Paeds · acute-care-resuscitation-and-toxicology
Paediatric basic and advanced life support
Also known as Paediatric CPR · Paediatric life support algorithm · Paediatric resuscitation · Paediatric advanced life support · PALS · ANZCOR paediatric algorithm
Fellowship guide to paediatric basic and advanced life support: the BLS sequence, high-quality chest compressions, the airway and ventilation ladder, defibrillation at 4 J per kilogram, adrenaline at 10 micrograms per kilogram, reversible causes, and post-arrest care.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A two-year-old is pulled blue and limp from a swimming pool. The clock has started, the algorithm must take over, and the decisions made in the next minute decide whether that child lives and how they live afterwards. Paediatric basic and advanced life support is the structured sequence of actions used to recognise, support and reverse cardiopulmonary arrest in an infant or child. Basic life support is the airway, breathing and circulation a single rescuer or a parent can deliver; advanced life support adds defibrillation, vascular access, drugs, an advanced airway and the search for reversible causes. [1] [6]
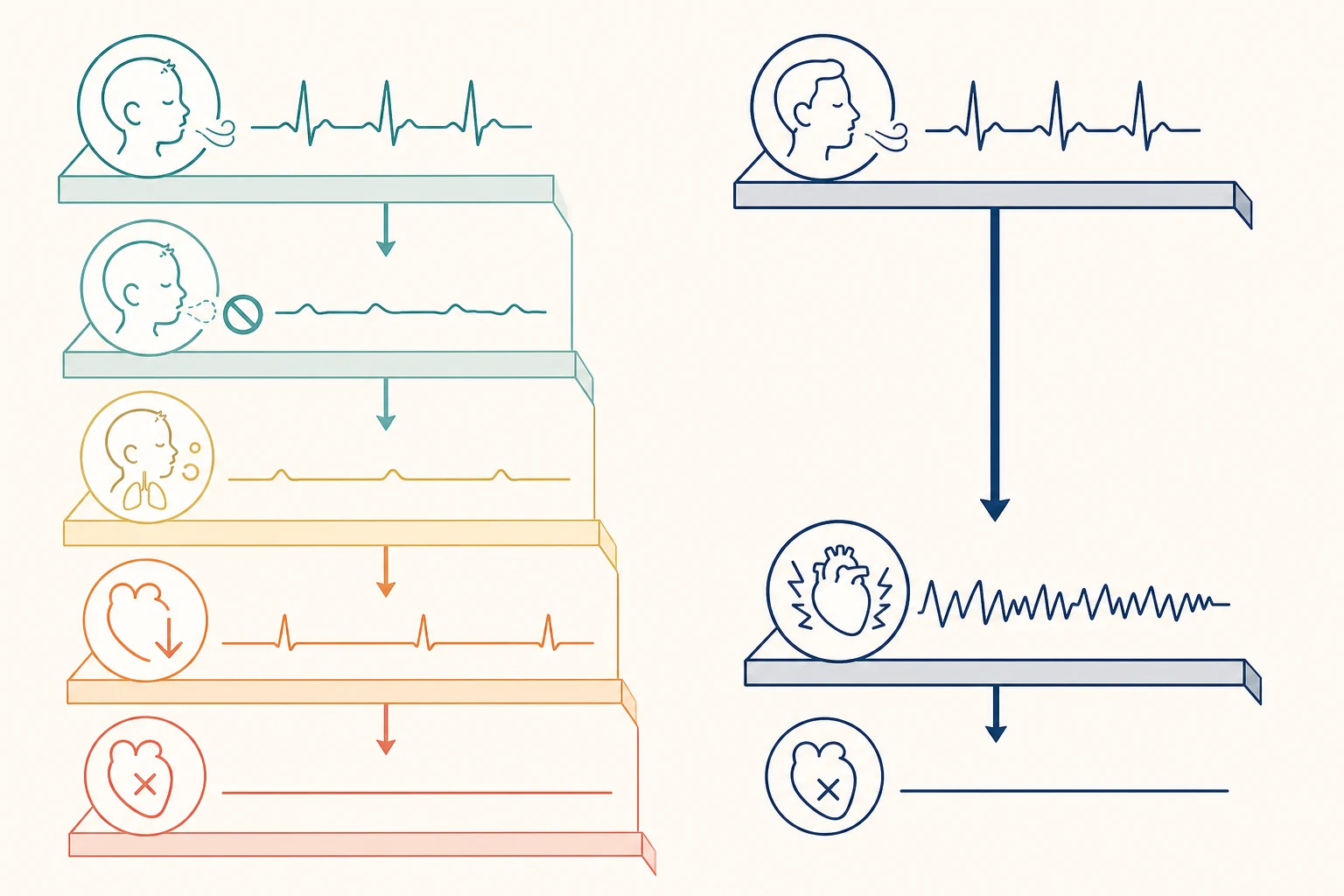
The single most important difference from adult resuscitation is the cause. Adults arrest most often from a sudden primary cardiac arrhythmia — ventricular fibrillation — in a heart that is still well oxygenated. Children arrest most often from a progressive asphyxial pathway: the airway obstructs or breathing fails, oxygen falls, bradycardia follows, and the heart stops only after the body is already deeply hypoxic. That difference drives the whole algorithm — it is why rescue breaths come before compressions, why compressions run at fifteen to two rather than thirty to two, and why ventilation quality matters as much as compression quality. [1] [2]
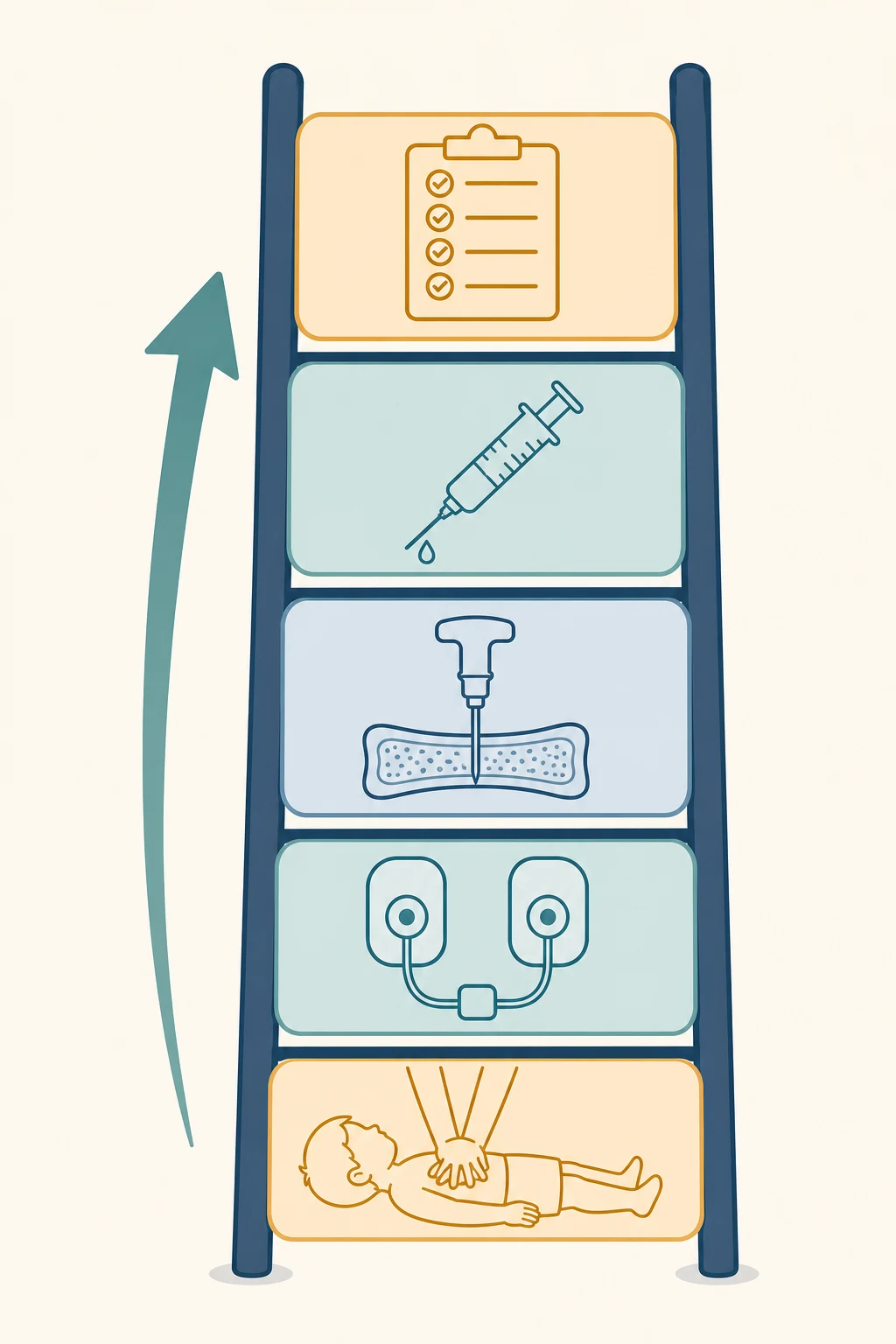
Holding the algorithm in your head means holding two ladders at once. The basic life support ladder climbs from responsiveness to airway to breathing to compressions. The advanced life support ladder adds rhythm recognition, defibrillation, vascular access, adrenaline and reversible-cause correction, looping every two minutes. The two run together, and the team that runs them well does so with clear roles, a leader, and a timer calling each cycle. [1]
Classification
A child in trouble is classified first by a single question asked at the bedside: is this child unresponsive and not breathing normally? A yes to both is a cardiac arrest until proven otherwise, and it triggers the full algorithm. Normal breathing, or just a brief gasp, does not count — gasping is agonal and is itself a sign of arrest. A child who is responsive but deteriorating is on the prevention pathway, not the arrest pathway, and belongs to the structured assessment of the deteriorating child. [1] [2]
Once in arrest, the rhythm on the monitor sorts every child into one of two management branches, and this fork decides whether a shock is given. Shockable rhythms are ventricular fibrillation and pulseless ventricular tachycardia, and they need immediate defibrillation. Non-shockable rhythms are asystole and pulseless electrical activity, and they need continuous high-quality cardiopulmonary resuscitation with adrenaline and a hunt for reversible causes. The branch is not fixed — a rhythm can flip between the two at any reassessment, which is why the team rechecks the monitor every two minutes. [1] [6]
Shockable versus non-shockable paediatric arrest
- Ventricular fibrillation or pulseless ventricular tachycardia
- Immediate defibrillation at 4 J per kilogram
- Adrenaline after the third shock
- More common in cardiac disease and some poisonings
- Asystole or pulseless electrical activity
- No shock — continuous high-quality CPR
- Adrenaline as soon as vascular access is obtained
- Driven by asphyxia, hypovolaemia and the four Hs and four Ts
Epidemiology & Risk Factors
Paediatric cardiac arrest is uncommon compared with adult arrest, but it is the crisis for which every general paediatrician must be prepared. Out-of-hospital cardiac arrest in children occurs at roughly eight to twenty per one hundred thousand children per year, and in-hospital arrest adds a similar burden concentrated in critical care and oncology settings. Survival to discharge sits near ten to fifteen per cent for out-of-hospital arrest but is substantially better, around thirty-five to forty-five per cent, for in-hospital arrest where the team, the monitor and the reversible causes are already to hand. [1] [11]
Risk concentrates wherever the asphyxial pathway can take hold. Infants are over-represented because of sudden infant death, airway obstruction and respiratory infections. Toddlers add drowning, foreign-body aspiration and poisoning. School-age children and adolescents add asthma, anaphylaxis, trauma and, in those with underlying heart disease, sudden arrhythmic death. A child with a known cardiac lesion, a complex chronic condition, or a recent severe respiratory or neurological illness sits at higher risk and arrests more often in hospital, where the prevention pathway matters most. [1] [6]
The factor that changes outcome more than any single intervention is bystander cardiopulmonary resuscitation. A child who receives bystander CPR before the ambulance arrives is roughly two to three times more likely to survive to discharge, and dispatcher-assisted telephone coaching closes the gap for untrained rescuers. This is why community CPR education and dispatcher-assisted instructions are public-health interventions, not just clinical skills, and why every paediatrician should be able to teach a parent the irreducible core — push hard, push fast, and do not stop. [11]
Pathophysiology
To lead a paediatric arrest well you must understand why the child stopped, because the algorithm is engineered to reverse that mechanism. Most children travel down an asphyxial pathway: the airway obstructs or breathing fails, alveolar oxygen falls, and arterial oxygen tension drops while carbon dioxide climbs. The hypoxic myocardium slows — first into a bradycardia and then into asystole or pulseless electrical activity. By the time the heart stops, the tissues have already sustained minutes of oxygen debt, which is why the first priority is to re-oxygenate the lung rather than to shock the heart. [1] [6]
This is the mirror image of the arrhythmic pathway that dominates adult arrest. There a primary electrical fault — usually ventricular fibrillation — stops a freshly oxygenated heart within seconds, and the decisive act is to deliver a shock before the myocardium exhausts its oxygen reserve. Children can and do arrest by this pathway, particularly those with underlying cardiac disease, channelopathies, or cardiotoxic poisoning, and when they do, early defibrillation is just as life-saving as it is in adults. The point is not that children never fibrillate — it is that the default mechanism is asphyxia, and the algorithm defaults accordingly. [1] [3]
A corollary of asphyxia-first physiology is that coronary and cerebral perfusion only recover once compressions build an aortic pressure, and that pressure collapses the moment compressions stop. Every interruption for a rhythm check, an intubation or a shock drains the pressure that took a minute to build. This is the physiological basis for the relentless rules of high-quality CPR — minimise interruptions, allow full recoil, and resume compressions the instant a shock is delivered. [4] [7]
Clinical Presentation
The presentation of arrest is stark and the window for recognition is narrow. The child is unresponsive and not breathing normally, with no signs of life. Agonal gasps are a sign of arrest, not of life, and must not be mistaken for effective breathing. Pulse checks are unreliable and should take no longer than ten seconds — in an infant, feel for the brachial pulse; in a child, the carotid. If there is no pulse, or a heart rate under sixty beats per minute with poor perfusion and no response to ventilation, begin chest compressions. [1] [4]
More useful than the arrest itself is the recognition of the child who is about to arrest, because prevention beats resuscitation every time. The deteriorating child shows it across five systems: an obstructed or increasingly effortful airway, a rising or falling respiratory rate with recession and head-bobbing, a heart rate at the extremes with prolonged capillary refill and mottled skin, an altered conscious state, and a falling urine output. A structured paediatric track-and-trigger score or a clinical gut-sense that this child looks wrong should summon senior help before the algorithm is ever needed. [1] [6]
The history surrounding an arrest points to its cause and its reversible treatment. A drowning, a choking episode, an asthma attack, an anaphylactic exposure, a toxic ingestion, a seizure, or a child with known heart disease each steer the team toward a specific arm of the algorithm and a specific reversible cause. In-hospital, the trend of the monitors in the minutes before the arrest usually tells the story — a climbing carbon dioxide, a falling oxygen, a widening QRS, or a dropping blood pressure. [1]
Differential Diagnosis
During the arrest itself, the differential is condensed to the reversible causes, because every paediatric arrest is assumed to have one until proven otherwise. The four Hs are hypoxia, hypovolaemia, hypo- or hyperkalaemia and other metabolic derangement, and hypo- or hyperthermia. The four Ts are tension pneumothorax, tamponade, toxins, and thrombosis. Holding these eight in a mental loop, and checking each against the history and the rhythm, is what separates a resuscitation that ends in recovery from one that ends in a flat line. [1] [5]
The four Hs and four Ts — reversible causes of paediatric arrest
- Hypoxia — the commonest paediatric cause
- Hypovolaemia — haemorrhage, dehydration, sepsis
- Hypo- or hyperkalaemia and metabolic derangement
- Hypo- or hyperthermia
- Tension pneumothorax — especially in ventilated children
- Tamponade — cardiac, after surgery or trauma
- Toxins — cardiotoxic drugs and poisons
- Thrombosis — pulmonary or cardiac
Hypoxia leads the list in children because it is the engine of the asphyxial pathway, and it is corrected by re-oxygenating the lung. Hypovolaemia is the next most common and is corrected with a fluid bolus. A wide-complex rhythm or a history of renal failure, chemotherapy, or ingestion points to potassium and the metabolic causes, where a blood gas and bedside electrolytes guide correction. Tension pneumothorax is suspected in a ventilated child with asymmetric breath sounds and hypotension, and it is decompressed with a needle then a drain. Toxins are inferred from the history and treated with specific antidotes. [1] [5]
Clinical & Bedside Assessment
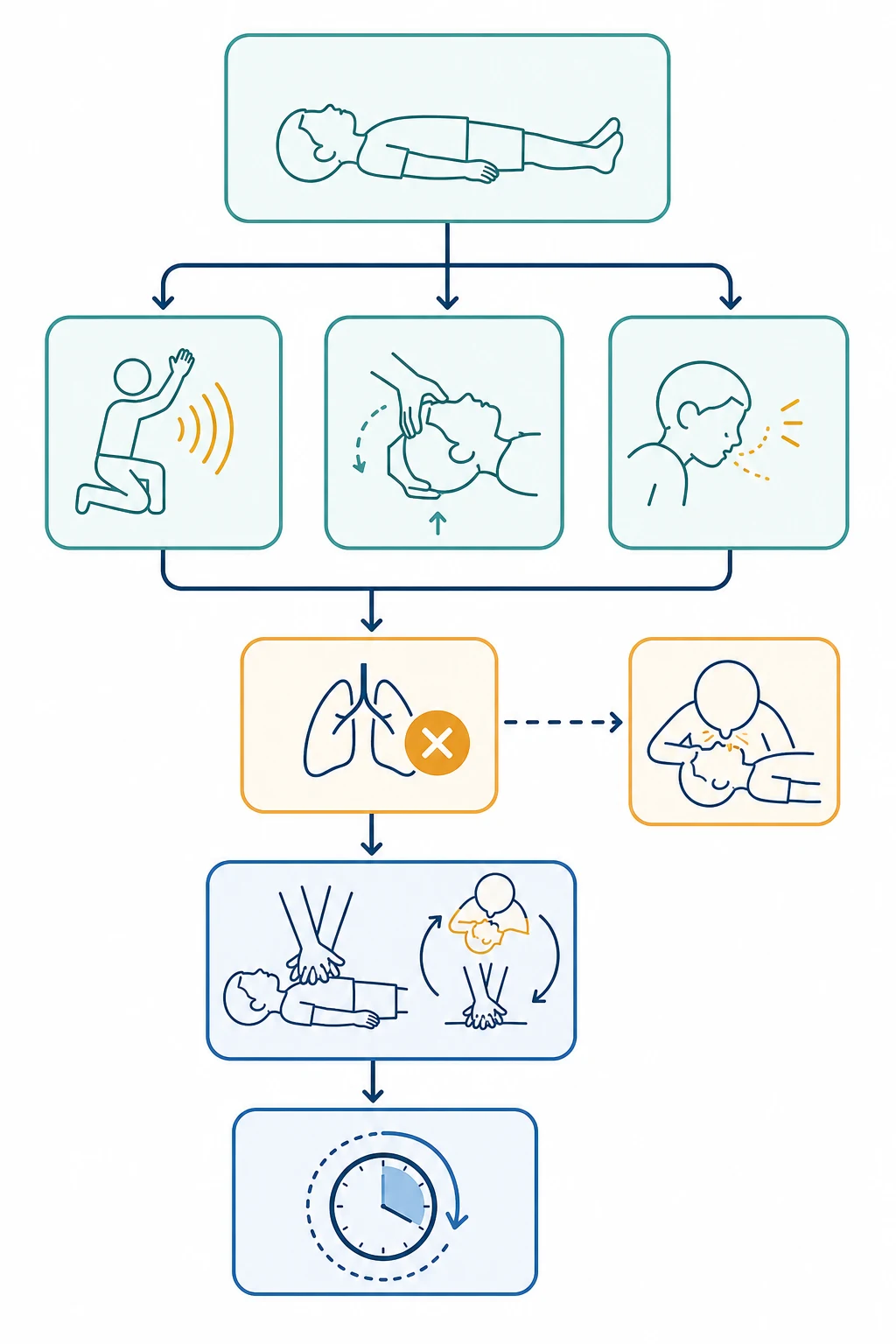
The assessment runs inside the algorithm, not beside it. The first ten seconds determine whether an arrest has occurred: tap and shout, open the airway with a head tilt and chin lift — or a jaw thrust if cervical injury is suspected — and look, listen and feel for normal breathing for no more than ten seconds. If the child is not breathing normally, call for help, send for the defibrillator, and give five rescue breaths before starting compressions. [1] [2]
Each rescue breath is delivered over about one second, with enough volume to produce gentle chest rise. Too much volume and too forceful a breath gastric-inflate the child and raise intrathoracic pressure, which drops cardiac output; too little and the hypoxic lung is never re-oxygenated. For an infant, a rescuer seals their mouth over the infant's mouth and nose; for a child, mouth-to-mouth with the nose pinched. A bag-valve-mask is the healthcare provider's airway of choice once equipment arrives, and the skill of a two-hand mask seal with a jaw thrust is one of the highest-yield in paediatric resuscitation. [1] [6]
High-quality paediatric CPR — the five non-negotiables
Assess and re-assess in two-minute cycles, not continuously. Continuous pulse and rhythm checking interrupts compressions and drains the aortic pressure that the cycle just built. The leader watches the clock, calls the rhythm check at two minutes, and the team pauses for no more than ten seconds while the defibrillator assesses — then compressions resume immediately, whatever the rhythm. Capnography adds a live readout: a carbon dioxide trace confirms an advanced airway and a return of a real value, and a rising end-tidal carbon dioxide is an early sign of return of spontaneous circulation. [1] [4]
Investigations
In the heat of arrest only a few investigations earn their place, and none should delay chest compressions or a shock. The single most useful bedside monitor is the end-tidal carbon dioxide trace, which confirms airway placement, tracks compression quality in real time, and signals a rising cardiac output before a pulse is palpable. A near-pair blood gas and a bedside glucose are drawn at the first vascular access and answer two questions that change management immediately: is this a metabolic or electrolyte arrest, and is the child hypoglycaemic. [1] [5]
Blood glucose must never be forgotten, because hypoglycaemia is a reversible cause of both the arrest and of ongoing neurological injury, and it is corrected with a bolus of intravenous dextrose. A venous or arterial blood gas quantifies the acidosis, the potassium, the haemoglobin and the carbon dioxide, and guides the correction of the metabolic arm of the four Hs. A chest radiograph and an echocardiogram, once the child is stable or during a pulseless phase, look for a pneumothorax, a tamponade, or a cardiogenic cause. Electrolytes, a toxicology screen and a coagulation profile round out the search for the cause once return of spontaneous circulation is achieved. [1] [5]
Management — Resuscitation
The first act of resuscitation is to ensure the scene is safe and to summon help. Confirm unresponsiveness, shout for help, and send a specific person to fetch the defibrillator and to call the arrest team. Open the airway, check breathing, and if the child is not breathing normally, give five rescue breaths. Then begin chest compressions. For a lone lay rescuer, a ratio of thirty compressions to two breaths is acceptable to simplify the skill; for two rescuers or healthcare providers, the ratio is fifteen to two, which delivers the extra ventilation the hypoxic child needs. [1] [2]
High-quality chest compressions
Dose
15 compressions to 2 ventilations (2 rescuers); compress one third of the anteroposterior chest depth (~4 cm infant, ~5 cm child) at 100–120 per minute
Compress in the right place and at the right depth. For an infant use two fingers in the lower half of the sternum, or — with two rescuers — the two-thumb encircling hands technique around the chest, which generates better compression depth and coronary perfusion. For a child use the heel of one or two hands over the lower half of the sternum. Compress one third of the anteroposterior depth of the chest — roughly four centimetres in an infant and five in a child — at one hundred to one hundred and twenty per minute, allowing full recoil and swapping compressors every two minutes to avoid fatigue. [1] [4]
The basic life support sequence
Check the scene is safe, check responsiveness, shout for help
Open the airway; look, listen and feel for normal breathing (max 10 seconds)
Give five rescue breaths, each about one second, gentle chest rise
Start chest compressions at 15:2 (2 rescuers) — one third chest depth, 100–120 per minute
Attach the defibrillator as soon as it arrives; assess rhythm every 2 minutes
Swap compressors every 2 minutes; resume compressions immediately after any shock
Management — Definitive & Stepwise
The moment the defibrillator arrives, attach the pads and read the rhythm, because a shockable rhythm changes the management at once. Ventricular fibrillation and pulseless ventricular tachycardia are shocked at four joules per kilogram, using a biphasic defibrillator and appropriately sized paediatric pads or paddles with paediatric energy attenuation if needed. After the shock, resume compressions immediately — do not pause to check a pulse — and continue for two minutes before reassessing. If the rhythm remains shockable, deliver a second shock at four joules per kilogram, resume CPR, and prepare adrenaline and amiodarone for the third shock onwards. [1] [5]
Defibrillation (biphasic)
Dose
4 joules per kilogram for the first and subsequent shocks
Adrenaline is the core drug of paediatric arrest. Give ten micrograms per kilogram — that is 0.1 millilitres per kilogram of the 1 in 10,000 concentration — by the intravenous or intraosseous route. In a non-shockable rhythm, give it as soon as vascular access is obtained and repeat every three to five minutes. In a shockable rhythm, give it after the third shock and repeat every three to five minutes. High-dose adrenaline is not recommended, because it has not been shown to improve survival to discharge and may worsen neurological outcome. Intraosseous access is the access of choice when intravenous cannulation is not immediate, and it should be placed early rather than after repeated failed cannulation attempts. [1] [12]
Adrenaline (epinephrine) 1:10,000
Dose
10 micrograms per kilogram (0.1 mL/kg of the 1:10,000 solution) intravenously or intraosseously; repeat every 3–5 minutes
For refractory ventricular fibrillation or pulseless ventricular tachycardia that persists after the third shock, give an antiarrhythmic. Amiodarone at five milligrams per kilogram intravenously or intraosseously is the first-line agent; lidocaine at one milligram per kilogram is an acceptable alternative. Observational evidence from in-hospital paediatric arrest suggests both improve return of spontaneous circulation in shockable rhythms, and either is preferable to no antiarrhythmic. Give fluid — ten millilitres per kilogram of isotonic crystalloid — when hypovolaemia is suspected, which it often is in sepsis, trauma and dehydration. [1] [8]
Specific Subtypes & Scenarios
The drowning child is the archetypal asphyxial arrest and is managed by the standard algorithm with an emphasis on ventilation. Give five rescue breaths and effective bag-mask ventilation early, because re-oxygenating the lung is the whole treatment, and be alert to hypothermia — cold water immersion means you must correct temperature and check the glucose. Resuscitation should generally be attempted even after prolonged submersion, because cold-water drowning in particular can recover with good neurological outcome. [1] [2]
Anaphylactic arrest combines asphyxia from upper-airway obstruction with distributive shock, and it demands adrenaline given intramuscularly early in the deteriorating phase and intravenously once in arrest, alongside fluid and a supraglottic or surgical airway plan if the upper airway is lost. Asthma arrest is hypoxaemic and hypercapnic; ventilate gently with a low rate and allow a long expiratory time to avoid air-trapping and a tension pneumothorax. The child with underlying cardiac disease arrests more often by a shockable pathway and may need early defibrillation, careful fluid balance, and liaison with a cardiology team. [1] [5]
The choking child is a pre-arrest emergency with its own brief algorithm. For a conscious infant, deliver up to five back blows between the shoulder blades, then up to five chest thrusts using two fingers on the lower sternum, alternating and checking the mouth — never perform blind finger sweeps. For a conscious child, use up to five back blows then up to five abdominal thrusts above the umbilicus. If the child becomes unconscious, begin the standard arrest algorithm. Cardiotoxic poisoning — tricyclic antidepressants, beta-blockers, calcium-channel blockers — produces wide-complex or bradycardic rhythms and is treated with sodium bicarbonate, glucagon, or specific antidotes alongside the algorithm. [1] [6]
In Australia and New Zealand, follow the ANZCOR paediatric guidelines: 15 to 2 compression-to-ventilation ratio for two or more rescuers, defibrillation at 4 joules per kilogram, and adrenaline at 10 micrograms per kilogram intravenously or intraosseously. The Advanced Paediatric Life Support course structure is the regional standard for team training.
[1][2]Complications & Pitfalls
The commonest failure in paediatric resuscitation is not a wrong dose but a wrong priority. The team that compresses before it ventilates, or that pauses compressions for a slow intubation, or that hunts for intravenous access for ten minutes before falling back on an intraosseous needle, has misread the asphyxial mechanism. Inadequate ventilation is the leading reason a child fails to recover, because the hypoxic lung is never re-oxygenated, and inadequate chest compression depth and fraction are the leading reasons the coronary perfusion never rebuilds. [1] [4]
Drug errors cluster around adrenaline and the defibrillation dose. Grabbing the 1 in 1,000 adrenaline ampoule delivers a tenfold overdose; giving adrenaline down an endotracheal tube delivers an unreliable dose that the modern guidelines no longer recommend; and a decimal slip in the millilitre calculation over- or under-doses a small child. The defibrillation dose must be four joules per kilogram, and a failure to switch on the paediatric attenuator, or to use paediatric pads, delivers an adult dose to an infant. The defence is pre-arrest preparation — pre-drawn drugs, a printed weight-based tape, and a team that rehearses. [1] [5]
Team failures are as dangerous as clinical ones. An unclear leader, two people compressing, nobody timing the cycles, and a rhythm check that nobody calls aloud all erode quality. The fix is structural: allocate roles before the arrest if possible, name a leader who does not touch the patient, call the time every two minutes, and use closed-loop communication for every drug and every shock. [1]
Prognosis & Disposition
Outcome after paediatric cardiac arrest is driven by the setting, the cause, the first rhythm, and the quality of the resuscitation. Children who arrest in hospital survive to discharge far more often than those who arrest out of hospital, and those with a shockable first rhythm generally do better than those with asystole — though shockable rhythms are less common in children. The duration of cardiopulmonary resuscitation matters: longer resuscitation is associated with lower survival and worse neurological outcome, which is why high-quality CPR and rapid reversible-cause correction are prognostic as well as therapeutic. [1] [7]
The neurological outcome is shaped by what happens in the hours after return of spontaneous circulation. The THAPCA trials showed that, in contrast to adults, routine therapeutic hypothermia did not improve overall survival with good neurological outcome in comatose children after cardiac arrest. The current standard is therefore to maintain normothermia and actively avoid fever — hyperthermia in the first twenty-four hours is associated with worse neurological injury — while individualised temperature strategies are still being studied. Normoxia and normocapnia, guided by pulse oximetry and capnography, complete the post-arrest neuroprotective bundle. [9] [10]
THAPCA-OH and THAPCA-IH (Moler 2015, 2017, NEJM)
Population: Comatose children after out-of-hospital and in-hospital cardiac arrest
Key finding
No significant difference in survival with good neurological outcome at 12 months in either trial
Practice change
Routine therapeutic hypothermia is not superior to normothermia in children after cardiac arrest; avoid hyperthermia and fever
Disposition after return of spontaneous circulation is to a paediatric intensive care unit, with attention to haemodynamic support, lung-protective ventilation, seizure surveillance with an electroencephalogram, glucose control, and the early involvement of the cardiology, neurology and toxicology teams as the cause dictates. A child who arrests out of hospital or in a smaller centre is retrieved by a paediatric retrieval team, with the airway secured and the haemodynamics supported in transit. The family is told honestly and early what happened and what the outlook is, and is offered support and follow-up. [1] [10]
Special Populations
Children with complex chronic conditions and technology dependence — home ventilators, tracheostomies, feeding tubes, congenital heart disease — arrest more often and more often in the community, and their families are usually their first responders. A rehearsed emergency tracheostomy change, a printed individualised emergency plan, and a family trained in basic life support are the difference between a recoverable event and a catastrophe. These children also arrest by a wider range of mechanisms, including equipment failure, respiratory decompensation and arrhythmia, so the team must listen to the family's account of the baseline and the change. [1] [5]
The child with single-ventricle physiology or a cardiomyopathy arrests more often by a shockable or a low-output mechanism and needs early cardiology input, careful fluid management, and a low threshold for defibrillation. The neonate in the first hours of life is managed by the neonatal life support algorithm, not the paediatric one — the distinction is ventilate first, with a 3 to 1 compression-to-ventilation ratio and 100 per cent oxygen once compressions begin. The pregnant adolescent adds the physiological changes of pregnancy and the need for left lateral uterine displacement, and is managed with the standard algorithm modified for maternal physiology. [1] [6]
In rural and remote settings the irreducible core is bystander CPR, a defibrillator, and early phone contact with a retrieval service, because the team and the equipment may be far away. Telehealth-supported resuscitation and dispatcher coaching extend the reach of the algorithm, and a generalist who can run BLS and early ALS until retrieval arrives is the pivot of the whole system. For these settings, preparation — a working defibrillator, a printed drug card, and a rehearsed team — matters more than any single dose recalled under pressure. [1] [11]
Evidence, Guidelines & Regional Differences
The current global standard rests on three pillars: the American Heart Association 2020 paediatric basic and advanced life support guideline, the European Resuscitation Council 2021 paediatric life support guideline, and the International Liaison Committee on Resuscitation 2021 consensus. The three agree on the fundamentals — the airway-breathing-compression order, the fifteen to two ratio, the four joules per kilogram defibrillation dose, the ten micrograms per kilogram adrenaline dose, and the avoidance of high-dose adrenaline. In Australia and New Zealand the ANZCOR guidelines align with these and are the regional authority. [1] [2] [3]
The focused updates of 2017 and 2018 refined two areas that examiners test heavily: compression quality and shockable-rhythm drug therapy. The 2017 basic life support update reaffirmed a rate of one hundred to one hundred and twenty per minute, a depth of one third of the chest, and minimisation of interruptions, and it accepted continuous chest-compression CPR for a lay rescuer who cannot or will not give breaths. The 2018 advanced life support update confirmed amiodarone or lidocaine for refractory ventricular fibrillation, on the basis of observational paediatric data, and refined the approach to extracorporeal CPR for selected in-hospital arrests. [4] [5]
A paediatric arrest, two minutes at a time
Where the evidence is still moving, answer with the current guideline and name the source. The role of extracorporeal membrane oxygenation CPR is growing for selected refractory in-hospital arrest in centres with the capability, though it is not yet a standard everywhere. The question of whether targeted temperature management should be individualised by arrest type is being re-examined by the ICECAP trial programme, which may refine the post-arrest temperature strategy in coming years. For now, the defensible answer in an exam and at the bedside is to maintain normothermia, avoid fever, and treat hyperoxia and hypocapnia. [1] [9]
Exam Pearls
- Most paediatric arrests are asphyxial — ventilate before you compress, and run 15 to 2, not 30 to 2, when two rescuers are present. [1]
- Defibrillate ventricular fibrillation and pulseless ventricular tachycardia at 4 joules per kilogram, biphasic. [1] [5]
- Adrenaline is 10 micrograms per kilogram intravenously or intraosseously — 0.1 mL per kilogram of the 1 in 10,000 solution — repeated every three to five minutes. [1] [12]
- High-dose adrenaline is not recommended; do not give adrenaline down the endotracheal tube. [1]
- Amiodarone 5 mg per kilogram (or lidocaine 1 mg per kilogram) after the third shock for refractory ventricular fibrillation. [1] [8]
- Compress at 100 to 120 per minute, one third of the chest depth, with full recoil and minimal interruptions; swap compressors every two minutes. [4]
- For choking: five back blows then five chest thrusts (infant) or abdominal thrusts (child); if unconscious, start the arrest algorithm. [1]
- After return of spontaneous circulation, maintain normothermia and avoid fever — the THAPCA trials did not show hypothermia superior to normothermia in children. [9] [10]
- Intraosseous access is first-line when intravenous cannulation is not immediate — place it early. [1]
- The four Hs and four Ts drive the reversible-cause search in every arrest — hold them in a mental loop and check each against the history. [1] [5]
- Capnography confirms airway placement, tracks compression quality, and a rising trace is an early sign of return of spontaneous circulation. [1]
- Bystander CPR roughly doubles or triples survival from out-of-hospital arrest — it is a public-health intervention as much as a clinical skill. [11]
References
- [1]Topjian AA Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Pediatrics, 2021.PMID 33087552
- [2]Maconochie IK European Resuscitation Council Guidelines 2021: Paediatric Life Support. Resuscitation, 2021.PMID 33773830
- [3]Olasveengen TM 2021 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation, 2022.PMID 34813356
- [4]Atkins DL 2017 American Heart Association Focused Update on Pediatric Basic Life Support and Cardiopulmonary Resuscitation Quality. Circulation, 2018.PMID 29114009
- [5]Duff JP 2018 American Heart Association Focused Update on Pediatric Advanced Life Support: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2018.PMID 30571264
- [6]Maconochie IK European Resuscitation Council Guidelines for Resuscitation 2015: Section 6. Paediatric life support. Resuscitation, 2015.PMID 26477414
- [7]Matos RI Duration of cardiopulmonary resuscitation and illness category impact survival and neurologic outcomes for in-hospital pediatric cardiac arrest. Circulation, 2013.PMID 23339874
- [8]Valdes SO Lidocaine versus amiodarone for pediatric in-hospital cardiac arrest: An observational study. Resuscitation, 2020.PMID 31954741
- [9]Moler FW Therapeutic Hypothermia in Children. N Engl J Med, 2015.PMID 26332558
- [10]Moler FW Therapeutic Hypothermia after In-Hospital Cardiac Arrest in Children. N Engl J Med, 2017.PMID 28118559
- [11]Goto Y Dispatcher-assisted conventional cardiopulmonary resuscitation and outcomes for paediatric out-of-hospital cardiac arrest. Resuscitation, 2022.PMID 34648920
- [12]Lin S Adrenaline for out-of-hospital cardiac arrest resuscitation: a systematic review and meta-analysis of randomized controlled trials. Resuscitation, 2014.PMID 24642404