Paeds · acute-care-resuscitation-and-toxicology
Opioid, sedative and recreational-drug toxicity
Also known as Paediatric opioid poisoning · Benzodiazepine and sedative overdose in children · Recreational drug toxicity in adolescents · Novel psychoactive substance toxicity · Naloxone and flumazenil in paediatric poisoning
A fellowship approach to the child or adolescent with opioid, sedative or recreational-drug toxicity: recognise the toxidrome from the bedside pattern, lead an ABCDE primary survey with oxygen, ventilation, glucose and access, titrate naloxone to effective ventilation rather than full wakefulness, reserve flumazenil for the narrow isolated-benzodiazepine case because it can precipitate seizures, manage sympathomimetic and serotonergic toxicity with benzodiazepines and cooling, correct ethanol-induced hypoglycaemia early, and call senior help and the Poisons Information Centre in parallel.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Opioid, sedative and recreational-drug toxicity is the harmful effect of a substance on the brainstem, the cardiovascular system or the body's temperature and metabolic balance, recognised first by the clinical pattern it produces and treated by supportive care plus a small number of antidotes. The child or adolescent arrives sedated, agitated, breathing slowly or racing, hot or cold, and your job in the first minute is to protect the airway, oxygenate, ventilate and find the pattern — not to identify the exact drug. [1] [2]
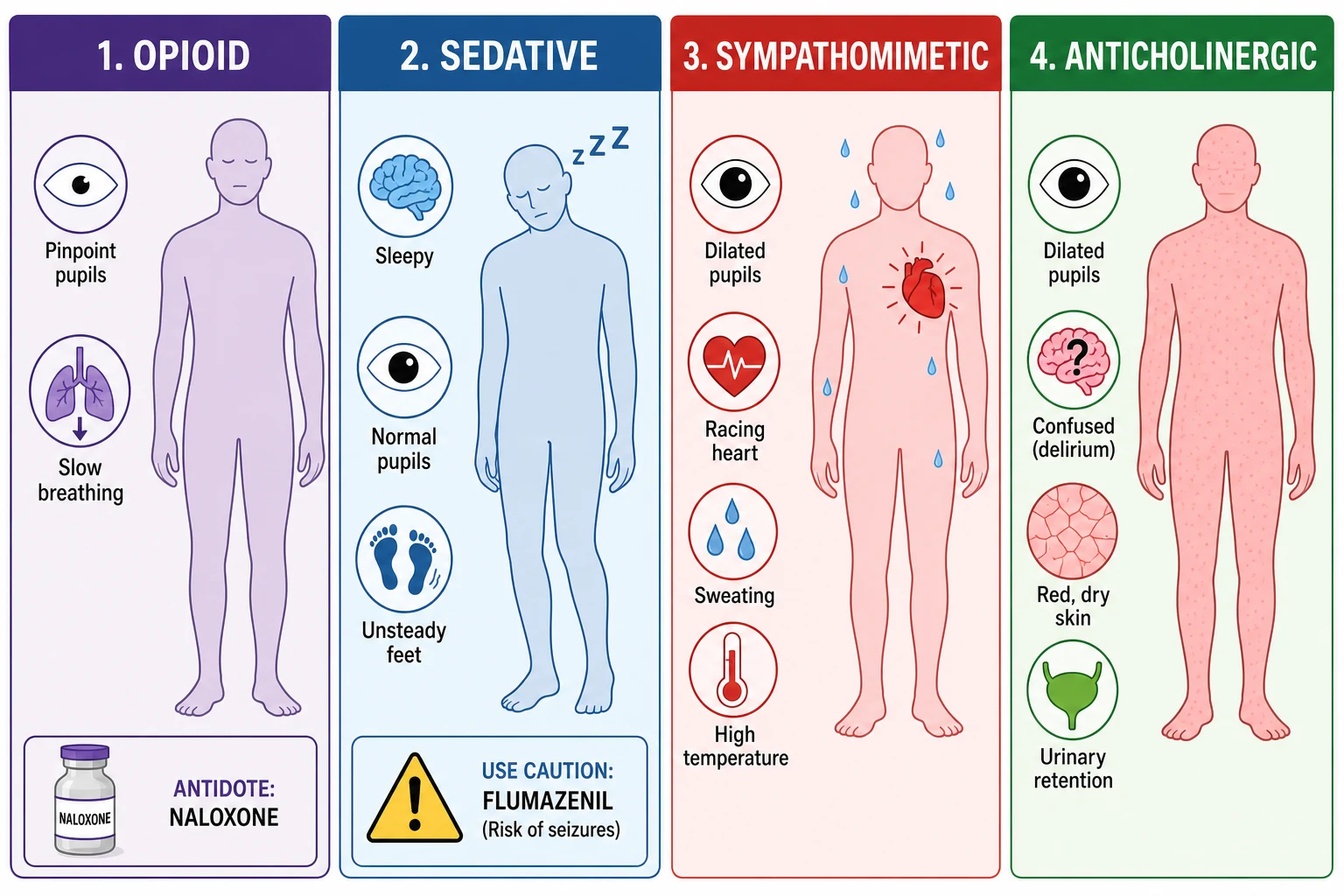
A toxidrome is a recognisable cluster of signs produced by a class of drug acting through a shared mechanism. Recognising the pattern is faster and more useful than waiting for a drug screen, and it points directly to the immediate treatment. The opioid pattern combines pinpoint pupils, slow shallow breathing and sedation. The sedative-hypnotic pattern combines sedation and ataxia with normal or near-normal pupils. The sympathomimetic pattern combines agitation, dilated pupils, a racing heart, high blood pressure and a hot sweaty body. The anticholinergic pattern adds dry, flushed skin and delirium to dilated pupils. [1]
Management is built around supportive care, because most poisoned children recover once the airway, breathing and circulation are held safe and the drug is metabolised. Naloxone reverses opioid respiratory depression but must be titrated to effective ventilation rather than full consciousness, both to avoid precipitating acute withdrawal and because the goal is to keep the child breathing safely. Flumazenil reverses benzodiazepines but is not routine, because it can precipitate seizures in exactly the patients who present with mixed or chronic use. Sympathomimetic and serotonergic toxicity is treated with benzodiazepines, cooling and fluids, with cyproheptadine considered for severe serotonin syndrome. [2] [8]
Classification
The single most useful classification is by toxidrome, because it converts a guessing game about the drug into a decision about the next action. Look at the pupils, the mental state, the vital signs and the skin, and the pattern emerges within a minute. [1]
Opioid
Mu-receptor agonism
- Pinpoint pupils (miosis), often less than 2 mm
- Slow, shallow breathing with sedation
- May be hypothermic and hypotensive at high doses
- Antidote: naloxone titrated to effective ventilation
Sedative-hypnotic
GABA-A enhancement
- Sedation, slurred speech and ataxia with near-normal pupils
- Respiratory depression possible but usually milder than opioid
- Benzodiazepines, ethanol, barbiturates, z-drugs
- Antidote: supportive care; flumazenil only in narrow isolated case, seizure caution
Sympathomimetic
Catecholamine surge
- Agitation, dilated pupils, tachycardia and hypertension
- Hot, sweaty skin with hyperthermia in severe cases
- MDMA, cocaine, amphetamine, pseudoephedrine
- Treatment: benzodiazepines first line, cooling and fluids; avoid beta-blocker monotherapy
Anticholinergic
Muscarinic blockade
- Dry, hot, flushed skin with dilated pupils
- Delirium, urinary retention and reduced bowel sounds
- Antihistamines, atropine, tricyclics in part
- Treatment: supportive; benzodiazepines for agitation; physostigmine in specialist units
Classification by intention and age frames the two peaks of paediatric toxicity. The toddler peak is exploratory ingestion of a caregiver's medication — an opioid, a benzodiazepine, an antihypertensive — found with a medicine bottle on the floor. The adolescent peak is intentional or recreational use of ethanol, MDMA, cocaine, benzodiazepines, ketamine, GHB or a novel psychoactive substance, often with co-ingestion and uncertainty about the dose. Both need the same ABCDE structure, but the differential, the doses, the safeguarding assessment and the disposition differ. [1] [3]
Epidemiology & Risk Factors
Poisoning is among the most common reasons a previously well child or adolescent presents acutely unwell. In young children the driver is access to medications and household substances in the home. In adolescents the driver is experimentation, intentional self-harm, and the recreational use of ethanol and a widening range of substances including opioids, benzodiazepines, MDMA, cocaine, ketamine, GHB and novel psychoactive substances. [1] [3]
Young child factors
- Exploratory ingestion of a caregiver's medication
- Opioids, benzodiazepines, ethanol and household products within reach
- Small body mass magnifies the dose per kilogram
- Ethanol causes profound hypoglycaemia in the young child
Adolescent factors
- Intentional use or self-harm; recreational experimentation
- Co-ingestion of ethanol, opioids, benzodiazepines, MDMA
- Fentanyl and analogues raise the risk of severe opioid toxicity
- Novel psychoactive substances add diagnostic uncertainty
System factors
- Rural or remote location with retrieval delay
- Limited access to the medication history and the scene
- After-hours or single-handed cover
- Communication, language and confidentiality barriers in the adolescent
Risk is magnified by opioid tolerance and its absence. An opioid-tolerant adolescent may carry a large dose without respiratory depression, while an opioid-naive toddler taking a single sustained-release tablet of a caregiver's opioid can arrest within the hour. The arrival of fentanyl and its analogues has raised the stakes, because these agents are potent, may require higher or repeated naloxone doses, and can recur as the opioid outlasts the antidote. Novel psychoactive substances complicate recognition, because they mimic and blur the classic toxidromes and escape standard drug screens. [2] [11]
Pathophysiology
Toxicity follows from the receptor the drug binds. Three mechanisms dominate the recreational and sedative picture, and each maps onto a toxidrome and its signature threat. [1] [2]
Opioids bind mu-receptors in the medullary respiratory centre, slowing the respiratory rate and the tidal volume until ventilation is inadequate. Pupillary constriction is the tell-tale sign, driven by mu-receptors in the Edinger-Westphal nucleus. The dominant threat is hypoxia from respiratory depression, and the antidote naloxone competes at the receptor to restore the drive to breathe. Sedative-hypnotics enhance GABA-A signalling, the brain's main inhibitory pathway, producing sedation, ataxia and at higher doses respiratory depression. Benzodiazepines act here, which is why flumazenil can reverse them, but also why removing GABA-mediated inhibition in a dependent or co-ingested brain can release seizures. [2] [8]
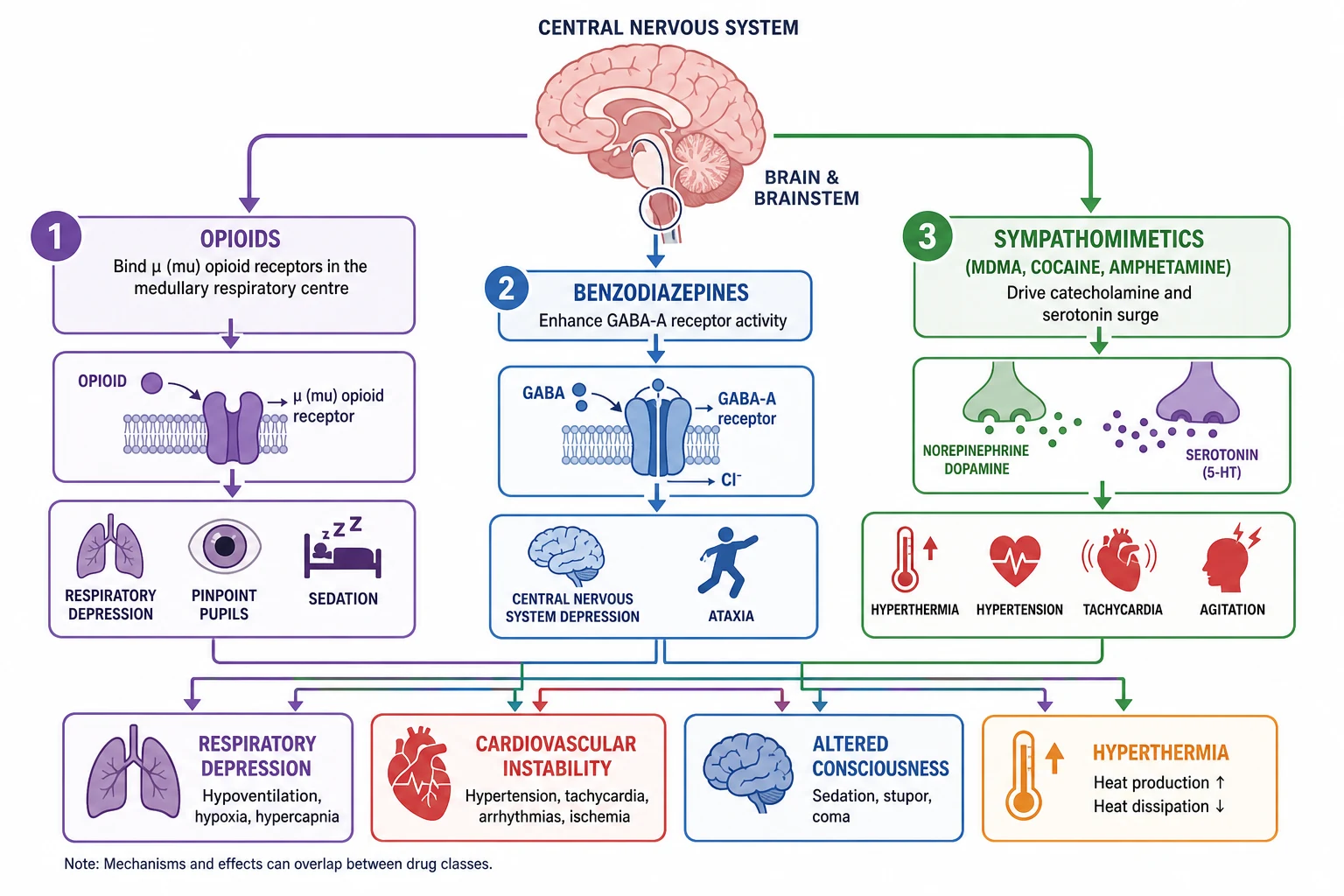
Sympathomimetics drive a catecholamine and serotonin surge. MDMA, cocaine and amphetamine release noradrenaline, dopamine and serotonin, producing agitation, tachycardia, hypertension, mydriasis and hyperthermia. MDMA is distinctive because it can also cause profound hyponatraemia through a combination of excess water intake and inappropriate antidiuretic hormone release, and because its serotonergic effect can tip the child into serotonin syndrome with rigidity, clonus and hyperthermia. Cocaine adds direct cardiovascular toxicity through coronary vasospasm and sodium-channel effects, which is why chest pain and arrhythmia are part of its presentation. [10] [12]
Ethanol causes the specific danger of hypoglycaemia in young children by suppressing hepatic gluconeogenesis while glycogen stores are small. A toddler who has ingested ethanol can become profoundly hypoglycaemic, and the low glucose worsens the cerebral depression. GHB produces a distinctive pattern of rapid deep coma with rapid spontaneous recovery as it is cleared, while ketamine produces a dissociative state with nystagmus, hypersalivation and a sympathomimetic tinge. Novel psychoactive substances, including synthetic cannabinoids, blur these patterns and can produce severe agitation, seizures and even acute kidney injury. [10] [11]
Clinical Presentation
Begin with the first impression and a hands-on primary survey, then convert what you see into a toxidrome rather than a drug name. State what you see objectively: "This adolescent is agitated, hot and sweaty with dilated pupils and a heart rate of 140 — that is a sympathomimetic picture." [1]
The opioid toxidrome combines pinpoint pupils, a slow respiratory rate with shallow breaths, and reduced conscious level. The child is cool and sedated, and the threat is hypoxic respiratory arrest. The sedative-hypnotic toxidrome combines sedation, slurred speech and ataxia with pupils that are normal or only slightly small; respiratory depression may be present but is usually milder than in opioid toxicity. The sympathomimetic toxidrome is the mirror image: agitation, dilated pupils, tachycardia, hypertension, diaphoresis and hyperthermia. The anticholinergic toxidrome adds dry, flushed skin, urinary retention and a confused, delirious mental state. [1] [10]
[1]Specific agents colour the pattern. MDMA presents with agitation, tachycardia and hyperthermia, and can progress to muscle rigidity, clonus and confusion signalling serotonin syndrome, or to collapse from hyponatraemia or a cardiac arrhythmia. Cocaine and amphetamine present with hypertension, tachycardia and chest pain, and can produce seizures and stroke. Ethanol in a young child presents with ataxia, sedation and the danger of hypoglycaemia; the child may be cold and clammy rather than warm. GHB presents as rapid deep coma, often with bradycardia and hypothermia, then rapid recovery over hours. Ketamine presents with a dissociative state, nystagmus and hypersalivation. Synthetic cannabinoids can produce severe agitation, seizures and vomiting. [10] [11]
Differential Diagnosis
A toxic cause is one explanation for an altered or collapsed child, and the resuscitation does not wait for certainty. Build the differential in a fixed order: what can kill now, what is most likely, what is reversible, and what is most harmful to miss. [1]
Metabolic and brain
- Hypoglycaemia from ethanol, beta-blocker or metabolic disease
- Hypoxia from any respiratory depressant or a primary respiratory cause
- Post-ictal state after an unrecognised seizure
- Meningoencephalitis or sepsis with altered conscious state
Toxic mimics
- Carbon monoxide poisoning in a drowsy household member
- Serotonin syndrome or neuroleptic malignant syndrome
- Anticholinergic or cholinergic poisoning
- Opioid plus benzodiazepine co-ingestion blurring the pupils
Traumatic and psychiatric
- Traumatic brain injury from collapse or assault
- Intracranial haemorrhage presenting as reduced conscious level
- Primary psychiatric presentation in the adolescent
- Functional or dissociative states overlapping with ketamine or GHB
The decisive point is that hypoglycaemia, hypoxia and a structural brain problem are missed only if you do not look for them. Check bedside glucose at the bedside in every suspected intoxication, because ethanol and beta-blocker overdose drop it fast and the low glucose is corrected in seconds with intravenous dextrose. Examine the pupils for asymmetry and the head for signs of injury. Keep sepsis and meningoencephalitis open when the child is febrile and drowsy, because fever can coexist with or mimic a sympathomimetic toxidrome. [1]
Clinical & Bedside Assessment
Run the ABCDE primary survey adapted to the poisoned child, then reassess after each intervention. The airway and breathing are the foreground, because respiratory depression is the common pathway to death in opioid and sedative toxicity. [1] [2]
Open and protect the airway, give high-flow oxygen to any child with respiratory depression or hypoxia, and ventilate with a bag and mask if breathing is inadequate. Check the bedside glucose at the bedside: a low reading is treated immediately with intravenous dextrose before any further assessment. Establish intravenous or intraosseous access. Assess the circulation for heart rate, blood pressure, capillary refill and temperature. Measure the temperature, because hyperthermia in MDMA or cocaine toxicity is an emergency that demands active cooling. Only then perform the focused toxicological examination. [1]
[1]The focused examination targets the toxidrome. Look at the pupils for size and reactivity, the mental state, the muscle tone and reflexes for rigidity or clonus, the mucous membranes and skin for dryness, sweating and temperature, the bowel sounds, and the bladder for retention. Take a collateral history from caregivers, friends or the ambulance crew: what was found at the scene, what bottles or paraphernalia were present, the timing, any access to medications in the home, and any recreational or intentional use. In the adolescent, take a brief, non-judgemental history that respects confidentiality while securing safety. Use a professional interpreter whenever needed. [1] [3]
The reassessment after each intervention is the examination that matters most. After naloxone, ask whether the respiratory rate and depth have improved and the child is breathing effectively, not whether they are fully awake. After benzodiazepines for a sympathomimetic picture, ask whether the agitation and the heart rate are settling and the temperature is falling. State the change you expected, and compare it with what actually happened. [2] [5]
Investigations
Stabilise first, then order each test for a named question. In suspected drug toxicity the immediate tests identify the reversible threats and the co-ingestants that change management, rather than naming the recreational drug. [1]
Immediate and bedside
- Bedside glucose in every case to catch ethanol or beta-blocker hypoglycaemia
- Blood gas to quantify ventilation, oxygenation and acid-base
- Temperature and a full set of vital signs including conscious level
- Electrocardiogram in the unknown or mixed overdose to screen for sodium-channel blockade
Core laboratory
- Paracetamol and salicylate levels in every intentional or unknown ingestion
- Electrolytes including sodium, renal function, creatine kinase and hepatic panel
- Ethanol level where it changes the management of a young child
- Beta-human chorionic gonadotropin in adolescent females
Targeted and supportive
- Quantitative drug levels only when they change management
- Chest imaging if aspiration or pulmonary oedema is suspected
- Computed tomography of the head if trauma or a structural lesion is possible
- Cultures if sepsis or meningoencephalitis remains on the differential
Interpret the tests as physiology and threat, not as a drug label. A low glucose is acted on in seconds. A metabolic acidosis with a large anion gap raises toxic alcohol or salicylate poisoning. A raised creatine kinase in MDMA toxicity signals rhabdomyolysis and drives fluid management to protect the kidney. A low sodium in an MDMA user points to water intoxication or inappropriate antidiuretic hormone and constrains fluid choice. The electrocardiogram in the unknown overdose screens for the widened QRS of sodium-channel blockade, which would redirect management toward sodium bicarbonate. [1] [10]
[1]Management — Resuscitation
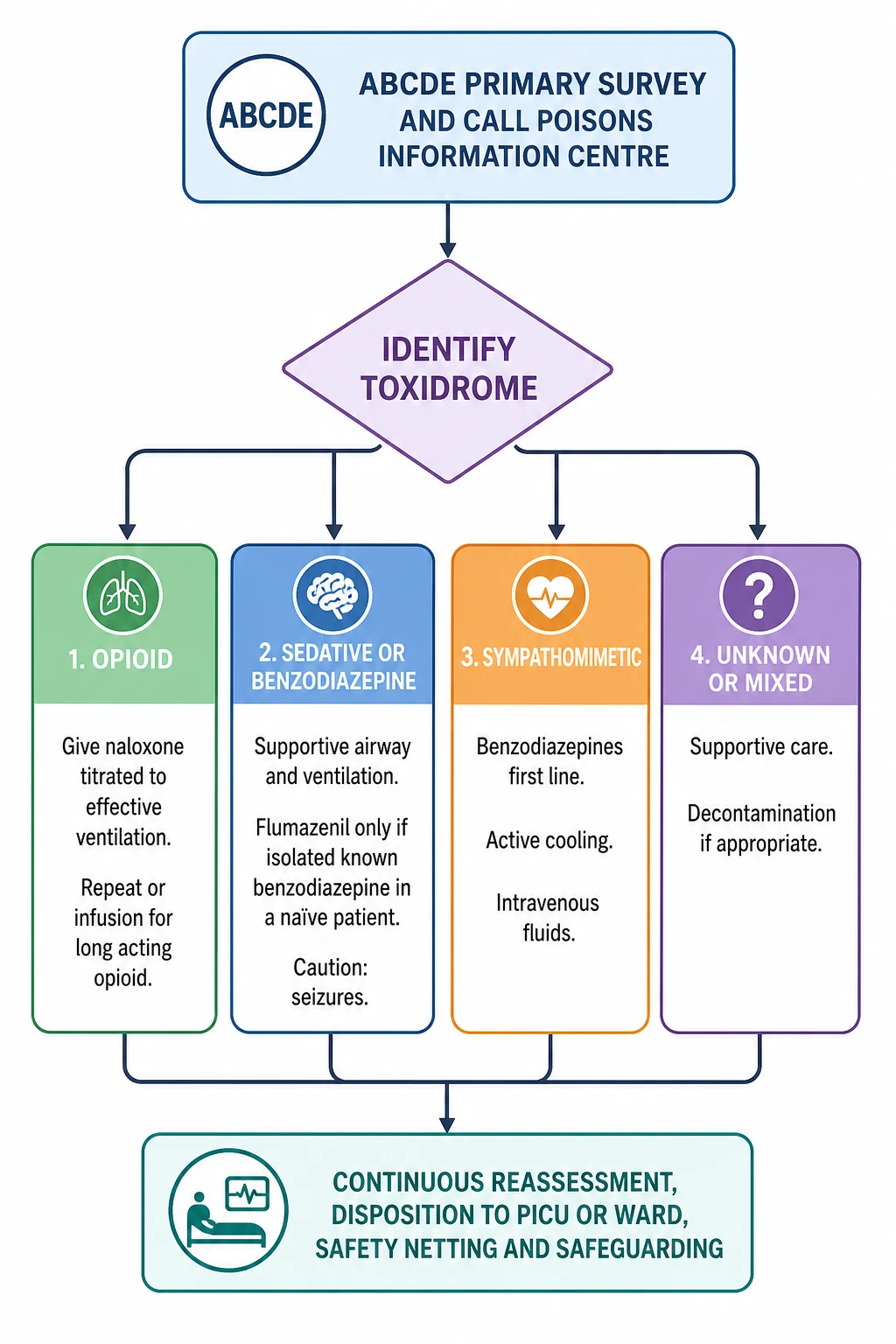
Resuscitation follows a fixed order: ABCDE primary survey, high-flow oxygen, bag-mask ventilation for apnoea, bedside glucose, intravenous access, a call for senior help and the Poisons Information Centre, and the targeted antidote or supportive care. Each element runs in parallel, and each action is followed by reassessment. [1] [2]
The first minutes in drug toxicity
Primary survey and call for help
Run the ABCDE survey; declare the concern; call the senior paediatric and resuscitation teams and the Poisons Information Centre; name a leader and allocate roles; bring age- and weight-appropriate equipment and monitoring.
Protect the airway and oxygenate
Open and protect the airway; give high-flow oxygen to any child with respiratory depression or hypoxia; ventilate with bag and mask if breathing is inadequate; prepare for a definitive airway in the deeply comatose child.
Check bedside glucose and establish access
Check glucose at the bedside and treat a low reading immediately with intravenous dextrose; gain intravenous or intraosseous access; send the core bloods including paracetamol and salicylate levels in the intentional ingestion.
Identify the toxidrome
From the pupils, mental state, vital signs and skin, name the opioid, sedative, sympathomimetic, anticholinergic or unknown pattern, and direct the targeted treatment.
Give the targeted antidote or supportive care
Naloxone for opioid respiratory depression titrated to effective ventilation; supportive airway and ventilation for the sedated child; benzodiazepines, cooling and fluids for sympathomimetic toxicity.
Reassess from the top
After every action return to airway, breathing, circulation, glucose and conscious level; judge the trend against the response you predicted; revise the plan.
Airway and breathing
The airway and breathing are the priority because respiratory depression is the common pathway to death in opioid and sedative toxicity. Open and protect the airway, give high-flow oxygen, and ventilate with bag and mask if breathing is inadequate. In the deeply comatose child or the one with an unprotected airway, prepare for a definitive airway and call for senior or intensive-care help early. Do not wait for an antidote to protect the airway; ventilation comes first. [1] [2]
Naloxone for opioid toxicity
Naloxone reverses opioid respiratory depression by competing at the mu-receptor. The principle that protects the child is to titrate naloxone to effective ventilation, not to full wakefulness. Reversing too far precipitates acute opioid withdrawal, agitation, vomiting and aspiration, and in rare cases pulmonary oedema, while the goal is simply to restore adequate breathing. [2] [5]
Naloxone — opioid respiratory depression
An initial naloxone dose of 10 micrograms per kilogram by the intravenous, intraosseous or intramuscular route is reasonable, repeated every two to three minutes until ventilation is effective. In the apnoeic or severely depressed child, where the priority is rapid reversal, a larger dose of up to 100 micrograms per kilogram per dose is used, to a maximum of 2 mg per dose. Intranasal naloxone is an alternative route with rapid systemic uptake in children, and a pilot randomised trial found intranasal administration feasible in paediatric opioid poisoning, though intravenous remains the fastest route when access is established. [4] [6]
Intranasal vs intravenous naloxone in paediatric opioid poisoning
Drug and Alcohol Dependence
Pilot randomised feasibility clinical trial in children with opioid poisoning
Key finding
Intranasal naloxone was feasible and acceptable in paediatric opioid poisoning, supporting the intranasal route where intravenous access is delayed.
Practice change
Intranasal naloxone is a practical first or alternative route in children, especially when intravenous access is difficult; titrate to effective ventilation and arrange monitoring for recurrence.
Naloxone has a short half-life of roughly 60 to 90 minutes, shorter than most opioids. A child who responds to a bolus can slip back into respiratory depression as the naloxone wears off, and this recurrence is the rule rather than the exception with long-acting agents such as methadone, sustained-release morphine or oxycodone, and fentanyl and its analogues. After the effective bolus dose is found, start a naloxone infusion at about two-thirds of that effective dose per hour, titrated to keep ventilation adequate, and observe the child for long enough to cover the duration of action of the opioid. [2] [5]
Flumazenil: the caution
Flumazenil reverses benzodiazepines at the GABA-A receptor, but it is not a routine reversal agent in the poisoned child. Removing GABA-mediated inhibition in a benzodiazepine-dependent patient, in a mixed overdose, or where a proconvulsant such as a tricyclic antidepressant has been co-ingested can precipitate seizures that are difficult to control. Paediatric case reports document seizure after flumazenil administration, and the standard teaching is to prefer supportive airway and ventilatory care over reversal. [7] [8]
[8] [9]The narrow circumstance in which flumazenil is considered is the isolated, known benzodiazepine ingestion in a benzodiazepine-naive patient with significant respiratory depression where airway and ventilation cannot be maintained, or the reversal of iatrogenic oversedation during procedural sedation. Even then, give it in small titrated increments of 10 micrograms per kilogram intravenously to a maximum of 500 micrograms per dose, with resuscitation equipment and a plan for seizure management to hand. The default for the poisoned child with benzodiazepine toxicity remains supportive: protect the airway, oxygenate and ventilate. [7] [9]
Sympathomimetic and serotonergic toxicity
Sympathomimetic toxicity from MDMA, cocaine or amphetamine is treated with benzodiazepines as first-line therapy, active cooling and intravenous fluids. Benzodiazepines calm the agitation, reduce the muscle activity that generates heat, lower the heart rate and blood pressure, and treat the serotonergic component. Use adequate titrated doses of a benzodiazepine such as diazepam or lorazepam. Cool the hyperthermic child actively with evaporative cooling, ice packs or cooled intravenous fluids, and treat the rhabdomyolysis with intravenous fluids to protect the kidney. [10] [12]
Benzodiazepine — sympathomimetic or serotonergic toxicity
Where MDMA or another serotonergic agent has produced serotonin syndrome with the triad of neuromuscular hyperexcitability (clonus, rigidity, hyperreflexia), autonomic instability and altered mental state, escalate the benzodiazepine dose, cool actively, and consider cyproheptadine in consultation with a toxicologist. Avoid beta-blocker monotherapy in cocaine and amphetamine toxicity, because blocking beta-2 vasodilation leaves unopposed alpha vasoconstriction and can paradoxically worsen hypertension. Severe refractory hypertension is treated with a direct vasodilator such as phentolamine, and chest pain from cocaine is managed as an acute coronary syndrome with aspirin, nitrates and benzodiazepines. [12]
Ethanol, GHB, ketamine and unknown agents
Ethanol intoxication in the young child carries the specific threat of hypoglycaemia. Check glucose at the bedside and treat a low reading immediately with intravenous dextrose, then sustain with a glucose-containing fluid and recheck, because the hypoglycaemia can recur. GHB and its precursors produce a rapid deep coma, often with bradycardia and hypothermia, and typically recover spontaneously over a few hours; management is supportive, protecting the airway and watching for the recovery. Ketamine produces a dissociative state with nystagmus and hypersalivation that settles with supportive care, benzodiazepines for distress, and attention to the airway. For the unknown or novel psychoactive substance, manage the toxidrome in front of you, secure the airway and circulation, and call the Poisons Information Centre and a toxicologist for specific guidance. [10] [11]
Management — Definitive & Stepwise
Once the first minutes are safe, definitive care moves to ongoing monitoring, sustained antidote therapy where needed, correction of metabolic and electrolyte disturbance, temperature control, and the clarification of the agent and the intent. This phase runs hour by hour with the trend, and the disposition follows the response. [1] [3]
Ongoing monitoring and sustained antidote therapy
Continue monitoring the airway, breathing, circulation, oxygen saturation, conscious level and temperature. For opioid toxicity from a long-acting agent, run a naloxone infusion and observe long enough to cover the duration of action of the opioid; for sustained-release preparations and methadone this is many hours. Reassess the adequacy of ventilation repeatedly, and titrate the infusion to keep the child breathing safely rather than fully awake. [2] [5]
Metabolic, electrolyte and temperature control
Correct the metabolic and electrolyte consequences. Treat MDMA hyponatraemia with fluid restriction and, in severe cases with seizures, hypertonic saline per local protocol. Treat rhabdomyolysis with adequate intravenous fluids to maintain urine output and protect the kidney. Drive the temperature down actively in severe hyperthermia, because sustained high temperature causes harm rapidly. Correct ethanol hypoglycaemia with dextrose and recheck. [10] [12]
Goals and disposition
Set explicit recovery endpoints and watch the trend toward them: a safe airway, effective ventilation, a normalising temperature, settling agitation, a normal glucose and electrolyte profile, and a protected kidney. A child who has required naloxone for a long-acting opioid is observed for many hours because of the risk of recurrence. A child with MDMA toxicity and rhabdomyolysis is observed until the creatine kinase trend is reassuring and the kidney function is stable. Asymptomatic children with accidental ingestions are observed for the relevant window — around four to six hours for most agents, longer for sustained-release preparations — before discharge with safety-netting. [1] [3]
Specific Subtypes & Scenarios
The structure stays the same, but age, agent, tolerance and setting change what you watch for, which antidote you reach for, and how early you escalate. [1]
Toddler exploratory ingestion
- Caregiver's opioid or benzodiazepine within reach
- Weight-based naloxone titrated to ventilation
- Check glucose early; ethanol drops it fast
- Poison-prevention counselling and safeguarding before discharge
Adolescent recreational use
- MDMA, cocaine, ethanol, ketamine, GHB or novel substances
- Frequent co-ingestion; consider paracetamol and salicylate levels
- Fentanyl and analogues may need higher or repeated naloxone
- Confidential, non-judgemental history with a safety plan and follow-up
Long-acting opioid
- Methadone, sustained-release morphine or oxycodone, fentanyl analogues
- Recurrence as naloxone wears off is the rule
- Start a naloxone infusion after the effective bolus is found
- Observe for many hours; consider intensive care
Unknown or novel agent
- Synthetic cannabinoids and novel psychoactive substances blur toxidromes
- Standard drug screens are unreliable
- Manage the pattern and call the Poisons Information Centre
- Escalate to a toxicologist and intensive care if unstable
In the toddler with exploratory ingestion, the dose per kilogram is magnified by the small body mass, and a single sustained-release opioid tablet can be lethal. The adolescent with intentional or recreational use often presents with co-ingestion and uncertainty about the dose; screen for paracetamol and salicylate regardless of the stated history, because these co-ingestions change the management and the prognosis. Fentanyl and its analogues may require higher or repeated naloxone doses, and the recurrence after a bolus is common enough that an infusion and prolonged observation are the safer default. [2] [11]
Complications & Pitfalls
Most preventable harm in paediatric drug toxicity comes from a small number of errors: giving flumazenil routinely, reversing naloxone to full wakefulness, missing hypoglycaemia, using a beta-blocker alone for cocaine, or neglecting the recurrence of a long-acting opioid. Each is a failure of the principle rather than a failure of knowledge. [1] [8]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Giving flumazenil routinely in the poisoned child | Seizures in chronic users, mixed or unknown overdoses and co-ingested proconvulsants | Reserve for isolated known benzodiazepine in a naive patient; prefer supportive airway and ventilation |
| Reversing naloxone to full wakefulness | Acute withdrawal, vomiting, aspiration, pulmonary oedema | Titrate to effective ventilation; start an infusion for long-acting opioids |
| Missing ethanol or beta-blocker hypoglycaemia | Cerebral depression worsens and the reversible cause is untreated | Check bedside glucose in every suspected intoxication; treat a low reading immediately |
| Beta-blocker monotherapy for cocaine | Unopposed alpha vasoconstriction worsens hypertension | Benzodiazepines first line; phentolamine for refractory hypertension |
| Neglecting a long-acting opioid | Recurrence of respiratory depression after the naloxone wears off | Observe long enough; start an infusion for methadone, sustained-release or fentanyl analogues |
| Attributing coma to a drug alone | Hypoglycaemia, hypoxia, head injury, sepsis and intracranial bleed are missed | Check glucose, oxygenation and the pupils; consider computed tomography and cultures |
| Forgetting co-ingestion in the adolescent | Paracetamol or salicylate overdose is missed and the window for antidote closes | Send paracetamol and salicylate levels in every intentional or unknown ingestion |
| Late escalation and retrieval | Support is unavailable when the child collapses again | Call senior, intensive care, retrieval and the Poisons Information Centre early |
After resuscitation, watch actively for harm from the toxicity itself and from its treatment: aspiration from reduced conscious level, pulmonary oedema from opioid over-reversal, rhabdomyolysis-induced kidney injury in MDMA toxicity, hyponatraemic seizures, serotonin syndrome, and the seizure that follows an ill-judged dose of flumazenil. The child who survives the first hour still needs meticulous ongoing care, and a new sign can mark a complication as readily as a relapse. [9] [10]
[1] [8]Prognosis & Disposition
Disposition follows the agent, the trend and the observation window, not a single reassuring reading. Consider the duration of action of the substance, the co-ingestants, the response to treatment, the local resources, the transport risk, and the social and mental-health context. [1] [3]
Intensive care or retrieval
- Airway compromise or the need for ventilation
- Naloxone infusion for a long-acting opioid or fentanyl analogue
- Severe hyperthermia, serotonin syndrome or uncontrolled seizures
- Haemodynamic instability or a widened QRS on the ECG
High-dependency or ward observation
- Symptomatic but stabilised child needing close monitoring
- Observation window for the agent not yet elapsed
- Reversal of opioid toxicity with recurrence risk
- Ongoing benzodiazepine and fluid management for sympathomimetic toxicity
Observation and discharge
- Asymptomatic after the relevant observation window
- No co-ingestant requiring a longer window
- Glucose, vital signs and conscious level normal
- Safety-net, poison-prevention advice, mental-health and social follow-up arranged
Outcome is generally good for children who receive prompt supportive care, because most agents are metabolised once the airway, breathing and circulation are held safe. The children who do worst are those with delayed airway protection, missed hypoglycaemia, severe hyperthermia from MDMA, cardiovascular instability from cocaine, or the rare but severe presentations of novel psychoactive substances. Survivors of an intentional or recreational presentation need a mental-health and social assessment before discharge, with a safety plan, harm-reduction advice, and clear follow-up, because the index event is a marker of ongoing risk. [1] [3]
Special Populations
Adapt how you assess, dose and escalate, but never lower the standard for recognising a toxidrome. The principles apply across ages and abilities; the differences are in tolerance, communication, drug handling and the social context. [1]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Toddler with exploratory ingestion | Weight-based naloxone; check glucose early; poison-prevention counselling and safeguarding | State the safe observation window for the specific agent |
| Opioid-tolerant adolescent | Balance reversal of life-threatening respiratory depression against precipitated withdrawal | Titrate to ventilation, not full wakefulness |
| Adolescent intentional or recreational use | Confidential, non-judgemental history; screen for paracetamol and salicylate; mental-health and social assessment | Safety plan and follow-up before discharge |
| Disability or neurodiversity | Use the caregiver's baseline for mental-state assessment; adapted communication | A changed baseline is the key sign |
| Indigenous, migrant or refugee | Use professional interpreters; respect cultural and family structures; address access barriers | Apply local consent, confidentiality and mandatory-reporting rules |
| Technology-dependent child | Assess child and device; consider the medication and the device as sources | The device may be both the source and the rescue |
Safeguarding runs in parallel with medical care, and immediate stabilisation comes first. An ingestion in a young child may reflect unsafe medication storage, neglect, or in rare cases an unsafe home environment, while an adolescent presentation may signal self-harm, exploitation or risk that needs a careful psychosocial assessment. Ask only necessary open, non-leading questions, document objective findings and spontaneous words, and use the local safeguarding and mental-health pathway. Reporting thresholds, consent rules and confidentiality provisions differ by Australian state or territory, UK nation, US state and Canadian province or territory. [1]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The structure of management — ABCDE primary survey, oxygen and ventilation, bedside glucose, access, the call to the Poisons Information Centre, and the targeted antidote — is consensus across the major paediatric and toxicology sources. The two areas of active evidence are the route and dose of naloxone and the role of flumazenil, and both refine rather than replace the supportive-care backbone. [1] [2]
Route and dose of naloxone for opioid reversal
Cureus (systematic review)
Systematic literature review of the optimal initial dose and route of naloxone for successful opioid reversal
Key finding
Both intranasal and intravenous naloxone successfully reverse opioid toxicity; the intravenous route is fastest when access is established, while intranasal administration is effective where access is delayed.
Practice change
Use the route that is fastest and safest in the child in front of you, and titrate to effective ventilation; arrange observation for recurrence, particularly after long-acting opioids.
On flumazenil, the evidence and the consensus are clear: it is not a routine reversal agent in the poisoned patient. Case reports and clinical experience show that seizures after flumazenil occur in exactly the children most often brought to the emergency department — chronic benzodiazepine users, mixed overdoses and co-ingestions with proconvulsants. The standard teaching is supportive airway and ventilatory care, with flumazenil reserved for the narrow case of an isolated, known benzodiazepine ingestion in a benzodiazepine-naive patient or for iatrogenic reversal. [7] [9]
On novel psychoactive substances, the evidence is sobering: synthetic cannabinoids and other novel agents produce severe toxicity that blurs the classic toxidromes and escapes standard drug screens, and management is predominantly supportive, with escalation to a toxicologist. The recreational landscape shifts faster than the testing does, which is why the toxidrome and the physiology, rather than the drug name, drive the first hour. [10] [11]
Jurisdictional implementation
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne clinical guidelines drive local implementation of poisoning management. The NSW Poisons Information Centre on 13 11 26 (0800 764 766 in New Zealand) gives 24-hour specialist advice and should be called early. ANZCOR Guideline 12.2 governs paediatric advanced life support. Drug availability, naloxone product strength, mental-health services and mandatory reporting remain state-, territory- or service-specific. In Aotearoa New Zealand, verify the active local poisons, retrieval and safeguarding pathways rather than borrowing an Australian threshold.
Exam Pearls
Recognition
- Recognise the toxidrome from the pattern, not the bottle
- Opioid: pinpoint pupils, slow shallow breathing, sedation
- Sedative: sedation and ataxia with near-normal pupils
- Sympathomimetic: agitation, mydriasis, tachycardia, hypertension, hyperthermia
- Anticholinergic: dry flushed skin, delirium, mydriasis
First minutes
- ABCDE, oxygen, ventilation, bedside glucose, access
- Call senior help and the Poisons Information Centre in parallel
- Identify the toxidrome; give the targeted antidote
- ECG in the unknown or mixed overdose
Naloxone
- Titrate to effective ventilation, not full wakefulness
- Initial 10 micrograms per kg, repeated; up to 100 micrograms per kg (max 2 milligrams) for apnoea
- Intranasal is a feasible alternative route in children
- Start an infusion for long-acting opioids and observe for recurrence
Flumazenil
- Not routine in the poisoned child — can precipitate seizures
- Contraindicated in chronic use, mixed or unknown overdose, proconvulsant co-ingestion, seizure disorder
- Reserve for isolated known benzodiazepine in a naive patient or iatrogenic reversal
- Default is supportive airway and ventilation
Sympathomimetic
- Benzodiazepines first line, cooling and fluids
- Avoid beta-blocker monotherapy in cocaine (unopposed alpha)
- Phentolamine for refractory hypertension; treat chest pain as ACS
- Cyproheptadine for severe serotonin syndrome with toxicology input
Pitfalls
- No routine flumazenil
- No naloxone to full wakefulness
- No missed bedside glucose
- No beta-blocker alone for cocaine
- No neglect of a long-acting opioid recurrence
“Recognise the toxidrome → ABCDE, oxygen, ventilation, glucose, access, call for help and the Poisons Information Centre → naloxone titrated to effective ventilation for opioid toxicity, infusion for long-acting agents → supportive airway and ventilation for the sedated child with flumazenil reserved for the narrow isolated case → benzodiazepines, cooling and fluids for sympathomimetic toxicity → correct ethanol hypoglycaemia → reassess, observe for the relevant window, and arrange safeguarding and mental-health follow-up.”
Viva: why titrate naloxone to ventilation, not wakefulness?
The goal of naloxone is to restore effective ventilation and prevent hypoxic death, not to make the child fully alert. Naloxone has a half-life of roughly 60 to 90 minutes, shorter than most opioids, and over-reversal precipitates acute opioid withdrawal with agitation, vomiting and aspiration, and in rare cases pulmonary oedema. A child reversed to wakefulness may also refuse further observation and slip back into respiratory depression as the naloxone wears off. Titrate in small increments until ventilation is adequate, then observe and, for a long-acting opioid, start an infusion.
Viva: when is flumazenil appropriate, and when is it dangerous?
Flumazenil reverses benzodiazepines at the GABA-A receptor, but removing GABA-mediated inhibition can release seizures. It is dangerous in chronic benzodiazepine users, in mixed or unknown overdoses, where a proconvulsant such as a tricyclic antidepressant has been co-ingested, and in a patient with a known seizure disorder. It is appropriate only in the narrow case of an isolated, known benzodiazepine ingestion in a benzodiazepine-naive patient with significant respiratory depression that cannot be managed supportively, or for iatrogenic reversal of procedural sedation. The default for the poisoned child is supportive airway and ventilation.
Structured oral: an adolescent with MDMA toxicity and hyperthermia
Recognise the sympathomimetic or serotonergic pattern: agitation, tachycardia, hypertension, mydriasis and hyperthermia, with rigidity and clonus pointing to serotonin syndrome. Run the ABCDE survey, secure the airway and give oxygen, check bedside glucose, establish access, and call the senior team, a toxicologist and the Poisons Information Centre. Give titrated benzodiazepines first line to control agitation and reduce heat generation, cool actively with evaporative cooling and cooled fluids, give intravenous fluids to protect the kidney from rhabdomyolysis, correct a low sodium carefully, and consider cyproheptadine for severe serotonin syndrome. Avoid beta-blocker monotherapy. Escalate to intensive care if hyperthermia is uncontrolled, seizures occur or the circulation is unstable, and arrange a mental-health and social assessment once the child is safe.
References
- [1]Hoffman, Robert J Toxidromes and a general approach to poisoning Archives of disease in childhood, 2025.PMID 39978865
- [2]Boyer, Edward W Management of opioid analgesic overdose The New England journal of medicine, 2012.PMID 22784117
- [3]Ball, Allison Naloxone and Buprenorphine Treatment for Adolescent Opioid Overdose and Opioid Use Disorder: A Review JAMA pediatrics, 2026.PMID 41661628
- [4]Gholami, N A pilot randomized feasibility clinical trial of intranasal vs. intravenous naloxone in pediatric opioid poisoning Drug and alcohol dependence, 2026.PMID 42413284
- [5]Aziz, R The Optimal Initial Dose and Route of Naloxone Administration for Successful Opioid Reversal: A Systematic Literature Review Cureus, 2024.PMID 38380203
- [6]Malmros Olsson, E Rapid systemic uptake of naloxone after intranasal administration in children Paediatric anaesthesia, 2021.PMID 33687794
- [7]Segev, O Flumazenil in the Treatment of Benzodiazepine Toxicity: The Experience of a Large Urban Tertiary Care Hospital The Israel Medical Association journal : IMAJ, 2026.PMID 42298935
- [8]Kreshak, Angela A Flumazenil administration in poisoned pediatric patients Pediatric emergency care, 2012.PMID 22531190
- [9]McDuffee, Andrew T Seizure after flumazenil administration in a pediatric patient Pediatric emergency care, 1995.PMID 7651879
- [10]Levine, Mark New Designer Drugs Emergency medicine clinics of North America, 2021.PMID 34215409
- [11]Assi, Salem Profile, effects, and toxicity of novel psychoactive substances: A systematic review of quantitative studies Human psychopharmacology, 2017.PMID 28631432
- [12]Lucyk, Sarah N Acute Cardiovascular Toxicity of Cocaine The Canadian journal of cardiology, 2022.PMID 35697321