Paeds · acute-care-resuscitation-and-toxicology
Hydrocarbon, caustic and household chemical exposure
Also known as Petroleum distillate ingestion in children · Hydrocarbon aspiration pneumonitis · Caustic ingestion in children · Alkali and acid corrosive ingestion · Household cleaner and detergent exposure
A fellowship approach to paediatric hydrocarbon, caustic and household chemical exposure. First identify the product. A hydrocarbon (petroleum distillate) threatens by aspiration, so never induce emesis, never lavage, and observe for six hours. A caustic agent threatens by corrosive injury, so keep nil by mouth, never neutralise, and arrange early endoscopy within twenty-four hours. Corticosteroids and prophylactic antibiotics are not routine. Call the poisons information centre early and tailor every rule to the product and the local protocol.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Household chemical exposure in a child is one of the most common presentations to paediatric emergency care, and the single most important skill is not memorising antidotes but reading the situation by the product. The product decides the dominant threat, the decontamination rule, the observation period and the need for endoscopy. A child who swallowed lamp oil is not the same as a child who swallowed drain cleaner, and a child who swallowed low-concentration household bleach is not the same as either. Grouping them as "poisoning" without separating the chemical class is the first and most dangerous error. [1] [6]
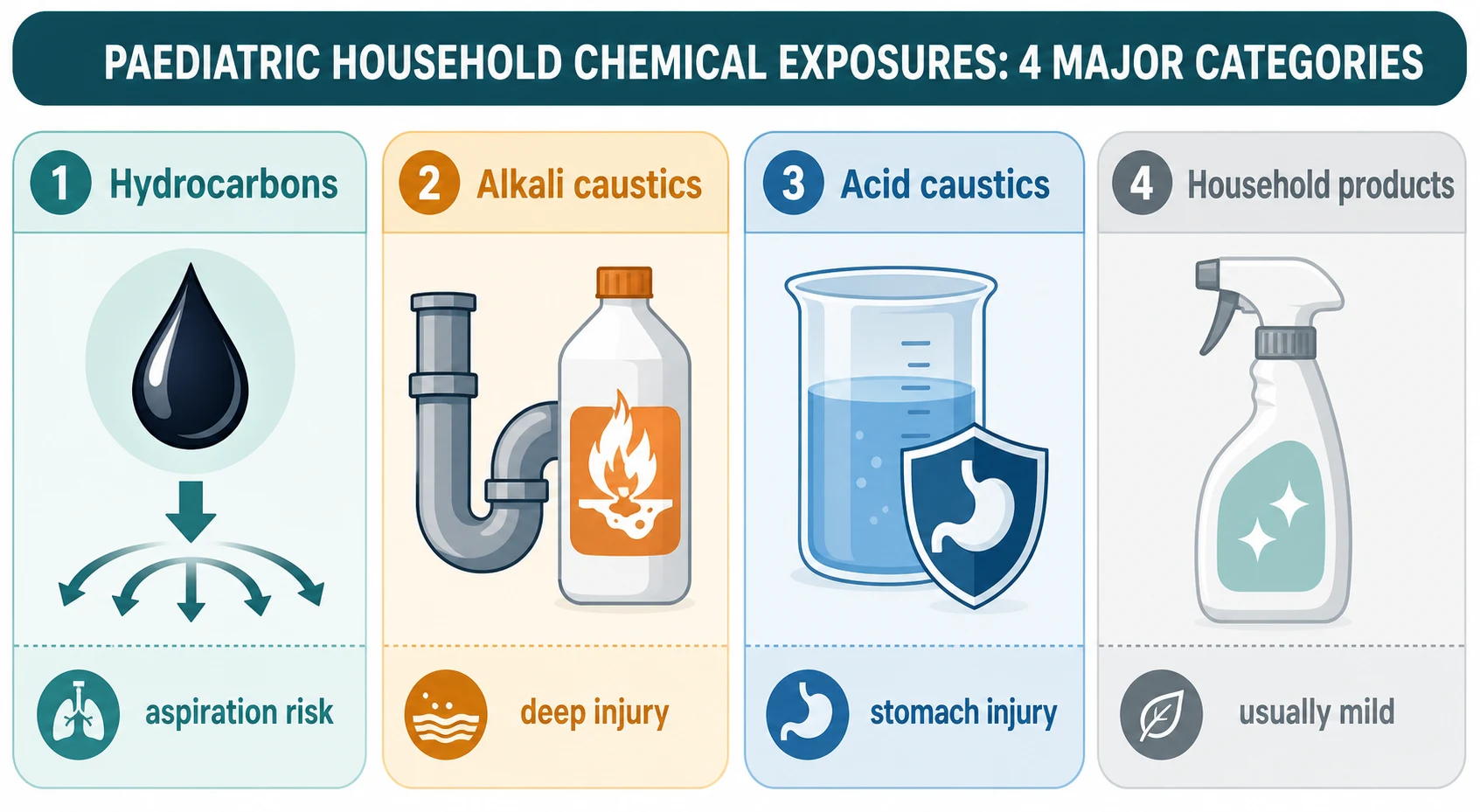
Three chemical classes account for almost all serious paediatric household exposure. Hydrocarbons are petroleum distillates (petrol, kerosene, lamp oil, lighter fluid, mineral spirits, turpentine) and some volatile solvents; their danger is aspiration, because their low viscosity and low surface tension let them spread into the alveoli and cause a chemical pneumonitis. Caustic agents are strong alkalis (sodium and potassium hydroxide in drain cleaners, oven cleaners, dishwasher tablets) and strong acids (sulfuric, hydrochloric, sulfamic acid in toilet bowl cleaners, battery acid, rust removers); their danger is corrosive injury of the gastrointestinal tract. The third class, low-concentration household products (household bleach, detergents, disinfectants), is usually only irritant and rarely causes serious injury unless the agent is concentrated, a capsule formulation, or a large volume is taken. [1] [2]
The shared principle that runs through every pathway is restraint. The interventions that are contraindicated here are as important as the ones that are indicated. Induced emesis, gastric lavage for hydrocarbons, and neutralisation of caustics each convert a contained exposure into a worse one. The modern approach is therefore supportive and product-specific: secure the airway and breathing, avoid the harmful reflexes of decontamination, observe or endoscope as the product demands, and call the poisons information centre early to confirm the product-specific rule. [1] [6]
Classification
Household chemical exposures are best classified by the chemical class, because the class decides the dominant injury pattern and the management pathway. Two questions sort almost every case: is the agent a hydrocarbon, and is it a caustic? [1] [5]
Hydrocarbons (petroleum distillates)
Aspiration is the threat
- Petrol, kerosene, lamp oil, lighter fluid, mineral spirits, turpentine
- Low viscosity and low surface tension allow rapid spread into the alveoli
- Lung injury is chemical pneumonitis, not systemic absorption
- Lamp oil carries one of the highest aspiration hazards and the worst outcomes
Alkali caustics
Liquefaction necrosis
- Sodium or potassium hydroxide in drain cleaners, oven cleaners, dishwasher tablets
- Saponifies fats and dissolves proteins, penetrating deeply through the oesophageal wall
- Oesophageal injury is usually worse than gastric injury
- High risk of stricture and of perforation in severe burns
Acid caustics
Coagulation necrosis
- Sulfuric, hydrochloric or sulfamic acid in toilet bowl cleaner, battery acid, rust remover
- Denatures protein into a firm coagulum (eschar) that tends to limit penetration
- The stomach rather than the oesophagus usually bears the brunt
- Systemic acidosis and gastric perforation are the dangerous complications
Low-concentration household products
Usually irritant only
- Household bleach below about 5 to 10 per cent sodium hypochlorite, dilute detergents, disinfectants
- Typically mild gastrointestinal or oral irritation
- Serious injury is uncommon unless the agent is concentrated, a capsule, or a large volume is taken
- Often managed by observation alone after a careful assessment
Two features of the product modify the class and deserve emphasis. The concentration changes everything within a class: household bleach at about 5 per cent sodium hypochlorite is usually only an irritant, whereas industrial bleach concentrate behaves like a caustic. The formulation matters as much as the concentration: liquid laundry detergent capsules and concentrated dishwasher tablets carry a disproportionate risk of severe injury, airway compromise and central-nervous-system depression compared with powder or dilute liquid formulations. Reading the container, not the label the carer remembers, is how these distinctions are made. [7] [11]
Epidemiology & Risk Factors
Accidental household chemical exposure is one of the leading reasons a young child is assessed for poisoning, and the pattern is driven overwhelmingly by age and access. Exploratory ingestion peaks in the toddler and preschool years, when mobility and mouthing behaviour meet unsafe storage. The single most reliable risk factor is access to the product: an open bottle, a decanted liquid in a food or drink container, or cleaning products stored at floor level within a child's reach. [2] [11]
Within the broad category, certain products are repeatedly associated with severe injury, and knowing them sharpens the assessment. Lamp oil, with its very low viscosity and low surface tension, carries one of the highest aspiration hazards and disproportionately poor outcomes. Concentrated industrial alkalis (drain cleaners, oven cleaners, dishwasher tablets) cause deep oesophageal necrosis. Liquid laundry detergent capsules cause a cluster of airway compromise, central-nervous-system depression and severe oesophagogastritis that is out of proportion to their size. The COVID-19 era produced a measurable surge in paediatric household cleaning product exposures as more concentrate was stored in the home, which is why product trends matter to the contemporary examiner. [9] [11]
Product factors
- Lamp oil and other very low-viscosity hydrocarbons
- Concentrated industrial alkalis (drain cleaner, oven cleaner, dishwasher tablet)
- Liquid laundry detergent capsules
- Acids in toilet bowl cleaner, battery acid or rust remover
Host and access factors
- Toddler or preschool age with exploratory behaviour
- Unsafe storage at child height or in unmarked containers
- Decanting cleaning products into food or drink containers
- Developmental disability or neurodiversity with reduced hazard awareness
System and context factors
- Increased home storage of cleaning concentrate during the COVID-19 pandemic
- Inadequate child-resistant packaging or flow restrictors
- Rural or remote location with delayed access to toxicology and surgical advice
- Carer misunderstanding of the product or its concentration
Most exposures are small-volume accidental ingestions by young children and do well with observation, but the children who come to harm are those who took a high-risk product (lamp oil, concentrated alkali, detergent capsule), presented after a delay, or deteriorated within the observation window. A minority are intentional ingestions by adolescents, where the volume is often larger, the product more dangerous, and the safeguarding and mental health response runs in parallel. [2] [11]
Pathophysiology
Understanding the mechanism of each chemical class turns the management rules from rote learning into logic. Hydrocarbons injure the lung because they spread; caustics injure the gut because they dissolve tissue; and the two mechanisms explain every contraindication in the topic. [1] [8]
A hydrocarbon threatens the lung, not the stomach. Petroleum distillates have a very low viscosity and a very low surface tension, so when even a small volume reaches the airway (by aspiration during swallowing, by reflux, or by vomiting), it does not pool. Instead it spreads rapidly across the alveolar surface, disrupts the surfactant layer, injures the alveolar-capillary membrane and sets off an intense inflammatory chemical pneumonitis. This is why aspiration, not systemic absorption, is the dominant threat, and why anything that provokes vomiting or lavage (which can precipitate aspiration) is contraindicated. Lung injury usually declares itself within the first six hours, which is the basis for the observation period. [8] [9]
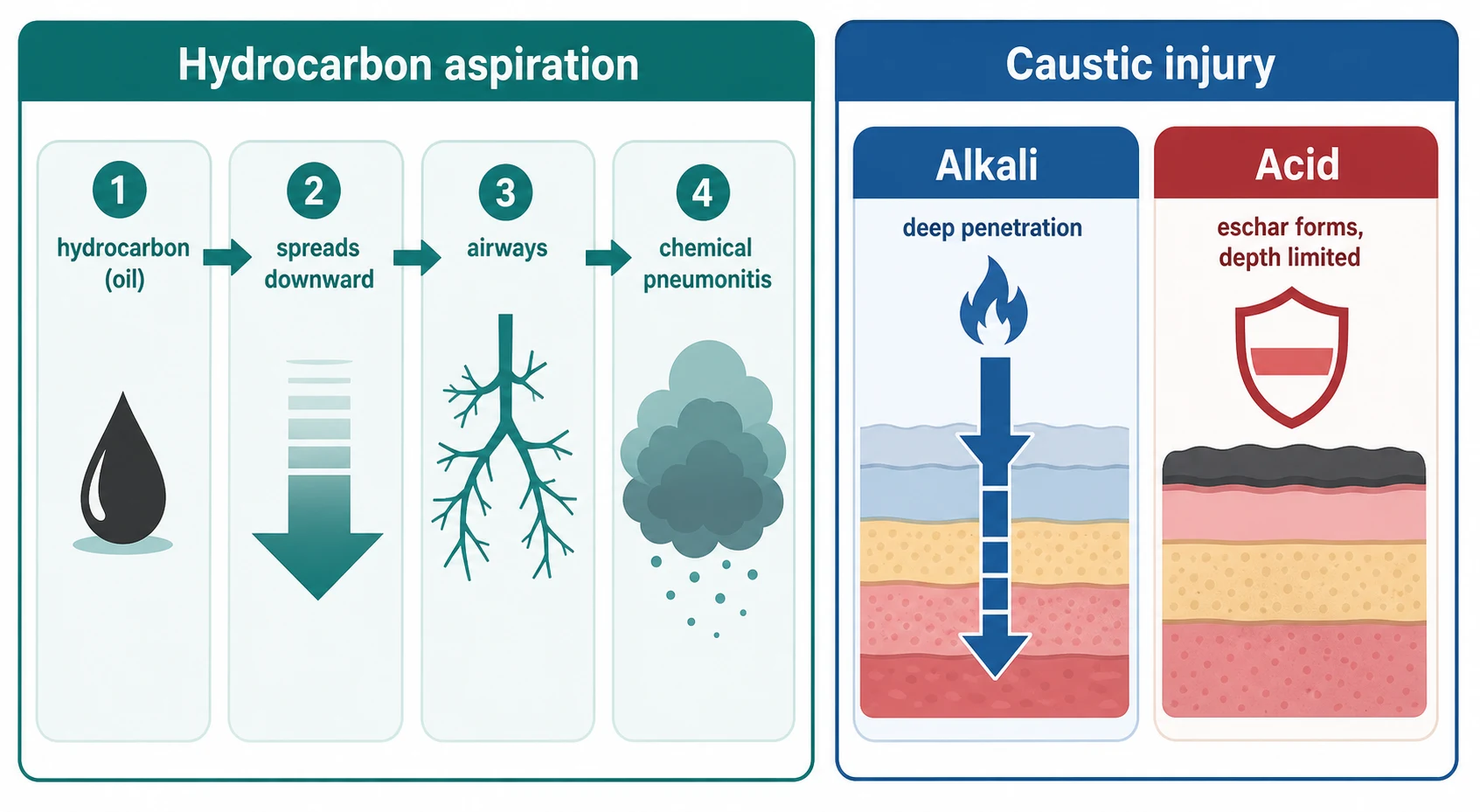
A caustic agent threatens the gastrointestinal tract, and the pattern of injury depends on whether it is an alkali or an acid. Alkalis (hydroxides) saponify fats and dissolve proteins, producing liquefaction necrosis that penetrates deeply through and beyond the oesophageal wall; this is why alkali ingestions characteristically cause severe oesophageal injury, strictures and perforation. Acids denature protein into a firm coagulum, an eschar, which tends to limit the depth of penetration, so acid ingestions characteristically spare the oesophagus and burn the stomach instead. The eschar is protective in the short term but can slough later. Understanding this explains why the surgical risk and the endoscopy grade differ between the two. [1] [3]
Some agents carry extra-systemic toxicity beyond their class effect, and these must be sought from the product history. Camphor (in some mothballs and vapour products) causes seizures. Halogenated hydrocarbons and aromatic hydrocarbons (benzene, toluene, chlorinated solvents) can cause hepatic, cardiac and central-nervous-system toxicity. Methaemoglobinaemia follows aniline and nitrobenzene. These extras do not replace the class pathway; they run alongside it and change the monitoring. [1] [6]
Clinical Presentation
The presentation is deceptively reassuring in the first hour, and this is the trap. A child who has taken a dangerous product is often well immediately afterwards, because the injury has not yet declared itself. The product and the observation period, not the early symptoms, drive the risk. [1] [6]
A hydrocarbon ingestion presents first with coughing, choking or gagging at the moment of aspiration, sometimes with vomiting. Over the next six hours the respiratory features evolve: tachypnoea, increased work of breathing, wheeze, crackles, and falling oxygen saturation. Fever may accompany the inflammatory pneumonitis. A child who is breathing comfortably at six hours, with normal oxygen saturation and a normal or unchanged chest X-ray, is very unlikely to develop serious lung injury thereafter. A child who coughs and vomits at the scene, or who becomes tachypnoeic during the observation, is signalling aspiration and needs escalation. [8] [9]
[8]A caustic ingestion presents with immediate pain, drooling, refusal to swallow, and vomiting, sometimes with haematemesis. Oral and oropharyngeal burns may be visible, and stridor or a muffled voice suggests airway involvement. Chest pain points to oesophageal injury; abdominal pain and guarding point to gastric injury or perforation. The dangerous corollary is that the oropharynx can look entirely normal while the oesophagus or stomach is deeply burned, so the presence of oral burns predicts severe injury but their absence does not exclude it. [1] [3]
Atypical and deceptive presentations deserve emphasis. The toddler found beside an open bottle with an unknown amount taken may look well and still deteriorate. The well-looking child after lamp oil can develop pneumonitis at six hours. The detergent-capsule ingestion can present with central-nervous-system depression and airway compromise rather than gastrointestinal signs. Each of these is a reason to trust the product and the observation period over the first impression. [9] [11]
Differential Diagnosis
When a child arrives symptomatic after a suspected chemical exposure, build the differential by the dominant threat and by what else could cause the same picture. The product history is the most discriminating single piece of information, but the differential guards against attributing everything to the wrong agent. [1] [5]
Respiratory mimics of hydrocarbon pneumonitis
- Viral or bacterial pneumonia with a coincident or preceding illness
- Bronchiolitis in an infant or toddler
- Foreign-body aspiration (including a button battery in the airway)
- Asthma or viral-induced wheeze
Surgical and caustic emergencies
- Oesophageal or gastric perforation with mediastinitis or peritonitis
- Button-battery impaction in the oesophagus causing caustic-like injury
- Foreign-body impaction with secondary inflammation
- Ingestion of a sharp object with mucosal laceration
Co-ingestion and systemic toxicity
- Co-ingested medication or recreational drug altering the conscious level
- Pesticide or hydrocarbon with systemic toxicity (camphor seizures, methaemoglobinaemia)
- Carbon monoxide or inhalational injury from a fire or heater
- An intentional overdose with a more dangerous co-ingestant
Irritant-only and benign exposures
- Low-concentration household bleach or detergent exposure
- Cosmetic or personal-care product ingestion
- Plant or low-toxicity substance exposure
- Usually managed by observation after a careful assessment
The practical point is that a symptomatic child after a caustic ingestion is presumed to have a significant injury until endoscopy shows otherwise, and a symptomatic child after a hydrocarbon ingestion is presumed to have evolving pneumonitis until the observation period and the chest X-ray settle the question. The button battery is the classic mimic of a caustic ingestion, because lodged batteries generate the same liquefaction necrosis; an urgent lateral neck and chest X-ray excludes an oesophageal battery when the history is uncertain. [1] [6]
Clinical & Bedside Assessment
Assessment begins with the airway, breathing and circulation of any poisoned child, then moves immediately to the single most useful act in this topic: identifying the product. The container is more valuable than any blood test. [1] [6]
Take a focused exposure history built around the product: the exact name and type of agent, its concentration and formulation, the estimated volume ingested, the time of exposure, the route (ingestion, inhalation, dermal or ocular), and any co-ingestant. Ask the carer to bring the container, and read the label yourself rather than relying on a remembered name, because the formulation (a capsule, a concentrate, an industrial strength) changes the risk more than the brand. Document the source of the history and confirm the product against a poisons database early. [2] [6]
[1]The examination then follows the dominant threat. For the hydrocarbon-exposed child, focus on the respiratory system: respiratory rate, work of breathing, oxygen saturation, auscultation, and the trend over the observation period. For the caustic-exposed child, focus on the airway first (stridor, drooling, voice), then the oropharynx, then the abdomen for tenderness or guarding that suggests perforation. For any dermal or ocular exposure, examine the affected tissue and begin copious irrigation immediately if the agent is a caustic or irritant. [1] [3]
A collateral history from carers, ambulance staff and the home setting is often decisive, especially when the amount is uncertain. Confirm the bottle, the label, the missing volume and whether the product was decanted. Use a professional interpreter whenever needed. Safeguarding assessment runs in parallel, because accidental access to unsafe storage, a therapeutic or cleaning error, and intentional self-harm each carry a different safety response. [2] [11]
Investigations
Investigations answer three questions: is there pulmonary injury, is there gastrointestinal injury or perforation, and is there a co-ingestant or systemic toxicity. Order each test for a named question, and do not over-investigate the well-looking child with a low-toxicity exposure. [1] [3]
Immediate and bedside
- Oxygen saturation and work of breathing monitored over the observation period (hydrocarbon)
- Point-of-care glucose for the drowsy or seizing child
- Blood gas and lactate for respiratory distress or systemic toxicity
- Pregnancy test in adolescent females
Core laboratory
- Chest X-ray for any symptomatic hydrocarbon exposure (may lag symptoms)
- Full blood count, electrolytes, acid-base and lactate for a significant caustic exposure
- Coagulation and group and hold before endoscopy or surgery
- Drug screen and paracetamol level when co-ingestion is suspected
Advanced and targeted
- Therapeutic endoscopy within twenty-four hours for a significant caustic ingestion
- Contrast swallow or computed tomography for suspected perforation, late presentation or fistula
- Lateral neck and chest X-ray to exclude a button battery when the history is uncertain
- Methaemoglobin level for aniline or nitrobenzene exposure
Interpret the chest X-ray with caution after a hydrocarbon ingestion. The classic finding is a chemical pneumonitis with bibasal or multilobar infiltrates, but radiographic changes can lag behind symptoms by hours. A normal early film does not exclude evolving lung injury; repeat it if symptoms develop or at the end of the observation period. For the caustic-exposed child, free air under the diaphragm on an erect chest or abdominal film suggests perforation and demands urgent surgical review. [8] [9]
The endoscopy is the decisive investigation in caustic ingestion. Its purpose is twofold: to grade the burn and so predict stricture and perforation risk, and to guide the feeding and surgical plan. The Zargar endoscopic classification grades the injury from grade zero (normal) through grade one (mucosal oedema and hyperaemia), grade two-a (superficial ulcers, bleeding, exudate), grade two-b (deep or discrete ulcers, friability, pseudomembrane), grade three-a (transmural ulcers with focal necrosis), to grade three-b (extensive necrosis). Grade three injuries predict stricture and perforation and define the group needing surgical readiness and long-term surveillance. [1] [4]
Management — Resuscitation
Resuscitation follows the standard poisoned-patient primary survey, then moves to the product-specific pathway. The first hour secures the airway, breathing and circulation, identifies the product, and institutes the contraindications that are as important as the active treatment. [1] [6]
The first hours in household chemical exposure
Primary survey and product identification
Secure the airway, breathing and circulation as for any poisoned child, and give oxygen for hypoxaemia. Identify the exact product and concentration from the container, read the label yourself, and call the poisons information centre with the product in hand.
Apply the contraindications
Do not induce emesis in any hydrocarbon or caustic ingestion. Do not perform gastric lavage for a hydrocarbon. Do not neutralise a caustic agent with a weak acid or alkali. These interventions worsen the injury and are never indicated as routine.
Decontaminate only where indicated
Activated charcoal does not bind hydrocarbons or caustics and is not indicated. For a dermal or ocular caustic exposure, begin copious irrigation with water or saline immediately and continue for at least fifteen to twenty minutes.
Start the product pathway
For a hydrocarbon, begin six-hour observation with monitoring of oxygen saturation and work of breathing, and a chest X-ray if symptomatic. For a caustic, keep the child nil by mouth, establish intravenous access, and arrange early endoscopy within twenty-four hours for a significant ingestion.
Escalate for deterioration
Escalate to intensive care for respiratory failure or airway compromise after a hydrocarbon, and to surgical and intensive care for suspected perforation or extensive necrosis after a caustic. Give a structured handover of the product, the time, the course and the current physiology.
Call the poisons centre
Contact the local poisons information centre early (Australia 13 11 26; New Zealand 0800 POISON; UK NPIS via Toxbase; US 1-800-222-1222). The observation period, endoscopy timing and product-specific rules are confirmed against the local protocol.
Why induced emesis, lavage and neutralisation are contraindicated
The contraindications follow directly from the mechanism. Induced emesis in a hydrocarbon ingestion converts a contained small-volume exposure into a large-volume aspiration, the very injury the management is trying to prevent; the same applies to gastric lavage, which provokes coughing and aspiration. Neutralising a caustic agent is contraindicated because the neutralisation reaction is exothermic and produces heat that worsens the burn, and acid-alkali reactions release gas that can distend and rupture an already damaged stomach. Activated charcoal does not adsorb hydrocarbons or caustics effectively and is not indicated. These are not optional refinements; they are the spine of safe care. [1] [8]
When ABCDE becomes advanced life support
A child who becomes comatose after a detergent-capsule ingestion, who loses the airway with drooling and stridor after a caustic, or who develops respiratory failure after a hydrocarbon aspiration needs immediate resuscitation and intensive care. If the child arrests, the paediatric arrest-dose anchors apply: intravenous or intraosseous adrenaline at 10 micrograms per kilogram (0.1 millilitres per kilogram of 1 in 10,000 adrenaline) every three to five minutes, and defibrillation at 4 joules per kilogram for a shockable rhythm. The full algorithm lives in the paediatric basic and advanced life support topic. [1]
[1] [8]Management — Definitive & Stepwise
Once the primary survey and the contraindications are in place, definitive management follows the product pathway. For a hydrocarbon the pathway is supportive and respiratory; for a caustic it is endoscopic and surgical. Corticosteroids and prophylactic antibiotics are not routine. [1] [6]
The hydrocarbon pathway
The hydrocarbon pathway is built around the six-hour observation. Observe every child with a definite hydrocarbon ingestion for six hours, monitoring the oxygen saturation and the work of breathing throughout. Perform a chest X-ray if the child becomes symptomatic, and at the discretion of the local protocol at the end of the observation period. A child who remains asymptomatic at six hours, with normal oxygen saturation and a normal or unchanged chest X-ray, can be discharged with a clear safety net. A child who develops respiratory symptoms, hypoxaemia or radiographic changes during the observation is admitted and treated with supportive respiratory care. [8] [9]
| Stage | Findings | Action |
|---|---|---|
| Asymptomatic at 6 hours | Normal oxygen saturation, normal or unchanged chest X-ray | Discharge with a safety net and poison-prevention advice |
| Mild respiratory symptoms | Tachypnoea, wheeze or crackles with acceptable oxygen saturation | Admit for supportive care and supplemental oxygen as needed |
| Moderate to severe | Hypoxaemia, marked work of breathing or respiratory failure | High-flow or non-invasive support; intensive care; consider mechanical ventilation |
| Refractory lung injury | Severe acute respiratory distress syndrome unresponsive to ventilation | Specialist retrieval; consider surfactant and extracorporeal membrane oxygenation |
Supportive respiratory care is the mainstay: supplemental oxygen for hypoxaemia, escalation to high-flow nasal therapy, non-invasive ventilation or mechanical ventilation for respiratory failure, and intensive care for the failing child. Corticosteroids are not recommended in hydrocarbon pneumonitis, because they do not improve outcome and add harm, and prophylactic antibiotics are not recommended, because the early illness is a chemical pneumonitis rather than an infection; treat proven secondary infection on its merits. In the rare case of refractory acute respiratory distress syndrome, lung-protective ventilation, surfactant and extracorporeal membrane oxygenation have been used successfully and warrant early specialist retrieval. [8] [10]
Supportive respiratory care in hydrocarbon pneumonitis (no specific antidote)
The caustic pathway
The caustic pathway is built around keeping the gut at rest and grading the injury endoscopically. Keep the child nil by mouth, establish intravenous access, give intravenous fluids and analgesia, and arrange early therapeutic endoscopy within twenty-four hours for any significant caustic ingestion. Do not neutralise, do not induce emesis, and do not give activated charcoal. A proton pump inhibitor is commonly given where mucosal injury is present, on the rationale of reducing acid load on the damaged mucosa, but it does not substitute for endoscopy and surgical readiness. [1] [3]
| Stage | Endoscopy grade | Management |
|---|---|---|
| No injury | Zargar grade 0 | Observe, advance diet as tolerated, discharge with advice |
| Superficial injury | Zargar grade 1 to 2a | Nil by mouth then graded diet, analgesia and proton pump inhibitor; observe for stricture |
| Deep injury | Zargar grade 2b to 3a | Nil by mouth, nasoenteric feeding if prolonged, surgical consultation; high stricture risk and surveillance |
| Extensive necrosis or perforation | Zargar grade 3b or free air | Urgent surgical review, broad-spectrum antibiotics for perforation, intensive care; high mortality |
The timing of endoscopy matters and is an examiner favourite. Endoscopy is best performed between six and twenty-four hours after ingestion. Before six hours the full depth of injury may not yet be apparent and the grade can be underestimated; after twenty-four hours the oedema and weakening of the wall raise the risk of iatrogenic perforation from the instrument. Endoscopy is deferred if there is suspected perforation, in which case a contrast study or computed tomography is preferred and surgery is involved. The endoscopy grade then drives the feeding plan, the need for a feeding tube, and the long-term surveillance for stricture. [1] [4]
Goals and monitoring
Set explicit endpoints. For the hydrocarbon pathway the targets are a stable, comfortable child with normal oxygen saturation and resolving radiographic changes. For the caustic pathway the targets are successful graded re-introduction of feeding, absence of perforation, and a surveillance plan for stricture in those with grade two-b or three injuries. Continue monitoring in a setting matched to severity, from observation for the well child to intensive care for established respiratory or multisystem failure. [3] [4]
Specific Subtypes & Scenarios
The resuscitation structure stays the same, but the product class, the concentration and the formulation change the observation, the endoscopy and the surgical readiness. [1]
Hydrocarbon ingestion
- Six-hour observation with oxygen saturation and work-of-breathing monitoring
- Chest X-ray if symptomatic; may lag symptoms early
- Supportive respiratory care; no routine steroids or antibiotics
- Discharge at six hours if asymptomatic with normal saturation and a clear safety net
Alkali caustic ingestion
- Dishwasher tablet, drain cleaner, oven cleaner, button battery
- Keep nil by mouth; early endoscopy within twenty-four hours
- Deep oesophageal injury with high stricture and perforation risk
- Surgical readiness and long-term stricture surveillance for deep burns
Acid caustic ingestion
- Toilet bowl cleaner, battery acid, rust remover
- Predominant gastric injury with a protective eschar
- Watch for systemic acidosis and gastric perforation
- Endoscopy within twenty-four hours; surgical readiness
Household bleach ingestion
- Low-concentration sodium hypochlorite is usually only an irritant
- Often managed by observation after a careful assessment
- Industrial concentrate behaves like a caustic and follows that pathway
- Endoscopy is reserved for symptomatic or large-volume exposure
Laundry detergent capsule
- Disproportionate risk of severe injury relative to size
- Central-nervous-system depression and airway compromise may dominate
- Severe oesophagogastritis possible; observe and escalate early
- Higher acuity of monitoring than for powder or dilute detergent
Dermal or ocular exposure
- Begin copious irrigation with water or saline immediately
- Continue for at least fifteen to twenty minutes
- Ocular alkali burn is an emergency: irrigate and seek urgent ophthalmology
- Assess for cutaneous burns after irrigation
Two scenarios deserve particular caution. A laundry detergent capsule ingestion is treated with a higher acuity than a powder exposure, because capsules are repeatedly associated with airway compromise, central-nervous-system depression and severe oesophagogastritis; observe these children closely and escalate early. An ocular caustic exposure is a true emergency, because alkali penetrates and destroys the cornea within minutes: begin copious irrigation immediately and continue for at least fifteen to twenty minutes, checking the pH, and seek urgent ophthalmology review. [9] [11]
Complications & Pitfalls
Most preventable harm in paediatric household chemical exposure comes from one of five errors: inducing emesis, performing gastric lavage on a hydrocarbon, neutralising a caustic, discharging a hydrocarbon-exposed child before the six-hour observation, and omitting or delaying endoscopy after a significant caustic ingestion. Each is a failure to apply the product pathway, not a failure of memory. [1] [6]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Inducing emesis | Converts a contained exposure into aspiration (hydrocarbon) or repeated mucosal injury (caustic) | Never induce emesis in a hydrocarbon or caustic ingestion |
| Gastric lavage of a hydrocarbon | Provokes coughing and aspiration into the lung | Do not lavage hydrocarbons; supportive care and observation instead |
| Neutralising a caustic | Exothermic reaction and gas production worsen the burn and risk perforation | Keep nil by mouth; no neutralisation; arrange early endoscopy |
| Discharging before six hours | Hydrocarbon pneumonitis can declare itself up to six hours after exposure | Observe for the full six hours with saturation monitoring before discharge |
| Omitting or delaying endoscopy | Deep caustic burns and perforation are missed, and stricture surveillance is not planned | Endoscope significant caustic ingestions between six and twenty-four hours |
| Reassured by normal early chest X-ray | Radiographic changes lag behind symptoms in hydrocarbon pneumonitis | Base escalation on saturation, work of breathing and the clinical course |
| Reassured by absent oral burns | The oesophagus can be deeply burned while the mouth looks normal | Presume significant caustic injury until endoscopy excludes it |
| Missing a button battery | A lodged battery mimics and causes caustic injury | Image with a lateral neck and chest X-ray when the history is uncertain |
Pulmonary complications follow hydrocarbon aspiration: chemical pneumonitis, acute respiratory distress syndrome, secondary bacterial infection, pneumatocele, pneumothorax and, less often, bronchiolitis obliterans. Caustic complications include oesophageal and gastric perforation with mediastinitis or peritonitis, oesophageal and gastric strictures, fistula, and a markedly increased lifetime risk of oesophageal cancer decades after a deep burn. A child who survives a deep caustic injury needs long-term surveillance, not just acute care. [1] [3]
[1] [3]Prognosis & Disposition
Disposition follows the product, the concentration, the clinical course and the social and safeguarding context. Most low-toxicity household exposures do well with observation; the children who do badly are those who took a high-risk product, presented after a delay, or deteriorated within the observation window. [2] [11]
Intensive care or retrieval
- Respiratory failure or airway compromise after a hydrocarbon aspiration
- Deterioration from a detergent-capsule ingestion with CNS depression
- Extensive necrosis or perforation after a caustic ingestion
- Refractory acute respiratory distress syndrome needing surfactant or ECMO
Ward or surgical admission
- Persistent respiratory symptoms after a hydrocarbon at six hours
- A caustic ingestion awaiting endoscopy or after a grade two to three burn
- Persistent pain, drooling or inability to feed
- A large-volume or high-concentration exposure under observation
Observation and discharge
- Asymptomatic at six hours after a hydrocarbon with normal saturation and a normal or unchanged chest X-ray
- A well child after a low-concentration household bleach or irritant exposure
- No co-ingestant and no safeguarding or mental health concern
- Carer understands the safety net and poison-prevention advice
Mortality from household chemical exposure is low when the product pathway is followed, but it is not zero: large-volume lamp-oil aspiration, concentrated industrial alkali with perforation, and detergent-capsule ingestion with airway compromise are the dangerous presentations. After a deep caustic burn the prognosis extends well beyond the acute admission, because strictures, nutritional compromise and late oesophageal malignancy demand years of surveillance. Give every family a clear safety net: what change to watch for, how urgently to act, and exactly where to return. [1] [3]
Special Populations
Adapt how you take the history, how you observe and how you escalate, but never lower the standard for the product pathway. The principles apply across ages and abilities; the differences are in access, communication, formulation risk and the social context. [2]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Toddler and preschool child | Exploratory ingestion is common and the amount is almost always uncertain; observe the full six hours and trust the product | Do not discharge early because the child looks well |
| Adolescent | Intentional ingestion may involve a large volume and a dangerous co-ingestant; take the history privately and sensitively | Do not rely on the adolescent's reported amount alone |
| Child with disability or neurodiversity | Compare with the caregiver's baseline; explore accidental access and unsafe storage; use adapted communication | A changed behaviour or feeding pattern may be the only sign |
| Dermal or ocular exposure | Begin copious irrigation immediately for a caustic or irritant; check ocular pH and seek urgent ophthalmology for alkali burns | Do not delay irrigation to obtain a history |
| Indigenous, migrant or refugee background | Use professional interpreters; respect cultural and family structures; address access and storage barriers | Apply local consent and mandatory-reporting rules |
Safeguarding runs in parallel with medical care, and immediate stabilisation comes first. Accidental access to unsafe storage, a cleaning-product error by a carer, and intentional self-harm each carry a different safety response. Ask only necessary open, non-leading questions, document objective findings and spontaneous words, and use the local safeguarding and mental health pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [11]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The structure of management is strongly endorsed across the major toxicology sources: secure the airway, identify the product, never induce emesis, never lavage a hydrocarbon, never neutralise a caustic, observe the hydrocarbon-exposed child for six hours, and endoscope the significant caustic ingestion within twenty-four hours. What remains less certain is the role of corticosteroids after deep caustic injury and the place of novel rescue therapies in refractory hydrocarbon pneumonitis, which are used selectively rather than routinely. [1] [6]
Ingestion of caustic substances (NEJM review)
New England Journal of Medicine
Landmark narrative review of the pathophysiology, assessment and management of caustic ingestion
Key finding
Caustic injury is determined by the agent, its concentration and its volume; endoscopy between six and twenty-four hours grades the burn and predicts stricture and perforation risk; neutralisation, induced emesis and activated charcoal are contraindicated.
Practice change
Established the modern standard of no neutralisation, no emesis, and timed endoscopy for caustic ingestion across international guidelines.
The FISPGHAN expert panel on paediatric ingestions and recent narrative reviews consolidate the contemporary approach across regions, emphasising early endoscopy for caustic injury, the avoidance of harmful decontamination, and the prevention of accidental access through child-resistant packaging and safe storage. The evidence against routine corticosteroids and prophylactic antibiotics in hydrocarbon pneumonitis is consistent, and recent work confirms that they do not improve outcome. [6] [8]
Steroids and antibiotics in acute hydrocarbon poisoning
Journal of Pharmacy Practice
Review of prophylactic corticosteroid and antibiotic use in children with acute hydrocarbon poisoning
Key finding
Prophylactic corticosteroids and antibiotics did not improve outcomes in hydrocarbon pneumonitis and are not recommended; the early illness is a chemical rather than an infective pneumonitis, and antibiotics should be reserved for proven secondary infection.
Practice change
Confirms that corticosteroids and prophylactic antibiotics are not routine in hydrocarbon pneumonitis.
Recent cohort and poison-data work sharpens the epidemiology and the high-risk products. National poison data show a measurable surge in paediatric household cleaning product exposures during the COVID-19 pandemic, driven by increased home storage of cleaning concentrate. Household bleach at usual concentrations is confirmed to be usually only an irritant in children, with endoscopy reserved for symptomatic or large-volume exposure, while concentrated formulations and detergent capsules carry disproportionate risk. [7] [11]
Jurisdictional implementation
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne chemical ingestion guideline and the Australian Therapeutic Guidelines (eTG) set the local pathway. The NSW Poisons Information Centre (13 11 26) should be called early; the New Zealand equivalent is the National Poisons Centre (0800 POISON). The observation period, endoscopy timing and product-specific rules follow the local protocol; verify them rather than borrowing an international threshold.
Exam Pearls
Recognition
- Identify the exact product from the container before anything else
- Classify as hydrocarbon, alkali caustic, acid caustic or low-concentration household product
- Hydrocarbon threat is aspiration; caustic threat is corrosive injury
- A well child can deteriorate within the observation window
Contraindications
- Never induce emesis in a hydrocarbon or caustic ingestion
- Never perform gastric lavage for a hydrocarbon
- Never neutralise a caustic agent
- Activated charcoal is not indicated for hydrocarbons or caustics
Hydrocarbon pathway
- Observe for six hours with oxygen saturation and work-of-breathing monitoring
- Chest X-ray if symptomatic; changes may lag symptoms
- Supportive respiratory care; no routine corticosteroids or antibiotics
- Discharge at six hours if asymptomatic with normal saturation and a clear safety net
Caustic pathway
- Keep nil by mouth; give intravenous fluids and analgesia
- Early endoscopy between six and twenty-four hours for a significant ingestion
- Zargar grade (0, 1, 2a, 2b, 3a, 3b) guides prognosis and the feeding plan
- Surgical readiness for suspected perforation or extensive necrosis
Pitfalls
- No early discharge before six hours for a hydrocarbon
- No reassurance from a normal early chest X-ray
- No reassurance from the absence of oral burns
- No missing a button battery, no delaying endoscopy, no neutralising a caustic
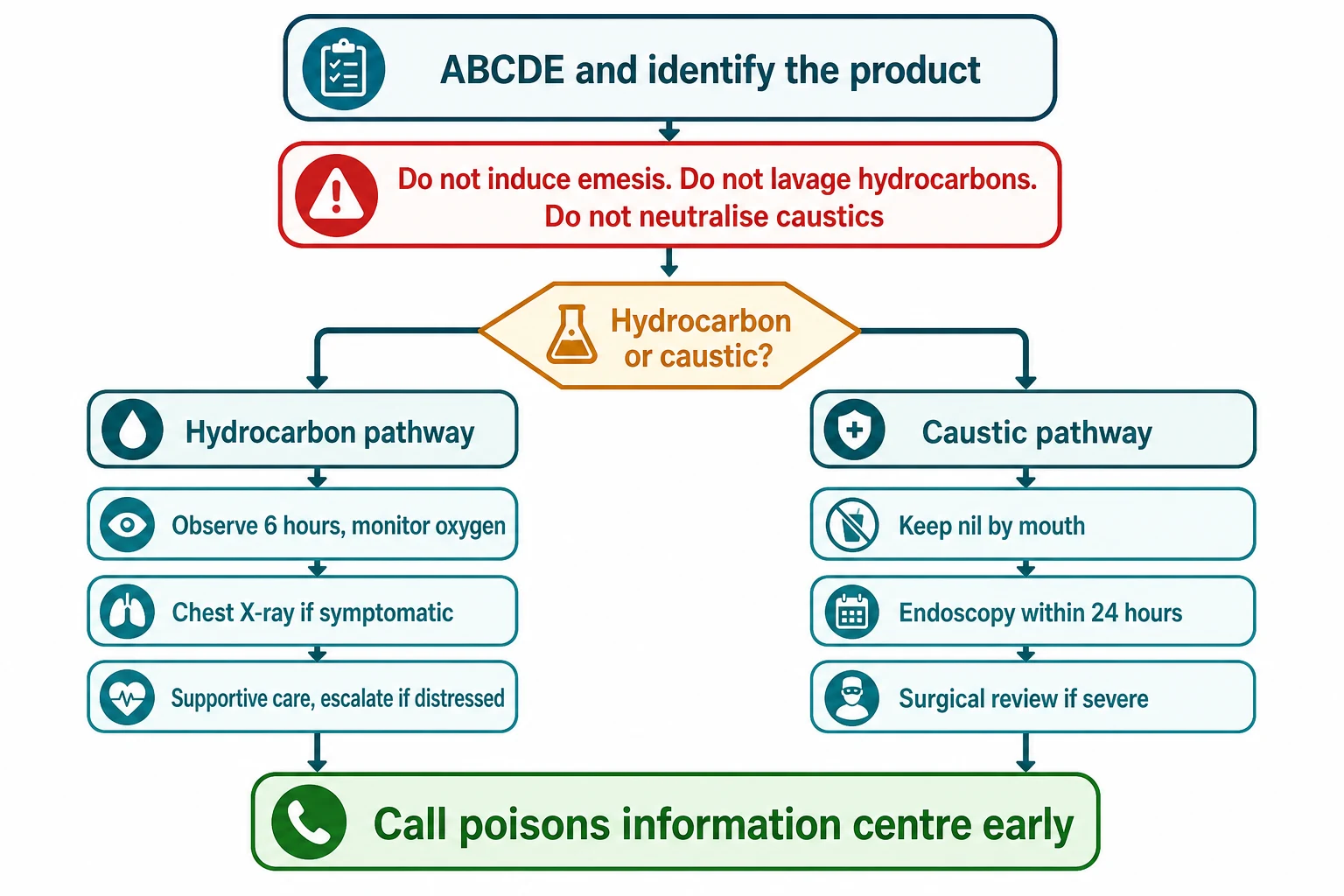
“Secure ABCDE and identify the product → apply the contraindications (no emesis, no lavage for hydrocarbons, no neutralisation for caustics) → hydrocarbon branch: six-hour observation, chest X-ray if symptomatic, supportive care → caustic branch: nil by mouth, early endoscopy within twenty-four hours, Zargar grading, surgical readiness → call the poisons information centre early.”
Viva: why is induced emesis contraindicated in a hydrocarbon ingestion?
A hydrocarbon injures by aspiration, not by systemic absorption. Its low viscosity and low surface tension let a small aspirated volume spread rapidly across the alveoli, disrupt surfactant and cause chemical pneumonitis. Inducing emesis provokes just such an aspiration and converts a contained small-volume exposure into a large-volume lung injury. The same logic excludes gastric lavage. The management is supportive and observational, not decontaminating.
Viva: why is endoscopy timed between six and twenty-four hours in caustic ingestion?
Before six hours the full depth of the caustic injury may not yet be apparent, so the endoscopy grade can be underestimated and the child under-treated. After twenty-four hours the developing oedema and wall weakening raise the risk of iatrogenic perforation from the endoscope. The six-to-twenty-four-hour window balances an accurate grade against a safe procedure, and the Zargar grade then drives the feeding, stricture-surveillance and surgical plan.
Structured oral: a toddler who swallowed drain cleaner
Secure the airway, breathing and circulation, identify the product as an alkali caustic, and keep the child nil by mouth. Do not induce emesis, do not neutralise, and do not give activated charcoal. Establish intravenous access, give fluids and analgesia, and arrange early endoscopy between six and twenty-four hours to grade the burn. Assess for perforation with free air on imaging and involve surgery early. Begin the safeguarding assessment in parallel. Plan long-term stricture surveillance if the endoscopy shows a grade two-b or three injury.
References
- [1]Hoffman RS, Burns MM, Gosselin S Ingestion of Caustic Substances New England Journal of Medicine, 2020.PMID 32348645
- [2]Beuhler MC, Feldman R, Gummin DD, Mowry JB, Rivers LJ, Brown K, et al 2024 Annual report of the National Poison Data System (NPDS) from America's Poison Centers: 42nd annual report Clinical Toxicology (Philadelphia, Pa.), 2025.PMID 41432769
- [3]Irlayıcı FI, Elmas A, Akcam M Corrosive substance ingestion in children: clinical features, management and outcomes in a tertiary care setting European Journal of Pediatrics, 2025.PMID 40802074
- [4]Bolia R, Sarma MS, Biradar V, Sathiyasekaran M, Srivastava A Current practices in the management of corrosive ingestion in children: A questionnaire-based survey and recommendations Indian Journal of Gastroenterology, 2021.PMID 33991312
- [5]Rogalidou M Ingestion of foreign bodies and caustic substances in children: a narrative review on clinical evaluation and management update Clinical and Experimental Pediatrics, 2026.PMID 41381079
- [6]Manfredi MA, Alvarez RP, Arai K, Cheema HA, Darma A, Elawad M, et al Global insights on the diagnosis, management, and prevention of pediatric ingestions: A report from the FISPGHAN expert panel JPGN Reports, 2025.PMID 40814587
- [7]Quitadamo P, di Lauri A, Albano R, Laudadio V, Gragnaniello P, Puoti MG, et al The effects of liquid bleach ingestion on children's esophageal and gastric mucosa Journal of Pediatric Gastroenterology and Nutrition, 2025.PMID 40341791
- [8]Das S, Behera SK, Xavier AS, Selvarajan S Prophylactic Use of Steroids and Antibiotics in Acute Hydrocarbon Poisoning in Children Journal of Pharmacy Practice, 2020.PMID 29673294
- [9]Reddy MV, Ganesan SL, Narayanan K, Jayashree M, Singhi SC, Nallasamy K, et al Liquid Mosquito Repellent Ingestion in Children Indian Journal of Pediatrics, 2020.PMID 31768860
- [10]Rufener CR, Friedman NA, Vaught JE, Harvey HA, Coufal NG Utilizing extracorporeal membrane oxygenation and surfactant in the management of severe acute respiratory distress syndrome due to hydrocarbon pneumonitis Perfusion, 2024.PMID 36548345
- [11]Kendric KJ, Durrani TS Trends in pediatric household cleaning product exposures before and during the COVID-19 pandemic: a national poison data system analysis (2016-2023) BMC Pediatrics, 2026.PMID 42168921