Paeds · acute-care-resuscitation-and-toxicology
Heat illness, hypothermia and environmental emergencies
Also known as Heat stroke · Heat exhaustion · Exertional heat illness · Accidental hypothermia · Environmental hypothermia · Acute mountain sickness · Altitude illness · Lightning injury · Electrical injury
Fellowship guide to heat illness, accidental environmental hypothermia and the principal environmental emergencies in children: the heat-illness spectrum and the cold-water-immersion cooling target, the Swiss hypothermia staging and the rewarming ladder with the hypothermic-arrest defibrillation rules, acute mountain illness with the Lake Louise score and the descent-first rule for high-altitude cerebral and pulmonary oedema, and the lightning reverse-triage and electrical-injury principles.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
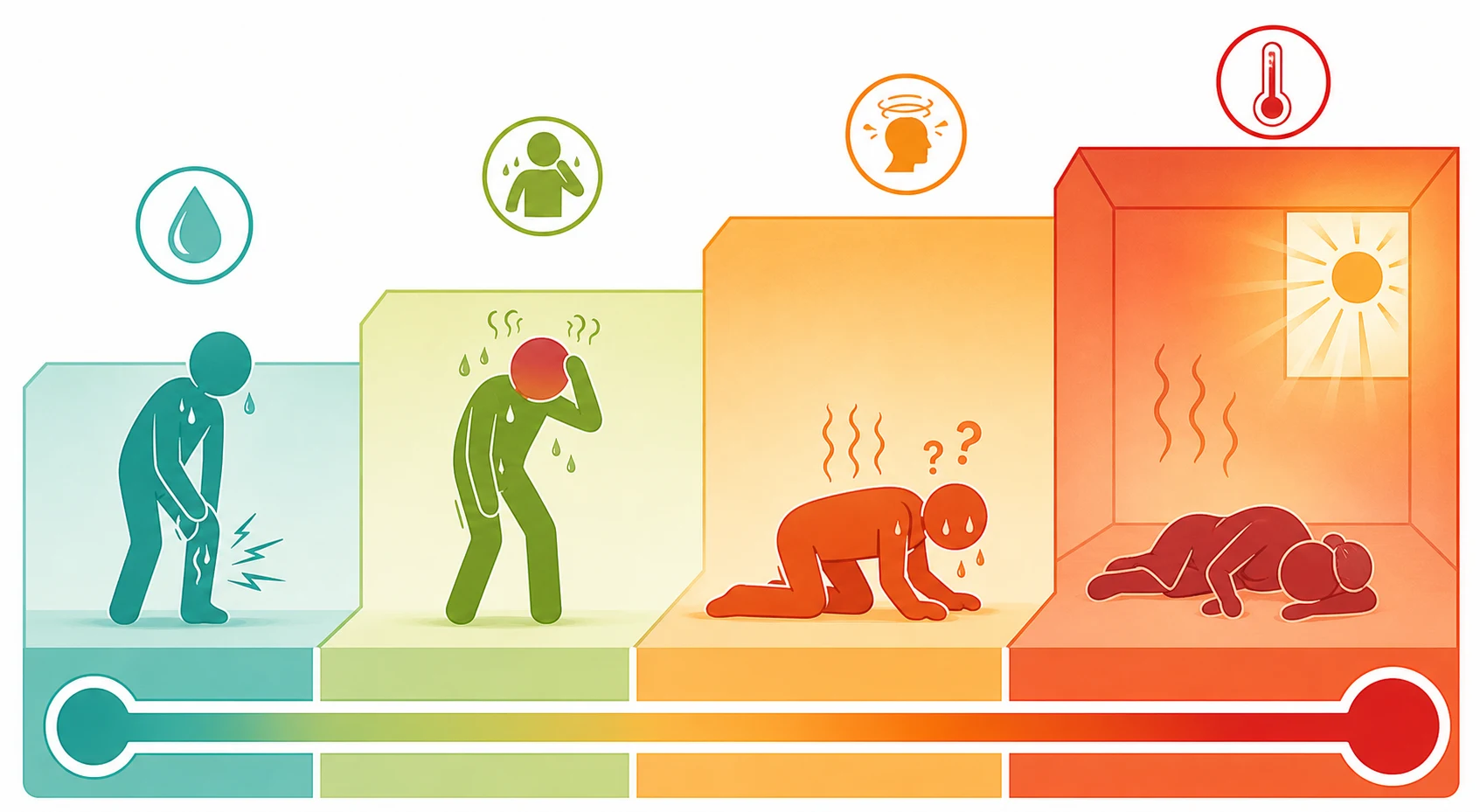
A teenager collapses mid-race on a forty-degree summer afternoon and is carried in hot, confused and sweating; a toddler is found cold and limp on a mountainside after a lost day in the wet; a school group returns from a high-altitude trek and one child has a headache and cannot walk a straight line. These are the three faces of the environmental-thermal emergency, and the decisions in the first minutes decide survival and the brain. Heat illness is the spectrum that runs from heat cramps through heat exhaustion to heat stroke, and heat stroke is defined as a core temperature over forty degrees Celsius accompanied by central nervous system dysfunction — confusion, agitation, ataxia, seizure or coma. The central nervous system feature is the pivot, because a hot child who is alert has heat exhaustion and a hot child who is not has heat stroke. [1] [4]
The two heat-stroke subtypes behave very differently. Exertional heat stroke strikes the young, fit athlete or military recruit during intense exercise in heat, often with sweating still present and a rapid onset, and it carries an excellent prognosis if cooled fast. Classic, non-exertional heat stroke strikes the elderly, the very young and the chronically ill during a heatwave without exercise, often with hot dry skin from anhidrosis, and it carries a high mortality driven by comorbidity and delayed presentation. The same temperature threshold and the same cooling principle apply to both, but the patient and the system differ. [2] [3]
Accidental hypothermia is an unintended fall in core temperature below thirty-five degrees from environmental cold exposure, and it is staged by the Swiss I to IV classification, which pairs the core temperature with the clinical state so that a rescuer can stage a child in the field. This leaf owns non-submersion environmental hypothermia — the child lost in the cold, the neonate in a cold room, the altitude trekker; the drowned hypothermic child is managed with the rescue-breath-first sequence in the sibling submersion leaf, and the rewarming ladder and the hypothermic-arrest rules are shared across both. [5] [6]
Around these two thermal extremes sit the environmental emergencies: acute altitude illness and its life-threatening cerebral and pulmonary forms, lightning injury, and electrical injury. Each has a single dominant treatment — descent for altitude, resuscitation for lightning, source removal and monitoring for electricity — and each rewards the clinician who knows the underlying physiology rather than reaching for a drug. This topic covers all three pillars to the depth a fellowship candidate must defend at viva. [8] [11]
Classification
Heat illness is classified by severity because each step changes both the treatment and the disposition. The spectrum begins with heat cramps, the brief, painful, involuntary muscle spasms that arise during or after intense exercise in heat from salt and water loss, and it climbs to heat exhaustion, in which the core temperature is elevated but under forty degrees and the child is sweaty, tachycardic, headachy and nauseated but mentally intact. Heat stroke is the threshold beyond which the central nervous system fails — a core over forty degrees with confusion, seizure or coma — and from that point the disease is one of multi-organ injury, not thermometry alone. [3] [4]
The two heat-stroke subtypes are then separated by the patient and the trigger. The same definition — core over forty degrees with central nervous system dysfunction — covers both, but the exertional form occurs in the young athlete during exercise with sweating often preserved, while the classic form occurs in the elderly or very young during a heatwave without exertion and often with anhidrosis and a high mortality. The staging of the two together is heat stroke, and the cooling ladder is identical. [1] [3]
The hypothermia axis is classified by the Swiss staging, which uses the core temperature and the clinical state so that a rescuer can stage a child in the field without relying on a thermometer alone. Stage one is mild, thirty-five to thirty-two degrees, with a clear conscious level and shivering. Stage two is moderate, thirty-two to twenty-eight degrees, with impaired consciousness. Stage three is severe, twenty-eight to twenty-four degrees, with unconsciousness but vital signs still present. Stage four is profound, below twenty-four degrees, with no detectable vital signs and a high risk of cardiac arrest. The stage sets the rewarming strategy, and in arrest it sets the defibrillation and drug rules. [5] [7]
Hypothermia severity by Swiss stage
- Core 35 to 32 degrees Celsius
- Clear consciousness, shivering
- Passive rewarming
- Low arrhythmia risk
- Core 32 to 28 degrees
- Impaired or altered consciousness
- Active external rewarming
- Arrhythmia risk rising
- Core 28 to 24 degrees
- Unconscious, vital signs present
- Active internal rewarming
- High arrhythmia risk, move gently
- Core below 24 degrees
- No vital signs, cardiac arrest risk
- Extracorporeal rewarming
- Nobody dead until warm and dead
Epidemiology & Risk Factors
Heat illness is a global and growing child-health problem, and heatwaves concentrate death in the most vulnerable. Classic non-exertional heat stroke rises sharply during heatwaves and kills the elderly and the very young disproportionately, while exertional heat stroke is one of the leading causes of sudden death in young athletes and military recruits. The risk is amplified by anything that impairs heat loss — anticholinergic and antipsychotic drugs, stimulants, beta-blockers and diuretics — and by conditions that reduce sweating, such as anhydrotic ectodermal dysplasia and cystic fibrosis, or that increase heat production, such as fever, obesity and exertion in heavy equipment. [2] [4]
The young child is uniquely vulnerable to both ends of the thermal spectrum for a single physiological reason. An infant has a high surface-area-to-mass ratio, a small metabolic reserve and a limited ability to sweat, redistribute blood or escape the environment, so an infant heats and cools faster than an adult. This is why a child left in a closed car in the sun reaches a fatal core temperature within minutes, why the neonate in a cold room becomes hypothermic quickly, and why the paediatric thresholds for both heat and cold exposure are lower than the adult. [2] [5]
Acute altitude illness affects children and adolescents who ascend faster than they acclimatise, typically above two thousand five hundred metres, with a risk that rises with the altitude reached, the speed of ascent and a previous history of altitude illness. Lightning and electrical injury in children cluster around outdoor sport, water recreation, metal structures and the temptation to shelter under trees in a storm, and the risk falls sharply with simple public-health measures — seeking proper shelter, avoiding water and metal, and staying indoors during the warning period. [8] [11]
Pathophysiology
To treat an environmental-thermal emergency you must hold the heat-balance equation in mind. The body's core temperature is set by the balance of heat production from metabolism and muscle, heat gained from the environment, and heat lost through radiation, convection, conduction and the evaporation of sweat, all of which the hypothalamus tunes by sweating and cutaneous vasodilation. Heat illness is what happens when the environmental heat load overwhelms those mechanisms, the core rises, and the protective systems themselves fail. [2] [4]
Heat stroke is not a set-point problem, and this is the single most important physiological point for the exam. In fever the hypothalamus has reset its target upward and antipyretics work by lowering that target, but in heat stroke the set point is normal and the body is simply losing its battle against an external heat load, so paracetamol and non-steroidal anti-inflammatory drugs do not lower the temperature and add no benefit — and paracetamol can compound the liver injury that heat stroke already causes. The definitive treatment is to remove the heat load and cool the body by physical means. Dantrolene, the specific therapy for malignant hyperthermia, has not been shown to improve outcome in heat stroke and is not recommended. [1] [3]
The injury in heat stroke is multi-organ and it is driven by the duration of the temperature above forty degrees as much as by the peak. Direct thermal damage to cells, gut-barrier breakdown with endotoxin translocation, a full systemic inflammatory response, and disseminated intravascular coagulation together injure the brain, the liver, the kidneys and the muscle, producing encephalopathy, acute liver injury, acute kidney injury and rhabdomyolysis. This is why the duration above forty degrees, and therefore the speed of cooling, is the chief determinant of survival. [1] [2]
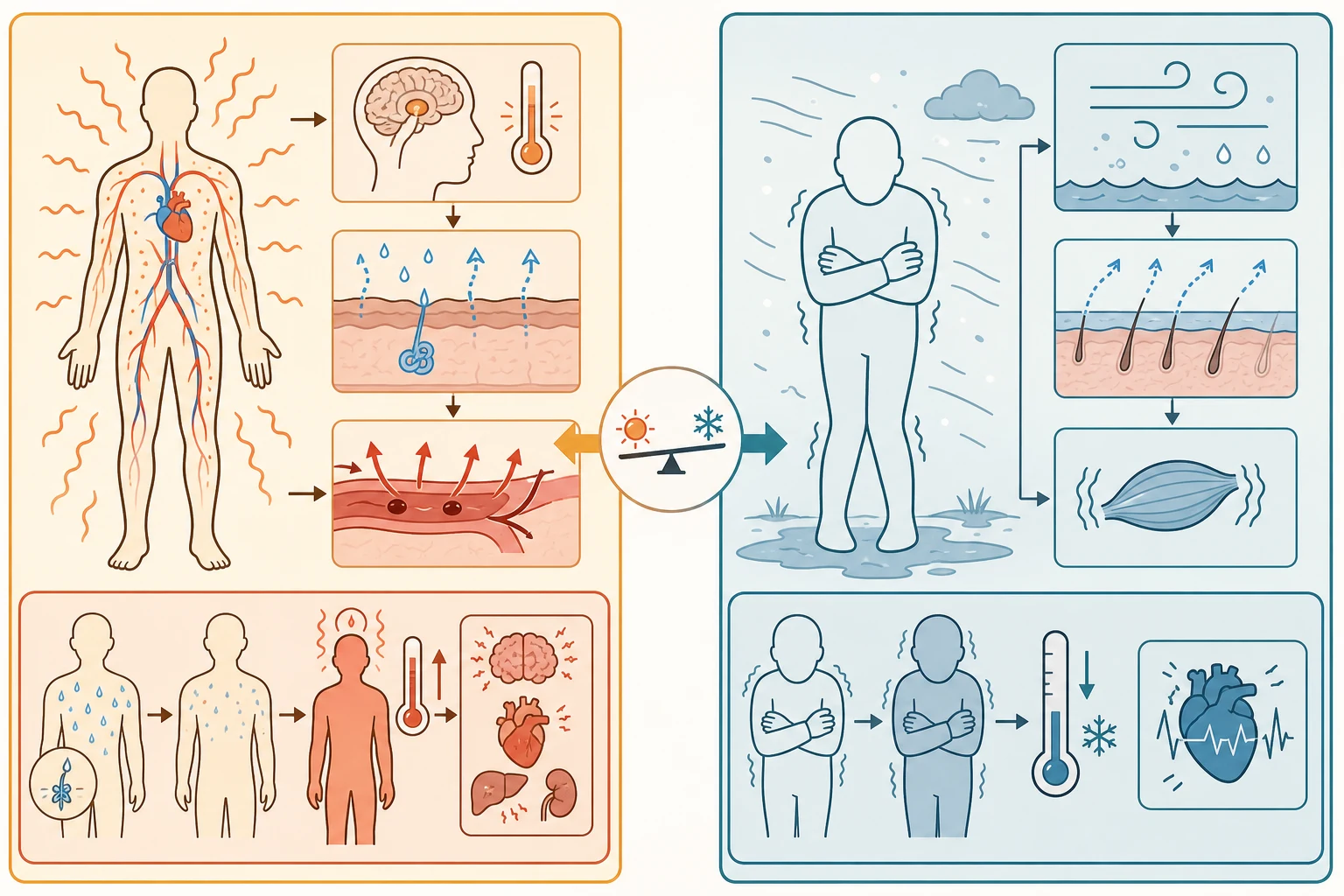
At the cold end, the infant loses heat rapidly because of the surface-area-to-mass ratio, and the neonate responds to cold with non-shivering thermogenesis in brown fat rather than shivering, a mechanism that exhausts quickly and deepens hypoxia. As the core temperature falls in any child, conduction slows, the PR and QT intervals lengthen, and the risk of ventricular arrhythmia rises sharply below thirty degrees. The cold myocardium is electrically irritable, which is why a jarring movement or rough handling can precipitate ventricular fibrillation — the practical rule that a cold child is moved gently. [5] [7]
Altitude illness is the consequence of hypobaric hypoxia: the inspired oxygen falls as the partial pressure of oxygen drops with altitude, and the body's responses — cerebral vasodilation and a rise in cerebral blood flow, and hypoxic pulmonary vasoconstriction — explain both the headache of acute mountain sickness and the brain and lung injury of the severe forms. High-altitude cerebral oedema is vasogenic oedema from a breakdown of the blood-brain barrier under hypoxic stress, and high-altitude pulmonary oedema is a non-cardiogenic oedema from uneven hypoxic pulmonary vasoconstriction that over-perfuses some capillaries and leaks fluid into the alveoli. [8] [9]
Clinical Presentation
The heat-exhaustioned child is hot, sweaty, tachycardic, headachy and nauseated, with a flushed skin and a core temperature that is elevated but under forty degrees, and the defining feature is that the mental state is intact. The child with heat stroke looks similar but the brain has failed: there is confusion, agitation, ataxia, a seizure, or a depressed conscious level, with a core temperature over forty degrees. The skin may be hot and dry in classic heat stroke from anhidrosis, but in exertional heat stroke sweating is often still present and profuse, so the absence of sweating must not be used to exclude heat stroke. The mental state, not the sweat, is the pivot. [1] [4]
At altitude the child develops a headache within six to twelve hours of ascent, typically above two thousand five hundred metres, accompanied by one or more of gastrointestinal upset, fatigue or weakness, and dizziness — the picture of acute mountain sickness captured by the 2018 Lake Louise score. The danger signs are new ataxia, which means high-altitude cerebral oedema until proven otherwise, and dyspnoea at rest with a cough and falling oxygen saturation, which mean high-altitude pulmonary oedema. Either is an emergency that demands immediate descent. [8] [10]
The lightning- or electrical-injured child may present in cardiac arrest, with a primary arrhythmia from the current, or with the cutaneous and systemic signs of the strike. Lightning can produce Lichtenberg figures — the transient fern-like skin pattern that is near-pathognomonic — tympanic membrane rupture, fixed and dilated pupils that are not a prognostic sign here, burns at the entry and exit points, and blunt injury from the blast or a fall. Electrical injury shows entry and exit wounds that are often small on the surface but conceal deep tissue damage, and it may present with an arrhythmia, a fracture, or rhabdomyolysis hours later. [11] [12]
A frequent trap is the well-looking child at the threshold. The athlete who collapses and then recovers quickly may still have had heat stroke and need cooling and observation, because the multi-organ injury can evolve over hours. The cold child who is found after paradoxical undressing — the dangerous phenomenon in which a profoundly hypothermic person feels hot and undresses — may be misjudged as intoxicated or assaulted, and the neonate with hypothermia may simply be feeding poorly and cold to touch. Each demands the structured thermal assessment before a disposition is made. [1] [6]
Differential Diagnosis
The differential of hyperthermia is the one an examiner probes hardest, because several conditions mimic heat stroke but need a different treatment. The first is sepsis, which can present with a high fever and encephalopathy in a hot child and which must be sought and treated with antibiotics alongside cooling. The second is thyroid storm, with its hyperadrenergic state, and the third is the group of drug-induced hyperthermias: malignant hyperthermia from volatile anaesthetics or succinylcholine, which responds to dantrolene; neuroleptic malignant syndrome from antipsychotics; serotonin syndrome from serotonergic drugs; and anticholinergic and sympathomimetic toxicity. [1] [4]
The hyperthermia differential — what distinguishes each from heat stroke
- Hot environment or exertion
- Core over 40 degrees
- Central nervous system dysfunction
- Antipyretics do not work; cool physically
- Volatile anaesthetic or succinylcholine trigger
- Hypercapnia, rigidity, hyperkalaemia
- Responds to dantrolene
- Set point normal
- Antipsychotic exposure, lead-pipe rigidity
- Days to weeks onset
- Bromocriptine, dantrolene
- Often slower and lower temperature
- Serotonergic drug, clonus, hyperreflexia
- Onset within a day
- Cyproheptadine, stop the agent
- Autonomic instability
The key to separating these is the history and the physical: a trigger for malignant hyperthermia, the rigidity and clonus of the drug-induced syndromes, and the environmental heat load of heat stroke. In practice a collapsed, hyperthermic child receives simultaneous cooling and a workup for sepsis and these mimics, because delay is dangerous and the conditions overlap. The cold child carries a different differential — hypoglycaemia, sepsis, intoxication, traumatic brain injury and endocrine failure all depress the conscious state and the temperature, and each is sought and corrected alongside rewarming. [1] [6]
At altitude, the differential of high-altitude cerebral oedema includes any cause of encephalopathy or a space-occupying lesion, and the differential of high-altitude pulmonary oedema includes pneumonia, asthma and a pulmonary embolus. After a lightning or electrical injury, the differential includes a primary cardiac event that presented outdoors and a simple fall — but the rule is to treat the environmental mechanism first, resuscitate aggressively, and seek the occult deep and cardiac injury. [8] [11]
Clinical & Bedside Assessment
The assessment of the collapsed environmental-thermal child runs inside the airway-breathing-circulation-disability-exposure framework, with two additions that the emergency demands. The first is a rectal core temperature at the first opportunity, because oral, tympanic and forehead measures are unreliable in heat stroke and in hypothermia, and a standard thermometer stops at thirty-four degrees and misses profound hypothermia. The second is a deliberate disability assessment — the Glasgow Coma Scale or AVPU — because the mental state is the pivot that separates heat exhaustion from heat stroke, and the ataxia test is the sign that separates acute mountain sickness from high-altitude cerebral oedema. [3] [5]
For the overheated child, remove from the heat, remove the clothing, secure the airway and give oxygen, establish intravenous access, and begin cooling immediately, before any investigation. Assess the conscious level, the hydration, the skin (hot and dry versus sweaty), and look for the features that point to a mimic — the rigidity of malignant hyperthermia, the clonus of serotonin syndrome, the lead-pipe rigidity of neuroleptic malignant syndrome. Check the glucose, because hypoglycaemia complicates both heat and cold and is easy to correct. [1] [4]
The overheated child — the first ten minutes
For the cold child, the assessment sets the Swiss stage by the core temperature and the clinical state — conscious and shivering for stage one, impaired for two, unconscious with vital signs for three, no vital signs for four — and this staging decides the rewarming. Handle the child gently throughout, because a jarring movement can precipitate ventricular fibrillation in the cold myocardium. After a lightning or electrical injury, examine the skin for entry and exit wounds and Lichtenberg figures, the ears for tympanic membrane rupture, the heart for an arrhythmia, and the limbs for compartment syndrome as the deep muscle injury evolves. [5] [11]
Investigations
Investigations in heat illness serve the search for multi-organ injury and for the mimics, and they never delay cooling. The core temperature confirms the diagnosis, a creatine kinase measures the rhabdomyolysis, liver function tests reveal the acute liver injury, a coagulation profile detects the disseminated intravascular coagulation, urea and electrolytes and a creatinine quantify the acute kidney injury, and a glucose and a blood gas define the metabolic state. A full blood count, a lactate and a septic screen are sent to separate sepsis, and a toxicology and drug history is sought for the drug-induced hyperthermias. [1] [2]
In hypothermia the low-reading core thermometer is mandatory, because a standard probe stops at thirty-four degrees and will report a profoundly hypothermic child as thirty-four. A blood gas and electrolytes quantify the metabolic acidosis and the electrolyte shifts, the glucose is checked because hypoglycaemia is common and correctable, and a coagulation profile and a full blood count round out the search for the complications. A chest radiograph looks for aspiration or pulmonary oedema, and a twelve-lead electrocardiogram, once the child is stable, shows the prolonged PR and QT and the Osborne J wave that characterise moderate and severe hypothermia. [5] [6]
At altitude, the oxygen saturation and the chest radiograph support the diagnosis of high-altitude pulmonary oedema where available, and a low saturations reading with a cough and dyspnoea at rest is enough to act. After an electrical injury, an electrocardiogram is taken on presentation and cardiac monitoring is continued, because a high-voltage exposure, a loss of consciousness, an arrhythmia or electrocardiographic changes all justify a period of monitoring for a late arrhythmia. Computed tomography of the brain is reserved for the confused child whose conscious state does not resolve with cooling or rewarming, to exclude an intracranial event. [8] [12]
Management — Resuscitation
The first act in heat stroke is to remove the heat load and begin cooling immediately, because the duration above forty degrees is the chief determinant of survival. Remove the child from the heat, remove the clothing, secure the airway and give oxygen, establish intravenous access, check and treat the glucose, and start cooling before any investigation is sent — the bloods are taken while the child is cooled, not before. Aggressive fluid resuscitation is guided by perfusion and by the haemodynamic state, because the heat-stroke child is hypovolaemic from sweating and vasodilation, but over-resuscitation is avoided in the failing lung. [1] [3]
Cold-water immersion (exertional heat stroke)
Dose
Immerse the body in cold or ice water at approximately 2 to 15 degrees, with the airway protected, until the core falls below 39 degrees Celsius
Where cold-water immersion is unavailable, the alternatives are evaporative cooling — tepid water sprayed over the skin with warm air fanned across it, which works well in dry heat — ice packs to the neck, groin and axillae, cooled intravenous fluid at around four degrees, and cooling blankets. Cooling is continued until the core reaches thirty-nine degrees, after which the child is observed for rebound hyperthermia and for the evolving multi-organ injury. Antipyretics are not given, because they do not work in heat stroke and paracetamol may add to the liver injury; dantrolene is not recommended. [3] [4]
For the cold child, the immediate measures are to remove the child from the cold, remove wet clothing, dry the skin, insulate with warm dry blankets including the head, and handle gently to avoid precipitating ventricular fibrillation. Establish intravenous or intraosseous access, give warmed fluid for hypovolaemia, check and treat the glucose, and measure a low-reading core temperature to set the rewarming strategy. In the hypothermic arrest, the core temperature directs the resuscitation, and the rules for defibrillation and drugs change below thirty degrees. [5] [7]
The first ten minutes for the collapsed environmental-thermal child
Remove the heat or the cold; remove clothing; airway, breathing, circulation
Oxygen and intravenous access; check and treat the glucose
Rectal or low-reading core temperature — never oral or tympanic
Heat stroke: begin cold-water immersion or evaporative cooling now; cool to below 39 degrees
Hypothermia: stage Swiss I to IV; dry, insulate, handle gently; begin matching rewarming
Altitude: assess for ataxia and dyspnoea at rest; prepare for immediate descent if either is present
Management — Definitive & Stepwise
The definitive management of heat stroke is rapid cooling to below thirty-nine degrees, followed by multi-organ support in an intensive care unit. Once cooled, the child is monitored for the encephalopathy, the rhabdomyolysis and the acute kidney and liver injury, and for the disseminated intravascular coagulation. The rhabdomyolysis is treated with intravenous fluid to maintain a urine output and to protect the kidney, and the failing organ receives its standard support. Early liaison with retrieval and intensive care is arranged for the multi-organ child, and the family is told honestly about the prognosis and the uncertainty of the first days. [1] [2]
The definitive management of accidental hypothermia branches on the Swiss stage, because the stage sets the rewarming ladder. For mild hypothermia, Swiss stage one, passive rewarming suffices: the child is conscious and shivering, so remove the wet clothing, insulate with blankets in a warm environment, and allow endogenous heat production to do the work, checking that the core rises steadily. For moderate, stage two, add active external rewarming with forced warm air at thirty-eight to forty-two degrees over the trunk, which is effective while the child still has a perfusing rhythm. [5]
Forced warm air rewarming (active external)
Dose
Forced warm air blanket at 38 to 42 degrees Celsius applied to the trunk
For severe, stage three, active internal rewarming is added: warmed humidified oxygen at forty-two to forty-six degrees, warmed intravenous crystalloid at around forty degrees, and consideration of body cavity lavage, while monitoring for rewarming shock and the afterdrop. For profound, stage four — the cold, pulseless child — the treatment is extracorporeal rewarming, because extracorporeal membrane oxygenation or cardiopulmonary bypass rewarms fastest, supports the circulation, and carries the best survival in hypothermic cardiac arrest. This shared ladder and the hypothermic-arrest rules are identical to those for the drowned hypothermic child in the sibling submersion leaf. [5] [7]
Warmed intravenous crystalloid (hypothermia)
Dose
0.9 per cent saline warmed to approximately 40 degrees Celsius, 10 to 20 mL per kilogram boluses titrated to perfusion

The hypothermic cardiac arrest has its own rules, and these are high-yield for the exam. Continue high-quality cardiopulmonary resuscitation without interruption, because prolonged resuscitation can succeed and the maxim holds that nobody is dead until they are warm and dead. If the rhythm is ventricular fibrillation and the core is below thirty degrees, deliver a single shock at the standard energy and, if it fails, withhold further shocks and resuscitation drugs until the core rises above thirty degrees, because the cold myocardium is refractory to both. Once above thirty degrees, resume standard shocks and drugs, but lengthen the interval between adrenaline doses because drug clearance is slowed, and escalate to extracorporeal rewarming as early as the system allows. [7]
The definitive management of acute altitude illness is descent, and the amount of descent depends on the severity. For acute mountain sickness, stop the ascent, rest, hydrate, give simple analgesia and antiemetics, and consider acetazolamide; the child improves over a day or two and may then ascend slowly. For high-altitude cerebral oedema and high-altitude pulmonary oedema, immediate descent is the definitive treatment, supplemented by oxygen, dexamethasone for the cerebral form, and nifedipine for the pulmonary form, with a portable hyperbaric chamber as a bridge where descent is delayed. [8] [9]
Acetazolamide (altitude illness)
Dose
Adults and older children 125 mg twice daily for prophylaxis or 250 mg twice daily for treatment; paediatric 2.5 mg per kilogram every 12 hours up to 250 mg per dose
The descent and drug rules for the severe forms are taught as a pair, because they are examined together. For high-altitude cerebral oedema, descend immediately and give dexamethasone, an eight-milligram loading dose then four milligrams every six hours, alongside oxygen; acetazolamide is added. For high-altitude pulmonary oedema, descend immediately, give oxygen and sit the child up, and add nifedipine slow-release thirty milligrams every twelve hours, with a phosphodiesterase inhibitor such as tadalafil as an alternative; dexamethasone may be added if cerebral features coexist. Descent remains the definitive act; the drugs support but do not replace it. [8] [9]
After a lightning strike, the principle is to resuscitate the apparently dead first, because a lightning arrest is survivable with prolonged cardiopulmonary resuscitation. In a mass-casualty lightning event, reverse the usual triage: those who are breathing and moving will survive, and those in arrest are the priority for resuscitation, which may need to be prolonged because the respiratory arrest from medullary stunning can outlast a spontaneously re-started heart. After an electrical injury, remove the source safely, resuscitate as needed, monitor the heart, and look for the deep tissue injury, the rhabdomyolysis and the compartment syndrome that evolve over hours. [11] [12]
Specific Subtypes & Scenarios
Classic non-exertional heat stroke in the heatwave is the scenario that tests the system as much as the clinician. An infant or an elderly person in a closed, hot dwelling during a heatwave presents hot, confused and often dry from anhidrosis, and the mortality is high because of comorbidity and delayed presentation. The treatment is the same rapid cooling and multi-organ support, but the public-health arm — heatwave plans, cool shelters, checking on the vulnerable, and never leaving a child in a car — is what prevents the next case. [1] [4]
Paediatric vehicular heatstroke is the catastrophic end of the heat-illness spectrum that a fellowship candidate must be able to discuss. The interior of a closed car in the sun rises rapidly, and a child left inside reaches a fatal core temperature within minutes, because the high surface-area-to-mass ratio and the limited sweating of the small child offer no defence. Prevention is the entire answer — never leaving a child unattended in a car, placing a reminder in the back seat, and the technology and public-education that the American Academy of Pediatrics and others advocate — and the child who is recovered is treated as any heat stroke, with rapid cooling. [2] [4]
The neonate and small child with environmental hypothermia is the cold counterpart. The neonate in a cold room or after a prolonged delivery becomes hypothermic quickly through a high surface-area-to-mass ratio and a limited metabolic reserve, and it responds to cold with non-shivering thermogenesis that exhausts and deepens hypoxia. Moderate and severe neonatal hypothermia are warmed actively with skin-to-skin contact, a radiant warmer and warmed humidity, and the rewarming is gentle and monitored for the afterdrop; the cold larger child is managed on the same Swiss staging and rewarming ladder as the adult, with doses scaled to weight. [5] [6]
In Australia and New Zealand, follow the ANZCOR Guideline 9.3.3 on hypothermia for the first aid and medical treatment of the cold child, with passive and active external rewarming for the milder stages and escalation to a retrieval and an extracorporeal service for the profound and arrested. The Royal Children's Hospital Melbourne clinical practice guidelines are the regional bedside reference for heat illness and environmental emergencies, and heatwave planning and hot-car prevention are coordinated with the state public-health authorities.
[5][6]Complications & Pitfalls
The commonest preventable failure in heat stroke is delayed cooling. A team that waits for bloods, for a transfer, or for a definitive core temperature before starting to cool has misread the disease — the duration above forty degrees is the chief determinant of survival, and the child is cooled from the moment of recognition. The second failure is giving antipyretics or dantrolene, which do not work in heat stroke, add no benefit, and with paracetamol may compound the liver injury; the definitive treatment is physical cooling. [1] [3]
In hypothermia the dangerous errors cluster around handling and the defibrillation rules. Rough handling, jarring transport, or sudden movement can precipitate ventricular fibrillation in the cold myocardium, which is why the child is moved gently and never roughly. Repeated shocks and escalating drug doses below thirty degrees are ineffective and divert effort from rewarming — the correct move is one shock, then rewarm. The afterdrop — a further fall in core temperature after rewarming begins — and rewarming shock from vasodilation must be anticipated with warmed fluids and continued monitoring. [5] [7]
At altitude, the lethal error is ascending with symptoms. A child with acute mountain sickness who ascends can progress to high-altitude cerebral or pulmonary oedema, and a child with ataxia or dyspnoea at rest has already crossed into the severe form and must descend immediately. After a lightning or electrical injury, the errors are the premature cessation of resuscitation in a survivable lightning arrest, and the under-recognition of the deep tissue and the cardiac injury that evolve after the burn. [8] [11]
Prognosis & Disposition
Outcome after heat stroke is driven by the duration above forty degrees, the speed of cooling, and the presence of multi-organ failure. Exertional heat stroke carries an excellent prognosis when cooled to below thirty-nine degrees within thirty minutes — survival approaches one hundred per cent — while classic heat stroke in the elderly and the chronically ill carries a high mortality driven by comorbidity and delayed presentation. The child is admitted to a paediatric intensive care unit for the multi-organ support, and the family is told honestly about the prognosis and the uncertainty of the first days. [1] [3]
National Athletic Trainers' Association exertional heat illness position statement (Casa 2015)
Population: Athletes and active populations at risk of exertional heat illness, from cramps to exertional heat stroke
Key finding
Cool-first-transport-second with cold-water immersion gives near-complete survival in exertional heat stroke when cooling is begun promptly
Practice change
Rapid recognition and immediate cold-water immersion are the standard of care; survival is determined by the speed of cooling, not by transport
Outcome after accidental hypothermia depends on the depth and the cause, with the cold-water exception that overturns the usual poor factors: a profoundly hypothermic child can recover intact after a prolonged arrest, provided the water was cold and the rewarming is carried through to a core of at least thirty-two degrees. The child is admitted for the rewarming and the multi-organ support, and retrieval to a centre with extracorporeal capability is arranged early for the cold, arrested child. Altitude illness resolves with descent and oxygen, and the lightning- and electrical-injured child is monitored for the late cardiac and soft-tissue complications. [5] [8]
Special Populations
Infants and small children are the population most vulnerable to both ends of the thermal spectrum, through the high surface-area-to-mass ratio and the limited thermoregulatory reserve, and they are protected by anticipatory guidance — never in a hot car, dressed for the cold, and supervised around water and altitude. Children with anhydrotic ectodermal dysplasia, cystic fibrosis, obesity, cardiac disease and those on anticholinergic, antipsychotic, stimulant or diuretic drugs have impaired heat tolerance and need an individualised heat plan, with restricted exertion in heat, early cooling and hydration. [2] [4]
Aboriginal, Torres Strait Islander, Maori, Pacific and remote-community children carry a disproportionate burden from environmental-thermal emergencies tied to housing, remote exposure and reduced access to cooling and warming, and these children are reached by community-led heatwave and cold-weather planning and by retrieval services rather than by emergency care alone. The pregnant adolescent adds the physiology of pregnancy and the need to manage both mother and fetus, and the child with a complex chronic condition tolerates both heat and cold poorly and needs an individualised environmental plan. [1] [5]
In rural and remote settings the irreducible core is bystander recognition, early contact with a retrieval service, gentle handling, and insulation, cooling or rewarming begun at the scene, because the tertiary centre and the extracorporeal service may be hours away. Telehealth-supported resuscitation and dispatcher coaching extend the reach of the algorithms, and a generalist who can cool a heat stroke, stage and rewarm a hypothermia, recognise the need for altitude descent, and resuscitate a lightning arrest until retrieval arrives is the pivot of the whole system. [3] [11]
Evidence, Guidelines & Regional Differences
The current standard rests on the Bouchama 2002 and Leon 2015 heat-stroke reviews, the Casa 2015 National Athletic Trainers' Association position statement on exertional heat illness, the Gauer 2026 review, the Brown 2012 and Darocha 2026 accidental hypothermia reviews, the European Resuscitation Council 2021 cardiac arrest in special circumstances guideline, the Luks 2024 Wilderness Medical Society altitude illness guideline and the 2008 medication and dosage paper, the Roach 2018 Lake Louise score, the Davis 2014 Wilderness Medical Society lightning injury guideline, and the Koumbourlis 2002 electrical injuries review. These agree on the fundamentals: the heat-stroke definition and cooling ladder, the Swiss staging and rewarming ladder, the descent-first altitude rule with the drug doses, the lightning reverse-triage principle, and the electrical-injury monitoring rule. [1] [8]
The first hours of an environmental-thermal emergency
Where the evidence is maturing, answer with the current guideline and name the source. The role of extracorporeal rewarming is expanding as access grows, the optimal cooling method beyond cold-water immersion is still refined, and the pharmacological prevention of altitude illness continues to be studied — but the descent-first rule and the cooling-first rule are stable and defensible. Routine therapeutic hypothermia after paediatric cardiac arrest is not supported by the THAPCA trials, so the standard is normothermia and avoidance of fever, with rewarming reserved for the genuinely hypothermic child. [5] [7]
Exam Pearls
- Heat stroke is a core temperature above forty degrees Celsius with central nervous system dysfunction; the mental state, not the sweat, is the pivot that separates exhaustion from stroke. [1]
- Cool exertional heat stroke first and transport second — cold-water immersion to a core below thirty-nine degrees within thirty minutes gives near-complete survival. [3]
- Antipyretics and dantrolene do not work in heat stroke; the hypothalamic set point is normal and the problem is environmental heat load. [1]
- Classic non-exertional heat stroke strikes the elderly and very young in a heatwave, often with hot dry skin; exertional heat stroke strikes the athlete in exercise, often still sweating. [2]
- Stage hypothermia by Swiss stages: stage one thirty-five to thirty-two degrees (conscious, shivering), stage two thirty-two to twenty-eight, stage three twenty-eight to twenty-four, stage four below twenty-four. [5]
- Rewarm passively for stage one, forced warm air at thirty-eight to forty-two degrees for stage two, active internal warmed oxygen and fluids for stage three, extracorporeal for stage four. [5]
- In hypothermic arrest, continue CPR, give one shock for ventricular fibrillation below thirty degrees, then withhold shocks and adrenaline until above thirty degrees; continue until the core is at least thirty-two degrees — nobody is dead until warm and dead. [7]
- Lake Louise 2018: a headache plus one or more of gastrointestinal upset, fatigue or dizziness after recent ascent above two thousand five hundred metres; ataxia means high-altitude cerebral oedema until proven otherwise. [10]
- Descent is the definitive treatment of high-altitude cerebral and pulmonary oedema; add dexamethasone for the cerebral, oxygen and nifedipine for the pulmonary, and acetazolamide for acute mountain sickness and prophylaxis. [8]
- Acetazolamide prophylaxis one hundred and twenty-five milligrams twice daily (paediatric two point five milligrams per kilogram every twelve hours); dexamethasone for cerebral oedema eight milligrams then four every six hours; nifedipine for pulmonary oedema thirty milligrams slow-release every twelve hours. [9]
- Lightning mass casualty: reverse triage — resuscitate the apparently dead first, because lightning arrest is survivable with prolonged cardiopulmonary resuscitation. [11]
- Electrical injury: monitor the heart, expect deep tissue injury disproportionate to the skin, and anticipate rhabdomyolysis and compartment syndrome. [12]
References
- [1]Bouchama A Heat stroke. N Engl J Med, 2002.PMID 12075060
- [2]Leon LR Heat stroke. Compr Physiol, 2015.PMID 25880507
- [3]Casa DJ National Athletic Trainers' Association Position Statement: Exertional Heat Illnesses. J Athl Train, 2015.PMID 26381473
- [4]Gauer RL Heat-Related Illnesses. Am Fam Physician, 2026.PMID 42101601
- [5]Brown DJ Accidental hypothermia. N Engl J Med, 2012.PMID 23150960
- [6]Darocha T Accidental hypothermia. Nat Rev Dis Primers, 2026.PMID 42393082
- [7]Lott C European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation, 2021.PMID 33773826
- [8]Luks AM Wilderness Medical Society Clinical Practice Guidelines for the Prevention, Diagnosis, and Treatment of Acute Altitude Illness: 2024 Update. Wilderness Environ Med, 2024.PMID 37833187
- [9]Luks AM Medication and dosage considerations in the prophylaxis and treatment of high-altitude illness. Chest, 2008.PMID 18321903
- [10]Roach RC The 2018 Lake Louise Acute Mountain Sickness Score. High Alt Med Biol, 2018.PMID 29583031
- [11]Davis C Wilderness Medical Society practice guidelines for the prevention and treatment of lightning injuries: 2014 update. Wilderness Environ Med, 2014.PMID 25498265
- [12]Koumbourlis AC Electrical injuries. Crit Care Med, 2002.PMID 12528784