Paeds · acute-care-resuscitation-and-toxicology
Oxygen, high-flow and non-invasive respiratory support
Also known as High-flow nasal cannula · HFNC · Nasal CPAP in children · Non-invasive ventilation in children · BiPAP in paediatrics
A fellowship approach to oxygen and non-invasive respiratory support in children: choose the right device for the right problem, dose high-flow nasal cannula by weight, set CPAP and BiPAP pressures correctly, know what each mode does physiologically, recognise when support is failing, and escalate to intubation without delay.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A six-month-old infant arrives with bronchiolitis, grunting and retracting, saturating 89 per cent in room air. You start oxygen — but which oxygen? A simple nasal cannula might be enough, or it might be too little. High-flow might rescue the child and avoid intubation, or it might delay it dangerously if the child is already tiring. CPAP could splint collapsing alveoli, or BiPAP might be needed if the carbon dioxide is climbing. The decision turns on three questions: what does the gas exchange problem look like, what can each device actually do about it, and how do you know when it is working or failing? This page teaches the whole ladder. [1] [7]
This hub owns the device logic for paediatric oxygen and non-invasive support. Sister pages carry the disease algorithms: respiratory distress and failure for the assessment framework, bronchiolitis for the commonest indication, acute severe asthma for a disease where the approach differs, and paediatric acute respiratory distress syndrome for the severe end. [9]
Overview & Definition
Think of respiratory support not as a list of gadgets but as a toolkit that addresses two separate problems. The first is hypoxaemia — the blood is not getting enough oxygen because gas exchange is failing. The second is ventilatory failure — the lungs are not moving enough air to clear carbon dioxide. Every device on the ladder addresses one or both, and matching the device to the problem is the central skill. [6]
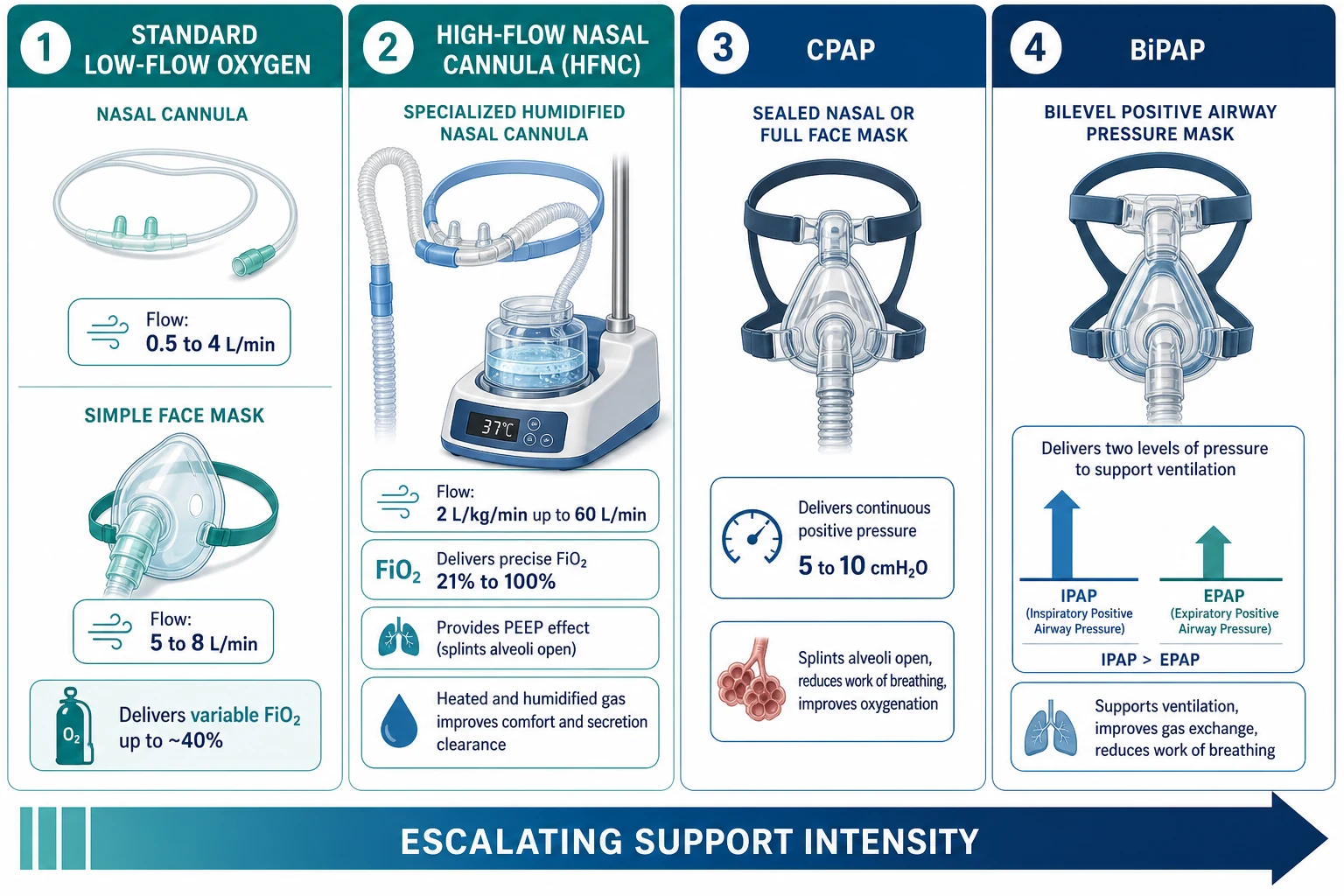
Standard oxygen therapy delivers oxygen-enriched gas through low-flow devices — nasal cannula or a simple face mask. It raises the fraction of inspired oxygen (FiO2) above the 21 per cent of room air, and in a child with normal ventilation this corrects mild hypoxaemia. But it delivers no pressure: it cannot splint collapsed alveoli, and it cannot reduce the work a tiring child expends with each breath. The FiO2 is also imprecise and varies with the child's inspiratory flow, mouth-breathing and leak. [10]
High-flow nasal cannula (HFNC) is the first step that does more than add oxygen. A specialised system delivers gas that is blended to a precise FiO2, heated to near body temperature (about 37 degrees), and fully humidified, at flows high enough to match or exceed a young child's own inspiratory demand — classically 2 L/kg/min, capped at about 60 L/min in older children. At those flows the device does four things at once: it washes CO2-rich gas out of the upper-airway dead space so each breath draws fresh gas, it meets inspiratory demand so the child's muscles do less work, it generates a modest positive end-expiratory pressure (PEEP) that splints the airways, and it delivers optimally conditioned gas that preserves mucociliary clearance. [5] [6]
Continuous positive airway pressure (CPAP) delivers a single, set positive pressure throughout the respiratory cycle via a sealed interface — a nasal mask, nasal prongs or a full face mask. Unlike HFNC, where PEEP is an incidental and variable by-product of flow, CPAP delivers a controlled, reliable distending pressure, typically 5 to 7 cmH2O in children. Its job is recruitment: it stents open alveoli that would otherwise collapse at end-expiration, raises functional residual capacity, reduces intrapulmonary shunt and so improves oxygenation. It is the tool of choice for hypoxaemic failure from recruitable lung disease. [9]
Bilevel positive airway pressure (BiPAP, or NIV) is CPAP plus a pressure boost. It cycles between a higher inspiratory positive airway pressure (IPAP) and a lower expiratory positive airway pressure (EPAP). The difference between them — the pressure support — actively augments each breath, increasing tidal volume and so improving ventilation and CO2 clearance. BiPAP is therefore the right tool when the problem is ventilatory: neuromuscular weakness, central hypoventilation, chest-wall deformity, or a child in hypercapnic failure who is tiring. [9]
Classification
Sort respiratory support devices along two axes: how much oxygen and flow they deliver, and whether they deliver positive pressure and ventilatory support. This double-axis map is what guides device selection at the bedside. [6] [7]
By oxygen and flow delivery — standard low-flow devices (nasal cannula, simple face mask, non-rebreather mask) provide variable, imprecise FiO2 at flows below the child's own inspiratory demand. High-flow systems (HFNC) provide a precise, blended FiO2 at flows that match or exceed demand. The practical distinction matters: low-flow devices are comfortable, cheap and universally available, but the delivered oxygen concentration drops whenever the child breathes harder or faster; high-flow systems hold the FiO2 stable regardless of effort. [10]
By pressure and ventilatory support — devices divide into three tiers. Open systems with no set pressure (low-flow oxygen, HFNC) cannot guarantee recruitment. Sealed systems delivering continuous pressure (CPAP) guarantee a distending pressure but provide no active inspiratory assistance. Sealed systems delivering two pressures (BiPAP) provide both a distending pressure and active ventilatory support. The pressure-support dimension is what separates oxygenation support from ventilation support. [9]
- Flow 0.5 to 4 L/min (child)
- FiO2 variable, roughly 24 to 40 per cent
- No positive pressure, no ventilatory support
- Comfortable and simple; best for mild hypoxaemia
- Flow 2 L/kg/min up to 60 L/min
- FiO2 precise 21 to 100 per cent, warmed and humidified
- Modest flow-dependent PEEP, reduced work of breathing
- Best for moderate distress where you want to avoid a sealed mask
- Continuous pressure 5 to 10 cmH2O via sealed mask
- FiO2 precise 21 to 100 per cent
- Reliable recruitment pressure, no active ventilation
- Best for hypoxaemic (type 1) failure from recruitable disease
- IPAP 10 to 20 cmH2O, EPAP 4 to 8 cmH2O (pressure support = IPAP minus EPAP)
- FiO2 precise 21 to 100 per cent
- Active ventilatory support augments tidal volume
- Best for hypercapnic (type 2) failure and neuromuscular weakness
Epidemiology & Risk Factors
Acute respiratory failure is the commonest reason a child needs critical-care support, and the transition from distress to failure is the pathway to cardiac arrest in most paediatric arrests — unlike adults, where the primary event is usually cardiac. Non-invasive support sits squarely in that gap: well chosen, it prevents intubation; poorly chosen, it delays it. [1] [7]
The children most likely to need HFNC or non-invasive ventilation share a few features. Infants under 12 months with viral bronchiolitis are by far the largest single group — bronchiolitis is the commonest lower-respiratory admission in this age band, and moderate-to-severe cases frequently require escalated support. [1] [2] Children with pre-existing vulnerability are over-represented: former premature infants with chronic lung disease, those with congenital heart disease and pulmonary hypertension, neuromuscular weakness (spinal muscular atrophy, muscular dystrophy, central hypoventilation), immunocompromise, and the technology-dependent child with a tracheostomy or home ventilation. [9]
Social determinants sharpen the risk. Tobacco-smoke exposure, incomplete immunisation (including palivizumab omission in eligible preterm infants), overcrowded housing and remote location all increase severity at presentation and the likelihood that support is needed. Indigenous children in Australia and New Zealand carry a disproportionate burden of severe lower-respiratory disease. These factors do not change the device choice, but they change the threshold at which you escalate and the speed at which you do it. [7]
Pathophysiology
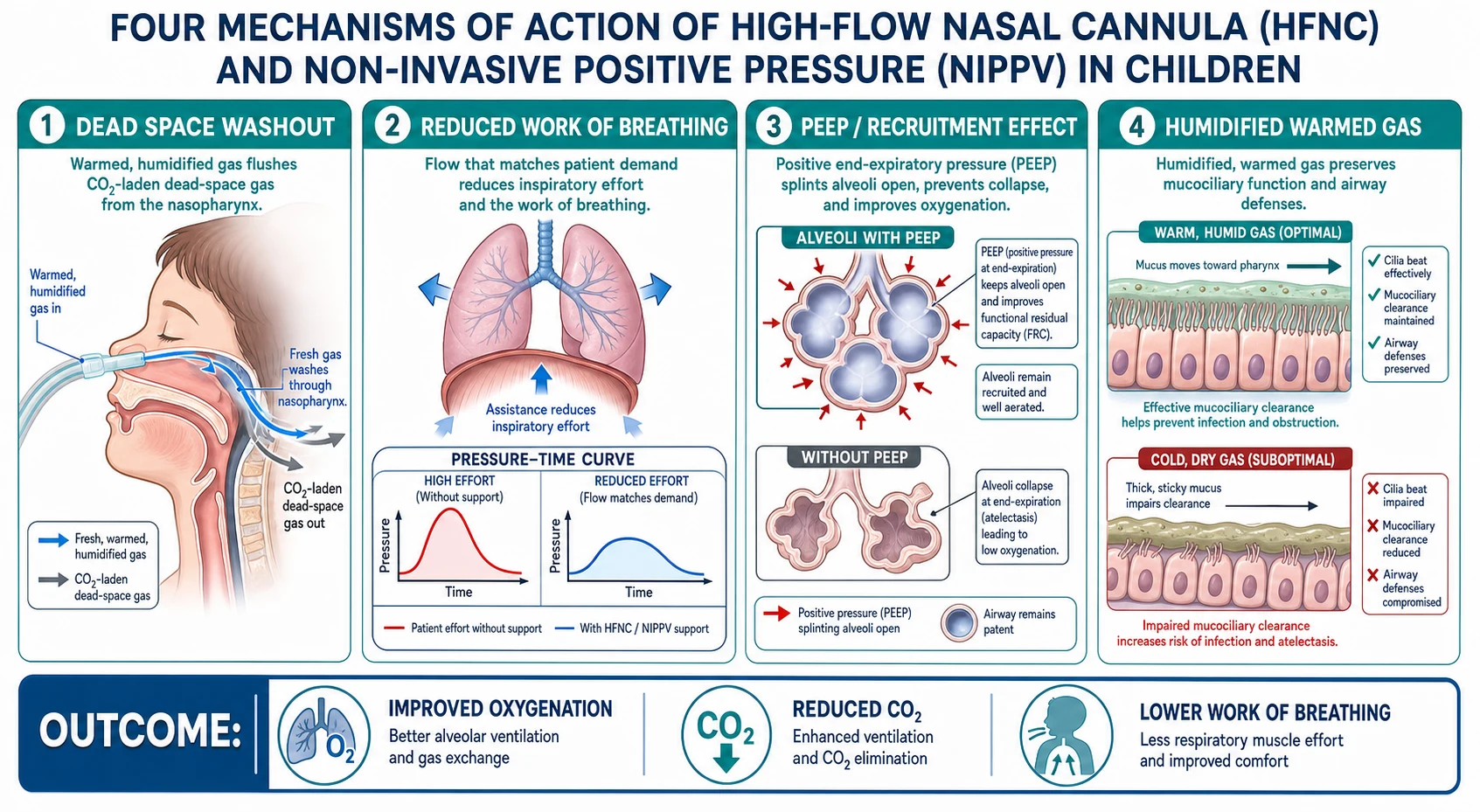
Understanding what each device actually does to the lungs — not just what it is called — is what allows you to choose correctly rather than reaching for whatever is familiar. Three physiological mechanisms separate the devices, and a fourth makes HFNC uniquely tolerable. [5] [6]
Dead-space washout. The nasopharynx and large airways contain gas that has already exchanged — rich in CO2, poor in oxygen. A child breathing normally must move this dead-space gas before fresh air reaches the alveoli. At high flows, HFNC constantly flushes the upper airway with fresh, oxygen-enriched gas, so each breath the child takes draws from a reservoir of clean gas rather than rebreathing CO2. The functional effect is that a higher proportion of each breath reaches the gas-exchange surface: dead space effectively shrinks, and the same tidal volume does more useful work. [5] [6]
Reduced work of breathing. When a child is in respiratory distress, inspiratory flow demand rises steeply. A low-flow device cannot match that demand — the child must generate large negative pressures to pull in air, which is exhausting. HFNC delivers flow at or above the child's inspiratory demand, so the respiratory muscles do less work per breath. CPAP and BiPAP reduce work differently: CPAP holds the airways and alveoli open so they do not collapse and need reopening each breath (a major energy cost), and BiPAP adds a pressure boost during inspiration that actively assists the breath. [5] [9]
Positive end-expiratory pressure and recruitment. In lung disease — pneumonia, bronchiolitis, pulmonary oedema, acute respiratory distress syndrome — small airways and alveoli tend to collapse at end-expiration. Each breath then has to prise them open again, and some stay collapsed, creating shunt (blood flowing past non-ventilated lung) that causes hypoxaemia refractory to oxygen alone. Positive pressure splints these units open, raising functional residual capacity, reducing shunt and improving oxygenation. HFNC generates a modest, flow-dependent PEEP (roughly 3 to 7 cmH2O depending on flow, leak and mouth position); CPAP delivers a set, reliable PEEP that you control. BiPAP's EPAP provides the same recruitment as CPAP, with the IPAP adding the ventilatory assist on top. [9]
Humidification and conditioning. High flows of cold, dry gas would dry the airway, thicken secretions and impair mucociliary clearance within minutes. The HFNC system heats the gas to near body temperature and saturates it with water vapour, so cilia keep beating normally and secretions stay thin and mobile. This is not a comfort feature — it is a mechanism of action, because retained secretions cause atelectasis and worsen gas exchange. [6]
How HFNC rescues a tiring infant (mechanistic chain)
High flow flushes CO2-rich dead-space gas from the nasopharynx
Flow meets inspiratory demand, so respiratory muscles do less work per breath
Flow-dependent PEEP splints small airways open at end-expiration
Warmed humidified gas keeps secretions thin and cilia beating
Net effect: better oxygenation, lower CO2, less effort, buying time
Clinical Presentation
The child who needs non-invasive support is the child whose own breathing is no longer adequate — but the device you reach for depends on whether the failure is oxygenation, ventilation, or both. Recognise what you see, then map it to the right tool. [7]
The hypoxaemic child (type 1 failure pattern). This child has a working pump but diseased lungs: tachypnoea, recession and grunting with oxygen saturations that stay low despite supplemental oxygen. The problem is shunt and collapsed alveoli. This is the child whose oxygenation will improve with positive pressure — CPAP to recruit, or HFNC to provide a PEEP effect plus dead-space washout. Typical causes are bronchiolitis, pneumonia, pulmonary oedema and acute respiratory distress syndrome. [1] [9]
The hypercapnic child (type 2 failure pattern). This child is either too weak to ventilate, has no drive to breathe, or has obstructed airflow so severely that CO2 accumulates. You may see shallow, rapid or irregular breathing, a diminishing respiratory effort, drowsiness, or a child who looks exhausted. The blood gas shows a rising PaCO2 with respiratory acidosis. This is the child who needs ventilatory support — BiPAP to augment tidal volume — not just oxygen or CPAP. Typical causes are neuromuscular weakness, central hypoventilation, severe asthma with a tiring child, or any infant in bronchiolitis who has crossed from type 1 into type 2 as fatigue sets in. [9]
The mixed or deteriorating child. Many children start hypoxaemic and become hypercapnic as they tire — the falling respiratory rate and quieting chest are the danger signs. This child needs an honest reassessment: if non-invasive support is not reversing the trend within a defined period, intubation is the answer, not a higher setting. [7]
Differential Diagnosis
The differential for a child needing respiratory support is not a list of diseases to memorise — it is a framework for deciding which device the pathophysiology demands. Group the causes by what they break. [7] [9]
Lower-airway obstruction (wheeze, prolonged expiration). Asthma and viral wheeze produce airway narrowing that raises the work of breathing and, in severe cases, causes CO2 retention. HFNC and BiPAP can help the tiring asthmatic, but the disease-specific treatment — bronchodilators, steroids, magnesium — is primary. CPAP is generally not first-line here. [7]
Small-airways disease with secretions and collapse (bronchiolitis). The archetypal HFNC indication: infants with moderate-to-severe bronchiolitis who are hypoxaemic and working hard. HFNC and CPAP both have trial evidence in this group, and current guidelines list both as acceptable for moderate-severe disease in critical care. [1] [3] [7]
Alveolar or interstitial disease (pneumonia, PARDS, pulmonary oedema). These cause shunt and refractory hypoxaemia that responds to recruitment. CPAP or BiPAP are the pressure devices of choice; HFNC may be a bridge in milder cases. In PARDS, the PALICC-2 guidelines address the role of non-invasive support as a lung-protective strategy to avoid intubation where feasible. [9]
Pump or drive failure (neuromuscular weakness, central hypoventilation, overdose). These cause pure ventilatory failure with preserved oxygenation early on. The child needs BiPAP to support ventilation, not CPAP alone. Missing this distinction and giving CPAP to a weak child is a classic error — it holds the airway open but does not move air. [9]
- Bronchiolitis, pneumonia, pulmonary oedema, PARDS
- Shunt and collapsed alveoli are the problem
- Needs recruitment pressure: HFNC, CPAP or BiPAP
- Neuromuscular weakness, central hypoventilation, tiring asthma
- Inadequate ventilation and CO2 retention are the problem
- Needs ventilatory support: BiPAP (not CPAP alone)
Clinical & Bedside Assessment
The decision to start, continue or escalate non-invasive support rests on a structured bedside assessment repeated at frequent intervals. Three axes — work, efficacy and effect of breathing — tell you whether the device is succeeding or failing. [7]
Work of breathing. Assess the effort the child is expending: respiratory rate against age-normal ranges, chest-wall recession (intercostal, subcostal, sternal), nasal flaring, tracheal tug, grunting, head-bobbing in infants and accessory-muscle use in older children. High and sustained work means the child is fighting; a falling rate with lessening effort in a child who is not improving means exhaustion. [7]
Efficacy of breathing. Assess whether the effort is achieving anything: air entry on auscultation (symmetry, depth), the character of breath sounds (wheeze, crackles, stridor), and chest rise. A child working hard with poor air entry has ineffective breathing — the pump is failing or the airways are too obstructed. [7]
Effect of breathing. Assess the physiological result: oxygen saturation by continuous pulse oximetry, colour, conscious state, capillary refill and heart rate. Persistent hypoxaemia, drowsiness or a rising heart rate with poor perfusion means support is not working. [7]
A key principle: on non-invasive support, reassessment must be frequent and documented. The standard approach is to assess within 30 to 60 minutes of starting, then at regular intervals, with a clear plan for what counts as failure and what the next step is. [7]
Investigations
Investigations on a child receiving non-invasive support serve two purposes: monitoring the trajectory of the respiratory failure and identifying the underlying cause. They never delay oxygen or support. [7]
Continuous pulse oximetry is the most important single monitor. It gives real-time feedback on oxygenation and is the primary tool for titrating FiO2. Interpret it in context: a child with chronic lung disease may have a lower baseline, and a child with poor perfusion may give a falsely low reading. A target saturation of 92 to 95 per cent is appropriate for most acute respiratory conditions; targets differ in specific diseases such as cyanotic congenital heart disease or hypercapnic chronic failure where oxygen can suppress respiratory drive. [7]
Capillary or venous blood gas distinguishes type 1 from type 2 failure and tracks the trend. A rising PaCO2 with falling pH on support is the clearest biochemical signal that non-invasive ventilation is failing and the child needs intubation. Blood gas does not need to be arterial in every child — capillary or venous CO2 trends are clinically useful, though arterial samples are needed for accurate PaO2 if oxygenation status is critical. [9]
Chest radiography identifies or confirms the cause — consolidation, hyperinflation, effusion, pneumothorax, pulmonary oedema — and is directed rather than routine. It also checks device position if there is concern. [7]
Blood tests and microbiology follow the suspected cause: full blood count and CRP for bacterial infection, blood cultures if sepsis is suspected, respiratory viral panel (the commonest positive result in infants), electrolytes to detect hyponatraemia in bronchiolitis or DKA, and blood glucose. In the febrile, shocked child, the sepsis work-up runs in parallel with respiratory support. [7]
SAFE
Management — Resuscitation
The immediate priority in any child needing respiratory support is to clear the airway, give oxygen, and decide whether the child is in extremis and needs bag-mask ventilation and intubation right now, or is stable enough for a trial of non-invasive support. [7]
Assess and clear the threat gate first. Before reaching for a device, confirm the airway is patent, position the child, suction secretions if obstructing, and give high-concentration oxygen by whatever means is immediately available (mask with reservoir) while you prepare. If the child is bradycardic, apnoeic, has a silent chest or altered conscious state, they are in or near arrest — start bag-mask ventilation and call for urgent intubation. Non-invasive support is for the child who is failing but still has a pulse, a drive to breathe and the physiological reserve to tolerate a trial. [7]
Start the right device for the problem. If the child is hypoxaemic with high work of breathing but still ventilating and not in extremis, start HFNC or low-flow oxygen. If the problem is alveolar collapse with refractory hypoxaemia, start CPAP. If the child is hypercapnic or has neuromuscular weakness, start BiPAP. Set the initial parameters, fit the interface carefully, and commit to a reassessment plan. [1] [9]
Define failure before you start. The most dangerous error is open-ended non-invasive support with no exit criterion. State the trigger for intubation at the outset: persistent or worsening hypoxaemia, a rising PaCO2, worsening acidosis, exhaustion, haemodynamic instability, or failure to improve within a defined window. [7]
Management — Definitive & Stepwise
Once the child is on support and the threat gate is clear, the management becomes a stepwise ladder of escalation and de-escalation, with disease-specific treatment running in parallel. Each step carries specific settings that must be set correctly. [1] [7]
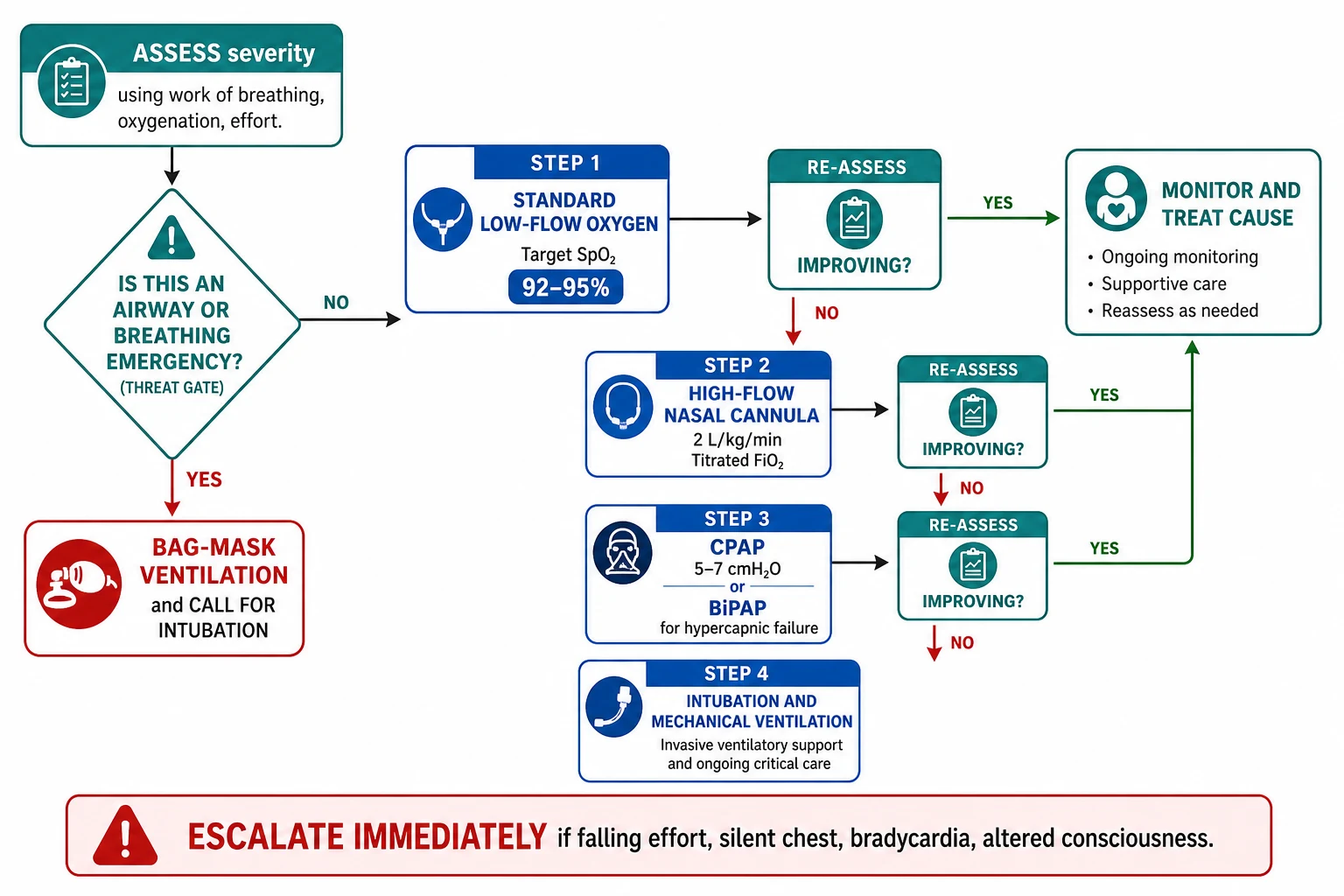
Step 1 — standard low-flow oxygen. Start with a nasal cannula at 0.5 to 2 L/min or a simple face mask at 5 to 8 L/min (never below 5 L/min for a mask, to avoid CO2 rebreathing) to achieve the target saturation. If the child improves and stabilises, continue, treat the cause, and wean as tolerated. If the work of breathing remains high or saturations are not maintained, escalate. [7]
Step 2 — high-flow nasal cannula. Initiate HFNC with a weight-based flow of 2 L/kg/min (commonly 1 to 2 L/kg/min, titrated upward), capped at about 60 L/min in older children. Set the FiO2 to the minimum that achieves the target saturation, weaning FiO2 before weaning flow. Use correctly sized nasal prongs that sit comfortably in the nares without occluding them completely. Reassess within 30 to 60 minutes. The landmark trial evidence in bronchiolitis shows HFNC reduces treatment failure compared with standard oxygen when used as primary therapy for moderate disease. [1] [2]
High-flow nasal cannula — starting parameters
Dose
Flow 2 L/kg/min (titrate 1 to 2 L/kg/min), FiO2 21 to 100 per cent to target SpO2
Step 3 — CPAP or BiPAP. If HFNC fails or the problem demands reliable pressure, escalate to CPAP or BiPAP. For CPAP, start at 5 to 7 cmH2O and titrate; the EPAP component of BiPAP provides the same recruitment. For BiPAP, set IPAP at 10 to 15 cmH2O and EPAP at 4 to 6 cmH2O, giving an initial pressure support of about 6 to 9 cmH2O, then titrate to achieve adequate tidal volume and CO2 clearance. Use a well-fitted mask with minimal leak. BiPAP is the right tool for hypercapnic failure, neuromuscular weakness and the tiring child. [9]
CPAP and BiPAP — starting parameters
Dose
CPAP 5 to 7 cmH2O continuous. BiPAP IPAP 10 to 15, EPAP 4 to 6 cmH2O (pressure support = IPAP minus EPAP)
Step 4 — intubation and mechanical ventilation. If the child fails non-invasive support — persistent hypoxaemia or hypercapnia, exhaustion, haemodynamic instability, loss of airway reflexes, or failure to improve within the defined window — proceed to intubation without further delay. Prepare for rapid sequence intubation with appropriate paediatric drug dosing and equipment. Continuing non-invasive support past the point of failure is the cardinal error. [7]
Weaning. When the child improves, wean in the reverse order: reduce FiO2 first toward 30 to 40 per cent, then reduce flow or pressure, monitoring for deterioration. Weaning HFNC flow can proceed by 0.5 to 1 L/kg/min decrements as tolerated. Transition from CPAP or BiPAP to HFNC or low-flow oxygen when the child maintains saturations and adequate ventilation on minimal pressure. [7]
Specific Subtypes & Scenarios
Bronchiolitis
Bronchiolitis is the condition that defines paediatric HFNC practice, and the evidence base is strongest here. The Franklin trial randomised infants with moderate bronchiolitis to HFNC versus standard oxygen and found treatment failure was halved (12 per cent versus 23 per cent), with most standard-oxygen failures successfully rescued by crossover to HFNC. [1] The Kepreotes trial, however, found no significant difference between HFNC and standard low-flow for moderate bronchiolitis at 24 hours, reminding us that the benefit is clearest in moderate-to-severe disease rather than mild cases. [2] The TRAMONTANE trial showed HFNC was non-inferior to nCPAP as initial therapy for bronchiolitis in young infants, supporting HFNC as an acceptable first-line critical-care modality. [3] Current PICU guidelines recommend HFNC or nCPAP for moderate-to-severe bronchiolitis that has failed standard oxygen. [7]
Neuromuscular weakness and central hypoventilation
Children with spinal muscular atrophy, muscular dystrophy, congenital myopathies or central hypoventilation syndromes develop hypercapnic respiratory failure — their pump is too weak or their drive is absent. These children need BiPAP, not CPAP: the problem is ventilation, not oxygenation or recruitment alone. A critical error is giving CPAP to a weak child, which holds the airway open but provides no active ventilatory assistance. Many of these children already use home BiPAP, so in acute illness the answer may be optimising their existing settings rather than starting fresh. [9]
Acute severe asthma
In acute severe asthma, the problem is severe lower-airway obstruction with high work of breathing and, in the tiring child, evolving hypercapnia. HFNC and BiPAP can reduce work of breathing and support ventilation, but they are adjuncts — the primary treatment is aggressive bronchodilation, systemic steroids and, in refractory cases, intravenous magnesium, ketamine or aminophylline. BiPAP is preferred over CPAP when CO2 is rising, because the pressure support augments ventilation against high airway resistance. Intubation in severe asthma is high-risk (periarrest from dynamic hyperinflation) and should be avoided if possible but not delayed once indicated. [7]
Paediatric acute respiratory distress syndrome
In PARDS, the PALICC-2 guidelines address non-invasive support as a strategy to avoid intubation where the disease is mild-to-moderate and the child can tolerate a sealed interface. HFNC may be a bridge; CPAP and BiPAP deliver the recruitment pressure and ventilatory support that hypoxaemic, recruitable lung disease demands. The decision to intubate is guided by oxygenation failure, rising CO2, exhaustion or multiorgan failure. [9]
The immunocompromised child
Immunocompromised children with acute respiratory failure are a special case: intubation carries a high mortality in this group, so a trial of non-invasive support to avoid intubation is often preferred. BiPAP is commonly used first-line. However, the same rules apply — define failure early and do not persist past the point where intubation becomes necessary. [9]
In Australia and New Zealand, HFNC is well established in PICU and increasingly in paediatric wards and retrieval services. The Ramnarayan trial (FIRST-HFNC) was a multicentre ANZ and UK study confirming that HFNC as first-line non-invasive support was non-inferior to CPAP for liberation from respiratory support in acutely ill children, with less nasal trauma — supporting HFNC as an acceptable first choice in many PICU settings. [4]
Complications & Pitfalls
Non-invasive support is generally safe, but it has specific complications and a set of classic errors that cause harm. Knowing them is what separates a practitioner who uses the tools well from one who gets caught out. [7]
Nasal trauma and pressure injury. Both HFNC prongs and CPAP or BiPAP masks can cause nasal bridge erosion, septal injury or facial pressure sores if the interface is too tight or the wrong size. The Ramnarayan trial found HFNC caused significantly less nasal trauma than CPAP — an advantage beyond efficacy. [4] Prevent injury with correct sizing, regular skin checks, and not over-tightening straps. [7]
Air leak and pneumothorax. Positive pressure can cause or worsen a pneumothorax, particularly in conditions with high airway pressures or trapped gas such as severe asthma or meconium aspiration. Sudden deterioration on support — hypoxaemia, asymmetrical air entry, hypotension — demands immediate consideration of tension pneumothorax and needle decompression if suspected. [7]
Aspiration and feed intolerance. Children on HFNC or CPAP may have impaired swallowing reflexes or gastric distension from swallowed gas. Vomiting or feed intolerance on support is an aspiration risk. Manage with nil-by-mouth status during acute escalation, nasogastric tube decompression, and cautious reintroduction of feeds once stable. [7]
The delayed-intubation error. The most dangerous pitfall is continuing non-invasive support past the point of failure — wearing rose-tinted glasses while the child tires and arrests. Define the failure criteria at the outset and honour them. A trial of HFNC or CPAP that fails is not a failure of judgement; refusing to intubate when the trial has failed is. [7]
The wrong-device error. Giving CPAP to a child with neuromuscular weakness (who needs ventilatory support, not recruitment alone) or giving HFNC to a child who needs reliable set PEEP are errors of mechanism-matching. Always ask: what does this child need — oxygen, flow, recruitment pressure, or ventilatory support? Then choose the device that delivers it. [9]
Prognosis & Disposition
For most children, the prognosis of acute respiratory failure treated with non-invasive support is excellent. The majority of infants with bronchiolitis who receive HFNC improve within 24 to 48 hours and avoid intubation entirely. [1] [7] Outcomes are driven less by the device itself than by the underlying disease, the child's comorbidities, and the timeliness of escalation when support fails. [9]
Disposition depends on the level of support and monitoring required. A child on low-flow oxygen with stable observations may be managed on a general ward. HFNC and CPAP or BiPAP require a higher level of monitoring — typically a high-dependency or PICU setting, or a ward with dedicated HFNC protocols and trained staff, depending on local policy. Any child on non-invasive support needs continuous pulse oximetry, ready access to blood gas analysis, and a clinician able to escalate to intubation. Retrieval services should be involved early for children in remote or rural settings who need escalation. [7]
The safety net. Before any child on non-invasive support is transferred, de-escalated or discharged, confirm that the underlying cause is treated, the trajectory is clearly improving, the support has been weaned to a safe level, and there is a plan for what to do if they deteriorate. Discharge planning should address the risk of recurrence, follow-up for chronic conditions, and parental education on warning signs. [7]
Special Populations
Neonates and young infants. Infants under 12 months are the largest group needing non-invasive support, principally for bronchiolitis. Their small airways, compliant chest wall and high oxygen demand make them deteriorate fast. HFNC is well established in this age group with a 2 L/kg/min flow protocol. Neonatal and ex-preterm infants may have different oxygenation targets and a higher risk of air leak; involve neonatology early for infants under a corrected age where jurisdiction-specific thresholds apply. [1] [7]
The technology-dependent child. Children with tracheostomies, home ventilation or chronic respiratory failure present with their own support already in place. In acute illness, optimise their existing settings, treat the precipitant, and involve their home-ventilation or complex-care team. These children may have different baseline saturations, abnormal airway anatomy and a high risk of decompensation. [9]
Immunocompromised children. As noted, this group benefits from non-invasive support to avoid intubation, but the risk of rapid deterioration is high. A lower threshold for ICU-level monitoring and early involvement of the oncology or immunology team is appropriate. [9]
Indigenous and remote-living children. Severe lower-respiratory disease is more common and more severe in Indigenous Australian and New Zealand children and in those with delayed access to care. In remote settings, early retrieval and pre-emptive discussion with the receiving PICU are part of safe practice. [7]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric non-invasive support has matured rapidly. The key trials and their messages are as follows. [1]
The Franklin trial (2018, NEJM) randomised infants with moderate bronchiolitis to HFNC versus standard low-flow oxygen. Treatment failure was 12 per cent with HFNC versus 23 per cent with standard oxygen; most standard-oxygen failures were rescued by crossover to HFNC without intubation. This established HFNC as an effective primary therapy for moderate bronchiolitis in infants. [1]
Franklin 2018 (NEJM)
Population: Infants with moderate bronchiolitis
Key finding
Treatment failure 12% vs 23% (HFNC reduced failure by about half)
The Kepreotes trial (2017, Lancet) found no significant difference between HFNC and standard low-flow for moderate bronchiolitis at 24 hours. The apparent discrepancy with Franklin is explained by differences in severity, definition of failure and crossover design — the message is that HFNC's advantage is clearest in moderate-to-severe disease, not in milder cases where standard oxygen would suffice. [2]
The TRAMONTANE trial (Milési 2017, Intensive Care Med) showed HFNC was non-inferior to nCPAP as initial therapy for bronchiolitis in young infants, supporting HFNC as an acceptable alternative to CPAP in this group. [3]
The Ramnarayan trial (FIRST-HFNC, 2022, JAMA) compared HFNC as first-line to CPAP in acutely ill children in PICU and found HFNC was non-inferior for the primary outcome of liberation from respiratory support, with significantly less nasal trauma. This supports HFNC as an acceptable first-line non-invasive modality across a range of diagnoses in PICU. [4]
The Memar meta-analysis (2026, BMC Pediatrics) pooled HFNC versus CPAP and conventional oxygen in paediatric acute respiratory failure, finding HFNC is a safe and effective alternative to CPAP with no significant difference in intubation rates, supporting the growing role of HFNC in paediatric critical care. [8]
The Milési 2023 PICU bronchiolitis guidelines provide consensus recommendations for severe bronchiolitis, endorsing HFNC or nCPAP as acceptable for moderate-to-severe disease after standard oxygen has failed, with HFNC flow of 2 L/kg/min. [7]
The PALICC-2 guidelines (Emeriaud 2023) address paediatric acute respiratory distress syndrome and discuss the role of non-invasive support as a lung-protective strategy. [9]
Exam Pearls
The falling respiratory rate is the single most examined danger sign on non-invasive support. A child whose rate drops, whose recession eases and whose chest quiets while saturations stay low or consciousness dims is exhausting — not recovering. This is the pre-arrest pattern, and the correct response is immediate escalation, never weaning. [7]
A practical point that examiners probe: HFNC delivers a PEEP effect, but it is flow-dependent and variable — not the reliable, set pressure of CPAP. If you need guaranteed recruitment pressure, CPAP or BiPAP is the right tool, not ever-higher HFNC flow. [4] [9]
Finally, the interface matters as much as the settings: the wrong-sized mask or prongs cause leak, trauma and treatment failure. Get the fit right, check the skin regularly, and do not over-tighten straps. The Ramnarayan trial showed HFNC's lower nasal-trauma rate is a genuine clinical advantage worth knowing. [4]
References
- [1]Franklin D A Randomized Trial of High-Flow Oxygen Therapy in Infants with Bronchiolitis. N Engl J Med, 2018.PMID 29562151
- [2]Kepreotes E High-flow warm humidified oxygen versus standard low-flow nasal cannula oxygen for moderate bronchiolitis (HFWHO RCT): an open, phase 4, randomised controlled trial. Lancet, 2017.PMID 28161016
- [3]Milési C High flow nasal cannula (HFNC) versus nasal continuous positive airway pressure (nCPAP) for the initial respiratory management of acute viral bronchiolitis in young infants: a multicenter randomized controlled trial (TRAMONTANE study). Intensive Care Med, 2017.PMID 28124736
- [4]Ramnarayan P Effect of High-Flow Nasal Cannula Therapy vs Continuous Positive Airway Pressure Therapy on Liberation From Respiratory Support in Acutely Ill Children Admitted to Pediatric Critical Care Units: A Randomized Clinical Trial. JAMA, 2022.PMID 35707984
- [5]Spentzas T Children with respiratory distress treated with high-flow nasal cannula. J Intensive Care Med, 2009.PMID 19703816
- [6]Haq I The evidence for high flow nasal cannula devices in infants. Paediatr Respir Rev, 2014.PMID 24472697
- [7]Milési C Clinical practice guidelines: management of severe bronchiolitis in infants under 12 months old admitted to a pediatric critical care unit. Intensive Care Med, 2023.PMID 36592200
- [8]Memar EHE Efficacy and safety of high-flow nasal cannula versus continuous positive airway pressure and conventional oxygen therapies in pediatric acute respiratory failure: a systematic review and meta-analysis. BMC Pediatr, 2026.PMID 42387462
- [9]Emeriaud G Executive Summary of the Second International Guidelines for the Diagnosis and Management of Pediatric Acute Respiratory Distress Syndrome (PALICC-2). Pediatr Crit Care Med, 2023.PMID 36661420
- [10]Coghill M Accuracy of a novel system for oxygen delivery to small children. Pediatrics, 2011.PMID 21727103