Paeds · acute-care-resuscitation-and-toxicology
Envenomation and marine bites
Also known as Snake bite · Funnel-web spider bite · Redback spider bite · Box jellyfish sting · Irukandji syndrome · Stingray injury · Pressure-immobilisation bandage
Fellowship guide to envenomation and marine bites in children: pressure-immobilisation first aid for snakes and funnel-web spiders, venom-induced consumption coagulopathy and neurotoxicity, Australian snake antivenom dosing, funnel-web and redback spider envenomation, box jellyfish and Irukandji syndromes, and hot-water first aid for stingray and stonefish injuries.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A seven-year-old is carried into a country emergency department an hour after stepping on a brown snake in long grass, an armband tight on his bitten forearm and a worried father beside him, and a toddler arrives screaming from a north Queensland beach with angry whip-marks across her legs. These are the two faces of paediatric envenomation, and the first decisions — the right bandage, the right fluid, the right antidote — decide the outcome. Envenomation is the process by which animal venom causes harmful effects after a bite or sting, and in the Australian and tropical context the creatures that matter are the terrestrial elapid snakes, the funnel-web and redback spiders, the box and Irukandji jellyfish, and the spined marine animals such as the stingray and stonefish. [1] [12]
The uniting principle is that envenomation is a time-dependent, toxin-driven emergency in which a child's smaller body mass means a given venom load reaches effective concentration sooner and at lower volumes than in an adult, so children are often more severely affected. The first-aid manoeuvre must match the creature — a pressure-immobilisation bandage for snakes, funnel-web spiders, blue-ringed octopus and cone snails whose venom travels in lymph, but hot water for the heat-labile venoms of the stingray, stonefish and bluebottle, and vinegar for the box jellyfish whose nematocysts keep discharging. The hospital response then searches for the venom's target organ — coagulation, nerve, muscle, kidney, or heart — and gives antivenom only when there is clinical or laboratory evidence of that injury. [5] [9]
Two ideas carry the whole topic. The first is that antivenom is a specific but hazardous treatment, given for proven envenomation rather than prophylactically, because every antivenom is a foreign protein that can cause immediate hypersensitivity or serum sickness. The second is that the observation strategy is as important as the antidote, because many snake bites are dry or minimally envenomating, and because the coagulopathy, myotoxicity and neurotoxicity declare themselves over hours that must not be cut short. [1] [6]
Classification
Envenomation is classified first by the creature and its venom's target organ, because the creature sets the first-aid manoeuvre and the target organ sets the investigation and the antivenom. The terrestrial elapid snakes produce four overlapping clinical syndromes that every candidate must name. Venom-induced consumption coagulopathy is the commonest, produced by the prothrombin-activating venoms of the brown, tiger and taipan snakes, and it presents with an unrecordable INR, a raised D-dimer and a low fibrinogen. Neurotoxicity is produced by the death adder (a postsynaptic blocker) and by the tiger snake and taipan (presynaptic), presenting with drooping eyelids, ophthalmoplegia and bulbar and respiratory weakness. Myotoxicity, from the mulga, tiger and rough-scaled snakes, causes rhabdomyolysis with a rising creatine kinase and dark urine. Renal failure and thrombotic microangiopathy complete the severe picture. [1] [3]

The spiders split cleanly by toxin and by first aid. The funnel-web spider of eastern Australia produces a neurotoxin that triggers massive neurotransmitter release — a catecholamine surge with salivation, sweating, muscle twitching, hypertension, pulmonary oedema and progressive paralysis — and it is managed with a pressure-immobilisation bandage and funnel-web spider antivenom. The redback spider produces alpha-latrotoxin, which causes severe local and radiating pain with sweating and piloerection but is rarely life-threatening, and it is managed with ice and analgesia, not a bandage. The two must never be confused, because bandaging a redback bite is useless and withholding a bandage from a funnel-web bite is dangerous. [6] [7]
First aid by creature
- Australian elapid snakes
- Funnel-web spider
- Blue-ringed octopus
- Cone snail — venom travels in lymph
- Stingray spine injury
- Stonefish sting
- Bluebottle (Physalia) sting
- Catfish, bullrout, sea urchin
- Box jellyfish (Chironex fleckeri)
- Irukandji (carybdeid) stings
- Deactivates undischarged nematocysts
- Then carefully remove tentacles
- Redback spider
- Most other spider bites
- No bandage required
- Reserve antivenom for severe cases
The marine stings are classified by the jellyfish type and the presence of a spine. The box jellyfish (Chironex fleckeri) is the most venomous animal in the sea, causing immediate agonising pain, characterful whip-like skin lesions and rapid cardiorespiratory collapse. The Irukandji syndrome, from small carybdeid jellyfish, is defined by its delayed catecholamine presentation twenty to forty minutes after a trivial sting — severe generalised pain, sweating, vomiting, hypertension and, in severe cases, cardiac failure. The bluebottle (Physalia) is the common non-tropical sting with immediate pain and linear urticaria, managed with hot water. The stingray and stonefish are spined injuries whose heat-labile venom is inactivated by hot water, with a stonefish antivenom for severe cases and a stingray injury managed as a contaminated penetrating wound. [9] [12]
Epidemiology & Risk Factors
Envenomation is a regional child-health problem shaped by geography, climate and behaviour. In Australia there are several thousand snake bites a year, with a handful of deaths, and most paediatric envenomation happens in the warmer months when children are barefoot in long grass, on farms, or at the coast. The Australian Snakebite Project, which prospectively enrolled patients over a decade, showed that the brown snake is responsible for most envenomation and most deaths, followed by the tiger snake and the taipan, and that children are over-represented among the severely envenomated because their smaller mass increases venom concentration per kilogram. [1]
The risk factors cluster by age and activity. Toddlers are bitten in gardens and farmyards while exploring; school-age children while walking in long grass, climbing rocks or handling creatures; and adolescents add alcohol, risk-taking and occupational exposure on farms and in the tropics. Aboriginal, Torres Strait Islander, Maori and Pacific children, and children in remote and tropical communities, carry a higher burden of both terrestrial and marine envenomation because of outdoor living, barefoot activity and proximity to venomous animals, and these children often present late after long retrievals. [10] [12]
Spider and marine envenomation have their own epidemiology. Funnel-web spider bites cluster in summer in coastal New South Wales after rain, when the male spiders wander, and a bite is a time-critical emergency because the toxin can kill a small child within hours. Redback spider bites are common year-round, are rarely life-threatening, and are the commonest reason antivenom is discussed in Australian emergency departments. The box jellyfish and Irukandji stings are confined to the tropical north during the warmer months and are a leading cause of marine envenomation presentation in coastal and island communities, with box jellyfish stings carrying a real risk of death within minutes. [7] [9]
Pathophysiology
To manage envenomation well you must connect each venom to the organ it injures, because the laboratory pattern and the antidote both follow the mechanism. The venom-induced consumption coagulopathy of the brown, tiger and taipan snakes is a true defibrination: the venom is a prothrombin activator that switches on the coagulation cascade, consumes clotting factors and fibrinogen, and generates fibrin degradation products, producing an unrecordable INR with a very high D-dimer and a low fibrinogen. The consumption resolves only as the liver resynthesises factors over one to three days, which is why a child can still have an unrecordable INR many hours after antivenom has neutralised the circulating venom — the antivenom stops the cause but the liver must replace the loss. [1] [4]
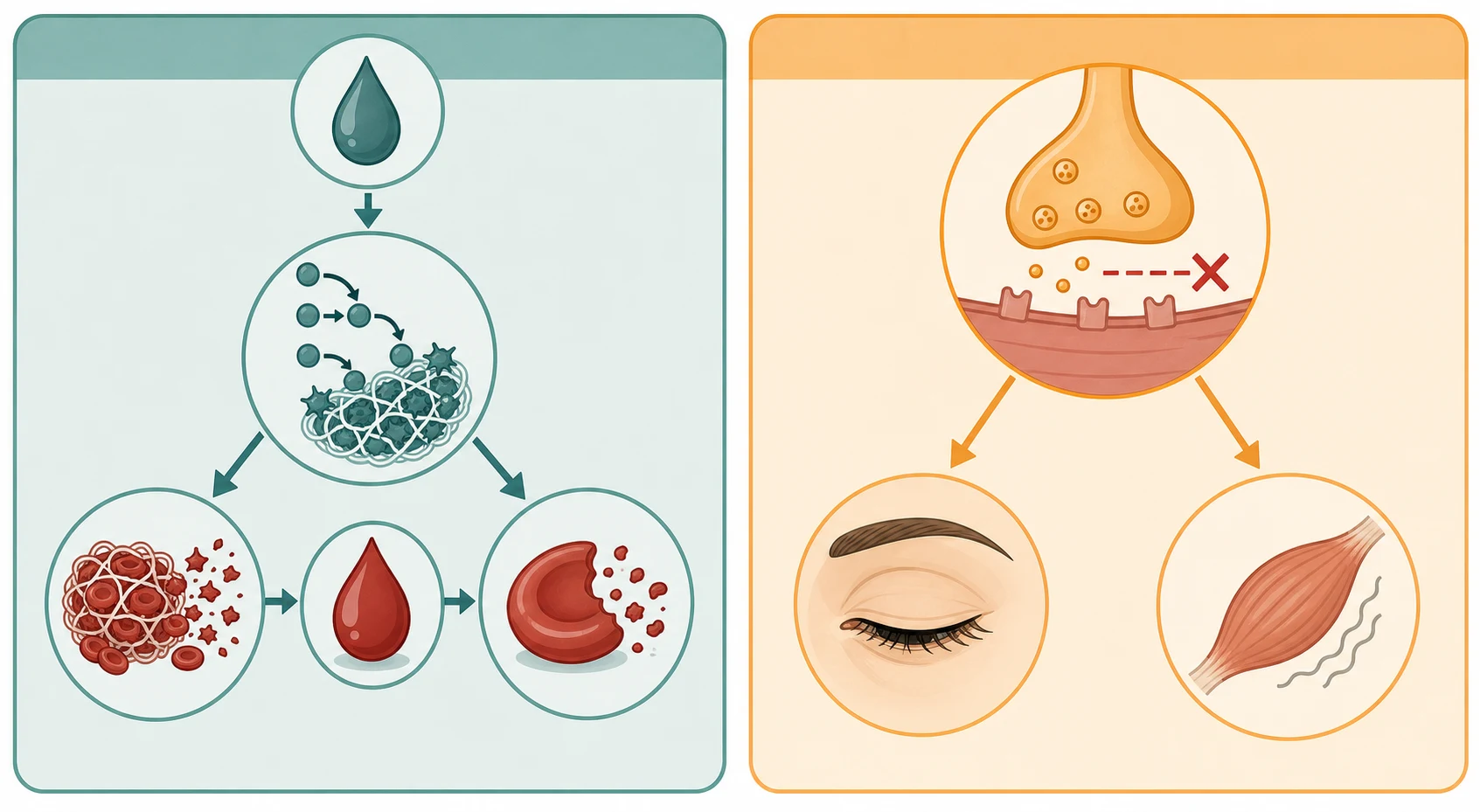
The neurotoxicity of the death adder is postsynaptic, blocking the acetylcholine receptor and producing a curare-like paralysis that may respond to antivenom and to neostigmine. The neurotoxicity of the tiger snake and taipan is presynaptic, damaging the nerve terminal so that paralysis is slower to reverse and may need prolonged ventilation, which is why early antivenom is emphasised before the nerve terminal is irreversibly damaged. The myotoxicity of the mulga, tiger and rough-scaled snakes directly injures skeletal muscle, releasing myoglobin and creatine kinase, darkening the urine and risking acute kidney injury from pigment nephropathy. [2] [3]
The funnel-web spider toxin (delta-hexatoxin) is a presynaptic neurotoxin that produces sustained acetylcholine and catecholamine release, explaining the characteristic autonomic storm — salivation, lacrimation, sweating, piloerection, hypertension and muscle fasciculation — followed by neuromuscular paralysis and pulmonary oedema. The box jellyfish venom is cardiotoxic and dermatonecrotic, the Irukandji venom triggers a delayed catecholamine surge, and the stingray and stonefish venoms are heat-labile tissue toxins that direct, blunt, heat-based first aid can inactivate. These mechanisms are why the first aid differs by creature and why the wrong first aid can make things worse. [7] [9]
Clinical Presentation
The presentation of a bitten or stung child ranges from the asymptomatic "dry bite" to sudden cardiorespiratory collapse, and the severity is often not apparent at first contact. A snake-bitten child may walk in looking well with a faint fang mark and no symptoms, yet harbour a life-threatening coagulopathy that declares itself only on the blood test, which is why every suspected snake bite is observed with serial coagulation until envenomation is excluded. The child with systemic features looks different — nauseated, diaphoretic, with abdominal pain, a tender regional lymph node, drooping eyelids, double vision, or dark urine — each pointing to a venom syndrome. [1]
The history must capture the time, the place and the activity. Record the time of the bite or sting, the geographical location and the circumstance (long grass, rock-climbing, wading at a tropical beach, gardening), what the creature looked like if it was seen, whether first aid was applied and how, and the onset, sequence and progression of symptoms. A photo of the dead snake can help identification but must never delay first aid or transfer, and a description of whip-like skin lesions after a tropical swim points straight to the box jellyfish. [9] [10]
The funnel-web spider bite is a clinical emergency with a distinctive course. Within minutes to an hour the child develops profuse salivation, lacrimation and sweating, piloerection, tingling around the mouth, muscle fasciculation, hypertension and a fast heart rate, progressing to pulmonary oedema, confusion and respiratory failure. The bite itself is painful with visible fang marks, and the syndrome is most severe in small children. The redback spider bite, by contrast, produces an immediate sharp pinprick, then escalating local pain, sweating and piloerection at the bite site and in the affected limb, sometimes with remote pain and sweating, malaise and headache, but it does not threaten the airway. [6] [7]
Differential Diagnosis
During the first hours the differential condenses to the causes that sit behind the presentation and that change management. A snake bite must be distinguished from a spider bite, a fall, or a simple laceration, and a child who collapses after a sting at a tropical beach is assumed to have a box jellyfish envenomation until proven otherwise. The coagulopathy of snake bite must be separated from other bleeding disorders, but its pattern — unrecordable INR with very high D-dimer and low fibrinogen after a definite bite — is distinctive. [1] [4]
The stingray injury carries a differential of its own because the barb is a penetrating weapon. A puncture wound to the chest or abdomen, as in the well-publicised cardiac injuries, is managed as major trauma with vascular and cardiac injury rather than as a simple sting, because the barb can lacerate the heart or a great vessel and leave a retained foreign body. A wound to the limb is a contaminated puncture with tissue and venom injury, at risk of infection with marine organisms including Vibrio species. [12]
Reversible considerations in the envenomed child
- Venom-induced consumption coagulopathy with occult bleeding
- Anaphylaxis to the venom or to antivenom
- Tension pneumothorax in the ventilated neurotoxic child
- Cardiac injury from a stingray barb to the chest
- Presynaptic neurotoxicity from tiger snake or taipan
- Funnel-web spider autonomic storm and paralysis
- Blue-ringed octopus tetrodotoxin paralysis
- Hypoglycaemia in the cold or exhausted child
The remaining differentials are the conditions that masquerade as envenomation or complicate it. Anaphylaxis to a sting, especially in the venom-allergic child, can mimic or coexist with envenomation and is treated with intramuscular adrenaline. The Irukandji syndrome is itself a differential of severe pain and hypertension after a tropical sting, and is missed if the trivial initial sting is forgotten and the delayed presentation is attributed to another cause. In the young child with an unwitnessed collapse and an unclear history, non-accidental injury and other toxin ingestion must be held in mind alongside envenomation. [10]
Clinical & Bedside Assessment
The assessment runs inside a calm, team-based sequence that begins with the first aid already in place. For a suspected snake or funnel-web spider bite, confirm that a pressure-immobilisation bandage is correctly applied — firm, from the fingers or toes up the whole limb, with a splint, and with the child kept still and calm — and leave it in place until envenomation is excluded in hospital, because removing it prematurely can release a bolus of venom. Run an airway, breathing, circulation and disability survey, attach oxygen and monitoring, establish intravenous access in an unaffected limb, and take the first bloods while the bandage stays on. [5]
The pressure-immobilisation bandage is examined heavily because it is the single most tested manoeuvre in this topic. Apply a broad crepe bandage over the bite site first, then bandage firmly from the digits up the whole limb — about as tight as a bandage for a sprained ankle, firm enough to obstruct lymphatic and venous flow but not arterial, checking that distal pulses and capillary refill remain — then immobilise the limb with a splint and keep the child still, because movement pumps venom along the lymphatics. The bandage is indicated for snake, funnel-web spider, blue-ringed octopus and cone snail envenomation, and it is not indicated for redback spider bites, jellyfish stings, or stingray and stonefish injuries. [5]
Pressure-immobilisation bandage — the RIGHT technique
The examination then searches each target organ. Look for fang or puncture marks, regional lymph node tenderness, and the whip-like lesions of a jellyfish sting; examine the eyes for ptosis and ophthalmoplegia and the mouth for drooling and a weak voice that signal bulbar neurotoxicity; palpate and move the muscles for the tenderness of myotoxicity; check the urine for haemoglobin and myoglobin; and repeat the observations and the blood tests at set intervals, because the syndromes evolve over hours. The child who is asymptomatic at one hour may still develop an unrecordable INR or a rising creatine kinase at four or six hours. [1] [3]
Investigations
Investigations serve two questions: which venom syndrome is present, and how severe is the organ injury. The cornerstone panel for any suspected snake bite is a coagulation profile (INR, activated partial thromboplastin time, fibrinogen and D-dimer), a creatine kinase, electrolytes and urea, a full blood count, a blood group and hold, and a urinalysis, repeated at intervals because the coagulopathy and myotoxicity evolve. An unrecordable INR with a very high D-dimer and a low fibrinogen confirms venom-induced consumption coagulopathy; a creatine kinase that climbs into the thousands confirms myotoxicity; and a rising creatinine with pigmenturia flags renal injury. [1] [3]
Where a laboratory is not immediately available, the twenty-minute whole blood clotting test is a bedside screen for coagulopathy. A few millilitres of venous blood are placed in a clean glass tube and left for twenty minutes; blood that has not clotted indicates a coagulopathy from a prothrombin-activating snake venom, and a scoping review of handheld and point-of-care tests confirms the value of this simple test where laboratory turnaround is slow. A positive test in an endemic region justifies antivenom while formal results are awaited. [4]
Venom identification guides the choice of monovalent antivenom and reduces exposure to polyvalent antivenom. A snake venom detection kit can be performed on a swab of the bite site, on urine or on blood, and it indicates which monovalent antivenom binds the venom. It is not used to decide whether to give antivenom — that decision is clinical and laboratory — and it should not delay antivenom in a severely envenomated child. For the jellyfish and marine stings the diagnosis is clinical from the history and the skin lesions, and a chest radiograph, troponin and blood gas are added for the child with suspected Irukandji or box jellyfish cardiotoxicity. [9] [10]
Management — Resuscitation
The first act is to confirm or apply the correct first aid and to resuscitate the airway, breathing and circulation. For a snake or funnel-web spider bite, keep the pressure-immobilisation bandage in place, keep the child still, give oxygen and attach monitoring, and establish intravenous access in an unaffected limb. For a box jellyfish sting, remove the child from the water, call for help, begin cardiopulmonary resuscitation if there is no pulse, and douse the adherent tentacles with vinegar for at least thirty seconds before they are carefully lifted off — never rub the area, and never use fresh water, which causes further nematocyst discharge. [5] [9]
Pressure-immobilisation bandage (snake and funnel-web bite)
Dose
Broad crepe bandage applied over the bite, then firmly from the fingers or toes up the whole limb, tight enough to obstruct lymphatic flow but not arterial supply, with a splint and the limb kept still
For the heat-labile venoms, hot water is the first aid. Immerse the stingray or stonefish wound, or the bluebottle sting, in water as hot as the child can tolerate — about forty-five degrees Celsius and not scalding — for up to twenty minutes, which inactivates the venom and relieves the pain, then explore the wound for a retained spine, irrigate and debride, give tetanus prophylaxis, and start antibiotics for the contaminated marine wound. Reassess the airway and breathing continuously in the funnel-web and neurotoxic snake-bitten child, because progression to respiratory failure can be rapid and may need bag-mask ventilation and intubation. [11] [12]
The first thirty minutes for the snake-bitten child
Confirm the pressure-immobilisation bandage is correct; keep the child still and calm
Airway, breathing, circulation; oxygen and monitoring; intravenous access in an unaffected limb
Send coagulation profile, creatine kinase, electrolytes, full blood count, group and hold, urinalysis
Repeat the bloods at set intervals; perform a 20-minute whole blood clotting test if laboratory is delayed
Give snake antivenom intravenously for systemic or laboratory envenomation; prepare for anaphylaxis
Leave the bandage in place until envenomation is excluded; admit and observe
Management — Definitive & Stepwise
The definitive treatment is antivenom, given intravenously for clinical or laboratory envenomation and chosen by the creature. For Australian elapid snake envenomation the Australian Snakebite Project supports an initial dose of one vial for the brown, tiger, taipan and death adder, with multiple vials often needed for the mulga or black snake, and polyvalent snake antivenom when the snake cannot be identified and the child is severely envenomated. The decision to give antivenom rests on systemic features or an abnormal coagulation profile or creatine kinase — not on the bite alone — because most bites are dry or minimally envenomating and antivenom is not without risk. [1] [2]
Australian snake antivenom ( CSL )
Dose
Initial one vial intravenously for brown, tiger, taipan and death adder; multiple vials may be needed for mulga or black snake; polyvalent if the snake cannot be identified
Every antivenom is a foreign protein that can cause an immediate hypersensitivity reaction in about five per cent of recipients and serum sickness days later, so the child is observed during and after the infusion, with resuscitation equipment ready. Routine premedication is not recommended. Anaphylaxis to antivenom is treated as any anaphylaxis — remove the infusion, give intramuscular adrenaline at ten micrograms per kilogram of one in one thousand, oxygen, fluids and an antihistamine — and then, balancing risk and benefit, the antivenom is often recommenced slowly because the underlying envenomation still needs neutralising. Serum sickness in the week after is treated with corticosteroids. [1] [8]
The spider and marine antivenoms have their own indications. Funnel-web spider antivenom is given intravenously, two vials initially and repeated, for any systemic envenomation, with atropine and glycopyrrolate to control the profuse secretions and supportive ventilation as needed; it is highly effective and has eliminated funnel-web deaths since its introduction. Redback spider antivenom is reserved for severe or refractory latrodectism, given intravenously, because the second Redback Antivenom Evaluation trial showed that intravenous antivenom was no better than placebo for pain and carried a reaction risk, so supportive care with opioids and benzodiazepines is the mainstay. Box jellyfish antivenom is given intravenously for cardiorespiratory compromise, with magnesium considered for the failing heart. Stonefish antivenom is given intramuscularly for severe or multiple-spine injuries after hot water first aid. [7] [8]
Funnel-web spider antivenom
Dose
Two vials intravenously initially, repeated as required until symptoms settle, with atropine or glycopyrrolate for secretions
Specific Subtypes & Scenarios
The asymptomatic snake bite is the scenario most rewarding a disciplined observation strategy. A child who looks well after a suspected bite may still have a venom-induced consumption coagulopathy, so the bandage stays on, bloods are sent and repeated at intervals, and the child is observed until coagulation and creatine kinase are normal on repeated testing. Only then is the bandage removed and the child considered for discharge, because removing the bandage earlier can release a bolus of venom and precipitate envenomation. [1]
The box jellyfish sting is the marine emergency that can kill within minutes. After vinegar dousing and tentacle removal, the child with collapse, cardiorespiratory arrest or severe pain is given intravenous box jellyfish antivenom, magnesium is considered for cardiovascular instability, and high-quality cardiopulmonary resuscitation is continued because the venom is cardiotoxic and recovery is possible. The whip-like, cross-hatched skin lesions are characteristic, and death has occurred in small children within twenty minutes of the sting. [9]
In Australia and New Zealand, follow the Australian Resuscitation Council and ANZCOR guidelines: the pressure-immobilisation bandage for snake, funnel-web spider, blue-ringed octopus and cone snail envenomation; vinegar dousing for box jellyfish and Irukandji stings; hot water for bluebottle, stingray and stonefish; and the specific CSL antivenoms for confirmed envenomation. The Royal Children's Hospital Melbourne clinical practice guideline on envenomation is the regional bedside reference, and the Poisons Information Centre on thirteen eleven twenty-six and the Clinical Toxinology Resources of the University of Adelaide support antivenom choice, especially for retrieval from rural and remote regions.
[5][9]The Irukandji syndrome declares itself twenty to forty minutes after a trivial carybdeid sting, with severe generalised muscle, back, abdominal or chest pain, sweating, vomiting, hypertension and a feeling of doom. The child is admitted for opioid analgesia, control of the catecholamine surge with magnesium, glyceryl trinitrate or an alpha-blocker, and cardiac monitoring for the troponin rise, pulmonary oedema and dysfunction that define the severe end of the syndrome. There is no specific antivenom, and supportive care over one to two days is usually sufficient. [10]
The stingray injury is managed as a contaminated penetrating wound with venom. After hot water immersion for up to twenty minutes, the wound is explored for a retained spine (which often breaks off and must be imaged and removed), irrigated and debrided, given tetanus prophylaxis, and covered with antibiotics against marine organisms including Vibrio species. A stingray wound to the chest or abdomen is a major trauma with a real risk of cardiac and great-vessel injury and is managed accordingly. [12]
Complications & Pitfalls
The commonest preventable failure in snake bite is premature removal of the pressure-immobilisation bandage. A bandage taken off in the first hour, before the coagulation profile is known, can release a bolus of lymphatic venom and precipitate envenomation in a child who had been well, which is why the bandage stays in place until envenomation is excluded on repeated blood tests. The corollary failure is applying the wrong first aid — bandaging a redback spider bite, washing a snake bite site, or using fresh water on a box jellyfish sting — each of which can make the envenomation worse. [1] [5]
A second group of pitfalls surrounds antivenom. Giving antivenom for a dry bite exposes the child to a hypersensitivity reaction for no benefit, which is why antivenom is reserved for clinical or laboratory envenomation; at the other extreme, withholding antivenom from a neurotoxic or coagulopathic child while waiting for venom detection can allow irreversible presynaptic nerve damage or major bleeding. A reaction to antivenom is treated as anaphylaxis with intramuscular adrenaline, and then a measured decision is made about whether and how to continue the antivenom. Failing to warn the family about serum sickness in the week after misses a treatable complication. [1] [8]
The remaining pitfalls are the late and remote complications. The coagulopathy carries a real risk of intracranial bleeding, the myotoxicity a risk of acute kidney injury from pigment nephropathy, and the funnel-web and neurotoxic snake bites a risk of prolonged ventilator dependence. The stingray wound carries a risk of retained spine and marine-organism infection, the box jellyfish sting a risk of late cardiomyopathy, and the Irukandji syndrome a risk of troponin rise and cardiac failure, so each child is observed for the complication that matches the creature. [2] [10]
Prognosis & Disposition
Outcome after envenomation is driven by the creature, the dose, the time to first aid and antivenom, and the quality of organ support. Most Australian snake bites are dry or minimally envenomating and do well with observation, while the brown snake is responsible for most deaths through coagulopathy-related bleeding and the taipan and death adder through neurotoxicity. Early pressure-immobilisation first aid and early antivenom for neurotoxic bites improve outcome, because presynaptic nerve damage is poorly reversible once established. [1] [2]
The Australian Snakebite Project, 2005-2015 (ASP-20)
Population: A decade of prospectively enrolled Australian snakebite patients across the continent
Key finding
Brown snake envenomation was commonest and caused most deaths; venom-induced consumption coagulopathy was the leading syndrome; initial one-vial antivenom dosing was supported for most species, with a hypersensitivity reaction in around five per cent
Practice change
Most Australian snake bites are dry or minimally envenomating; antivenom is reserved for clinical or laboratory envenomation, and a single initial vial suffices for most species
The funnel-web spider has caused no deaths since the introduction of funnel-web antivenom, and the box jellyfish remains one of the few creatures that can kill a child within minutes, with survival depending on immediate vinegar, cardiopulmonary resuscitation and antivenom. The Irukandji syndrome usually resolves over one to two days with supportive care, though severe cases need intensive care for cardiac dysfunction. The redback spider bite is almost never fatal, and the RAVE-II trial reshaped practice by showing that intravenous redback antivenom offered little benefit over placebo for pain, shifting care toward analgesia. [7] [8]
Disposition follows the severity. The asymptomatic snake-bitten child is observed until coagulation is normal on repeated testing; the envenomated child is admitted, often to a paediatric intensive care unit for neurotoxic, coagulopathic or box jellyfish envenomation; and the child in a rural or remote centre is retrieved by a paediatric retrieval team with the airway secured and the bandage in place. The family is told honestly about the time course of recovery — that the INR may stay abnormal for days after antivenom — and about the risk of serum sickness, and the child is followed up to exclude the late complications of each syndrome. [1] [3]
Special Populations
Children in remote and tropical communities carry the highest burden of envenomation and the longest times to definitive care, so the irreducible core for these children is correct bystander first aid, early contact with a retrieval and a poisons information service, and a generalist who can run the pressure-immobilisation, vinegar and hot-water algorithms until help arrives. Aboriginal, Torres Strait Islander, Maori and Pacific children, and children in coastal and island communities, are reached by community-led prevention — wearing shoes, clearing long grass, swimming inside stinger nets in the tropics, and wearing protective clothing — rather than by emergency care alone. [10] [12]
The small child is more severely affected by a given venom load because venom concentration per kilogram is higher, so a brown snake or box jellyfish envenomation in a toddler can be rapidly life-threatening. Dose all antivenoms and drugs by weight, anticipate early airway and breathing failure in the funnel-web and neurotoxic snake-bitten child, and keep the parents at the bedside because the frightened child is harder to examine and to keep still. The child with a complex chronic condition or a bleeding tendency is more vulnerable to the coagulopathy and the renal complications, and the pregnant adolescent adds the physiology of pregnancy and the need to consider the fetus when choosing antivenom and imaging. [1]
In the returned traveller the creature is often unfamiliar, the bite or sting happened overseas, and the relevant antivenom may be an exotic CSL product held centrally. Take a precise travel and exposure history, assume the worst until envenomation is excluded, and contact the poisons information and toxinology services early for antivenom sourcing and advice. The prevention message for every family is concrete — wear shoes in long grass, do not handle snakes or spiders, swim inside stinger nets in the tropical season, wear protective footwear on reefs, and know the pressure-immobilisation, vinegar and hot-water first aid. [6] [9]
Evidence, Guidelines & Regional Differences
The current standard rests on the Australian Snakebite Project series, which prospectively defined the clinical syndromes and the antivenom practice for Australian elapids; the Isbister reviews of spider and marine envenomation; the Currie work on the box jellyfish; the Nickson and Tibballs descriptions of the Irukandji syndrome; the Cochrane review of jellyfish sting interventions that established hot water as effective first aid; and the Berling review of marine envenomations. The Australian Resuscitation Council and ANZCOR guidelines set the regional first aid — pressure-immobilisation for snakes and funnel-webs, vinegar for box jellyfish and Irukandji, and hot water for bluebottle, stingray and stonefish — and the Royal Children's Hospital Melbourne guideline is the paediatric bedside reference. [1] [11]
The first hours of a snake-bitten child
Where the evidence is still maturing, the answer follows the current guideline and names the source. The RAVE-II trial redefined redback antivenom use by showing limited benefit, shifting practice toward analgesia; the role of magnesium in box jellyfish and Irukandji cardiotoxicity continues to be studied; and the optimal antivenom dose for the mulga and black snake and for presynaptic neurotoxicity is still refined by the ASP series. Point-of-care coagulation devices are expanding access to the twenty-minute whole blood clotting test in remote regions, and community-led prevention remains the most effective intervention. [3] [8]
Exam Pearls
- Apply a pressure-immobilisation bandage for snake, funnel-web spider, blue-ringed octopus and cone snail envenomation — never for redback spider, jellyfish, stingray or stonefish. [5]
- Bandage from the fingers or toes up the whole limb, as firm as a sprained-ankle bandage, with a splint, and leave it in place until envenomation is excluded on repeated blood tests. [5]
- Do not wash a snake bite site — the venom on the skin is used for identification — and do not cut, suck, or apply a tourniquet. [1]
- The four snake syndromes are venom-induced consumption coagulopathy, neurotoxicity, myotoxicity, and renal failure or thrombotic microangiopathy. [1]
- Venom-induced consumption coagulopathy shows an unrecordable INR with a very high D-dimer and a low fibrinogen; the INR recovers over one to three days as the liver resynthesises factors. [4]
- Give snake antivenom intravenously for clinical or laboratory envenomation — one vial for brown, tiger, taipan and death adder; polyvalent if the snake is unidentified; expect a hypersensitivity reaction in around five per cent. [1]
- Antivenom does not normalise the INR at once — it stops the cause; the liver must replace the consumed factors, so a persistently abnormal INR after antivenom is expected. [1]
- Funnel-web spider bite is a pressure-immobilisation emergency treated with intravenous funnel-web antivenom; redback spider bite is treated with ice and analgesia, not a bandage. [6]
- Redback antivenom has limited benefit — the RAVE-II trial showed intravenous antivenom was no better than placebo for pain — so reserve it for severe refractory cases. [8]
- For the box jellyfish, douse tentacles with vinegar for at least thirty seconds, then remove them, and give intravenous box jellyfish antivenom for cardiorespiratory collapse. [9]
- For the bluebottle, stingray and stonefish, use hot water at about forty-five degrees for up to twenty minutes; give stonefish antivenom intramuscularly for severe or multiple-spine injury. [11]
- Irukandji syndrome presents twenty to forty minutes after a trivial sting with severe pain, sweating and hypertension — admit for analgesia and cardiac monitoring. [10]
- The twenty-minute whole blood clotting test: unclotted venous blood after twenty minutes means a coagulopathy, guiding antivenom where laboratory turnaround is slow. [4]
- Treat antivenom anaphylaxis with intramuscular adrenaline at ten micrograms per kilogram of one in one thousand, then decide whether to continue the antivenom. [1]
References
- [1]Johnston CI, Ryan NM, Page CB, et al. The Australian Snakebite Project, 2005-2015 (ASP-20). Med J Aust, 2017.PMID 28764620
- [2]Johnston CI, O'Leary MA, Isbister GK. Australian taipan (Oxyuranus spp.) envenoming: clinical effects and potential benefits of early antivenom therapy - Australian Snakebite Project (ASP-25). Clin Toxicol (Phila), 2017.PMID 27903075
- [3]Johnston CI, Isbister GK. Australian snakebite myotoxicity (ASP-23). Clin Toxicol (Phila), 2021.PMID 33156703
- [4]Abouyannis M, Marriott AE, et al. Handheld Point-of-Care Devices for Snakebite Coagulopathy: A Scoping Review. Thromb Haemost, 2025.PMID 39214143
- [5]Little M. Harm due to the use of pressure bandage immobilisation in patients bitten by snakes in Australia. Clin Toxicol (Phila), 2023.PMID 37668172
- [6]Isbister GK, Fan HW. Spider bite. Lancet, 2011.PMID 21762981
- [7]Isbister GK, Gray MR, et al. Funnel-web spider bite: a systematic review of recorded clinical cases. Med J Aust, 2005.PMID 15850438
- [8]Isbister GK, Page CB, Buckley NA, et al. Randomized controlled trial of intravenous antivenom versus placebo for latrodectism: the second Redback Antivenom Evaluation (RAVE-II) study. Ann Emerg Med, 2014.PMID 24999282
- [9]Currie B. Clinical implications of research on the box-jellyfish Chironex fleckeri. Toxicon, 1994.PMID 7886690
- [10]Nickson CP, Waugh EB, Jacups SP, Currie BJ. Irukandji syndrome case series from Australia's Tropical Northern Territory. Ann Emerg Med, 2009.PMID 19409658
- [11]McGee RG, Miller G, Lassig CJ, et al. Interventions for the symptoms and signs resulting from jellyfish stings. Cochrane Database Syst Rev, 2023.PMID 37272501
- [12]Berling I, Isbister G. Marine envenomations. Aust Fam Physician, 2015.PMID 25688956