Paeds · acute-care-resuscitation-and-toxicology
Initial stabilisation of major paediatric head injury
Also known as Paediatric traumatic brain injury · Severe paediatric head injury · Paediatric major trauma with brain injury · Neuroprotection in paediatric TBI · Raised ICP in head-injured child
A fellowship approach to the initial stabilisation of a child with major traumatic brain injury. Run the primary survey with cervical spine protection, intubate for GCS of 8 or below, oxygenate and ventilate to normocapnia, avoid hypotension with isotonic fluid, treat raised intracranial pressure with hyperosmolar therapy and 30-degree head-up positioning, give early seizure prophylaxis, obtain urgent CT, and escalate to neurosurgery and retrieval before local support is exceeded.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
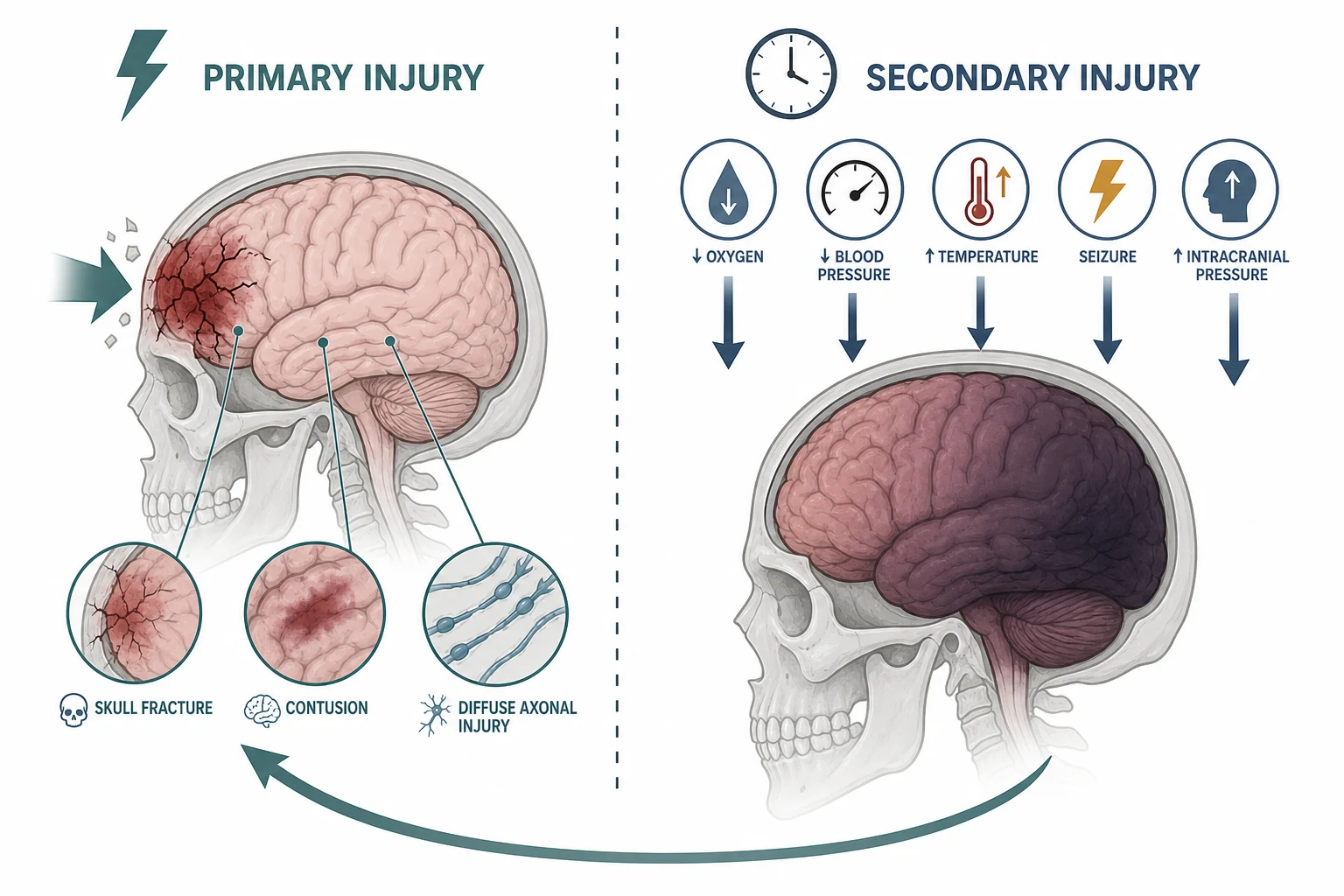
Major paediatric head injury is traumatic brain injury severe enough to threaten the brain through either the primary mechanical damage at impact or the cascade of secondary injury that follows. The initial stabilisation is built around one principle: the primary injury has already happened and cannot be undone, but the secondary injury is preventable. Hypoxia, hypotension, hypercapnia, raised intracranial pressure, fever, seizure and hyperglycaemia each worsen outcome, and each is treatable from the moment the child arrives. [1] [11]
The stabilisation method is the ABCDE primary survey adapted for trauma: cervical spine control is added to Airway, and a rapid neurological assessment is woven through Disability. The defining rule is the same as any primary survey: treat each life threat as you find it, then reassess from A. The difference is that in head injury, every action has a cerebral price. Intubation, ventilation, fluid, sedation and positioning all change intracranial pressure, cerebral perfusion and oxygen delivery, so each intervention is chosen with the brain in mind. [1] [8]
[1] [7]Neuroprotection is not a separate protocol bolted onto resuscitation. It is the organising principle that shapes every decision in the primary survey: which fluid, which ventilation target, which position, which drug for induction, and when to image. A child with a Glasgow Coma Scale of 8 or below needs a definitive airway, and that airway is best secured with a neuro-friendly rapid sequence technique that avoids both hypoxia and the surge in intracranial pressure that rough laryngoscopy can cause. [1] [11]
The neuroprotective primary survey
Cervical spine and Airway
Apply manual in-line stabilisation, fit a correctly sized hard collar, and assess whether the airway is open and protected. Intubate for GCS 8 or below, or for loss of airway reflexes.
Breathing and ventilation
Give high-flow oxygen to correct hypoxia, then ventilate to normocapnia. Target oxygen saturation at least 94 percent and a partial pressure of carbon dioxide in the normal range. Avoid prophylactic hyperventilation.
Circulation and perfusion
Control external bleeding, gain access, and treat hypotension with isotonic crystalloid boluses. Avoid hypotonic fluids. Maintain a systolic blood pressure appropriate for age.
Disability and neuroprotection
Check GCS, pupils, glucose and posture. Position the head 30 degrees up and midline. Treat clinical or radiological raised intracranial pressure with hyperosmolar therapy and give seizure prophylaxis in high-risk cases.
Exposure and urgent imaging
Expose for other injuries while keeping the child warm. Arrange urgent CT of the head and cervical spine when stable enough to scan. Call neurosurgery and retrieval early.
Classification
Traumatic brain injury is classified by severity using the Glasgow Coma Scale, and the severity band sets the tempo and the first actions. The classification is clinical, assessed after resuscitation of immediate life threats, not at the moment of first contact with an unstable child. [1]
| Severity | GCS (after resuscitation) | Immediate implication |
|---|---|---|
| Mild | 13 to 15 | Observe and screen for CT; most discharged; watch for deterioration |
| Moderate | 9 to 12 | Close monitoring, early CT, low threshold for intubation if deteriorating |
| Severe | 3 to 8 | Definitive airway, neuroprotection bundle, urgent CT, neurosurgical referral, consider ICP monitoring |
The paediatric Glasgow Coma Scale modifies the verbal response for preverbal children, because a toddler cannot reliably follow commands or give oriented speech. Use the age-appropriate version, and if you are unsure, default to the motor response, which is the most prognostically weighted component. A child who does not open their eyes, does not vocalise and withdraws only to pain is already in the severe band. [1]
A second classification separates the mechanism of primary injury. Closed head injury includes diffuse axonal injury from acceleration-deceleration forces, contusions from coup-contrecoup impacts, and extradural or subdural haematomas from vascular disruption. Penetrating injury is less common in children but carries a high mortality. Open injury, with a skull fracture communicating with the outside or a basal skull fracture, needs early antibiotics and neurosurgical input. [11]
Extradural haematoma
- Arterial bleeding, classically middle meningeal
- Lucid interval then rapid deterioration
- Underlying fracture often temporal
- Surgical emergency: evacuate before herniation
Subdural haematoma
- Venous bleeding from bridging veins
- May be bilateral; consider abusive head trauma in infants
- Brain injury often more diffuse
- Lower threshold for safeguarding assessment
Diffuse axonal injury
- Shearing of white matter tracts
- Immediate and profound coma
- CT may look deceptively normal early
- Prognosis relates to severity and secondary injury
Raised ICP and herniation
- Mass effect or oedema raising intracranial pressure
- Cushing triad is a late pre-terminal sign
- Unilateral pupil, posture change, falling GCS
- Treat immediately and escalate to neurosurgery
Epidemiology & Risk Factors
Traumatic brain injury is a leading cause of death and disability in children and young people worldwide. Falls are the most common mechanism in younger children, while road traffic collisions, assaults and sport account for more injuries in adolescents. The children at highest risk of poor outcome are those who suffer secondary insults during the prehospital and early emergency phases: a single episode of hypoxia or hypotension can double the mortality of severe traumatic brain injury. [8] [10]
The Excellence in Prehospital Injury Care for Children study, known as EPIC4Kids, evaluated the effect of implementing out-of-hospital traumatic brain injury treatment guidelines in a large statewide system. The findings reinforced that protocol-driven prehospital care, focused on avoiding hypoxia and hypotension, is associated with improved survival in children with moderate to severe traumatic brain injury. This is the evidence base for treating every prehospital and emergency decision as a neuroprotective decision. [10]
Mechanism risk factors
- Road traffic collision, especially pedestrian or cyclist
- Fall from a height greater than twice the child's height
- High-speed projectile or assault
- Non-accidental injury, especially in infants under one year
Physiological risk factors
- Pre-existing hypoxia or hypotension at scene
- Coagulopathy or anticoagulant therapy
- Seizure at the scene or in transit
- Large or expanding intracranial haematoma on imaging
System risk factors
- Long prehospital time or delayed retrieval
- No paediatric neurosurgical service on site
- Rural or remote location
- Incomplete observations or monitoring gaps
Infants are particularly vulnerable for two reasons. Their large head-to-body ratio and weak neck musculature increase the risk of acceleration-deceleration injury, and abusive head trauma, including shaking impact, is a major cause of severe brain injury in children under one year. Any infant with an inconsistent history, retinal haemorrhages, or injuries inconsistent with the stated mechanism must trigger safeguarding alongside medical stabilisation. [11]
Pathophysiology
The primary injury is the irreversible mechanical event: fracturing bone, tearing blood vessels and shearing axons at the moment of impact. Nothing you do in the emergency department reverses it. The secondary injury is everything that follows, and it is where stabilisation makes its difference. The secondary cascade is driven by derangements that are all preventable or treatable: hypoxia, hypotension, hypercapnia, raised intracranial pressure, fever, seizure and hyperglycaemia. [1] [11]
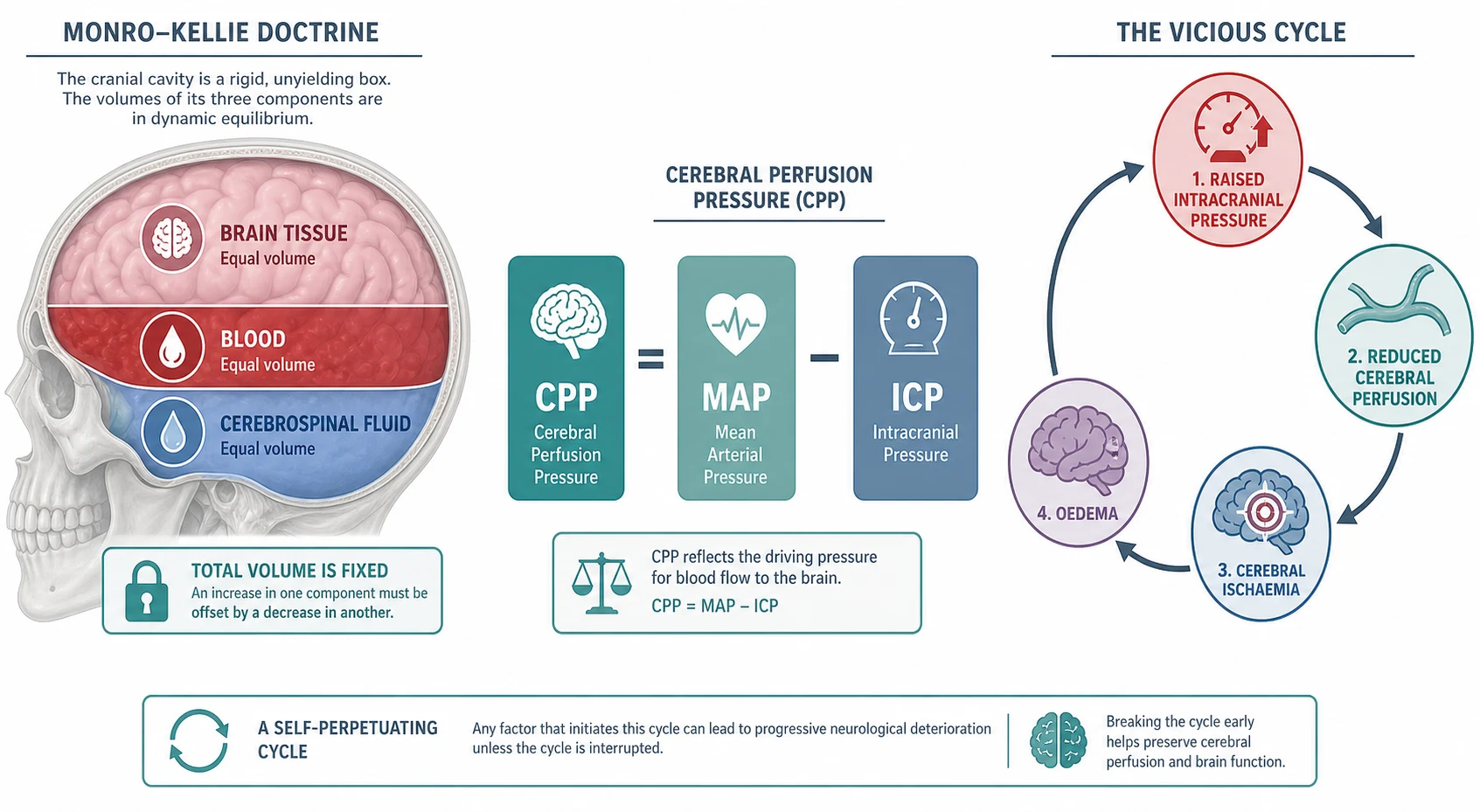
The Monro-Kellie doctrine is the foundation. The skull is a rigid container holding brain tissue, blood and cerebrospinal fluid at a fixed total volume. When an intracranial haematoma or cerebral oedema adds volume, the normal components are displaced first, and intracranial pressure stays near normal. Once this compensatory reserve is spent, any further volume increase causes a steep rise in intracranial pressure. This is why a child can look well for hours and then deteriorate in minutes: the reserve has been exhausted. [1]
Cerebral perfusion pressure is the pressure that drives blood through the brain, and it equals mean arterial pressure minus intracranial pressure. Two practical conclusions follow. First, hypotension is doubly dangerous because it lowers the driving pressure while the intracranial pressure may be rising. Second, a raised intracranial pressure erodes cerebral perfusion from the other side. Both must be managed simultaneously, which is why neuroprotection is not a single intervention but a bundle. [7] [9]
Cerebral autoregulation is the brain's ability to maintain constant blood flow across a range of blood pressures. After traumatic brain injury, autoregulation is often impaired, so cerebral blood flow becomes passively dependent on systemic blood pressure. In that state, a drop in blood pressure translates directly into a drop in cerebral perfusion, and the child has no safety margin. This is why maintaining an age-appropriate blood pressure is not merely supportive care but a direct neuroprotective act. [9]
The vicious cycle is the final common pathway. Raised intracranial pressure reduces cerebral perfusion, ischaemia generates cytotoxic oedema, oedema raises intracranial pressure further, and the cycle accelerates toward herniation. The clinical signs of herniation, such as a unilateral dilated pupil, decerebrate posture or the Cushing response of hypertension with bradycardia, are late and pre-terminal. The goal of stabilisation is to intervene before these signs appear. [1] [12]
Clinical Presentation
The first question is whether the child has a major head injury at all, and the answer comes from the mechanism, the conscious level and the focal signs. Begin before you touch the child. From the doorway, note the level of interaction, the breathing pattern, the posture and any obvious external injury. A child who is lying still, not responding to voice, or showing an abnormal posture is in the severe band until proven otherwise. [1] [8]
Glasgow Coma Scale and the paediatric modification
Use the Glasgow Coma Scale for every head-injured child, and use the age-app paediatric version for preverbal children. The motor response carries the most prognostic weight. Record the score, the time, and the trend, because a falling GCS is more alarming than any single number. A drop of two points or more, or any deterioration in the verbal or motor response, is an emergency requiring immediate reassessment and escalation. [1]
Pupils and posture
Check pupil size and reactivity early and repeat it. An unilateral dilated pupil that reacts poorly to light suggests third nerve compression from ipsilateral uncal herniation, and it is a neurosurgical emergency. Bilateral dilated, fixed pupils suggest severe brainstem injury or a reversible cause such as hypothermia or drug effect. Look for abnormal posture: decorticate (flexion) and decerebrate (extension) posturing indicate progressively deeper brain dysfunction. [1] [11]
Signs of skull fracture and raised intracranial pressure
Look for signs of a basal skull fracture: periorbital bruising, bruising behind the ear over the mastoid, cerebrospinal fluid leak from the nose or ear, and haemotympanum. A depressed or palpable skull fracture, or an open wound communicating with the fracture, needs early neurosurgical input and prophylactic antibiotics. Signs of raised intracranial pressure include a falling conscious level, vomiting, headache in an older child, and the Cushing response of hypertension with bradycardia and irregular breathing, which is a late sign. [1] [11]
| Sign | What it suggests | Immediate action |
|---|---|---|
| GCS 8 or below | Severe TBI; unable to protect airway | Rapid sequence intubation with neuro-friendly agents |
| Falling GCS by 2 or more points | Expanding intracranial lesion or rising ICP | Reassess, prepare for imaging, escalate to neurosurgery |
| Unilateral dilated pupil | Third nerve compression, impending uncal herniation | Hyperosmolar therapy now, urgent CT, neurosurgery |
| Cushing triad | Critically raised ICP, pre-terminal | Treat as herniation; immediate escalation |
| Basal skull fracture signs | Underlying basal fracture, possible CSF leak | Avoid nasogastric tube; arrange CT; give antibiotics |
| Post-traumatic seizure | Seizure, possibly status | Treat with benzodiazepine; consider prophylaxis |
Cervical spine
Assume a cervical spine injury in every major head injury until it is cleared clinically or radiologically. Keep manual in-line stabilisation in place, fit a correctly sized hard collar, and use head blocks and tape for transport. Do not remove the collar to examine the neck until the child is stable and cervical spine clearance is planned. [8]
Differential Diagnosis
The immediate question is rarely what caused the head injury but what is causing the current physiology, because a child with major trauma can have multiple simultaneous threats. Build the differential in the same order as any primary survey: what can kill now, what is most likely, what is reversible, and what is most harmful to miss. [1]
ICP-DRIVE
Always keep the reversible mimics open. Hypoglycaemia in a child who has been fitting, vomiting or not eating can produce a depressed conscious level that resolves with glucose. Poisoning, including opioid or sedative ingestion, can coexist with head trauma and depress consciousness independently. Non-accidental injury, especially in an infant, is both a common cause of severe brain injury and a diagnosis that is easy to miss in the rush of stabilisation. Stabilise first, but keep these causes actively in mind and investigate in parallel. [11]
Must not miss
- Expanding intracranial haematoma needing evacuation
- Cervical spine injury with cord compression
- Status epilepticus or non-convulsive seizure
- Abusive head trauma in an infant
- Hypoglycaemia or electrolyte disturbance
Common coexisting
- Polytrauma with chest, abdominal or pelvic injury
- Long-bone or facial fractures
- Coagulopathy from anticoagulants or liver injury
- Aspiration or lung contusion causing hypoxia
Mimics and modifiers
- Intoxication or recreational drug use in adolescents
- Pre-existing developmental or neurological disability
- Post-ictal state after a seizure
- Hyponatraemia or other metabolic disturbance
Clinical & Bedside Assessment
The assessment is the ABCDE primary survey adapted for trauma and neuroprotection. Cervical spine control is added to Airway, and the neurological assessment is rapid but repeated. Every finding drives a specific neuroprotective action, and reassessment is continuous. [1] [8]
A - Airway with cervical spine control
Assess whether the airway is open and protected. A child with a major head injury often has a depressed conscious level, lost gag reflex, or obstruction from blood, vomit or facial injury. Keep manual in-line stabilisation throughout airway manoeuvres. The threshold for intubation is a Glasgow Coma Scale of 8 or below, because below this level the child cannot reliably protect the airway or maintain adequate ventilation. Also intubate for loss of airway reflexes, inadequate ventilation despite oxygen, or a rapidly deteriorating conscious level. [1]
When intubating, use a rapid sequence technique with preoxygenation and a neuro-friendly induction. Avoid coughing, bucking and prolonged laryngoscopy, because each raises intracranial pressure. The induction agent should provide anaesthesia without causing hypotension; the historical concern about ketamine raising intracranial pressure has been challenged by evidence that it does not significantly raise intracranial pressure in ventilated children with severe traumatic brain injury. A muscle relaxant is essential to prevent movement during laryngoscopy. Confirm tube position with waveform capnography immediately. [5]
B - Breathing and ventilation
Give high-flow oxygen to any child who is hypoxic, and target an oxygen saturation of at least 94 percent. The ventilation target is normocapnia, not hypocapnia. Avoid prophylactic hyperventilation, because lowering the partial pressure of carbon dioxide below the normal range causes cerebral vasoconstriction, reduces cerebral blood flow, and risks cerebral ischaemia. Reserve temporary mild hyperventilation for the acute signs of impending herniation while definitive treatment is prepared. Use waveform capnography to guide ventilation, because clinical assessment of ventilation rate is unreliable in an emergency. [1]
C - Circulation and perfusion
Assess the whole circulation: heart rate, pulse quality, capillary refill, blood pressure and skin temperature. Control external bleeding with direct pressure. Gain intravenous or intraosseous access. If the child is in shock, give boluses of isotonic crystalloid, typically 10 mL per kilogram aliquots, and reassess after each. Use 0.9 percent saline or a balanced crystalloid, never hypotonic fluids, because hyponatraemia worsens cerebral oedema. Avoid hypotension aggressively, because even a single episode is associated with worse outcome. If multiple boluses are needed, seek the cause of ongoing loss and consider blood products and vasoactive support. [1] [7]
[1]D - Disability
Use the Glasgow Coma Scale and record the score, the time and the trend. Check pupils for size and reactivity, and look for abnormal posture. Check bedside glucose immediately, because hypoglycaemia is common in injured children and worsens outcome. Treat any dangerous low glucose now. If the child is seizing, treat with first-line benzodiazepine at five minutes of ongoing convulsion. Position the head 30 degrees up and midline to promote venous drainage and reduce intracranial pressure, provided the cervical spine is protected and the child is stable. [1] [11]
E - Exposure and environment
Expose the child fully to identify other injuries while preventing hypothermia, because hypothermia causes coagulopathy and worsens outcome. Look for signs of basal skull fracture, depressed fracture, and other trauma. Keep the child warm with blankets, warmed fluids and ambient temperature control. Begin safeguarding assessment in parallel, particularly in infants. [8]
[1]Focused history
Take a focused history in parallel using a SAMPLE frame: symptoms, allergies, medications, past history, last meal and events. The mechanism and time of injury, any loss of consciousness, seizure, vomiting, anticoagulant use and the child's baseline developmental level are the key data. In an infant, ask about the mechanism in detail and whether the history is consistent with the injuries, because inconsistent accounts raise the possibility of abusive head trauma. [11]
Investigations
The first investigation is bedside glucose, taken the moment consciousness is assessed. It is fast, cheap, and a dangerous low is immediately treatable. Do not delay stabilisation for any test. The definitive investigation for major head injury is an urgent CT scan of the head, obtained once the child is stable enough for transport to the scanner. [1]
Immediate and bedside
- Bedside glucose for every head-injured child with altered consciousness
- Waveform capnography for any intubated child
- Arterial or venous blood gas for ventilation, perfusion and metabolic state
- Point-of-care coagulation if anticoagulated or suspected liver injury
Targeted imaging
- Urgent CT head for any moderate or severe TBI once stable enough to scan
- CT cervical spine for all major head injury until cleared
- Consider CT chest, abdomen and pelvis if polytrauma is suspected
- Never send an unstable child to CT without monitoring, escort and a rescue plan
Laboratory
- Full blood count, coagulation, electrolytes, glucose and group and save
- Blood alcohol and drug screen in adolescents where relevant
- Drug levels if the child is on antiepileptics
- Minimum necessary blood volume in small children
The indications for urgent CT head after head injury include a Glasgow Coma Scale below 15 at two hours after injury, suspected open or depressed skull fracture, signs of basal skull fracture, a post-traumatic seizure, any focal neurological deficit, a dangerous mechanism, and more than one episode of vomiting. These criteria follow the NICE head injury guideline and local adaptations. In a child with severe TBI already intubated for airway protection, CT is obtained as soon as the child is stable enough for the scan. [11]
Intracranial pressure monitoring is indicated for severe traumatic brain injury, typically a Glasgow Coma Scale of 8 or below with an abnormal CT scan showing haematoma, oedema or compressed basal cisterns. It is also considered when the CT is normal but two or more high-risk features are present, such as age over 40, hypotension, or a motor posturing response. Neuromonitoring, including intracranial pressure and brain tissue oxygenation, guides targeted therapy in the paediatric intensive care unit, but the decision to monitor and the threshold are made with the neurocritical care team. [1] [12]
[1]Management — Resuscitation
Resuscitation of major head injury is neuroprotective resuscitation: the primary survey is run in the order that protects the brain. Every action is chosen for its effect on cerebral oxygenation, perfusion pressure and intracranial pressure. The child is treated as a whole, and the goal is to prevent secondary injury while the definitive neurosurgical plan is assembled. [1]
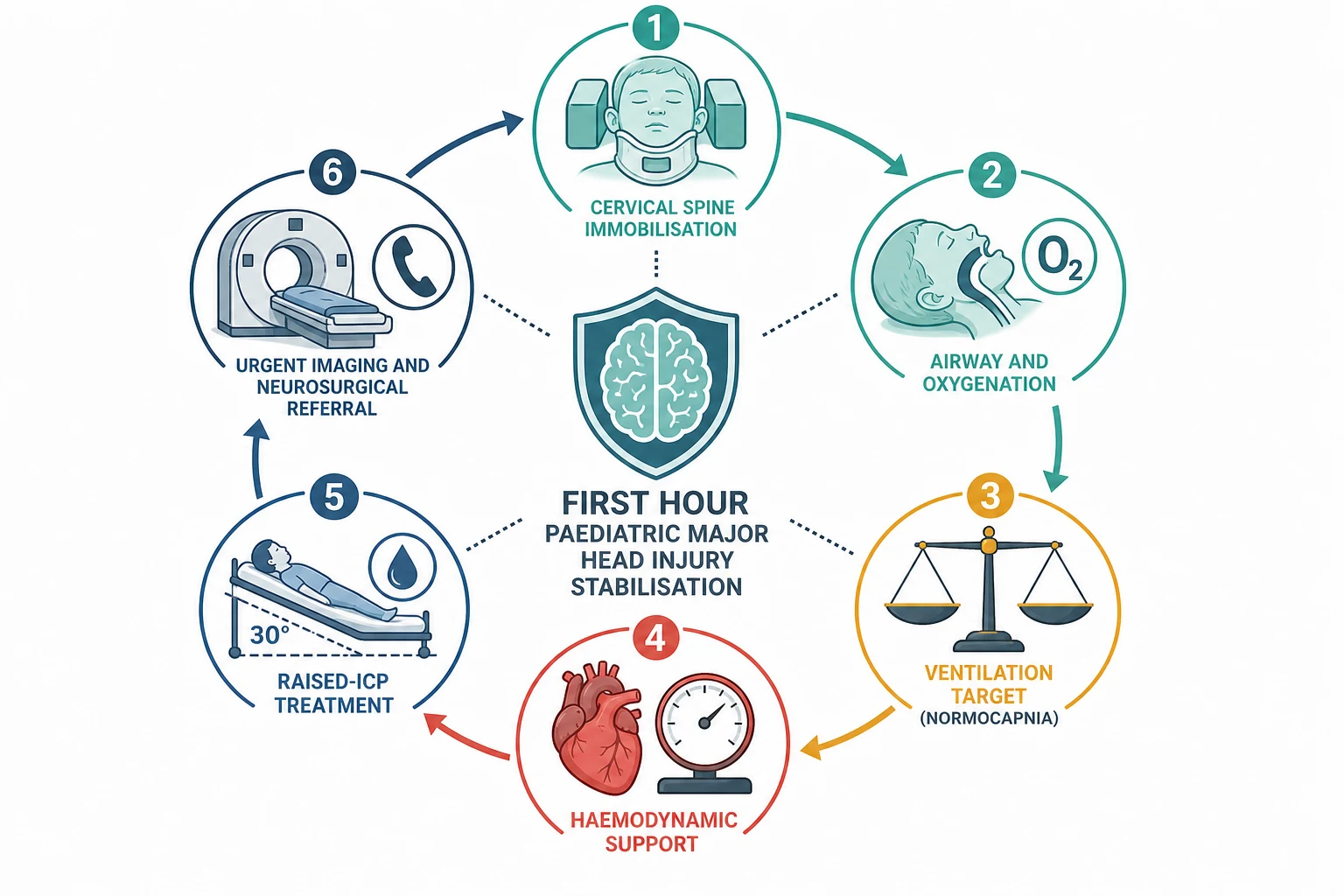
The first 15 minutes
Organise and immobilise
Call for help, name a leader, and allocate roles. Apply manual in-line stabilisation, fit a hard collar, and bring age-appropriate monitoring and equipment.
Secure the airway
Intubate for GCS 8 or below using rapid sequence induction with a neuro-friendly agent and muscle relaxant. Confirm with waveform capnography.
Oxygenate and ventilate
Give high-flow oxygen and ventilate to normocapnia. Target saturation at least 94 percent. Avoid prophylactic hyperventilation.
Support the circulation
Control bleeding, gain access, give isotonic crystalloid boluses for shock. Maintain age-appropriate blood pressure. Avoid hypotonic fluids.
Protect the brain
Position head 30 degrees up and midline. Check glucose and correct dangerous lows. Give seizure prophylaxis in high-risk cases. Treat signs of raised ICP with hyperosmolar therapy.
Image and escalate
Arrange urgent CT of head and cervical spine when stable. Call neurosurgery and retrieval early. Transfer monitoring, trend and contingency.
Airway: when and how to intubate
Intubate any child with a Glasgow Coma Scale of 8 or below, loss of airway protective reflexes, inadequate ventilation despite oxygen, or a rapidly deteriorating conscious level. Use a rapid sequence technique with preoxygenation. Choose an induction agent that maintains haemodynamic stability and cerebral perfusion; avoid hypotension at induction. A systematic review and multicentre evidence have shown that ketamine does not cause a clinically significant rise in intracranial pressure in ventilated children with severe traumatic brain injury, challenging the older teaching that it is contraindicated. Use a muscle relaxant, confirm tube placement with waveform capnography, and secure the tube carefully before transport. [1] [5]
Ventilation: the normocapnia rule
The ventilation target is normocapnia. Maintain the partial pressure of carbon dioxide in the normal range, using waveform capnography to guide the rate and tidal volume. Do not hyperventilate prophylactically. Hypocapnia causes cerebral vasoconstriction and reduces cerebral blood flow, and routine prophylactic hyperventilation is associated with worse outcome. Reserve temporary mild hyperventilation for the acute signs of impending herniation, such as a unilateral dilated pupil or decerebrate posture, while hyperosmolar therapy and neurosurgical escalation are prepared. [1]
Circulation: avoid hypotension
Even a single episode of hypotension after severe traumatic brain injury is associated with a doubling of mortality. Maintain an age-appropriate systolic blood pressure, treat hypovolaemia with isotonic crystalloid, and investigate and control ongoing blood loss. Avoid hypotonic fluids, because hyponatraemia worsens cerebral oedema. If shock persists despite fluid resuscitation, consider blood products and vasoactive support, and escalate to critical care. The mean arterial pressure and discharge outcomes in severe paediatric traumatic brain injury study reinforced the association between blood pressure and outcome, supporting aggressive prevention of hypotension. [1] [7]
[1] [7]Raised intracranial pressure: first-line measures
Start the general measures the moment severe traumatic brain injury is recognised. Elevate the head of the bed to 30 degrees and keep the head midline to promote venous drainage. Ensure adequate sedation, analgesia and muscle relaxation in the intubated child to prevent coughing, bucking and pain-driven rises in intracranial pressure. Maintain normoxia, normocapnia and normotension. Avoid hyperglycaemia and treat fever to maintain normothermia. These measures are the foundation, and every subsequent escalation builds on them. [1]
Management — Definitive & Stepwise
After the primary survey has stabilised the child, definitive management moves to hyperosmolar therapy for raised intracranial pressure, seizure prophylaxis, temperature and glucose control, urgent imaging and neurosurgical referral. The neuroprotection bundle continues throughout, and reassessment from A never stops. [1] [11]
Hyperosmolar therapy: hypertonic saline and mannitol
Hyperosmolar therapy reduces intracranial pressure by drawing water out of the brain along an osmotic gradient. The two agents in common use are 3 percent hypertonic saline and mannitol. The guidelines for the acute medical management of severe traumatic brain injury in infants, children and adolescents, the Brain Trauma Foundation second edition, list 3 percent saline as an option for the treatment of intracranial hypertension. A bolus of 3 percent saline, typically in the range of 2 to 5 mL per kilogram, is widely used to treat acute rises in intracranial pressure, with monitoring of serum sodium to avoid exceeding approximately 155 to 160 mmol per litre. [1]
A JAMA Network Open study compared intracranial pressure measurements before and after hypertonic saline or mannitol treatment in children with severe traumatic brain injury, and found that both agents reduce intracranial pressure, with hypertonic saline showing a numerically greater effect. A 2025 outcome study from the same network compared clinical outcomes between the two agents and found no statistically significant difference in mortality, supporting the use of either agent based on local protocol and patient factors. A systematic review and meta-analysis confirmed comparable efficacy for intracranial pressure reduction, reinforcing that both are acceptable first-line agents. [2] [3] [4]
Mannitol is given as a bolus of 0.25 to 0.5 g per kilogram intravenously, and it can be repeated. Monitor serum osmolality and avoid mannitol if the osmolality exceeds approximately 320 mOsm per litre, because above this threshold the risk of renal injury and rebound intracranial hypertension rises. Mannitol can cause hypovolaemia through its diuretic effect, so monitor the circulation and replace intravascular volume with isotonic fluid. [1]
| Feature | 3 percent hypertonic saline | Mannitol |
|---|---|---|
| Typical bolus dose | 2 to 5 mL per kg of 3 percent solution | 0.25 to 0.5 g per kg intravenously |
| Effect on ICP | Reduces ICP; may have greater effect than mannitol | Reduces ICP; osmotic diuresis |
| Monitoring | Serum sodium, avoid exceeding 155 to 160 mmol per litre | Serum osmolality, avoid exceeding 320 mOsm per litre |
| Circulation | Expands circulating volume; lower risk of hypovolaemia | Diuretic effect; risk of hypovolaemia; replace volume |
| Evidence | Both effective for ICP reduction; no significant mortality difference in recent studies | Both effective; long clinical experience |
Seizure prophylaxis
Post-traumatic seizures worsen secondary brain injury by raising metabolic demand, intracranial pressure and oxygen consumption. Early seizure prophylaxis is recommended for children at high risk, typically those with severe traumatic brain injury and an abnormal CT scan, for the first seven days after injury. Levetiracetam or phenytoin are the common agents, chosen with local protocol and the child's profile. Prophylaxis is not indefinite: seven days covers the period of highest early seizure risk. Treat any actual clinical seizure with first-line benzodiazepine and investigate the cause. [1]
Glucose, temperature and sodium
Keep the bedside glucose in the normal range. Hypoglycaemia worsens outcome and is immediately treatable, while hyperglycaemia is associated with worse outcome and should be avoided. Maintain normothermia and treat fever aggressively, because each degree of fever raises cerebral metabolic demand. Monitor serum sodium and manage it within the target range set by the neurocritical care team, because both hyponatraemia and extreme hypernatraemia carry risks. [1] [11]
Indications for neurosurgery and decompression
Call neurosurgery at the point of recognising severe traumatic brain injury, not after the CT confirms an operable lesion. Operable intracranial haematomas, such as an expanding extradural or subdural haematoma, need urgent evacuation. Decompressive craniectomy is a second-tier therapy for refractory intracranial hypertension that has not responded to medical treatment, and the decision is made by the neurosurgical and neurocritical care team. Early referral allows planning for transfer, operating theatre readiness and ongoing intensive care. [1] [11]
Hypertonic Saline vs Mannitol (JAMA Network Open)
JAMA Network Open
Multicentre observational study of ICP measurements before and after treatment in children with severe TBI
Key finding
Both hypertonic saline and mannitol reduced ICP; hypertonic saline showed a numerically greater reduction.
Practice change
Both agents remain acceptable first-line therapy; local protocol and patient factors guide the choice.
Transfer and retrieval
Call retrieval as soon as the child may need monitoring, imaging or neurosurgical care that the current service cannot provide. Discuss the child's physiology, the treatment underway, the expected response, the escort and equipment, the transport time and weather, the safest destination and the contingency if transfer is delayed. Keep the neuroprotection bundle running throughout transfer, with continuous monitoring and a named owner for the next escalation. [8]
[8]Specific Subtypes & Scenarios
The neuroprotective primary survey stays the same, but age, mechanism, presentation and setting change what you look for and how early you escalate. In each scenario, stabilise first, identify the failing system, and activate the correct pathway. [1]
Infant with possible abusive head trauma
- Inconsistent history or mechanism inconsistent with injuries
- Retinal haemorrhages, subdural haematomas, rib or long-bone fractures
- Stabilise first; activate safeguarding in parallel
- Document objectively; preserve evidence when safe
Extradural haematoma
- Lucid interval then rapid deterioration
- Temporal fracture on imaging
- Surgical emergency: evacuate before herniation
- Neurosurgery called the moment CT shows the lesion
Child with coagulopathy
- Anticoagulant therapy or inherited bleeding disorder
- Higher risk of intracranial haematoma expansion
- Reverse anticoagulation early
- Lower threshold for urgent CT
Polytrauma
- Chest, abdominal or pelvic injury coexisting with head injury
- Tension pneumothorax, cardiac tamponade or haemorrhage can mimic brain injury
- Treat the most dangerous threat first
- Whole-child resuscitation, not head injury in isolation
Post-traumatic seizure
- Treat convulsive seizure with benzodiazepine at five minutes
- Check and correct glucose
- Give prophylaxis if high-risk severe TBI
- Keep infection and metabolic causes open
Rural or remote hospital
- Call retrieval before the child needs support unavailable locally
- State equipment, staff, weather, distance and communication limits
- Run the full neuroprotection bundle during the wait
- Package monitoring, access and handover for transport
Technology-dependent child
- Assess the child and the device in parallel
- Use the personal emergency plan and specialty pathway
- Bring caregiver expertise into the escalation
- Do not assume baseline observations are normal
Adolescent with possible intoxication
- Stabilise first; do not attribute reduced consciousness solely to alcohol
- Drug and alcohol screen when relevant
- Create private history time when safe
- Explain confidentiality and its safety limits
Child with pre-existing disability
- Obtain the individual baseline for consciousness and function
- Use the personal emergency plan and caregiver knowledge
- Adapt communication and examination
- Do not lower the standard for recognising deterioration
Complications & Pitfalls
Most harm in paediatric head injury stabilisation comes from preventable secondary injury. The child is stabilised, then sent for imaging without ongoing monitoring, or hyperventilated to a low carbon dioxide, or given hypotonic fluid, or not intubated soon enough. Each of these is a failure of neuroprotection, and each is avoidable. [1] [6]
The multicentre site survey of prehospital and emergency management of paediatric traumatic brain injury found substantial variability in adherence to guideline-recommended practices, including delays in intubation and variability in ventilation targets. Guideline adherence matters: the EPIC4Kids study showed that protocol-driven prehospital care focused on avoiding hypoxia and hypotension is associated with improved survival. The practical lesson is that the neuroprotection bundle is only effective if it is applied consistently and early. [6] [8] [10]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Delaying intubation for GCS 8 or below | Aspiration, hypoxia, hypercapnia worsen secondary injury | Intubate early with rapid sequence and a neuro-friendly agent |
| Prophylactic hyperventilation | Cerebral vasoconstriction causes ischaemia | Target normocapnia; reserve hyperventilation for impending herniation |
| Hypotonic fluid for resuscitation | Hyponatraemia worsens cerebral oedema | Use isotonic crystalloid exclusively |
| Single hypotensive episode accepted | Doubles mortality after severe TBI | Maintain age-appropriate blood pressure aggressively |
| Sending an unstable child to CT unescorted | Deterioration in the scanner with no rescue | Stabilise first; send with monitoring, escort and a plan |
| Missing cervical spine injury | Cord damage during airway manoeuvres or movement | Assume C-spine injury until cleared; use in-line stabilisation |
| Not checking glucose | Hypoglycaemia mimics or worsens brain injury | Check bedside glucose early in every altered child |
| Attributing reduced consciousness to intoxication alone | Intracranial injury missed | Keep intracranial causes open; scan when indicated |
| Forgetting safeguarding | Abusive head trauma missed | Stabilise first; document objectively; activate the pathway |
Watch for the harms of treatment itself. Over-aggressive fluid resuscitation can cause pulmonary oedema and worsen oxygenation. Excessive hypernatraemia from hypertonic saline can cause renal injury and rebound. Mannitol can cause hypovolaemia through diuresis. Prolonged hyperventilation causes cerebral ischaemia. Each intervention has a cerebral price, and the response must be measured, not assumed. [1] [2]
[1] [8]Prognosis & Disposition
Disposition follows the severity of the brain injury, the trend in conscious level and physiology, the CT findings, the response to treatment and the available local resources. Children with severe traumatic brain injury need paediatric intensive care and neurosurgical access, and those with moderate injury need close observation and repeated reassessment. [1] [11]
PICU or neurosurgical centre
- Severe TBI (GCS 8 or below) or any deterioration
- Operable intracranial haematoma on CT
- Need for ICP monitoring or vasoactive support
- Any need for monitoring or care unavailable locally
Ward or high-dependency
- Moderate TBI with stable observations and normal CT
- Requires close neurological observation
- Observed for delayed deterioration
- Named escalation pathway in place
Discharge when defensible
- Mild TBI with GCS 15, normal CT and no high-risk features
- Stable and improving after observation
- Caregiver understands warning signs
- Specific safety net, follow-up and pending-result ownership agreed
The discharge safety net for a child sent home after a mild head injury must state what changes to watch for, how urgently to act, and exactly where or how to get help. Persistent or worsening headache, repeated vomiting, increasing drowsiness, confusion, seizure, weakness or visual changes are reasons to return immediately. Use teach-back to confirm caregiver understanding, document it, and connect the family to the medical home or primary care. After a critical event, explain what happened and what remains uncertain, invite questions, and consider debriefing for the child, family and team. [1]
Outcome after severe paediatric traumatic brain injury depends on the severity of the primary injury, the quality of neuroprotection, the presence of secondary insults, and the timeliness of surgical and intensive care. Children have greater potential for recovery than adults, but also a longer period of vulnerability to developmental disruption. Long-term follow-up addresses cognitive, behavioural, physical and educational needs. [11]
Special Populations
Adapt how you assess, communicate and examine, but never lower the standard for recognising deterioration or applying the neuroprotection bundle. Evidence is sparse for some adaptations, so present them as safer practice rather than proven improvements. [1]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Infant with possible abusive head trauma | Lower threshold for CT, retinal examination, skeletal survey; safeguarding in parallel | Stabilise first; do not delay resuscitation for safeguarding procedures |
| Child with pre-existing disability or neurodiversity | Obtain individual baseline; use personal emergency plan; adapt communication | Do not attribute abnormal signs to baseline without reassessment |
| Technology-dependent child | Assess child and device; use caregiver expertise; personal emergency plan | Do not assume baseline observations are normal for age |
| Adolescent with intoxication | Drug and alcohol screen; private history; keep intracranial causes open | Do not attribute reduced consciousness to alcohol alone |
| Rural or remote setting | Call retrieval early; run full neuroprotection bundle during wait | Do not delay resuscitation for transport logistics |
| Indigenous or migrant family | Professional interpreter; culturally safe communication; understand access barriers | Do not let communication barriers delay neuroprotection |
Safeguarding runs in parallel with medical care, but immediate stabilisation and safety come first. Ask only necessary open, non-leading questions. Explain confidentiality and information sharing, document objective findings and spontaneous words, preserve evidence when safe, and use the local safeguarding pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [11]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The foundational guideline for severe paediatric traumatic brain injury is the Brain Trauma Foundation second edition, published in 2012 as Guidelines for the Acute Medical Management of Severe Traumatic Brain Injury in Infants, Children, and Adolescents. It provides evidence-based recommendations on hyperosmolar therapy, ventilation, blood pressure targets, seizure prophylaxis and ICP monitoring. The Brain Trauma Foundation has since transitioned to a Living Evidence model that updates recommendations as new evidence accrues. [1]
The evidence base has important gaps. Many recommendations are extrapolated from adult studies, and paediatric-specific randomised trials are rare. The choice between hypertonic saline and mannitol has been studied in observational and systematic-review evidence but not in a large definitive paediatric randomised trial. Both agents reduce intracranial pressure, and recent outcome studies show no significant mortality difference, so the choice often depends on local protocol and the individual child's physiology. [2] [3] [4]
The historical concern that ketamine raises intracranial pressure has been challenged by a multicentre study showing no clinically significant acute rise in ventilated children with severe traumatic brain injury. This is an evolving area, and ketamine is increasingly used as an induction agent in paediatric neurotrauma, particularly where haemodynamic stability is a priority. [5]
Jurisdictional implementation
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne head injury guideline supports local implementation of CT decision rules, observation and escalation. Retrieval systems, observation protocols and mandatory reporting remain state, territory or service specific. The RACP General Paediatrics Advanced Training Curriculum frames acute neurotrauma within Learning Objective 2.2.3 and 2.4.4. In Aotearoa New Zealand, verify the active local retrieval and neurosurgical referral system rather than borrowing an Australian threshold.
Global and low-resource settings: the principles of neuroprotection are universal, but resource constraints change implementation. Avoidable hypoxia and hypotension are the most modifiable causes of poor outcome worldwide. Protocol-driven prehospital care, early oxygen, normocapnic ventilation, isotonic fluid for hypotension, and rapid referral to the nearest neurosurgical capability are the high-yield interventions regardless of setting.
Exam Pearls
Concept
- Primary injury is fixed; secondary injury is preventable
- Neuroprotection is the organising principle of every action
- The brain needs oxygen, perfusion, normocapnia, cool, seizure-free
Primary survey
- ABCDE with cervical spine control
- Intubate for GCS 8 or below with rapid sequence
- Oxygen and normocapnia; no prophylactic hyperventilation
- Isotonic fluid; maintain age-appropriate blood pressure
- Head 30 degrees up and midline
Raised ICP
- General measures first: position, sedation, normocapnia, normotension
- Hyperosmolar: 3 percent saline bolus or mannitol
- Cushing triad is late and pre-terminal
- Unilateral pupil is herniation until proven otherwise
Escalation
- Call neurosurgery at recognition, not after CT
- Call retrieval before local support is exceeded
- Urgent CT when stable enough to scan
- Never send an unstable child to CT alone
Pitfalls
- No delayed intubation
- No prophylactic hyperventilation
- No hypotonic fluid
- No unescorted CT
- Do not forget glucose, C-spine and safeguarding
“Recognise major head injury and call for help → ABCDE with C-spine control → intubate for GCS 8 or below → oxygen and normocapnia → isotonic fluid and maintain blood pressure → head 30 degrees up → hyperosmolar therapy for raised ICP → seizure prophylaxis → urgent CT → neurosurgery and retrieval early.”
Viva: the child who needs intubation
A child with a Glasgow Coma Scale of 8 or below after head injury cannot protect their airway. Intubate using rapid sequence induction with preoxygenation, a neuro-friendly induction agent that maintains blood pressure, and a muscle relaxant. Confirm with waveform capnography. Avoid coughing, bucking and prolonged laryngoscopy, because each raises intracranial pressure. Secure the tube before transport, and keep manual in-line stabilisation throughout.
Viva: the ventilation target
Target normocapnia. Do not hyperventilate prophylactically, because hypocapnia causes cerebral vasoconstriction and ischaemia. Use waveform capnography to guide the rate. Reserve temporary mild hyperventilation for the acute signs of impending herniation, such as a unilateral dilated pupil, while hyperosmolar therapy and neurosurgical escalation proceed.
Structured oral: hypertonic saline or mannitol?
Both agents reduce intracranial pressure. The JAMA Network Open comparison found a numerically greater reduction with hypertonic saline, and a 2025 outcome study found no significant difference in mortality between the two. In practice, 3 percent saline is increasingly preferred first-line in paediatric practice because it expands circulating volume rather than causing diuresis, but the choice follows local protocol. Monitor serum sodium with saline and serum osmolality with mannitol.
References
- [1]Kochanek, Patrick M Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents--second edition Pediatric critical care medicine, 2012.PMID 22217782
- [2]Kochanek, Patrick M Comparison of Intracranial Pressure Measurements Before and After Hypertonic Saline or Mannitol Treatment in Children With Severe Traumatic Brain Injury JAMA network open, 2022.PMID 35267036
- [3]Chong, Shu-Ling Clinical Outcomes of Hypertonic Saline vs Mannitol Treatment Among Children With Traumatic Brain Injury JAMA network open, 2025.PMID 40067302
- [4]Afridi, Ayesha Therapeutic comparison of hypertonic saline and mannitol in pediatric intracranial hypertension: a systematic review and meta-analysis Child's nervous system, 2025.PMID 41420712
- [5]Laws, Jenna C Acute Effects of Ketamine on Intracranial Pressure in Children With Severe Traumatic Brain Injury Critical care medicine, 2023.PMID 36825892
- [6]Pajer, Heather B Adherence to Guidelines for Managing Severe Traumatic Brain Injury in Children American journal of critical care, 2021.PMID 34467382
- [7]Erickson, Sara L Mean Arterial Pressure and Discharge Outcomes in Severe Pediatric Traumatic Brain Injury Neurocritical care, 2021.PMID 33108627
- [8]Mai, Gavin Prehospital and emergency management of pediatric traumatic brain injury: a multicenter site survey Journal of neurosurgery Pediatrics, 2023.PMID 38716719
- [9]Lele, Anil V Cerebral Autoregulation-guided Management of Adult and Pediatric Traumatic Brain Injury Journal of neurosurgical anesthesiology, 2023.PMID 37523326
- [10]Gaither, Jarrod B Effect of Implementing the Out-of-Hospital Traumatic Brain Injury Treatment Guidelines: The Excellence in Prehospital Injury Care for Children Study (EPIC4Kids) Annals of emergency medicine, 2021.PMID 33187749
- [11]de Carvalho Panzeri Carlotti, Artur P Management of severe traumatic brain injury in pediatric patients: an evidence-based approach Neurological sciences, 2025.PMID 39476094
- [12]Agrawal, Sachin Neuromonitoring in Children with Traumatic Brain Injury Neurocritical care, 2024.PMID 37386341