Paeds · acute-care-resuscitation-and-toxicology
Oesophageal and gastrointestinal foreign-body ingestion
Also known as Foreign-body ingestion · Button battery ingestion · Coin ingestion · Magnet ingestion · Oesophageal food bolus impaction
A fellowship approach to the child who has swallowed a foreign body. The single decision that changes everything is whether a button battery or a complete oesophageal obstruction is lodged in the oesophagus, because both demand emergency endoscopic removal within two hours. Use a plain anteroposterior chest and abdominal radiograph with a lateral view to identify batteries and magnets, apply NASPGHAN and ESPGHAN urgency categories for every other object, observe blunt gastric objects that are below threshold size, and consult early for sharp, long, multiple-magnet and button-battery ingestions.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old is brought in after swallowing a coin. The clinical question is not whether to remove it, but where it sits, what it is, and how quickly it must come out. Foreign-body ingestion means any object swallowed into the gastrointestinal tract, and the practical classification is built around the objects that kill or main children when managed by a generic observe-and-wait rule. [1] [11]
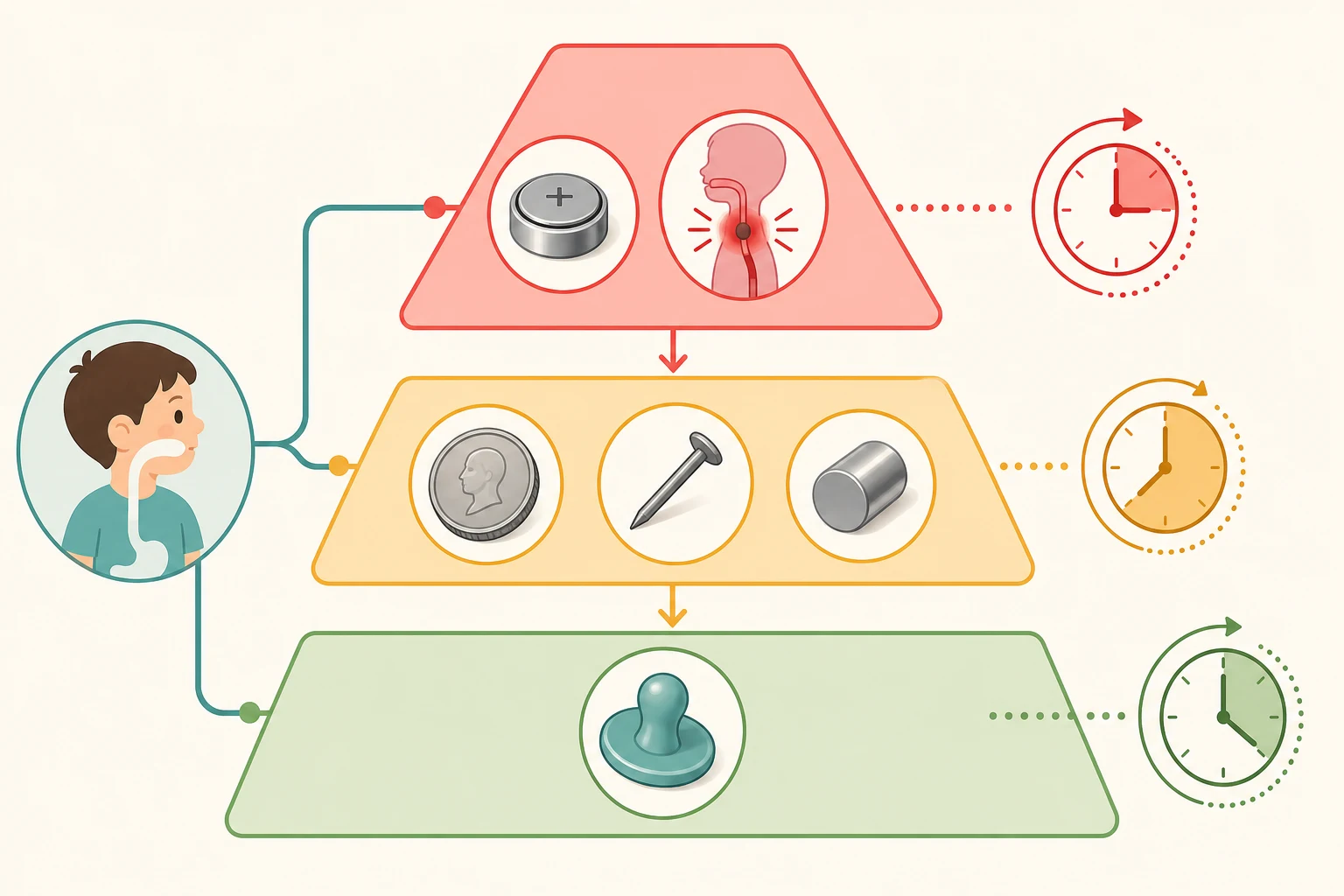
Three object types override any observation strategy. A button battery lodged in the oesophagus generates hydroxide ions by electrolysis of tissue fluid, creating a local alkaline burn that can perforate within hours. Multiple magnets, or a magnet paired with a metal object, can trap bowel walls between them and cause pressure necrosis, fistula, volvulus and perforation. Sharp objects such as pins, needles and safety pins can perforate anywhere along the tract. Each of these has its own timing rule. [3] [6] [8]
The site of lodgement matters as much as the object. The oesophagus has three classic narrowing points where objects lodge: the cricopharyngeus at the thoracic inlet, the aortic arch and carina crossing, and the lower oesophageal sphincter. About two thirds of oesophageal coins lodge at the thoracic inlet. An object that has passed the pylorus usually transits spontaneously, with the exception of sharp, long or magnetic objects. [1] [11]
Classification
Foreign-body ingestions are classified by the object and by its anatomical site, because these two axes together set the urgency. The NASPGHAN Endoscopy Committee clinical report and the ESPGHAN guideline define the urgency tiers that frame every management decision. [1] [2]
| Object | In the oesophagus | In the stomach or beyond |
|---|---|---|
| Button battery | EMERGENCY endoscopy within 2 hours | Observe if asymptomatic and beyond pylorus; urgent removal if symptomatic or not progressing |
| Coin | URGENT endoscopy within 24 hours even if asymptomatic | Observe if asymptomatic; repeat radiograph if not passed in 4 weeks |
| Sharp object (pin, needle, open safety pin) | URGENT endoscopy within 24 hours or sooner | URGENT removal if in stomach; surgical review if beyond pylorus |
| Single magnet | Endoscopic removal | Remove if accessible; close radiographic follow-up for any second magnet or metal |
| Multiple magnets or magnet plus metal | EMERGENCY or urgent removal | Surgical and endoscopic review; remove to prevent inter-loop fistula |
| Long object greater than 6 cm or wide object greater than 2.5 cm | Endoscopic or surgical removal | Unlikely to pass the duodenum; remove endoscopically if possible |
| Meat bolus with complete obstruction | EMERGENCY endoscopy within 2 hours | Not applicable |
| Meat bolus with incomplete obstruction | Endoscopy within 24 hours | Not applicable |
The thresholds are deliberate. Objects longer than 6 centimetres or wider than 2.5 centimetres rarely negotiate the duodenal sweep, and button batteries 20 millimetres or larger in children younger than five years carry the greatest risk of lodgement and severe injury. [1] [4]
Epidemiology & Risk Factors
Foreign-body ingestion is one of the most common paediatric emergency presentations. Peak age is between six months and three years, the developmental window of mouthing and exploration, and coins account for the majority of ingested objects in most series. Button-battery ingestions are less common than coin ingestions but carry an order of magnitude greater risk of severe and fatal injury. [1] [4]
Litovitz analysed 8648 battery-ingestion cases reported to a national poison centre and showed that the risk of a severe or fatal outcome rose sharply when the battery was 20 millimetres or larger and the child was younger than four years. The Tran systematic review and pooled analysis of individual patient-level data confirmed that severe complications cluster in the oesophagus, present within hours of lodgement, and may evolve into aorto-oesophageal or tracheo-oesophageal fistula days to weeks after the battery is removed. [4] [5]
Children at highest risk of ingestion, and of poor outcome, share identifiable features: developmental age under five years, neurodevelopmental disability, oesophageal motility disorder or prior oesophageal surgery, a household with accessible loose batteries or magnets, and refugee or migrant families unfamiliar with local product-safety advice. Recognising these features should lower the threshold for imaging when the history is uncertain. [11] [9]
Pathophysiology
A coin sitting in the oesophagus causes harm by pressure necrosis against the oesophageal wall over hours to days. A button battery does far worse, faster, and by a different mechanism. Within minutes of lodgement the battery drives electrolysis of tissue water, generating hydroxide ions at the negative pole. The local pH climbs above 12, producing a liquefactive alkaline burn analogous to caustic soda ingestion. This is the dominant mechanism of early injury. [3] [8]
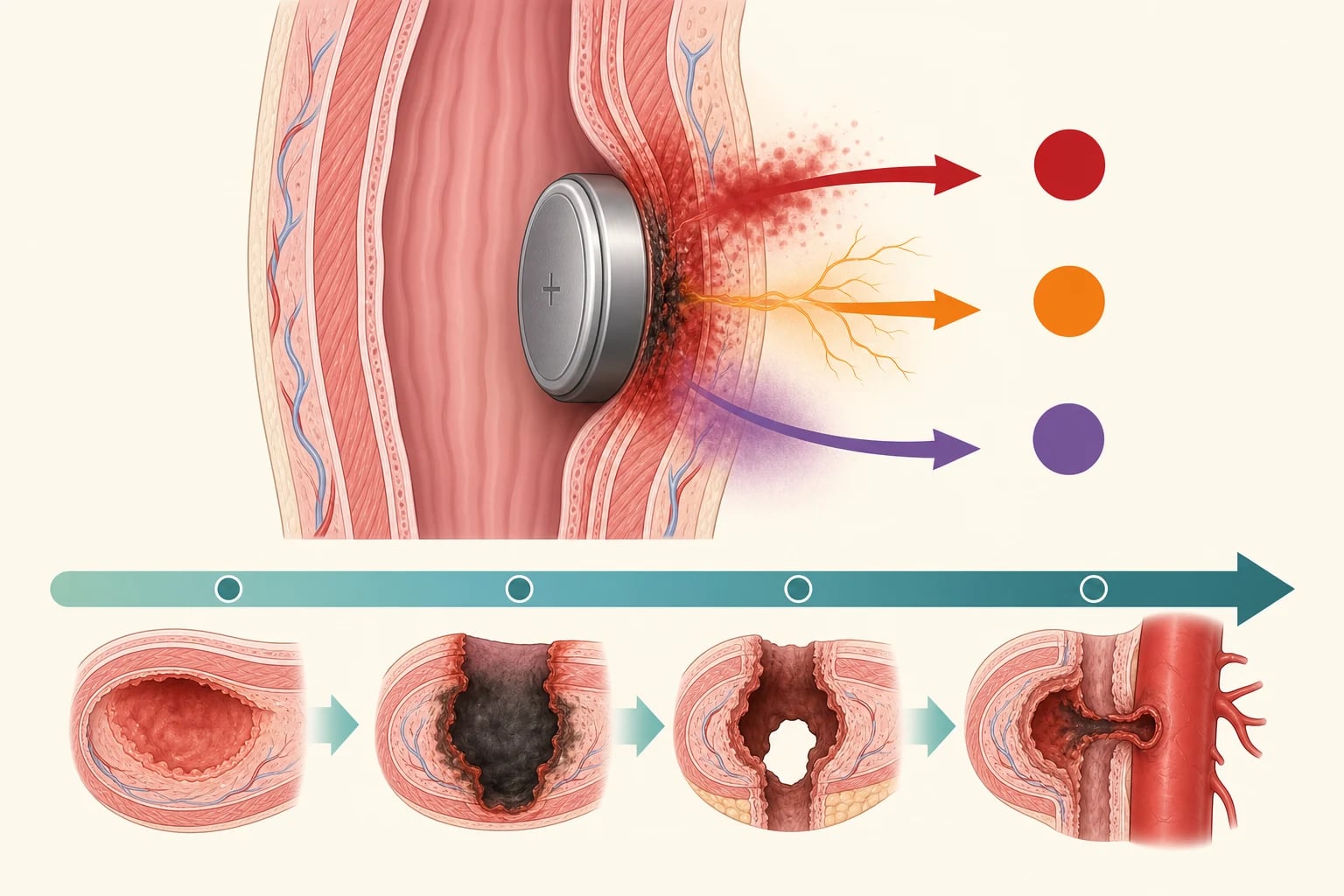
Two further mechanisms compound the burn. The electrical current itself injures tissue at the contact site, and sustained pressure adds ischaemic necrosis. The combined injury can erode through the full oesophageal wall into the aorta or trachea. Critically, the inflammatory cascade does not stop when the battery is removed: fistula and perforation can declare days to weeks later, so post-removal observation and re-imaging are mandatory when injury is suspected. [3] [5]
Magnets injure by an entirely different route. When two or more magnets, or a magnet and a ferrous metal object, sit in adjacent loops of bowel, they attract across the bowel walls, trap the intervening tissue, and cause pressure necrosis, fistula, volvulus, and perforation without any chemical burn. The first sign may be peritonitis from perforation, so any radiograph showing more than one radiopaque object that could be a magnet must be treated as high-risk until counted and located precisely. [6]
Clinical Presentation
Most children with a swallowed object are brought in by a caregiver who saw the ingestion, but a substantial minority present with symptoms alone. The history should capture the suspected object, the time of ingestion, the number of objects if magnets or batteries are possible, any symptoms since, and any underlying oesophageal or neuromuscular disorder. A missing history does not exclude the diagnosis. [1] [11]
An oesophageal object, whatever it is, causes drooling, dysphagia, refusal of food or drink, retrosternal discomfort, wheeze, or a persistent cough from tracheal compression. A child who cannot swallow their own saliva has complete obstruction and is at aspiration risk. A gastric or distal object is usually asymptomatic, but abdominal pain, vomiting, fever or distension suggest obstruction, perforation or fistula. [2] [7]
Red-flag presentations are specific enough to anchor a diagnosis. Haematemesis, coffee-ground vomiting or melaena after a known or suspected battery ingestion is the presentation of aorto-oesophageal fistula until proven otherwise, and it carries a high mortality. Bilious vomiting, severe abdominal pain or peritonism after a magnet ingestion suggests volvulus or perforation. Stridor, wheeze or recurrent pneumonia in an infant may be the late presentation of a chronically lodged oesophageal foreign body. [3] [6] [12]
Differential Diagnosis
The differential splits into what the object is, what it is mimicking, and what is causing the symptoms when no object is found. The most important mimic is the coin-versus-button-battery confusion on a plain radiograph. A button battery shows a halo or double-ring sign on the anteroposterior view and a step-off at its rim on the lateral view, whereas a coin appears as a solid disc. A stacked pair of coins can mimic a battery, and so can some magnets. When the radiograph is not diagnostic, treat the object as a battery until proven otherwise. [10]
Symptom mimics include odynophagia or dysphagia from oesophagitis, infectious pharyngitis, retropharyngeal abscess, asthma and gastro-oesophageal reflux. A wheezy or coughing infant may have an unsuspected oesophageal foreign body rather than bronchiolitis, especially if symptoms are unilateral, persistent or atypical. Always consider ingestion when the presentation does not fit a common pattern. [12] [2]
The non-accidental and developmental differential also belongs here. Recurrent foreign-body ingestion, or ingestion of unusual or dangerous objects, raises the question of supervision neglect, an unsafe home environment, pica associated with iron deficiency, or autism spectrum disorder. These do not change the acute management but should be flagged for social work and developmental follow-up. [11]
Clinical & Bedside Assessment
Begin with an airway, breathing and circulation screen, because a complete oesophageal obstruction can compromise the airway with pooled secretions, and a mediastinal catastrophe from a battery can present as shock. A child who is drooling continuously, unable to handle secretions, or in respiratory distress is an emergency and needs nothing else before the endoscopy team is called. [1]
Inspect the oropharynx for drooling, pooled secretions, an embedded object, or signs of caustic injury, but do not perform a blind finger sweep or attempt removal of an object you cannot fully see, because these manoeuvres can push the object into the airway or perforate the oesophagus. Examine the neck, chest and abdomen for subcutaneous emphysema from perforation, localised tenderness, and signs of peritonism. Document the time of ingestion and the time of last food, because both affect anaesthetic timing. [2] [11]
Take a structured history that names the object if possible. Ask the caregiver to bring a matching object or its packaging, especially for batteries and toys containing magnets. Count the number of missing magnets from a toy set, because more than one magnet changes management entirely. Ask about oesophageal disease, prior surgery, and bleeding tendency, all of which change the threshold for endoscopy and the choice of technique. [1] [6]
Investigations
The only first-line investigation is a plain radiograph of the chest and abdomen, including anteroposterior and lateral views. The lateral view distinguishes a battery from a coin, locates the object in three dimensions, and reveals a second magnet or a second object behind the first. Include the entire abdomen to track objects that have passed the pylorus. Hand-held or bedside metal detectors are an alternative for confirmed coin ingestion in some centres, but they do not characterise the object and should not replace radiography when a battery is possible. [1] [10]
Radiographic signs that distinguish a button battery from a coin
Blood tests add nothing in the stable child. Request a full blood count, group and hold, cross-match, venous gas and lactate only when perforation, fistula or significant bleeding is suspected, because these change the operative and intensive-care plan. Computed tomography or contrast oesophagography is reserved for the complicated or delayed presentation, suspected fistula, or post-removal reassessment of a deep burn; it is not a screening test. [3] [5]
The most important investigation decision is the timing of endoscopy, which is both diagnostic and therapeutic. Endoscopy confirms the object, grades any mucosal injury, allows retrieval, and at the same time inspects for impending perforation. The urgency of endoscopy is set entirely by the object, the site, and the symptoms, as set out in the Classification section. [1] [2]
Management — Resuscitation
A child who is drooling, distressed, or showing signs of airway compromise from a complete oesophageal obstruction is an emergency. Call the anaesthetic and endoscopy teams in parallel, keep the child upright and nil by mouth, suction secretions from the mouth, and move to theatre for emergency endoscopic removal within two hours. Do not wait for further imaging if the airway is threatened. [1] [2]
For a confirmed or suspected oesophageal button battery, every minute counts. The ESPGHAN position paper supports endoscopic removal within two hours of presentation regardless of symptoms, because alkaline necrosis is already underway. Where removal will be delayed and the child is older than twelve months, has no evidence of perforation, and the battery is confirmed in the oesophagus, a honey or sucralfate demulcent can be given by mouth while awaiting endoscopy. The ESPGHAN-endorsed dose of honey is approximately 10 millilitres every ten minutes up to six doses, with a smaller volume of 5 millilitres in children under one year; honey is contraindicated in infants under twelve months because of botulism risk. These agents are adjuncts, never substitutes, for emergency removal. [3] [9]
Honey (as a temporising demulcent for a confirmed oesophageal button battery)
Dose
10 mL by mouth every 10 minutes, up to 6 doses
Resuscitation for the complicated ingestion follows the same principle. For suspected perforation or fistula, give nothing by mouth, establish wide-bore intravenous access, start intravenous fluids and a proton-pump inhibitor, give broad-spectrum antibiotics, cross-match blood, and call paediatric surgery and intensive care. For suspected aorto-oesophageal fistula presenting with haematemesis, massive transfusion capability, interventional radiology and cardiothoracic surgery must be mobilised alongside endoscopy. These children can exsanguinate within minutes of a sentinel bleed. [3] [8]
Management — Definitive & Stepwise
Once the object is identified and located, definitive management follows the NASPGHAN and ESPGHAN urgency tiers. Endoscopy is the workhorse for oesophageal objects, for gastric sharp objects, and for magnets within reach. The technique is chosen by the endoscopist: a Roth net, polypectomy snare, retrieval forceps, or an overtube to protect the airway and allow repeated passes. [1] [2]
Definitive management sequence
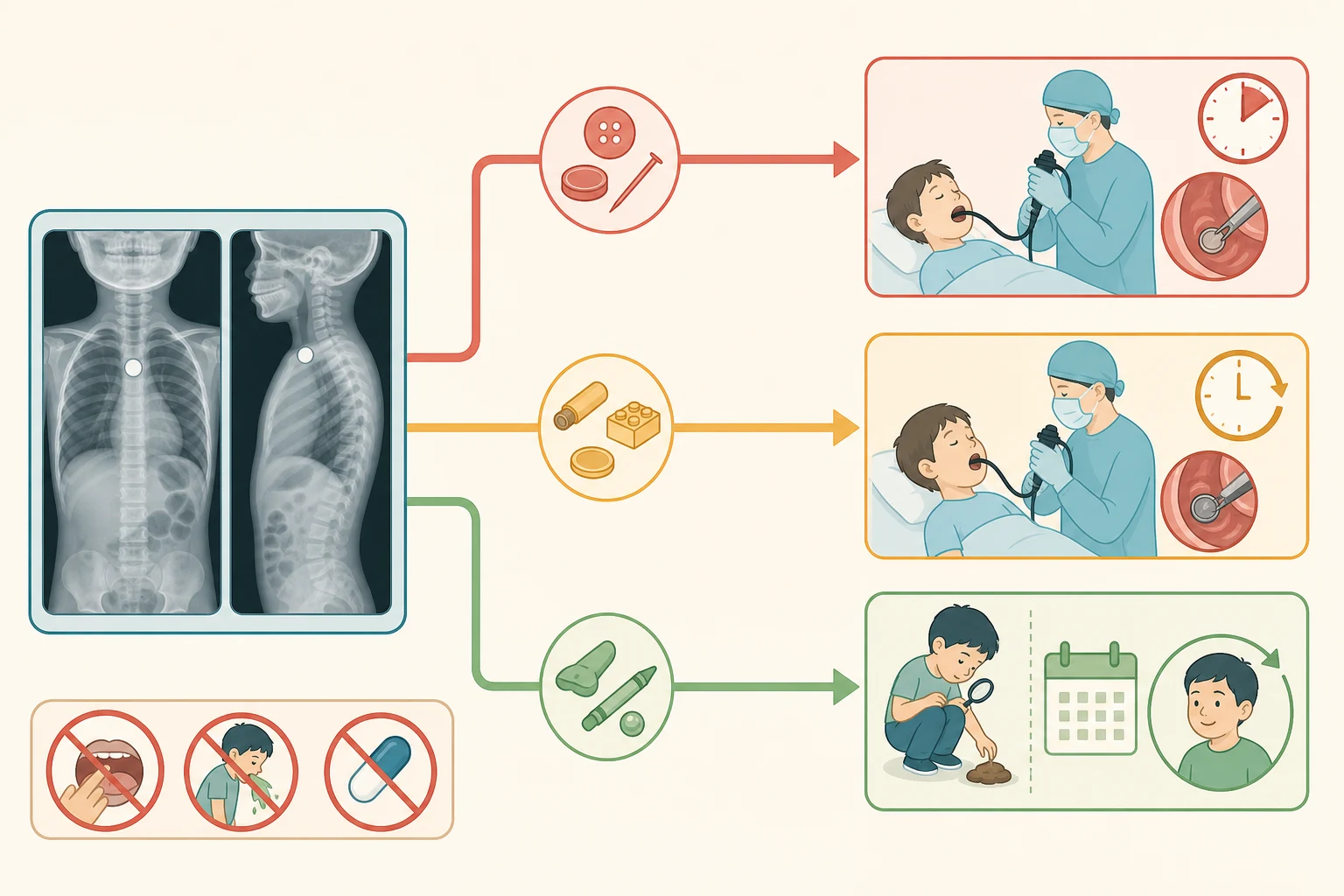
Confirm object and site with AP and lateral chest and abdominal radiograph before disposition
Apply urgency tier: emergency within 2 hours for oesophageal battery or complete obstruction; urgent within 24 hours for oesophageal coin, sharp object, or single magnet; observe blunt gastric objects below threshold size
For oesophageal battery with delayed endoscopy, consider honey or sucralfate demulcent if older than 12 months and no perforation
Endoscopic retrieval by trained paediatric gastroenterologist or surgeon, with anaesthetic airway protection
Inspect mucosa at retrieval and grade the burn; admit and observe for any deep oesophageal injury
For blunt gastric objects managed by observation, instruct the family to check stools, return for abdominal pain or fever, and repeat radiograph at 4 weeks if not passed
Involve surgery early for sharp objects beyond the pylorus, multiple magnets, long or wide objects, and any sign of perforation or fistula
After endoscopic removal of an oesophageal battery or sharp object, the next decision is whether the mucosal injury requires inpatient observation and further imaging. Supergrade injuries confined to the mucosa may be observed briefly and discharged with safety-net advice. Deep injuries extending into the submucosa or muscle, and any child with a battery removed more than twelve hours after lodgement, should be admitted for observation because of the risk of delayed perforation and fistula. [3] [5]
For asymptomatic coins and small blunt objects already in the stomach, observation at home is safe provided there is no prior gastrointestinal surgery, no sharp edge, and the object is below threshold size. Ask the caregiver to check the stools for the object, to return urgently with abdominal pain, vomiting, fever or bleeding, and to attend for a repeat radiograph at four weeks if the object has not been seen to pass. Mantegazza and colleagues derived and validated a nomogram predicting the need for endoscopic or surgical intervention from object type, site and size, which can support the decision in borderline cases. [7] [1]
Specific Subtypes & Scenarios
Button battery lodged in the oesophagus is the archetype of the time-critical ingestion. Endoscopic removal within two hours is the standard. If removal will be delayed, give a honey or sucralfate demulcent to the eligible child, keep the child nil by mouth and upright, and alert anaesthetics, surgery and intensive care. After removal, grade the burn, observe for delayed complications, and schedule endoscopic follow-up for any deep injury. [3] [9]
Button battery beyond the pylorus in an asymptomatic child can usually be observed, with daily radiographs to confirm progression and urgent removal if it stalls or the child becomes symptomatic. ESPGHAN favours a shorter observation window than NASPGHAN for larger batteries and younger children, so confirm the local policy. Any sign of abdominal pain, vomiting, fever or bleeding mandates surgical review. [3] [1]
Coins in the oesophagus are removed urgently, within twenty-four hours, even when asymptomatic, because pressure necrosis and ulceration develop over time. Coins in the stomach in an asymptomatic child with no prior surgery are observed. Disc batteries in the stomach behave like coins if the child is well, but the threshold for removal is lower for larger batteries and younger children. [1] [11]
Sharp objects such as open safety pins, needles and toothpicks carry a high perforation risk anywhere in the tract. Remove them endoscopically if they are in the oesophagus or stomach. Once beyond the pylorus, the decision is shared with surgery: serial radiographs and close observation if the object is progressing, operative retrieval if it stalls, perforates, or causes symptoms. [1] [2]
Multiple magnets, or a magnet with a metal object, are managed as high-risk wherever they sit. Endoscopic removal if reachable; otherwise surgical consultation, because inter-loop trapping can produce pressure necrosis, fistula and volvulus without warning symptoms. A single magnet is followed closely to confirm no second magnet exists. The Quitadamo ESPGHAN-endorsed review sets out the contemporary algorithm. [6]
Meat bolus impaction in children is less common than in adults but follows the same rule. Complete obstruction with drooling is an emergency within two hours because of aspiration risk. Incomplete obstruction can wait up to twenty-four hours for endoscopy. Avoid meat tenderiser and glucagon in children; the evidence base is poor and the harms real. [2] [1]
Long or wide objects greater than 6 centimetres long or 2.5 centimetres wide are unlikely to pass the duodenum. Remove them endoscopically if within reach, or refer for surgical retrieval if they have passed the pylorus and are not progressing. [1]
Complications & Pitfalls
The preventable complications cluster around two errors: failing to recognise a button battery as a battery, and treating every swallowed object as a coin to be observed. Both lead to delayed endoscopy, and delayed endoscopy is the single greatest predictor of severe oesophageal injury, fistula and death. [4] [5]
The Tran pooled analysis found that major complications, including perforation, fistula, stenosis, vocal-cord paralysis and death, were strongly associated with oesophageal lodgement, larger battery size, younger age, and longer time to removal. Aorto-oesophageal fistula is the most feared complication and may present as a sentinel herald bleed days to weeks after removal. Tracheo-oesophageal fistula presents with coughing after feeds or recurrent pneumonia. Oesophageal strictures can present weeks later with dysphagia. [5] [3]
Classic pitfalls include misreading a battery as a coin on radiograph, failing to obtain a lateral view, sending an asymptomatic child home without confirming the object has passed the pylorus, missing a second magnet, attempting a blind finger sweep or inducing vomiting, and discharging a child after battery removal without safety-net advice about delayed bleeding. Each of these is a recurring cause of adverse events in published case series. [10] [12]
Prognosis & Disposition
Most swallowed objects that reach the stomach pass spontaneously without intervention, and the vast majority of children do well. The prognosis is determined almost entirely by whether a button battery lodged in the oesophagus was recognised and removed quickly, and whether magnets were identified and retrieved before they could cause inter-loop injury. [1] [11]
Disposition follows the object and the mucosal injury. Children who have had an uncomplicated endoscopic removal of a coin, a small sharp object, or a non-oesophageal battery that has already passed can be discharged with safety-net advice. Children who have had an oesophageal button battery removed, or any deep mucosal burn, are admitted for observation and scheduled endoscopic follow-up. Children with suspected perforation, fistula, or multiple magnets go to theatre and then to a high-dependency or intensive-care setting as the procedure dictates. [3] [8]
Safety-net advice must be explicit and written. Tell the family what symptoms to watch for, including drooling, chest or abdominal pain, vomiting, fever, bleeding, coughing after feeds, and dysphagia. State how urgently to return, where to go, and that a sentinel bleed after a battery injury is an emergency. For discharged children with retained gastric objects, give a clear four-week repeat-radiograph plan. [9] [1]
Special Populations
Children with oesophageal motility disorder, prior oesophageal atresia repair, or eosinophilic oesophagitis are far more likely to lodge objects, including food boluses, and have a higher rate of stricture and perforation. Lower the threshold for imaging in these children and involve their specialist team early. [2] [11]
Children with neurodevelopmental disability or autism may not give a clear history, may present late with behavioural change or refusal to eat, and may have recurrent ingestions. A high index of suspicion, a low threshold for radiography, and a developmental and safeguarding review for recurrence are essential. [11]
Infants under one year are at particular risk from button batteries because their small oesophageal diameter lodges even small batteries, and honey is contraindicated as a demulcent because of infant botulism. The threshold for emergency endoscopy is lower, and the post-removal observation period is longer. [3]
Refugee, migrant and remote families may be unfamiliar with local product-safety messaging about button batteries and high-powered magnets, may face language and access barriers, and may present late. Use a professional interpreter, provide written safety information in the family's language, and link the family to primary care and product-safety resources to reduce recurrence. [9]
Evidence, Guidelines & Regional Differences
The evidence base is largely observational, built from large poison-centre case series, retrospective cohort studies and systematic reviews of individual patient data, because randomised trials are neither feasible nor ethical. The NASPGHAN Endoscopy Committee clinical report, the ESPGHAN foreign-body and caustic ingestion guideline, and the ESPGHAN button-battery position paper together set the international standard for object-and-site urgency tiers. [1] [2] [3]
Where the guidelines agree is more important than where they differ. All three recommend emergency endoscopic removal of an oesophageal button battery within two hours, urgent removal of oesophageal coins within twenty-four hours, surgical and endoscopic consultation for multiple magnets, and observation of asymptomatic blunt gastric objects below threshold size. The Tran systematic review and pooled analysis of individual patient-level data underpins the timing of severe complications, and the Mantegazza nomogram offers a decision-support tool for predicting the need for intervention. [5] [7]
Australia and Aotearoa New Zealand: The Royal Children's Hospital Melbourne foreign-body ingestion guideline and the Australian Journal of General Practice button-battery update carry the ANZ operational detail. The Australian Competition and Consumer Commission button-battery product-safety standard mandates child-resistant compartments for products sold with button batteries, and families should be directed to it for prevention advice. Local poison information centres, reachable on 13 11 26 in Australia and 0800 764 766 in New Zealand, support triage in real time. [9]
Where the guidelines differ is in the observation window for an asymptomatic button battery that has passed the pylorus. NASPGHAN permits observation for up to four days in selected older children with smaller batteries, while ESPGHAN favours a shorter window or earlier removal, particularly for younger children and larger batteries. State the local policy rather than inventing a universal rule. [1] [3]
Exam Pearls
References
- [1]Kramer, Robert E Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee Journal of pediatric gastroenterology and nutrition, 2015.PMID 25611037
- [2]Oliva, Sara Foreign body and caustic ingestions in children: A clinical practice guideline Digestive and liver disease, 2020.PMID 32782094
- [3]Mubarak, Ahmed Diagnosis, Management, and Prevention of Button Battery Ingestion in Childhood: A European Society for Paediatric Gastroenterology Hepatology and Nutrition Position Paper Journal of pediatric gastroenterology and nutrition, 2021.PMID 33555169
- [4]Litovitz, Toby Preventing battery ingestions: an analysis of 8648 cases Pediatrics, 2010.PMID 20498172
- [5]Tran, Cat Complications of button battery ingestion or insertion in children: a systematic review and pooled analysis of individual patient-level data World journal of pediatrics, 2024.PMID 39168931
- [6]Quitadamo, Pierluigi Magnetic foreign body ingestion in pediatric age Digestive and liver disease, 2024.PMID 37985250
- [7]Mantegazza, Christian Foreign body ingestion in children: Definition of a nomogram to predict surgical or endoscopic intervention Digestive and liver disease, 2024.PMID 37586909
- [8]Leinwand, Katherine Button Battery Ingestion in Children: A Paradigm for Management of Severe Pediatric Foreign Body Ingestions Gastrointestinal endoscopy clinics of North America, 2016.PMID 26616899
- [9]Park, Sarah J Button battery injury: An update Australian journal of general practice, 2022.PMID 35773156
- [10]Whelan, Rebecca Button battery versus stacked coin ingestion: A conundrum for radiographic diagnosis International journal of pediatric otorhinolaryngology, 2019.PMID 31404782
- [11]Gurevich, Yonah Foreign body ingestion in pediatric patients Current opinion in pediatrics, 2018.PMID 30036203
- [12]Eliason, Melvin J Button battery ingestion in children Current opinion in otolaryngology and head and neck surgery, 2017.PMID 28858893