Paeds · acute-care-resuscitation-and-toxicology
Humane restraint and behavioural support in emergency care
Also known as Acute behavioural disturbance in children · Paediatric agitation management · Rapid tranquillisation in children · De-escalation in the emergency department · Physical restraint of children · Chemical restraint in paediatric emergency care
A fellowship approach to the child or young person with acute behavioural disturbance in the emergency department. Run a primary survey and treat medical causes first, lead verbal de-escalation and environmental modification, offer oral medication with consent before any injection, escalate to parenteral rapid tranquillisation only when oral fails or is unsafe, reserve physical restraint for grave and imminent danger with minimum force and minimum duration by a trained team, monitor every sedated child for respiratory depression, QTc prolongation and oversedation, and debrief the child, family and team afterwards.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Acute behavioural disturbance is what you see at the bedside before you know why: a child or young person whose behaviour has escalated to the point where they are a risk to themselves, to others, or to their own assessment and treatment. The presenting behaviour is pacing, shouting, threatening, throwing, self-harming, refusing, withdrawing, posturing or striking out. The job of the paediatric team in the emergency department is not to diagnose a psychiatric illness first; it is to keep everyone safe, find the drivers of the behaviour, settle the child by the least restrictive means that work, and only then hand on to mental health, paediatric, toxicology, developmental or safeguarding services as the cause demands. [1]
The defining frame is that acute behavioural disturbance is a behaviour, not a diagnosis. A wide range of medical, psychiatric, toxicological, developmental and situational drivers converge on the same final behaviour, and the differential is broadest at the moment the child arrives. This is why a calm, structured, least-restrictive approach that protects the brain and the airway while the cause is identified outperforms a reflex to sedate or restrain. [2] [3]
[1] [5]The clinical and ethical anchor is the least-restrictive principle: the intervention that is sufficient to keep the child and others safe, and no more. Autonomy is the default; restriction is the exception, justified each time by imminent risk of serious harm, carried out with minimum force and minimum duration, and reviewed continuously. Restraint and sedation without consent are governed by mental health, guardianship and child-protection legislation, which varies across Australian states and territories, Aotearoa New Zealand, the United Kingdom and North America. Know the forms and thresholds that apply in your jurisdiction before you need them. [1] [2]
Classification
Acute behavioural disturbance is classified along two axes that together drive the immediate response. The first axis is the severity of the agitation. The Behavioural Activity Rating Scale (BARS) is a seven-point bedside scale widely used in the agitation literature to grade severity and to mark response to intervention. A score of 1 is difficult to arouse (oversedated), 4 is the baseline, 5 is signs of overactivity with calming on request, 6 is acute overactivity not calming on request, and 7 is violent. A BARS of 6 to 7 is the threshold for considering parenteral medication if de-escalation fails; a BARS of 4 to 5 is the threshold for verbal de-escalation and oral medication. [1]
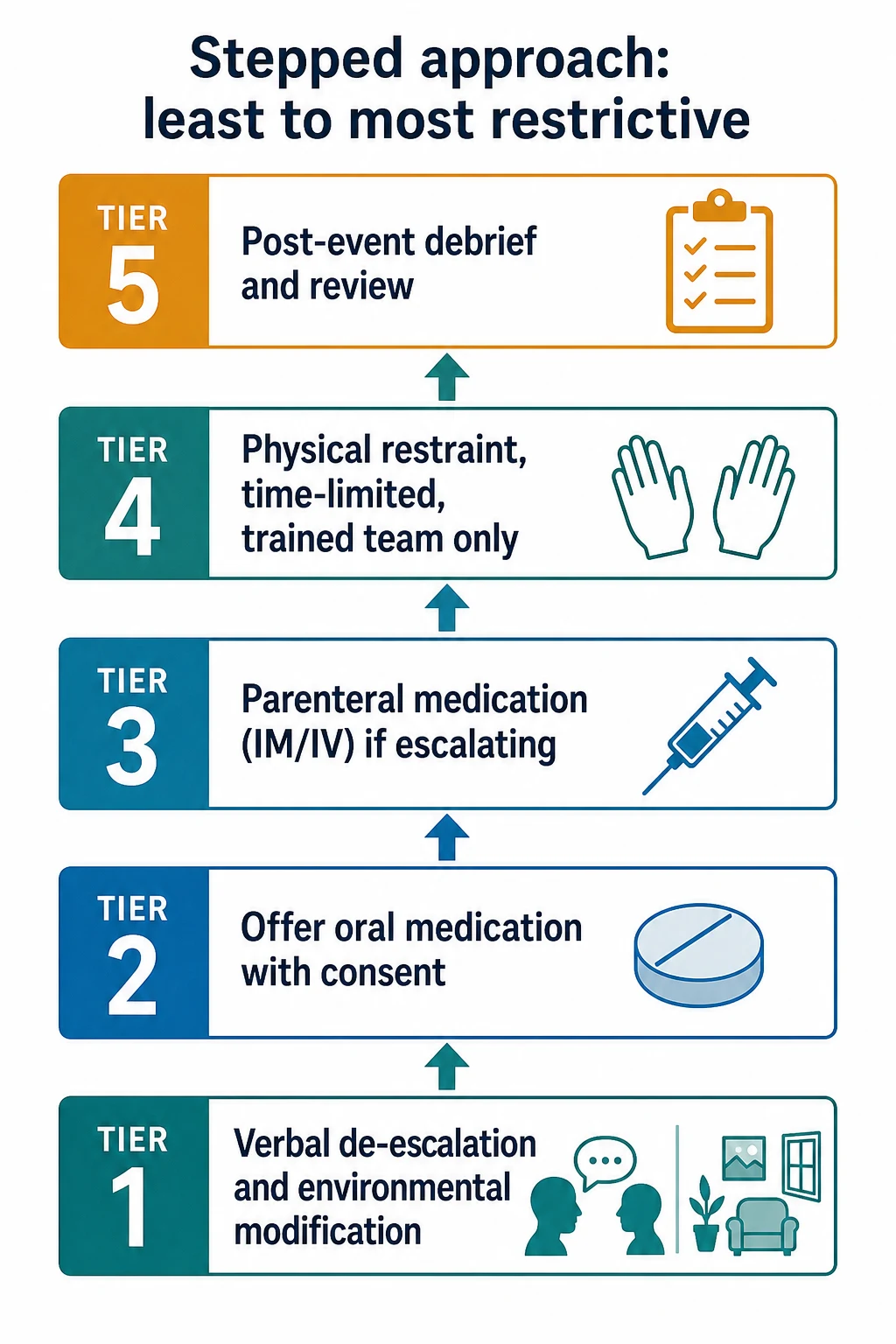
The second axis is the intervention ladder, ordered from least to most restrictive. The five tiers run from verbal and environmental de-escalation, through oral medication offered with consent, through parenteral rapid tranquillisation when oral is refused or unsafe, to physical restraint as a last resort when grave and imminent danger cannot be prevented any other way, with mandatory debrief and review at the apex. Movement up the ladder is triggered by failure of the lower step and by rising risk; movement back down is the goal of every intervention. [1] [1]
The boundaries between chemical restraint, rapid tranquillisation, procedural sedation and anaesthesia are worth naming precisely. Chemical restraint and rapid tranquillisation both describe the use of medication to settle acute agitation when de-escalation has failed; rapid tranquillisation usually implies parenteral administration for severe agitation. Procedural sedation is the use of medication to enable a necessary, planned procedure in a monitored child; it is not what is being done in acute behavioural disturbance. Anaesthesia is the loss of consciousness and protective reflexes required for surgery or intubation. Acute behavioural disturbance management aims for calming without loss of airway reflexes; the moment the child becomes unrousable, the situation has crossed into procedural sedation territory and the airway, breathing and circulation must be managed as such. [1] [5]
Epidemiology & Risk Factors
Paediatric mental health presentations to emergency departments have risen in volume and acuity across Australia, Aotearoa New Zealand, the United Kingdom and North America over the last decade, and acute behavioural disturbance is a growing share of those presentations. The epidemiology matters because it shapes the readiness of the department, the training of staff, and the lived experience of the child and family. Children with autism spectrum disorder and attention deficit hyperactivity disorder are over-represented in emergency mental health presentations and have a higher rate of agitation, restraint and adverse drug events than their neurotypical peers. [6]
The child factors that increase the risk of acute behavioural disturbance are well mapped: autism spectrum disorder, intellectual disability, attention deficit hyperactivity disorder, communication disorder, sensory processing disorder, acquired brain injury, neurodegeneration, a history of trauma, and a prior episode of restraint or seclusion. The situational and systemic factors that escalate agitation in the emergency department are equally important and more modifiable: long waits, bright fluorescent lighting, noise, overcrowding, the removal of a trusted adult, the use of clinical uniforms, language barriers, cultural dislocation, and prior adverse healthcare experiences. Recognising the situational drivers is a clinical act: it shifts the response from escalating the child to changing the environment. [1] [6]
Complex chronic illness and technology dependence change the baseline. A child with cerebral palsy, a genetic syndrome, an acquired brain injury or a neurodegenerative condition may have a baseline behaviour that looks disturbed to staff who do not know them, may communicate distress through behaviour rather than words, and may decompensate rapidly with the doses used in their neurotypical peers. Knowing the baseline is the first step in any plan. [6]
Aboriginal and Torres Strait Islander, Maori, refugee, asylum-seeking, out-of-home-care and youth-justice children experience restraint and sedation disproportionately. The reasons are structural and include intergenerational trauma, cultural dislocation, communication barriers, racism, and the criminalisation of distress. Cultural safety is a clinical safety issue here: a de-escalation plan that ignores culture will escalate rather than calm. Restrained children are over-represented among Indigenous youth in custody, and a restraint event in this group is both a clinical and a human-rights event. [7]
Restraint-related deaths in children and young people, while rare, share recurring features: positional asphyxia, hyperactive delirium with physiological collapse, aspiration, and cardiac arrest in the context of intoxication or medical illness. These features drive every operational rule that follows: the airway is visible and protected at all times, no face-down or hobble restraint, vital signs are monitored continuously during restraint, medical review is immediate after any restrictive intervention, and the child with hyperactive delirium is treated as a medical emergency. [7]
Pathophysiology
Acute behavioural disturbance is the behavioural output of a brain that has lost the ability to regulate its own threat response. The prefrontal cortex, which normally inhibits and shapes behaviour, is functionally down-regulated. The amygdala and the limbic threat system, which generate the fight-flight response, are overactive. The sympathetic nervous system surges: tachycardia, hypertension, sweating, tachypnoea, mydriasis. Behaviourally this looks like pacing, shouting, threatening and striking out; physiologically it is preparing the body for violence. [1]
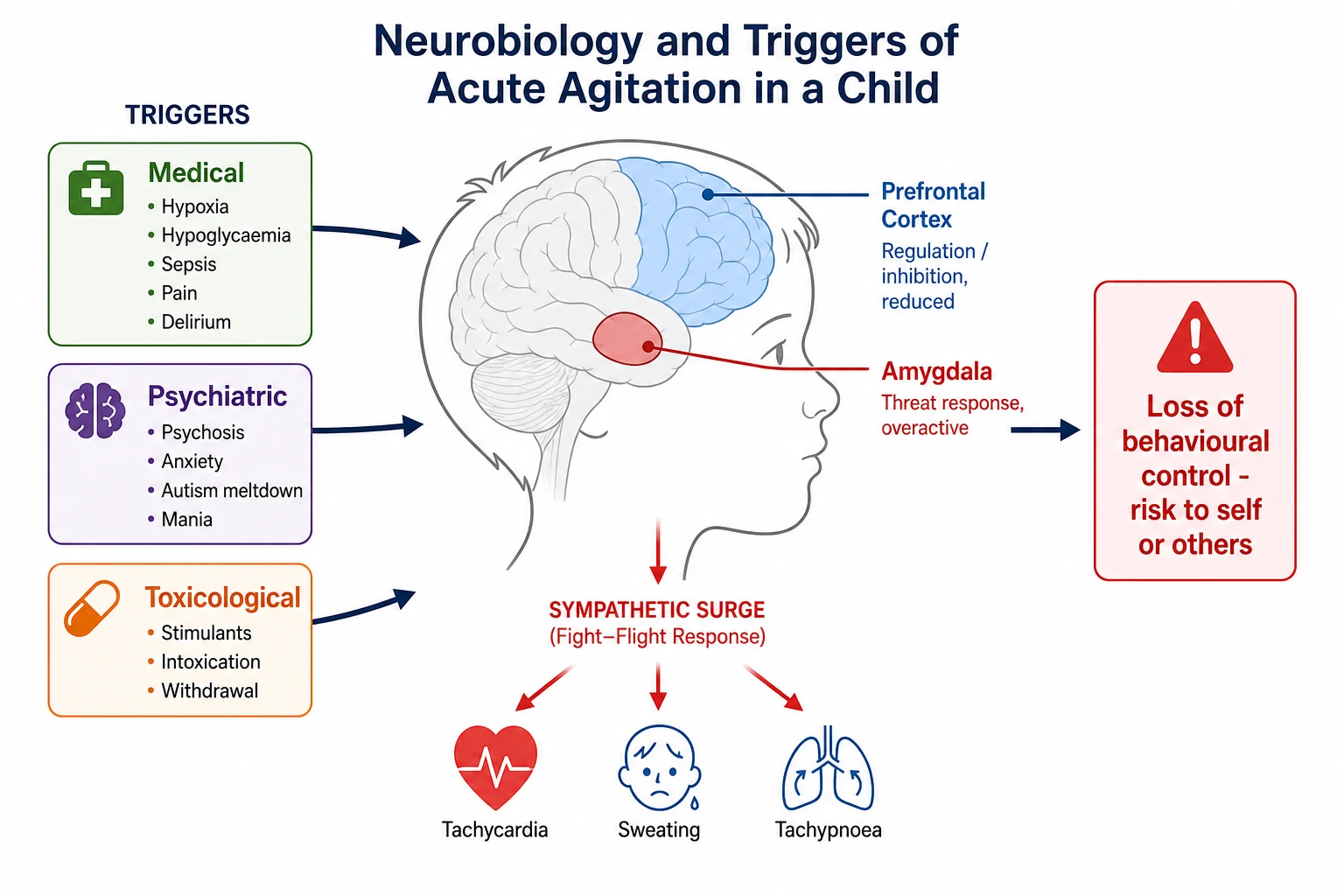
The drivers of this final common pathway group into four families. Medical drivers include hypoxia, hypercapnia, hypoglycaemia, sepsis, central nervous system infection, raised intracranial pressure, post-ictal state, pain, urinary retention, constipation, electrolyte disturbance, hyperthyroidism, adrenal crisis, and delirium from any cause. Psychiatric drivers include first-episode psychosis, manic episode with mixed features, severe anxiety, post-traumatic stress, acute stress reaction, and severe depression with agitation. Toxicological drivers include sympathomimetic intoxication (methamphetamine, MDMA, cocaine, synthetic cathinones), anticholinergic toxidrome, serotonin syndrome, alcohol and benzodiazepine withdrawal, GHB withdrawal, and hepatic encephalopathy. Developmental drivers include autistic meltdown, attention deficit hyperactivity disorder with emotional dysregulation, and intellectual disability with behavioural crisis. The four families are not mutually exclusive; an intoxicated autistic adolescent with a head injury may have all four. [1] [7]
The agents used to settle the child act on the same neurobiology. Benzodiazepines potentiate gamma-aminobutyric acid type A receptors and dampen the limbic system; this is calming but also airway-threatening in higher doses, and can cause paradoxical disinhibition in children, particularly those with intellectual disability. Antipsychotics block dopamine D2 receptors and serotonin 5-HT2A receptors; this is calming but also produces extrapyramidal effects, akathisia, QT prolongation, hypotension and the neuroleptic malignant syndrome. Ketamine antagonises N-methyl-D-aspartate receptors and produces a dissociative state; useful in severe hyperactive delirium in adults, it carries risk of hypersalivation, hypertension and emergence phenomenon, and its place in paediatric agitation is limited and cautious. Dexmedetomidine is an alpha-2 agonist that produces sedation without respiratory depression; its place in acute agitation is emerging but not first-line. [1] [8]
The QT prolongation with antipsychotics deserves attention because it can kill quietly. Haloperidol, droperidol and ziprasidone each prolong the QT interval by blocking the rapid component of the delayed rectifier potassium current. The risk is amplified by structural heart disease, electrolyte disturbance (hypokalaemia, hypomagnesaemia, hypocalcaemia), other QT-prolonging drugs (macrolides, fluoroquinolones, ondansetron, methadone), bradycardia, and the cumulative dose. Droperidol transiently prolongs the QT interval even in healthy children at standard doses, although the change is usually clinically insignificant; the point is to know the cardiac history and the concurrent medication list before the first injection, and to check an ECG when risk accumulates. [9]
The physiological cost of untreated severe agitation is real and is the reason hyperactive delirium with severe agitation is a medical emergency. Sustained muscle activity produces rhabdomyolysis with hyperkalaemia, acidosis and acute kidney injury. Hyperthermia worsens the metabolic picture and can precipitate disseminated intravascular coagulation. The combination of hyperkalaemia, acidosis and a prolonged QT interval sets up the cardiac arrest that has been described in restraint deaths regardless of label. This is why severe, sustained agitation in a child is treated as a time-critical medical emergency rather than a behavioural problem. [7]
Clinical Presentation
Acute behavioural disturbance presents as a behaviour you can see and describe. The first clinical act is to describe it objectively and chronologically in the notes: what the child is doing, when it started, what changed it, and what is happening now. Phrases such as "agitated and aggressive" are insufficient; "pacing the cubicle, shouting at staff, threw a water bottle at the wall at 14:32, no injuries, calmed briefly when mother entered" is the level of description that drives decisions. [1]
The Behavioural Activity Rating Scale (BARS) anchors severity in a number that the team can share and re-measure. A score of 4 is the calm, awake baseline. A score of 5 is overactive but calms on request. A score of 6 is acutely overactive and not calming on request, the threshold for considering parenteral medication. A score of 7 is violent, the threshold for restraint and rapid tranquillisation together. Repeating the BARS at intervals documents the response to intervention and is the marker the team should look for when deciding whether to re-dose, to step down, or to escalate. [1]
Collateral history is gathered from every available source, often in parallel with de-escalation. The parent or caregiver, the school, the ambulance crew, the police, the referring clinician and the electronic record are all sources. The questions are: what is the child's usual baseline, what has changed, what are the triggers, what is the recent medication and adherence, what substances are involved, is there an advance or behavioural care plan, and what has worked or failed before. A child with a known positive behaviour support plan should be managed through that plan where possible. [1]
The clinical features that point to a medical or toxicological driver rather than a primary psychiatric one are the discriminators that protect the medical child from being sedated through a deteriorating illness. They are: fever, abnormal observations (tachycardia, hypertension or hypotension, hypoxia, fever or hypothermia, abnormal respiratory rate), focal neurological signs, abnormal pupil size or reactivity, abnormal movements (tremor, rigidity, clonus, myoclonus, dystonia), autonomic instability (diaphoresis or dry skin, flushing, pallor), incontinence, and fluctuating consciousness. Any one of these in an agitated child shifts the response from psychiatric de-escalation alone to a parallel medical work-up. [5] [7]
Delirium deserves a separate mention because it is the medical mimic most often mistaken for psychiatric agitation. Delirium is an acute, fluctuating disturbance of attention and awareness caused by a medical condition. It produces disorganised thinking, perceptual disturbance (illusions, hallucinations), sleep-wake disturbance, and either hyperalert or hypoalert states. The hyperalert form looks exactly like psychiatric agitation; the difference is the fluctuation, the disorientation, the underlying medical cause, and the response to treating that cause. Treating delirium with a benzodiazepine (unless the cause is alcohol or benzodiazepine withdrawal) worsens it; treating it with a low-dose antipsychotic while working up the cause is the standard approach. [1]
Autistic meltdown is its own physiology. It is the response of an overwhelmed nervous system to sensory overload, communication failure, routine disruption, pain, or co-occurring medical illness. It is not defiance, not attention-seeking, not a behavioural choice. The child in meltdown cannot process language, cannot reason, and cannot self-regulate; they need co-regulation from a trusted adult, reduction of sensory input, and time. Escalating to sedation or restraint in the early phase of a meltdown typically worsens the trajectory; calming the environment and bringing in a known person usually settles it. Recognising meltdown is a clinical skill, and a child with a known autism diagnosis and a positive behaviour support plan should be managed through that plan first. [6]
The presentation changes with age. Neonates and young infants present with irritability, inconsolable cry, altered feeding or altered tone; the differential is medical and broad, including sepsis, meningitis, metabolic disturbance, intracranial bleed, abusive head trauma and pain. Preschool children may present with severe tantrum, head-banging, breath-holding or acute behavioural change; the medical differential remains broad and safeguarding is always open. School-age children may present with acute behavioural dysregulation in the context of developmental disorder, family stress, bullying or first presentation of a primary psychiatric disorder. Adolescents present most often with intoxication, self-harm, first-episode psychosis, mood disorder with mixed features, family violence, or youth-justice contact. [6]
Differential Diagnosis
The differential is built in the order that protects the child: what can kill the child now, what is most likely, what is reversible, and what is most harmful to miss. The "kill now" and "reversible" categories overlap and are addressed first: hypoxia, hypoglycaemia, sepsis, central nervous system infection, raised intracranial pressure, status epilepticus and post-ictal state, toxidromes, hyperthermia, and pain. [1]
The can't-miss mimics are the medical causes that masquerade as psychiatric agitation: hypoglycaemia, hypoxia, intracranial bleed, sepsis, intoxication and non-accidental injury. Each has a single resolving action: hypoglycaemia resolves with a bedside glucose and treatment; hypoxia resolves with oxygen saturation and oxygen; intracranial bleed resolves with imaging; sepsis resolves with cultures and antibiotics; intoxication resolves with a careful toxin history and supportive care; non-accidental injury resolves with a safeguarding response. Running through these before reaching for a sedative is the discipline of the differential. [1]
A second discriminator runs through the differential: the tempo and context of the behaviour. Acute agitation in a previously well child, with no psychiatric history, in the context of physical symptoms or signs, is medical. Acute agitation in a child with a known mental health diagnosis, with a recognisable trigger, with the same pattern as previous episodes, is more likely to be psychiatric. Acute agitation in a child with autism or intellectual disability, with a recognisable sensory or communication trigger and no new medical features, is more likely to be developmental. The discriminator is not the behaviour itself but what surrounds it. [6]
Clinical & Bedside Assessment
The primary survey in an agitated child is adapted for safety. Staff safety is assessed first: is anyone in immediate danger, are enough trained staff present, is the room safe, is the exit clear. A leader is named, roles are assigned, and a plan is set. Airway, breathing, circulation, disability and exposure are then assessed as far as the child allows, with the calm lead clinician at eye level and the team positioned to support rather than confront. [1]
The bedside ten-second triage for medical drivers runs alongside the primary survey: bedside glucose, oxygen saturation, temperature, respiratory rate, pulse, capillary refill, pupil size and reactivity, posture, tone, and the level of consciousness on AVPU. Any abnormality in this set redirects the response toward the medical cause. A bedside glucose is checked in any agitated child with altered consciousness, and a dangerous low is treated immediately. [1]
Capacity to consent is assessed and recorded in every agitated child or adolescent who can engage. The framework varies: in Australia a child or young person who has sufficient understanding and intelligence to understand the proposed treatment is a mature minor and can consent (Gillick competence); in the United Kingdom the analogous test is Fraser competence for those under sixteen and the Mental Capacity Act 2005 for those sixteen and over. When capacity is impaired and the treatment is necessary to prevent serious harm, treatment proceeds under the relevant mental health or guardianship legislation, with the statutory forms completed and the reasons documented. [1] [2]
The signs that suggest a medical or toxicological driver requiring investigation before or alongside sedation are the same signs that anchor the differential: fever, hypertension, mydriasis, nystagmus, tremor, rigidity, clonus, hyperreflexia, dry or sweaty skin, and abnormal movements. Their presence widens the work-up and narrows the choice of agent: for example, an antipsychotic is avoided when an anticholinergic toxidrome is suspected, and a benzodiazepine is preferred when alcohol or benzodiazepine withdrawal is the driver. [7]
Examination of the restrained or sedated child is completed once control is achieved. A full top-to-toe examination looks for injury from self-harm or restraint, injury from a fall or assault, marks of injection, signs of ingestion, focal neurological findings, an intra-abdominal cause, and any sign of non-accidental injury. A child who has been restrained must be examined for restraint-related injury: bruising, abrasion, musculoskeletal injury, and any sign of airway compromise or aspiration during the event. [1]
In Australia and Aotearoa New Zealand, the relevant legislation varies by jurisdiction. Each Australian state and territory has its own Mental Health Act and its own Guardianship Act, with statutory forms for emergency treatment without consent and for the use of restraint. Aotearoa New Zealand operates under the Mental Health (Compulsory Assessment and Treatment) Act 1992. Know the local forms, the criteria, and the time limits before you need them, and involve the on-call mental health clinician early.
The common technique errors in approaching an agitated child are well described and worth naming so they can be avoided. Approaching head-on, towering over the child, prolonged or intense eye contact, multiple staff speaking at once, sudden movements, escalating ultimatums, ignoring known sensory needs, and using a uniformed or security presence as the first response all reliably worsen the situation. The corrective posture is well described: approach at an angle, drop to eye level, minimise eye contact, one calm voice, slow movements, offer choices rather than demands, and respect the personal space. [1] [1]
Investigations
The mandatory investigations for the acutely agitated child are few and immediate: bedside glucose, oxygen saturation, full set of observations, temperature, and a weight (estimated from a length-based tape if unknown, then measured directly as soon as safe). A weight is mandatory before any weight-based drug is given. [1]
A 12-lead ECG is indicated before or soon after sedation in any child with a cardiac history, syncope, a family history of sudden death, an electrolyte abnormality, concurrent QT-prolonging drugs, methamphetamine or other stimulant intoxication, a high cumulative dose of a QT-prolonging antipsychotic, or any clinical feature suggesting a cardiac cause. The QT interval is measured manually, typically in lead II or V5, and corrected for heart rate using the Bazett formula at the bedside. A QTc of greater than 460 ms in males, greater than 470 ms in prepubescent children, or greater than 480 ms after puberty is concerning and warrants review of the sedation plan and the medication list. A QTc of greater than 500 ms is high risk for torsades de pointes. [8] [9]
Blood tests are sent when the clinical picture suggests a medical or toxicological driver: full blood count, electrolytes (including magnesium and phosphate), calcium, glucose, lactate, creatine kinase (especially in methamphetamine intoxication or sustained severe agitation), a drug or alcohol screen as indicated, ammonia if an inborn error or hepatic encephalopathy is suspected, thyroid function, and a venous blood gas in the unwell child. The samples are taken early so results return in time to matter; they must not delay stabilisation. [7]
Neuroimaging is indicated when there are focal neurological signs, a head injury, an abnormal Glasgow Coma Scale or abnormal pupils, suspected raised intracranial pressure, a first-episode psychosis with neurological soft signs, or a post-ictal state that is not resolving. The choice between computed tomography and magnetic resonance imaging depends on urgency and modality availability, with computed tomography the first-line in the emergency setting. [1]
An infectious work-up is indicated in any febrile agitated child: urine, blood culture, and consideration of lumbar puncture (once the child is safe and the contraindications excluded) for cerebrospinal fluid. Meningococcal, pneumococcal and herpes simplex polymerase chain reaction testing is guided by the clinical picture. The empiric antibiotic and aciclovir regimen is guided by the local guideline and is not delayed while waiting for imaging or lumbar puncture. [1]
A urine or serum drug screen is a clinical tool, not a routine test, and its limitations must be understood. Standard immunoassays detect a limited panel of substances (common opioids, cannabinoids, amphetamines, cocaine, benzodiazepines), miss many synthetic agents (synthetic cathinones, fentanyl analogues, novel benzodiazepines), and can produce false positives and false negatives. A positive screen does not explain the agitation and a negative screen does not exclude intoxication; the clinical picture drives management. [7]
Management — Resuscitation
The immediate response to an acutely agitated child is an organisational act before it is a medical one. Ensure the safety of staff, the child and others first: clear the area of hazards and of other patients, move furniture, remove access to weapons or ligature points, and ensure the exit is clear. Call for help early: senior paediatric staff, mental health, security if available and trained, and a clinical lead. Name a team leader, assign roles, draw up the drugs you might need, prepare monitoring and emergency airway equipment, and plan the exit and the debrief before you act. [1] [1]
The primary survey runs in parallel and protects the medical child. Oxygen is given for hypoxia. A bedside glucose is checked and treated. An ongoing seizure at five minutes is treated as status epilepticus. Hyperthermia is cooled. Pain is treated. The medical child who looks agitated because they are hypoxic, hypoglycaemic, septic, fitting, in pain or delirious is settled by treating the cause, not by sedating through the deterioration. [1]
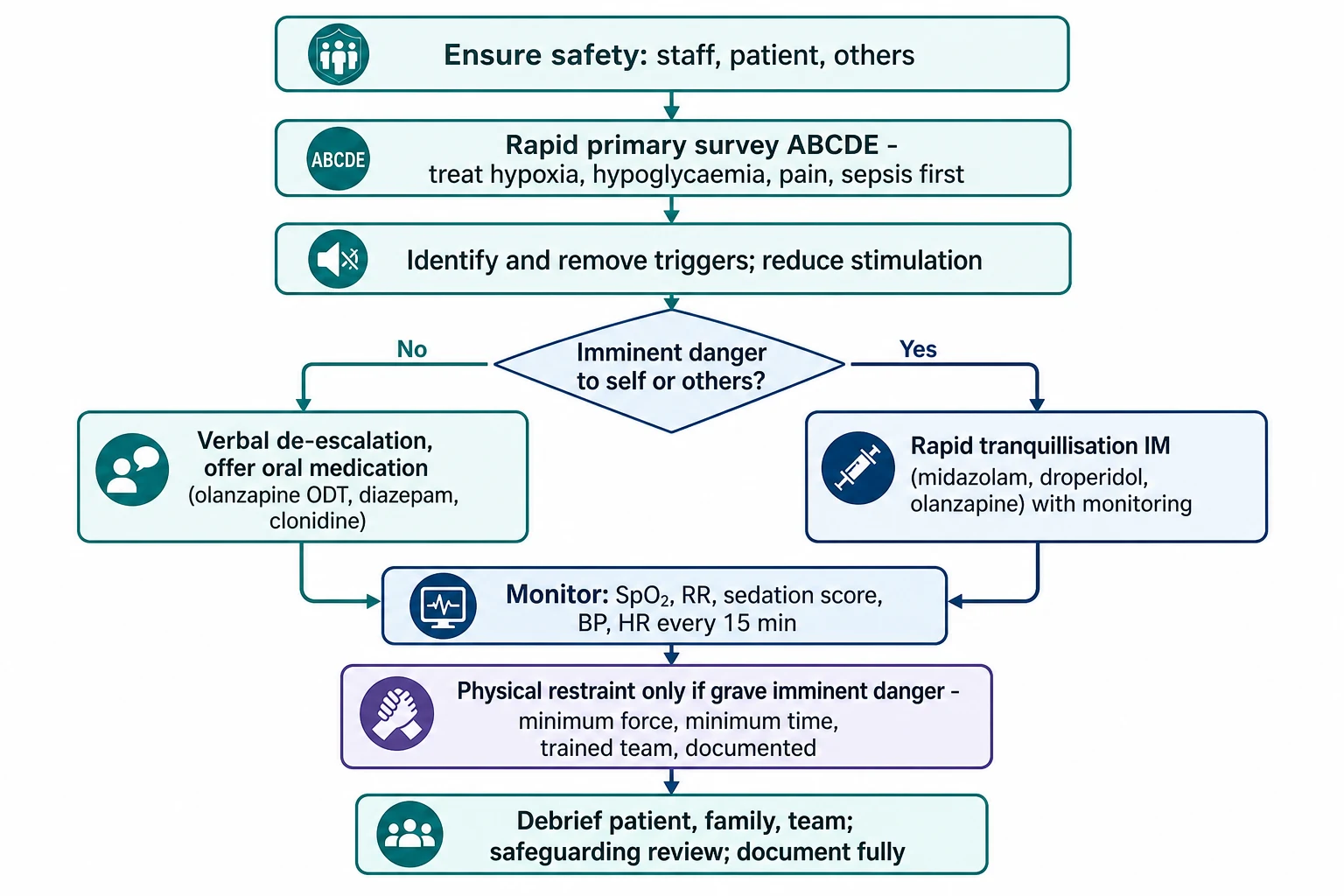
Verbal de-escalation is the universal first intervention and is given a genuine trial before pharmacological escalation. The evidence-based components are well established: respect personal space and keep a safe distance; do not be provocative (drop to eye level, hands visible, calm voice); establish verbal contact with one clinician and one voice; use concise language the child can process; identify what the child wants and what they are feeling; listen closely to what is said; agree or agree to disagree where possible; set clear, reasonable limits; offer choices and reasonable optimism; and debrief later. A genuine trial of de-escalation, with environmental modification, settles the majority of agitated children and young people without medication. [1] [1]
Environmental modification works with de-escalation and is often the more powerful lever. Move the child to a low-stimulation single room if possible. Reduce lighting and noise. Remove hazards and access to ligature points or weapons. Keep a trusted parent, caregiver or support person present if it is safe to do so. Offer food, drink or a blanket if appropriate. Remove clinical uniforms and equipment that signal threat. Offer sensory items the child knows (headphones, weighted blanket, fidget) where available. Reduce the number of staff visible while keeping enough for safety. [1]
Pharmacological intervention is indicated when de-escalation has failed, when the severity of agitation (BARS 6 to 7) makes oral or non-pharmacological management unsafe, or when essential medical care cannot be provided any other way. The principle is to offer oral medication with consent first, escalating to parenteral only when oral is refused, unsafe, or unlikely to act fast enough to prevent serious harm. The PEAChY-O randomised controlled trial demonstrated that oral medication is effective as first-line therapy for paediatric agitation in the emergency department, supporting the oral-first approach. [3] [4]
Oral first-line agents (RCH Melbourne)
The first-line parenteral agents for rapid tranquillisation are intramuscular midazolam, intramuscular droperidol, and intramuscular olanzapine. The choice of agent depends on the suspected driver, the cardiac history, the concurrent medications, the prior response, and the local guideline. The Royal Children's Hospital Melbourne guideline lists representative intramuscular doses: midazolam 0.1 to 0.2 mg per kg, droperidol 0.1 to 0.14 mg per kg in younger children and 5 to 10 mg in older adolescents, and olanzapine 2.5 to 5 mg in younger or smaller children and 5 to 10 mg in adolescents. The exact dose, route and re-dosing interval must be confirmed against your current local guideline and the child's weight before administration. [1]
[8]Monitoring after any parenteral sedation is mandatory and is where most preventable harm is detected. Pulse oximetry, respiratory rate, sedation score, blood pressure and heart rate are recorded at least every 15 minutes for at least one hour after the dose, longer if the child remains drowsy. An ECG is monitored if a QT-prolonging agent has been used in a high-risk child. The sedation score used is the locally adopted tool; the goal is calming with the child rousable, not loss of airway reflexes. Emergency equipment is immediately available throughout: suction, oxygen, bag-valve-mask, advanced airway, reversal agents (naloxone for opioids, flumazenil for benzodiazepines), and the resuscitation trolley. [1] [1]
The rule for re-dosing is conservative: assess the response at the interval set by the local guideline (typically 15 to 30 minutes for intramuscular agents), use a different agent class for the second dose where possible to limit cumulative respiratory depression, avoid stacking cumulative doses, and involve a senior clinician in the decision. A child who is escalating despite an adequate dose of a first-line agent is a child who needs senior review, a wider differential, and consideration of a higher level of care. [1]
Management — Definitive & Stepwise
The full stepped-care ladder brings together the resuscitation elements above with the longer arc of definitive care. The trigger to move up the ladder is failure of the lower step combined with rising risk; the trigger to move down is response. The ladder is not a one-way street: a child who is settled by parenteral medication is moved back to oral medication and de-escalation as soon as it is safe to do so. [1] [1]
Stepped-care ladder for acute behavioural disturbance
Step 1: Verbal and environmental de-escalation. A calm lead clinician at eye level, one voice, low-stimulation room, remove hazards, trusted adult present. A genuine trial is given before pharmacological escalation.
Step 2: Oral medication with consent. Olanzapine orally disintegrating tablet, diazepam or clonidine, chosen by driver and age. Offer the choice, explain the purpose, allow the child to take it. The PEAChY-O 2025 RCT supports oral as effective first-line.
Step 3: Parenteral rapid tranquillisation when oral is refused, unsafe, or unlikely to act fast enough. Intramuscular midazolam, droperidol or olanzapine, chosen by driver and cardiac risk. Monitor every 15 minutes for at least one hour.
Step 4: Physical restraint for grave and imminent danger that cannot be prevented any other way. Minimum force, minimum duration, trained team with a named leader, airway visible at all times, reassessed every 15 minutes, documented and debriefed.
Step 5: Debrief and review. With the child when able, with the family, and with the team. Safeguarding review. Update the behavioural care plan. Notify per local restraint reporting framework.
The PEAChY-O randomised controlled trial (Bourke 2025, Annals of Emergency Medicine) is the most directly relevant trial in paediatric agitation. It compared oral medication with standard care for the emergency management of agitation in children and young people, and found oral medication to be effective as first-line therapy. The trial was designed and reported from a paediatric emergency network in Australia and Aotearoa New Zealand and is supported by a published protocol (Bourke 2023, BMJ Open). It anchors the oral-first approach in randomised evidence rather than tradition. [3] [4]
PEAChY-O (Bourke 2025)
Randomised controlled trial of oral medication versus standard care for the emergency management of agitation in children and young people
Population: Children and young people presenting to participating paediatric emergency departments in Australia and Aotearoa New Zealand with acute agitation
Key finding
Oral medication was effective as first-line therapy for paediatric agitation, supporting an oral-first approach where the child will accept it.
Practice change
First pharmacological intervention in the agitated child or young person should be oral wherever possible; reserve parenteral rapid tranquillisation for refusal, safety concern, or failure of oral.
Choosing between agents is a clinical judgement informed by the suspected driver, the age and weight, the cardiac and QT history, the concurrent medications, the seizure risk, the prior response, and the local guideline. For a primary psychiatric agitation in an adolescent with no cardiac concerns, an atypical antipsychotic (olanzapine) is a reasonable first-line oral choice, with a benzodiazepine as an alternative. For alcohol or benzodiazepine withdrawal, a benzodiazepine is preferred and an antipsychotic is avoided as first-line for the withdrawal itself. For methamphetamine intoxication, benzodiazepines are first-line to reduce the sympathetic surge, with an antipsychotic second-line under ECG monitoring. For delirium, treat the cause and use a low-dose antipsychotic if needed, avoiding benzodiazepines unless the cause is withdrawal. For autistic meltdown, prioritise sensory regulation and a trusted adult and reserve a low-dose atypical antipsychotic for severe or prolonged episodes. [1] [7]
Ketamine has a limited and cautious place in paediatric acute agitation. Adult pre-hospital and emergency evidence supports its use for severe hyperactive delirium or excited delirium in adults, where its rapid onset and dissociative effect are advantageous. Paediatric evidence is limited, and concerns include hypersalivation, hypertension, emergence phenomenon, and the difficulty of monitoring an adolescent who has been given a dissociative dose in a busy emergency department. Where it is used, it is used at a dissociative dose with continuous monitoring and a clear plan for airway management; in most paediatric settings, it is not first-line. [1]
Parenteral rapid tranquillisation (RCH Melbourne, representative)
Physical restraint is reserved for grave and imminent danger that cannot be prevented any other way. The indications are narrow: a child actively and imminently causing serious harm to self or others, where de-escalation and pharmacological management have failed or cannot be safely initiated. The form of restraint is the least restrictive that is effective: holding by trained staff for the shortest time needed, then mechanical restraint only if holding is insufficient, then seclusion in a designated, safe, ligature-checked room only if mechanical restraint is insufficient. The team delivering restraint is trained and led, with named roles, an airway observer, and a timekeeper. The child is held in a position that keeps the airway visible and unobstructed at all times; face-down (prone), hobble and strangulation-risk positions are prohibited. Vital signs and the mental state are checked continuously during restraint, and the child is reassessed at least every 15 minutes for the duration of the restraint. The event is documented contemporaneously and debriefed afterwards. [1] [1] [7]
Post-incident care is part of the management, not an afterthought. The child is medically reviewed for injury, for aspiration, for restraint-related injury, and for any sign of physiological deterioration; creatine kinase, renal function and electrolytes are checked after sustained severe agitation. A debrief is held with the child when they are able, with the family, and with the team, using a structured format (Plan-Do-Study-Act or equivalent). A safeguarding review is automatic for any child in care and for any unexplained or repeated restraint. The behavioural care plan is updated. Notification is made under the local restraint reporting framework and under the mental health legislation where it applies. A follow-up appointment is arranged with the relevant service (paediatric, mental health, developmental, or safeguarding). [1] [11]
For a child with a known behavioural emergency care plan, positive behaviour support plan or advance directive, the plan is the first reference and changes the response. The plan typically identifies the early signs, the de-escalation strategies that work, the medications and doses that have helped or caused adverse effects, the trusted adults, the communication aids, the sensory regulation strategies, and the escalation pathway. Following the plan is both clinically safer and legally and ethically stronger than starting from scratch. [6] [1]
Specific Subtypes & Scenarios
The child with autism spectrum disorder and intellectual disability in meltdown is the scenario in which the standard escalation fails most often. Sensory regulation comes first: reduce light and noise, remove unnecessary staff, offer the child's own sensory items, and bring in the trusted adult. Communication is adapted: use the child's communication aids, allow processing time, give one instruction at a time, and respect non-verbal signals. A low-dose atypical antipsychotic is reserved for severe or prolonged episodes, and a benzodiazepine is used with caution because paradoxical disinhibition is more common in this group. Olanzapine orally disintegrating tablet is often preferred because it can be given without water and without the child having to swallow. Children with autism and ADHD are over-represented among emergency mental health presentations and among restraint events; the response to this group is a marker of the quality of the service. [6]
Methamphetamine and other sympathomimetic intoxication in an adolescent is a medical emergency as much as a behavioural one. The presentation is tachycardia, hypertension, mydriasis, sweating, agitation, hyperthermia, and (with severe or sustained intoxication) rhabdomyolysis, hyperkalaemia, acute kidney injury and cardiac arrhythmia. Benzodiazepines are first-line: they reduce the sympathetic surge, settle the agitation, lower the temperature and treat the muscle activity. An antipsychotic is added second-line for refractory agitation, with ECG monitoring because both the methamphetamine and the antipsychotic prolong the QT interval. Creatine kinase, renal function and electrolytes are monitored; hyperthermia is cooled actively. The recent paediatric case series from Malashock and colleagues documents the clinical pattern and the therapeutic role of antipsychotics. [7]
Anticholinergic toxidrome and serotonin syndrome are medical mimics with specific management. Anticholinergic toxidrome (hot as a hare, dry as a bone, red as a beet, blind as a bat, mad as a hatter) is managed with benzodiazepines and cooling; an antipsychotic is avoided because of its additive anticholinergic effect, and physostigmine is reserved for specialist toxicology care. Serotonin syndrome (spontaneous or inducible clonus, hyperreflexia, autonomic instability, agitation, diaphoresis, hyperthermia) is managed by stopping the serotonergic drugs, benzodiazepine, cooling and cyproheptadine for severe cases; an antipsychotic is avoided. Both are toxin-related and benefit from early toxicology consultation. [7]
Alcohol and benzodiazepine withdrawal in an adolescent is managed with a benzodiazepine taper (a long-acting agent such as diazepam, symptom-triggered using a validated scale), thiamine, fluid and electrolyte correction, and a calm environment. The agitation is treated with the benzodiazepine itself rather than an antipsychotic, because the underlying problem is benzodiazepine or gamma-aminobutyric acid withdrawal. Severe withdrawal (delirium tremens, seizures) is managed in a high-dependency or intensive care setting. [1]
Delirium is treated by identifying and treating the cause (infection, drug, metabolic, electrolyte, pain, urinary retention, constipation, withdrawal), with a low-dose antipsychotic (haloperidol or quetiapine) if the agitation is severe. A benzodiazepine is avoided unless the cause is alcohol or benzodiazepine withdrawal, because benzodiazepines worsen delirium from other causes. The child is nursed with orientation cues, sleep-wake cycle protection, and family presence. [1]
First-episode psychosis in an adolescent is managed with an antipsychotic, a calm environment, early involvement of youth mental health services, family support, and avoidance of high-dose or combined agents that increase the risk of adverse effects without improving outcome. Capacity, consent and the relevant mental health legislation are assessed and documented. The longer-term plan is made with the specialist service. [8]
Acute behavioural disturbance in a preverbal or developmentally delayed child is managed with a focus on medical causes, weight-based dosing, sensory regulation, parent involvement, and a lower threshold for senior and PICU support. The differential in this group is broad and the child's ability to cooperate with assessment is limited; the threshold for investigation and for escalation is lower than in a verbal adolescent. [1]
The child or young person in youth-justice custody is managed with the relevant legislation and restraint authority in mind, with a forensic medical assessment, with safeguarding notification, with trauma-informed care, and with cultural safety given the over-representation of Indigenous youth in custody. The clinical encounter is also a legal and human-rights encounter, and the documentation supports both. [7]
The self-harming and refusing adolescent is managed with a risk assessment, a capacity assessment, application of the least-restrictive principle, an offer of oral medication, and (where capacity is impaired and serious harm is imminent) treatment under the mental health legislation. Family and advocate involvement is encouraged where safe. The encounter is a clinical assessment of risk and a therapeutic engagement, not a confrontation. [1] [2]
Complications & Pitfalls
The complications of sedation are the complications of the agents used. Respiratory depression and airway loss are the most immediate, particularly with benzodiazepines, with the combination of an antipsychotic and a benzodiazepine, and with any agent given to a child who is also intoxicated. Aspiration follows airway loss. Hypotension follows the antipsychotics and the benzodiazepines, and is amplified by hypovolaemia and concurrent medication. Oversedation is the failure mode of repeated dosing without adequate reassessment. QT prolongation and torsades de pointes follow the antipsychotics (haloperidol, droperidol, ziprasidone) and are amplified by structural heart disease, electrolyte disturbance and concurrent QT-prolonging drugs. Extrapyramidal effects (acute dystonia, akathisia, parkinsonism) follow the antipsychotics, particularly the first-generation agents, and are more common in antipsychotic-naive children. Neuroleptic malignant syndrome is rare but life-threatening. Serotonin syndrome follows combinations of serotonergic agents. Paradoxical disinhibition follows benzodiazepines, particularly in children with intellectual disability. The emergence phenomenon follows ketamine. [8] [11] [12]
The complications of physical restraint are physical and psychological. Positional asphyxia is the most feared and is the reason no child is restrained face-down or in a hobble and the airway is visible at all times. Aspiration, musculoskeletal injury, pressure injury, rhabdomyolysis and hyperthermia are described. The psychological impact is substantial: re-traumatisation, post-traumatic stress, the loss of the therapeutic relationship, and the impact on future engagement with healthcare. These are not soft outcomes; they are clinical outcomes that change the trajectory of the child's care. [1] [7]
The classic errors are the errors that recur across case series and coronial findings. Missing a medical cause (hypoglycaemia, hypoxia, sepsis, intracranial bleed) is the error that kills; treating the deterioration as a behavioural problem and sedating through it is its mechanism. Using physical restraint before de-escalation is the error that harms. Combining intramuscular olanzapine with a parenteral benzodiazepine without close monitoring is the error that causes airway loss. Inadequate post-sedation monitoring is the error that allows oversedation to progress to respiratory arrest. Restraining a child face-down or in a hobble is the error that causes positional asphyxia. Restraining without a named leader is the error that allows force to escalate. Failing to debrief is the error that allows the cycle to repeat. Failing to escalate to senior or PICU is the error that allows a deteriorating child to deteriorate further. Treating a behavioural crisis as a criminal matter is the error that damages the child and the service. [1] [1]
The iatrogenic spiral is worth naming because it is preventable. A medication is given; an adverse effect appears (oversedation, extrapyramidal effect, hypotension); the adverse effect is misread as worsening agitation; a further medication is given; the child tips into respiratory or cardiovascular collapse. The corrective is monitoring, recognition of the adverse effect for what it is, and senior review before any second dose. [8]
Antipsychotic-naive children have a high rate of adverse effects. The ETAPE naturalistic study of antipsychotic-naive children and adolescents reported a high incidence of adverse events, including sedation and extrapyramidal effects, in the first weeks of treatment. In the acute setting this means start low, monitor closely, and warn the family about the common effects. The follow-up work of Menard and colleagues describes the emergence of psychiatric adverse events during antipsychotic treatment in antipsychotic-naive children, which is relevant to the post-discharge plan and the handover to the mental health service. [11] [12]
The legal and ethical pitfalls are the pitfalls of treating without consent or legal authority, of disproportionate force, of prolonged restraint, of restraint as punishment, of failure to notify under mental health legislation, and of failure to report a child in care. Each of these is avoidable by knowing the local legislation, by involving the on-call mental health clinician early, by documenting the indications and the proportionality, and by treating a restraint event as a reportable clinical event. [1] [7]
[1]Prognosis & Disposition
Disposition is determined by the cause, the response to intervention, the ongoing risk, the capacity, the social supports, the prior plans, and the need for specialist input. The child who is medically well, whose agitation has settled, whose reversible trigger has been addressed, who is not at ongoing risk of harm, and who has a safe environment and a follow-up plan can be discharged from the emergency department with a written safety-net. The child who needs ongoing medical observation, who is still agitated, who has a complex social situation, who needs psychiatric or developmental assessment, or who needs treatment of an underlying medical cause is admitted to a paediatric ward. The child with a primary psychiatric diagnosis, ongoing risk, and the capacity to benefit from a therapeutic milieu is admitted to a child or adolescent mental health unit, with the relevant mental health legislation applied if capacity is impaired. [1]
The child who has oversedation, airway compromise, cardiovascular instability, or hyperactive delirium with physiological derangement is admitted to PICU or a high-dependency unit, with retrieval to a tertiary centre if local resources are exceeded. The threshold for PICU is lower in the child who has received cumulative sedation, who has a prolonged QTc, who is acidotic or hyperkalaemic from sustained agitation, or who has underlying cardiorespiratory disease. [1]
Post-crisis follow-up is part of the disposition and is arranged before discharge: outpatient mental health, paediatric review, behavioural plan update, safeguarding plan, school liaison, family support, cultural support, and peer support where available. The follow-up is not a referral that may or may not happen; it is a booked appointment with a named service. [1]
The prognosis of restraint itself includes the psychological impact (post-traumatic stress, re-traumatisation, the loss of the therapeutic relationship, the impact on future engagement with healthcare) and is mitigated by debrief, by follow-up, by an updated behavioural care plan, and by a service-level commitment to restraint minimisation. Children and young people who have been restrained are more likely to be restrained again, and the most effective intervention to break the cycle is a proactive positive behaviour support plan and a trauma-informed service. [11] [7]
The safety-net advice to families is explicit and written: renewed agitation, new physical symptoms (drowsiness, breathing difficulty, chest pain, palpitations, weakness), oversedation, suicidal ideation, or any concern about the child's safety should trigger return. The family is given the names and contact details of the follow-up service and the number for emergency services. [1]
Special Populations
The autistic child and the child with intellectual disability are the population in which the standard approach most often fails and most often harms. A positive behaviour support plan is the first reference where one exists. Sensory regulation is first-line: reduce light and noise, remove unnecessary staff, offer the child's own sensory items, allow processing time. Communication is adapted to the child's means (aids, pictures, single words, allow processing time). A trusted adult is present where safe. A low-dose atypical antipsychotic is reserved for severe or prolonged episodes, and a benzodiazepine is used with caution because paradoxical disinhibition is more common. Olanzapine orally disintegrating tablet is often preferred because it can be given without water and without swallowing. Weight-based dosing is mandatory. Children with autism and ADHD are over-represented in emergency mental health presentations and among restraint events, and the response to this group is a marker of the quality of the service. [6]
The adolescent with capacity to refuse is approached through the legal and ethical framework for capacity and consent. In Australia, a child or young person with sufficient understanding and intelligence to understand the proposed treatment is a mature minor and can consent (Gillick competence). In the United Kingdom, the analogous tests are Fraser competence for those under sixteen and the Mental Capacity Act 2005 for those sixteen and over. When capacity is impaired and serious harm is imminent, treatment proceeds under the relevant mental health or guardianship legislation, with the statutory forms completed and the reasons documented. Family and advocate involvement is encouraged where safe. [1] [2]
The Aboriginal, Torres Strait Islander and Maori child is approached through cultural safety. Cultural consultation is sought early; family is included; the recognition of intergenerational trauma shapes the de-escalation; the post-incident support is culturally appropriate. Cultural safety is a clinical safety issue in this group: a de-escalation plan that ignores culture will escalate rather than calm, and the over-representation of Indigenous children and young people in restraint statistics is both a clinical and a human-rights concern. [7]
The refugee, asylum-seeking and migrant child is approached through an interpreter, trauma-informed care, a cultural formulation, the recognition of pre-arrival trauma, and the involvement of the guardian. Language barrier is a clinical risk in this group because it converts communication failure into behavioural escalation. [1]
The child in out-of-home care is approached with a safeguarding notification, the involvement of the carer and the statutory authority, trauma-informed care, a behavioural plan review, and the recognition of attachment disruption. A restraint event in a child in care is a significant event that triggers a statutory review. [1]
The child or young person in youth-justice custody is approached with the legislation and the restraint authority in mind, a forensic medical assessment, a safeguarding obligation, trauma-informed care, and cultural safety given the over-representation of Indigenous youth. The clinical encounter is also a legal encounter, and the documentation supports both. [7]
The child with complex chronic illness or technology dependence is approached through the baseline: a baseline behaviour that looks disturbed to staff who do not know them, a communication style that uses behaviour rather than words, a device that may have failed, a rapid decompensation with standard doses, and a higher threshold for senior support and for PICU. Knowing the child and their baseline is the first step. [6]
The developmentally delayed or preverbal child is approached with a focus on medical causes, weight-based dosing, the parent as the primary soother, sensory regulation, and a lower threshold for senior and PICU support. The differential in this group is broad and the child's ability to cooperate with assessment is limited; the threshold for investigation and escalation is lower than in a verbal adolescent. [1]
The child or young person who is gender or sexually diverse is approached with their chosen name and pronouns, with trauma-informed care, with recognition of minority stress, with the involvement of family of choice where safe, and with safeguarding if family rejection is part of the picture. [1]
The pregnant adolescent is approached with the fetal considerations in mind, the pharmacokinetic changes of pregnancy, the medication safety profile in pregnancy, and safeguarding and social support. [1]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric acute behavioural disturbance management has strengthened substantially in recent years, with the PEAChY-O programme providing randomised evidence for an oral-first approach. The PEAChY-O protocol (Bourke 2023, BMJ Open) set out the rationale and design for a randomised controlled trial of oral medication for paediatric agitation, and the PEAChY-O trial (Bourke 2025, Annals of Emergency Medicine) reported that oral medication was effective as first-line therapy. These papers, together with the Hilt 2008 paper on agitation treatment for paediatric emergency patients and the recent pharmacotherapy descriptive work, anchor current paediatric practice. [1] [3] [4] [5]
The adult rapid-tranquillisation literature provides the indirect evidence that has shaped paediatric practice. The TREC trial (TREC Collaborative Group, BMJ 2003) compared intramuscular midazolam with intramuscular haloperidol plus promethazine for agitation in adult psychiatric emergency rooms, finding that midazolam was more rapidly sedating; the trial has informed adult practice internationally and, by analogy rather than direct evidence, has shaped paediatric guidance. Adult ketamine evidence for severe agitation is more substantial but is not directly transferable to children. [2]
The adverse-effect literature in children shapes the cautious dosing. The ETAPE naturalistic study (Menard 2019, European Neuropsychopharmacology) reported the incidence of adverse events in antipsychotic-naive children and adolescents treated with antipsychotic drugs, with a high rate of adverse effects in the first weeks. The follow-up work (Menard 2022, Child and Adolescent Psychiatry and Mental Health) described the emergence of psychiatric adverse events during antipsychotic treatment in antipsychotic-naive children. The Hilt editorial on best practices in child antipsychotic use monitoring (Hilt 2021) summarises the monitoring framework. The droperidol-QT work in children (Scott 2015) documents the transient QT effect of droperidol in children undergoing cardiac surgery, a useful reference for the QT conversation in acute agitation. [8] [9] [11] [12]
The controversy over the term "excited delirium syndrome" deserves a clear statement. The term has been used in law-enforcement and emergency-medicine literature to describe the state of severe agitation, autonomic dysregulation and physiological collapse that has been associated with restraint deaths. In 2023 to 2024, the American College of Emergency Physicians withdrew its 2009 white paper endorsement of the term, and the American Psychiatric Association stated that it is not a recognised psychiatric diagnosis. The clinical lesson is independent of the label: a hyperactive, severely agitated patient with autonomic dysregulation is in a medical emergency with risk of cardiovascular collapse, rhabdomyolysis, hyperkalaemia and sudden death, and must be treated as such. [7]
The controversy over ketamine for severe agitation in pre-hospital and emergency settings continues. Adult evidence supports efficacy; paediatric evidence is limited and the concerns (hypersalivation, hypertension, emergence phenomenon, monitoring difficulty) keep ketamine off the first-line list in most paediatric guidance. Where it is used, it is used at a dissociative dose with continuous monitoring and a clear airway plan. [1]
The evidence is weak or absent in important areas of paediatric practice: randomised trials of physical restraint techniques, optimal agent combinations and sequences, long-term psychological outcomes of restraint in children, and cultural-safety interventions and their measurable effect. These gaps shape the research agenda and remind the clinician that much of current practice rests on observational evidence, expert consensus and adult data extrapolated to children. [3]
Lived-experience and consumer perspectives are reshaping the agenda. Restraint minimisation, trauma-informed service design, peer support in the emergency department, sensory rooms, advance directives for psychiatric care, and post-restraint debrief as standard are the interventions being demanded and evaluated. These perspectives are increasingly represented in guideline development and in service design. [11] [7]
Exam Pearls
The single highest-yield rule in paediatric acute behavioural disturbance is that medical causes are sought and treated before sedation, and that hypoxia and hypoglycaemia are the most reversible and most missed. A bedside glucose and an oxygen saturation are checked in any agitated child with altered consciousness; the medical child who is agitated because they are hypoxic or hypoglycaemic is settled by treating the cause, not by sedating through the deterioration. [1]
De-escalation is always first-line, and oral medication is preferred to parenteral wherever the child will accept it. The PEAChY-O 2025 randomised controlled trial anchors the oral-first approach in randomised evidence and is the trial to cite. [3] [4]
MEDICS
Never combine intramuscular olanzapine with a parenteral benzodiazepine in the same syringe or the same visit without close monitoring. The combination risks severe respiratory depression, hypotension and airway loss; the US Food and Drug Administration has warned against it. If a second agent is needed after a reasonable interval, choose an agent from a different class where possible, give it sequentially, and increase the intensity of monitoring. [8]
The Behavioural Activity Rating Scale (BARS) is the bedside severity tool most quoted in the agitation literature. A score of 4 is the calm baseline; 5 is overactive with calming on request; 6 is acutely overactive not calming on request (the threshold for considering parenteral medication); 7 is violent. Repeating the BARS at intervals documents the response and supports the re-dose decision. [1]
Droperidol and haloperidol prolong the QT interval. An ECG is required before or after a dose in a child with a cardiac history, an electrolyte disturbance, concurrent QT-prolonging drugs, methamphetamine intoxication, or a high cumulative dose. A QTc of greater than 460 ms in males, greater than 470 ms in prepubescent children, or greater than 480 ms after puberty is concerning; a QTc of greater than 500 ms is high risk for torsades de pointes and warrants cardiology review. [8] [9]
Antipsychotic-naive children have a high rate of adverse effects; the ETAPE study documented the incidence in the first weeks of treatment. Start low, titrate, monitor, and warn the family. [11]
Physical restraint is a last-resort, time-limited, team-delivered, leader-named, documented and debriefed intervention. A child in restraint is never face-down and never in a hobble; the airway is visible at all times; vital signs and mental state are checked continuously; the restraint is reassessed at least every 15 minutes. [1]
A restrained child is a vulnerable child. A safeguarding review is automatic for any child in care and for any unexplained or repeated restraint. The restraint event is a reportable clinical event under the local framework and under the relevant mental health legislation. [1] [7]
The term "excited delirium" is contested and has been withdrawn by major colleges. The clinical lesson is independent of the label: a hyperactive, severely agitated patient with autonomic dysregulation is in a medical emergency with risk of cardiovascular collapse, and must be treated as such. [7]
Australian states and territories each have their own Mental Health Act and Guardianship Act; Aotearoa New Zealand operates under the Mental Health (Compulsory Assessment and Treatment) Act 1992. Know your jurisdiction's forms and thresholds for emergency treatment without consent before you need them, and involve the on-call mental health clinician early. [1]
Autistic meltdown is physiological, not behavioural. Sensory regulation, communication aids and a trusted adult are first-line; escalation worsens the trajectory. A child with a known positive behaviour support plan is managed through that plan first. [6]
Benzodiazepines can cause paradoxical disinhibition in children, especially those with intellectual disability. Choose an atypical antipsychotic first when the driver is developmental. [1]
Weight-based dosing is mandatory. Estimate weight from a length-based tape if unknown, then weigh the child as soon as it is safe. A drug given without a weight in a child is an error waiting to happen. [1]
Post-sedation monitoring minimum: oxygen saturation, respiratory rate, sedation score every 15 minutes for at least one hour; blood pressure and heart rate at the same interval; ECG if a high-risk agent or dose. Have naloxone and flumazenil available if an opioid or benzodiazepine has been given. [1]
Debrief after every restrictive intervention: with the child when able, with the family, and with the team. Update the behavioural care plan. Notify per local restraint reporting. The debrief is part of the treatment, not an optional add-on. [11]
[1]References
- [1]Hilt, Robert J; Woodward, Thomas A Agitation treatment for pediatric emergency patients Journal of the American Academy of Child and Adolescent Psychiatry, 2008.PMID 18216715
- [2]TREC Collaborative Group Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine BMJ, 2003.PMID 14512476
- [3]Bourke, Elin M; Borland, Edith M; Phillips, Richard; et al Pharmacological emergency management of agitation in children and young people: protocol for a randomised controlled trial of oral medication (PEAChY-O) BMJ Open, 2023.PMID 36997250
- [4]Bourke, Elin M; Kochar, Ajit; Phillips, Richard; et al PEAChY-O: Pharmacological Emergency Management of Agitation in Children and Young People: A Randomized Controlled Trial of Oral Medication Annals of Emergency Medicine, 2025.PMID 39955661
- [5]Brasel, Kathryn; LaScala, Enza Pharmacotherapy for Agitation Management in a Pediatric Emergency Department Pediatric Emergency Care, 2025.PMID 39841042
- [6]Bourke, Elin M; Say, Daniel F; Anderson, Vikki; et al Emergency mental health presentations in children with autism spectrum disorder and attention deficit hyperactivity disorder Journal of Paediatrics and Child Health, 2021.PMID 33963626
- [7]Malashock, Hannah R; Yeung, Cynthia; Chai, Paul R; et al Pediatric Methamphetamine Toxicity: Clinical Manifestations and Therapeutic Use of Antipsychotics-One Institution's Experience Journal of Medical Toxicology, 2021.PMID 33442836
- [8]Hilt, Robert J Editorial: Best Practices in Child Antipsychotic Use Monitoring Journal of the American Academy of Child and Adolescent Psychiatry, 2021.PMID 33176169
- [9]Scott, James P; Stuth, Eckhard A; Stucke, Andreas G; et al Droperidol transiently prolongs the QT interval in children undergoing single ventricle palliation Pediatric Cardiology, 2015.PMID 25087057
- [10]Minghetti, Silvia; Vannini, Mara; Pellegrino, Paola; et al Epidemiological and Psychopharmacological Study About Off-Label Treatment in Child and Adolescent Psychiatric Emergencies: A Tertiary/Single Center Experience Pediatric Emergency Care, 2022.PMID 35686968
- [11]Menard, Marie Laurence; Thummler, Sylvie; Giannitelli, Manuel; et al Incidence of adverse events in antipsychotic-naive children and adolescents treated with antipsychotic drugs: Results of a multicenter naturalistic study (ETAPE) European Neuropsychopharmacology, 2019.PMID 31699516
- [12]Menard, Marie Laurence; Auby, Pauline; Cruzel, Charlotte; et al Emergence of psychiatric adverse events during antipsychotic treatment in AP-naive children and adolescents Child and Adolescent Psychiatry and Mental Health, 2022.PMID 36371250