Paeds · acute-care-resuscitation-and-toxicology
Iron, salicylate and toxic alcohol poisoning
Also known as Paediatric iron overdose · Paediatric salicylate poisoning · Methanol poisoning in children · Ethylene glycol poisoning in children · Desferrioxamine for iron toxicity · Fomepizole for toxic alcohol poisoning · High-anion-gap metabolic acidosis from poisoning · Urinary alkalinisation for salicylate
A fellowship approach to the child who has ingested iron, salicylate or a toxic alcohol: recognise the shared high-anion-gap metabolic acidosis and the poison-specific signature (the four-stage corrosive course and radiopaque tablets of iron, the mixed respiratory alkalosis plus anion-gap acidosis and tinnitus of salicylate, the dual anion-gap plus osmolal-gap with visual or renal-crystal clues of methanol and ethylene glycol), give the correct weight-based antidote (intravenous desferrioxamine 15 mg per kg per hour for iron, urinary alkalinisation to urine pH 7.5 to 8.0 for salicylate, intravenous fomepizole 15 mg per kg loading for toxic alcohols), decontaminate by poison, and avoid the three lethal traps of latent-phase reassurance, salicylate intubation without maintained hypocapnia, and waiting for toxic-alcohol levels before fomepizole.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
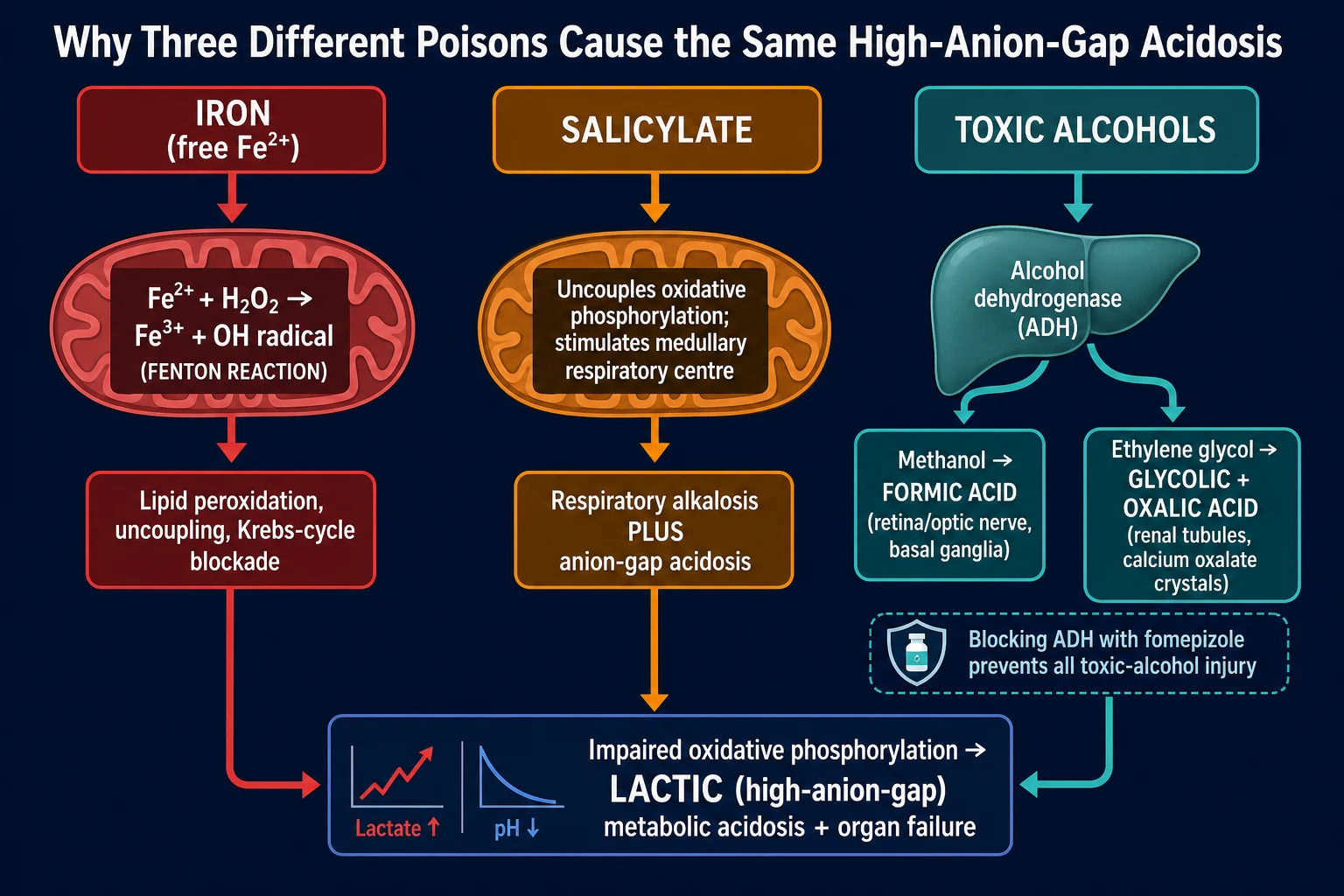
A child arrives with vomiting, fast deep breathing and a falling level. The venous gas shows a metabolic acidosis with a wide anion gap. The list of causes is long, but in paediatric toxicology three ingestions dominate this picture because each, by a different route, disables the mitochondrion: iron, salicylate, and the toxic alcohols methanol and ethylene glycol. Holding the three together is not a memory trick; it is how the examiner frames the question, because the resuscitation is shared while the antidote is poison-specific. [3] [10]
The unifying mechanism is impaired oxidative phosphorylation. Free iron catalyses the Fenton reaction, generating hydroxyl radicals that peroxidise mitochondrial membranes. Salicylate directly uncouples oxidative phosphorylation in the same way it does in the mitochondrion of a febrile cell. Methanol and ethylene glycol are harmless until hepatic alcohol dehydrogenase converts them to formic and oxalic acid, which inhibit mitochondrial cytochrome oxidase and precipitate in renal tubules. In every case the cell falls back on anaerobic glycolysis, lactate accumulates, and the child develops a high-anion-gap metabolic acidosis. The organ that fails first differs (the liver in iron, the brain and lung in salicylate, the retina and kidney in the toxic alcohols), but the metabolic signature is shared. [3] [10]
The clinical skill the examiner is testing is whether you can read the poison-specific clues out of the shared acidosis, give the correct weight-based antidote, choose the right decontamination, and avoid the three lethal traps that kill children: discharging during the deceptive iron latent phase, intubating a salicylate-toxic child without maintaining the hypocapnia that has been keeping them alive, and waiting for toxic-alcohol levels before starting fomepizole. Each trap is a failure to understand mechanism, not a failure of memory. [1] [6] [9]
Classification
The single most useful bedside classification sorts the three by their mechanism and their signature, because this decides the antidote. Iron injures by free-radical catalysis; salicylate by direct uncoupling and respiratory-centre stimulation; the toxic alcohols by enzyme-generated organic acids. Each carries a clue that the others do not. [3] [10]

Iron
Free-radical catalyst
- Mechanism: Fenton reaction (Fe2+ plus H2O2 produces hydroxyl radical) uncouples oxidative phosphorylation and blocks the Krebs cycle
- Signature: corrosive gastrointestinal injury in a four-stage course; radiopaque tablets on abdominal X-ray; hyperglycaemia and leucocytosis
- Antidote: intravenous desferrioxamine (deferoxamine) 15 mg per kg per hour
- Decontamination: whole-bowel irrigation; charcoal is useless because iron is a metal
Salicylate
Direct uncoupler
- Mechanism: uncouples oxidative phosphorylation AND directly stimulates the medullary respiratory centre
- Signature: mixed respiratory alkalosis plus high-anion-gap metabolic acidosis with tinnitus and deep rapid breathing
- Enhanced elimination: urinary alkalinisation with intravenous sodium bicarbonate to urine pH 7.5 to 8.0, potassium kept above 4 mmol per L
- Decontamination: activated charcoal 1 g per kg within 1 to 2 hours (salicylate IS adsorbed)
Toxic alcohols
Enzyme-generated acids
- Mechanism: hepatic alcohol dehydrogenase converts methanol to formic acid and ethylene glycol to glycolic and oxalic acid
- Signature: high-anion-gap acidosis PLUS elevated osmolal gap; visual loss in methanol, calcium oxalate crystalluria and AKI in ethylene glycol
- Antidote: intravenous fomepizole 15 mg per kg loading, started on suspicion, do not wait for levels
- Decontamination: none useful; charcoal and whole-bowel irrigation do not help small alcohols
A second axis classifies each poison by dose and stage. For iron the decisive number is the elemental iron ingested in mg per kg, not the salt weight; for salicylate the decisive distinction is acute versus chronic salicylism, which changes the dialysis threshold; for the toxic alcohols the decisive axis is the laboratory stage, because the osmolal gap dominates early and the anion gap dominates late. Each axis drives a specific decision, and conflating them is a classic error. [2] [5]
Epidemiology & Risk Factors
These three poisonings have a paediatric face. Iron remains one of the leading causes of accidental poisoning death in young children wherever adult prenatal or iron tablets are stored unsafely; a toddler needs only a handful of ferrous sulphate tablets to reach a lethal elemental dose. Salicylate poisoning in children is most often acute accidental ingestion of adult aspirin or oil of wintergreen, with a smaller burden of deliberate self-harm in adolescents. The toxic alcohols reach children through illicit or contaminated alcohol, windscreen washer, antifreeze, paint thinner and, in recent outbreaks, methanol-contaminated hand sanitiser. [1] [4] [11]
The risk of a severe outcome clusters around three questions for every ingestion: how much was taken (calculated as elemental iron for iron, mg per kg for salicylate, mL per kg for the toxic alcohols), what formulation (immediate-release versus sustained-release), and how quickly the correct antidote was started. A young age and low weight raise the mg per kg burden of even a small number of tablets; sustained-release and enteric-coated formulations delay and prolong absorption, distorting the expected timeline; co-ingestion with paracetamol is common in adolescent self-harm and compounds hepatic injury. [2] [4]
Dose-related
- Iron: elemental iron over 40 mg per kg significant, over 60 severe; a few adult ferrous sulphate tablets exceed 40 mg per kg in a 10 kg toddler
- Salicylate: oil of wintergreen is highly concentrated; as little as 4 mL can kill a toddler
- Toxic alcohols: a potentially toxic methanol dose is around 0.1 mL per kg; lethal around 0.5 to 1 mL per kg
- Co-ingestion with paracetamol in adolescent self-harm worsens hepatic prognosis and masks the picture
Formulation-related
- Sustained-release and enteric-coated iron and aspirin delay and prolong absorption
- Peak levels shift from 4 to 6 hours to 8 to 12 hours or beyond
- Repeat levels and longer observation are mandatory; never discharge at 6 hours
- Liquid iron and methyl salicylate absorb rapidly with an early severe peak
Patient and system factors
- Young infant or child with low reserve and a low weight-based threshold
- Chronic salicylate therapy (Kawasaki, rheumatic disease) raises tissue levels
- Renal or hepatic disease reduces clearance and lowers the dialysis threshold
- Rural or remote setting with transport delay: call retrieval early
Pathophysiology
The reason the three poisons share a metabolic signature is that they all disable the mitochondrion, but by three different doors. Following each pathway to its organ target explains every clinical feature and every antidote. [3] [10]
Iron. The body has no excretory route for iron; all balance is at absorption. In overdose, absorbed iron exceeds the binding capacity of transferrin and circulates as free iron. Free iron is directly corrosive to the gastrointestinal mucosa, producing the haemorrhagic gastritis of stage 1. It is then taken up by cells, especially hepatocytes, and catalyses the Fenton reaction: Fe2+ plus hydrogen peroxide yields Fe3+ plus the hydroxyl radical. The hydroxyl radical peroxidises mitochondrial membranes, uncouples oxidative phosphorylation, inhibits aconitase in the Krebs cycle, and inhibits the sodium-potassium ATPase. The cell switches to anaerobic glycolysis and generates lactate; the centrilobular hepatocyte, the most metabolically active cell in the liver, dies first, producing the zone-3 necrosis shared with paracetamol. Free iron also directly inhibits thrombin, which is why the early coagulopathy precedes hepatic synthetic failure. [3]
Salicylate. Salicylate crosses into the mitochondrion and directly uncouples oxidative phosphorylation, increasing oxygen consumption and heat production (the hyperthermia is an uncoupling effect, not a set-point fever, so antipyretics do not help). It also directly stimulates the medullary respiratory centre, producing the primary respiratory alkalosis that characterises the early adult picture. The third effect is disturbance of the Krebs cycle, generating ketoacids and organic acids. The net result is the mixed respiratory alkalosis plus high-anion-gap metabolic acidosis. In children, the metabolic acidosis tends to dominate from the outset, and hypoglycaemia, including cerebral hypoglycaemia with a normal plasma glucose, is a particular threat. [6]
Toxic alcohols. Methanol and ethylene glycol are themselves only mildly intoxicating; the injury is downstream of alcohol dehydrogenase. Methanol is converted to formaldehyde and then to formic acid, which inhibits mitochondrial cytochrome c oxidase in the retina and optic nerve (causing the snowstorm vision and blindness) and injures the basal ganglia. Ethylene glycol is converted to glycoaldehyde, glycolic acid (the main acid load), glyoxylic acid and finally oxalic acid, which chelates calcium and precipitates as calcium oxalate crystals in the renal tubules, causing acute tubular necrosis and hypocalcaemia. Because the toxicity is downstream of one enzyme, blocking alcohol dehydrogenase with fomepizole prevents all of it, which is why fomepizole is started on suspicion and not on a level. [9] [10]
Clinical Presentation
The presentation is built from the shared metabolic acidosis plus the poison-specific clues. The examiner tests whether you can read both layers at the bedside. [1] [6] [10]
Iron follows a stereotyped four-stage course. Stage 1 (0 to 6 hours) is direct corrosive gastrointestinal injury: vomiting, often haematemetic, abdominal pain and diarrhoea, with dehydration and hypovolaemic shock in the significant ingestion. Stage 2 (6 to 24 hours) is the deceptive latent phase: the child looks better while iron is being sequestered by transferrin and is about to spill into tissues. Stage 3 (12 to 48 hours) is systemic toxicity and the killer: high-anion-gap metabolic acidosis, shock, hepatic failure with transaminases over 1000, coagulopathy, renal failure and CNS depression. Stage 4 (4 to 6 weeks) is late gastric or pyloric outlet obstruction from scarring, presenting with post-prandial vomiting and weight loss. [1]
Salicylate presents with tinnitus, deafness, nausea, vomiting and deep rapid breathing (hyperpnoea is the cardinal sign, both rate and depth). The child is often febrile, sweaty and agitated. Severe poisoning brings confusion, seizures, coma and non-cardiogenic pulmonary oedema. The mixed respiratory alkalosis plus anion-gap metabolic acidosis on the venous gas, with tinnitus, is the signature. In chronic salicylism (the child on long-term aspirin), the neurotoxic picture dominates and is easily mistaken for delirium or sepsis. [5] [6]
The toxic alcohols present in two phases. Early there is only intoxication (ataxia, slurred speech, drowsiness) with a high osmolal gap. Hours later the organic acids appear and the child develops Kussmaul breathing from the metabolic acidosis. Methanol then declares itself with visual symptoms: blurred vision, snowstorm vision, photophobia, optic disc hyperaemia or oedema, and progression to blindness; basal ganglia signs may follow. Ethylene glycol declares itself with oliguria and flank pain from acute kidney injury, with calcium oxalate crystals in the urine, hypocalcaemia and a prolonged QT. [9] [11]
Atypical presentations
- Sustained-release iron or aspirin: delayed and prolonged stage 1; never discharge at 6 hours
- Co-ingested ethanol with a toxic alcohol delays the acidosis by competing for alcohol dehydrogenase, which can lull the clinician
- The young infant may show only poor feeding, floppiness and irritability
- Chronic salicylism may present as isolated confusion in a child on long-term aspirin
Features triggering safeguarding
- Repeated iron ingestion in a toddler with unsafe storage of adult tablets
- Adolescent deliberate self-harm ingestion requiring psychosocial assessment
- Discrepant history or delayed presentation suggesting neglect
- Document objectively and run safeguarding in parallel with resuscitation
Differential Diagnosis
The differential is the differential of the high-anion-gap metabolic acidosis, built in a fixed order: what can kill now, what is most likely, what is reversible, what is most harmful to miss. [6] [10]
Iron
- History of iron-tablet ingestion; calculate elemental iron mg per kg
- High-anion-gap metabolic acidosis with raised lactate; hyperglycaemia and leucocytosis
- Radiopaque tablets on abdominal X-ray in roughly 30 to 50 percent
- Serum iron over 500 microgram per dL; normal osmolal gap; no visual symptoms
Salicylate
- Mixed respiratory alkalosis plus high-anion-gap metabolic acidosis with tinnitus
- Hyperpnoea (rate and depth), hyperthermia, agitation, dehydration
- Serum salicylate level high; normal osmolal gap
- Treat with urinary alkalinisation and dialysis; check paracetamol co-ingestion
Toxic alcohols
- High-anion-gap acidosis PLUS elevated osmolal gap (the dual gap)
- Methanol: visual symptoms and optic disc changes; ethylene glycol: calcium oxalate crystals, AKI, hypocalcaemia
- Serum methanol or ethylene glycol level over 20 mg per dL
- Treat with fomepizole on suspicion; do not wait for levels
Mimics
- Diabetic ketoacidosis: hyperglycaemia, ketones, normal osmolal gap
- Lactic acidosis from shock, sepsis or metformin: high lactate, no toxin history
- Alcoholic or starvation ketoacidosis: low or near-normal glucose
- Isopropanol: ketosis (acetone) WITHOUT a high anion-gap acidosis; fomepizole NOT indicated
The key manoeuvre at the bedside is to send iron, salicylate and paracetamol levels together with a measured serum osmolality, and to calculate both the anion gap and the osmolal gap. A normal osmolal gap with radiopaque tablets and a high iron level closes the case for iron; a mixed respiratory alkalosis with tinnitus closes it for salicylate; a dual gap with visual or crystal clues closes it for the toxic alcohols. Always exclude co-ingested paracetamol in the deliberate self-harm ingestion, because paracetamol centrilobular necrosis compounds iron hepatitis and needs N-acetylcysteine. [1] [7]
Clinical & Bedside Assessment
Assess the child as an integrated whole, then layer the poison-specific history and examination on top. The history quantifies risk in minutes; the examination grades severity; together they decide the antidote and the decontamination. [1] [6]
History. Establish the time since ingestion, the agent (iron salt and formulation, aspirin or oil of wintergreen, methanol or ethylene glycol source), the elemental-iron dose or the volume of toxic alcohol, co-ingestants (especially paracetamol and ethanol), the intent (accidental versus self-harm), and the child's weight. Ask specifically about prenatal tablets, sustained-release preparations, and access to adult medications or household chemicals. In suspected toxic alcohol, ask about illicit alcohol, hand sanitiser, windscreen washer and antifreeze. [2]
Examination. Perform a focused ABCDE: heart rate and quality, blood pressure, respiratory rate AND depth (hyperpnoea is the salicylate cardinal sign), capillary refill, temperature, conscious level, and the abdomen for tenderness. In suspected methanol, examine the eyes: visual acuity, colour vision, fields, pupils and fundoscopy for optic disc hyperaemia. In suspected ethylene glycol, look for tetany from hypocalcaemia and feel for flank tenderness. A bedside capillary glucose is mandatory in every salicylate ingestion because cerebral hypoglycaemia can coexist with a normal plasma glucose. [6]
[1]The bedside assessment closes with a stated synthesis: the agent and the elemental dose, the current stage or severity, the specific antidote and its trigger, the decontamination plan, and the escalation timeline to the poisons centre and PICU. State this aloud to the team; a child with a high-anion-gap acidosis and an unclear history is treated empirically while levels are pending. [9]
Investigations
Stabilise first, then order each test for a named question. The investigation bundle has three layers: the shared metabolic tests, the poison-specific tests, and the rule-out co-ingestion tests. [1] [10]
Shared metabolic
- Venous blood gas: pH, bicarbonate, lactate, base excess
- Serum electrolytes plus calculated anion gap (Na minus Cl plus HCO3; normal 8 to 12 mmol per L)
- Capillary glucose: mandatory in salicylate for cerebral hypoglycaemia
- Measured serum osmolality by freezing-point depression plus calculated osmolality and the osmolal gap
Poison-specific
- Serum iron at 4 to 6 hours (over 500 microgram per dL significant); repeat at 8 to 12 hours for sustained-release
- Serum salicylate level (over 300 mg per L mild, 450 to 700 moderate, over 700 severe)
- Serum methanol and ethylene glycol levels: confirmatory, not decision-making
- Abdominal X-ray for radiopaque iron tablets; urine microscopy for calcium oxalate crystals
Rule-out co-ingestion and severity
- Serum paracetamol level at 4 hours; apply the Rumack-Matthew nomogram
- Serum ethanol level (high ethanol delays toxic-alcohol toxicity and confounds the osmolal gap)
- Coagulation, LFTs, renal function, calcium, FBC; ECG for QT in ethylene glycol
- Pregnancy test in adolescent girls; beta-hCG before antidotes in pregnancy
Interpret the osmolal gap with the timing caveat firmly in mind. The osmolal gap is the difference between the measured osmolality (by freezing-point depression, because vapour-pressure osmometers miss volatile alcohols) and the calculated osmolality (2 times sodium plus glucose plus urea, all in mmol per L). A normal osmolal gap is roughly minus 10 to plus 10 mOsm per kg; a gap over 20 strongly suggests a toxic alcohol or ethanol, but a normal gap late does not exclude the diagnosis because the parent has been metabolised. The empiric threshold to start fomepizole is a documented ingestion with acidosis, or a high anion-gap acidosis of unknown cause with an elevated osmolal gap, or strong clinical suspicion: do not wait for the methanol or ethylene glycol level. [9] [10]
[10]Management — Resuscitation
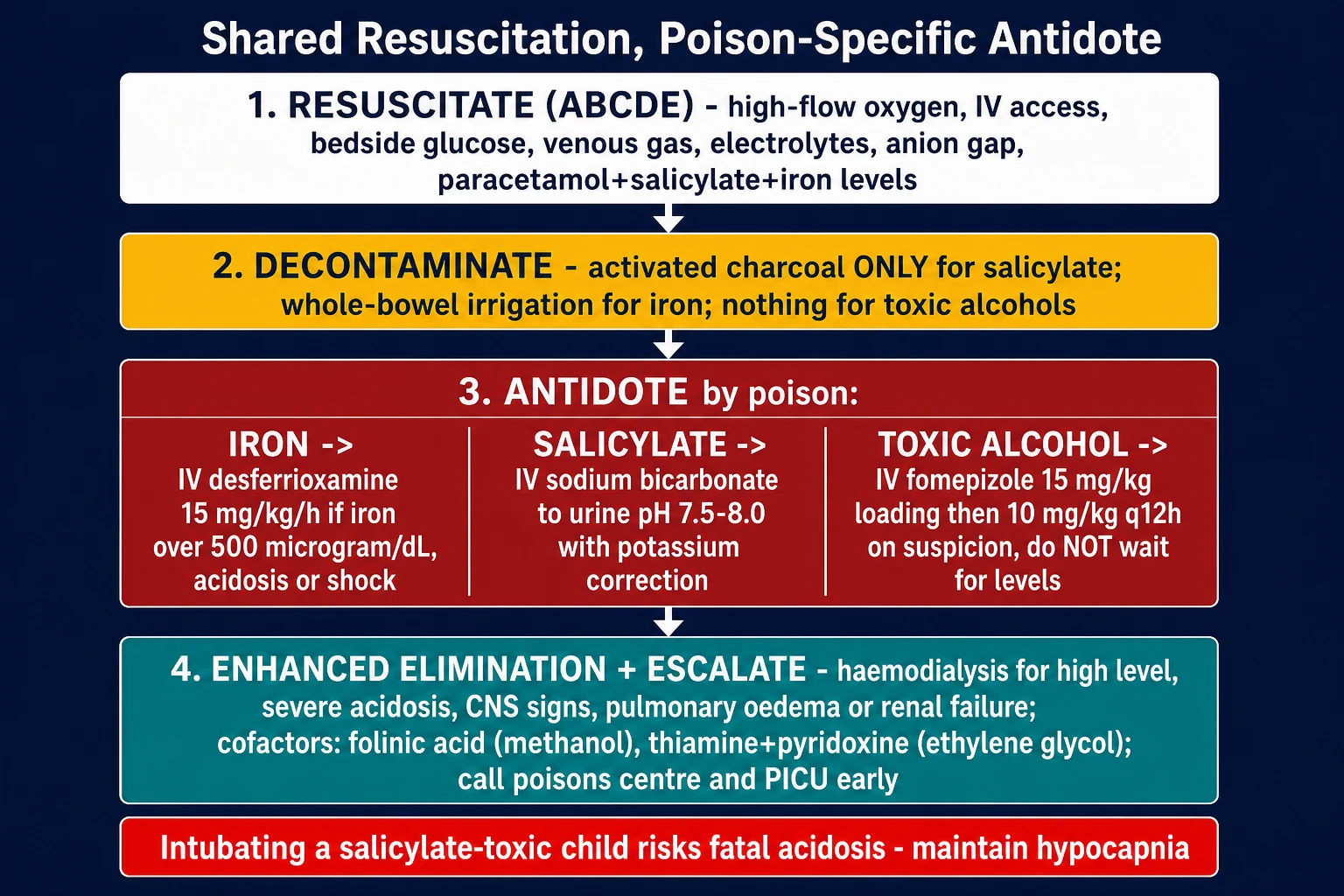
Resuscitation is shared across the three poisons and runs in parallel with the investigations and the first dose of antidote. The aims are to restore perfusion, secure the airway, support the compensatory hyperventilation of salicylate toxicity, take bloods before the antidote, and avoid the useless or harmful interventions. [1] [9]
The shared first-hour resuscitation bundle
Recognise and call for help
Declare the concern, call the senior paediatric, resuscitation and poisons-centre teams, name a leader, allocate roles, and bring weight-appropriate equipment and monitoring. Call retrieval early if dialysis, ventilation or intensive care may be needed locally unavailable.
Secure airway and breathing
Give high-flow oxygen if hypoxic; support ventilation if ineffective. In salicylate toxicity, DO NOT blunt the compensatory hyperventilation: if intubation is unavoidable, give a bicarbonate bolus, pre-oxygenase, use rapid sequence, and set the ventilator to maintain pre-intubation hypocapnia.
Establish access and take bloods before antidote
Gain IV or IO access; draw iron, salicylate, paracetamol, osmolality, electrolytes, anion gap, gas, glucose, coagulation, LFTs and renal function BEFORE desferrioxamine or fomepizole, which alter the assays.
Restore the circulation with reassessed fluid
Give isotonic crystalloid in weight-based aliquots of 10 to 20 mL per kg, stating the expected response and reassessing after each. Add dextrose in salicylate toxicity to prevent cerebral hypoglycaemia; correct dangerous hypoglycaemia immediately.
Decontaminate by poison
Activated charcoal 1 g per kg within 1 to 2 hours for salicylate (it IS adsorbed); whole-bowel irrigation for iron and for sustained-release aspirin bezoars; nothing useful for the toxic alcohols.
Give the poison-specific antidote on its trigger
Start intravenous desferrioxamine for iron over 500 microgram per dL, acidosis or shock; urinary alkalinisation for symptomatic salicylate; intravenous fomepizole on suspicion of a toxic alcohol. Do not wait for confirmatory levels to start fomepizole.
Reassess from the top
After every action, return to airway, breathing, circulation and consciousness, judge the trend in the anion gap and the level, and revise the plan for dialysis and escalation.
Management — Definitive & Stepwise
Once the shared resuscitation is running, definitive management moves to the poison-specific antidote, enhanced elimination, and the cofactors. Each antidote has an explicit weight-based dose and an explicit trigger, and the antidote and dialysis run in parallel where both are indicated. [1] [9]
Iron: intravenous desferrioxamine and whole-bowel irrigation
Desferrioxamine (deferoxamine) is a siderophore that binds free iron in a stable 1 to 1 complex, ferrioxamine, which is excreted in the urine and gives it the characteristic vin-rose colour. It is the definitive treatment for significant iron toxicity. [1] [3]
Intravenous desferrioxamine (deferoxamine) — iron toxicity
Whole-bowel irrigation with polyethylene-glycol electrolyte solution is the decontamination of choice for iron because activated charcoal does not adsorb a metal. Give it via a nasogastric tube at 20 to 40 mL per kg per hour (around 500 mL per hour in a young child) until the rectal effluent is clear and no tablets remain on a repeat abdominal X-ray. Continue it even after starting desferrioxamine if tablets remain. Activated charcoal is useless and obscures the endoscopic view; this is the single most important negative instruction in iron overdose. [1]
Salicylate: urinary alkalinisation and dialysis
The cornerstone of enhanced elimination in salicylate poisoning is urinary alkalinisation with intravenous sodium bicarbonate, titrated to a urine pH of 7.5 to 8.0. The mechanism is ion-trapping: unionised salicylic acid diffuses into the alkaline tubular urine, is deprotonated to the impermeant salicylate anion, and is trapped for urinary excretion. Renal clearance rises roughly five-fold at urine pH 8 versus pH 5. [6] [7]
Hypokalaemia prevents urinary alkalinisation from working because the kidney retains potassium by exchanging it for hydrogen, acidifying the tubular fluid; correct the potassium to over 4 mmol per L before and during alkalinisation. Add dextrose to the fluids to prevent cerebral hypoglycaemia. Modern practice has moved away from forced alkaline diuresis (large fluid volumes) toward urinary alkalinisation alone with modest fluid, because the active component is the alkalinisation, not the volume, and large volumes risk pulmonary oedema. [6] [8]
Haemodialysis is indicated for a salicylate level over 700 mg per L in acute poisoning (over 600 in chronic), severe metabolic acidosis with arterial pH under 7.20 to 7.25 unresponsive to bicarbonate, CNS toxicity (confusion, seizures, coma), non-cardiogenic pulmonary oedema, renal failure or an inability to alkalinise the urine, and clinical deterioration despite standard therapy. Use a bicarbonate-based dialysate and a paediatric circuit. After dialysis, continue alkalinisation and recheck the level every 2 to 4 hours for at least 12 to 24 hours because of rebound redistribution from tissue stores. [7] [8]
Toxic alcohols: fomepizole, cofactors and dialysis
The definitive intervention is to block alcohol dehydrogenase. Fomepizole (4-methylpyrazole) is a direct competitive inhibitor of alcohol dehydrogenase with no central nervous system effect, no hypoglycaemia and no monitoring burden, and it is preferred over ethanol in children for all of these reasons. Start it on suspicion, based on a documented ingestion with acidosis, a high anion-gap acidosis of unknown cause with an elevated osmolal gap, or the clinical picture (visual symptoms, calcium oxalate crystals); do not wait for the methanol or ethylene glycol level. [9] [10]
Intravenous fomepizole — toxic alcohol poisoning
Give the metabolic cofactors in parallel: folinic acid (leucovorin) 1 mg per kg intravenously (up to 50 mg) every 4 to 6 hours for suspected methanol, because folate-dependent metabolism speeds formate clearance; and thiamine and pyridoxine (vitamin B6) for suspected ethylene glycol, because they divert glyoxylate to non-toxic metabolites. Give intravenous sodium bicarbonate to target a serum pH over 7.20 to 7.30; in methanol this also traps formate in its anionic form and speeds renal clearance. Replace calcium in ethylene glycol only if symptomatic (tetany, seizures, QT prolongation), because over-correction worsens calcium oxalate deposition. Haemodialysis is indicated for a methanol or ethylene glycol level over 50 mg per dL, severe or worsening acidosis, renal failure, visual symptoms, or significant electrolyte disturbance; continue fomepizole through and after dialysis. [9] [10]
| Poison | First-line antidote | Decontamination | Dialysis threshold |
|---|---|---|---|
| Iron | Intravenous desferrioxamine 15 mg per kg per hour | Whole-bowel irrigation; charcoal useless | Iron over 1000 microgram per dL or refractory acidosis (consider) |
| Salicylate | Urinary alkalinisation with sodium bicarbonate to urine pH 7.5 to 8.0 | Activated charcoal 1 g per kg within 1 to 2 hours | Level over 700 mg per L acute or over 600 chronic; CNS or pulmonary signs; severe acidosis; renal failure |
| Methanol | Intravenous fomepizole 15 mg per kg loading plus folinic acid | None useful | Level over 50 mg per dL; severe acidosis; visual symptoms; renal failure |
| Ethylene glycol | Intravenous fomepizole 15 mg per kg loading plus thiamine and pyridoxine | None useful | Level over 50 mg per dL; severe acidosis; renal failure |
Specific Subtypes & Scenarios
The resuscitation structure stays the same, but the agent, the formulation, the age and the setting change what you watch for, which decontamination you choose, and how early you escalate. [2] [11]
Toddler accidental iron
- Calculate elemental iron mg per kg at once from the salt and tablet count
- Over 40 mg per kg: resuscitate, serum iron at 4 to 6 hours, whole-bowel irrigation
- Intravenous desferrioxamine for iron over 500 microgram per dL, acidosis or shock
- Prevention: child-resistant packaging and safe storage; poison-control education
Sustained-release iron or aspirin
- Delayed and prolonged absorption distorts stage 1 and shifts the peak to 8 to 12 hours
- Draw levels at 4 to 6 hours AND repeat at 8 to 12 hours
- Observe for at least 12 to 24 hours; never discharge at 6 hours
- Low threshold for whole-bowel irrigation and chelation
Methyl salicylate (oil of wintergreen)
- Highly concentrated: 1 mL equals roughly 1.4 g of aspirin; 4 mL can kill a toddler
- Treat any ingestion as life-threatening regardless of small volume
- Activated charcoal within 1 hour; aggressive urinary alkalinisation; early dialysis
- Paediatric ICU; notify the poison centre
Chronic salicylism
- Child on long-term aspirin (Kawasaki, rheumatic disease)
- Neuro-predominant picture; lower dialysis threshold (over 600 mg per L)
- Level under-correlates with severity because of greater tissue distribution
- Treat as acute-on-chronic; do not be reassured by a moderate level
Toxic alcohol in a child
- Illicit or contaminated alcohol, hand sanitiser, windscreen washer, antifreeze
- Start fomepizole on suspicion; paediatric weight-based dosing
- Co-ingested ethanol delays the acidosis by competing for alcohol dehydrogenase
- Paediatric dialysis circuit; cofactors folinic acid, thiamine, pyridoxine
Rural or remote setting
- Call retrieval and the poisons centre in parallel with resuscitation
- Begin antidote before transfer if locally available
- State the dialysis, ventilation and intensive-care needs and the transport time
- Agree a contingency for deterioration or transport delay
In pregnancy, maternal outcome determines fetal outcome. Iron overdose in pregnancy typically involves prenatal iron, and intravenous desferrioxamine is indicated for severe maternal toxicity despite placental transfer, because untreated maternal iron toxicity is far more dangerous to the fetus than chelation. Salicylate crosses the placenta and the fetus is acidotic relative to the mother, so salicylate is ion-trapped in the fetal central nervous system; maternal alkalinisation alkalinises the fetus and reduces trapping. Involve obstetrics and monitor the fetus throughout. [1] [6]
Complications & Pitfalls
Most preventable harm in these three poisonings comes from one of three errors: being reassured by the iron latent phase, intubating the salicylate-toxic child without maintaining hypocapnia, or waiting for toxic-alcohol levels before fomepizole. Each is a failure to understand mechanism, not a failure of memory. [1] [6] [9]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Discharging during the iron latent phase | The child looks well while iron spills into tissues and stage 3 follows | Disposition rests on the serum iron and the acidosis, not the appearance; observe for sustained-release |
| Giving activated charcoal for iron | Charcoal does not adsorb a metal; it is useless and obscures endoscopy | Use whole-bowel irrigation with polyethylene glycol for iron; charcoal only for salicylate |
| Intubating salicylate without hypocapnia | Loss of compensatory hyperventilation lets PaCO2 rise and the child crashes | Pre-oxygenase, give a bicarbonate bolus, and set the ventilator to maintain pre-intubation hypocapnia |
| Waiting for toxic-alcohol levels before fomepizole | Every hour of delay converts more parent alcohol into toxic metabolite | Start fomepizole on suspicion from the dual gap or the clinical picture |
| Failing to correct hypokalaemia in salicylate | Urinary alkalinisation fails because the kidney acidifies the tubular fluid | Keep potassium over 4 mmol per L before and during alkalinisation |
| Unit-confusion on the salicylate level | 70 mg per dL equals 700 mg per L equals the dialysis threshold | Confirm the local unit before deciding on dialysis |
| Prolonged desferrioxamine | Acute lung injury and Yersinia enterocolitica sepsis from prolonged chelation | Stop when the iron is falling and the acidosis has resolved; do not chelate to zero |
| Missing rebound after dialysis or stopping alkalinisation | Tissue stores redistribute into the blood to toxic levels | Recheck the level every 2 to 4 hours for 12 to 24 hours; resume treatment if it rises |
After resuscitation, watch actively for harm from the disease and the treatment: non-cardiogenic pulmonary oedema in salicylate, desferrioxamine lung injury and Yersinia sepsis in iron chelation, ethanol-induced hypoglycaemia if ethanol is used for a toxic alcohol, and acute kidney injury from ethylene glycol. The late complications are gastric or pyloric outlet obstruction at 4 to 6 weeks after iron, permanent visual loss after methanol, and chronic kidney disease after ethylene glycol. [1] [10]
[1] [6] [9]Prognosis & Disposition
Disposition follows the trend in the level and the response to treatment, not a single reassuring number. Consider the agent and dose, the formulation, the severity and reversibility of organ dysfunction, the local resources, the transport risk, and whether the family can carry the plan forward. [1] [7]
ICU or retrieval
- Any stage-3 iron feature: shock, acidosis, hepatic failure, coma
- Salicylate over 700 mg per L, CNS signs, pulmonary oedema, severe acidosis, need for dialysis
- Toxic alcohol with visual symptoms, renal failure, severe acidosis, or need for dialysis or prolonged fomepizole
- Need for mechanical ventilation, vasoactive support or a paediatric dialysis circuit
Admit or high-dependency
- Symptomatic but stable moderate toxicity on antidote and responding
- Sustained-release iron or aspirin requiring 12 to 24 hour observation with serial levels
- Co-ingestion being worked up; psychosocial assessment in progress
- A named escalation pathway exists
Discharge from ED
- Asymptomatic throughout with a clearly falling level and normal acid-base
- Immediate-release formulation observed for at least 6 hours
- No residual tablets on abdominal X-ray; no CNS or pulmonary signs
- Psychosocial and safeguarding assessment complete; return precautions and poison-centre number given
Modern series report iron mortality under 5 percent with prompt chelation, and acute salicylate mortality under 1 percent when recognised early. The toxic alcohols carry significant morbidity from visual loss and renal failure when treatment is delayed. The strongest modifiable predictor of death in all three is the delay to the correct antidote. Give the family a clear safety net: what change to watch for, how urgently to act, where to return, and how to secure the agent. [1] [4]
Special Populations
Adapt how you assess, dose and escalate, but never lower the standard for recognising the high-anion-gap acidosis. The principles apply across ages and abilities; the differences are in weight, reserve, drug handling and the social context. [1] [11]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Toddler (1 to 4 years) | Calculate elemental iron mg per kg; weight-based charcoal 1 g per kg, desferrioxamine and fomepizole; paediatric whole-bowel-irrigation rate | A few adult tablets exceed the toxic dose; do not be reassured by small numbers |
| Adolescent deliberate self-harm | Exclude paracetamol co-ingestion at 4 hours; psychosocial assessment after medical stabilisation; secure the agent | Safeguarding and mental-health pathways run in parallel with resuscitation |
| Chronic salicylate therapy | Treat as acute-on-chronic; lower dialysis threshold (over 600 mg per L); neurotoxic picture dominates | Level under-correlates with severity because of tissue distribution |
| Pregnancy | Desferrioxamine indicated for severe maternal iron toxicity; maternal alkalinisation protects the acidotic fetus in salicylate | Maternal outcome determines fetal outcome |
| Chronic kidney or liver disease | Lower clearance and lower dialysis threshold; altered protein binding in salicylate | Escalate on physiology and risk context |
| Technology-dependent or developmentally disabled child | Compare with the caregiver's baseline; use the personal emergency plan and adapted communication | A changed baseline is the key sign, not a single number |
Safeguarding runs in parallel with medical care, and immediate stabilisation comes first. Iron and salicylate poisoning can arise from neglect, unsafe storage of adult medications, induced or fabricated illness, or adolescent self-harm. Ask only necessary open, non-leading questions, document objective findings and spontaneous words, and use the local safeguarding pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [2]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The structure of management for all three poisons is strongly endorsed by the major toxicology sources: resuscitate, decontaminate by poison, give the weight-based antidote on its trigger, and enhance elimination with dialysis when indicated. What remains source-specific is the exact threshold for dialysis and the local preference for fomepizole over ethanol, which must be verified against the active regional guideline. [7] [9]
EXTRIP salicylate workgroup
Annals of Emergency Medicine
Systematic review and expert consensus on extracorporeal treatment for salicylate poisoning
Key finding
Intermittent haemodialysis is the modality of choice for severe salicylate poisoning; dialysis is recommended at a level over 700 mg per L in acute poisoning (over 600 chronic), or for severe acidosis, CNS signs, pulmonary oedema or renal failure.
Practice change
EXTRIP set the modern dialysis thresholds for salicylate poisoning and confirmed intermittent haemodialysis as first-line extracorporeal therapy.
The Brent 2009 New England Journal of Medicine review established fomepizole as the preferred antidote for ethylene glycol and methanol poisoning, demonstrating efficacy and a far better safety profile than ethanol, particularly in children where ethanol causes CNS depression and hypoglycaemia. Fomepizole has since replaced ethanol as first line wherever it is available. The paediatric case series confirm weight-based dosing and the need for paediatric dialysis circuits. [9] [11]
For iron, the AACT/EAPCCT 2005 consensus (Manoguerra) set the out-of-hospital triage thresholds still in use: refer to the emergency department for any symptoms, any ingestion over 40 mg per kg elemental iron, any sustained-release ingestion over 40 mg per kg, or any intentional ingestion; home observation is acceptable only for asymptomatic ingestions under 20 mg per kg. Whole-bowel irrigation is endorsed by the AACT/EAPCCT as the decontamination of choice for iron, and the 2023 clinical-toxicology consensus reaffirmed that activated charcoal has no role in metal poisoning. [2] [1]
For salicylate, the Prescott 1982 BMJ study established that alkalinisation of the urine, not large fluid volumes, is the active component of enhanced elimination, moving practice away from forced alkaline diuresis toward urinary alkalinisation alone. The rebound phenomenon after dialysis or cessation of alkalinisation is now well characterised and drives serial-level monitoring for 12 to 24 hours. [6] [8]
Jurisdictional implementation
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne clinical practice guidelines on iron, salicylate and toxic-alcohol poisoning support local implementation, and the Australasian poisons centres (Poisons Information Centre on 13 11 26 in Australia, 0800 764 766 in New Zealand) provide 24-hour telephone advice. Fomepizole availability, retrieval systems and dialysis circuits remain state, territory or service specific. In Aotearoa New Zealand, verify the active local pathways and fomepizole stock rather than borrowing an Australian threshold.
Exam Pearls
Recognition
- Shared lesion: high-anion-gap metabolic acidosis from impaired oxidative phosphorylation
- Iron: corrosive four-stage course, radiopaque tablets, elemental-iron dose
- Salicylate: mixed respiratory alkalosis plus anion-gap acidosis, tinnitus, hyperpnoea
- Toxic alcohols: dual anion-gap plus osmolal gap, visual loss or calcium oxalate crystals
Decontamination
- Activated charcoal 1 g per kg within 1 to 2 hours for salicylate only
- Whole-bowel irrigation for iron and sustained-release aspirin bezoars
- Nothing useful for the toxic alcohols
- Charcoal is useless for iron (a metal) and for toxic alcohols (small molecules)
Antidotes
- Iron: intravenous desferrioxamine 15 mg per kg per hour for iron over 500 microgram per dL, acidosis or shock
- Salicylate: urinary alkalinisation to urine pH 7.5 to 8.0 with potassium over 4 mmol per L
- Toxic alcohols: intravenous fomepizole 15 mg per kg loading on suspicion, do not wait for levels
- Cofactors: folinic acid (methanol), thiamine and pyridoxine (ethylene glycol)
Dialysis
- Salicylate over 700 mg per L acute or over 600 chronic, CNS or pulmonary signs, severe acidosis, renal failure
- Toxic alcohol level over 50 mg per dL, severe acidosis, visual symptoms, renal failure
- Iron over 1000 microgram per dL or refractory acidosis (consider)
- Continue fomepizole through and after dialysis; recheck salicylate for rebound
Lethal traps
- No discharge during the iron latent phase
- No charcoal for iron
- No salicylate intubation without maintained hypocapnia
- No waiting for toxic-alcohol levels before fomepizole
“Recognise the shared high-anion-gap acidosis and read the poison-specific signature → resuscitate and decontaminate by poison → give the weight-based antidote on its trigger (desferrioxamine for iron, alkalinisation for salicylate, fomepizole for toxic alcohols) → enhance elimination with dialysis when indicated → avoid the three lethal traps and escalate before local support is exceeded.”
Viva: why is charcoal useless for iron and toxic alcohols but works for salicylate?
Activated charcoal adsorbs organic molecules by surface binding. Salicylate is an organic acid and binds charcoal well, so it is the one of the three that charcoal helps. Iron is a metal, not an organic molecule, so charcoal does not bind it and is useless; the decontamination of choice for iron is whole-bowel irrigation with polyethylene glycol. The toxic alcohols are small molecules that charcoal does not adsorb in any clinically useful quantity, and they are absorbed rapidly, so charcoal has no role; the intervention that matters is blocking alcohol dehydrogenase with fomepizole. [1] [9]
Viva: why does a normal osmolal gap late not exclude a toxic alcohol?
Early in toxic-alcohol poisoning the unmetabolised parent alcohol is osmotically active, so the osmolal gap is high. As alcohol dehydrogenase converts the parent to organic acids, the parent disappears (the osmolal gap falls) and the acids accumulate (the anion gap rises). A clinician who measures the gaps only late sees a normal osmolal gap with a high anion gap and may wrongly dismiss the diagnosis. The correct reading is that the two gaps are inversely related over time; treat on the clinical picture and the anion gap, and start fomepizole on suspicion. [10]
Structured oral: salicylate-toxic child needing intubation
A salicylate-toxic child compensates their metabolic acidosis with hyperventilation; the low PaCO2 is keeping them alive. Intubation removes that compensation: sedation, paralysis and a normally-set ventilator let PaCO2 rise, pH fall, salicylate shift into the central nervous system, and the child can crash within minutes. If intubation is unavoidable, give a bicarbonate bolus and optimise the pH first, pre-oxygenase, use rapid sequence, set the ventilator to a respiratory rate of 20 to 30 with the minute ventilation matched to the pre-intubation hypocapnia, and have haemodialysis ready because the acidosis will worsen. [6] [7]
References
- [1]Chang, Timothy P; Rangan, Cyrus Iron poisoning: a literature-based review of epidemiology, diagnosis, and management Pediatric Emergency Care, 2011.PMID 21975503
- [2]Manoguerra, Anthony S; Erdman, Andrew R; Booze, Laura L; Christianson, George; Wax, Paul M; Scharman, Elizabeth J; Woolf, Alan D; Keyes, Daniel C; Olson, Kent R; Chyka, Peter; Caravati, E Martin; Troutman, William G Iron ingestion: an evidence-based consensus guideline for out-of-hospital management Clinical Toxicology, 2005.PMID 16255338
- [3]Rafati Rahimzadeh, Milad; Rafati Rahimzadeh, Mahsa; Kazemi, Sara; Moghadamnia, Ali Akbar Iron; benefits or threatens (with emphasis on mechanism and treatment of its poisoning) Human and Experimental Toxicology, 2023.PMID 37526177
- [4]Chandran, Jeethu; Khanna, Kshitij; Jayashree, M; Gautam, Vikas; Sharma, Aruna; Singh, Meenu Accidental iron poisoning in children - Experience from a teaching institution Journal of Family Medicine and Primary Care, 2023.PMID 38074262
- [5]Gaudreault, Pierre; Temple, Anthony R; Lovejoy, Frederick H Jr The relative severity of acute versus chronic salicylate poisoning in children: a clinical comparison Pediatrics, 1982.PMID 7122154
- [6]Snodgrass, Wirt Salicylate toxicity Pediatric Clinics of North America, 1986.PMID 3960612
- [7]Juurlink, David N; Gosselin, Sophie; Kielstein, Jan T; Ghannoum, Marc; Lavergne, Valerie; Nolin, Thomas D; Hoffman, Robert S; EXTRIP Workgroup Extracorporeal treatment for salicylate poisoning: systematic review and recommendations from the EXTRIP workgroup Annals of Emergency Medicine, 2015.PMID 25986310
- [8]O'Keefe, Meghan; Stanton, Michele; Feldman, Ruth; Theobald, Jennifer Incidence of rebound salicylate toxicity following cessation of urine alkalinization Clinical Toxicology, 2023.PMID 37427892
- [9]Brent, Jeffrey Fomepizole for ethylene glycol and methanol poisoning New England Journal of Medicine, 2009.PMID 19458366
- [10]Kraut, Jeffrey A; Xing, Xuejing Toxic Alcohols New England Journal of Medicine, 2018.PMID 29342392
- [11]Lin, Po-Yin; Hsu, Chien-Chang; Chen, Chih-Hsien; Huang, Yi-Chun; Lee, Chee-Jen; Chen, Chien-Chang Use of fomepizole in pediatric methanol exposure: the first case report in Taiwan and a literature review Pediatrics and Neonatology, 2016.PMID 24332660