Paeds · acute-care-resuscitation-and-toxicology
Burns assessment, resuscitation and safeguarding
Also known as Paediatric burn assessment · Paediatric burn resuscitation · Modified Parkland in children · Lund and Browder burn assessment · Burns safeguarding
A fellowship approach to the burned child inside an organised burn-care system. Stop the burning process and cool with running water for 20 minutes within 3 hours of injury, estimate percent total body surface area with an age-adjusted Lund and Browder chart, recognise the threatened airway and inhalation injury, start modified-Parkland fluid resuscitation at or above 10 percent TBSA and titrate to urine output, run safeguarding in parallel, apply the burns-centre referral criteria, and hand over safely.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A burn is an injury to the skin and deeper tissues caused by thermal, electrical, chemical or radiation energy. In a child the same injury behaves differently from the same injury in an adult, because a smaller body loses fluid and heat faster, the head and legs take up a different share of body surface area, and the history is often shaped by the developmental stage and the caregivers around the child. The burned child is therefore managed inside an organised burn-care system that runs from pre-hospital first aid through a burns centre and a rehabilitation pathway, and your job at the bedside is the front of that system. [1] [3]
The acute encounter has one rhythm. You stop the burning process, cool the burn, and keep the child warm. You run a primary survey adapted for the burn, looking hardest for the threatened airway and inhalation injury. You estimate the percent total body surface area burned, or TBSA, with an age-adjusted chart, and you judge depth at the bedside. You start formal fluid resuscitation for the larger burn and titrate it to urine output. In parallel with all of this, you keep safeguarding open, because a burn in a child is a sentinel event that is inflicted, neglected or accidental more often than is comfortable. [2] [9]
[2] [8]Most children present with a small scald or contact burn that needs cooling, analgesia, a dressing and follow-up. A minority present with a major burn that needs the full resuscitation pathway and a burns centre. The skill the examiner is testing is the triage between the two: which child can go home, which needs admission, and which needs a retrieval and a burn surgeon in the next hour. That triage rests on three numbers (the percent TBSA, the depth, and the time of injury) and one judgement (is the story consistent with the burn). [1] [10]
The first five minutes of a paediatric burn call
Stop and cool
Stop the burning process, remove clothing and jewellery, and cool with running water for 20 minutes within 3 hours of injury while keeping the rest of the child warm.
Airway and oxygen
Assess for inhalation injury; singed hair, soot, voice change or stridor mean call airway expertise and plan an early definitive airway.
Assess size and depth
Estimate percent TBSA with an age-adjusted Lund and Browder chart, exclude erythema, and judge depth at the bedside.
Resuscitate and analgesia
Gain access, give weight-based analgesia, and start modified-Parkland Hartmann for 10 percent TBSA or more plus maintenance in the young child.
Refer and safeguard
Apply the burns-centre referral criteria, run safeguarding in parallel, document objectively, and agree the destination with retrieval.
Classification
Classify the burn along three axes that together decide the tempo and the destination: depth, size (percent TBSA), and mechanism with special sites. Depth drives the surgical decision and the prediction of scarring. Size drives fluid resuscitation and admission. Mechanism and special-site involvement drive referral to a burns centre. The three are independent and must all be stated, because a small full-thickness burn on the hand can be more harmful than a large superficial scald on the back. [1] [3]
Burn depth runs from the surface down. Superficial (epidermal) burns are erythema alone, blanch, are painful, and are excluded from TBSA. Superficial dermal burns are pale pink, blistered, blistering, blanching and very painful because nerve endings are intact. Deep dermal burns are fixed red or pale, may blister, do not blanch, and have reduced sensation. Full-thickness burns are white, waxy, leathery or charred, do not blister, do not blanch, and are often painless because the nerve endings are destroyed. The depth matters because deep dermal and full-thickness burns are unlikely to heal within three weeks and usually need surgical assessment. [1] [3]
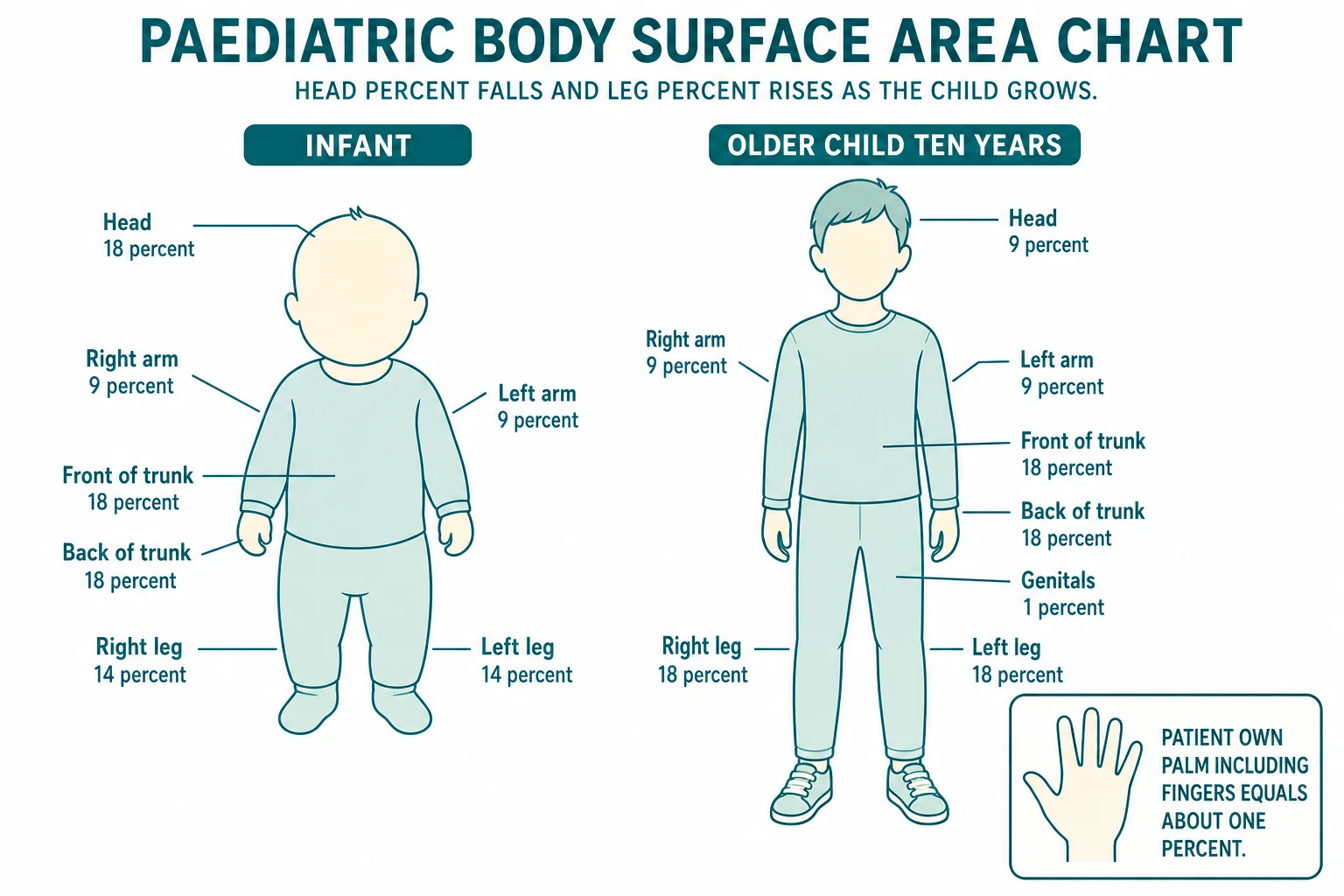
Size is the percent of total body surface area that is partial- or full-thickness, never including erythema. The Rule of Nines (head 9, each arm 9, front trunk 18, back trunk 18, each leg 18, genitals 1) is calibrated to the adult and is wrong in small children, whose head is much larger and legs much smaller. The age-adjusted Lund and Browder chart corrects for this by changing the head and leg proportions with age. As a quick check, the patient own palm including the fingers is about one percent of TBSA, which is useful for small or patchy burns. These estimates are imprecise at the bedside, which is why a measured chart or app is used, and the burn is re-mapped after cleaning. [2] [6]
| Depth | Bedside findings | What you do first |
|---|---|---|
| Superficial (epidermal) | Erythema, blanching, painful, no blisters | Exclude from TBSA; cooling and analgesia; not a surgical burn |
| Superficial dermal | Pale pink, blistered, blanches, very painful | Cool, dress, analgesia; likely to heal within 2 to 3 weeks; follow up |
| Deep dermal | Fixed red or pale, may blister, does not blanch, reduced sensation | Refer to burns service; likely surgical assessment; unlikely to heal within 3 weeks |
| Full thickness | White, waxy, leathery or charred; no blanch; often painless | Refer to burns centre; surgical assessment and likely excision and grafting |
Mechanism and special sites drive referral. The burns that concern you most are not the largest but the ones in the wrong place or caused by the wrong energy: special sites (face, hands, feet, perineum, genitalia, major joints), electrical and chemical injury, circumferential burns, and any inhalation injury. These override size and trigger a burns-centre consultation even when the area is small. Safeguarding is a classification axis in its own right: an inconsistent history, an immersion pattern, or a burn in a non-mobile infant moves the child into a parallel child-protection pathway while you resuscitate. [9] [10]
Epidemiology & Risk Factors
Burns are among the commonest causes of unintentional injury in children beyond infancy, and the great majority are preventable scalds and contact injuries in the home. Hot beverages, bath water, kettles, irons, hair straighteners, radiators and barbecues dominate in the toddler and preschool age group. Flame injury rises in the school-age child and adolescent, and electrical and chemical injury becomes more common with risk-taking behaviour. Enclosed-space fires carry the additional threat of inhalation injury and carbon monoxide and cyanide exposure. [1] [9]
Children are not small adults in two ways that change everything. First, the proportion of the head to the body changes with age: the head is about 18 percent of TBSA in an infant and falls toward the adult 9 percent by late childhood, while each leg rises from about 14 percent toward 18 percent. Using an adult chart in an infant therefore under-estimates a head burn and over-estimates a leg burn, and that error flows directly into the fluid calculation. Second, the surface area is large relative to body mass, so the infant and toddler lose heat and fluid faster than the adult at every stage of cooling and resuscitation. [2] [5]
Two epidemiological facts the examiner rewards. First, deliberate harm and neglect account for a meaningful minority of paediatric burns, and a single burn in a non-mobile infant, an immersion pattern, or an inconsistent history carries a high probability of inflicted injury until proven otherwise. Second, variation in paediatric burn care is large across hospitals, and adherence to a small set of process measures (cooling, TBSA estimation, fluid titration, referral) is associated with better outcome, which is exactly what the organised burn-care system is built to deliver. [9] [10]
Pathophysiology
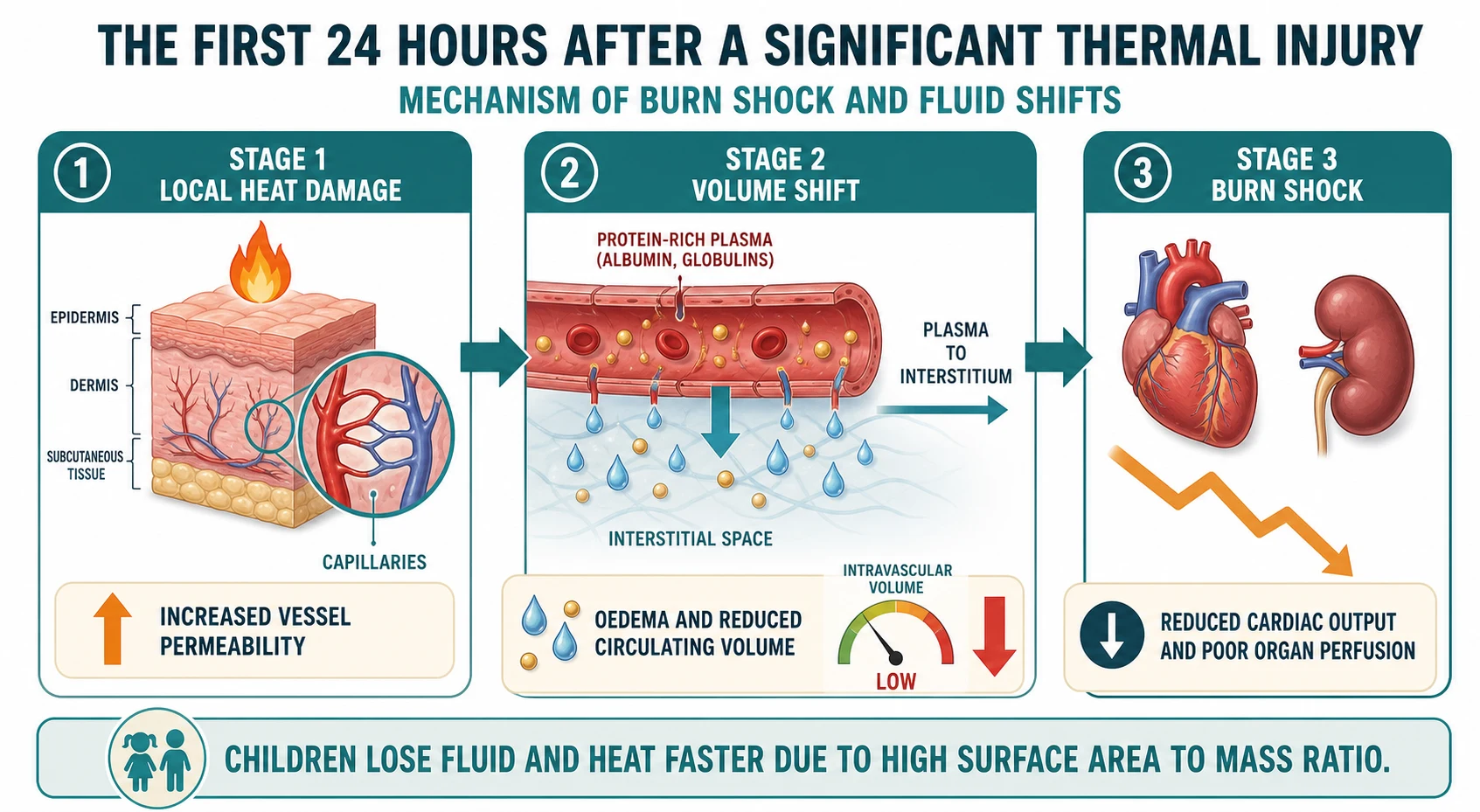
A significant burn produces a local and a systemic injury, and the systemic injury is what kills. Locally, the heat creates three concentric zones: a central zone of coagulation that is dead, a surrounding zone of stasis that is ischaemic but potentially salvageable, and an outer zone of hyperaemia that will recover. The aim of early cooling and resuscitation is to rescue the zone of stasis by restoring perfusion and preventing progression to full-thickness necrosis. Cooling within minutes reduces the depth of injury; delayed cooling does not. [1] [4]
Systemically, a burn of about 10 percent TBSA or more in a child triggers an inflammatory response that opens the capillary bed. Over the first 24 hours, capillary permeability rises, and a protein-rich plasma leaks from the intravascular space into the interstitium, producing burn oedema and reducing the circulating volume. The result is burn shock, which is predominantly hypovolaemic with an inflammatory component, and which develops over hours rather than minutes. This is the physiology that the modified-Parkland formula is designed to replace. [2] [7]
The choice of fluid matters. Hartmann solution (compound sodium lactate) is the standard resuscitation fluid because it is balanced and approximates the extracellular space; large volumes of normal saline produce hyperchloraemic acidosis and worsen outcome. The formula gives a starting volume, not a target, and it is titrated hourly to urine output. The clock starts at the time of injury, not at arrival, because the leak began at the burn; the first half of the 24-hour volume is given in the first 8 hours from the time of burn, and the second half over the next 16 hours. [2] [7]
Infants and small children carry two extra physiological risks. Their glycogen stores are small and their metabolic rate is high, so a burned infant can become hypoglycaemic during resuscitation; glucose-containing maintenance fluid is added to the burn resuscitation in the young child, alongside the Hartmann resuscitation volume. Their surface area is large relative to mass, so cooling and exposure can drop the temperature fast, and active warming is part of resuscitation, not comfort care. A cold child is harder to resuscitate, coagulopathic, and metabolically unstable. [2] [3]
Inhalation injury adds a direct airway and lung insult on top of the burn. Heat damages the upper airway and produces oedema that can develop over hours; soot, toxins and smoke particulates inflame the lower airway and impair gas exchange; carbon monoxide binds haemoglobin and starves tissue of oxygen; and cyanide released from burning plastics blocks cellular respiration. The clinical point is that the airway can look safe at 30 minutes and be lost at 3 hours, which is why suspected inhalation injury triggers an early definitive airway plan rather than watchful waiting. [8] [2]
Clinical Presentation
Begin before you touch the child. From the pre-alert and the doorway, capture the mechanism (hot fluid, contact, flame, electrical, chemical), the time of injury, the enclosed-space exposure, and the first aid already given. Note the age and the estimated weight, because every dose and every fluid calculation in the burn child is weight-based. Describe what you see objectively: a child who is hoarse after an enclosed fire, with soot in the mouth and singed nasal hair, is telling you about the airway before you lift the chin. [8] [2]
The threatened airway is the first thing you look for and the one you must not miss. Look for singed nasal and facial hair, soot in the mouth or sputum, a changed voice, a hoarse cry, drooling, stridor, and facial or neck swelling. Any of these in an enclosed-space fire moves the child towards an early definitive airway. The window is finite: oedema develops over hours, and a child you could intubate at 30 minutes may be impossible at 3 hours. Call airway expertise early and agree a calibrated plan, rather than waiting for stridor to make the decision for you. [8] [2]
Depth presents as described in Classification. The practical bedside point is that depth is hard to judge in the first hour because the burn is still evolving, the skin is wet, and pain makes assessment difficult. A first assessment is provisional; re-evaluate after cooling and cleaning, and again at 24 and 48 hours, and accept that even experienced burn surgeons revise their depth estimate over time. Be honest about uncertainty, and let the burns service make the final call on deep burns. [3] [1]
Inhalation injury and carbon monoxide poisoning present together after an enclosed fire. Hoarseness, cough, carbonaceous sputum, and respiratory distress indicate smoke injury to the airway and lung. Confusion, a reduced conscious state, headache and lactataemia suggest carbon monoxide or cyanide, and the pulse oximetry reading can look falsely reassuring because carboxyhaemoglobin is read as oxyhaemoglobin by standard devices. A venous gas with carboxyhaemoglobin is the bedside test, and a high level means high-flow oxygen for a prolonged period. [8] [2]
Airway threat
- Singed nasal or facial hair
- Soot in the mouth or sputum
- Voice change, hoarse cry, drooling
- Stridor or developing facial swelling
- Enclosed-space fire
- Plan early definitive airway; do not wait for stridor
Circumferential burn
- Full-thickness limb burn
- Pain on passive stretch
- Cool, pale or poorly perfusing digits
- Tight constricting torso burn limiting ventilation
- Refer urgently; consider escharotomy
- Monitor perfusion and ventilation continuously
Safeguarding pattern
- Inconsistent history for the developmental stage
- Delay in presentation
- Stocking-glove or immersion distribution
- Contact pattern in a non-mobile infant
- Repeated or unexplained presentation
- Run the safeguarding pathway in parallel
A circumferential burn of a limb or the chest is a presentation that changes the urgency. A full-thickness burn forms a rigid eschar that does not expand as the limb swells, so perfusion distal to the burn falls and compartment syndrome develops; on the chest, a tight eschar limits ventilation. Look for pain on passive stretch, cool or pale digits, reduced pulse, and rising ventilatory pressures, and refer urgently to a burns centre for consideration of escharotomy. Do not wait for the pulse to disappear. [2] [8]
Differential Diagnosis
Build the burn differential in a fixed order: what can kill now, what is most likely, what is reversible, and what is most harmful to miss. What can kill now is the threatened airway, inhalation injury, and burn shock. What is most likely is the domestic scald or contact burn. What is reversible is the depth of injury, by cooling. What is most harmful to miss is inflicted injury, because a missed safeguarding case returns with a worse injury or does not return at all. [9] [1]
| Problem | Distinguish by | First action |
|---|---|---|
| Threatened airway | Singed hair, soot, voice change, stridor after enclosed fire | Early definitive airway with senior airway help; high-flow oxygen |
| Inhalation or carbon monoxide | Confusion, reduced conscious state, lactataemia; carboxyhaemoglobin | High-flow oxygen for a prolonged period; consider cyanide antidote in enclosed fire |
| Burn shock | 10 percent TBSA or more; cool, tachycardic child with poor perfusion | Modified-Parkland Hartmann titrated to urine output; warm the child |
| Circumferential limb or chest burn | Tight full-thickness eschar; pain on passive stretch; reduced perfusion | Urgent burns-centre referral; consider escharotomy; do not wait for pulse loss |
| Inflicted or neglected burn | Inconsistent history; immersion or contact pattern; non-mobile infant | Stabilise first; document objectively; run safeguarding pathway in parallel |
Keep the dermatological mimics in mind, because not every blistering rash is a burn. Stevens-Johnson syndrome and toxic epidermal necrolysis produce widespread epidermal loss with mucosal involvement and target lesions, and they coexist with drug exposure and infection rather than with thermal mechanism. Staphylococcal scalded skin syndrome produces superficial peeling with positive Nikolsky sign in an unwell young child. Phytophotodermatitis (lime and sunlight) produces streaky erythema and blistering on sun-exposed areas. A careful mechanism, distribution and drug history distinguishes these from a burn, but a major mucocutaneous reaction can mimic a large burn and needs the same airway, fluid and analgesia principles. [1] [9]
The safeguarding differential deserves a paragraph of its own because it is the one most often missed. Distinguish an accidental scald from an inflicted immersion burn by the history, the distribution and the margins. Accidental scalds from a pulled cup produce irregular splash marks over the head, neck and upper trunk with superficial depth and a clear history of a spill. Inflicted immersion burns produce a sharp tide-mark, a stocking or glove distribution on a limb, or a doughnut-sparing pattern on the buttocks where the child was held against the cooler bath floor, and the history does not fit the developmental stage or the burn. A delay in presentation, a non-mobile infant with any burn, and repeated presentation raise the probability of inflicted injury or neglect until proven otherwise. [9]
Why must the differential be revised after each reassessment? Because the burn evolves. An airway that was safe can be lost; a depth that was superficial dermal can deepen; a child who looked well can develop burn shock as the leak progresses. The differential is a live document, not a single statement at the doorway. [2] [8]
Clinical & Bedside Assessment
The primary survey of the burn child is the standard ABCDE adapted for the burn, and the adaptation is in what you look hardest for at each letter. At A, look for the inhalation signs and protect a threatened cervical spine if there is a fall or blast. At B, look for respiratory distress, reduced air entry, and the chest compliance change of a constricting torso burn. At C, look for shock and confirm the percent TBSA that drives fluid. At D, check the conscious state for carbon monoxide and cyanide, and the bedside glucose. At E, expose fully but briefly to map the burn, then warm immediately. [2] [8]
Estimating TBSA is a bedside skill the examiner will press. Use the age-adjusted Lund and Browder chart, not the Rule of Nines. Draw the burn on the chart's body map, count the partial- and full-thickness areas only, and exclude erythema. For small or patchy burns, use the patient palm including fingers as one percent. Record the number as a single percent TBSA, because that number drives the fluid calculation and the admission decision. If the area is uncertain after cleaning, re-map and document the second estimate; bedside and app-based estimates disagree often, and the burn is re-mapped at the burns centre. [5] [6]
Assessing depth is the second bedside skill. Examine the burn after cooling, in good light. Look at colour (pink, fixed red, white, waxy, charred), test for blanching with firm pressure, look for blisters, assess sensation (a deep burn is less painful because the nerves are destroyed), and note capillary return. Map depth onto the same chart as area. State your uncertainty openly: depth evolves, and a burn that looks superficial dermal at one hour may declare itself deep dermal at 48 hours. A first assessment is provisional, and the burns service makes the final surgical call. [1] [3]
Special-site assessment changes the referral. Examine the face for airway and eye involvement, the hands for function and digital perfusion, the feet for weight-bearing and perfusion, the perineum and genitalia for urinary retention and infection risk, and the major joints for contracture risk. A small burn at any of these sites triggers a burns-centre consultation, because the long-term functional outcome is determined by the site as much as by the size. Document function and perfusion at the first assessment, because the trend matters. [2] [3]
Take a focused history in parallel without delaying stabilisation. Capture the mechanism (what burned, temperature, contact time, enclosed space), the time of injury (which sets the fluid clock), the first aid given (water, duration, time from injury), the immunisation and tetanus status, the past medical history and any relevant disability, and the safeguarding context (who was present, the developmental stage, prior presentations). Caregiver concern that the child is different from usual is information, not anxiety. Ask open, non-leading questions and record the exact words used to describe the mechanism. [9] [2]
Document the burn objectively and completely. Draw the burn on a Lund and Browder map in the chart, state the percent TBSA and the depth by region, photograph the burn with consent and a ruler for scale (this is also safeguarding evidence), and record the time of injury and the first aid given. Objective, timed documentation is what transfers the child safely forward, supports the safeguarding assessment, and protects the child and the team. Confronting the family is never part of this; the pathway is run in parallel, by the right people, with the right consent. [9] [10]
Investigations
Name the question before you order any test, because most burns need very few investigations in the first hour. The immediate bedside investigations are oxygen saturation, a credible blood pressure and pulse, a point-of-care glucose (especially in the infant and toddler, who can become hypoglycaemic), and an ECG in any electrical injury. A venous gas with lactate and carboxyhaemoglobin is drawn when inhalation is suspected, and a blood group and crossmatch is taken at first access for the larger burn. [2] [8]
The carboxyhaemoglobin level answers the carbon monoxide question. A level drawn on air or on oxygen estimates the exposure, but it falls with time and with oxygen, so a normal level does not exclude significant exposure in a child who has been on oxygen for an hour. Treat the child, not the number: a child with a history of enclosed fire and confusion or reduced conscious state receives high-flow oxygen for a prolonged period regardless of the initial reading. A high lactate that does not clear with fluids raises cyanide toxicity from burning plastics, and a low threshold for the cyanide antidote kit is appropriate in the severely poisoned enclosed-fire child. [8]
Blood tests for the larger burn are drawn at first access and answer three questions: is there anaemia or coagulopathy (full blood count, coagulation), is the child ready for transfusion and theatre (group and crossmatch), and is there electrolyte or renal disturbance (urea, creatinine, electrolytes). These are sent at the first cannula, not as a separate venepuncture, and they are repeated as the resuscitation evolves. A beta-hCG is considered in the adolescent girl. [2] [7]
Imaging is conditional on the question. A chest radiograph is taken when there is blast, inhalation or a constricting torso burn. Bronchoscopy and laryngoscopy assess the airway and lower respiratory tract in suspected inhalation injury, usually at the burns or intensive care unit. Computed tomography is reserved for the child with associated major trauma. Photography is an investigation of the burn itself: serial photographs at fixed intervals document healing and support the safeguarding record. An unstable child belongs in resuscitation or theatre, not in a scanner. [8] [2]
Management — Resuscitation
Run the resuscitation as a team, and the first team action is to stop the burning process and cool the burn. Remove clothing and jewellery, irrigate chemicals, and cool the burn with cool running water, about 8 to 25 degrees Celsius, for 20 minutes, ideally within 3 hours of injury. The evidence is that 20 minutes of cool running water reduces burn depth and improves outcome, and that benefit persists when cooling is started up to 3 hours after the burn. Ice, iced water and very cold water are harmful because they cause vasoconstriction that deepens the burn and because they produce hypothermia, which the small child reaches fast. Throughout cooling, keep the rest of the child covered and warm. [4] [3]
Cool running water (first aid)
Protect the airway next. Any child with signs of inhalation injury after an enclosed fire is a child with a finite window for a safe airway. Call senior airway expertise early, prepare a calibrated difficult-airway plan, and have a low threshold for a definitive airway before oedema closes it. Repeated traumatic attempts at intubation in a swollen airway make the next attempt harder. Give high-flow oxygen, and treat carbon monoxide and cyanide as described. Do not wait for stridor; stridor is a late sign in the burned airway and the airway may already be lost. [8] [2]
Hartmann solution (compound sodium lactate) — modified-Parkland burn resuscitation
For the larger burn, start formal fluid resuscitation at 10 percent TBSA or more. The modified-Parkland calculation is 3 mL of Hartmann per kilogram per percent TBSA over the first 24 hours, with half of that volume in the first 8 hours from the time of injury. In the infant and young child, add glucose-containing maintenance fluid in addition to the resuscitation volume, because the burned infant can become hypoglycaemic. The formula is a starting point, not a target: titrate the rate hourly to a urine output of 1 mL per kilogram per hour in children under about 30 kg, and 0.5 mL per kilogram per hour in larger children and adolescents. A falling output means give more; a rising output means give less. [2] [7]
Weight-based vs body-surface-area-based fluid predictions in paediatric burns
Burns
Comparison of weight-based and body-surface-area-based formulae for predicting 24-hour fluid resuscitation volume in paediatric burn patients.
Key finding
Formulae give materially different predicted volumes for the same child, reinforcing that the calculated volume is a starting point to be titrated to physiological endpoints such as urine output, not a target.
Practice change
Modified-Parkland calculation is the starting estimate; hourly titration to urine output and perfusion, not the formula, decides the actual rate.
Analgesia is part of resuscitation, not an afterthought, and undertreated pain in a burn is harmful and common. Give weight-based titrated analgesia early: intranasal fentanyl or intravenous morphine, with paracetamol as the foundation, and reassess the response. Procedural sedation, where used for dressing, follows its dedicated paediatric pathway with monitoring and trained staff. A child in pain cannot be assessed properly and does not breathe well. [3] [2]
Correct a dangerous low glucose immediately in the burned young child, because hypoglycaemia is a real risk during resuscitation in the infant and toddler, and it is missed easily. Check glucose at the bedside early and again during resuscitation, and treat a low value with intravenous glucose. Active warming is part of resuscitation: keep the child covered, use warmed fluids and a radiant warmer, and target a normal temperature, because a cold child is harder to resuscitate, coagulopathic, and metabolically unstable. [2] [3]
Management — Definitive & Stepwise
Once the child is cool, oxygenated, analgesed and the fluid plan is running, move to definitive wound care and disposition. Cover the burn with cling film after cooling and assessment; cling film reduces pain by protecting exposed nerve endings and allows the burn to be seen without removing the dressing. Do not apply topical creams, especially not silver sulfadiazine, at this stage, because they obscure the burn for assessment and are not first-line emergency department management; dressings and topical agents are chosen with the burns service. Routine antibiotics are not given prophylactically in the first instance. [3] [2]
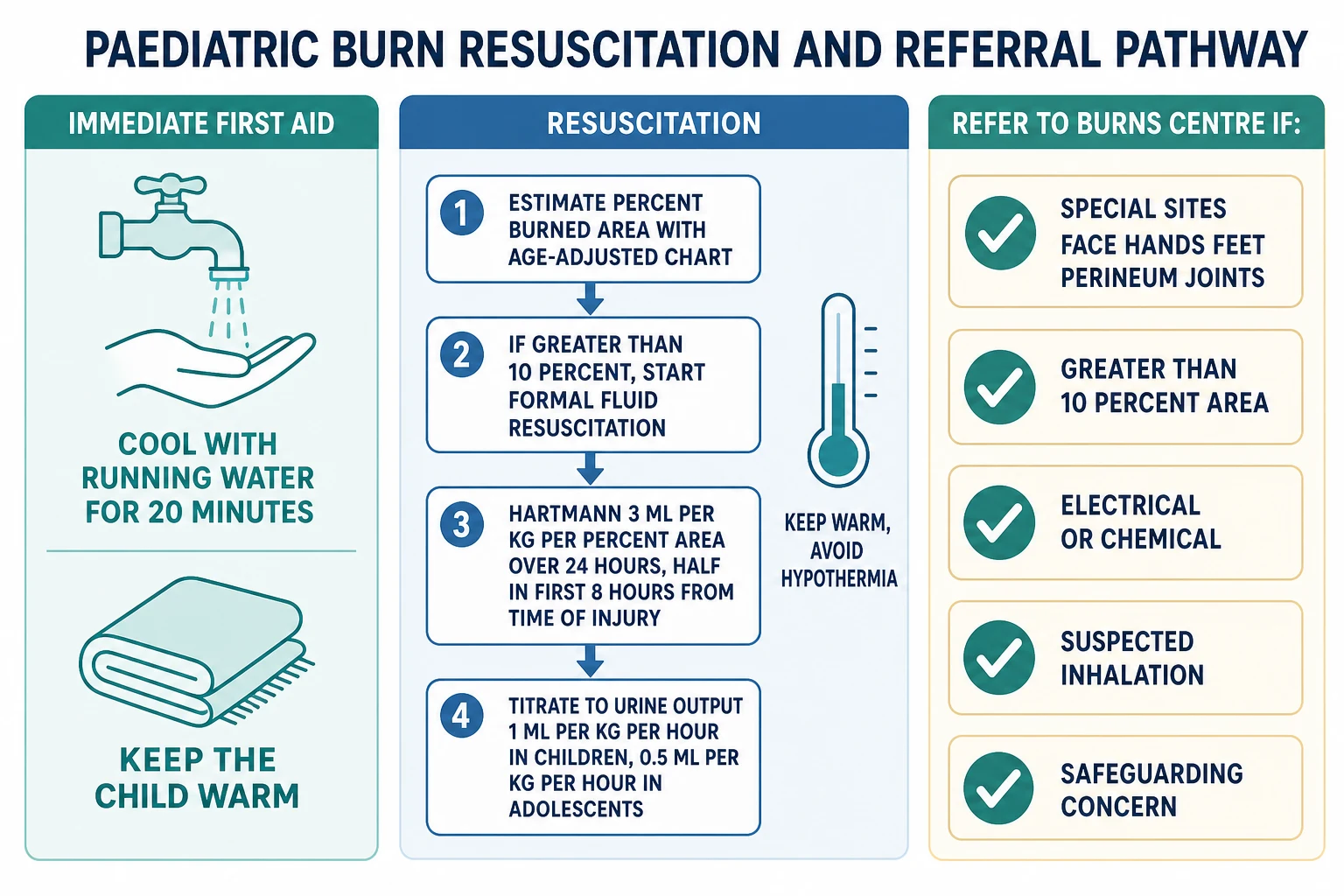
Check tetanus status and give prophylaxis according to the local schedule, with tetanus immunoglobulin for the child with uncertain immunisation status or a contaminated wound. Decide the destination from size, depth, site, mechanism, age and safeguarding, not from one observation. Apply the burns-centre referral criteria, and remember that safeguarding concern alone is a referral criterion: a child with suspected inflicted injury is discussed with the burns service and the child-protection team together, not managed in isolation. [2] [9]
Construct a fluid plan that combines resuscitation and maintenance and monitor it hourly. Reassess urine output, perfusion, capillary refill, temperature and conscious state at each interval, and adjust the rate: a falling output means under-resuscitation and a rising output means over-resuscitation, and both are dangerous. Over-resuscitation causes oedema, compartment syndrome and pulmonary compromise; under-resuscitation causes poor perfusion and renal injury. The formula gives the starting point; the child gives the answer. [2] [7]
A defensible disposition requires sustained stability, a controlled airway, a running fluid plan with a documented urine output trend, an agreed surgical and referral plan, a structured handover, and a usable safety net. Confirm caregiver understanding with teach-back, document the warning signs, the urgency and the access route, and name who owns pending results. Run safeguarding documentation and referral in parallel with the clinical plan, and never let a safeguarding concern wait for the diagnosis to settle. [10] [9]
Specific Subtypes & Scenarios
The infant or toddler needs the most adaptation. Estimate TBSA with the age-adjusted chart, add glucose-containing maintenance to the resuscitation, warm actively, and keep a high threshold of suspicion for safeguarding, because a burn in a non-mobile infant carries a high probability of inflicted injury until proven otherwise. Hypoglycaemia and hypothermia develop fast and are missed easily, so check glucose and temperature early and often. [2] [9]
The child with suspected inhalation injury needs an early definitive airway, high-flow oxygen, a venous gas with carboxyhaemoglobin and lactate, and a low threshold for cyanide antidote in the severe enclosed-fire child. They are transferred to a burns or intensive care service for ongoing airway and respiratory support, and bronchoscopy is performed there to grade the injury. The airway is reassessed continuously, because the swelling evolves. [8] [2]
The child with a circumferential limb or chest burn needs urgent burns-centre referral and consideration of escharotomy. Monitor perfusion of the digits and ventilation of the chest continuously, document the trend, and do not delay transfer for the procedure if the local team cannot perform it. A pulse that was present can be lost; a chest that was ventilating can become restrictive. [2] [8]
Electrical injury is deceptive because the skin damage underestimates the deep tissue injury. Apply cardiac monitoring and an ECG, look for an entry and exit wound, assess for compartment syndrome, and arrange burns-centre transfer. Chemical injury is managed by copious water irrigation, identifying the agent, brushing dry powders off before irrigation, continuing irrigation, and seeking specialist advice for specific agents such as hydrofluoric acid, which causes hypocalcaemia and deep tissue injury. [2] [8]
The small contact or scald burn that meets no referral criterion is cooled, dressed, given analgesia, and discharged with follow-up and a safety net. The safety net states what to watch for (spreading redness, increasing pain, fever, reduced use of a hand, reduced perfusion), how urgently to act, and exactly where to get help. A first-aid and prevention conversation with the family is part of the encounter, because most of these burns are preventable. [3] [10]
The child with suspected inflicted burn or scald is resuscitated and stabilised first, with safeguarding running in parallel. Stabilise the airway and the burn, document objectively with a Lund and Browder map and photographs, ask only necessary open non-leading questions, preserve clothing and the dressing for forensic review, and activate the local child-protection pathway. Do not confront the family; the pathway is run by the right people, with the right consent, at the right time. The inflicted-burns-and-scalds topic carries the deeper forensic detail. [9]
In a rural or remote setting, cool the burn, start the fluid plan, keep the child warm, and call retrieval and the burns centre in parallel, before local support is exceeded. State the current problem, the percent TBSA and depth, the special sites, the time of injury, the first aid and fluid given, the airway status, the safeguarding context, the expected response, the destination, and the contingency for deterioration and transfer delay. Transport time is a clinical variable that you manage, not discover. [10] [2]
The child who has swallowed or inserted a button battery is a burns-adjacent emergency that crosses safeguarding and surgical lines. A battery lodged in the oesophagus causes local tissue damage within hours through electrolysis and liquefaction, and a delay of even a few hours can produce a fistula, a stricture, or a fatal haemorrhage. Suspected button battery in the oesophagus is an urgent endoscopy within hours, not observation; do not wait for symptoms to develop. This presentation sits inside the safeguarding assessment whenever the history is unclear. [11] [9]
Complications & Pitfalls
Most preventable harm comes from acting in the wrong order or stopping too early. No cooling at all, ice instead of running water, cooling to hypothermia, underestimating TBSA, and forgetting the airway are classic and dangerous errors. Prevent them by stating at every step what you will assess, what you will do, what change you expect, and what you will reassess. The burn is a live problem, not a single declaration at the door. [2] [4]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| No cooling, or ice instead of running water | Burn deepens; vasoconstriction and hypothermia | 20 minutes of cool running water within 3 hours of injury; keep the child warm |
| Rule of Nines in a small child | Wrong TBSA; wrong fluid calculation | Use the age-adjusted Lund and Browder chart |
| Including erythema in TBSA | Over-estimation; over-resuscitation | Count partial- and full-thickness only; exclude erythema |
| Fluid clock from arrival, not time of burn | Under-delivery in the first 8 hours | Calculate from the time of injury |
| Large-volume normal saline | Hyperchloraemic acidosis | Use balanced Hartmann solution; titrate to urine output |
| Waiting for stridor before intubation | Airway lost to evolving oedema | Plan early definitive airway; call senior help early |
| Delaying circumferential burn referral | Compartment syndrome; restrictive chest | Refer urgently; consider escharotomy; do not wait for pulse loss |
| Confronting the family on safeguarding | Loss of trust and of safety | Stabilise first; document objectively; run the pathway in parallel |
Both under- and over-resuscitation are harmful. Under-resuscitation causes poor perfusion, acute kidney injury and deepening of the zone of stasis; over-resuscitation causes oedema, compartment syndrome and pulmonary compromise. The defence is hourly titration to urine output and perfusion, not loyalty to a formula. Watch for the late complications once the child is stable: wound infection and sepsis, scarring and contracture, itch and psychosocial impact, and missed safeguarding. Each has its own pathway, and each is reduced by adherence to the small set of process measures that define good burn care. [7] [10]
[2] [9]Prognosis & Disposition
Outcome is determined by the size and depth of the burn, the presence and severity of inhalation injury, the age and comorbidity of the child, the speed of cooling and resuscitation, the avoidance of secondary injury, and the capability and timeliness of definitive burns care. Children have greater physiological reserve than adults but can decompensate steeply, so a good outcome depends on early cooling, an accurate TBSA, a titrated fluid plan, an early definitive airway when needed, and a system that delivers the right care in time. [10] [2]
Theatre or critical care
- Threatened or lost airway from inhalation injury
- Major burn with burn shock needing titrated resuscitation
- Circumferential burn needing escharotomy
- Carbon monoxide or cyanide poisoning
- Safeguarding concern with an unsafe home
Admission or burns centre transfer
- 10 percent TBSA or more receiving modified-Parkland
- Special-site burn (face, hands, feet, perineum, joints)
- Full-thickness burn likely to need surgery
- Electrical, chemical or inhalation injury
- Safeguarding concern in progress
Discharge only when defensible
- Small area, no special site, no safeguarding concern
- Depth likely to heal within 2 to 3 weeks
- Adequate analgesia and a usable safety net
- Carer understanding confirmed and follow-up agreed
An executable safety net states what change to watch for (spreading redness, increasing pain, fever, reduced use of a hand, reduced perfusion, reduced conscious state), how urgently to act, and exactly where to get help. It states when review will occur, who owns pending results, and what to do if access is difficult. After the encounter, explain honestly to the child and family what happened, what remains uncertain, what the scarring and rehabilitation pathway looks like, and what the next steps are. A recurrent or unexplained presentation needs senior review and reconsideration of safeguarding. [9] [12]
Long-term outcome includes scarring, contracture, itch, and the psychosocial impact of a visible burn on the child and the family. Partial-thickness burns in children produce measurable scar and quality-of-life effects at 3 and 6 months, and early engagement with the burns and rehabilitation pathway reduces these. The encounter is not over at discharge; the safety net and the follow-up are part of the treatment. [12] [10]
Special Populations
Adapt how you observe and communicate, but never lower the standard for recognising deterioration. The infant and toddler receives the age-adjusted chart, glucose-containing maintenance, active warming, and a high safeguarding threshold. The child with chronic disease, immunocompromise, neurodisability or limited mobility is assessed against their personal baseline, with attention to a burn that may interact with a device or a pressure area, and with their emergency plan where one exists. [2] [9]
The adolescent needs private time and the chance to speak alone, with questions about consent, self-harm and risk, and a clear explanation of confidentiality and its limits. The technology-dependent child is assessed with their device and personal baseline in mind. For indigenous, migrant, asylum-seeking or remote families, use cultural safety and a professional interpreter, and address the access and transport barriers that change what a discharge plan can deliver. [9] [10]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Infant or toddler | Age-adjusted TBSA, glucose maintenance, active warming, high safeguarding threshold | Hypoglycaemia and hypothermia develop fast; check often |
| Chronic disease, immunocompromise or neurodisability | Personal baseline; device and pressure-area interaction | A chronically abnormal observation is not automatically safe |
| Adolescent | Private time; ask about self-harm and consent; explain confidentiality limits | Confidentiality has safety limits; safeguarding duties still apply |
| Indigenous, migrant or remote family | Cultural safety; professional interpreter; address access and transport | Retrieval and safeguarding routes remain jurisdiction-specific |
Safeguarding runs in parallel with burn care, but immediate stabilisation and safety come first. Ask only necessary open, non-leading questions. Explain confidentiality and information sharing, document objective findings and the exact words used to describe the mechanism, preserve clothing and the dressing for forensic review when safe, and use the local safeguarding pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory, so name the jurisdiction you are operating in. [9] [10]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The strongest evidence in paediatric burns supports the simplest actions. Twenty minutes of cool running water within 3 hours of injury reduces burn depth and improves outcome; this has observational and laboratory support and is consistent across guidelines. The age-adjusted Lund and Browder chart is the standard for paediatric TBSA estimation, and the Rule of Nines is wrong in small children because it ignores the changing proportion of the head and legs. Modified-Parkland resuscitation with balanced Hartmann solution, started at 10 percent TBSA or more and titrated to urine output, is the consensus starting point, but the exact formula and the role of colloid remain debated. [4] [2]
Cool running water first aid and burn outcome
Burns and Lancet Child and Adolescent Health
Synthesis of observational and experimental studies of cool running water first aid in partial-thickness paediatric burns, with mechanistic work on depth of injury.
Key finding
Cool running water for 20 minutes, ideally within 3 hours of injury, reduces burn depth, the need for grafting, and time to healing. Ice and very cold water are harmful.
Practice change
Established as the standard of first aid across ANZ, UK, US and Canadian guidance.
Where the evidence is weaker: the exact fluid formula in the youngest children, the role of routine antibiotics, the ideal dressing for partial-thickness burns, and the prediction of long-term scar outcome. Variation in paediatric burn care across hospitals is large, and adherence to a small set of process measures (cooling, TBSA estimation, fluid titration, referral, safeguarding) is associated with better outcome, which is the core argument for managing the burned child inside an organised burn-care system rather than in isolation. State the strength and the population of each rule you quote. [10] [2]
Jurisdictional implementation
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne Burns guideline and the Australian and New Zealand Burn Association support practice. Cooling with running water for 20 minutes within 3 hours, modified-Parkland Hartmann at 3 mL per kg per percent TBSA, titration to urine output of 1 mL per kg per hour in children and 0.5 mL per kg per hour in adolescents, and referral to a burns centre for special sites, 10 percent TBSA or more, full thickness, electrical, chemical, inhalation, comorbidity and safeguarding concern are the standard. Retrieval is coordinated through state services, and mandatory reporting and consent remain jurisdiction-specific.
[2][3]Global and low-resource settings: the principles of cooling, age-adjusted TBSA, modified-Parkland resuscitation and referral are globally applicable, but the system around them varies. Adapt activation, fluid, blood-bank and retrieval expectations to local resources, and do not transplant a protocol uncritically across populations and capabilities.
Exam Pearls
First aid
- Cool with running water for 20 minutes within 3 hours of injury
- No ice, no very cold water
- Keep the rest of the child warm
- Remove clothing and jewellery
Assessment
- Age-adjusted Lund and Browder chart, not the Rule of Nines
- Exclude erythema from percent TBSA
- Patient palm including fingers is about 1 percent
- Re-map after cleaning; depth evolves over 48 hours
Resuscitation
- Formal fluid at 10 percent TBSA or more
- Hartmann 3 mL per kg per percent over 24 hours
- Half in the first 8 hours from the time of injury
- Add glucose maintenance in the young child
- Titrate to urine output: 1 mL/kg/h under 30 kg, 0.5 mL/kg/h adolescents
- Avoid large-volume normal saline
Airway and inhalation
- Singed hair, soot, voice change, stridor need early definitive airway
- Carboxyhaemoglobin and lactate in enclosed fires
- Cyanide antidote in severe enclosed-fire poisoning
- Circumferential burn needs urgent referral and escharotomy
Referral
- Special sites: face, hands, feet, perineum, major joints
- 10 percent TBSA or more
- Full thickness, electrical, chemical, inhalation
- Comorbidity and any safeguarding concern
Safeguarding
- Objective documentation and Lund and Browder map
- Non-leading questions; photograph with consent
- Run the pathway in parallel; do not confront the family
- Button battery in the oesophagus is urgent endoscopy within hours
“Stop and cool for 20 minutes within 3 hours → age-adjusted Lund and Browder, exclude erythema → recognise the airway and inhalation → modified-Parkland Hartmann at 10 percent or more, titrate to urine output → refer for special sites, large area, full thickness, electrical, chemical, inhalation, comorbidity or safeguarding → run safeguarding in parallel and hand over safely.”
Viva: a toddler with a scald and a normal-looking airway
Describe the child objectively, then cool the burn with running water for 20 minutes within 3 hours of injury while keeping the child warm. Run ABCDE adapted for the burn, looking hardest for the airway and inhalation. Estimate the percent TBSA with an age-adjusted Lund and Browder chart, exclude erythema, and judge depth. Start modified-Parkland Hartmann at 3 mL per kg per percent over 24 hours with half in the first 8 hours from the time of injury if the burn is 10 percent or more, add glucose maintenance in the young child, and titrate to a urine output of 1 mL per kg per hour. Take a focused history, apply the burns-centre referral criteria, run safeguarding in parallel, and hand over safely. [2] [3]
Viva: an enclosed-fire child with a hoarse voice
A hoarse voice after an enclosed fire is a threatened airway. I call senior airway expertise early, prepare a calibrated difficult-airway plan, and have a low threshold for an early definitive airway before oedema closes it. I give high-flow oxygen, draw a venous gas with carboxyhaemoglobin and lactate, and treat carbon monoxide with prolonged high-flow oxygen; a high lactate that does not clear with fluids raises cyanide toxicity and a low threshold for the cyanide antidote kit. I cool and assess the burn, start the fluid plan, and transfer to a burns or intensive care service for ongoing airway and respiratory support, with bronchoscopy performed there. I do not wait for stridor.
Structured oral: safeguarding in a non-mobile infant with a scald
I stabilise the airway and the burn first, then run safeguarding in parallel. I document the burn objectively on a Lund and Browder map and photograph it with consent, ask only necessary open non-leading questions and record the exact words, preserve the clothing and the dressing for forensic review, and activate the local child-protection pathway. A burn in a non-mobile infant carries a high probability of inflicted injury until proven otherwise, so I discuss the child with the burns service and the child-protection team together. I do not confront the family, and I keep the child safe while the assessment proceeds.
References
- [1]Hettiaratchy, S Initial management of a major burn: I--overview BMJ, 2004.PMID 15217876
- [2]Hettiaratchy, S Initial management of a major burn: II--assessment and resuscitation BMJ, 2004.PMID 15242917
- [3]Cuttle, Leila Management of non-severe burn wounds in children and adolescents: optimising outcomes through all stages of the patient journey The Lancet Child and Adolescent Health, 2022.PMID 35051408
- [4]Cuttle, Leila The efficacy of Aloe vera, tea tree oil and saliva as first aid treatment for partial thickness burn injuries Burns, 2008.PMID 18603378
- [5]Colson, Christopher D EasyTBSA as a method for calculating total body surface area burned: a validation study Emergency Medicine Journal, 2023.PMID 36639224
- [6]Choi, Jooyoung Practical Computer Vision Application to Compute Total Body Surface Area Burn: Reappraising a Fundamental Burn Injury Formula in the Modern Era JAMA Surgery, 2022.PMID 34817552
- [7]Stevens, Jacob V Weight-based vs body surface area-based fluid resuscitation predictions in pediatric burn patients Burns, 2023.PMID 35351355
- [8]Toon, Marcus H Management of acute smoke inhalation injury Critical Care and Resuscitation, 2010.PMID 20196715
- [9]Mullen, Sophie Fifteen-minute consultation: Childhood burns: inflicted, neglect or accidental Archives of Disease in Childhood - Education and Practice, 2019.PMID 29934360
- [10]Kazis, Lewis E Development of clinical process measures for pediatric burn care: Understanding variation in practice patterns Journal of Trauma and Acute Care Surgery, 2018.PMID 29140950
- [11]Krom, H The incidence and complication rate of pediatric battery ingestion in the Netherlands European Journal of Pediatrics, 2026.PMID 41563491
- [12]Gee Kee, Emma L Scar outcome of children with partial thickness burns: A 3 and 6 month follow up Burns, 2016.PMID 26546385