Paeds · acute-care-resuscitation-and-toxicology
Cardiotoxic and psychotropic medication poisoning
Also known as Paediatric tricyclic antidepressant poisoning · Beta-blocker overdose in children · Calcium channel blocker poisoning in children · Antipsychotic overdose and QT prolongation · High-dose insulin euglycaemic therapy in paediatric overdose
A fellowship approach to the child or adolescent with cardiotoxic and psychotropic medication poisoning: read the ECG and the toxidrome first, lead an ABCDE primary survey with continuous ECG monitoring and bedside glucose, give hypertonic sodium bicarbonate for tricyclic antidepressant cardiotoxicity with a widened QRS, start high-dose insulin euglycaemic therapy for severe beta-blocker and calcium channel blocker overdose, distinguish calcium channel blocker hyperglycaemia from beta-blocker presentation, manage antipsychotic QT prolongation, torsades and neuroleptic malignant syndrome, reserve intravenous lipid emulsion and extracorporeal support for refractory cases, and call the Poisons Information Centre and a toxicologist early.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Cardiotoxic and psychotropic medication poisoning is the harmful effect of a prescribed drug on the heart's electrical system or its pumping, recognised first by the ECG and the bedside pattern and treated by supportive care plus a small number of targeted antidotes. The child or adolescent arrives bradycardic or hypotensive, with a widened QRS or a long QT, and your job in the first minute is to protect the airway, attach a continuous ECG, check a bedside glucose, and read the strip — because the QRS width and the QT length decide the antidote. [1] [9]
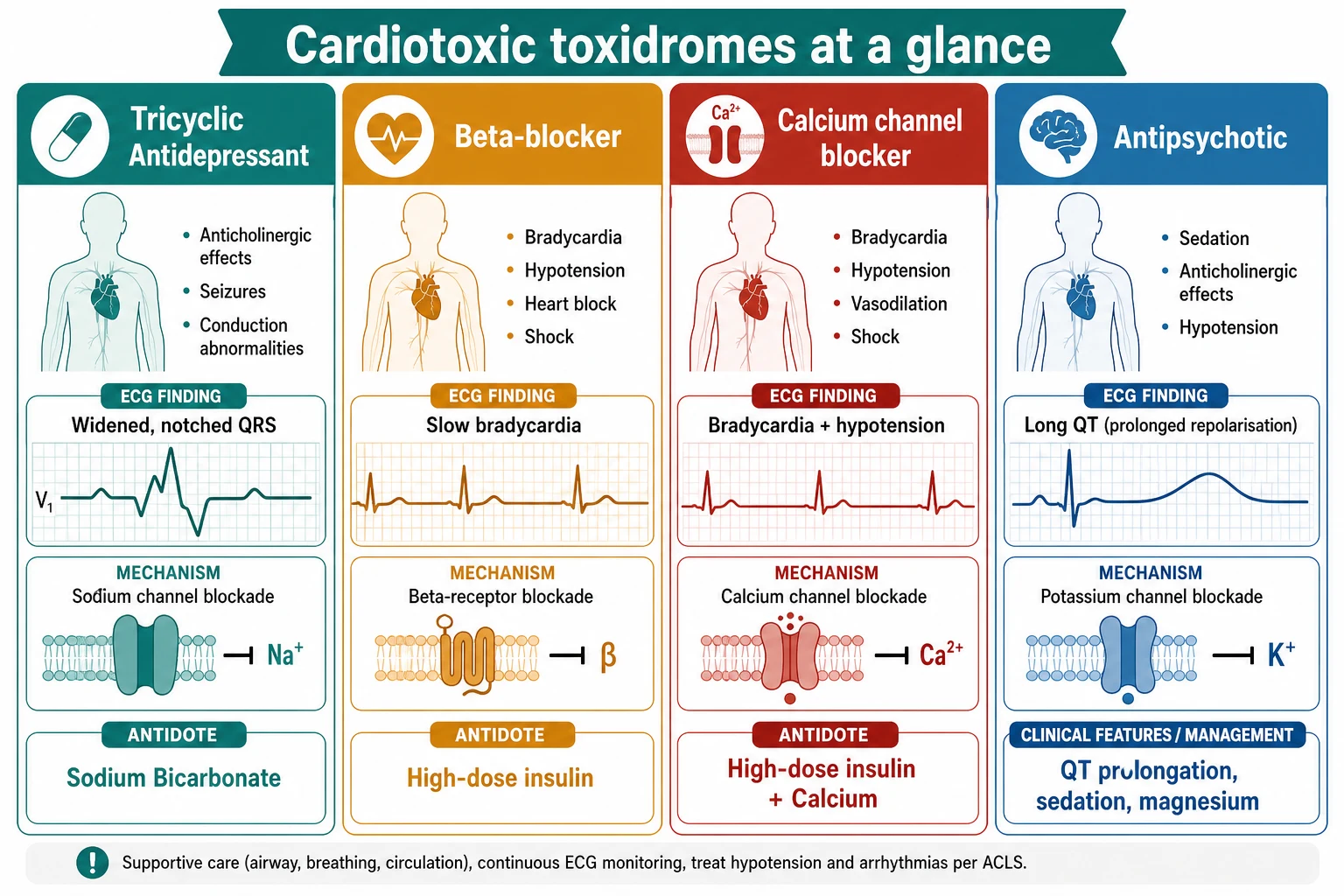
A toxidrome is a recognisable cluster of signs produced by a class of drug acting through a shared mechanism, and the cardiotoxic toxidromes are read from the heart. The tricyclic antidepressant pattern combines a widened QRS with an anticholinergic picture and hypotension. The beta-blocker and calcium channel blocker patterns combine bradycardia and hypotension with poor perfusion. The antipsychotic pattern combines sedation and QT prolongation. Recognising the pattern is faster and more useful than waiting for a drug level, and it points directly to the immediate treatment. [1] [4]
Management is built around supportive care, because most cardiotoxic drugs are metabolised once the airway, the breathing, the circulation and the perfusion are held safe. Sodium bicarbonate is the specific antidote for sodium-channel-blockade cardiotoxicity and is given to a defined trigger and a defined endpoint. High-dose insulin euglycaemic therapy is the key therapy for severe beta-blocker and calcium channel blocker overdose, shifting the failing myocardium onto a more efficient fuel. Intravenous lipid emulsion and extracorporeal support are rescue options for the child who does not respond to standard care. [2] [3]
Classification
The single most useful classification is by the ECG and the ion channel the drug blocks, because it converts a guessing game about the bottle into a decision about the next action. Look at the QRS width and the QT length, add the rate and the blood pressure, and the cardiotoxic class emerges within a minute. [1] [4]
Tricyclic antidepressant
Sodium-channel blockade
- Widened, notched QRS with a tall R wave in aVR
- Anticholinergic picture: dry, flushed, dilated pupils, reduced bowel sounds
- Hypotension from alpha-1 blockade plus negative inotropy; seizures
- Antidote: intravenous sodium bicarbonate 1 to 2 mL per kg of 8.4 per cent, repeated to narrow QRS
Beta-blocker
Beta-receptor blockade
- Bradycardia, hypotension, AV block and poor perfusion
- Propranolol adds sodium-channel blockade: seizures and a widened QRS
- Glucose usually normal; bronchospasm in the asthmatic child
- Key therapy: high-dose insulin euglycaemic therapy; calcium and atropine as adjuncts
Calcium channel blocker
L-type calcium-channel blockade
- Bradycardia with hypotension and vasodilation (dihydropyridines) or myocardial depression (verapamil, diltiazem)
- Hyperglycaemia from blocked insulin release: a discriminator from beta-blockers
- Sustained-release forms deteriorate late; constipation and drowsiness
- Key therapy: intravenous calcium plus high-dose insulin euglycaemic therapy, then vasopressors
Antipsychotic
Potassium-channel (hERG) blockade
- QT prolongation with torsades risk; sedation and anticholinergic effects
- Hypotension from alpha-1 blockade; extrapyramidal signs
- Neuroleptic malignant syndrome: hyperthermia, rigidity, altered consciousness
- Management: intravenous magnesium, correct potassium and magnesium, avoid other QT drugs
Classification by intention and age frames the two peaks of paediatric cardiotoxic poisoning. The toddler peak is exploratory ingestion of a grandparent's verapamil or nifedipine — a single sustained-release tablet can be lethal in a small body. The adolescent peak is deliberate overdose of a tricyclic antidepressant, quetiapine or a beta-blocker, often with ethanol and uncertainty about the dose. Both need the same ABCDE structure and the same ECG-led approach, but the doses, the observation window and the safeguarding assessment differ. [8] [9]
Epidemiology & Risk Factors
Cardiotoxic prescription medications are among the most dangerous paediatric ingestions because a single adult dose can kill a child. Calcium channel blockers and tricyclic antidepressants consistently lead mortality series of paediatric poisoning, and the risk is magnified by the small body mass of the toddler and by sustained-release formulations that absorb slowly and then poison late. [1] [9]
Young child factors
- Exploratory ingestion of a grandparent's or caregiver's medication
- Verapamil, diltiazem, nifedipine, tricyclic antidepressants within reach
- Small body mass magnifies the dose per kilogram
- Sustained-release tablets poison late and outlast the first assessment
Adolescent factors
- Deliberate self-harm overdose of tricyclics, quetiapine, beta-blockers
- Frequent co-ingestion of ethanol and other drugs
- Uncertainty about the dose and the timing
- Access to multiple prescriptions in the home
System factors
- Rural or remote location with retrieval delay
- Limited access to the medication history and the bottle
- After-hours or single-handed cover
- Delayed availability of intensive care and extracorporeal support
Risk is magnified by formulation and co-ingestion. A sustained-release verapamil preparation is the classic late-deteriorator: the child looks well for several hours and then descends into refractory shock, which is why the observation window must be long. Co-ingestion of ethanol deepens the sedation and drops the blood pressure; co-ingestion of two cardiotoxins blurs the ECG and demands combined antidotes. Underlying cardiac disease, long-QT medication and electrolyte disturbance all lower the threshold for arrhythmia. [4] [8]
Pathophysiology
Toxicity follows from the ion channel or receptor the drug blocks, and four mechanisms dominate the cardiotoxic picture. Each maps onto a toxidrome and its signature ECG threat, and each points to a different antidote. [1] [4]
Tricyclic antidepressants bind the fast cardiac sodium channel and slow the phase 0 upstroke of the ventricular action potential. Slowed depolarisation slows conduction through the His-Purkinje system and the myocardium, which widens the QRS, and the slow conduction is what allows re-entry and ventricular arrhythmia. A tall R wave in lead aVR reflects the rightward conduction shift. TCAs also block alpha-1 receptors (causing hypotension), muscarinic receptors (the anticholinergic picture) and potassium channels (adding QT prolongation), and they antagonise GABA, which is why seizures complicate severe poisoning. [2] [9]
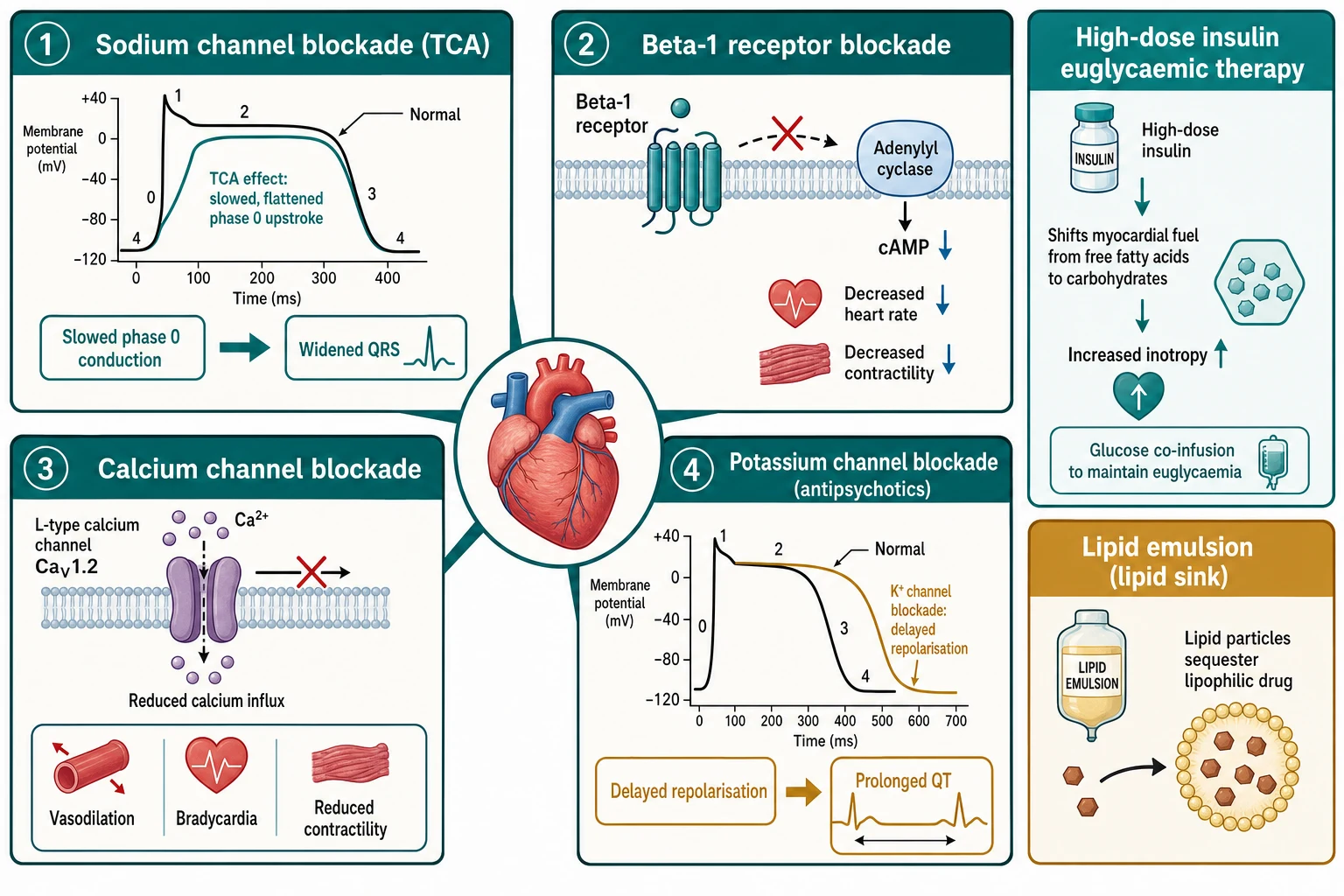
Beta-blockers occupy the beta-1 adrenergic receptor, reducing the Gs-to-adenylyl-cyclase-to-cAMP cascade that normally drives heart rate, contractility and AV conduction. The result is bradycardia, AV block and negative inotropy. Some beta-blockers add direct sodium-channel blockade (the membrane-stabilising effect), most notably propranolol, which is why propranolol overdose can widen the QRS and cause seizures on top of the bradycardia. Calcium channel blockers block the L-type calcium channel in cardiac myocytes, in the SA and AV nodes, and in vascular smooth muscle. The non-dihydropyridines verapamil and diltiazem cause profound bradycardia, AV block and myocardial depression, while the dihydropyridines (such as nifedipine and amlodipine) cause predominant vasodilation. Calcium channel blockade also blocks insulin release from the pancreatic beta cell, which is why calcium channel blocker overdose produces hyperglycaemia while beta-blocker overdose does not. [4] [5]
Antipsychotics block the delayed-rectifier potassium channel (the hERG channel) and lengthen the action potential, which prolongs the QT interval and sets up early after-depolarisations and torsades de pointes. They also block alpha-1 receptors (hypotension), histamine and muscarinic receptors (sedation and anticholinergic effects) and dopamine receptors (extrapyramidal effects). The neuroleptic malignant syndrome is a separate, idiosyncratic consequence of central dopamine blockade, producing hyperthermia, lead-pipe rigidity, altered consciousness and autonomic instability with a rising creatine kinase. [7] [8]
Two adjunct mechanisms deserve a place in the fellowship answer. High-dose insulin euglycaemic therapy works by shifting the failing, toxin-depressed myocardium onto carbohydrate metabolism, restoring inotropy while glucose is co-administered to keep the patient euglycaemic; it also corrects the toxin-induced insulin resistance seen in calcium channel blocker overdose. Intravenous lipid emulsion creates an intravascular lipid phase (the lipid sink) that sequesters lipophilic drug and lowers its free concentration at the tissues, a mechanism now applied to several lipophilic cardiotoxins beyond its original local-anaesthetic role. [3] [6]
Clinical Presentation
Begin with the first impression, a continuous ECG and a hands-on primary survey, then convert what you see into a cardiotoxic class rather than a drug name. State what you see objectively: "This adolescent is drowsy and hypotensive with a QRS of 140 milliseconds and dry flushed skin — that is tricyclic antidepressant toxicity with sodium-channel blockade." [1]
The tricyclic antidepressant picture combines an anticholinergic toxidrome (dry, flushed skin, dilated pupils, urinary retention, reduced bowel sounds) with the cardiac signature: a widened, notched QRS, a tall R wave in aVR, hypotension and tachycardia that can degenerate into bradycardia and ventricular arrhythmia. Severe poisoning adds seizures, respiratory depression and a rapid descent into shock. The beta-blocker picture is bradycardia with hypotension and AV block, with propranolol adding seizures and a widened QRS. The calcium channel blocker picture is bradycardia with hypotension and vasodilation (dihydropyridines) or profound myocardial depression (verapamil, diltiazem), and the bedside glucose is often high. [2] [4]
[1] [2]The antipsychotic picture combines sedation with QT prolongation, anticholinergic effects, extrapyramidal signs and postural hypotension; torsades de pointes is the feared arrhythmia, and the neuroleptic malignant syndrome presents hours to days after exposure with hyperthermia, rigidity, confusion and autonomic instability. A mixed or sustained-release ingestion is the trap: the child can look well for hours and then deteriorate, which is why the observation window must be long and the reassessment frequent. [7] [8]
Differential Diagnosis
A toxic cause is one explanation for a bradycardic, hypotensive or widened-QRS child, and the resuscitation does not wait for certainty. Build the differential in a fixed order: what can kill now, what is most likely, what is reversible, and what is most harmful to miss. [1]
Cardiac and metabolic
- Hyperkalaemia producing a wide-QRS bradycardia: treat first with calcium
- Hypothermia with bradycardia and a slow, wide complex
- Myocarditis or cardiomyopathy with a low-output state
- Structural heart disease or a primary arrhythmia such as congenital long QT
Toxic mimics
- Local anaesthetic systemic toxicity from bupivacaine: widened QRS and arrest
- Digoxin toxicity with bradycardia and AV block
- Other sodium-channel blockers (class I antiarrhythmics, cocaine)
- Co-ingested ethanol, opioid or sedative deepening the depression
Systemic and situational
- Sepsis with myocardial depression and poor perfusion
- Hypoglycaemia contributing to a reduced conscious level
- Addisonian crisis with bradycardia and hypotension
- Raised intracranial pressure with bradycardia and hypertension
The decisive point is that hyperkalaemia, hypoglycaemia and a primary cardiac cause are missed only if you do not look for them. Check a bedside glucose and a venous gas in every suspected cardiotoxic ingestion, because a low glucose is corrected in seconds and a high potassium is corrected with calcium. The hyperglycaemia of a calcium channel blocker overdose is a useful discriminator: a bradycardic, hypotensive child with a high glucose points to a calcium channel blocker rather than a beta-blocker. The response to a targeted antidote also confirms the diagnosis — a QRS that narrows after sodium bicarbonate is tricyclic cardiotoxicity. [4] [9]
Clinical & Bedside Assessment
Run the ABCDE primary survey adapted to the cardiotoxic-poisoned child, then reassess after each intervention. The continuous ECG and the circulation are the foreground, because cardiotoxic drugs kill through arrhythmia and shock. [1] [4]
Open and protect the airway, give high-flow oxygen, and ventilate with a bag and mask if breathing is inadequate or the conscious level is depressed. Attach a continuous cardiac monitor and obtain a 12-lead ECG at the bedside, measuring the QRS width and the corrected QT. Check the bedside glucose immediately, because calcium channel blocker overdose raises it and beta-blocker overdose can occasionally drop it. Establish intravenous or intraosseous access. Assess the circulation for heart rate, blood pressure, capillary refill, skin temperature and perfusion, and measure the temperature. [1] [2]
[1] [2]The focused examination targets the cardiotoxic class. Look at the pupils (dilated and dry in anticholinergic or antipsychotic toxicity), the skin (flushed and dry in anticholinergic, poorly perfused in shock), the muscle tone (lead-pipe rigidity in neuroleptic malignant syndrome), the glucose (high in calcium channel blocker overdose) and the perfusion. Take a collateral history from caregivers or the ambulance crew: what bottles or blister packs were found, how many are missing, the timing, whether the formulation is sustained-release, and any access to multiple prescriptions. Preserve the bottles. [4] [9]
The reassessment after each intervention is the examination that matters most. After sodium bicarbonate, ask whether the QRS has narrowed and the blood pressure improved. After high-dose insulin, ask whether the heart rate, the perfusion and the lactate are improving, while watching the glucose and potassium. State the change you expected, and compare it with what actually happened. [2] [3]
Investigations
Stabilise first, then order each test for a named question. In suspected cardiotoxic poisoning the immediate tests identify the reversible threats and the co-ingestants that change management, rather than naming the drug. [1]
Immediate and bedside
- Continuous ECG with serial QRS width and corrected QT
- Bedside glucose in every case (high in CCB, occasionally low in BB)
- Venous gas for pH, lactate and acid-base
- Electrolytes including potassium and magnesium
Core laboratory
- Paracetamol and salicylate levels in every intentional or unknown ingestion
- Renal function, hepatic panel and creatine kinase
- Beta-human chorionic gonadotropin in adolescent females
- Troponin if myocardial injury is suspected
Targeted and supportive
- Quantitative drug levels only when they change management
- Chest imaging if aspiration or pulmonary oedema is suspected
- Cultures if sepsis remains on the differential
- Serial ECGs through the observation window for sustained-release poisonings
Interpret the tests as physiology and threat, not as a drug label. A low glucose is acted on in seconds; a high glucose in a bradycardic child points to a calcium channel blocker. A metabolic acidosis with a rising lactate signals worsening shock and the need to escalate. A low potassium or magnesium during high-dose insulin therapy must be corrected because hypokalaemia and hypomagnesaemia prolong the QT and invite torsades. The serial ECG is more useful than a single tracing, because the QRS and QT trends track both deterioration and response. [3] [7]
[1] [9]Management — Resuscitation
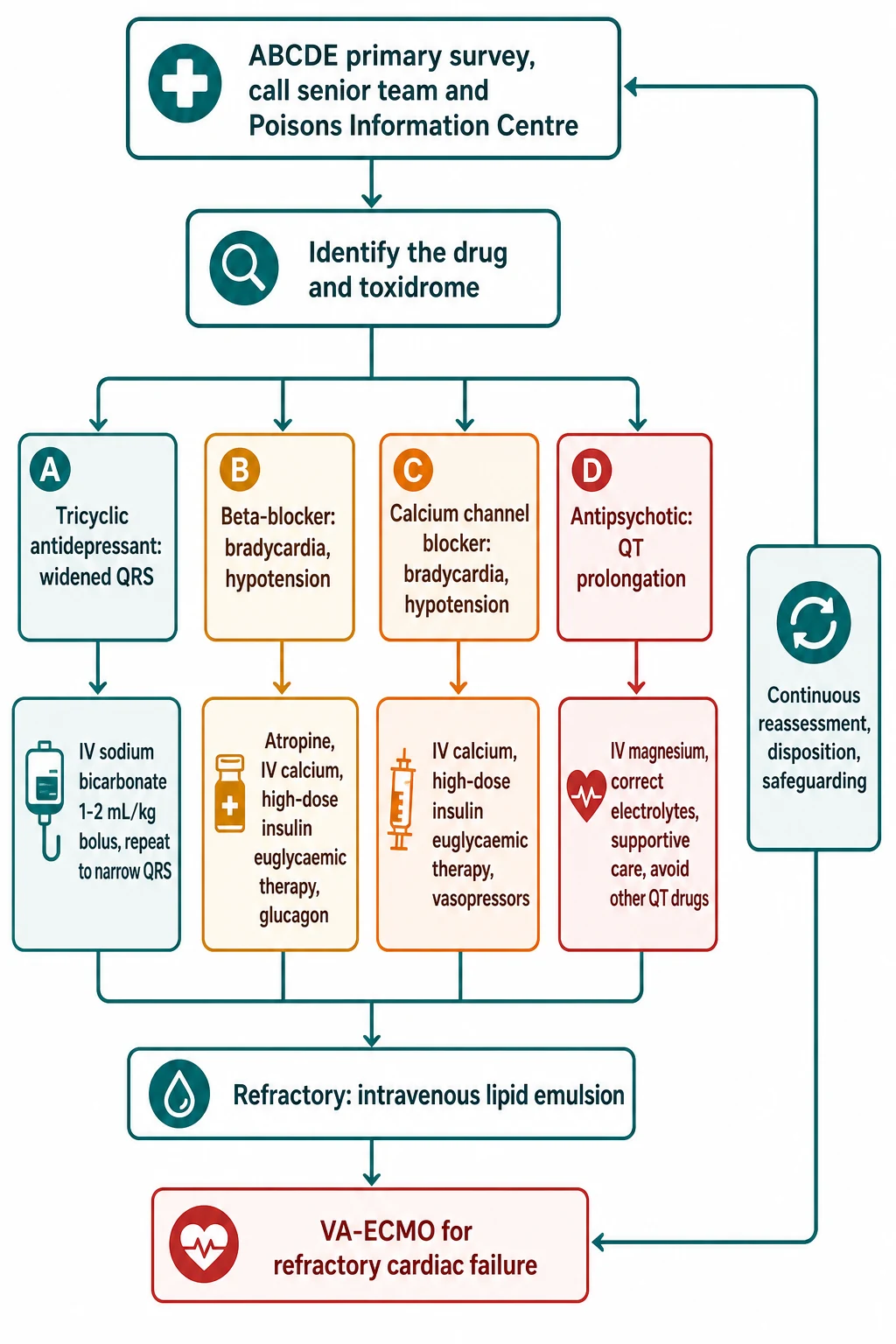
Resuscitation follows a fixed order: ABCDE primary survey, high-flow oxygen, bag-mask ventilation for apnoea or a depressed airway, bedside glucose, intravenous access, continuous ECG, a call for senior, intensive-care and Poisons Information Centre help, and the targeted antidote. Each element runs in parallel, and each action is followed by reassessment of the strip and the circulation. [1] [2]
The first minutes in cardiotoxic poisoning
Primary survey and call for help
Run the ABCDE survey; declare the concern; call the senior paediatric, resuscitation and intensive-care teams and the Poisons Information Centre; name a leader and allocate roles; bring age- and weight-appropriate equipment and monitoring.
Protect the airway and attach the ECG
Open and protect the airway; give high-flow oxygen; ventilate with bag and mask if breathing is inadequate; attach a continuous monitor and obtain a 12-lead ECG; measure the QRS width and the corrected QT.
Check bedside glucose and establish access
Check glucose at the bedside (high in calcium channel blocker, occasionally low in beta-blocker); gain intravenous or intraosseous access; send the core bloods including paracetamol and salicylate levels in the intentional ingestion.
Read the strip and identify the class
From the QRS width, the QT length, the rate and the blood pressure, name the tricyclic, the beta-blocker or calcium channel blocker, the antipsychotic or the unknown pattern, and direct the targeted antidote.
Give the targeted antidote
Sodium bicarbonate for the tricyclic widened QRS; calcium and high-dose insulin for the beta-blocker and calcium channel blocker; magnesium and electrolyte correction for the antipsychotic QT; supportive care for all.
Reassess from the top
After every action return to the airway, breathing, circulation, ECG, glucose and conscious level; judge the trend against the response you predicted; escalate to lipid emulsion and extracorporeal support for refractory cases.
Tricyclic antidepressant cardiotoxicity and sodium bicarbonate
The widened QRS of a tricyclic antidepressant is sodium-channel blockade, and the antidote is hypertonic sodium bicarbonate. Sodium bicarbonate works by three mechanisms: the sodium load overcomes the channel blockade and speeds conduction, the alkalinisation raises the pH and reduces the free fraction of the drug, and the extracellular sodium narrows the QRS. The trigger is a widened QRS (over 100 milliseconds), a ventricular arrhythmia or hypotension, and the endpoint is a narrowed QRS and a serum pH of 7.45 to 7.55. [2] [9]
Sodium bicarbonate 8.4 per cent — tricyclic cardiotoxicity
The common pitfalls with bicarbonate are well described: giving it without a clear trigger or endpoint, failing to repeat the bolus to narrow the QRS, and forgetting that hyperventilation adds an alkalinising effect in the intubated child. A ventricular arrhythmia in tricyclic poisoning is treated with sodium bicarbonate first, not with a class Ia or Ic antiarrhythmic — quinidine, procainamide and flecainide each worsen sodium-channel blockade, and amiodarone is avoided for the same reason. If the arrhythmia persists, expert consensus supports intravenous lipid emulsion, and refractory cardiac arrest is an indication for prolonged cardiopulmonary resuscitation and extracorporeal support. [2] [6]
Beta-blocker and calcium channel blocker overdose
Severe beta-blocker and calcium channel blocker overdose cause bradycardia, hypotension and myocardial depression that is poorly responsive to atropine and escalating inotropes alone. The modern approach layers intravenous calcium, high-dose insulin euglycaemic therapy, vasopressors and, for refractory cases, lipid emulsion and extracorporeal support. [3] [4]
Intravenous calcium provides a bolus of extracellular calcium that overcomes the channel blockade and transiently improves contractility and blood pressure. Calcium gluconate 10 per cent (0.6 mL per kg, 60 mg per kg) or calcium chloride 10 per cent (0.2 mL per kg, 20 mg per kg) is given intravenously and can be repeated, with attention to the IV access — calcium chloride needs a central line or a large, reliable cannula because it is irritant in extravasation. [4]
High-dose insulin euglycaemic therapy (HIET)
High-dose insulin euglycaemic therapy is the key therapy for severe overdose of either class. It shifts the failing myocardium onto carbohydrate metabolism and restores inotropy, and it corrects the toxin-induced insulin resistance of calcium channel blocker overdose. The dose is an insulin bolus of 1 unit per kilogram followed by an infusion of 0.5 to 1 unit per kilogram per hour, with a dextrose infusion to keep the patient euglycaemic; the response builds over 15 to 45 minutes, and the glucose and potassium must be checked hourly because insulin drives both down. Atropine, glucagon, vasopressors and cardiac pacing are adjuncts rather than replacements for insulin. A systematic review of propranolol toxicity confirms that high-dose insulin and lipid emulsion are the interventions most consistently associated with improvement. [3] [5]
Treatments for propranolol toxicity (systematic review)
European Journal of Clinical Pharmacology
Systematic review of current approaches and evidence for the treatment of propranolol toxicity
Key finding
High-dose insulin euglycaemic therapy and intravenous lipid emulsion were the interventions most consistently associated with haemodynamic improvement in severe propranolol toxicity, alongside standard supportive care and vasopressors.
Practice change
Reach for high-dose insulin euglycaemic therapy early in severe beta-blocker (especially propranolol) overdose rather than escalating inotropes alone, and prepare lipid emulsion for refractory cases.
Antipsychotic poisoning and the QT
Antipsychotic overdose prolongs the QT and risks torsades de pointes. The management is electrolyte correction first (potassium above 4 mmol per L and magnesium above 0.8 mmol per L, because hypokalaemia and hypomagnesaemia lengthen the QT), intravenous magnesium for QT prolongation or torsades, and the strict avoidance of every other QT-prolonging drug, including many antiemetics, antibiotics and methadone. [7] [8]
Magnesium sulfate — QT prolongation or torsades
Torsades de pointes that is sustained or recurrent is treated with intravenous magnesium, the correction of potassium and magnesium, and electrical cardioversion or overdrive pacing if the child is unstable. The neuroleptic malignant syndrome is managed supportively — cessation of the antipsychotic, active cooling, benzodiazepines, and correction of the fluid, electrolyte and renal consequences of the rhabdomyolysis — with dantrolene and bromocriptine considered in specialist consultation for severe cases. Sedation, hypotension and the anticholinergic effects are managed supportively, with the airway protected if the conscious level is depressed. [7] [8]
Refractory poisoning: lipid emulsion and extracorporeal support
When a lipophilic cardiotoxic drug (a tricyclic antidepressant, a beta-blocker or a calcium channel blocker) does not respond to the targeted antidote, intravenous lipid emulsion is the next rescue therapy. The mechanism is the lipid sink: the lipid phase sequesters the lipophilic drug and lowers its free concentration at the heart and brain. A 2025 narrative review confirms its place as an adjunct for selected severe lipophilic drug toxicity, guided by a toxicologist. [6]
Refractory cardiotoxic shock or cardiac arrest unresponsive to bicarbonate, calcium, insulin, vasopressors and lipid emulsion is an indication for veno-arterial extracorporeal membrane oxygenation, which bridges the child while the drug is metabolised. Early activation of an extracorporeal service is essential, because the window for cannulation is narrow and the retrieval time is long. [10]
Management — Definitive & Stepwise
Once the first minutes are safe, definitive care moves to continuous haemodynamic and ECG monitoring, sustained antidote therapy, electrolyte and glucose control, and the clarification of the agent and the formulation. This phase runs hour by hour with the trend, and the disposition follows the response. [1] [4]
Ongoing monitoring and sustained antidote therapy
Continue continuous ECG, blood pressure and perfusion monitoring, with serial QRS and corrected QT measurement. For tricyclic poisoning, repeat sodium bicarbonate to keep the QRS narrow and the pH in the target range, then watch for recurrence as the bicarbonate is metabolised. For beta-blocker and calcium channel blocker overdose, titrate the high-dose insulin infusion to the perfusion and the lactate, and replace potassium and glucose as needed. For antipsychotic overdose, keep the potassium and magnesium corrected and the QT monitored until it normalises. [2] [3]
Electrolyte, glucose and perfusion control
Correct the metabolic consequences actively. Replace potassium during high-dose insulin therapy to keep it above 4 mmol per L, and give dextrose to maintain euglycaemia. Treat the hyperglycaemia of calcium channel blocker overdose with the insulin infusion rather than separate hypoglycaemics, because the insulin serves both the glucose and the inotropy. Drive the perfusion with fluids, vasopressors and the antidotes, watching the lactate fall and the capillary refill improve as the endpoints. [3] [4]
Goals and disposition
Set explicit recovery endpoints and watch the trend toward them: a safe airway, a narrowed QRS, a normalising QT, an adequate blood pressure and perfusion, a falling lactate, and a stable glucose and electrolyte profile. A child who has received sodium bicarbonate for tricyclic cardiotoxicity is observed until the ECG has normalised and stayed normal, because the QRS can re-widen. A child with a sustained-release calcium channel blocker ingestion is observed for at least 12 to 24 hours because of the risk of late deterioration. Asymptomatic children with immediate-release ingestions are observed for the relevant window before discharge with safety-netting. [1] [4]
Specific Subtypes & Scenarios
The structure stays the same, but age, agent, formulation and setting change what you watch for, which antidote you reach for, and how early you escalate. [1]
Toddler verapamil or nifedipine
- Grandparent's sustained-release tablet; a single dose can be lethal
- Bradycardia with hypotension and hyperglycaemia
- Calcium plus high-dose insulin euglycaemic therapy early
- Observe 12 to 24 hours for sustained-release delayed toxicity; poison-prevention counselling
Adolescent tricyclic overdose
- Widened QRS with anticholinergic picture and hypotension
- Sodium bicarbonate 1 to 2 mL per kg of 8.4 per cent to narrow QRS
- No flumazenil if a tricyclic is suspected: it can precipitate seizures
- Check paracetamol and salicylate levels; arrange mental-health assessment
Sustained-release CCB
- Late and outlasting the initial resuscitation
- Start calcium and high-dose insulin euglycaemic therapy early
- Prepare lipid emulsion and VA-ECMO for refractory shock
- Long observation window; escalate to retrieval before local support is exceeded
Antipsychotic with QT/NMS
- QT prolongation with torsades risk; correct potassium and magnesium
- Intravenous magnesium for torsades; avoid other QT-prolonging drugs
- Neuroleptic malignant syndrome: cooling, benzodiazepines, supportive care
- Monitor CK and renal function; admit for ongoing care
In the toddler with exploratory ingestion of a grandparent's verapamil, the dose per kilogram is magnified by the small body mass, and a sustained-release preparation can deteriorate hours after a well-looking presentation; calcium and high-dose insulin euglycaemic therapy are started early and the child is observed for at least 12 to 24 hours. The adolescent with a deliberate tricyclic overdose and a widened QRS receives sodium bicarbonate to narrow the QRS, while flumazenil is withheld because it can precipitate seizures when a proconvulsant such as a tricyclic has been co-ingested. A mixed beta-blocker and calcium channel blocker overdose is the scenario where combined high-dose insulin euglycaemic therapy is most clearly indicated, layering calcium, insulin and vasopressors. [3] [9]
Complications & Pitfalls
Most preventable harm in paediatric cardiotoxic poisoning comes from a small number of errors: throwing a class Ia or Ic antiarrhythmic at a tricyclic-induced rhythm, forgetting glucose and potassium during high-dose insulin, missing sustained-release delayed toxicity, withholding bicarbonate for a borderline QRS, or escalating inotropes alone in a beta-blocker or calcium channel blocker overdose. Each is a failure of the principle rather than a failure of knowledge. [1] [2]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Class Ia or Ic antiarrhythmic for a tricyclic rhythm | Worsens sodium-channel blockade and the arrhythmia | Sodium bicarbonate first; lipid emulsion for refractory; never quinidine, procainamide, flecainide or amiodarone |
| Forgetting glucose and potassium during HIET | Hypoglycaemia and hypokalaemia; the latter prolongs the QT | Check glucose and potassium hourly; replace potassium to above 4 mmol per L; give dextrose to maintain euglycaemia |
| Missing sustained-release delayed toxicity | The child deteriorates after a reassuring phase | Observe 12 to 24 hours for sustained-release CCB; reassess the ECG and perfusion frequently |
| Withholding bicarbonate for a borderline QRS | The arrhythmia and the hypotension worsen | Give bicarbonate for a QRS over 100 ms or hypotension; repeat to narrow the QRS and raise the pH |
| Escalating inotropes alone in BB or CCB overdose | Poor response; delayed definitive therapy | Start calcium and high-dose insulin euglycaemic therapy early; add vasopressors and prepare lipid emulsion and ECMO |
| Giving flumazenil when a tricyclic may be co-ingested | Seizures from removed GABA inhibition | Avoid flumazenil in mixed or unknown overdose; prefer supportive airway and ventilation |
| Attributing bradycardia to a single drug | Hyperkalaemia, hypoglycaemia, sepsis and a cardiac cause are missed | Check glucose, gas, potassium and the ECG; keep non-toxic causes open |
| Late escalation and retrieval | Support is unavailable when the child collapses again | Call senior, intensive care, retrieval and the Poisons Information Centre early; activate ECMO before arrest |
After resuscitation, watch actively for harm from the toxicity itself and from its treatment: ventricular arrhythmia and hypoxic brain injury from delayed sodium bicarbonate, hypoglycaemia and hypokalaemia from high-dose insulin, hypercalcaemia and pancreatitis from repeated calcium doses, pancreatitis and acute respiratory distress syndrome from lipid emulsion, and aspiration from a depressed airway. The child who survives the first hour still needs meticulous ongoing care, and a new ECG change or a falling blood pressure can mark a complication as readily as a relapse. [6] [9]
[1] [2]Prognosis & Disposition
Disposition follows the agent, the formulation, the trend and the observation window, not a single reassuring reading. Consider the duration of action of the substance, the sustained-release nature, the co-ingestants, the response to treatment, the local resources, the transport risk, and the social and mental-health context. [1] [4]
Intensive care or retrieval
- Cardiotoxic shock, a ventricular arrhythmia or the need for HIET
- Sustained-release poisoning with ECG or haodynamic instability
- Lipid emulsion or VA-ECMO required or being prepared
- A widened QRS or a long QT that has not normalised
High-dependency or ward observation
- Symptomatic but stabilised child needing close monitoring
- Observation window for a sustained-release ingestion not yet elapsed
- Ongoing insulin, calcium or bicarbonate therapy
- Rising or falling trend in QRS, QT or lactate
Observation and discharge
- Asymptomatic after the relevant observation window
- Immediate-release ingestion with a normal ECG and perfusion
- Glucose, vital signs, QRS and QT normal and stable
- Safety-net, poison-prevention advice, and mental-health and social follow-up arranged
Outcome depends on the speed of airway protection, the early reading of the ECG, and the prompt use of the targeted antidote. The children who do worst are those with delayed bicarbonate for a tricyclic arrest, sustained-release verapamil ingestion with late shock, and large co-ingestions. Outcome is generally good when the airway, breathing, circulation and the ECG are held safe and the targeted antidote is given early. Survivors of a deliberate overdose need a mental-health and social assessment before discharge, with a safety plan and clear follow-up, because the index event is a marker of ongoing risk. [1] [8]
Special Populations
Adapt how you assess, dose and escalate, but never lower the standard for reading the ECG and the toxidrome. The principles apply across ages and abilities; the differences are in weight-based dosing, drug handling, communication and the social context. [1]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Toddler exploratory ingestion | Weight-based calcium, insulin and bicarbonate; long observation for sustained-release | A single sustained-release tablet can be lethal; observe 12 to 24 hours |
| Child with cardiac disease or on a QT drug | Lower threshold for QT monitoring and magnesium; avoid other QT-prolonging drugs | Underlying conduction disease amplifies the toxicity |
| Adolescent deliberate overdose | Confidential, non-judgemental history; paracetamol and salicylate levels; mental-health assessment | Do not let confidentiality delay safety or safeguarding |
| Child with disability or neurodiversity | Use the caregiver's baseline for mental-state and extrapyramidal assessment | Altered baseline obscures early toxicity |
| Rural or remote location | Early retrieval and toxicologist contact; activate ECMO service early | Transport time is long; escalate before local support is exceeded |
Safeguarding runs in parallel with medical care, and immediate stabilisation comes first. An ingestion in a young child may reflect unsafe medication storage, neglect, or an unsafe home environment, while an adolescent presentation may signal self-harm or risk that needs a careful psychosocial assessment. Ask only necessary open, non-leading questions, document objective findings and spontaneous words, and use the local safeguarding and mental-health pathway. Reporting thresholds, consent rules and confidentiality provisions differ by Australian state or territory, UK nation, US state and Canadian province or territory. [1]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The structure of management — ABCDE primary survey, oxygen and ventilation, continuous ECG, bedside glucose, access, the call to the Poisons Information Centre, and the targeted antidote — is consensus across the major paediatric and toxicology sources. The four areas of active evidence are sodium bicarbonate for tricyclic cardiotoxicity, high-dose insulin euglycaemic therapy for beta-blocker and calcium channel blocker overdose, intravenous lipid emulsion, and extracorporeal support; each refines rather than replaces the supportive-care backbone. [1] [2]
On sodium bicarbonate, the mechanism and the expert consensus are clear, but the evidence base is largely mechanistic and observational, and recent review highlights the common pitfalls of giving it without a trigger or an endpoint. On high-dose insulin euglycaemic therapy, observational data and a systematic review of propranolol toxicity support its early use in severe beta-blocker and calcium channel blocker overdose, with glucose and potassium monitoring. On lipid emulsion, a 2025 narrative review confirms its place as an adjunct for selected severe lipophilic drug toxicity. On extracorporeal support, case series and reports describe veno-arterial ECMO bridging refractory calcium channel blocker overdose to recovery. [2] [5]
Jurisdictional implementation
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne clinical guidelines drive local implementation of poisoning management. The NSW Poisons Information Centre on 13 11 26 (0800 764 766 in New Zealand) gives 24-hour specialist advice and should be called early. ANZCOR Guideline 12.2 governs paediatric advanced life support. Drug availability, insulin and calcium product strengths, lipid emulsion stocking and the location of paediatric ECMO services remain state-, territory- or service-specific. In Aotearoa New Zealand, verify the active local poisons, retrieval and safeguarding pathways rather than borrowing an Australian threshold.
Exam Pearls
Recognition
- Read the ECG and the toxidrome first, not the bottle
- Tricyclic: widened QRS, anticholinergic picture, hypotension, tall R in aVR
- Beta-blocker: bradycardia, hypotension, AV block; propranolol adds seizures and wide QRS
- Calcium channel blocker: bradycardia with hypotension and hyperglycaemia
- Antipsychotic: QT prolongation, sedation, extrapyramidal signs, NMS
First minutes
- ABCDE, oxygen, ventilation, continuous ECG, bedside glucose, access
- Call senior, intensive care and the Poisons Information Centre in parallel
- Measure the QRS width and the corrected QT
- Send paracetamol and salicylate levels in every intentional ingestion
Tricyclic and sodium bicarbonate
- Bicarbonate 1 to 2 mL per kg of 8.4 per cent for a widened QRS, ventricular arrhythmia or hypotension
- Repeat to narrow the QRS and raise the pH to 7.45 to 7.55
- Never give class Ia or Ic antiarrhythmics or amiodarone for a tricyclic rhythm
- Lipid emulsion and ECMO for refractory cases
Beta-blocker and CCB
- High-dose insulin euglycaemic therapy: 1 unit/kg then 0.5 to 1 unit/kg/hr with glucose
- Calcium gluconate 0.6 mL/kg of 10 per cent or calcium chloride 0.2 mL/kg of 10 per cent
- Monitor glucose and potassium hourly; keep potassium above 4 mmol per L
- Hyperglycaemia points to CCB; watch for sustained-release late deterioration
Antipsychotic
- Correct potassium and magnesium; keep potassium above 4 mmol per L
- Magnesium 25 to 50 mg/kg for QT prolongation or torsades
- Avoid every other QT-prolonging drug
- NMS: cooling, benzodiazepines, supportive care, CK and renal monitoring
Pitfalls
- No class Ia or Ic antiarrhythmic for a tricyclic
- No forgotten glucose or potassium during HIET
- No reassurance in a sustained-release well-looking phase
- No flumazenil when a tricyclic may be co-ingested
“Read the ECG and the toxidrome → ABCDE, oxygen, ventilation, continuous ECG, glucose, access, call for help and the Poisons Information Centre → sodium bicarbonate for the tricyclic widened QRS → calcium and high-dose insulin euglycaemic therapy for the beta-blocker and calcium channel blocker → magnesium and electrolyte correction for the antipsychotic QT → lipid emulsion and VA-ECMO for refractory cases → reassess, observe for the relevant window, and arrange safeguarding and mental-health follow-up.”
Viva: why sodium bicarbonate for the tricyclic widened QRS?
The widened QRS of tricyclic antidepressant poisoning is sodium-channel blockade, and sodium bicarbonate is the antidote by three mechanisms. The sodium load overcomes the channel blockade and speeds conduction, narrowing the QRS. The alkalinisation raises the pH and reduces the free fraction of the drug by increasing its protein binding and shifting it off the receptor. The extracellular sodium raises the gradient that the channel needs. Give 1 to 2 mL per kilogram of 8.4 per cent intravenously, repeated to narrow the QRS and raise the serum pH to 7.45 to 7.55, and never substitute a class Ia or Ic antiarrhythmic, which worsens the blockade.
Viva: what is high-dose insulin euglycaemic therapy and when is it used?
High-dose insulin euglycaemic therapy is the key therapy for severe beta-blocker and calcium channel blocker overdose with shock or myocardial depression. It shifts the failing, toxin-depressed myocardium onto carbohydrate metabolism and restores inotropy, and it corrects the toxin-induced insulin resistance of calcium channel blocker overdose. The dose is insulin 1 unit per kilogram intravenous bolus then 0.5 to 1 unit per kilogram per hour, with a dextrose infusion to maintain euglycaemia and hourly glucose and potassium monitoring. Calcium and vasopressors are given in parallel, and lipid emulsion and ECMO are prepared for refractory cases.
Structured oral: a toddler who has taken a grandparent's sustained-release verapamil
Recognise the calcium channel blocker picture: bradycardia with hypotension and, typically, hyperglycaemia. Run the ABCDE survey, secure the airway and give oxygen, attach a continuous ECG, check the bedside glucose, establish access, and call the senior team, intensive care, retrieval and the Poisons Information Centre. Start intravenous calcium and high-dose insulin euglycaemic therapy early, add vasopressors, and prepare intravenous lipid emulsion and veno-arterial ECMO for refractory shock. Because the formulation is sustained-release, observe for at least 12 to 24 hours for late deterioration, and run poison-prevention counselling and safeguarding alongside the medical care.
References
- [1]Hoffman, Robert J; Nillas, Anthony Toxidromes and a general approach to poisoning Archives of Disease in Childhood, 2025.PMID 39978865
- [2]Chan, Brandon S; Buckley, Nicholas A Common pitfalls in the use of hypertonic sodium bicarbonate for cardiac toxic drug poisonings Clinical Toxicology (Philadelphia), 2024.PMID 38597366
- [3]Roperia, Vikrant; Kiani, Ahsan Zaheer High-Dose Insulin Euglycemic Therapy in Concomitant Beta-Blocker and Calcium Channel Blocker Overdose Journal of Investigative Medicine High Impact Case Reports, 2025.PMID 40642834
- [4]Suarez, Francis; Koyfman, Alex Pearls and Pitfalls for the Emergency Clinician: Beta Blocker and Calcium Channel Blocker Toxicity Journal of Emergency Medicine, 2026.PMID 41833262
- [5]Hu, Yi; Mujahid, Kaleem Effectiveness of treatments for propranolol toxicity: a systematic review of current approaches and evidence European Journal of Clinical Pharmacology, 2026.PMID 41546730
- [6]Nendumba, Gosberthan; Blackman, Stephen Use of intravenous lipid emulsions in drug-induced toxicities: a 2025 narrative review Annals of Intensive Care, 2025.PMID 41247632
- [7]Besag, Frank M C; Vasey, Maxine J Neurological Adverse Effects of Antipsychotic Medication in Children and Young People Paediatric Drugs, 2026.PMID 41498920
- [8]Darke, Shane; Duflou, Joanne Characteristics and toxicology of adult deaths due to quetiapine toxicity in Australia, 2000-2024 Journal of Forensic Sciences, 2025.PMID 40588799
- [9]Frithsen, Iliana L; Simpson, William M Jr Recognition and management of acute medication poisoning American Family Physician, 2010.PMID 20112890
- [10]Cheon, Jae Hee; Miller, Matthew Beyond vasopressor support: VA-ECMO for refractory calcium channel blocker overdose South African Medical Journal, 2025.PMID 41378535