathway
Non-accidental injury
- Inconsistent history for the injury or developmental stage
- Neuroimaging for abusive head trauma; document objectively
- Stabilise first, run safeguarding in parallel
- Ask only necessary non-leading questions; activate the local pathway
Technology-dependent child
- Assess the child and any device such as a shunt in parallel
- Ask what normal function looks and sounds like
- Use the personal emergency plan and the specialty pathway
- Compare with the personal baseline, not population norms
Immunocompromised child
- Absence of fever does not exclude serious infection
- Consider opportunulent and atypical pathogens
- Sample without delaying treatment for instability
- Escalate on physiology and risk context
Rural or remote setting
- Call retrieval before the child needs support unavailable locally
- State equipment, staff, weather, distance and communication limits
- Agree a delayed-transfer contingency driven by acuity
- Package monitoring, access and handover for transport
Complications & Pitfalls
Most harm begins when the reversible causes are not sought, or when a reassuring number ends the assessment. The single most preventable error is missing a dangerous low glucose, because hypoglycaemic brain injury is avoidable and treatable. Prevent this by checking a bedside glucose in every child, by acting on a dangerous low immediately, and by never waiting for the laboratory. [4] [5]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Bedside glucose not checked | Reversible hypoglycaemic brain injury is missed | Check a point-of-care glucose in every child with altered consciousness and correct a dangerous low now |
| AVPU treated as a number | The components that predict airway threat are hidden | Convert any V, P or U to a formal GCS and record the components |
| Lumbar puncture before raised pressure excluded | Herniation can be precipitated | Exclude raised intracranial pressure and stabilise before any lumbar puncture |
| Seizure allowed to run beyond five minutes | Status becomes harder to terminate and risks secondary injury | Activate first-line treatment at five minutes; do not wait for two failed doses |
| Hypercapnia unrecognised | Raised carbon dioxide worsens intracranial pressure | Control ventilation and confirm with capnography or a blood gas |
| Premature closure on one cause | A second dangerous cause is missed | Keep infection, pressure, toxin, metabolic and safeguarding open in parallel |
| Unstable child sent to imaging | Airway or circulation fails unmonitored | Stabilise and escort with a rescue plan; secure the airway first if needed |
| Safeguarding postponed for diagnosis | Immediate safety and evidence are lost | Stabilise first while objective documentation and the pathway proceed in parallel |
| Adult doses or equipment | Age, weight and reserve are ignored | Use age, weight and the local paediatric cognitive aid |
| Poor handover | Trend, timed actions and contingency disappear | Use a structured transfer with read-back and named ownership |
Watch for anchoring on the referral diagnosis, ordering tests only to confirm it, and carrying forward a label that silences bedside concern. After stabilisation, look actively for harm from treatment: airway or access complications, fluid or osmotic therapy effects, heat loss, repeated sampling, and medication error. The fact that the child did not arrest does not prove an intervention was harmless. [2]
[2] [4] [9]Prognosis & Disposition
Disposition follows the trend and response, the mechanism, and the support needed. Consider the child's age and reserve, the duration and severity of the reduced conscious level, the reversibility of the cause, treatment harm, local support, transport risk, and whether the family can carry out the plan. [2] [9]
Critical care or retrieval
- Reduced conscious level that is worsening or not recovering
- Need for intubation, neurocritical care, osmotic therapy or neurosurgery unavailable locally
- Raised intracranial pressure or ongoing status epilepticus
- Transport risk that needs early specialist planning
Ward or high-dependency
- Improving but not yet at baseline, or a cause still being defined
- Monitoring and staffing can detect and respond to failure
- Pending neuroimaging, electroencephalography or results that change disposition
- A named escalation pathway exists
Discharge only when defensible
- Sustained return to baseline after appropriate reassessment
- No unresolved immediate threat or high-harm cause
- Dangerous low glucose explained and a prevention plan agreed
- Specific warning changes, access route, follow-up and pending-result ownership agreed
A safety net states what change to watch for, how urgently to act, and exactly where to get help. It states when review will occur, who owns pending results, and what to do if access is difficult. "Return if worried" alone is not enough. Check understanding with teach-back, document it, and connect the family to the medical home, primary care or community team. After a critical event, explain what happened and what remains uncertain, invite questions, and consider debriefing for the child, family and team. [1]
Special Populations
Adapt how you observe, communicate and examine, but never lower the standard for recognising deterioration. Evidence is sparse for consciousness assessment tools in disability, neurodiversity, technology dependence and many low-resource settings; present these adaptations as safer practice, not as proven improvements in diagnostic accuracy. [1] [11]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Young infant | Treat non-specific change as high-risk; check glucose early; consider inborn errors and abusive head trauma | Use the local Newborn Life Support to Paediatric Life Support boundary; do not apply an older-child pathway at birth |
| Complex or technology-dependent child | Establish personal baseline, device and shunt function and the emergency plan; assess child and device in parallel | A chronically abnormal level is not automatically safe; compare with the personal baseline |
| Severe neurodisability | Establish usual interaction, tone, movement and pain expression; treat caregiver-described change as evidence | Adaptation improves communication, not proven diagnostic sensitivity |
| Immunocompromised child | Absence of fever does not exclude serious infection; consider atypical pathogens | Do not delay time-critical treatment for complete sampling in an unstable child |
| Adolescent | Create private time; ask about substances, self-harm and pregnancy; explain confidentiality limits | Confidentiality has safety limits; safeguarding duties still apply |
| Indigenous, migrant or remote family | Use cultural safety and a professional interpreter; address access and transport barriers | Retrieval and safeguarding routes remain jurisdiction-specific |
Safeguarding runs in parallel with medical care, but immediate stabilisation and safety come first. Ask only necessary open, non-leading questions. Explain confidentiality and information sharing, document objective findings and spontaneous words, preserve evidence when safe, and use the local safeguarding pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [11]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The structure of the disability assessment is consensus across the major resuscitation sources. The Glasgow Coma Scale is the standard repeatable measure of consciousness, the AVPU screen is the accepted rapid adjunct, and a bedside glucose is mandated for any child with altered consciousness. What differs across sources is the precise hypoglycaemia threshold by age and the detail of status epilepticus and raised intracranial pressure management, which are source- and population-specific. [1] [2]
ESETT (and paediatric EcLiPSE)
Lancet and Health Technology Assessment
Double-blind randomised comparison of second-line anticonvulsants for established convulsive status epilepticus, with a dedicated paediatric trial
Key finding
Levetiracetam, fosphenytoin and valproate were broadly comparable for terminating established status; the paediatric EcLiPSE trial favoured levetiracetam over phenytoin for safety.
Practice change
Second-line treatment of paediatric status is guided by these trials, with levetiracetam commonly preferred; follow the local pathway and weight-appropriate doses.
Cerebral oedema during diabetic ketoacidosis remains a leading cause of death in children with the condition, and identifying the children at highest risk guides cautious fluid and insulin strategy and close neurological monitoring. Autoimmune encephalitis is increasingly recognised in children and joins infection in the differential when a child presents with altered consciousness, movement disorder or psychiatric features and infection is excluded. [8] [9]
There is no universal hypoglycaemia threshold, AVPU-to-GCS conversion table, or intracranial pressure target that fits every child. Attach each rule to its population, purpose, conditions and jurisdiction, and quote the local source rather than inventing precision. [4] [5]
Jurisdictional implementation
Australia and Aotearoa New Zealand: ANZCOR Guideline 12.2 is the 2026 regional paediatric advanced life support source. The Royal Children's Hospital Melbourne altered-conscious-state and hypoglycaemia guidelines support local implementation. Retrieval systems, observation charts, mandatory reporting and consent remain state-, territory- or nation-specific.
Global and low-resource settings: WHO ETAT adapts emergency triage, assessment and treatment mainly for low-resource hospitals and non-specialists. Population-specific thresholds and slower resource escalation must stay attached to that context.
Exam Pearls
Doorway and primary survey
- Treat altered consciousness as an emergency
- Secure airway, oxygen and ventilation; treat shock first
- Upstream hypoxia, hypercapnia and shock are common causes
Disability assessment
- AVPU screens; GCS measures
- Any V, P or U converts to an age-adapted GCS
- Record pupils, posture, tone, seizure time and bedside glucose
- A GCS of 8 or below flags a threatened airway
Reversible causes
- DEFG: check and correct glucose now
- Treat an ongoing convulsion at five minutes
- Recognise raised intracranial pressure and impending herniation
- Keep AEIOU-TIPS open in parallel
Investigations
- Point-of-care glucose in every child
- Neuroimaging when a focal lesion is suspected, after stability
- Lumbar puncture only when raised pressure is excluded
- EEG when non-convulsive status is suspected
Pitfalls
- No forgotten glucose
- No AVPU as a number
- No lumbar puncture before pressure is excluded
- No seizure beyond five minutes
- No unstable child to imaging unescorted
- No adult doses or equipment
“Secure A, B and C; AVPU then GCS; check glucose immediately and correct a dangerous low now; treat seizure at five minutes; recognise and treat raised intracranial pressure; keep infection, toxin, metabolic and safeguarding open; escalate before local support is exceeded.”
Viva: the drowsy feverish child
Do not anchor on a single diagnosis. Secure the airway and give oxygen, screen with AVPU and convert below Alert to a Glasgow Coma Scale, check the bedside glucose now, look for neck stiffness and a rash, and keep meningitis, encephalitis, sepsis, seizure and metabolic causes open. Give time-critical antimicrobials per the local pathway, arrange neuroimaging if there are focal signs, and perform a lumbar puncture only when the child is stable and raised pressure is excluded.
Viva: the child who does not wake after a seizure
Time is the key question. Confirm the convulsion has stopped clinically. A child who fails to recover as expected may be in non-convulsive status, may have a residual sedative effect, or may have a metabolic or structural cause. Recheck the glucose, run an electroencephalogram, reassess the Glasgow Coma Scale components and the pupils, and escalate to critical care if consciousness does not improve.
Structured oral: the infant with an inconsistent story
Stabilise first. Secure the airway, oxygen and circulation, check the glucose, and perform the disability assessment. Take an open, non-leading history, examine for cutaneous and skeletal signs of injury, and arrange neuroimaging for suspected abusive head trauma. Document objective findings and the spontaneous words used, and activate the local safeguarding pathway in parallel with medical care. Do not let the inconsistent story delay resuscitation.
References
- [1]Hoffmann, Florian Comparison of the AVPU Scale and the Pediatric GCS in Prehospital Setting Prehospital emergency care, 2016.PMID 26954262
- [2]Kirschen, Michael P Inter-Rater Reliability Between Critical Care Nurses Performing a Pediatric Modification to the Glasgow Coma Scale Pediatric critical care medicine, 2019.PMID 30946292
- [3]Czaikowski, Barbara L A pediatric FOUR score coma scale: interrater reliability and predictive validity Journal of neuroscience nursing, 2014.PMID 24556655
- [4]Faustino, E Vincent S Hypoglycemia in critically ill children Journal of diabetes science and technology, 2012.PMID 22401322
- [5]Honarmand, Kash Society of Critical Care Medicine Guidelines on Glycemic Control for Critically Ill Children and Adults 2024 Critical care medicine, 2024.PMID 38240484
- [6]Chamberlain, James M Efficacy of levetiracetam, fosphenytoin, and valproate for established status epilepticus by age group (ESETT): a double-blind, responsive-adaptive, randomised controlled trial Lancet (London, England), 2020.PMID 32203691
- [7]Appleton, Richard E Levetiracetam as an alternative to phenytoin for second-line emergency treatment of children with convulsive status epilepticus: the EcLiPSE RCT Health technology assessment (Winchester, England), 2020.PMID 33190679
- [8]Cellucci, Tiffany Clinical approach to the diagnosis of autoimmune encephalitis in the pediatric patient Neurology neuroimmunology and neuroinflammation, 2020.PMID 31953309
- [9]Dunger, David B Predicting cerebral edema during diabetic ketoacidosis The New England journal of medicine, 2001.PMID 11172161
- [10]Chávez-Bueno, Servio Bacterial meningitis in children Pediatric clinics of North America, 2005.PMID 15925663
- [11]Roy, Anil A Neuroimaging of Non-Accidental Injury Current pediatric reviews, 2015.PMID 26219740
- [12]Gonzalez-Urdiales, Paula Pediatric Intentional Self-poisoning Evaluated in the Emergency Department: An International Study Pediatric emergency care, 2021.PMID 32541402