Paeds · acute-care-resuscitation-and-toxicology
Hypovolaemic and haemorrhagic shock
Also known as Haemorrhagic shock · Hypovolaemic shock · Massive transfusion in children · Damage control resuscitation · Tranexamic acid in paediatric trauma
A fellowship approach to hypovolaemic and haemorrhagic shock in children. Recognise compensated shock before hypotension, control catastrophic bleeding first, resuscitate with aliquots of crystalloid for non-haemorrhagic loss and with blood products and damage control resuscitation for haemorrhage, give tranexamic acid within three hours of injury, run a paediatric massive transfusion protocol, prevent the lethal triad, and escalate early to surgical and critical-care support.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A pale, tachycardic child with cool limbs and a rapid, thready pulse after a fall from a height is in shock until you prove otherwise. That child has hypovolaemic shock: the heart cannot deliver enough oxygen to the tissues because circulating volume has been lost. The loss is either of blood (haemorrhagic shock, from trauma, a gastrointestinal bleed or surgery) or of fluid and electrolytes (non-haemorrhagic hypovolaemia, from diarrhoea, vomiting, diabetic ketoacidosis, burns or fluid shifted into a third space). The mechanism differs, but the early priority is the same: restore perfusion before the child decompensates. [1] [2]
The decisive clinical skill is not naming the shock but recognising it before the blood pressure drops. Children defend their blood pressure fiercely through tachycardia and vasoconstriction, so compensated shock is common, looks deceptively well, and is missed by anyone who waits for hypotension. Once you find signs of poor perfusion, treat the direction of change: a child moving from anxious and tachycardic to drowsy and mottled is failing, regardless of the number on the cuff. [2] [11]
Haemorrhagic shock needs a different resuscitation strategy from non-haemorrhagic hypovolaemia, and confusing the two harms children. Crystalloid alone in major bleeding dilutes clotting factors, worsens acidosis and hypothermia, and drives the coagulopathy that kills the bleeding trauma patient. So the fork in the road is early: if the child is bleeding, stop the bleeding and resuscitate with blood products; if the child is volume-depleted without bleeding, resuscitate with fluid aliquots. This topic holds both pathways, with the haemorrhagic pathway carrying the massive transfusion protocol, tranexamic acid and damage control resuscitation. [5] [9]
[2] [5]Classification
Shock is graded by how much volume has been lost and how hard the child is working to compensate. The Advanced Trauma Life Support four-class system is widely taught, but it was derived from adults and fits children imprecisely, because a young child's tachycardia and vasoconstriction can mask a large loss. Use the classes to frame your thinking, and then trust the integrated examination over any single threshold. [2] [5]
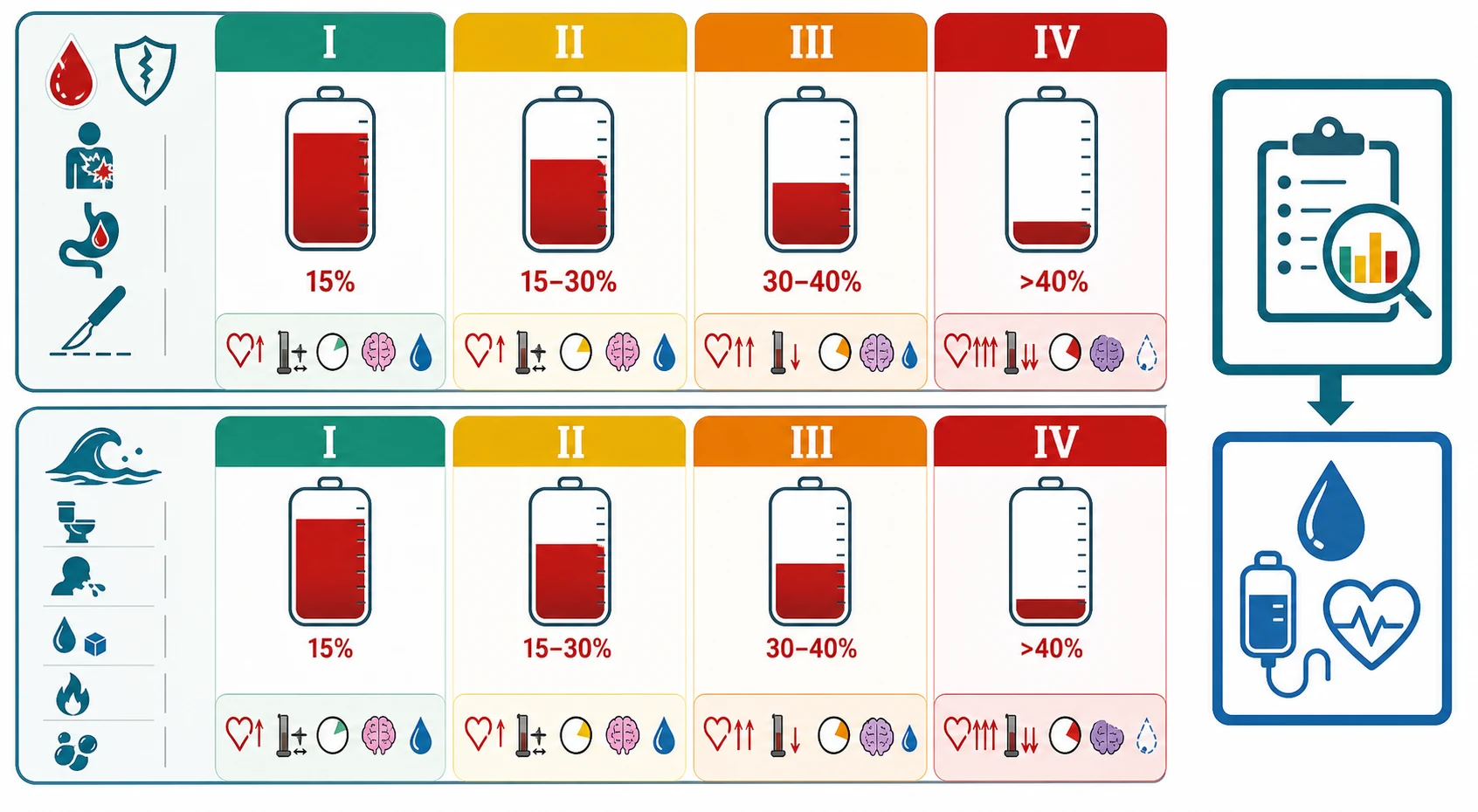
In Class I, less than 15 per cent of blood volume is lost and the child looks well with only mild anxiety. Class II, a 15 to 30 per cent loss, brings tachycardia, a narrowed pulse pressure as diastolic pressure rises from vasoconstriction, and delayed capillary refill. Class III, 30 to 40 per cent lost, shows overt shock: marked tachycardia, hypotension, altered mental state and reduced urine output. Class IV, more than 40 per cent lost, is pre-terminal: profound tachycardia giving way to bradycardia, severe hypotension, lethargy and anuria. The boundary between classes is a clinical judgement, and a young infant can reach Class III physiology with deceptively little visible change. [2] [11]
| Class | Approximate loss | Heart rate | Blood pressure and pulse | Perfusion and brain | Urine output |
|---|---|---|---|---|---|
| I | Under 15 per cent | Normal to mildly raised | Normal | Cool peripheries, anxious, alert | Normal |
| II | 15 to 30 per cent | Tachycardia | Normal systolic, narrowed pulse pressure | Delayed capillary refill, pale | Mildly reduced |
| III | 30 to 40 per cent | Marked tachycardia | Hypotension | Cold mottled skin, altered consciousness | Oliguria |
| IV | Over 40 per cent | Tachycardia then bradycardia | Profound hypotension, weak pulses | Lethargic or unresponsive | Anuria |
Haemorrhagic causes
Blood loss
- Blunt or penetrating trauma, including long-bone and pelvic fractures
- Intra-abdominal injury: solid organ (liver, spleen) or hollow viscus
- Gastrointestinal bleed: varices, peptic ulcer, Meckel diverticulum, intussusception
- Surgical or procedural bleeding, or post-tonsillectomy haemorrhage
- Neonatal intracranial or extracranial haemorrhage
Non-haemorrhagic causes
Fluid and electrolyte loss
- Diarrhoea and vomiting, the commonest global cause
- Diabetic ketoacidosis with osmotic diuresis and dehydration
- Burns with plasma loss across damaged skin
- Third-space losses: sepsis capillary leak, pancreatitis, bowel obstruction
- Oliguric renal failure or uncontrolled polyuria
Epidemiology & Risk Factors
Hypovolaemic and haemorrhagic shock spans the whole of childhood, but the dominant cause shifts with age. In infants worldwide, diarrhoeal dehydration remains the leading cause of hypovolaemic shock, while in adolescents, trauma and gastrointestinal bleeding dominate. The practical point for a fellowship candidate is that the same physiological response carries different implications in different children: a fixed-stroke-volume neonate fails faster, and a teenager with occult blood loss hides it longer. [2] [4]
Trauma is the leading killer of children beyond infancy in high-income countries, and haemorrhage is the leading preventable cause of trauma death. The children who die from bleeding are those in whom control and resuscitation were delayed, which is why the entire haemorrhagic pathway is built around speed: recognise, compress, transfuse and operate early. The 2023 paediatric traumatic haemorrhagic shock consensus conference exists precisely to drive that tempo. [5]
Child and presentation factors
- Young infant with fixed stroke volume and little reserve
- Adolescent with concealed internal bleeding or GI blood loss
- Anticoagulant, antiplatelet or bleeding-disorder medication
- Recent surgery, liver disease or splenomegaly
- Non-accidental injury with concealed blood loss
Setting and system factors
- Rural or remote location with delayed surgical and transfusion access
- Limited blood bank, massive transfusion protocol or laboratory turnaround
- Single-handed or after-hours cover
- Transport time and weather delaying definitive control
- Communication barriers delaying the trauma call
The evidence that should temper enthusiasm for blind fluid in trauma comes from settings very different from a resourced emergency department. The FEAST trial showed that bolus fluid increased mortality in African children with severe febrile illness, a population without intensive-care rescue. The lesson is not that fluid is always harmful, but that a fluid strategy cannot be transplanted across populations, shock types and rescue resources. In a bleeding child you reach for blood early and give crystalloid sparingly, and you reassess after every aliquot. [3] [5]
Pathophysiology
Children compensate, then collapse. Understanding the cascade tells you why hypotension is a late sign and why a tachycardic, cool child is already in trouble. When volume is lost, baroreceptors sense the fall in preload and trigger a sympathetic surge. Heart rate rises to protect cardiac output, and vasoconstriction shunts blood to the brain and heart while sacrificing the skin, gut and kidneys. Blood pressure holds. This compensated phase can persist through a substantial loss, which is exactly what makes it dangerous: the child looks better than they are. [2] [11]
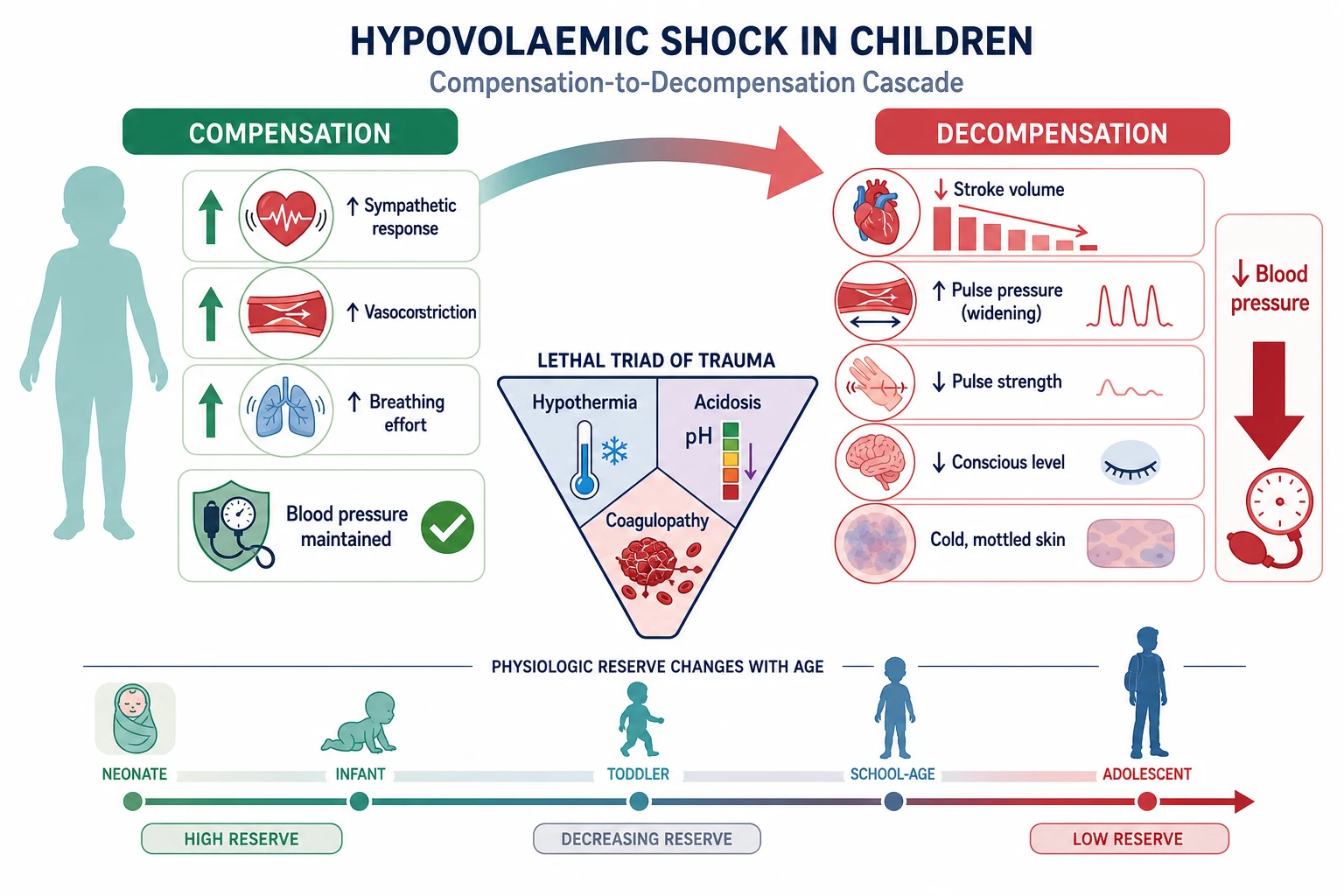
In young infants the compensatory reserve is thinner. The neonatal stroke volume is relatively fixed, so cardiac output depends almost entirely on heart rate. Tachycardia is therefore both the earliest sign and the most important vital sign to act on, and a falling heart rate in a shocked infant is pre-arrest, not recovery. As loss continues past roughly 30 per cent, vasoconstriction can no longer hold the pressure, the pulse pressure widens, the systolic pressure falls, and consciousness drops. Waiting for this moment to diagnose shock is the classic fatal error. [1] [11]
In haemorrhagic shock a second, separate catastrophe unfolds alongside the volume loss: the lethal triad of trauma. Hypothermia from exposure and cold fluids impairs the coagulation cascade, acidosis from poor perfusion and chloride-rich fluids inactivates enzymes and catecholamines, and coagulopathy from clotting-factor loss, consumption and dilution prevents clot formation. Each limb worsens the others, producing a spiral toward irreversible shock and exsanguination. Damage control resuscitation exists to break this spiral by warming the child, correcting acidosis with perfusion, giving balanced blood products and avoiding dilutional coagulopathy. [5] [9]
LETHAL
At the tissue level, shock is a story of oxygen debt. Cells starved of oxygen switch to anaerobic metabolism, generate lactate, and lose the energy to maintain membrane pumps. Cell death and organ failure follow, and the window to reverse this is short. This is why resuscitation is measured against perfusion endpoints rather than blood pressure alone: a normal pressure with a rising lactate and cold skin means the child is still in trouble. [2] [4]
Clinical Presentation
Begin with the doorway impression and let it set the tempo. A child who is pale, sweaty, still and tachycardic, or who has cool mottled limbs and weak interaction, is in shock whether or not the blood pressure is low. Describe what you see in concrete terms, declare your concern, and call for help before you finish examining. The history of injury, bleeding, diarrhoea, polyuria or surgery frames the cause, but it never delays resuscitation. [1] [2]
Work through the circulation as a bundle. Feel central and peripheral pulses: a weak, thready pulse with a narrow or imperceptible volume is more informative than the blood pressure. Measure capillary refill with the technique stated (firm pressure on the sternum or a fingertip for five seconds, then release, at a stated ambient temperature), and treat a refill beyond three seconds as abnormal. Read the skin for colour and temperature, integrate the heart rate against the age-appropriate range, and check the mental state and the urine output. Shock is the sum of these, never one of them alone. [2] [11]
| Age band | Upper normal heart rate (beats per minute) | Upper normal respiratory rate (breaths per minute) |
|---|---|---|
| Neonate | 160 | 60 |
| Infant (1 to 12 months) | 160 | 50 |
| Toddler (1 to 2 years) | 150 | 40 |
| Preschool (3 to 5 years) | 140 | 35 |
| School-age (6 to 11 years) | 120 | 30 |
| Adolescent (12 years and over) | 100 | 25 |
In trauma, look for the bleeding you can see and the bleeding you cannot. Obvious external haemorrhage from a limb wound demands immediate pressure or a tourniquet. Concealed loss hides in the chest, abdomen, pelvis, retroperitoneum and around long-bone fractures: a distended abdomen, pelvic instability, a flail segment or a swollen thigh each signal major internal loss. A femur fracture can hold a litre and a half of blood in an adult-sized adolescent; a splenic or liver injury can exsanguinate quietly. Expose the child fully but keep them warm, and re-examine after every intervention. [5]
In non-haemorrhagic hypovolaemia the history points to the loss: days of diarrhoea and vomiting, polyuria and weight loss in diabetic ketoacidosis, a scald or flame burn, or a septic child with capillary leak. The shock picture is the same, but the cause directs the fluid: balanced crystalloid aliquots for dehydration and third-space loss, specific pathway care for diabetic ketoacidosis, burns and sepsis. Link to those dedicated topics for their full algorithms. [2] [4]
[1] [2]Differential Diagnosis
Hold two lists at once. The first names the type of shock, because hypovolaemic shock must be separated from septic, cardiogenic and obstructive shock before you commit to a fluid strategy. The second names the source of the volume loss, because bleeding needs control and dehydration needs rehydration. The two lists run in parallel as the ABCDE survey and the focused history narrow the cause. [2]
Separate hypovolaemic shock from
- Septic or distributive shock: warm peripheries early, broad infection signs, capillary leak
- Cardiogenic shock: hepatomegaly, gallop, murmurs, abnormal rhythm on ECG
- Obstructive shock: tension pneumothorax, cardiac tamponade, pulmonary embolism
- Anaphylaxis: rapid onset after exposure, urticaria, stridor, bronchospasm
- Mixed physiology is common in sepsis with capillary leak and relative hypovolaemia
Find the source of loss
- External or concealed trauma: limb, chest, abdomen, pelvis, retroperitoneum
- Gastrointestinal bleeding: haematemesis, melaena, intussusception, Meckel
- Gastroenteritis dehydration with stool and vomit losses
- Diabetic ketoacidosis with osmotic diuresis
- Burns with plasma loss, or sepsis with third-space sequestration
A defensible synthesis sounds like this: "This child has compensated shock with tachycardia, weak pulses and a four-second capillary refill but a preserved blood pressure, sustained after a bicycle-versus-car collision with abdominal tenderness. My leading threat is intra-abdominal haemorrhage, so I am controlling the airway and breathing, gaining access, activating the massive transfusion protocol and calling surgery now, while I keep a septic, cardiogenic and obstructive cause open until the picture changes." [1] [5]
Clinical & Bedside Assessment
The assessment is structured, fast and hands-on. Run the ABCDE primary survey, treat each threat as you find it, and weigh the circulation findings as a whole. Keep the child warm, minimise handling that worsens distress and heat loss, and reassess after every action. Bedside glucose is mandatory whenever consciousness is altered, because hypoglycaemia accompanies shock and worsens outcome. [1] [2]
Airway and breathing
Protect the airway and give high-flow oxygen in failure. In trauma, protect the cervical spine in line throughout. Assess the respiratory rate, effort and air entry, and confirm a credible oxygen-saturation trace. A shocked child is often tachypnoeic from acidosis and pain as well as respiratory disease, so interpret the rate against the whole picture. Effective ventilation supports perfusion and corrects the acidosis that deepens shock. [1] [11]
Circulation
Integrate pulses, perfusion, capillary refill, skin colour and temperature, blood pressure, mental state and urine output. Compare the heart rate with the age-appropriate range and act on the trend. Gain vascular access early and without letting repeated failed attempts delay care: two large-bore cannulae where possible, and intraosseous access the moment intravenous access is not immediate in a collapsing child. Control obvious bleeding before you reach for fluid. [1] [5]
Disability and exposure
Check the mental state with AVPU and convert any response below Alert to a formal age-adapted Glasgow Coma Scale. Altered consciousness in shock signals decompensation and threatens the airway. Check bedside glucose immediately and correct a dangerous low through the local pathway. Examine for the source of loss while keeping the child warm and covered, and start safeguarding documentation in parallel whenever injury is unexplained or inconsistent. [1]
[1]Working weight
Obtain a measured weight if it is safe and immediate; otherwise announce and document a single working weight in kilograms with its source and time, and use the local paediatric cognitive aid for all drug and transfusion calculations. Re-weigh at the first safe opportunity. Massive transfusion and tranexamic acid dosing both depend on an accurate weight, so settle this early and explicitly. [5] [7]
Investigations
Stabilise first, and order each test for a named question. In haemorrhagic shock, point-of-care haemoglobin, lactate, point-of-care coagulation and ionised calcium guide the resuscitation, but they never delay activation of the massive transfusion protocol. In non-haemorrhagic hypovolaemia, electrolytes, glucose, ketones and renal function frame the cause and the fluid composition. Imaging answers whether there is a surgical source of bleeding. [2] [5]
Immediate and bedside
- Point-of-care haemoglobin and lactate to quantify loss and perfusion
- Point-of-care international normalised ratio and ionised calcium in major haemorrhage
- Blood gas for acidosis, base deficit and ventilation
- Bedside glucose for every shocked child
- Cross-match, group and save at the moment of access
Conditional on a question
- Full blood count, electrolytes, renal and hepatic function, coagulation
- Amylase or lipase and trauma panels where indicated
- Type and screen before transfusion when time allows
- Pregnancy test for adolescent females with shock or abdominal pain
Targeted imaging
- Focused assessment with sonography in trauma within operator competence
- Contrast computed tomography in a stable child to define injury
- Never move an unstable child to imaging without escort, monitoring and a rescue plan
- Angiography and embolisation when interventional control is the plan
Interpret the results as physiology and trend, not binary reassurance. A haemoglobin can be normal in the first minutes of acute haemorrhage because whole blood is lost; it falls as fluid redistributes. A rising lactate and worsening base deficit signal ongoing hypoperfusion even when the blood pressure looks acceptable. A prolonged international normalised ratio and low ionised calcium in major transfusion demand correction in parallel with the blood. Reassess the child against every result, and never let a normal number overrule a child who is worsening. [2] [9]
Management — Resuscitation
Resuscitation has one rule: restore perfusion by stopping the loss and replacing what is missing, in the correct order, with the correct fluid, and reassess after every action. The first divergence is between bleeding and not bleeding, because that choice changes the first fluid from crystalloid to blood products. State your plan aloud, allocate roles, and run the resuscitation as a team. [1] [5]
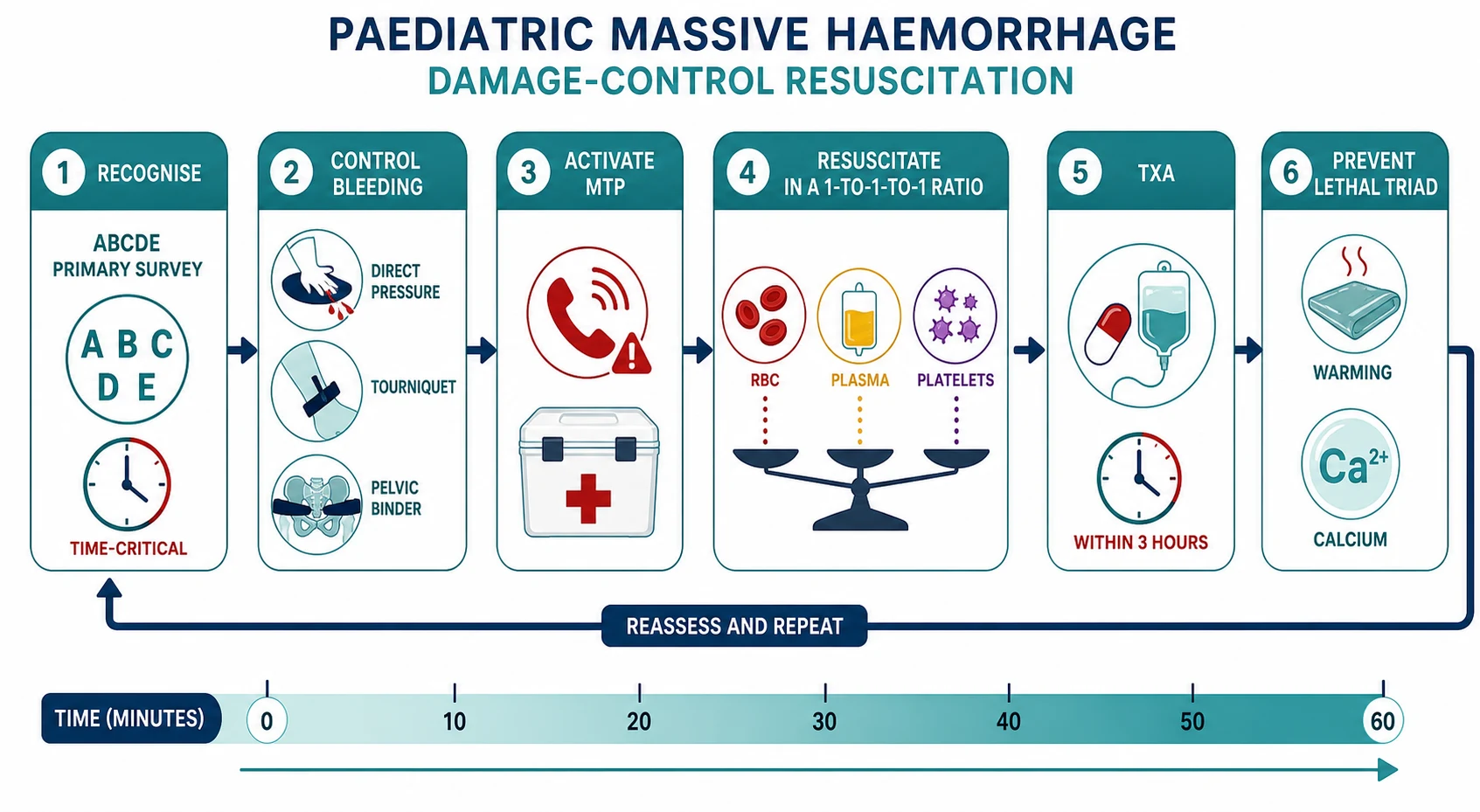
The first fifteen minutes of haemorrhagic shock
Recognise and call
Declare shock, call the resuscitation and surgical teams, name a leader, allocate roles, and bring the massive transfusion protocol, blood warmer and age-appropriate equipment.
Control the bleeding
Apply direct pressure to external haemorrhage; place a windlass tourniquet for limb bleeding that pressure does not control; apply a pelvic binder for suspected pelvic fracture.
Secure access and samples
Place two large-bore cannulae or intraosseous needles; take point-of-care haemoglobin, lactate, coagulation, ionised calcium and glucose; send a group and cross-match.
Activate the protocol
Trigger the massive transfusion protocol and request balanced blood products in a ratio near one-to-one-to-one; do not wait for laboratory confirmation.
Give tranexamic acid
If the injury is within three hours, give tranexamic acid at the paediatric dose and infusion; avoid it beyond three hours.
Prevent the lethal triad
Warm the child actively, use a blood warmer, correct ionised calcium, and avoid chloride-rich crystalloid over-resuscitation.
Reassess and escalate
Recheck perfusion, lactate and haemoglobin; move to definitive surgical or interventional control; arrange critical-care or retrieval support.
Stop the bleeding
External haemorrhage is controlled by direct, sustained pressure. For a limb bleed that pressure does not control, place a windlass tourniquet proximal to the wound and note the application time. For a suspected unstable pelvic fracture, apply a pelvic binder and do not repeatedly palpate the pelvis, because movement restarts bleeding. Concealed internal bleeding needs surgical or interventional radiology control, so summon that expertise the moment you suspect it. Bleeding control is the first resuscitation step, because no amount of blood product replaces ongoing loss. [5]
Fluid for non-haemorrhagic hypovolaemia
When the child is volume-depleted without bleeding, give aliquots of balanced crystalloid. A bolus of 10 to 20 mL per kilogram is the standard aliquot, given over five to twenty minutes and titrated to perfusion endpoints. State the response you expect before each bolus, reassess after each, and stop for fluid overload or no benefit. The first-hour total is a ceiling, not a target: the Surviving Sepsis Campaign 2026 children's guideline supports up-front boluses with careful reassessment and explicit attention to fluid balance, and the FEAST trial warns that blind fluid algorithms harm. [3] [4]
Balanced crystalloid bolus for hypovolaemic shock
Dose
10 to 20 mL per kg per aliquot
Massive transfusion protocol
Major haemorrhage demands blood, not crystalloid. Activate the paediatric massive transfusion protocol the moment the transfusion need is likely to exceed one blood volume or the child is in haemorrhagic shock with ongoing loss. The protocol delivers balanced components, typically a ratio of red cells to plasma to platelets near one-to-one-to-one, in pre-packed boxes that arrive without waiting for each laboratory result. The goal is to prevent dilutional coagulopathy and to replace what is lost with what is lost: whole-blood equivalents. [8] [9]
Massive transfusion dosing
Dose
Red cells 10 to 20 mL per kg; fresh frozen plasma 10 to 20 mL per kg; platelets 5 to 10 mL per kg
Run the protocol alongside damage control principles. Warm every unit through a blood warmer and warm the child actively, because hypothermia disables coagulation. Replace calcium, because the citrate in stored blood binds calcium and hypocalcaemia depresses cardiac function and clotting. Watch the potassium, because rapid transfusion of stored red cells can cause life-threatening hyperkalaemia. Check the point-of-care international normalised ratio and fibrinogen and correct them, because coagulopathy is both a cause and a consequence of ongoing bleeding. [5] [9]
[5] [9]Tranexamic acid
Tranexamic acid inhibits plasminogen activation and stabilises clot, and it saves lives in trauma when given early. The CRASH-2 trial in injured adults showed that tranexamic acid reduced all-cause mortality and bleeding death when given within three hours of injury, with the greatest benefit in the first hour. After three hours the benefit disappears and late administration may increase mortality, so the time window is a hard clinical rule, not a suggestion. [6] [10]
The paediatric dose is a loading infusion followed by a maintenance infusion. The CRASH-2 trial used one gram intravenously followed by one gram over eight hours in adults, and the widely adopted paediatric weight-based equivalent is 15 milligrams per kilogram as a loading dose (to a maximum of one gram) followed by 2 milligrams per kilogram per hour for at least eight hours or until bleeding stops (to a maximum of one gram for the maintenance course). Give it as early as possible, and certainly within three hours of injury. [7] [10]
Tranexamic acid for traumatic haemorrhage
Dose
Loading 15 mg per kg (maximum 1 g), then infusion 2 mg per kg per hour for at least 8 hours (maximum 1 g for the maintenance course)
Permissive hypotension and balanced resuscitation
In adult trauma, a deliberately lower target blood pressure during active bleeding is used to reduce clot disruption before surgical control. The evidence in children is limited and the 2023 paediatric consensus advises caution rather than a universal hypotensive target: aim for adequate perfusion and organ preservation, accept a lower than baseline pressure only in the actively bleeding child before definitive control, and restore a normal-for-age pressure once bleeding is controlled. Apply this judiciously, and never to a child with a traumatic brain injury, who needs a cerebral perfusion pressure that hypotension destroys. [5]
When shock becomes arrest
If the child becomes unresponsive with absent or agonal breathing and no central pulse, move directly into the paediatric arrest algorithm. The arrest-dose anchors are intravenous or intraosseous adrenaline at 10 micrograms per kilogram every three to five minutes, and defibrillation at 4 joules per kilogram for a shockable rhythm. The complete pathway lives in the paediatric basic and advanced life support topic. Massive haemorrhage is a reversible cause of arrest, so run transfusion and bleeding control in parallel with chest compressions. [1]
Management — Definitive & Stepwise
After the child is stabilised, move to definitive control of the cause without stopping reassessment. The cause-specific pathway takes over: surgery or interventional radiology for uncontrolled bleeding, specific rehydration protocols for dehydration and diabetic ketoacidosis, burns-fluid formulas for major burns, and the sepsis bundle for septic shock with capillary leak. Reassessment never pauses, because a temporarily stabilised child can re-bleed or deteriorate as the resuscitation continues. [2] [5]
From resuscitation to definitive control
Confirm control of bleeding
Reassess external and internal loss; ensure pressure, tourniquet and binder are effective; move to surgery, angioembolisation or endoscopic control for ongoing loss.
Stabilise physiology
Sustain perfusion with blood products or fluid, correct hypocalcaemia and acidosis, maintain normothermia, and reverse coagulopathy with targeted products.
Run the cause pathway
Move to the surgical, rehydration, diabetic ketoacidosis, burns or sepsis pathway as the evidence becomes clear, without dropping reassessment.
Agree monitoring and destination
Specify the location, staff, observation intensity, transfusion needs, the next sign of failure and the action if bleeding recurs.
Retrieve or transfer safely
Arrange critical-care or retrieval escort with monitoring, access, blood products and a contingency for deterioration during transport.
Hand over and document
Transfer a structured summary of mechanism, timed actions, products given, response, complications, pending results and the named contingency owner.
Definitive bleeding control is surgical or interventional in almost every case of major haemorrhage. A damage control surgery philosophy prioritises rapid control of bleeding and contamination over definitive repair, leaving the child physiologically intact to recover in intensive care. Engage the surgical and anaesthetic teams early, because the decision to operate is made on physiology and mechanism, not on a single scan. For gastrointestinal bleeding, endoscopic control and specific therapies such as octreotide for varices run alongside resuscitation. [5] [9]
Correction of the lethal triad
Prevent and correct the lethal triad throughout resuscitation. Warm the child with forced-air warming, warmed fluids and a raised ambient temperature, aiming for normothermia. Correct acidosis by restoring perfusion and avoiding chloride-rich fluids, and treat the cause rather than giving bicarbonate blindly. Reverse coagulopathy with balanced products, cryoprecipitate or fibrinogen concentrate for low fibrinogen, and proton-pump inhibitors or specific agents for gastrointestinal bleeding. Calcium is replaced to maintain a normal ionised calcium, because the citrate in transfused blood chelates it. [5] [9]
Early surgical, critical-care and retrieval consultation
Call for help the moment the need appears, not after local options are exhausted. Discuss the likely surgical source, the transfusion and blood-bank capacity, the critical-care and ventilation needs, and the retrieval distance and mode. In rural and remote settings, retrieval is called in parallel with resuscitation so that transport is not the rate-limiting step in definitive control. The exact thresholds, escort and destination remain local or regional, but the principle is universal: escalate early. [5]
| Domain | Content that must cross the boundary |
|---|---|
| Identity and weight | Age, measured or working weight with source, baseline, medications including anticoagulants, and allergies |
| Mechanism and source | Injury or loss mechanism, suspected bleeding source, external and concealed loss, and tourniquet or binder times |
| Physiology and trend | ABCDE findings, age-adjusted observations, perfusion endpoints, lactate and base deficit, and direction of change |
| Actions and products | Fluid, blood products and tranexamic acid given with times, ratios, calcium and warming, and the response |
| Local limits | Access, blood bank, surgical, critical-care and transport capacity, and the requested destination or support |
| Family and safety | Caregiver communication, professional interpreter, safeguarding information, and the immediate safety plan |
| Contingency | Next failure marker, action if bleeding recurs, and named ownership until transfer is complete |
Specific Subtypes & Scenarios
The resuscitation principles are constant, but the source, the setting and the child change what you emphasise. In each scenario, stabilise first, identify the failing system, activate the correct pathway, and state the facts specific to that source. [2] [5]
Traumatic haemorrhage
- Control external loss first; pelvic binder for pelvic fracture
- Activate the massive transfusion protocol early
- Tranexamic acid within 3 hours of injury
- Surgical or angioembolisation control for concealed loss
- Minimise crystalloid; resuscitate with blood
Gastrointestinal bleed
- Variceal versus non-variceal assessment changes therapy
- Endoscopic control alongside resuscitation
- Specific agents such as octreotide or proton-pump inhibitors
- Cross-match early; anticipate rebleeding
- Consider portal hypertension and coagulopathy
Diabetic ketoacidosis
- Hypovolaemia from osmotic diuresis, not bleeding
- Cautious crystalloid aliquots; avoid rapid shifts
- Insulin and fluid are both time-critical
- Watch for cerebral oedema during correction
- Link to the dedicated diabetic ketoacidosis pathway
Burns
- Plasma loss across damaged skin
- Parkland or local formula for fluid alongside aliquots
- Airway threatened in inhalation injury
- Hypothermia and electrolyte shifts
- Link to the burns pathway
Neonate
- Fixed stroke volume: heart-rate dependent and fast to collapse
- Consider intracranial or extracranial haemorrhage
- Duct-dependent lesions mimic shock; check pre- and post-ductal saturations
- Use neonatal weight-based dosing throughout
- Early senior and neonatal team input
Adolescent
- Concealed internal loss, ectopic pregnancy, self-harm
- Private history for substances, restraint, eating disorders
- Confidentiality with its safety limits
- Adult-sized physiology still needs paediatric dosing by weight
- Non-accidental injury and safeguarding in parallel
Rural and remote
- Call retrieval in parallel with resuscitation
- Limited blood bank and surgical capacity
- State equipment, staff, weather and distance limits
- Pre-package blood products and monitoring for transport
- Contingency for deterioration during delay
Anticoagulated child
- Reverse anticoagulation early and specifically
- Lower threshold for blood products
- Coagulation and drug-specific reversal guides
- Bleeding may be occult and disproportionate
- Engage haematology immediately
Complications & Pitfalls
Most preventable harm comes from three errors: waiting for hypotension, over-resuscitating bleeding with crystalloid, and delaying the massive transfusion protocol. Each of these is avoidable with a disciplined approach that treats shock as a perfusion problem and bleeding as a blood-product problem. Record the problem, the expected response, the actual response and the next escalation at every step. [2] [5]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Waiting for hypotension to diagnose shock | Compensated shock is missed until near-collapse | Diagnose from the whole circulation; act on tachycardia, perfusion and trend |
| Resuscitating bleeding with crystalloid | Dilutional coagulopathy and the lethal triad | Control bleeding and reach for blood products early; keep crystalloid minimal |
| Delayed massive transfusion activation | Blood arrives too late to prevent coagulopathy | Trigger the protocol on physiological and mechanistic grounds, not on labs |
| Tranexamic acid beyond three hours | Late dosing may increase mortality | Give within three hours, ideally the first hour; avoid beyond three hours |
| Unmanaged hypothermia, acidosis, hypocalcaemia | The lethal triad deepens and clot fails | Warm actively, use a blood warmer, correct ionised calcium, avoid chloride load |
| Normal haemoglobin taken as reassurance | Early haemorrhage reads falsely normal | Trend haemoglobin and lactate; treat the physiology |
| Repeated failed intravenous attempts | Resuscitation window lost | Move to intraosseous access without delay |
| Imaging before stability | Transport destabilises the bleeding child | Stabilise and escort; use focused bedside ultrasound if competent |
| Forgetting safeguarding | Non-accidental injury evidence is lost | Document objectively; run the pathway in parallel with care |
Watch for complications of the treatment itself. Massive transfusion brings hypocalcaemia, hyperkalaemia, hypothermia, dilutional coagulopathy, transfusion-related acute lung injury and circulatory overload. Tourniquets left too long cause ischaemic injury, so record the time and review it. Pelvic binders and splints need correct sizing. Repeated blood sampling and painful procedures cause harm and distress. The child who did not arrest is not proof that every intervention was harmless, so audit the resuscitation honestly. [8] [9]
[5] [9]Prognosis & Disposition
Disposition follows the trend, the response and the need for definitive control, not a single reassuring observation. Consider the severity and duration of shock, the reversibility of the cause, the transfusion and surgical needs, the treatment harm, and the local capacity for monitoring and rescue. A child who needed a massive transfusion protocol belongs in intensive care or a retrieval system, regardless of how well they look at the end of resuscitation, because rebleeding and coagulopathy can unfold over hours. [2] [5]
Critical care or retrieval
- Ongoing or uncontrolled haemorrhage
- Massive transfusion protocol activated
- Need for surgical, ventilation or vasoactive support unavailable locally
- Transport risk requiring specialist planning
High-dependency or ward
- Bleeding controlled but rebleeding risk remains
- Ongoing transfusion or correction of the lethal triad
- Close monitoring of perfusion, haemoglobin and coagulation
- A named escalation pathway exists
Discharge only when defensible
- Stable perfusion after non-haemorrhagic rehydration with a clear cause
- No ongoing loss or transfusion need
- Safeguarding addressed and caregiver understanding confirmed
- Specific warning changes, access route, follow-up and pending-result ownership agreed
A safety net states what change to watch for, how urgently to act, and exactly where to get help. It names the next review, the owner of pending results, and the plan if bleeding recurs or access is difficult. "Return if worried" alone is not enough for a child who has had a major haemorrhage. After a critical event, explain what happened, invite questions, and offer debriefing to the child, family and team. [5] [9]
Special Populations
Adapt how you assess and communicate, but never lower the standard for recognising shock. Evidence for recognition tools is sparser in complex, technology-dependent and disabled children, and in many low-resource settings, so present these adaptations as safer practice rather than as proven improvements in diagnostic accuracy. [2]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Neonate or young infant | Treat non-specific change and tachycardia as high-risk; fixed stroke volume means rapid collapse; check glucose early | Use neonatal weight-based dosing; consider duct-dependent and haemorrhagic causes |
| Complex or technology-dependent child | Establish personal baseline and device function; assess child and device in parallel | A chronically abnormal observation is not automatically safe; compare with the personal baseline |
| Severe neurodisability | Establish usual interaction, tone and pain expression; treat caregiver-described change as evidence | Adaptation improves communication, not proven diagnostic sensitivity |
| Anticoagulated child | Reverse anticoagulation early and specifically; lower threshold for blood products | Engage haematology; bleeding may be occult and disproportionate |
| Adolescent | Create private time; ask about pregnancy, ectopic risk, substances and self-harm; explain confidentiality limits | Confidentiality has safety limits; safeguarding duties still apply |
| Indigenous, migrant or remote family | Use cultural safety and a professional interpreter; address transport and access barriers | Retrieval and safeguarding routes remain jurisdiction-specific |
Safeguarding runs in parallel with medical care. In any injured child, ask whether the history fits the injury and the developmental stage, document objective findings and the child's spontaneous words, and use the local pathway. Non-accidental injury can present as concealed haemorrhage, and the evidence on the skin and in the history may be the only chance to protect the child. Immediate stabilisation and safety always come first. [5]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The physiology of compensation and decompensation is well established, and the harm of waiting for hypotension is undisputed. The adult-derived ATLS shock classes are taught widely but fit children imprecisely, because tachycardia and vasoconstriction mask loss. Massive transfusion ratios, tranexamic acid timing and permissive hypotension in children lean heavily on adult data, registries and consensus, with comparatively few paediatric randomised trials. Read each recommendation against its population, its evidence grade and the available rescue resources. [5] [9]
CRASH-2
Lancet
Randomised, placebo-controlled trial of tranexamic acid versus placebo in 20,211 adult trauma patients with, or at risk of, significant haemorrhage
Key finding
Tranexamic acid given within three hours of injury reduced all-cause mortality and bleeding death; benefit was greatest in the first hour, and late administration beyond three hours was not beneficial and may be harmful.
Practice change
Give tranexamic acid as early as possible in major trauma, within three hours of injury, and avoid it beyond that window.
The 2023 paediatric traumatic haemorrhagic shock consensus conference consolidated practice across prevention of death from haemorrhage, balanced resuscitation, tranexamic acid within three hours, and caution with permissive hypotension in children. It is a multi-discipline consensus rather than a randomised trial, and it explicitly flags where paediatric evidence is limited. The Surviving Sepsis Campaign 2026 children's guideline anchors fluid-bolus philosophy and reassessment for the non-haemorrhagic and septic end of the spectrum. [4] [5]
The FEAST trial remains the cautionary anchor for blind fluid algorithms. It showed that bolus saline or albumin increased mortality in African children with severe febrile illness compared with no bolus, in a setting without intensive-care rescue. Its lesson is that a fluid strategy must fit the population, the shock type and the rescue available, not that every bolus is harmful. In a bleeding child you give blood early and crystalloid sparingly; in dehydration you give balanced aliquots with reassessment. [3]
Jurisdictional implementation
Australia and Aotearoa New Zealand: ANZCOR Guideline 12.2 is the 2026 regional paediatric advanced life support source. The Royal Children's Hospital Melbourne shock recognition and management and major trauma guidelines support local implementation, alongside the acceptable ranges for physiological variables. Massive transfusion protocol box contents, blood-bank logistics, tourniquet policy, retrieval arrangements and mandatory reporting differ by state, territory and service. In Aotearoa New Zealand, verify the active local trauma, retrieval and safeguarding system rather than borrowing an Australian threshold.
Global and low-resource settings: the leading cause of hypovolaemic shock in children worldwide is dehydration from gastroenteritis, and the WHO Integrated Management of Childhood Illness and ETAT frameworks guide fluid therapy in resource-limited settings. Their population-specific, slower and more cautious fluid approach must stay attached to that context, which is exactly the lesson FEAST reinforces. Tranexamic acid is included in the WHO Model List of Essential Medicines for trauma, and access to safe blood remains a global challenge.
Exam Pearls
Recognition
- Shock is a perfusion problem, not a blood-pressure problem
- Diagnose from tachycardia, weak pulses, prolonged capillary refill, cold mottled skin, altered consciousness, oliguria
- Hypotension is late (Class III or IV)
- Normal haemoglobin early in acute haemorrhage
First fork
- Bleeding or not bleeding decides the first fluid
- Bleeding: control loss, blood products, tranexamic acid
- No bleeding: balanced crystalloid aliquots
Haemorrhagic pathway
- Control bleeding: pressure, tourniquet, pelvic binder
- Activate massive transfusion protocol early
- Balanced ratio near 1 to 1 to 1
- Tranexamic acid 15 mg/kg load then 2 mg/kg/h, within 3 hours
- Prevent lethal triad: warm, calcium, avoid chloride overload
Resuscitation facts
- Crystalloid aliquot 10 to 20 mL/kg
- Red cells, plasma 10 to 20 mL/kg; platelets 5 to 10 mL/kg
- Tranexamic acid within 3 hours, ideally first hour
- Intraosseous access without delay
- Adrenaline 10 micrograms/kg and defibrillation 4 J/kg at arrest
Pitfalls
- No waiting for hypotension
- No crystalloid-only for bleeding
- No delayed MTP
- No tranexamic acid beyond 3 hours
- No forgetting calcium, warming, potassium
“Recognise shock before hypotension → stop bleeding → bleeding means blood products and tranexamic acid within 3 hours, no bleeding means balanced crystalloid aliquots → activate massive transfusion protocol early → prevent the lethal triad → escalate to surgery, critical care and retrieval before local support is exceeded.”
Viva: the tachycardic child with a normal blood pressure
"This child has compensated shock. The tachycardia, weak central pulses, four-second capillary refill and cool mottled skin are signs of poor perfusion despite a preserved blood pressure, and waiting for hypotension would be a classic and dangerous error." Then branch on the cause: if bleeding, control the loss and reach for blood products and tranexamic acid within three hours; if dehydration, give balanced crystalloid aliquots and reassess after each. State the expected response, reassess from the circulation, and escalate to surgery, critical care or retrieval early.
Viva: when do you give tranexamic acid, and when do you not?
Give tranexamic acid to a child with significant traumatic haemorrhage as early as possible, ideally in the first hour and certainly within three hours of injury, because the CRASH-2 trial showed reduced mortality within that window. Use the paediatric dose of 15 milligrams per kilogram loading then 2 milligrams per kilogram per hour. Do not give it beyond three hours of injury, because the benefit disappears and late administration may increase mortality. Run it as part of the local massive haemorrhage protocol alongside blood products, not as a substitute for bleeding control.
Structured oral: rural retrieval of a bleeding child
State the current problem and the resuscitation under way. Control external bleeding, activate the massive transfusion protocol, give tranexamic acid within three hours if indicated, and keep crystalloid minimal. Call retrieval in parallel, state the blood-bank, surgical, staff and transport limits, and agree the destination, the products to continue, the expected deterioration and the contingency for delay. Hand over a structured summary of mechanism, timed products, response and the named contingency owner.
References
- [1]Topjian, Alexa A Part 4: Pediatric Basic and Advanced Life Support 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Pediatrics, 2021.PMID 33087552
- [2]Bjorklund, Ashley Pediatric Shock Review Pediatrics in review, 2023.PMID 37777656
- [3]Maitland, Kathryn Mortality after fluid bolus in African children with severe infection The New England journal of medicine, 2011.PMID 21615299
- [4]Weiss, Scott L Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026 Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2026.PMID 41869844
- [5]Russell, Russell T Pediatric traumatic hemorrhagic shock consensus conference recommendations The journal of trauma and acute care surgery, 2023.PMID 36245074
- [6]CRASH-2 trial collaborators Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial Lancet (London, England), 2010.PMID 20554319
- [7]Borgman, Matthew A Tranexamic acid in pediatric hemorrhagic trauma The journal of trauma and acute care surgery, 2023.PMID 36044459
- [8]Noland, Daniel K Massive transfusion in pediatric trauma: An ATOMAC perspective Journal of pediatric surgery, 2019.PMID 30389149
- [9]Neff, Lucas P Massive Transfusion in Pediatric Patients Clinics in laboratory medicine, 2021.PMID 33494884
- [10]Beno, Suzan Tranexamic acid in pediatric trauma: why not? Critical care (London, England), 2014.PMID 25043066
- [11]Fleming, Susannah Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies Lancet (London, England), 2011.PMID 21411136