Paeds · acute-care-resuscitation-and-toxicology
Mechanical ventilation principles in children
Also known as Paediatric mechanical ventilation · Invasive ventilation in children · Paediatric lung-protective ventilation · PICU ventilation principles · Ventilator modes in children
Fellowship guide to mechanical ventilation principles in children: why a child is intubated, how the ventilator delivers a breath, how the modes differ in what they control and what they let the patient do, and the lung-protective strategy that sets low tidal volume, limited plateau pressure, optimised PEEP and permissive hypercapnia that now governs the paralysed diseased lung. Covers the settings a candidate must be able to justify, the weaning and liberation approach including spontaneous breathing trials and post-extubation non-invasive support, sedation and the difficulty of translating adult liberation protocols to children, ventilator-associated pneumonia prevention, and the way every choice is judged against the type of respiratory failure in front of you.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Mechanical ventilation in children is the delivery of positive-pressure breaths through an invasive artificial airway, almost always an endotracheal tube, in order to take over or assist the work of breathing when the child's own gas exchange or respiratory effort has failed. The decision to intubate is therefore a decision that oxygenation, ventilation, or the effort of breathing has become unsafe, and ventilation is bought at a price, because the very act of pushing gas into diseased lung can injure it. The organising principle of modern paediatric practice is lung-protective ventilation, which deliberately limits how much each breath stretches the lung so that the ventilator supports recovery rather than adding harm. [3] [1]
The topic rewards a candidate who holds three things in mind at once. The first is the indication, because ventilation is started for apnoea or exhausted effort, for refractory hypoxaemia, for failure to clear carbon dioxide, or to protect the airway and reduce work of breathing in shock. The second is the mode, which is simply the rule the ventilator follows to deliver each breath: what it controls, what the patient is allowed to trigger, and how hard it works. The third is the protective target, the low tidal volume and limited pressure that translate the insight that overdistending an injured lung makes it worse into numbers set on the machine. [3] [2]
Classification
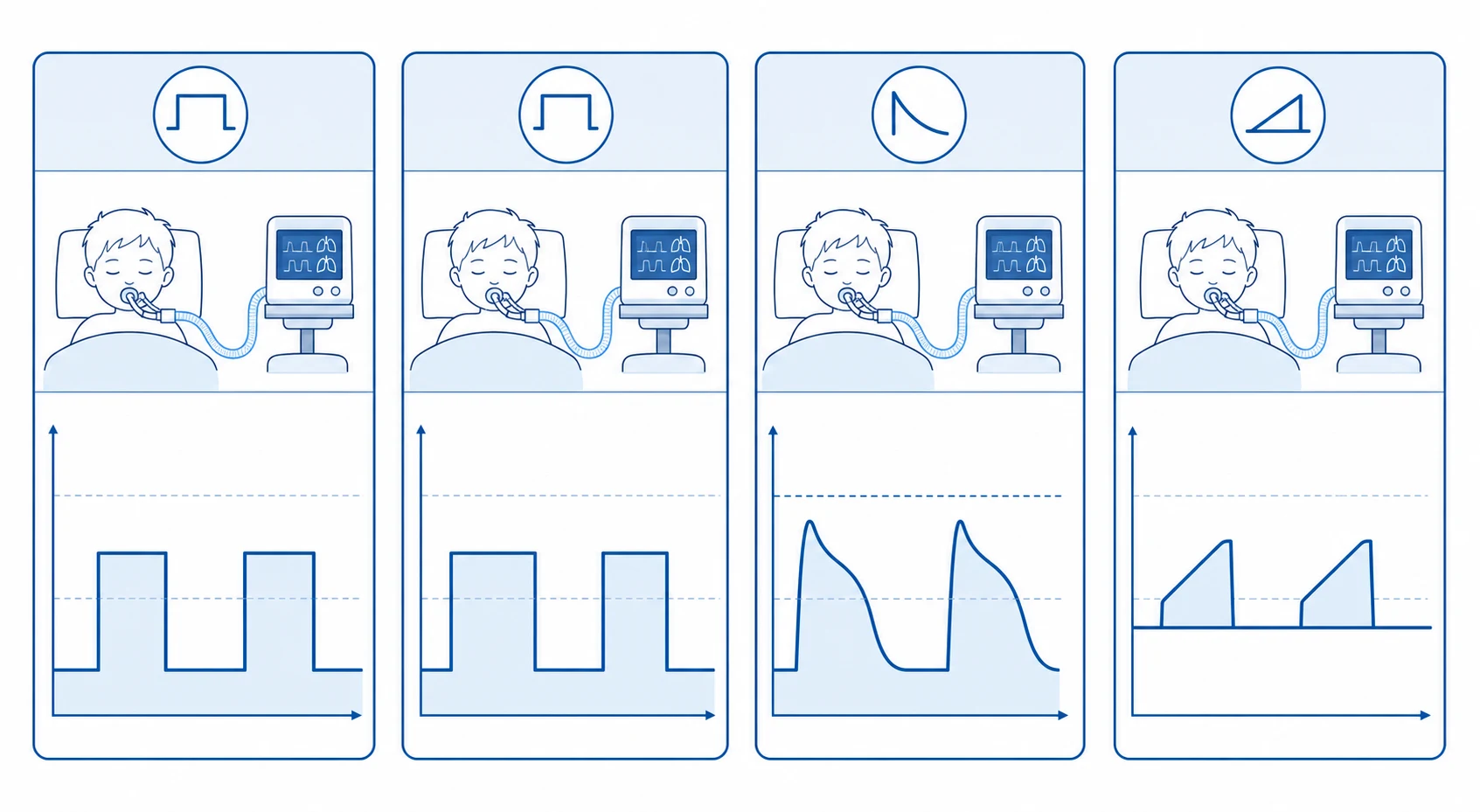
Ventilator modes are best understood by what each breath controls and how much the patient participates, rather than by memorising trade names. A volume-controlled breath guarantees a set tidal volume and lets the pressure rise as far as the lung and tube resistance dictate, which is useful when you want a reliable delivered volume but demands close attention to the pressure that results. A pressure-controlled breath instead fixes the inspiratory pressure and lets the volume vary with how compliant the lung is at that moment, giving a decelerating flow pattern that many clinicians favour for diseased lung. The hybrid mode, pressure-regulated volume control, holds a volume target while varying the pressure breath to breath, attempting to deliver a consistent tidal volume at the lowest necessary pressure. [10] [3]
The second axis is how much the patient drives the breath. Continuous mandatory ventilation delivers every breath, machine-triggered or patient-triggered, at the full set pressure or volume. Synchronised intermittent mandatory ventilation delivers a set number of full machine breaths synchronised to the patient's own efforts, while allowing the child to breathe spontaneously between them. Pressure support is the weaning mode: each spontaneous effort is augmented by a set amount of pressure so the patient does the work of triggering but the ventilator reduces the load. Modern ventilators often blend these into dual modes, but the examiner wants the candidate to state plainly what is controlled, what is supported, and what the patient must do. [10]
Epidemiology & Risk Factors
Mechanical ventilation is among the most common invasive therapies delivered in a paediatric intensive care unit, used in a substantial minority of all admissions and most often for acute respiratory failure, perioperative support, neurological compromise and shock. The international PARDIE study quantified paediatric acute respiratory distress syndrome, the archetype of the diseased lung that needs protective ventilation, and found it more common than previously assumed, with mortality that remains significant and that concentrates in the most severe and hypoxaemic children. [6]
The children who need ventilation, and who are most vulnerable to its complications, are a recognisable population. Infants and young children dominate because their airways are small, their respiratory reserve is limited, and their chest wall is compliant so they fatigue quickly. Under this sits the burden of specific diseases: viral bronchiolitis and pneumonia, asthma, sepsis and shock, aspiration and near-drowning, congenital heart disease after surgery, and the neuromuscular and chronically ventilated child who returns with intercurrent illness. Prematurity, immunocompromise, chronic lung disease and airway malacia all raise both the chance of needing ventilation and the chance of a complicated course. [6] [3]
Pathophysiology
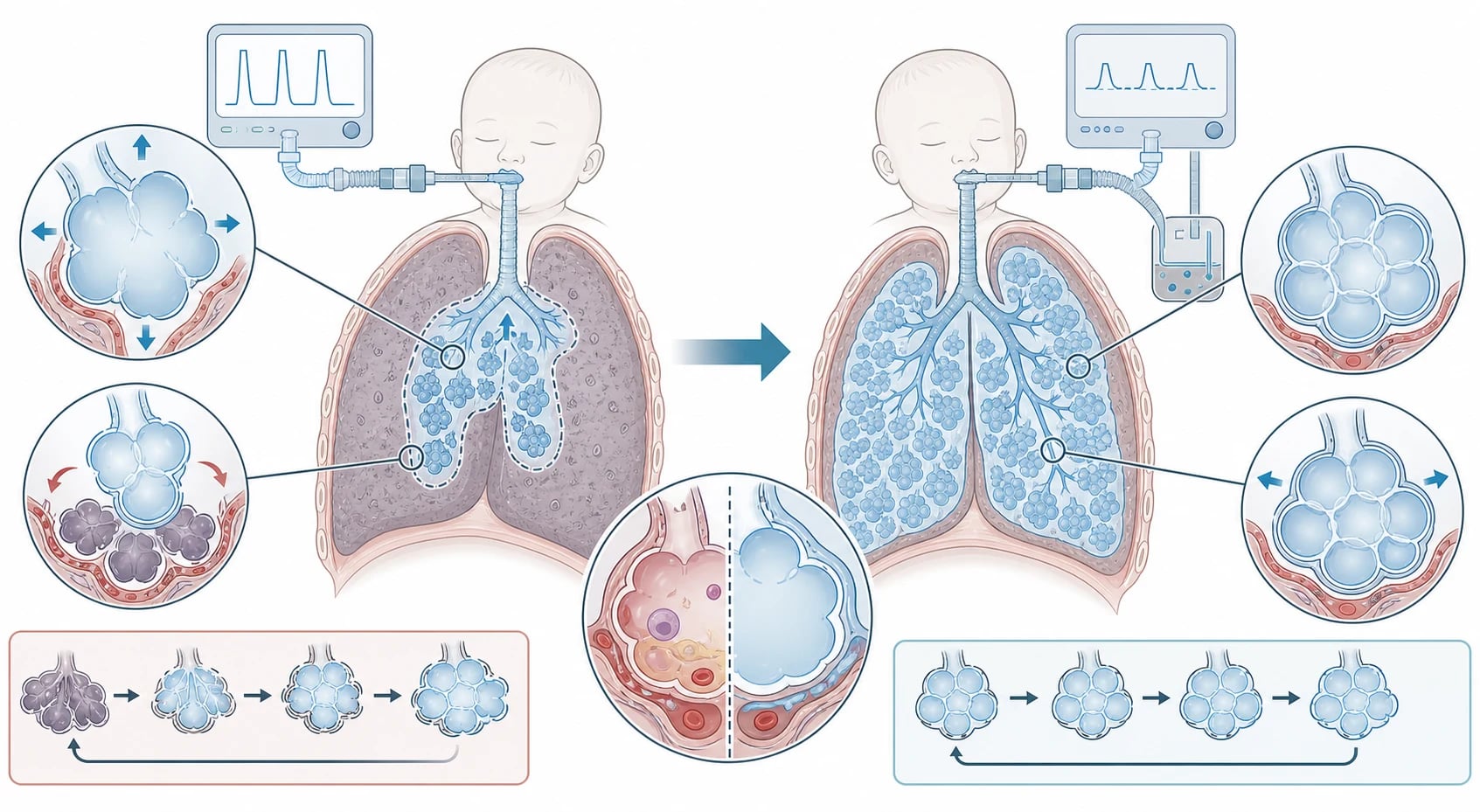
The reason a diseased lung needs protection is that the lung in acute respiratory distress is not uniformly injured. The aerated portion, the so-called baby lung, is small and easily overdistended, while dependent regions are collapsed and recruit poorly. Pushing a conventional tidal volume into this small aerated baby lung stretches it with every breath, and the injury that results, ventilator-induced lung injury, has several mechanisms that a candidate should be able to name. Volutrauma is injury from excessive tidal volume overstretching alveoli; barotrauma, now understood as pressure-mediated harm, is closely linked; atelectrauma is the repeated shear stress of alveoli opening and collapsing at low end-expiratory pressure; and biotrauma is the systemic inflammatory release triggered by mechanical injury that can drive multi-organ dysfunction. [1] [2]
Lung-protective ventilation is the physiological answer to each of these mechanisms. A low tidal volume, set against predicted body weight rather than actual weight, limits volutrauma by reducing how far each breath stretches the baby lung. Positive end-expiratory pressure holds alveoli open at end-expiration, raising functional residual capacity, improving oxygenation and preventing the cyclic collapse that causes atelectrauma. Limiting the inspiratory plateau pressure caps the transpulmonary stress delivered each breath, and accepting a mildly elevated carbon dioxide, so long as the pH is preserved, allows smaller tidal volumes and lower pressures than would otherwise be needed. The practical target set by the second Pediatric Acute Lung Injury Consensus Conference is a tidal volume around 6 to 8 millilitres per kilogram of predicted body weight, lower, toward 4 to 6, in severe disease, a plateau pressure at or below 28 centimetres of water, and a driving pressure, the gap between plateau and positive end-expiratory pressure, at or below 15. [2] [5]
Clinical Presentation
The child who needs mechanical ventilation arrives in one of several ways, and recognising the trajectory is the first clinical skill. Some present as apnoea or a depressed conscious state that has abolished airway protection or respiratory drive, common in the infant with bronchiolitis, the seizing child, or the child with raised intracranial pressure. Others present as exhaustion, with tachypnoea giving way to bradypnoea, accessory-muscle use, paradoxical breathing, fatigue and a rising carbon dioxide that signals the muscles are failing. A third group presents as refractory hypoxaemia, where oxygenation cannot be maintained despite high-flow or non-invasive support, the hallmark of parenchymal lung disease and acute respiratory distress. [3]
The ventilated child is then examined for how the machine and the patient are interacting, and this bedside reading is itself a clinical skill. Increased work of breathing despite the ventilator suggests asynchrony, inadequate support or a fighting patient. A falling oxygen saturation suggests derecruitment, a plugged tube, pneumothorax or worsening lung disease. The signs of patient-ventilator asynchrony, double-triggering, breath-stacking, missed triggers and ineffective efforts, are visible at the bedside and matter because they prolong ventilation and worsen lung injury. The candidate is expected to read the whole picture: the child, the monitor, the ventilator screen and the waveforms together. [10] [3]
Differential Diagnosis
Before settling on a ventilator strategy, the clinician decides which of several physiological failures is driving the child, because the failure selects the emphasis of the support. A failure of oxygenation, the hallmark of shunt and low ventilation-perfusion matching in consolidated lung, demands attention to mean airway pressure, positive end-expiratory pressure and the inspired oxygen. A failure of ventilation, a rising carbon dioxide from inadequate minute volume, demands attention to the tidal volume and respiratory rate. A failure of effort, where exhausted or weak muscles cannot sustain the work, demands that the ventilator take over the work of breathing while the cause is treated. Many children combine more than one, and naming which dominates is what makes the settings defensible. [3]
Deterioration in a child already ventilated has its own differential that the examiner expects to hear rehearsed as a structured response. The useful framework is to divide causes into those of the airway and circuit, such as a blocked, kinked or displaced tube, a disconnected circuit or a plugged endotracheal tube; those of the lung, such as right mainstem intubation, pneumothorax, atelectasis, consolidation or worsening oedema; and those of the patient and machine, such as agitation and asynchrony, inadequate sedation, a machine fault or a migration of the tube. Working through airway, lung and patient in order is the bedside discipline that finds the reversible cause fast. [10]
Clinical & Bedside Assessment
The bedside assessment of a ventilated child has two layers. The first is the child: the depth and rate of breathing, whether it is comfortable and synchronised or fighting the ventilator, the pattern and equality of chest movement, air entry on auscultation, the oxygen saturation and the capillary refill and perfusion that speak to shock. The second is the machine and the numbers: the set mode, the tidal volume delivered and the tidal volume exhaled, the peak and plateau pressures, the positive end-expiratory pressure, the inspired oxygen, and the alarm limits. A candidate who can read both, and relate the numbers to the child, is demonstrating the competence the exam is testing. [10]
Waveforms and graphics deserve specific attention because they are how asynchrony is detected at the bedside. The pressure, flow and volume traces reveal whether the patient is triggering effectively, whether breaths are stacked, whether the set inspiratory time suits the patient's neural timing, and whether the expiratory flow has returned to baseline before the next breath begins, the sign of inadequate expiratory time that risks air-trapping. Capnography is essential and continuous: the end-tidal carbon dioxide tracks ventilation and trends with the arterial value, and a sudden fall warns of a fall in cardiac output, a blocked tube, a circuit leak or a pneumothorax. [3] [10]
Investigations
Blood gas analysis is the central investigation, and the distinction between arterial and capillary sampling matters in a ventilated child. An arterial line allows repeated sampling and direct measurement of the oxygen partial pressure that calculates the oxygenation index, the marker of severity in paediatric acute respiratory distress syndrome, defined as the mean airway pressure multiplied by the inspired oxygen fraction divided by the arterial oxygen partial pressure, with a rising oxygenation index marking worsening disease. Capillary and venous gases track the carbon dioxide and pH reliably but do not inform the oxygenation index, so an arterial gas is sought when oxygenation severity must be quantified. [1] [2]
Imaging and monitoring frame the ventilator course rather than making the diagnosis alone. A chest radiograph confirms tube position, excludes right mainstem intubation and pneumothorax, and tracks the lung disease, while point-of-care ultrasound and, in severe disease, computed tomography refine the picture. Continuous monitoring combines pulse oximetry, capnography and the ventilator graphics, and is supplemented by regular blood gases. The oxygenation index, trended over time, is the single most useful summary number in severe disease because it bundles the cost of oxygenation, the inspired oxygen and the mean airway pressure, into one severity measure. [1] [6]
Management — Resuscitation
When a child is intubated, the immediate task is to secure the airway, confirm tube placement and set safe initial ventilator settings, then titrate to the blood gas and the disease. Tube placement is confirmed by bilateral air entry, chest rise, waveform capnography over several breaths, and post-intubation imaging, because capnography is the single most reliable bedside confirmation and oesophageal intubation is lethal if missed. The initial settings follow a lung-protective philosophy from the outset: a tidal volume around 6 to 8 millilitres per kilogram predicted body weight, a respiratory rate appropriate to age, a positive end-expiratory pressure to keep the lung recruited, and the lowest inspired oxygen that keeps the saturation in the target range. [3] [2]
In the child with parenchymal lung disease or acute respiratory distress, the protective settings are tightened deliberately. Tidal volume is reduced toward 4 to 6 millilitres per kilogram in severe disease, the inspiratory plateau pressure is held at or below 28 centimetres of water, positive end-expiratory pressure is titrated to optimise oxygenation without overdistending, and permissive hypercapnia is accepted so long as the pH is preserved above about 7.20. Wong and colleagues showed in a controlled trial that a structured lung-protective protocol built on these targets was associated with improved survival in paediatric acute respiratory distress syndrome, which is why the strategy is now the default rather than a rescue measure. [2] [5]
Setting up lung-protective ventilation
Confirm tube placement with bilateral air entry and continuous waveform capnography
Set a tidal volume near 6 to 8 millilitres per kilogram predicted body weight, lower in severe disease
Choose an age-appropriate respiratory rate and an inspiratory time that suits the disease
Titrate positive end-expiratory pressure to recruit the lung and optimise oxygenation
Set the lowest inspired oxygen that holds saturation in the target range
Hold the inspiratory plateau pressure at or below 28 centimetres of water
Accept permissive hypercapnia with a pH above about 7.20
Check an early blood gas and adjust the rate, volume and oxygen against it
Management — Definitive & Stepwise
Definitive ventilation is a dynamic process of titration, synchronisation and daily liberation assessment, not a set-and-forget prescription. Each day the team asks whether the disease is recovering, whether the support can be reduced, and whether the child is ready to begin liberation. Positive end-expiratory pressure and inspired oxygen are weaned first as oxygenation improves, the mode is moved toward one that allows spontaneous breathing such as pressure support, and analgesia and sedation are lightened in step. The discipline is to reduce support the moment it is safe to do so, because every unnecessary day of ventilation adds risk. [4] [3]
Ventilator liberation is now guided by an international clinical practice guideline that frames it as a deliberate, tested process rather than clinical intuition. The guideline endorses a spontaneous awakening trial or a coordinated awakening and breathing trial, in which sedation is reduced and the patient is observed breathing with reduced support, as the most effective screening step. A child who tolerates this moves to a formal extubation readiness test, typically a short spontaneous breathing trial on low pressure support and low or zero positive end-expiratory pressure, and is extubated if gas exchange, effort and secretion clearance remain adequate. [4]
Planning does not stop at extubation, because preventing reintubation is part of liberation. In infants and young children, and in those with chronic lung or airway disease who are predicted to fail, the systematic review and network meta-analysis by Iyer and colleagues found that high-flow nasal cannula, continuous positive airway pressure and bilevel support all reduced extubation failure compared with conventional oxygen therapy, with non-invasive ventilation offering the strongest effect. Electing the right post-extubation support before the tube comes out, rather than reacting after the child fails, is how the liberation strategy closes. [11] [4]
Stepwise ventilator liberation
Each day assess whether the underlying disease is resolving and support is reducible
Wean positive end-expiratory pressure and inspired oxygen first as oxygenation improves
Lighten sedation and move the mode toward pressure support
Perform a spontaneous awakening and breathing trial as a screening step
Run a formal extubation readiness test on low pressure support
Confirm adequate gas exchange, effort and secretion clearance before extubating
Plan post-extubation non-invasive support for predicted failure, especially in infants
Monitor closely after extubation and reintubate promptly if liberation fails
Specific Subtypes & Scenarios
Paediatric acute respiratory distress syndrome is the scenario that most completely exercises lung-protective ventilation, because here the diseased lung is most vulnerable to the ventilator and the protective targets matter most. The consensus definition, refined by the second Pediatric Acute Lung Injury Consensus Conference, diagnoses it from new respiratory failure within seven days, bilateral opacities not explained by effusion or collapse, and origin not fully cardiac, with severity graded by the oxygenation index or, where arterial blood is unavailable, by the oxygen saturation index. Management is built on low tidal volume, plateau pressure limitation, optimised positive end-expiratory pressure and permissive hypercapnia, and the disease is commoner and deadlier than historically appreciated, as the PARDIE study showed. [1] [6] [2]
The child with status asthmaticus poses the opposite mechanical problem, and the strategy differs in a way an examiner rewards. Here the threat is dynamic hyperinflation and air-trapping from severe obstruction, so ventilation is deliberately slow, with a low respiratory rate, a long expiratory time, and acceptance of a high carbon dioxide so long as the pH is tolerated, in order to avoid stacking gas that cannot escape and causing a pneumothorax or impaired venous return. The bronchiolitic infant is intubated most often for apnoea rather than refractory hypoxaemia, tolerates a gentle approach, and is a common candidate for early non-invasive support and rapid liberation. [3] [10]
Across Australia, New Zealand and comparable systems, mechanical ventilation in children is delivered in paediatric intensive care units by intensivists using lung-protective targets aligned with the Pediatric Acute Lung Injury Consensus Conference and the Paediatric Mechanical Ventilation Consensus Conference recommendations. Retrieval services ventilate children for transport with portable devices, and the move toward non-invasive support for the milder end of respiratory failure has shifted intubation toward the sicker child. Guideline frameworks are internationally aligned, and regional differences are pragmatic, turning on access to paediatric intensive care, retrieval and post-extubation respiratory support rather than on the physiological principles themselves. [3] [4]
Complications & Pitfalls
The complications of mechanical ventilation divide into those of the invasive airway, those of the diseased lung, and those of prolonged immobility and sedation. The endotracheal tube itself causes trauma to the airway, can block or displace, and is the gateway to ventilator-associated pneumonia, which lengthens intensive care stay and adds mortality, so preventing it with a bundle of head-of-bed elevation, oral hygiene, closed suction, daily sedation review and prompt liberation is a core duty. Positive pressure can cause a pneumothorax, can depress cardiac output by raising intrathoracic pressure, and over time contributes to muscle weakness and critical illness polyneuropathy. [9] [3]
The pitfalls are errors of reasoning as much as of technique. The recurring mistakes are ventilating a diseased lung with a conventional tidal volume that overdistends it, chasing a normal carbon dioxide with volumes and pressures that injure the lung, silencing an alarm rather than finding its cause, failing to wean because the team has not assessed readiness, and extubating without a plan for post-extubation support. A quieter pitfall is treating pain and agitation lightly, because the resulting asynchrony and breath-stacking are themselves a source of lung injury, so analgesia-first sedation is part of protection, not a comfort measure. [2] [10]
Prognosis & Disposition
Prognosis in the ventilated child is dominated by the underlying disease and its severity, but the ventilator strategy changes the outcome in the diseases most vulnerable to harm. In paediatric acute respiratory distress syndrome, mortality remains significant and concentrates in the most severe and hypoxaemic children, yet lung-protective ventilation is one of the few interventions shown to improve survival, as Wong and colleagues demonstrated. For most children with self-limiting respiratory infections, the course is one of support through the illness and liberation as it resolves, and the duration of ventilation tracks the disease more than the technology. [6] [5]
Disposition is a recovery-planning exercise as much as a medical one. The child is ready to leave intensive care when the disease is resolving, support has been weaned to minimal levels or the child is extubated and stable, and the team is confident that ongoing ward-level care is safe. For children with chronic respiratory failure or neuromuscular disease, disposition may involve a planned transition to non-invasive or home ventilation, and the ventilated child with a prolonged or complex course often needs rehabilitation for acquired weakness and a coordinated recovery plan. [3] [4]
Special Populations
Infants and young children are the defining special population, and their physiology changes how ventilation is delivered. The infant airway is narrow and easily blocked by secretions, the chest wall is compliant and the functional residual capacity low, and the oxygen consumption per kilogram is high, so infants desaturate quickly and tolerate apnoea poorly. These features explain why small endotracheal tubes, careful humidification, meticulous suctioning and a low threshold for non-invasive support characterise infant ventilation, and why post-extubation failure is common enough to warrant planned non-invasive support. [11] [3]
The child with chronic lung disease, neuromuscular weakness, or a technology-dependent airway needs ventilation planned around chronic fragility. The bronchopulmonary dysplasia infant, the child with cerebral palsy and scoliosis, and the child with a tracheostomy for chronic airway obstruction all have reduced reserve, difficulty clearing secretions, and a higher risk of a complicated course, so their ventilation is gentler, their weaning more cautious, and their liberation planned with post-extubation support and a clear airway-clearance strategy. Immunocompromised children face a disproportionate mortality from respiratory failure and benefit from early, lung-protective support with a low threshold for expert input. [6] [9]
Evidence, Guidelines & Regional Differences
The guideline backbone for paediatric ventilation is a small set of consensus documents a candidate should be able to name. The original Pediatric Acute Lung Injury Consensus Conference report established the definition of paediatric acute respiratory distress syndrome and the lung-protective targets that followed, and its successor, the PALICC-2 executive summary, updated the definition, severity grading and management recommendations. The Paediatric Mechanical Ventilation Consensus Conference recommendations address the practical ventilation of critically ill children across modes and settings, and the PALISI international guideline on ventilator liberation governs weaning and extubation. [1] [2] [3] [4]
The trial and cohort evidence fills in the specifics and the boundaries. The PARDIE study quantified the incidence and mortality of paediatric acute respiratory distress syndrome; Wong showed that a lung-protective protocol improved survival; the PALISI guideline distilled the liberation evidence into a daily awakening and breathing trial and a formal extubation readiness test; and Iyer's network meta-analysis established that post-extubation non-invasive support reduces reintubation in infants and young children. Two large sedation trials temper enthusiasm: the RESTORE and SANDWICH trials found that protocolised sedation and ventilator-liberation strategies did not, in their primary analysis, shorten the duration of mechanical ventilation in children, a reminder that adult protocols do not translate directly. [6] [5] [4] [11] [7] [8]
Regional differences are pragmatic rather than conceptual. High-income systems agree on the physiological principles, the lung-protective targets, and the tested liberation pathway, but they differ in access to paediatric intensive care, in retrieval capability for the ventilated child, and in the availability of post-extubation respiratory support. In Australia and New Zealand the equity dimension, particularly for rural and remote families and for Indigenous children transferred far from home for intensive care, shapes how the service is organised around the family rather than what the physiological target is. [3] [4]
Exam Pearls
Lung-protective settings — 'PROTECT'
References
- [1]Pediatric Acute Lung Injury Consensus Conference Group Pediatric acute respiratory distress syndrome: consensus recommendations from the Pediatric Acute Lung Injury Consensus Conference. Pediatr Crit Care Med, 2015.PMID 25647235
- [2]Emeriaud G; López-Fernández YM; Iyer NP; Blackwood B; Curley MAQ; Dobyns EL; et al Executive Summary of the Second International Guidelines for the Diagnosis and Management of Pediatric Acute Respiratory Distress Syndrome (PALICC-2). Pediatr Crit Care Med, 2023.PMID 36661420
- [3]Kneyber MCJ; de Luca D; Calderini E; Jarreau PH; Javouhey E; Lopez-Fernandez Y; et al Recommendations for mechanical ventilation of critically ill children from the Paediatric Mechanical Ventilation Consensus Conference (PEMVECC). Intensive Care Med, 2017.PMID 28936698
- [4]Abu-Sultaneh S; Iyer NP; Fernández A; Bauman S; Carroll CL; Cheifetz IM; et al Executive Summary: International Clinical Practice Guidelines for Pediatric Ventilator Liberation, A Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network Document. Am J Respir Crit Care Med, 2023.PMID 36583619
- [5]Wong JJM; Dang H; Gan CS; Phua HP; Goh RSY; Mok YH; et al Lung-Protective Ventilation for Pediatric Acute Respiratory Distress Syndrome: A Nonrandomized Controlled Trial. Crit Care Med, 2024.PMID 38920618
- [6]Khemani RG; Smith L; Lopez-Fernandez YM; Shi H; Rapoport S; Newth CJL; et al Paediatric acute respiratory distress syndrome incidence and epidemiology (PARDIE): an international, observational study. Lancet Respir Med, 2019.PMID 30361119
- [7]Curley MA; Wypij D; Watson RS; Grant MJ; Asaro LA; Dodson BL; et al Protocolized sedation vs usual care in pediatric patients mechanically ventilated for acute respiratory failure: a randomized clinical trial. JAMA, 2015.PMID 25602358
- [8]Blackwood B; Tume LN; Morris KP; Swinton F; Turnbull KL; Linke-Heer D; et al Effect of a Sedation and Ventilator Liberation Protocol vs Usual Care on Duration of Invasive Mechanical Ventilation in Pediatric Intensive Care Units: A Randomized Clinical Trial. JAMA, 2021.PMID 34342620
- [9]Chang I; Schibler A Ventilator Associated Pneumonia in Children. Paediatr Respir Rev, 2016.PMID 26527358
- [10]Egbuta C; Easley RB Update on ventilation management in the Pediatric Intensive Care Unit. Paediatr Anaesth, 2022.PMID 34882910
- [11]Iyer NP; Rotta AT; Essouri S; Schiller O; Mhanna MJ; St Julien JP; et al Association of Extubation Failure Rates With High-Flow Nasal Cannula, Continuous Positive Airway Pressure, and Bilevel Positive Airway Pressure vs Conventional Oxygen Therapy in Infants and Young Children: A Systematic Review and Network Meta-Analysis. JAMA Pediatr, 2023.PMID 37273226