Paeds · acute-care-resuscitation-and-toxicology
Button-battery and magnet ingestion
Also known as Button battery ingestion in children · Disc or lithium cell ingestion · High-powered magnet ingestion · Neodymium magnet ingestion · Oesophageal foreign body emergency
A fellowship approach to the child with suspected button-battery or magnet ingestion. Treat any oesophageal button battery as a time-critical emergency requiring endoscopic removal within two hours, recognise the mechanism of alkaline liquefaction at the negative pole and the risk of delayed life-threatening fistula and perforation, give honey or sucralfate as a bridge in the eligible child older than twelve months who can swallow while awaiting removal, manage two or more magnets as a high-risk situation because attracting magnets across bowel walls cause fistula, obstruction and perforation, and run safeguarding and prevention in parallel.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Button-battery and magnet ingestion describes the accidental, and occasionally intentional, swallowing of a disc or lithium cell battery, or of one or more small permanent magnets, by an infant or child. Both are common, both can be asymptomatic at first, and both can kill within hours of an event the family may not have witnessed. The shared message is that an innocent-looking household object, retained in the oesophagus or trapped between bowel loops, can inflict devastating injury long before the child looks unwell. [1] [3]
The two threats work through different mechanisms but share a single clinical discipline: act on the possibility, image early, and remove an oesophageal battery or attracting magnets before tissue is destroyed. A button battery trapped against the oesophageal mucosa generates hydroxide by electrolysis of tissue water at its negative pole, producing alkaline liquefaction necrosis that worsens by the minute and continues after the battery is removed. Two or more magnets, or a magnet and any ferrous object, attract one another across opposing bowel walls, trapping and ischaemia the intervening tissue until a fistula, perforation or volvulus forms. [1] [9]
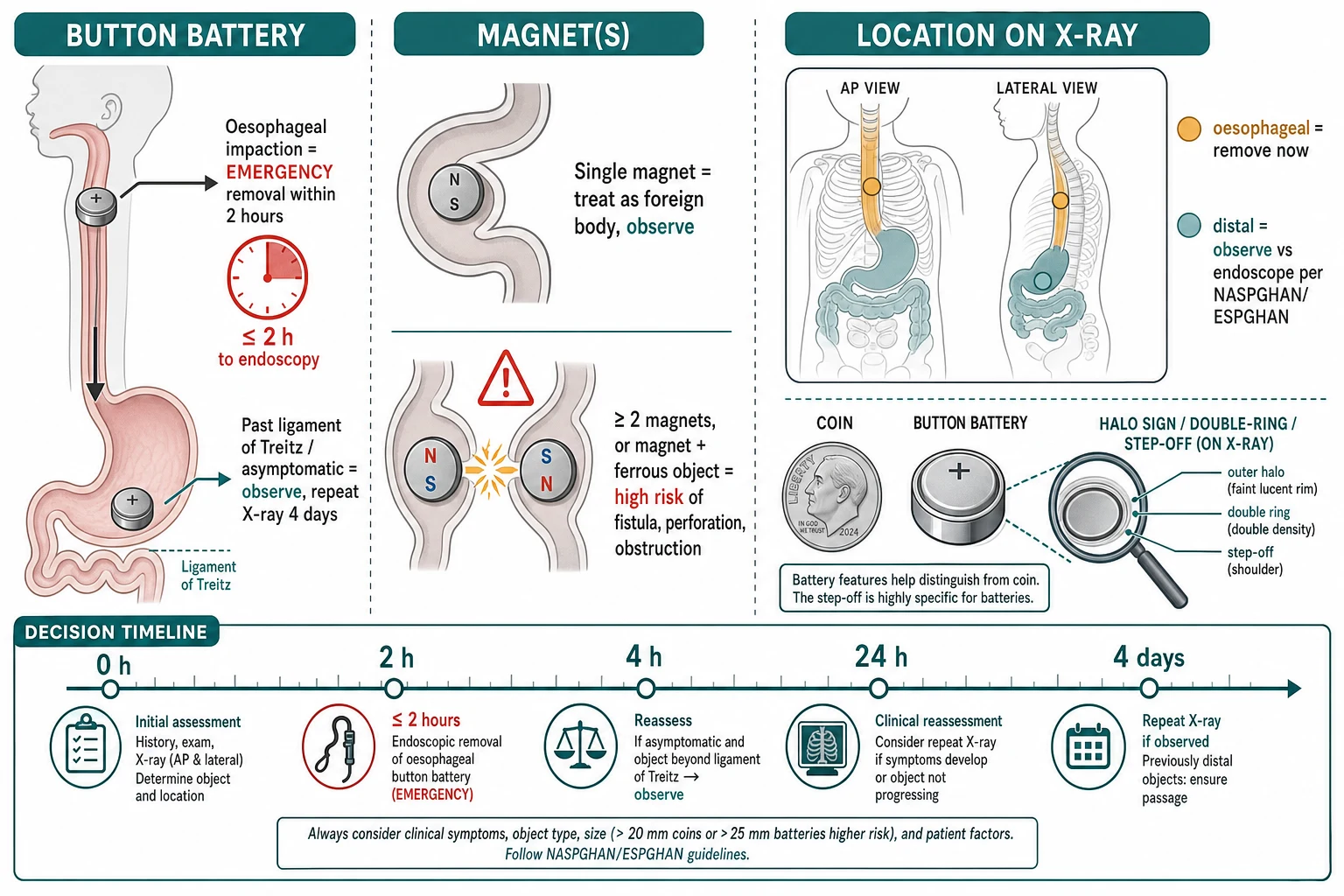
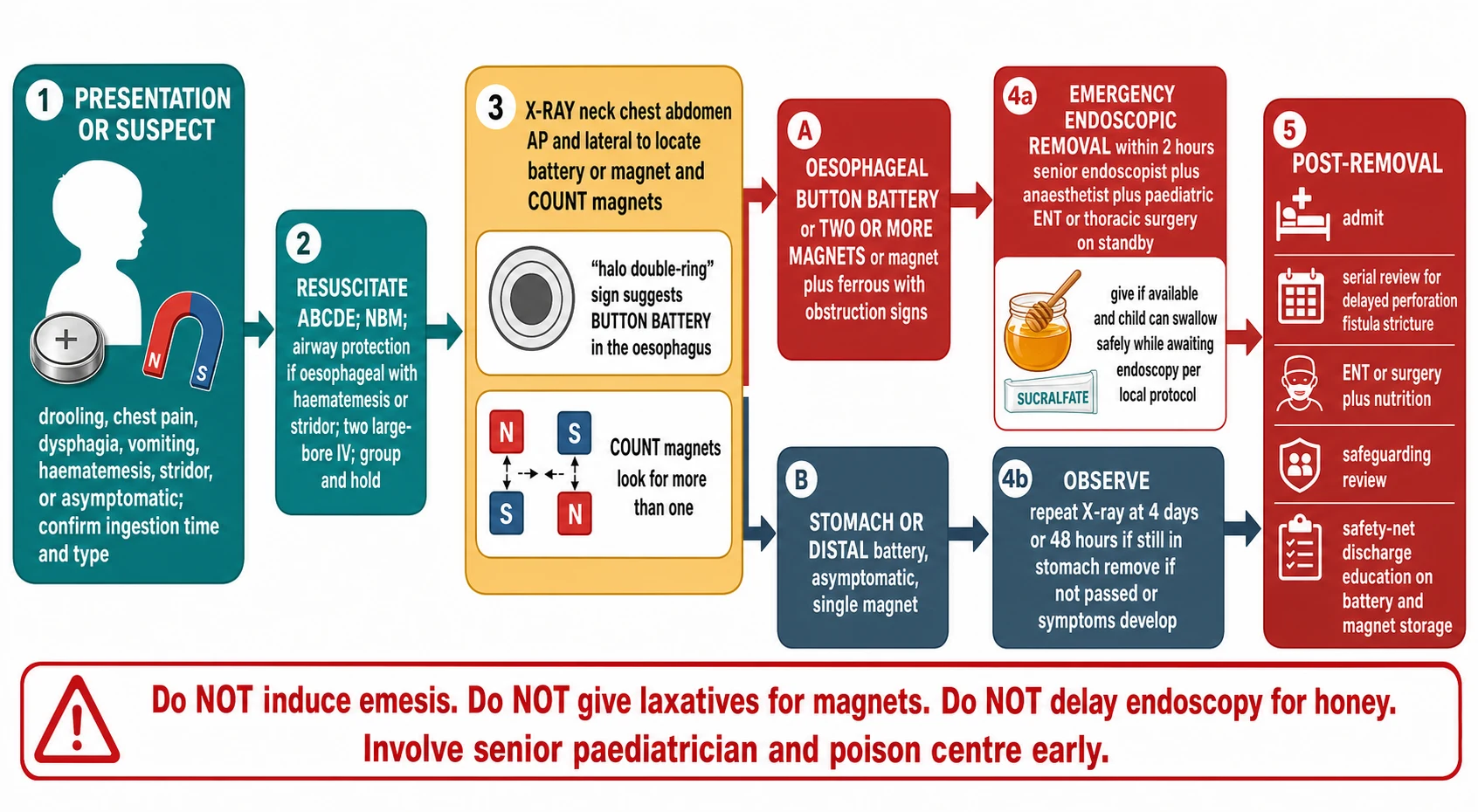
[1] [2]The clinical approach runs inside the broader paediatric primary survey. Airway, breathing and circulation are supported first, because drooling, stridor, haematemesis or a child who cannot protect their airway may signal an oesophageal battery or a complication. The history seeks the object, the time of ingestion, the type and number if known, and any symptoms. A single radiograph confirms the location, distinguishes a battery from a coin, and counts magnets. The plan then divides sharply by location and object: oesophageal battery and attracting magnets are emergencies; a distal, asymptomatic single object can often be observed with planned repeat imaging. [2] [9]
The first hour of suspected battery or magnet ingestion
Suspect and confirm
Ask about ingestion time, object type and symptoms. Treat drooling, dysphagia, chest pain, haematemesis, stridor or vomiting as an oesophageal battery until proven otherwise.
Resuscitate
Secure airway and breathing, give oxygen, establish access, and keep the child nil by mouth. Protect the airway aggressively if there is stridor or haematemesis.
Localise and count
Take one radiograph from nasopharynx to anus in AP and lateral views. Identify the halo or double-ring sign of a battery, confirm oesophageal versus gastric position, and count magnets.
Bridge if eligible
For an oesophageal battery in a child older than twelve months who can swallow safely, give honey 10 millilitres every ten minutes up to six doses while awaiting removal. It never replaces endoscopy.
Remove or observe
Oesophageal battery and two or more magnets get emergency removal within two hours. A distal asymptomatic single object is observed with planned repeat imaging.
Reassess and protect
Watch for delayed perforation, fistula and stricture after removal. Run safeguarding and prevention education in parallel, and give a clear safety net.
Classification
Classify the ingestion on three axes at once: what the object is, where it sits, and how many there are. These three answers drive almost every decision that follows, because a battery in the oesophagus behaves nothing like a battery in the stomach, and two magnets behave nothing like one. [2] [9]
| Axis | Category | What it means | First response |
|---|---|---|---|
| Object | Button or lithium cell battery | Disc cell that generates hydroxide and direct-current injury when lodged against mucosa | Confirm location; remove oesophageal batteries within two hours |
| Object | Single magnet | One permanent magnet, usually neodymium, that cannot attract across tissue alone | Treat as a standard foreign body; observe and repeat image |
| Object | Two or more magnets, or magnet plus ferrous object | Components that attract across bowel walls and trap intervening tissue | Treat as high-risk; remove if in the stomach or beyond reach of endoscopy, or if any signs develop |
| Location | Oesophageal | Object lodged from cricopharyngeus to gastro-oesophageal junction | Emergency, time-critical removal within two hours for a battery |
| Location | Stomach or distal bowel | Object has passed the gastro-oesophageal junction | Observe asymptomatic batteries and single magnets; remove if not passed or symptomatic |
| Number | One versus many | Count magnets carefully on imaging | Two or more magnets change the plan from observe to remove |
The radiograph itself helps classification. A button battery seen face-on shows a characteristic halo or double-ring caused by the step between the larger positive casing and the smaller negative casing, and on a lateral view a step-off or notch at one edge distinguishes it from a coin. The halo and double-ring signs are the bedside signals that an apparently round radio-opacity is a battery and not a coin, and they should be sought deliberately on every film. [1] [3]
Magnet classification turns on the count. A single magnet carries the low-grade risk of any foreign body, but two or more magnets, or a magnet paired with a coin, battery fragment or other ferrous object, can attract one another through opposing loops of bowel, compressing and ischaemia the trapped wall until a fistula, perforation or volvulus forms. Counting the magnets on imaging, and asking the family how many were in the set, is therefore a clinical act, not a clerical one. [9] [12]
Epidemiology & Risk Factors
Button-battery and magnet ingestions cluster in mobile infants and preschool children who explore the world with their mouths. Button batteries are now ubiquitous in hearing aids, remote controls, toys, flameless candles, watches and key fobs, and the larger twenty-millimetre lithium cells cause the most severe injuries because they are large enough to lodge in a child's oesophagus and powerful enough to injure rapidly. High-powered neodymium magnet sets, sold as desk toys and building sets, are the dominant cause of severe multiple-magnet injuries. [3] [11]
Button battery
- Peak age under six years; mobile infants and preschool children
- Larger 20 mm lithium cells lodge in the oesophagus and injure fastest
- Hearing aids, remote controls, toys and flameless candles are common sources
- Most events are unwitnessed, and the family often does not know a battery was swallowed
High-powered magnet
- Neodymium desk-toy and building-set magnets cause severe injuries
- Two or more magnets, or a magnet plus a ferrous object, are the dangerous pattern
- Regulatory sales bans reduce exposures; relaxation brings them back
- Older children and adolescents may ingest magnets intentionally
Child and context
- Developmental mouthing behaviour in mobile infants and toddlers
- Neurodevelopmental disability and pica raise recurrence risk
- Easy household access to unsecured batteries and magnets
- Rural and remote location changes escalation and retrieval timing
Safeguarding signal
- Recurrent ingestion warrants a safeguarding and supervision review
- Multiple batteries or magnets accessible to the child
- Inconsistent history or delayed presentation
- Keep prevention and supervision open alongside acute care
Severity rises with battery size, with oesophageal position, and with longer contact time. The larger twenty-millimetre lithium cells account for the majority of severe and fatal outcomes, and a battery retained in the oesophagus for more than a few hours carries a steeply rising risk of perforation and fistula. High-powered magnet exposures fell after regulatory action restricting sales, then rose again when those restrictions eased, illustrating how the epidemiology follows the marketplace as much as child behaviour. [11] [10]
Pathophysiology
A button battery injures the oesophageal wall through three converging mechanisms that all intensify the longer the battery remains in contact. The dominant mechanism is electrolysis: the battery, bathed in oesophageal mucus and tissue fluid, acts as a galvanic cell and splits water at its negative pole, generating hydroxide ions that drive a local alkaline burn. Alkali liquefies tissue, so the injury penetrates deeply and progressively rather than forming the limited eschar of an acid burn. The second mechanism is direct-current injury, a low-voltage electrical burn concentrated at the negative pole, and the third is pressure necrosis from the disc-shaped foreign body pressing on the mucosa. [1] [7]
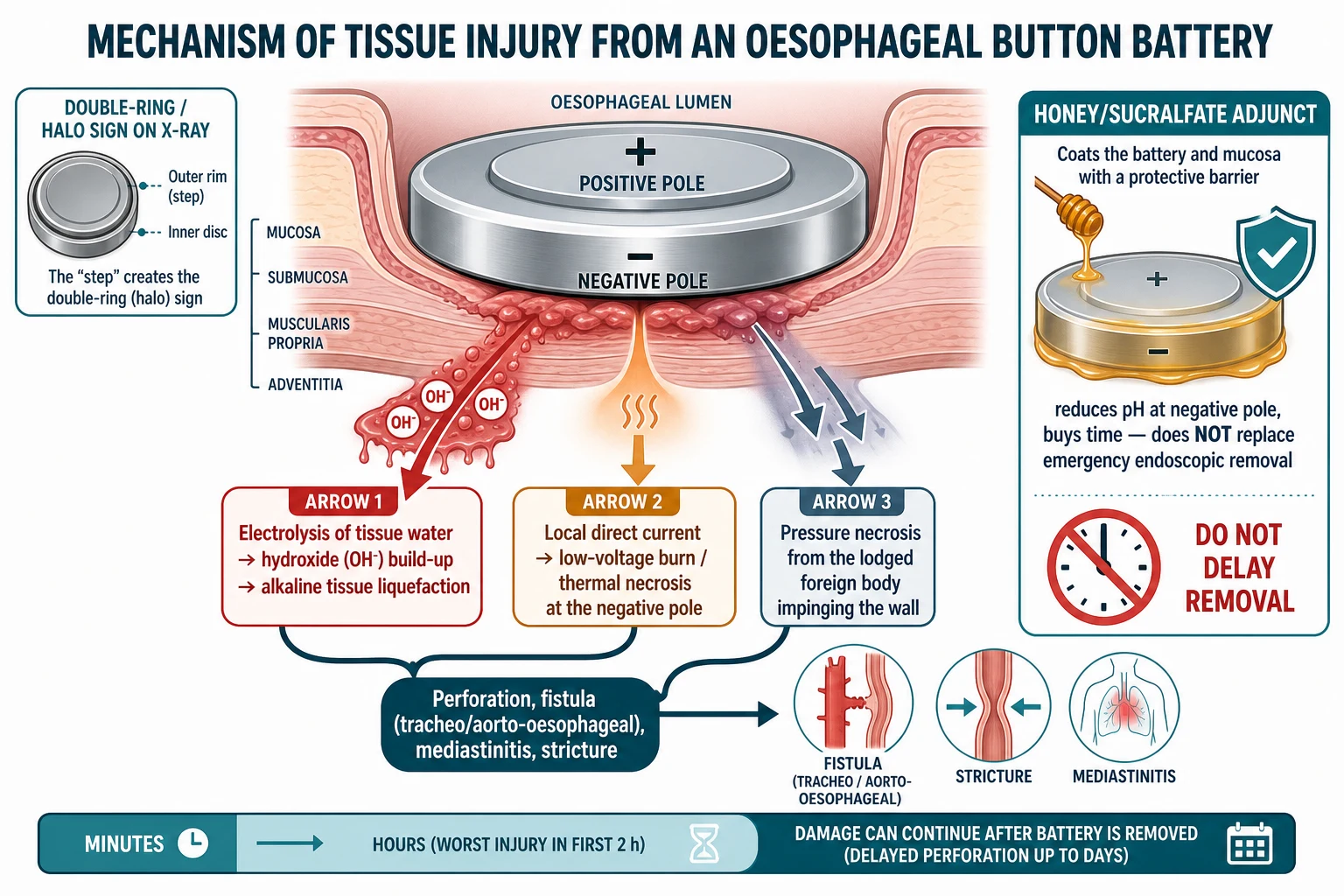
Two features of this mechanism determine clinical behaviour. First, the injury is time-dependent and begins within minutes to hours, which is why a battery in the oesophagus cannot wait. Second, the damage can continue after the battery is removed, because tissue weakened by alkali liquefaction and electrical injury may necrose and perforate days to weeks later. The most feared late complication is an aorto-oesophageal or tracheo-oesophageal fistula, in which the burn erodes into a great vessel or the airway and presents as massive, often fatal haematemesis or haemoptysis days to weeks after an apparently successful removal. [1] [3]
The honey and sucralfate adjuncts work on this same mechanism. Weak acids such as honey, and the protective coating sucralfate, reduce the pH at the negative pole and limit hydroxide generation, buying time while the child awaits endoscopy. The porcine model evidence is consistent and the human case series is growing, but these are adjuncts, not treatments: they reduce injury only if given early and they never replace emergency removal. [6] [7]
Magnets injure through an entirely different mechanism. Two or more magnets, or a magnet and any ferrous object, attract one another across opposing loops of bowel, compressing and trapping the intervening wall. The compressed wall becomes ischaemic, ulcerates, and eventually fistulates, perforates or twists into a volvulus. Because the magnets can sit silently in separate bowel loops for hours to days before attracting through the walls, a well-looking child can harbour a catastrophic injury, which is why the magnet count, not the symptom count, drives the decision. [9] [12]
Clinical Presentation
The presentation spans the spectrum from a completely well child brought in because a parent saw them swallow something, to a child in shock with airway obstruction, haematemesis or peritonitis. The history matters enormously and is often the only clue, because many events are unwitnessed and the symptoms of an oesophageal battery overlap with common, less dangerous conditions. Ask specifically about the object, the number, the time of ingestion, and the symptoms since. [1] [4]
Oesophageal battery
- Drooling, dysphagia, refusing food or drink
- Chest or abdominal pain, vomiting
- Haematemesis or coffee-ground vomit
- Stridor, cough or wheeze from airway compression
- Fever, distress or shock if perforation or mediastinitis
Stomach or distal battery
- Often asymptomatic
- Mild abdominal discomfort
- Reduced appetite or irritability in an infant
- Symptoms only if it lodges distally or causes injury
Multiple magnets
- Initially well, then abdominal pain and vomiting
- Symptoms may lag hours to days as the magnets attract
- Ileus, peritonitis or shock when perforation or volvulus occur
- A well child with a known multiple-magnet ingestion is still high-risk
Late or severe
- Massive haematemesis days to weeks later suggests aorto-oesophageal fistula
- Dysphagia or food refusal after removal suggests stricture
- Recurrent chest infections suggest tracheo-oesophageal fistula
- Hoarseness or vocal-cord palsy from recurrent laryngeal injury
Examination begins with the primary survey. Airway obstruction, stridor, drooling, respiratory distress or shock place the child in the emergency pathway and may demand airway protection before any imaging. The abdomen is examined for tenderness, guarding or peritonism that suggests perforation or obstruction from magnets, and the oropharynx is inspected for burns or a retained battery, though a negative mouth inspection never excludes an oesophageal or gastric battery. [4] [8]
A focused history establishes the time window that determines urgency. The single most important question is when the ingestion happened, because an oesophageal battery is an emergency measured in hours. Ask about the source object, the number of batteries or magnets in the household, any symptoms, and any prior ingestions. In a preverbal child, the parent's account of found packaging, a missing battery, or a child playing with a remote control may be the only thread. [1] [11]
Differential Diagnosis
The differential of a round radio-opacity in a child's oesophagus is short but consequential, because mistaking a battery for a coin, or a magnet for a bead, changes the entire plan. Build the differential around what the object is, what it is doing, and what else could cause the symptoms. [2] [3]
HIDES A COIN
| Object | Radiographic features | Risk profile | Management implication |
|---|---|---|---|
| Button battery | Halo and double-ring on AP view, step-off or notch on lateral view | High if oesophageal; alkaline liquefaction and delayed fistula | Emergency endoscopic removal within two hours if oesophageal |
| Coin | Smooth, uniform density, no halo or step-off | Low; usually passes or is removed electively if oesophageal | Observe or elective removal; not time-critical |
| Single magnet | Round, dense, single density; may look like a bead | Low alone, but a second magnet or ferrous object changes everything | Observe and repeat image; re-examine the count carefully |
| Two or more magnets | Multiple round densities, may be in different bowel loops | High; attract across bowel walls and cause fistula and perforation | Remove if within reach, or observe closely with surgical standby |
| Food bolus or bead | May be radiolucent and invisible on plain film | Variable; usually lower risk | Endoscopy if symptomatic or oesophageal |
A speakable synthesis sounds like this: "This three-year-old has a round radio-opacity in the upper oesophagus with a halo sign and a step-off on the lateral view, so this is a button battery, not a coin. It has been there for at least three hours, so I am treating this as a time-critical emergency. I have secured the airway and access, the child is over twelve months and can swallow, so I am giving honey as a bridge while I mobilise emergency endoscopy within the two-hour target, and I am keeping aorto-oesophageal fistula, perforation and safeguarding open in parallel." [1] [5]
Clinical & Bedside Assessment
Assess and support airway, breathing and circulation before detailed examination. A child with an oesophageal battery may drool, obstruct, or bleed, and a child with peritonitis from magnets may be in shock; these are the presentations that demand immediate stabilisation and senior help. Keep the child nil by mouth until the object is located, because the plan may change to emergency endoscopy within minutes. [4] [8]
[1] [2]Examine the radiograph deliberately for the halo and double-ring signs of a battery, and for the step-off or notch at one edge on the lateral view. When magnets are suspected, count them, because the difference between one and two changes the plan from observe to remove. A lateral view helps confirm whether two densities represent a single battery seen end-on or two separate objects. [3] [12]
The history runs in parallel using a focused frame: the object and number if known, the time of ingestion, the source in the home, the symptoms since, any prior ingestions, and the child's developmental background. Ask the parent to bring the device or packaging, because identifying the battery size and chemistry refines the risk. In adolescents, ask privately about intentional ingestion or self-harm when it is safe to do so, because magnet ingestion in this group may be intentional. [1] [10]
After each assessment, state and document one sentence: what the object is, where it sits, how long it has been there, and what you will do next. This spoken synthesis is what examiners listen for, and it keeps the team coordinated as the tempo rises toward removal. [4] [5]
Investigations
Stabilise first, then order investigations that change the immediate plan. The decisive investigation is the plain radiograph; most other tests are conditional on the object, the location, and the child's stability. A normal examination never overrules a battery on the film, and a sick child is never sent to radiology unescorted. [2] [8]
Immediate
- Single radiograph nasopharynx to anus in AP and lateral views
- Locate the object and distinguish battery from coin
- Count magnets carefully
- Bedside glucose and observations if the child is unwell
Conditional
- Bloods including group and hold if haematemesis or surgery is likely
- Cross-table lateral if the AP view is equivocal
- Repeat radiograph at planned intervals for an observed object
- Electrocardiogram if the child is unstable or there is concern for great-vessel injury
Targeted and post-removal
- Contrast swallow only after removal if a fistula or stricture is suspected
- Endoscopy is both diagnostic and therapeutic for oesophageal batteries
- CT angiography if an aorto-oesophageal fistula is suspected
- Direct visualisation of the burn at endoscopy grades the injury and guides follow-up
Interpret the radiograph as mechanism and risk, not as a static picture. A battery in the oesophagus is an emergency regardless of how well the child looks; a battery in the stomach of an asymptomatic child can usually be observed. Two magnets in different loops are high-risk even if the child is well, because the attraction can begin at any time. A repeat film is part of management, not an afterthought, for any object that is observed rather than removed. [2] [9]
[1] [3]Management — Resuscitation
Suspected battery or magnet ingestion triggers a coordinated response. Declare the concern, call the senior paediatrician, endoscopist, anaesthetist and, where relevant, paediatric surgery and ENT, name a leader, allocate roles, and prepare age- and weight-appropriate equipment and monitoring. Assess and support the airway and circulation, keep the child nil by mouth, and take the localising radiograph while the team assembles. [4] [8]
The first minutes when an oesophageal battery is found
Call the team
Declare the finding, call the senior paediatrician, endoscopist, anaesthetist and surgical or ENT support, name a leader and allocate roles.
Secure A, B and C
Give oxygen, establish access, keep the child nil by mouth, and protect the airway aggressively if there is stridor, drooling or haematemesis.
Confirm location and time
Confirm the oesophageal position on the radiograph and record the time since ingestion to frame the two-hour target.
Give the bridge
In a child older than twelve months who can swallow safely, give honey 10 millilitres every ten minutes up to six doses while awaiting endoscopy.
Remove within two hours
Mobilise emergency endoscopic removal within two hours of presentation, with senior endoscopy, anaesthesia and surgical standby.
Reassess and admit
After removal, admit for serial review of delayed perforation, fistula and stricture, and arrange follow-up endoscopy and nutrition support.
The honey and sucralfate bridge
For a child with a suspected or confirmed oesophageal button battery who is older than twelve months, is able to swallow safely, and has no airway compromise, suspected perforation, sepsis or known allergy, give honey 10 millilitres, roughly two teaspoons, by mouth every ten minutes for up to six doses while awaiting endoscopic removal. Sucralfate is the alternative where honey is unavailable or unsuitable, dosed at 1 gram per 10 kilograms of body weight. These adjuncts reduce the pH at the negative pole and limit hydroxide generation, buying time within the removal window. They are never a substitute for endoscopy, they must not delay removal, and honey is contraindicated in infants under twelve months because of the botulism risk. The human evidence remains limited to case series and extrapolation from animal models, so present the adjunct as a promising bridge informed by a systematic review and porcine data, not as a proven standard. [6] [7]
Multiple magnets
Treat two or more magnets, or a magnet paired with a ferrous object, as a high-risk situation even when the child is well. If the magnets are within endoscopic reach in the stomach or proximal duodenum, remove them; if they are beyond endoscopic reach and the child is asymptomatic, observe closely with surgical standby and repeat imaging, removing them if they fail to progress or if any symptoms develop. Never give laxatives or induced emesis, because moving magnets or raised intraluminal pressure can precipitate obstruction or bring attracting magnets into apposition. [9] [12]
Airway protection
A child with stridor, drooling, haematemesis or a threatened airway from an oesophageal battery needs airway protection by an experienced clinician, using a rapid sequence approach and age-appropriate equipment. Anaesthetic considerations are significant: the battery may have caused oedema or a fistula, the airway may be distorted, and the shared airway between anaesthetist and endoscopist must be planned in advance. Never sedate or paralyse a threatened airway without the people and plan to secure it. [8]
[1] [6]Management — Definitive & Stepwise
After resuscitation and the localising film, move to the definitive plan that matches the object, the location and the count, without stopping reassessment. The oesophageal battery and attracting magnets follow time-critical removal pathways; the distal, asymptomatic single object follows an observation pathway with planned repeat imaging and a clear removal trigger. [2] [5]
From resuscitation to the right ongoing plan
Name the expected result
State the change you expect in airway safety, object location, and tissue injury after each planned action.
Choose the pathway by object and location
Oesophageal battery to emergency endoscopy within two hours; attracting magnets to removal or surgical standby; distal single object to observation.
Agree monitoring and contingency
Specify the location, staff, observation intensity, the response owner, the next sign of failure, and the plan if transfer is delayed.
Arrange retrieval if needed
Call retrieval before local support is exceeded for a child needing endoscopy, surgery or critical care unavailable locally.
Plan follow-up
Arrange repeat endoscopy for stricture, nutrition support, speech and swallow assessment, and prevention and safeguarding review.
Hand over and dispose
Transfer the ingestion time, object and count, removal time, burn grade, unresolved risks, follow-up plan, and the safety net for the family.
An oesophageal battery is removed endoscopically within two hours, ideally by a senior endoscopist with anaesthetic and surgical or ENT standby. The burn is graded at removal, and the child is admitted for serial observation because delayed perforation and fistula can develop over days to weeks. A battery in the stomach of an asymptomatic child can be observed with a repeat radiograph at four days, and removed if it has not passed or if symptoms develop. A standardised institutional protocol that routes the child from presentation to removal without delay reduces time to removal and is now considered best practice. [5] [1]
Call retrieval or transfer when the child needs endoscopy, surgery or critical care that the local service cannot reliably provide. Discuss the likely support, present monitoring and access, equipment and staff limits, transport time and weather, the safest destination, the escort, expected deterioration, and the plan if transfer is delayed. A child with an oesophageal battery in a rural hospital should not wait for transfer to begin the bridge or the airway plan; start locally and retrieve in parallel. [4] [8]
Specific Subtypes & Scenarios
The assessment framework stays the same, but the object, the location and the child change what you look for and how urgently you act. In each scenario, confirm the object, confirm the location, and activate the correct pathway while running safeguarding and prevention in parallel. [1]
Oesophageal button battery
- Two-hour endoscopic removal target regardless of symptoms
- Honey or sucralfate bridge in eligible children over twelve months
- Grade the burn and admit for delayed-complication surveillance
- Watch for aorto-oesophageal and tracheo-oesophageal fistula days to weeks later
Stomach or distal battery
- Asymptomatic children can be observed
- Repeat radiograph at four days, sooner if symptomatic
- Remove if not passed or if any symptoms develop
- Larger batteries are less likely to pass spontaneously
Two or more magnets
- High-risk even when well
- Remove if within endoscopic reach
- Surgical standby and repeat imaging if beyond reach
- No laxatives, no induced emesis
Single magnet
- Treat as a standard foreign body
- Observe and repeat image
- Re-examine the count — a second magnet changes the plan
- Remove if symptomatic or not progressing
Late presentation after battery removal
- Massive haematemesis suggests aorto-oesophageal fistula
- Dysphagia and food refusal suggest stricture
- Recurrent chest infection suggests tracheo-oesophageal fistula
- Hoarseness suggests recurrent laryngeal nerve injury
Rural or remote setting
- Start the bridge and airway plan locally before transfer
- Call retrieval in parallel with resuscitation
- State equipment, staff, weather and distance limits
- Agree a delayed-transfer contingency driven by acuity
Neurodevelopmental disability or pica
- Higher recurrence risk
- Establish the personal baseline and supervision plan
- Engage carers and the disability team in prevention
- Safeguarding review for recurrent ingestion
Adolescent intentional ingestion
- Create private history time when safe
- Ask about self-harm and the intent behind magnet ingestion
- Explain confidentiality and its safety limits
- Activate mental-health and safeguarding pathways
Suspected great-vessel fistula
- Massive haematemesis days to weeks after a battery
- Do not pass a nasogastric tube blindly
- Mobilise endovascular and surgical teams immediately
- CT angiography if the child is stable enough
Complications & Pitfalls
Most harm begins when an oesophageal battery is not recognised as time-critical, when the adjunct is mistaken for treatment, or when the magnet count is not taken seriously. The most preventable error is waiting on an oesophageal battery because the child looks well, because severe injury can begin within two hours of contact and the risk rises steeply thereafter. The second is assuming the honey bridge has solved the problem and delaying endoscopy. [1] [6]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Oesophageal battery observed rather than removed | Alkaline liquefaction and direct-current injury progress by the hour | Remove endoscopically within two hours regardless of symptoms |
| Adjunct given, endoscopy delayed | The bridge only buys time; it does not treat the injury | Treat the two-hour target as fixed whether or not honey is given |
| Honey given to an infant under twelve months | Infant botulism risk | Reserve honey for children over twelve months; use sucralfate otherwise |
| Single neck or chest film only | Battery at cricopharyngeus or magnet in stomach missed | Image nasopharynx to anus in AP and lateral |
| Magnets not counted | Two magnets change the plan from observe to remove | Count magnets and ask how many were in the set |
| Laxatives or induced emesis for magnets | Moving magnets can precipitate obstruction and apposition | No laxatives, no induced emesis for suspected magnets |
| Child sent home after removal without surveillance | Delayed perforation and fistula missed | Admit and observe for delayed complications; arrange follow-up endoscopy |
| Mistaking a battery for a coin | Time-critical injury treated as a low-risk coin | Seek the halo, double-ring and step-off signs on every film |
| Unstable child sent to imaging unescorted | Airway or circulation fails unmonitored | Stabilise and escort with a rescue plan |
| Prevention and safeguarding omitted | Recurrence and supervision gaps unaddressed | Run prevention education and safeguarding review in parallel |
Watch for anchoring on a reassuring symptom or a normal examination. A well child with a battery in the oesophagus is still an emergency, and a well child with two magnets in different loops is still high-risk. After removal, look actively for delayed harm: perforation, mediastinitis, fistula, stricture and recurrent laryngeal nerve palsy. The fact that the battery came out whole does not prove the injury has stopped. [1] [4]
[1] [6] [9]Prognosis & Disposition
Disposition follows the object, the location, the burn grade at removal, and the support the child needs. Consider the time to removal, the severity of the injury, the risk of delayed complications, local resources, transport risk, and the family's ability to carry out the plan and the prevention advice. [1] [5]
Emergency removal and admission
- Oesophageal battery removed within two hours
- Burn grade on removal determines surveillance intensity
- Admit for delayed perforation, fistula and stricture
- Severe burns need PICU, surgery, ENT and nutrition support
Observation pathway
- Distal asymptomatic battery or single magnet
- Repeat imaging at planned intervals
- Remove if not passed or symptomatic
- Clear removal trigger and named owner
Discharge only when defensible
- Object passed or removed without injury
- No unresolved immediate threat
- Prevention and supervision plan agreed with the family
- Specific warning signs, access route, follow-up and pending-result ownership
A safety net states what change to watch for, how urgently to act, and exactly where to get help. It names the warning signs of delayed perforation and fistula — chest pain, fever, haematemesis, dysphagia, abdominal pain — and the route back to care. Check understanding with teach-back, document it, and connect the family to primary care and the prevention pathway. After a severe event, explain what happened and what remains uncertain, invite questions, and consider debriefing for the child, family and team. [1] [3]
Special Populations
Adapt how you assess, communicate and prevent, but never lower the standard for recognising a time-critical battery or attracting magnets. Evidence is sparse for ingestion patterns in disability, pica and many low-resource settings; present these adaptations as safer practice, not as proven improvements in outcome. [3] [11]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Mobile infant and toddler | Treat mouthing-age access to batteries and magnets as the core risk; secure all compartments | Developmental mouthing is normal; the hazard is access, not behaviour |
| Neurodevelopmental disability or pica | Higher recurrence risk; engage carers and the disability team in supervision and prevention | A chronically supervised setting is not automatically safe; review access |
| Complex or technology-dependent child | Hearing-aid and device batteries are common sources; assess device and child together | Device batteries must be secured even in a supervised setting |
| Adolescent intentional ingestion | Create private time; ask about self-harm and intent behind magnet ingestion; explain confidentiality limits | Confidentiality has safety limits; safeguarding duties still apply |
| Indigenous, migrant or remote family | Use cultural safety and a professional interpreter; address access, transport and prevention | Retrieval and safeguarding routes remain jurisdiction-specific |
Prevention is part of acute care, because recurrence is common and the household hazard usually persists. Counsel the family to secure battery compartments with tape and screwdrivers, to keep spare batteries and magnets out of reach, to buy child-resistant packaging, and to share the message with carers and family. Safeguarding runs in parallel when ingestion is recurrent, when supervision is inadequate, or when the history is inconsistent; immediate stabilisation and safety come first, followed by objective documentation and the local pathway. [3] [11]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The two-hour removal target for oesophageal button batteries, the alkaline-liquefaction mechanism, and the high-risk status of multiple magnets are consensus across the major guidelines. The NASPGHAN Endoscopy Committee clinical report and the ESPGHAN position paper frame the management of ingested foreign bodies and button batteries, and institutional protocols that reduce time to removal are associated with better outcomes. What differs across sources is the detail of the honey and sucralfate adjuncts, the repeat-imaging interval for observed batteries, and the operative thresholds for magnets beyond endoscopic reach, which are source- and setting-specific. [1] [2]
Honey and sucralfate as injury-reducing adjuncts
Frontiers in Pediatrics and Annals of Emergency Medicine
Systematic review of human reports and experimental porcine oesophageal models testing topical honey and sucralfate against saline control after battery placement
Key finding
Topical honey and sucralfate reduced pH-driven injury at the negative pole when given early in animal models; human evidence remains limited to case series and extrapolation, and the adjuncts never replaced endoscopic removal.
Practice change
Give honey or sucralfate as a bridge in eligible children over twelve months while mobilising emergency removal within two hours; do not delay endoscopy for the adjunct.
High-powered magnet injuries follow the marketplace: exposures fell when sales were restricted and rose again when restrictions eased, which is why regulation is treated as a public-health intervention alongside clinical care. Delayed complications after battery removal — aorto-oesophageal fistula, stricture, tracheo-oesophageal fistula — remain the leading causes of death, and their recognition days to weeks after an apparently successful removal is a core teaching point. [11] [3]
There is no universal repeat-imaging interval, adjunct dose, or magnet-removal threshold that fits every child and every setting. Attach each rule to its population, purpose, conditions and jurisdiction, and quote the local source rather than inventing precision. [1] [9]
Jurisdictional implementation
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne button-battery-ingestion guideline supports local implementation of the two-hour removal target, the honey or sucralfate bridge, and magnet management. Retrieval systems, mandatory reporting and product-safety regulation follow the ACCC and state or territory frameworks; high-powered magnet sales have been the subject of Australian product-safety interventions.
Global and low-resource settings: the WHO poison-prevention framework and national poisons centres adapt management to local resources. In settings without on-site endoscopy, start the bridge and airway plan locally and retrieve to a centre that can remove the battery within the window; population-specific thresholds and slower resource escalation must stay attached to that context.
Exam Pearls
[1] [2] [9]Viva: the drooling three-year-old
Do not wait for the child to look unwell. Confirm the ingestion and time, secure the airway and access, take one radiograph nasopharynx to anus, and if there is a halo sign in the oesophagus arrange emergency endoscopic removal within two hours. Give honey as a bridge in the eligible child while you mobilise the team, and keep aorto-oesophageal fistula, perforation and safeguarding open in parallel.
Viva: the well child with two magnets
A well child with two or more magnets is still high-risk, because the magnets can attract across bowel walls at any time and cause fistula, perforation and volvulus. Remove if within endoscopic reach; if beyond reach, observe closely with surgical standby and repeat imaging, and remove if they fail to progress or if any symptoms develop. Do not give laxatives or induced emesis.
Structured oral: late haematemesis after a battery removal
Massive haematemesis days to weeks after a battery removal is an aorto-oesophageal fistula until proven otherwise and is often fatal. Mobilise endovascular and surgical teams immediately, do not pass a nasogastric tube blindly, and arrange CT angiography if the child is stable enough. The lesson is that delayed complications after removal are the leading cause of death, and surveillance must continue for weeks.
References
- [1]Mubarak, Marwan Diagnosis, Management, and Prevention of Button Battery Ingestion in Childhood: A European Society for Paediatric Gastroenterology Hepatology and Nutrition Position Paper Journal of pediatric gastroenterology and nutrition, 2021.PMID 33555169
- [2]Kramer, Robert E Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee Journal of pediatric gastroenterology and nutrition, 2015.PMID 25611037
- [3]Eliason, Melisa J Button battery ingestion in children Current opinion in otolaryngology and head and neck surgery, 2017.PMID 28858893
- [4]Funk, Erin M Button Battery Ingestion in Children: An Educational Review for Perioperative Nursing Journal of perianesthesia nursing, 2025.PMID 38878031
- [5]Goh, Samuel Pediatric Esophageal Button Battery Protocol Reduces Time From Presentation to Removal The Laryngoscope, 2024.PMID 38934450
- [6]Schmidt, Yannick M The use of honey in button battery ingestions: a systematic review Frontiers in pediatrics, 2023.PMID 37842023
- [7]Chiew, Andis Graeme Home Therapies to Neutralize Button Battery Injury in a Porcine Esophageal Model Annals of emergency medicine, 2024.PMID 37725021
- [8]Eck, James B Anesthetic Implications of Button Battery Ingestion in Children Anesthesiology, 2020.PMID 32011339
- [9]Altokhais, Turki Magnet Ingestion in Children Management Guidelines and Prevention Frontiers in pediatrics, 2021.PMID 34422734
- [10]Seguier-Lipszyc, Elhanan Multiple magnet ingestion in children: A problem on the rise Journal of paediatrics and child health, 2022.PMID 35841278
- [11]Middelberg, Leah K Warning Labels and High-Powered Magnet Exposures Pediatrics, 2022.PMID 36189482
- [12]Han, Younghoon Ingestion of multiple magnets in children Journal of pediatric surgery, 2020.PMID 31937446