Paeds · acute-care-resuscitation-and-toxicology
Major trauma and paediatric trauma systems
Also known as Paediatric major trauma · Paediatric trauma primary survey · Trauma team and team activation · Paediatric trauma system and retrieval · Damage control resuscitation in children
A fellowship approach to the injured child within an organised paediatric trauma system. Run a trauma primary survey that controls catastrophic haemorrhage first and protects the cervical spine, lead a structured trauma team with defined roles, use weight-based fluid and early blood for haemorrhagic shock, avoid the lethal triad, apply paediatric imaging decision rules, escalate to a paediatric trauma centre before local support is exceeded, and reassess after every intervention.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Major trauma means serious injury that carries a threat to life, limb or function, and in children it is managed by a system rather than by a single clinician. That system has three moving parts: pre-hospital triage that sends the right child to the right place, a hospital trauma team that runs a structured primary survey, and a retrieval and definitive-care network that catches the child when local resources are exceeded. Your job at the bedside is the middle layer, but you must understand the whole system because your decisions feed into it. [6] [11]
The paediatric primary survey is the ABCDE method adapted for trauma. The adaptation matters: a child who is bleeding to death exsanguinates before an airway problem kills them, so many services teach <C>ABCDE, controlling catastrophic external haemorrhage first, then proceeding through airway with cervical spine control, breathing, circulation, disability and exposure. You treat each life threat the moment you find it, then you return to the start and reassess. This treat-as-found, reassess-from-the-top discipline is what separates a trauma team from a crowd of clinicians around a trolley. [6] [8]
[6] [11]Trauma resuscitation is damage control, not definitive repair. The first goal is to stop the bleeding, restore perfusion, prevent hypothermia, acidosis and coagulopathy, and keep the brain perfused and oxygenated. Definitive surgery, imaging for every injury, and the full secondary survey come after the child is stable, and some of them come after transfer to a centre that can deliver them. Ordering a scan on an unstable child is a classic and dangerous error. [5] [8]
The first five minutes of a paediatric trauma call
Pre-arrival and team
Receive a pre-alert, confirm the trauma team is activated with named roles, and prepare age- and weight-appropriate airway, access and warming equipment.
Handover and <C>A
Take a structured pre-hospital handover, then control catastrophic haemorrhage with direct pressure or a tourniquet before airway work.
A to E, treat as found
Run airway with cervical spine control, breathing, circulation, disability and exposure in order, treating each threat the moment it is found.
Reassess and escalate
Return to the top after every intervention; if injury severity exceeds local capability, activate retrieval and paediatric trauma centre referral in parallel.
Secondary survey
Once the child is stable, take an AMPLE history, perform a head-to-toe secondary survey, apply imaging decision rules, and re-evaluate.
Classification
Classify the injured child along three axes that together decide the tempo and the destination: physiological severity, anatomical injury pattern, and system capability. Physiological severity is what you assess at the bedside and it drives immediate actions. Anatomical pattern and system capability drive triage, transfer and definitive care. The two must not be confused: a child can have a dangerous anatomical injury while still looking compensated, which is why mechanism and physiology are both part of activation. [7] [11]
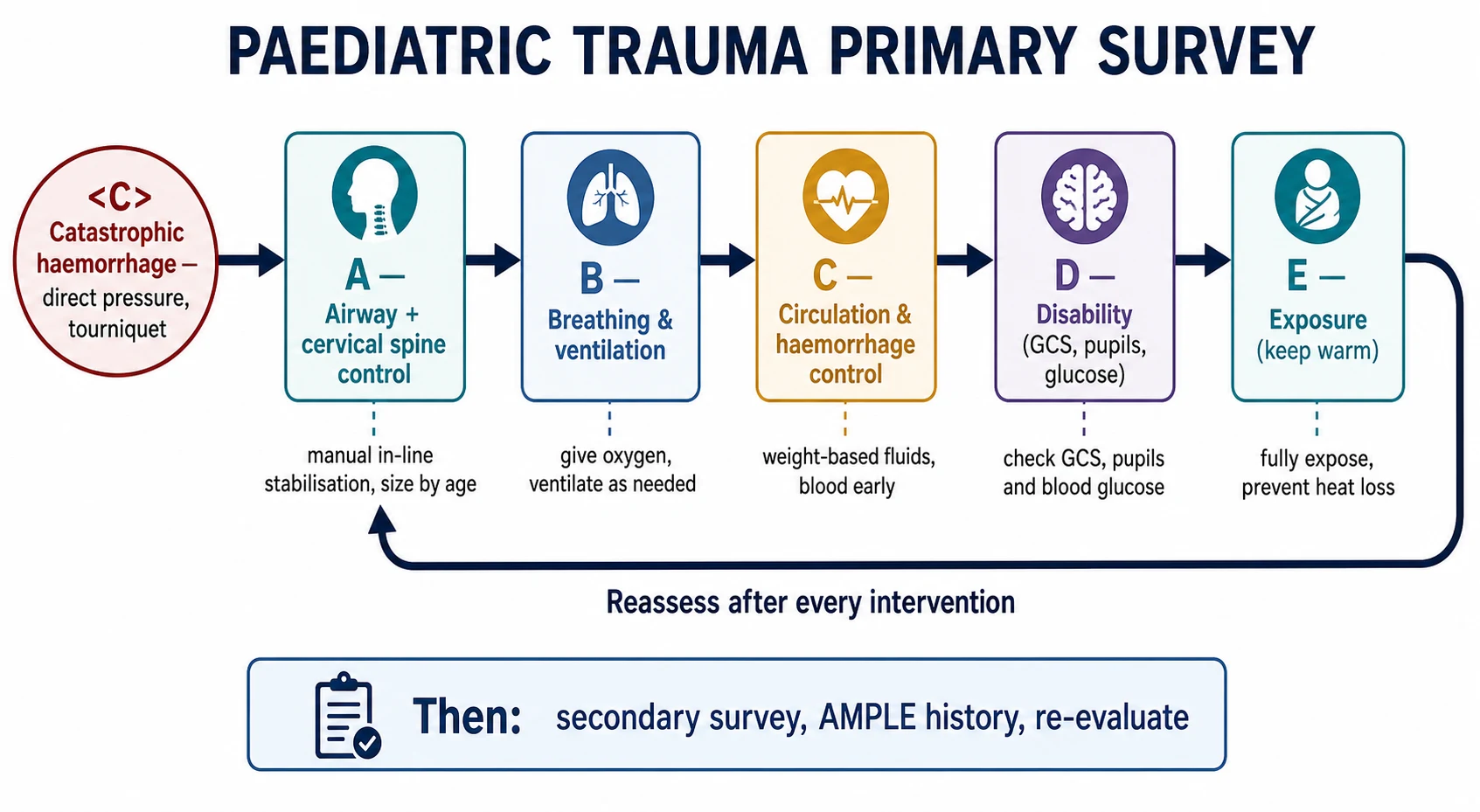
| Step | Question | Find | First action |
|---|---|---|---|
| <C> Catastrophic haemorrhage | Is there exsanguinating external bleeding? | Arterial or junctional bleeding, massive blood loss | Direct pressure, then tourniquet or wound packing; control before airway |
| A — Airway with C-spine | Is the airway open and protected? | Abnormal sound or silence, obstruction, blood, vomit; threatened cervical spine | Manual in-line stabilisation, suction, airway adjuncts; call airway expertise early |
| B — Breathing | Is breathing and ventilation effective? | Rate, effort, air entry, symmetry, tracheal position, oxygen saturation | High-flow oxygen in failure; needle decompression for tension; chest drain for haemo- or pneumothorax |
| C — Circulation | Is perfusion adequate and is bleeding controlled? | Pulse rate and quality, capillary refill, skin colour and temperature, blood pressure, external and internal bleeding | Control loss; weight-based aliquots of balanced crystalloid, move to blood early in haemorrhagic shock |
| D — Disability | Is the brain threatened? | AVPU or paediatric GCS, pupils, posture, seizure, bedside glucose | Protect airway and oxygenation; targeted GCS under 9 means definitive airway and neurosurgery; treat seizure and low glucose |
| E — Exposure | Is there a hidden injury or a temperature threat? | Wounds, bruising pattern, burn, device problem, hypothermia | Expose fully but briefly; warm actively; preserve warmth and dignity; start safeguarding documentation |
Triage and activation criteria classify how sick the child is at system level. A trauma team activation is triggered by physiological, anatomical and mechanistic criteria, and it assembles a team in advance of arrival rather than after the child is found to be unstable. Under-triage misses the seriously injured child; over-triage activates the team too often but errs toward safety. Children are systematically under-triaged because their physiology hides severity, which is why age-adjusted activation criteria and a low threshold matter. [10] [7]
Physiological severity
Bedside, drives actions
- Respiratory distress versus failure
- Compensated versus decompensated shock
- Alert, responsive to voice, pain, or unresponsive
- Hypothermia and base deficit
- Drives immediate resuscitation steps
Anatomical pattern
Injuries, drives referral
- Head, torso, long-bone and pelvic injury
- Burn surface area and airway involvement
- Penetrating versus blunt mechanism
- Combined and multisystem injury
- Drives specialist and operative referral
System capability
Resources, drives destination
- On-site paediatric surgery, orthopaedics and neurosurgery
- Paediatric intensive care and blood bank
- Interventional and CT availability
- Retrieval distance and time
- Drives transfer to a paediatric trauma centre
Epidemiology & Risk Factors
Injury is the leading cause of death and acquired disability in children beyond the first year of life across high-income countries, and the burden in absolute terms is far greater in low- and middle-income settings. Road traffic crashes, falls, drownings, burns and assaults dominate by age and context. The practical point for the resuscitation bay is that mechanism changes the pre-test probability of serious injury and therefore the threshold for activation, imaging and senior involvement. [11] [7]
Children are not small adults in a way that changes both injury pattern and physiology. A disproportionately large head, an elastic chest wall, a shallow and anterior pelvis, and open growth plates produce patterns the examiner must anticipate: more traumatic brain injury, fewer rib fractures despite serious intrathoracic injury, and growth-plate injuries that are easy to miss. The same elasticity that hides injury also hides physiological severity, because tachycardia and vasoconstriction maintain blood pressure until reserve is nearly gone. [11] [8]
Mechanism factors
- High-energy fall, motor-vehicle crash or pedestrian impact
- Ejection, death of another occupant, prolonged extraction
- Penetrating injury to head, neck or torso
- Crush or blast injury
- Burn, submersion or electrical injury
Child factors
- Young age and small body size
- Chronic disease, anticoagulation or technology dependence
- Large head and compliant chest wall
- Open growth plates
- Communication barrier or neurodisability
System factors
- Distance from a paediatric trauma centre
- Limited paediatric surgery, blood bank or intensive care
- Retrieval time and weather
- Language and cultural barriers
- After-hours and single-handed cover
Two epidemiological facts the examiner rewards. First, severely injured children have better survival when treated in a paediatric trauma centre or an adult centre with paediatric capability, which is why triage and transfer matter as much as bedside care. Second, preventable trauma deaths cluster in the hours after arrival and are usually about haemorrhage control, the airway, and escalation that came too late, which is exactly what the primary survey and trauma team are built to prevent. [12] [8]
Pathophysiology
The injured child dies, in order, from airway loss, tension pneumothorax, uncontrolled haemorrhage, and an expanding intracranial lesion. Understanding that order is what justifies the survey. Catastrophic haemorrhage and airway obstruction kill in minutes; a tension pneumothorax kills before a slow intracranial bleed. Each step of the survey protects the next, and treating in the wrong order is a common and fatal error. [6] [8]
Children compensate and then collapse. Tachycardia, vasoconstriction and increased respiratory effort preserve blood pressure and interaction for a time, but they cost reserve and raise oxygen demand. In a bleeding or hypoxic child, a falling or abnormally low heart rate is an ominous sign of decompensation, not calming. Waiting for hypotension to recognise shock is the classic error, because blood pressure is maintained until late. In trauma, hypotension in the bay is an independent predictor of death. [8]
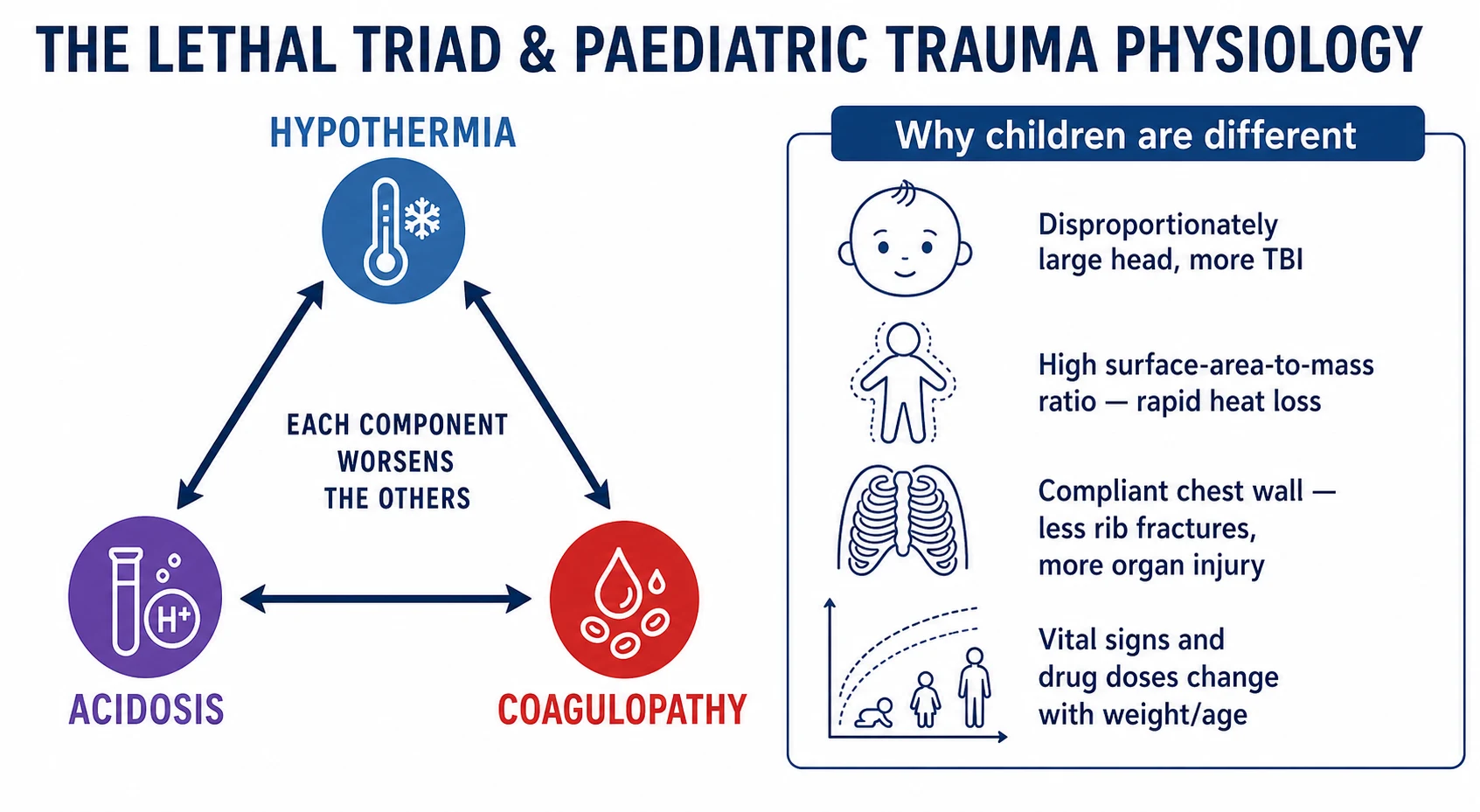
The lethal triad is the central reason damage control resuscitation exists. Massive bleeding produces shock and tissue hypoperfusion, which produces acidosis. Exposure and crystalloid infusion produce hypothermia, and acidosis and hypothermia both disable coagulation factors and platelets, producing traumatic coagulopathy. The triad is self-reinforcing and it kills, so resuscitation is designed to break it: warm the child, minimise crystalloid, give balanced blood products early, and correct acidosis by restoring perfusion. A deranged international normalised ratio or base deficit in an injured child signals that the triad is already established. [5] [3]
Age-specific physiology changes what each step shows. Neonates and infants have a relatively fixed stroke volume and depend on heart rate to maintain cardiac output, so bradycardia in a hypoxic child is pre-arrest. The compliant chest wall may show no rib fractures despite a serious intrathoracic injury, so rely on mechanism and breathing assessment, not the absence of fractures. The large head and weak neck muscles make traumatic brain injury and cervical spine injury more common at the upper cervical level in younger children. Heat loss is rapid because surface area is large relative to mass, so active warming is part of resuscitation, not comfort care. [11] [6]
Clinical Presentation
Begin before you touch the child. From the doorway, note the mechanism from the pre-hospital handover, the child's appearance and interaction, tone and posture, breathing effort and symmetry, colour, and any obvious external bleeding. Describe what you see objectively: a child who is pale, quiet, grunting and mottled after a pedestrian impact tells the team more than a child who is labelled as "stable". [6] [10]
What each step shows in trauma
At <C> and A, look for exsanguinating external haemorrhage at the limbs, neck, axillae and groin, and control it before airway work. Then assess airway patency, abnormal sound or silence, obstruction by blood or vomit, and the need to protect a threatened cervical spine. A child with a possible cervical spine injury is kept in neutral alignment with manual in-line stabilisation, not left in an ill-fitting collar; the large head of a young child may need padding under the torso to avoid neck flexion. Summon airway expertise early. [6] [2]
At B, look for a rate outside the range for age, increased work, reduced or unequal air entry, tracheal deviation, and a credible oxygen saturation. Tension pneumothorax presents with respiratory distress, hypoxia, tracheal deviation away from the affected side, reduced air entry and signs of shock; it is a clinical diagnosis treated by needle decompression followed by a chest drain, not by waiting for imaging. An open or flail chest, a massive haemothorax and pulmonary contusion are each found by the same bedside assessment. [6] [11]
At C, integrate pulse rate and quality, capillary refill, skin colour and temperature, blood pressure, and evidence of external and internal bleeding. Shock in trauma is hypovolaemic until proven otherwise, but remember obstructive causes such as tension pneumothorax and cardiac tamponade. Hypotension is late: a useful paediatric approximation for the lower limit of systolic blood pressure is about 70 mmHg in infants, 70 plus twice the age in years for children aged 1 to 10 years, and about 90 mmHg in older children and adolescents. A blood pressure below this, or a downward trend in a child who still looks unwell, is dangerous. [8] [6]
At D, use AVPU for speed and convert any response below alert, or a persistently concerning child, to a formal paediatric Glasgow Coma Scale. Check pupils for size and symmetry, note posture and movement, time any seizure, and check bedside glucose whenever consciousness is altered. A Glasgow Coma Scale below 9, a worsening score, or a lateralising sign raises intracranial pressure and triggers definitive airway, ventilation to a near-normal carbon dioxide, early imaging and neurosurgical referral. [6] [1]
At E, expose the child fully but briefly to find every wound, the back and the log-rolled spine, then cover and warm immediately. The skin often holds the diagnosis and the safeguarding evidence: patterned bruising, a bite mark, a seat-belt sign, a burn in an unusual distribution, or an injury inconsistent with the stated mechanism. Hypothermia is a threat to be prevented, not an afterthought. [6] [11]
| Life stage | High-value change from usual | Adaptation in the survey |
|---|---|---|
| Neonate or infant | Non-specific change, poor feeding, apnoea; large head and weak neck | Check glucose early; pad under torso to avoid neck flexion; lower threshold for activation |
| Toddler and preschool | Loss of play or speech; fall or non-accidental injury possible | Examine with caregiver; consider safeguarding with inconsistent history or patterned injury |
| School-age child | Pedestrian or cycle injury; hidden abdominal and spinal injury | Take the history from the child; apply PECARN rules for imaging decisions |
| Adolescent | High-energy mechanism, risk-taking, substance use, self-harm | Create private time; screen for substances and mental-health risk; explain confidentiality limits |
Differential Diagnosis
Build the trauma differential in a fixed order: what can kill now, what is most likely, what is reversible, and what is most harmful to miss. The primary survey names the failing system, not the disease; the named diagnosis emerges as the secondary survey and imaging clarify the picture. Keep the dangerous causes open until focused assessment settles them. [6] [8]
| System | Immediately reversible life threat | First action |
|---|---|---|
| Airway | Airway obstruction, blood or vomit; cervical spine injury | Position, suction, adjuncts, manual in-line stabilisation; definitive airway if threatened |
| Breathing | Tension pneumothorax, massive haemothorax, flail chest | Needle decompression then chest drain for tension; oxygen; assist ventilation |
| Circulation | Exsanguinating haemorrhage, hypovolaemic shock, tamponade | Direct pressure or tourniquet, balanced blood products, pericardiocentesis for tamponade |
| Disability | Hypoglycaemia, expanding intracranial haematoma, seizure | Correct glucose; definitive airway and neurosurgery for raised pressure; treat seizure |
| Exposure | Hypothermia, hidden burn or wound, safeguarding concern | Warm actively; document objectively; run safeguarding in parallel |
Keep mimics and modifiers in mind. Breath-holding, syncope, a seizure at the moment of a minor fall, and pain can produce abnormal physiology that is not itself the injury, but they must not close the survey prematurely. Equally, a dangerous mechanism with initially normal physiology can still hide a serious injury, so mechanism keeps the threshold for imaging and observation low. The injury you cannot yet see is the one that hurts the child later, which is why a normal first survey is followed by a careful secondary survey and a period of observation for the high-risk child. [6] [11]
Safeguarding stays open while you resuscitate. An inconsistent history, a delay in presentation, a patterned injury, or any bruising in a non-mobile infant raises non-accidental injury, which coexists with accidental trauma more often than is comfortable. Stabilise and preserve the child's safety first, document objectively and photograph where appropriate, ask only necessary non-leading questions, and activate the local safeguarding pathway in parallel. Reporting thresholds and agencies differ by jurisdiction. [6] [11]
Clinical & Bedside Assessment
The primary survey is the hands-on assessment, and it runs to the same contract as the seriously ill child, adapted for trauma. State what you will assess at each letter, treat the threat you find, declare the change you expect, and reassess from the top. Closed-loop communication, a named leader, and pre-assigned roles turn the survey into team resuscitation. [6] [10]
Take a focused AMPLE history in parallel without delaying stabilisation: allergies, medications (especially anticoagulants), past medical history, last meal, and the events and mechanism of injury. Mechanism from the pre-hospital team, the time of injury, the estimated blood loss at the scene, and any interventions already given shape the differential and the threshold for activation. Caregiver concern that the child is different from usual is information, not anxiety. [6] [11]
Examination technique is adapted for trauma and for age. Keep the cervical spine protected throughout, use manual in-line stabilisation for any airway manoeuvre in the at-risk child, and log-roll as a team to examine the back. Use age-appropriate equipment sized by length or weight, and confirm the working weight early because every drug and device in trauma is weight-based. Examine the least distressing areas first in a frightened young child, and involve the caregiver where it helps. [6] [7]
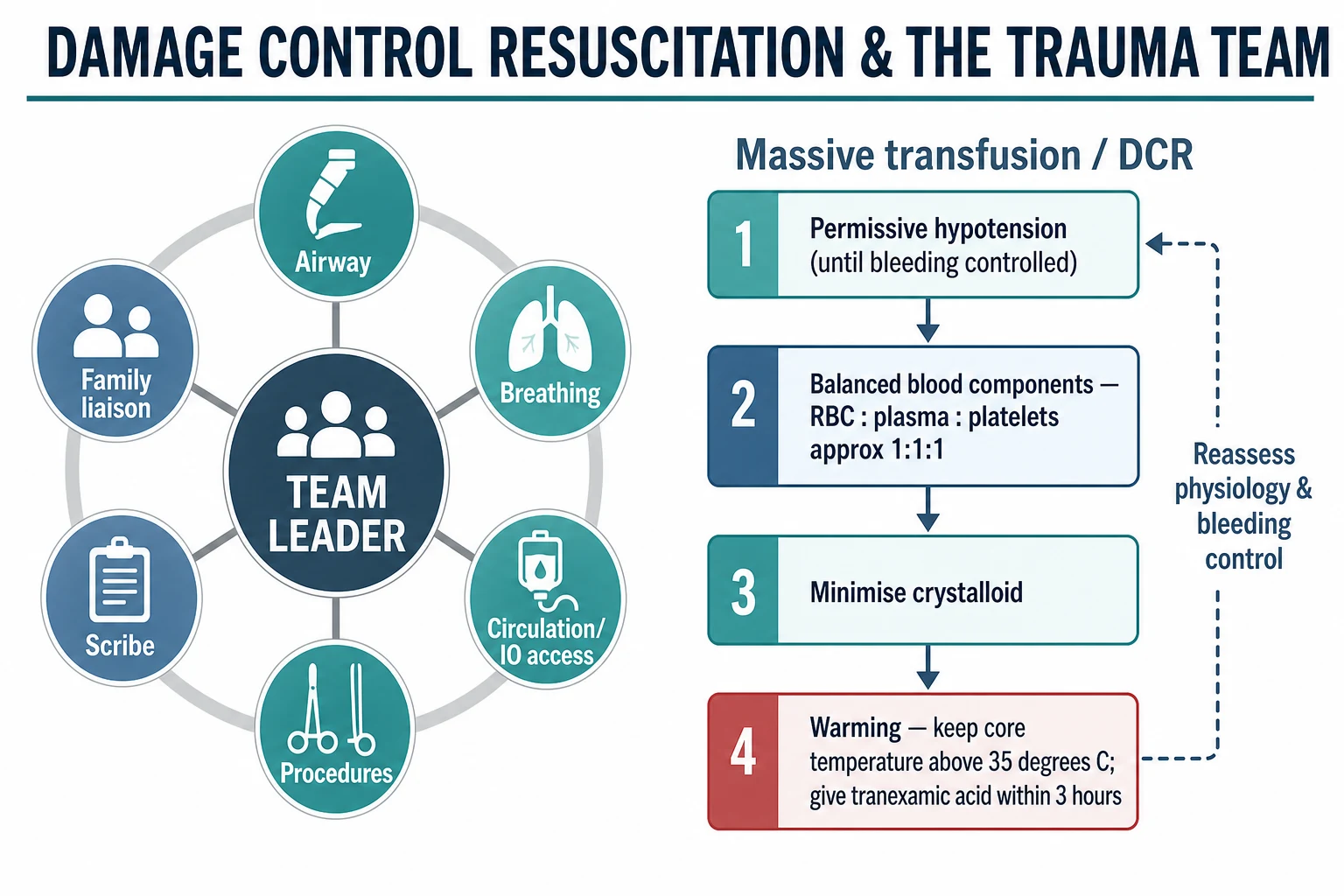
| Role | Primary responsibility |
|---|---|
| Team leader | Stands back, runs the survey, allocates tasks, makes decisions, owns the plan and the escalation |
| Airway doctor | Manages airway and cervical spine, prepares for definitive airway when needed |
| Circulation or access clinician | Controls haemorrhage, gains intravenous or intraosseous access, runs fluids and blood products |
| Procedures clinician | Performs decompression, chest drain, splintage and pelvic binding as tasked |
| Scribe | Documents timed physiology, actions, response and pending tasks; calls out deterioration |
| Bedside and family nurse | Monitors, prepares equipment, and supports and updates the family |
The structured synthesis after each pass transfers the whole picture forward. A good one-line summary names identity and working weight, the mechanism, the current physiological state, the controlled and uncontrolled threats, the actions taken and the response, the prioritised differential, and the next contingency with a named owner. This synthesis is what the retrieval team and the trauma centre need to receive, and it is the skeleton of the formal handover. [6] [11]
Investigations
Name the question before you order any test, because every investigation can delay stabilisation or move an unstable child into an unsafe place. In the primary survey the immediate investigations are bedside: oxygen saturation, a credible blood pressure and pulse, a point-of-care glucose, and an ECG when indicated. A venous gas with lactate and base deficit, a full blood count, coagulation including the international normalised ratio, and a blood group and crossmatch are drawn at the first access, because they answer the questions of perfusion, coagulopathy and transfusion readiness. [5] [8]
A rising or already deranged international normalised ratio and a worsening base deficit are not reassurance; they are evidence that the lethal triad is established, that transfusion is needed, and that control of haemorrhage is incomplete. An early lactate that fails to clear predicts ongoing bleeding and worse outcome. Read these as physiology and trend, not as single reassuring numbers. [3] [8]
Imaging is conditional on the child being stable enough to move. A focused assessment with sonography in trauma, within operator competence, answers whether there is free fluid in the abdomen or pericardial effusion in an unstable child, and it can guide the decision to operate rather than scan. Plain films of the chest and pelvis are quick and answer life-threatening thoracic and pelvic injury at the bedside. Computed tomography is the definitive modality for the stable child with significant mechanism, but it requires a safe transfer plan, monitoring and escort; an unstable child belongs in theatre or being resuscitated, not in a scanner. [6] [11]
Apply paediatric imaging decision rules to avoid over-investigation and radiation. The PECARN head-injury rule identifies children at very low risk of clinically important brain injury who can avoid computed tomography, and the PECARN cervical spine rule identifies children at low risk of cervical spine injury who can avoid imaging after blunt trauma. Using these rules in the appropriate, low-risk child reduces unnecessary scans without missing serious injury, and stating the rule you are applying is a viva-grade answer. [1] [2]
Management — Resuscitation
Run the resuscitation as a team. Confirm a named leader, closed-loop communication, continuous monitoring, and age- and weight-appropriate equipment and warming. Control catastrophic haemorrhage first with direct pressure and, for exsanguinating limb bleeding, a tourniquet; junctional bleeding may need wound packing. Then protect the airway and cervical spine, support breathing, restore the circulation, protect the brain, and warm and expose the child, treating each threat as found. [6] [5]
For the airway, maintain manual in-line stabilisation during any airway manoeuvre in the at-risk child. If the airway is threatened or protected poorly, move to a definitive airway with a rapid-sequence technique sized to age and weight, and prepare for the difficult paediatric airway. Do not attempt repeated traumatic intubations without the right support; summon airway expertise early. At breathing, give high-flow oxygen in failure, decompress a tension pneumothorax and place a chest drain for a haemo- or pneumothorax, and assist ventilation when breathing is ineffective. [6] [11]
For circulation, decide shock is present, decide the likely type, state the expected response, and treat the source. In haemorrhagic shock the priority is to stop the bleeding and give blood early rather than to chase a fixed crystalloid volume. Give balanced crystalloid in weight-based aliquots of 10 to 20 mL per kilogram, reassessing after each, and minimise the total crystalloid because it worsens coagulopathy and hypothermia. Move to balanced blood products early in confirmed or suspected major haemorrhage. [5] [8]
TIC-TOC (pilot)
Academic Emergency Medicine
Pilot randomised trial of tranexamic acid versus placebo in children with traumatic injury and intracranial haemorrhage or solid organ injury.
Key finding
The pilot established feasibility and safety of a paediatric tranexamic acid trial; it was not powered for a definitive efficacy outcome.
Practice change
Tranexamic acid remains a reasonable antifibrinolytic option in paediatric major haemorrhage when given early (within 3 hours of injury); the definitive efficacy trial is ongoing.
For massive transfusion and damage control, transfuse balanced blood components aiming for a ratio of red cells to plasma to platelets of approximately 1 to 1 to 1, give tranexamic acid early when major haemorrhage is present, and keep the child warm with a core temperature above 35 degrees Celsius. Permissive hypotension is accepted in the bleeding adult and older child until haemorrhage is controlled, but it is used cautiously in children and not at all when there is an associated traumatic brain injury, because the injured brain needs perfusion. Reassess coagulation, haemoglobin, calcium and acid-base throughout. [4] [5]
For disability, protect the airway and oxygenation first, treat any seizure, correct a dangerous low glucose immediately, and target a Glasgow Coma Scale and pupillary response that show a perfused and oxygenated brain. A Glasgow Coma Scale below 9, a falling score, or a lateralising sign triggers a definitive airway, ventilation to a near-normal carbon dioxide, urgent imaging and neurosurgical referral. For exposure, keep the child warm and covered, complete the log-roll, and run safeguarding documentation in parallel. [6] [1]
Management — Definitive & Stepwise
Once the child is stable, move to the secondary survey: a head-to-toe examination, the AMPLE history, re-evaluation of every limb and the spine, and the application of imaging decision rules. Reassess from the top after every significant intervention, because stability is a state that can be lost. Definitive management is by injury pattern: operative or interventional control of haemorrhage, neurosurgery for an expanding intracranial lesion, orthopaedic and pelvic stabilisation, and the management of burns and internal injuries in their dedicated pathways. [6] [11]
Analgesia is part of definitive care, not an afterthought. Inadequate analgesia is harmful and common, and it does not improve diagnostic accuracy. Use weight-based titrated analgesia, commonly an opioid such as intranasal fentanyl or intravenous morphine, alongside non-pharmacological measures and splintage, and document the response. Procedural sedation, where used, follows its dedicated paediatric pathway with monitoring and trained staff. [6] [11]
Decide the destination and the monitoring intensity from the trend and the capability gap, not from one observation. Specify the level of care the child needs, whether that is theatre, paediatric intensive care, a high-dependency or ward bed with close observation, or a safe discharge with a structured safety net. Run early retrieval and paediatric trauma centre consultation in parallel with resuscitation, not after local options are exhausted, and package the escort, monitoring and contingency for transfer. [12] [7]
A defensible disposition requires sustained stability, resolved or controlled threats, an executed imaging and surgical plan, a structured handover, and a safety net the family can use. Confirm caregiver understanding with teach-back, document the warning signs, the urgency and the access route, and name who owns pending results. After a critical event, debrief the child and family, invite questions, and offer team debriefing. [6] [11]
Specific Subtypes & Scenarios
The injured neonate or infant has little physiological reserve and may present non-specifically; check glucose early, keep them warm, pad under the torso if the cervical spine is at risk, and lower the threshold for activation. The child with a threatened cervical spine is kept in manual in-line stabilisation, assessed with the PECARN cervical spine rule where appropriate, and cleared clinically only when criteria are met; collar-related pressure injury is avoided by proportionate, well-fitted immobilisation and early clearance. [2] [11]
The bleeding child in haemorrhagic shock is managed with damage control resuscitation: early balanced blood products, minimised crystalloid, tranexamic acid within 3 hours, active warming, and surgical or interventional control of the source. A child with a severe traumatic brain injury needs a definitive airway, oxygenation and near-normal carbon dioxide, early imaging and neurosurgery, and avoidance of hypotension, because the injured brain is exquisitely sensitive to secondary injury from hypoxia and hypoperfusion. [5] [1]
The child with suspected non-accidental injury is resuscitated and stabilised first, with safeguarding documentation, non-leading questions and the local pathway running in parallel; the physical findings are recorded objectively, photographed where appropriate, and the child is protected while care proceeds. The technology-dependent child is assessed with their personal baseline and device in mind, using their emergency plan where one exists. [6] [11]
In a rural or remote setting, activate the trauma system and call retrieval at the first indication that injury severity may exceed local capability, in parallel with resuscitation. State the current problem, the resources available, the expected response, the destination, the contingency for deterioration and for transfer delay, and the handover. Do not wait until local options have failed; transport time is a clinical variable that you manage, not discover. [7] [12]
The multisystem or polytrauma child is prioritised by the threat to life: haemorrhage and airway first, brain next, then limbs and the reconstructive plan. A mass-casualty or disaster context applies triage principles that prioritise the most salvageable, and it may force difficult allocation decisions that should follow the local protocol and senior command. [11] [6]
Complications & Pitfalls
Most preventable harm comes from acting in the wrong order or stopping too early. Treating an airway before controlling exsanguinating haemorrhage, scanning an unstable child, accepting a normal blood pressure as proof there is no shock, or declaring the child stable without a secondary survey are all classic errors. Prevent them by stating the failing system, the expected response, the actual response and the next escalation at every step. [6] [8]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Airway before catastrophic haemorrhage | The child exsanguinates during airway work | Control external bleeding with pressure or tourniquet first |
| Waiting for hypotension to diagnose shock | Hypotension is late and predicts death | Integrate heart rate, refill, skin and trend; treat early |
| Large crystalloid volumes | Worsens coagulopathy and hypothermia | Minimise crystalloid; move to blood early; reassess after each aliquot |
| Scanning an unstable child | Deterioration in an unmonitored scanner | Resuscitate and operate; scan only when transfer is safe |
| Adult equipment, doses or collar sizing | Age and weight ignored | Use length- or weight-based sizing and the paediatric cognitive aid |
| Under-triage of children | Severity hidden by compensation | Use age-adjusted activation criteria and a low threshold |
| Late retrieval call | Preventable death after delay | Activate retrieval in parallel with resuscitation |
| Safeguarding deferred for diagnosis | Safety and evidence lost | Stabilise first; document and run the pathway in parallel |
| Inadequate analgesia | Harm and distress without diagnostic benefit | Give titrated weight-based analgesia and reassess |
Watch for the lethal triad once it is established, because it is harder to reverse than to prevent. Hypothermia, acidosis and coagulopathy predict death in massive haemorrhage, so warming, early blood, and minimised crystalloid are preventive, not reactive. After stabilisation, look actively for treatment-related harm: airway or access complications, transfusion reaction, missed injury, pressure injury from immobilisation, and the psychological impact on the child and family. [5] [3]
[6] [8]Prognosis & Disposition
Outcome is determined by the severity and duration of physiological insult, the speed of haemorrhage control, the presence and severity of traumatic brain injury, the avoidance of secondary injury, and the capability and timeliness of definitive care. Children have greater physiological reserve than adults but can decompensate steeply, so a good outcome depends on early recognition and a system that delivers the right care in time, not on heroics at the bedside. [8] [12]
Theatre or critical care
- Uncontrolled or ongoing haemorrhage
- Severe traumatic brain injury needing neurosurgery
- Respiratory or circulatory failure requiring organ support
- Need for expertise or monitoring unavailable locally
High-dependency or ward
- Controlled physiology but significant mechanism or injury
- Pending imaging, surgical or specialist opinion
- Observation needed for evolving injury
- Named escalation pathway in place
Discharge only when defensible
- Low-risk mechanism and normal physiology sustained
- Imaging rules applied and no high-risk injury
- Adequate analgesia and a usable safety net
- Carer understanding confirmed and follow-up agreed
An executable safety net states what change to watch for, how urgently to act, and exactly where to get help. It states when review will occur, who owns pending results, and what to do if access is difficult. A recurrent or unexplained presentation needs senior review and reconsideration of safeguarding. After a critical event, explain to the family what happened and what remains uncertain, invite questions, and offer debriefing for the child, family and team. [6] [11]
Special Populations
Adapt how you observe and communicate, but never lower the standard for recognising deterioration. The neonate and infant is treated with a low threshold for activation, early glucose, active warming and Newborn Life Support at birth where relevant. The technology-dependent child is assessed against their personal baseline and device, using their emergency plan. The child with severe neurodisability is assessed against their usual interaction, tone and pain expression, and caregiver-described change is treated as evidence. [6] [11]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Neonate or infant | Low activation threshold, early glucose, warm, pad under torso for C-spine | Use Newborn Life Support at birth; do not apply an older-child pathway uncritically |
| Technology-dependent child | Personal baseline, device and emergency plan assessed in parallel | A chronically abnormal observation is not automatically safe; compare with baseline |
| Severe neurodisability | Use usual interaction, tone and pain expression; treat carer-described change | Adaptation improves communication, not proven diagnostic sensitivity |
| Adolescent | Private time; ask about substances, self-harm and consent; explain confidentiality limits | Confidentiality has safety limits; safeguarding duties still apply |
| Indigenous, migrant or remote family | Cultural safety and a professional interpreter; address access and transport barriers | Retrieval and safeguarding routes remain jurisdiction-specific |
Safeguarding runs in parallel with trauma care, but immediate stabilisation and safety come first. Ask only necessary open, non-leading questions. Explain confidentiality and information sharing, document objective findings and spontaneous words, preserve evidence when safe, and use the local safeguarding pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [6] [11]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The primary survey structure is consensus and is taught consistently by Advanced Trauma Life Support and its regional equivalents, which run catastrophic haemorrhage control first and then airway with cervical spine control, breathing, circulation, disability and exposure, with reassessment after every intervention. The order of the letters is not in dispute; the doses, ratios, transfusion targets and imaging rules attached to each step are source- and population-specific. [6] [11]
PECARN head-injury rule
Lancet
Large prospective cohort of children with minor head injury, deriving prediction rules for clinically important brain injury.
Key finding
Identifies a substantial group of children at very low risk of clinically important brain injury in whom computed tomography can be safely avoided.
Practice change
Widely adopted to reduce unnecessary cranial computed tomography in low-risk children without missing serious injury.
Damage control resuscitation in children, including balanced transfusion ratios and minimised crystalloid, is supported by observational and registry evidence and by expert consensus, because definitive paediatric randomised trials are difficult to run. The ATOMAC group has shaped paediatric massive transfusion practice, and the TIC-TOC pilot established the feasibility of a paediatric tranexamic acid trial without delivering a definitive efficacy result. Read the strength of each recommendation in this light: strong on structure and early blood, weaker on exact ratios and drug doses. [4] [9]
The BIG score, which combines base deficit, international normalised ratio and Glasgow Coma Scale, predicts mortality in paediatric blunt trauma and is a useful research and triage tool; it does not replace bedside judgement. Paediatric trauma centre care is associated with better survival for severely injured children than care in non-specialised centres, which is why triage and early transfer matter. State the strength and the population of each rule you quote. [3] [12]
Jurisdictional implementation
Australia and Aotearoa New Zealand: trauma is managed through state and territory trauma systems with designated paediatric major trauma centres. The Royal Children's Hospital Melbourne major-trauma guideline and the Royal Australasian College of Surgeons Early Management of Severe Trauma course support local practice. Retrieval is coordinated through state services, and mandatory reporting and consent remain jurisdiction-specific.
Global and low-resource settings: the principles of <C>ABCDE, haemorrhage control, and damage control resuscitation are globally applicable, but the system around them varies. Adapt activation, imaging, blood-bank and retrieval expectations to local resources, and do not transplant protocols uncritically across populations and capabilities.
Exam Pearls
System and team
- Injury is the leading cause of death beyond infancy
- Pre-hospital triage, trauma team, retrieval network
- Named leader, closed-loop communication, defined roles
- Low threshold to activate in children
Primary survey
- <C>ABCDE: control catastrophic haemorrhage first
- Airway with cervical spine control; treat as found
- Reassess from the top after every intervention
Resuscitation facts
- Minimise crystalloid; give balanced blood early
- Balanced components at a ratio near 1:1:1
- Tranexamic acid within 3 hours of injury
- Keep core temperature above 35 degrees Celsius
- Lower-limit systolic BP roughly 70 plus twice age in years
Brain and imaging
- GCS under 9 means definitive airway and neurosurgery
- Protect the brain: avoid hypoxia and hypotension
- Apply PECARN head and cervical spine rules in the low-risk child
Escalation
- Paediatric trauma centre care improves survival for severe injury
- Call retrieval in parallel with resuscitation
- Structured handover and a usable safety net
Pitfalls
- No airway before haemorrhage control
- No waiting for hypotension
- No scanning of an unstable child
- No adult doses or collar sizing
- Safeguarding runs in parallel
“Activate the system and the team → <C>ABCDE treating each threat as found → stop the bleeding and break the triad → protect the brain → apply imaging rules → escalate to a paediatric trauma centre before local support is exceeded → reassess and hand over.”
Viva: the stable-looking child after a high-energy mechanism
Describe the child objectively, then state that mechanism keeps the threshold low despite normal physiology. Run the primary survey in order, control any external bleeding, protect the airway and cervical spine, confirm a credible blood pressure and perfusion trend, check glucose, and warm the child. Complete the secondary survey, apply PECARN imaging rules where appropriate, observe for the evolving injury, and keep a low threshold to escalate.
Viva: when does the bleeding child get blood instead of crystalloid?
Early. I give balanced crystalloid in weight-based aliquots of 10 to 20 mL per kilogram, reassessing after each, but I minimise the total crystalloid because it worsens coagulopathy and hypothermia. In confirmed or suspected major haemorrhage I move to balanced blood products at a ratio near 1 to 1 to 1, give tranexamic acid within 3 hours, actively warm the child, and arrange surgical or interventional control of the source. I reassess haemoglobin, coagulation, calcium and acid-base throughout. [5] [4]
Structured oral: rural retrieval of a polytrauma child
I activate the trauma system and call retrieval in parallel with resuscitation, before local support is exceeded. I state the current problem, the controlled and uncontrolled threats, the resources available, the expected response, the destination, the contingency for deterioration and for transfer delay, and the structured handover. I package the escort, monitoring and blood plan for transfer, keep the family informed, and document objectively.
References
- [1]Kuppermann, Nathan Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study Lancet (London, England), 2009.PMID 19758692
- [2]Leonard, Julie C PECARN prediction rule for cervical spine imaging of children presenting to the emergency department with blunt trauma: a multicentre prospective observational study The Lancet Child and Adolescent Health, 2024.PMID 38843852
- [3]Davis, Anna L The BIG Score and Prediction of Mortality in Pediatric Blunt Trauma The Journal of pediatrics, 2015.PMID 26118931
- [4]Noland, Daniel K Massive transfusion in pediatric trauma: An ATOMAC perspective Journal of pediatric surgery, 2019.PMID 30389149
- [5]Russell, Russell T Damage-control resuscitation in pediatric trauma: What you need to know The journal of trauma and acute care surgery, 2023.PMID 37314396
- [6]Galvagno, Samuel M Jr Advanced Trauma Life Support Update 2019: Management and Applications for Adults and Special Populations Anesthesiology clinics, 2019.PMID 30711226
- [7]Mora, Molly C Pediatric trauma triage: A Pediatric Trauma Society Research Committee systematic review The journal of trauma and acute care surgery, 2020.PMID 32301877
- [8]Leeper, Christine M Too little too late: Hypotension and blood transfusion in the trauma bay are independent predictors of death in injured children The journal of trauma and acute care surgery, 2018.PMID 29389838
- [9]Nishijima, Daniel K Traumatic injury clinical trial evaluating tranexamic acid in children (TIC-TOC): A pilot randomized trial Academic emergency medicine : official journal of the Society for Academic Emergency Medicine, 2022.PMID 35266589
- [10]Herren, Andri Pediatric Trauma and Trauma Team Activation in a Swiss Pediatric Emergency Department: An Observational Cohort Study Children (Basel), 2023.PMID 37628376
- [11]Ciorba, Madalina C Polytrauma in Children—Epidemiology, Acute Diagnostic Evaluation, and Treatment Deutsches Arzteblatt international, 2024.PMID 38471125
- [12]Russell, Kathryn Pediatric trauma center vs. adult trauma center: which is better? Current opinion in anaesthesiology, 2023.PMID 36745064