Paeds · acute-care-resuscitation-and-toxicology
Paracetamol poisoning
Also known as Acetaminophen poisoning in children · Paracetamol overdose · N-acetylcysteine for paracetamol toxicity · Rumack-Matthew nomogram · Paracetamol-induced hepatotoxicity
A fellowship approach to paediatric paracetamol poisoning: take a focused time-of-ingestion history, plot a single acute ingestion on the Rumack-Matthew nomogram at four hours using the 150 mg per litre treatment line, give activated charcoal early when indicated, and start intravenous N-acetylcysteine when the level is on or above the treatment line, when the ingestion is staggered or of unknown time, or when hepatotoxicity is already present. Give NAC empirically when in doubt, watch the ALT and the coagulation trend, and escalate to a liver unit the moment King's College criteria are met.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Paracetamol (acetaminophen) poisoning is the most common paediatric poisoning presentation worldwide and remains a leading, preventable cause of acute liver failure. At therapeutic doses paracetamol is safely conjugated by the liver, but after an overdose the conjugation pathways saturate and a greater fraction is metabolised by cytochrome P450 2E1 into the reactive intermediate N-acetyl-p-benzoquinone imine (NAPQI). NAPQI is normally detoxified by glutathione, but once glutathione is depleted it binds hepatocytes and causes centrilobular necrosis. The antidote, N-acetylcysteine (NAC), works by restoring glutathione and by directly conjugating NAPQI, and it is most effective when given early. [1] [2]
The decisive clinical skill is therefore not memorising doses but taking an accurate time-of-ingestion history and using the Rumack-Matthew nomogram correctly. The nomogram relates the serum paracetamol concentration to the time after a single acute ingestion, and the treatment line decides whether NAC is indicated. It is valid only for a single acute ingestion with a known time, and only for a level drawn at four hours or later. A staggered ingestion (multiple doses over hours), an unknown-time ingestion, a repeated supratherapeutic dosing history, or a level drawn before four hours cannot be plotted on the nomogram and demand a different decision rule. [1] [4]
The modern approach treats paracetamol poisoning as a protocolised, region-dependent pathway. The treatment line, the NAC regimen and the threshold to treat staggered ingestions differ between guidelines, and the local poisons information centre or toxicology service should be consulted early. The principles, however, are universal: estimate risk from the history, measure the level at the right time, give NAC when indicated, monitor the liver and coagulation trend, and escalate when liver failure develops. [2] [4]
Classification
Paracetamol poisoning is best classified by the ingestion pattern, because the pattern decides whether the nomogram can be used and how the decision to treat is made. [1] [4]
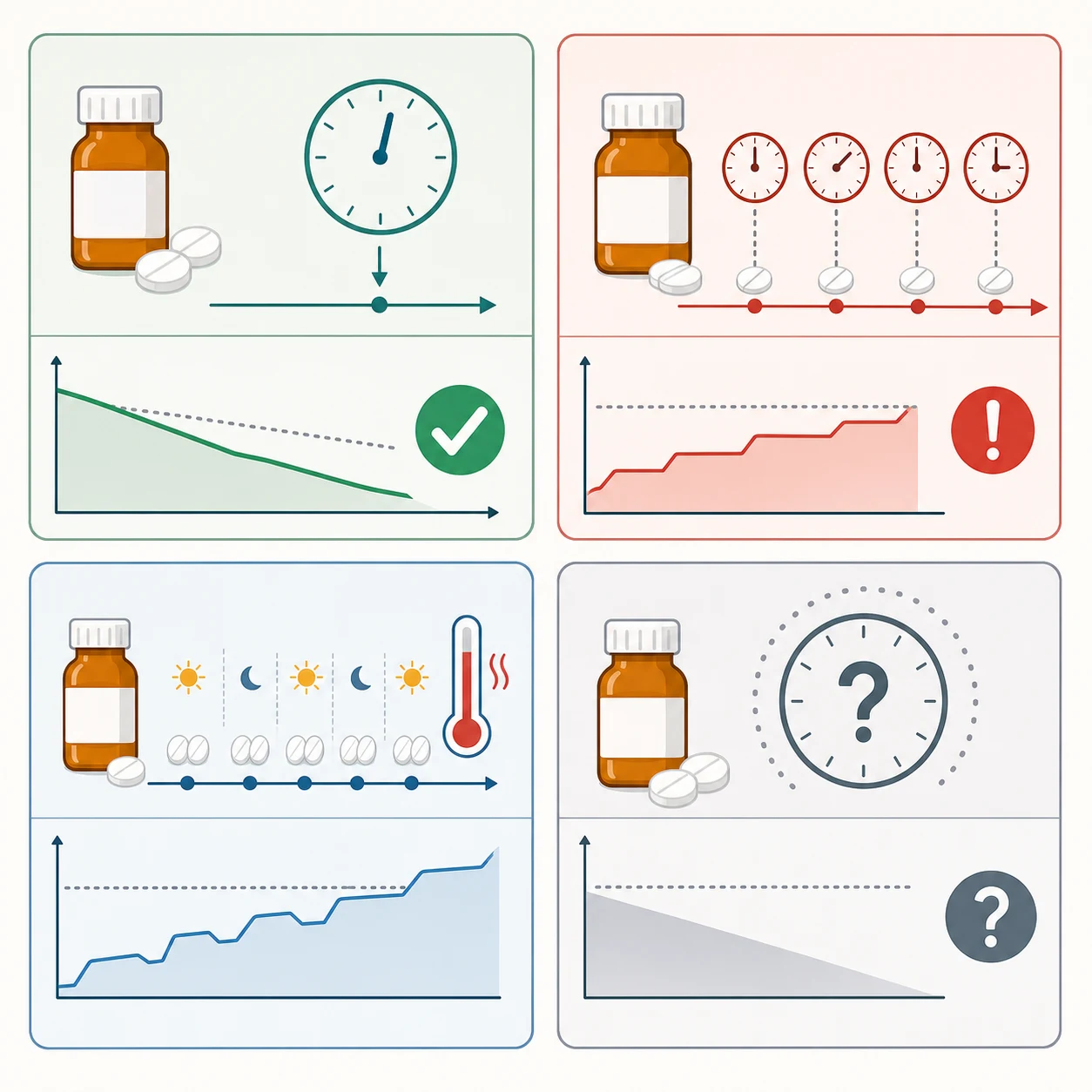
Single acute ingestion, known time
Use the nomogram
- One ingestion over less than one to two hours with a reliable time
- Plot the four-hour or later paracetamol level on the Rumack-Matthew nomogram
- Treat with NAC if the level is on or above the 150 mg per litre treatment line
- Most accurate and protocolised pathway
Staggered ingestion
Never plot on the nomogram
- Two or more doses taken over hours rather than at one time
- The nomogram is invalid and must not be used
- Treat with NAC empirically regardless of the level
- Higher risk of hepatotoxicity than a single equivalent dose
Repeated supratherapeutic dosing
Cumulative toxicity
- Multiple doses above the recommended daily maximum over days
- Common in febrile, fasting or vomiting children
- Use the repeated-supratherapeutic-dosing risk assessment, not the nomogram
- Occult paracetamol is a recognised cause of indeterminate paediatric acute liver failure
Unknown-time ingestion
Treat empirically
- Time of ingestion cannot be reliably established
- Do not plot the nomogram against an assumed time
- Measure the level and the ALT and INR, and give NAC empirically
- Stop NAC only when toxicity is excluded by a falling, normal level and normal liver function
The clinical phase adds a second axis of classification that tracks the evolution of injury. In phase one, the first twenty-four hours, the child is often asymptomatic or has nausea and vomiting. In phase two, twenty-four to seventy-two hours, right upper quadrant pain appears with a rising ALT and INR. In phase three, seventy-two to ninety-six hours, hepatotoxicity peaks and hepatic failure with encephalopathy may develop. Phase four, beyond five days, is either recovery or progression to transplant or death. Most children present in phase one, when the history and nomogram, not the symptoms, drive the decision. [1] [11]
Epidemiology & Risk Factors
Paracetamol is widely available, present in most homes, and the leading agent in paediatric poisoning presentations across Australia, the United Kingdom and North America. Intentional self-harm predominates in adolescents, while accidental exploratory ingestion and therapeutic dosing error predominate in younger children. The pattern matters because the dose, the timing and the intention change the risk of hepatotoxicity and the safeguarding response. [2] [11]
The children at highest risk of harm are those who take a large or staggered ingestion, present late, or have factors that deplete glutathione or induce cytochrome P450 2E1. Fever, fasting, dehydration, malnutrition and chronic illness all reduce the threshold at which glutathione is overwhelmed. In adolescents, deliberate self-harm ingestions are frequently large and co-ingested with other substances. In younger children, the danger is often a therapeutic error: a concentrated formulation, a repeated dose by a second carer, or an intravenous dose miscalculated by weight. [1] [12]
Ingestion factors
- Large single ingestion or staggered doses over hours
- Co-ingestion of opioids, sedatives or other substances
- Sustained-release or modified-release formulation
- Late presentation beyond the effective charcoal window
Host factors
- Fever, fasting, dehydration or malnutrition (glutathione depletion)
- Chronic illness or hepatic dysfunction
- Cytochrome P450 2E1 induction (chronic alcohol exposure in adolescents)
- Young age with a weight-based dosing error
System factors
- Unsafe home storage of liquid paracetamol concentrates
- Carer confusion between infant and older-child formulations
- Intravenous paracetamol dosing error on the ward
- Rural or remote location with delayed access to a level and toxicology advice
Children are relatively resistant to a single acute dose per kilogram compared with adults, because of greater glucuronidation capacity and a larger liver-to-body-mass ratio. This does not protect them from a large overdose, a staggered ingestion or repeated supratherapeutic dosing. Repeated dosing above the recommended daily maximum in a febrile, fasting child can cause serious hepatotoxicity without a single definable overdose, and occult paracetamol exposure is a recognised cause of indeterminate paediatric acute liver failure. [7] [8]
Pathophysiology
Paracetamol toxicity is the story of a single reactive metabolite overwhelming a finite detoxifying reserve. Understanding this pathway explains why timing matters, why NAC works, and why late presentation is dangerous. [1] [3]
At therapeutic doses, about ninety per cent of a paracetamol dose is conjugated by glucuronidation and sulfation into non-toxic metabolites, and only a small fraction is oxidised by cytochrome P450 2E1 to NAPQI. The glutathione reserve then detoxifies this NAPQI and the cell is unharmed. After an overdose the conjugation pathways saturate, a larger fraction is shunted through cytochrome P450 2E1, and NAPQI accumulates. Once hepatic glutathione falls to about thirty per cent of normal, NAPQI is no longer buffered: it binds covalently to hepatocyte proteins, particularly in the oxygen-rich centrilobular (zone three) region, and causes confluent hepatocellular necrosis. [1] [3]
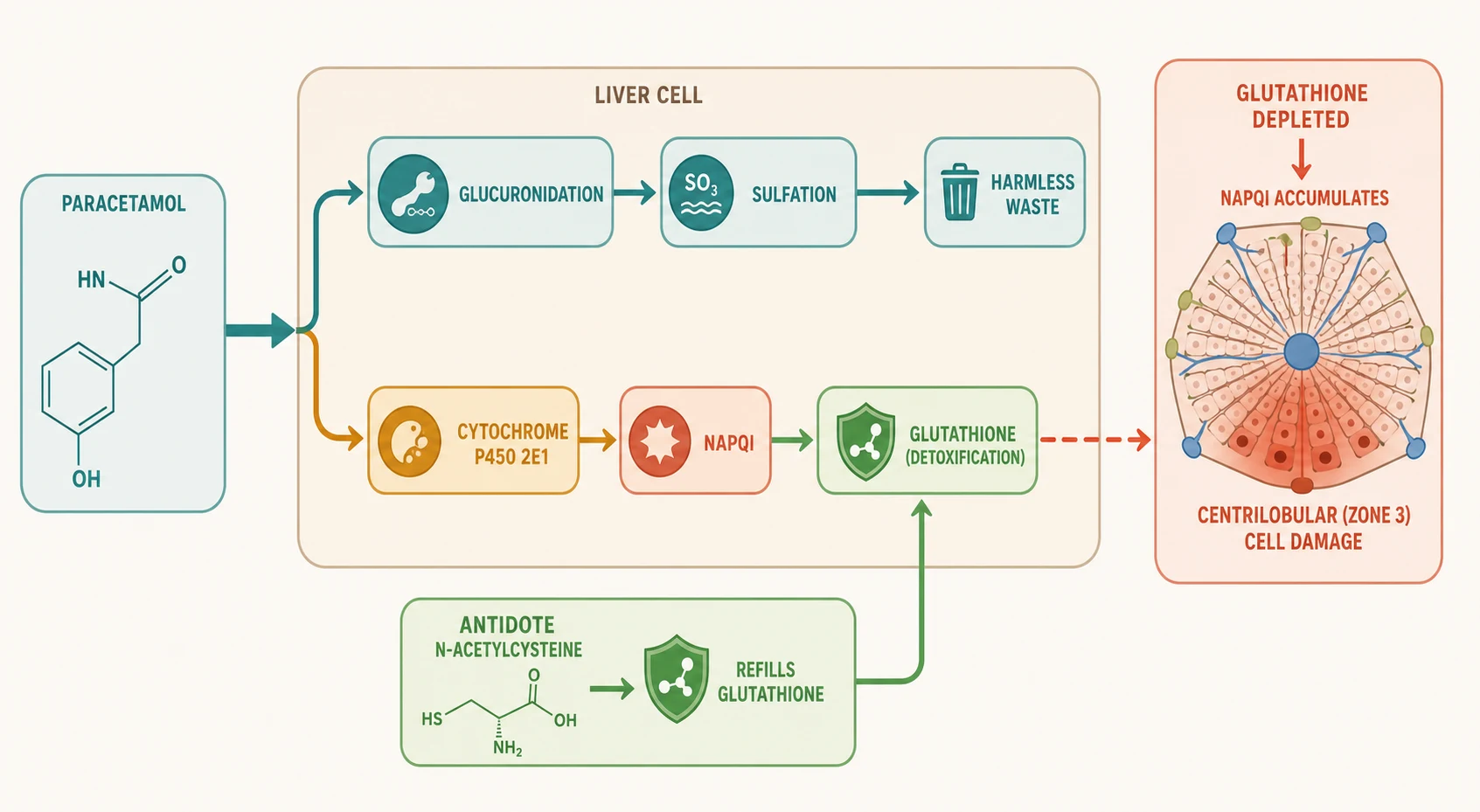
N-acetylcysteine is the antidote because it is a glutathione precursor and a sulfhydryl donor. It replenishes glutathione so that residual NAPQI can be detoxified, and it can conjugate NAPQI directly. It is most effective when given within eight hours of a single acute ingestion, when glutathione is being depleted but before binding and necrosis are established. Given later, NAC still improves outcomes even in established hepatotoxicity and acute liver failure, so a late presentation is never a reason to withhold it. [1] [4]
Why does the time-of-ingestion history matter so much? Because NAPQI production is a function of the dose and the time elapsed. The nomogram converts a single paracetamol concentration into a risk estimate by anchoring it to the time since ingestion and assuming first-order decline on a semilogarithmic scale. A concentration that is reassuring at ten hours would have been dangerous at four, and a concentration plotted against the wrong time gives a false sense of safety. This is why a reliable history, a level drawn at four hours or later, and a nomogram used only for single acute ingestions are all essential. [1] [4]
Clinical Presentation
The presentation of paracetamol poisoning is deceptively unremarkable in the early phase, and this is the trap. A child who has taken a potentially hepatotoxic dose is often completely well for the first day. Symptoms are not a reliable guide to risk; the history and the level are. [1] [11]
In the first twenty-four hours (phase one) the child may be asymptomatic or have nausea, vomiting, pallor and malaise. These early symptoms reflect the direct gastric irritant effect and the central emetic effect of paracetamol, not hepatotoxicity, and they correlate poorly with the eventual severity. In phase two, twenty-four to seventy-two hours after ingestion, right upper quadrant abdominal pain develops as the liver becomes tender, and the ALT begins to rise while the paracetamol level falls. This is the phase where a rising ALT with a normalising paracetamol level is sometimes mistaken for recovery; it is the opposite. [1] [11]
[1]In phase three, seventy-two to ninety-six hours, hepatotoxicity peaks. Jaundice, coagulopathy, hypoglycaemia and encephalopathy mark established acute liver failure. Lactic acidosis, renal failure and multi-organ dysfunction may follow. A child who reaches this phase needs a liver transplant centre, not a general ward. Phase four, beyond five days, is either recovery of hepatic regeneration or progression to death or transplant. The clinical task is to intervene in phase one so the child never reaches phase three. [8] [10]
Atypical or deceptive presentations deserve emphasis. The adolescent who has taken a large staggered ingestion for self-harm may minimise the history; the carer who gave repeated doses may not recognise it as an overdose; the young child who found a bottle may have an uncertain time of ingestion. Each removes the nomogram from the decision and demands empirical NAC. [1] [4]
Differential Diagnosis
Paracetamol poisoning is the most common cause of paediatric acute liver failure, but it is not the only one, and a child with acute liver injury needs a broad differential even when paracetamol is implicated. Build the differential by mechanism: toxin, infection, metabolic, ischaemic and structural. [8]
Other toxins and drugs
- Iron, salicylate or toxic alcohol co-ingestion
- Valproate, isoniazid or mushroom (Amanita) hepatotoxin
- Herbal, complementary or recreational substances
- Send a paracetamol level and a broad drug screen when the history is uncertain
Infective hepatitis
- Viral hepatitis A, B or E with a hepatitis pattern
- Epstein-Barr virus, cytomegalovirus or herpes simplex hepatitis
- Sepsis with hepatic dysfunction
- Fever and a hepatitis illness point here rather than to pure toxin
Metabolic and systemic
- Wilson disease presenting as acute liver failure
- Inborn errors of metabolism in the young child
- Autoimmune hepatitis
- Ischaemic hepatitis from shock or cardiac arrest
Structural
- Biliary obstruction or cholangitis
- Budd-Chiari syndrome
- Veno-occlusive disease
- Imaging and the pattern of liver enzymes help separate these
The practical point is that an elevated paracetamol-protein adduct or a clear ingestion history confirms paracetamol as the cause, but a child arriving in acute liver failure of indeterminate cause should still have paracetamol measured and an empirical NAC course considered, because occult paracetamol exposure is documented in children whose liver failure was labelled indeterminate. [7] [8]
Clinical & Bedside Assessment
Assessment begins with the airway, breathing and circulation of any poisoned child, then moves to a focused history aimed at answering one question: is this a single acute ingestion with a known time, or not? The answer decides everything that follows. [1] [4]
Establish the preparation and formulation of paracetamol (immediate-release liquid or tablet, or modified-release), the amount taken, the time of ingestion as precisely as possible, and whether more than one dose was taken over a period. Ask about co-ingestants, intent, underlying illness, fasting and fever, and any treatment already given. In an adolescent, take the self-harm history privately and sensitively; in a younger child, clarify the formulation strength because infant and older-child liquids differ in concentration tenfold. Document the time you were told and the source of the history, because the nomogram is only as reliable as the time. [1] [11]
[1]Examine for the clinical phases. In phase one the child is often well; abdominal tenderness, pallor or vomiting may be present but are non-specific. In phases two and three look for right upper quadrant tenderness, jaundice, bruising (coagulopathy), drowsiness (encephalopathy), and signs of dehydration or multi-organ involvement. A declining conscious level, a metabolic acidosis or bleeding demand immediate escalation. Repeat the focused examination through the admission, because the trajectory of signs tracks the trajectory of injury. [1] [10]
A collateral history from carers, ambulance staff and the home setting is often decisive, especially in the young child or the adolescent who is withholding information. Confirm the bottle, the formulation and the missing volume where possible. Use a professional interpreter whenever needed. Safeguarding assessment runs in parallel, because accidental access to unsafe storage, therapeutic error and intentional self-harm each carry a different safety response. [11] [12]
Investigations
Investigations answer three questions: what is the paracetamol concentration at the right time, is there hepatotoxicity already, and is there a co-ingestant or complication. Order each test for a named question and time the paracetamol level correctly. [1] [4]
Immediate and bedside
- Paracetamol level at four hours after a single acute ingestion (repeat if before four hours)
- Point-of-care glucose: hypoglycaemia marks established liver failure
- Blood gas and lactate: a metabolic acidosis signals severe toxicity
- Pregnancy test in adolescent females
Core laboratory
- ALT or AST, INR and prothrombin time tracked serially through the course
- Renal function, electrolytes, venous bicarbonate and creatinine
- Lipase if abdominal pain is prominent
- Drug screen and salicylate level when co-ingestion is suspected
Advanced and targeted
- Arterial blood gas and lactate in established toxicity for King's College criteria
- Paracetamol-protein adducts when the cause of liver failure is indeterminate
- Hepatitis serology, copper and autoimmune markers in the broad differential
- Liver ultrasound when a structural cause is considered
Interpret the paracetamol level against the ingestion pattern, not in isolation. For a single acute ingestion with a known time, plot the level at four hours or later on the Rumack-Matthew nomogram using the 150 mg per litre treatment line. A level drawn before four hours cannot be interpreted and must be repeated at four hours. For a staggered, repeated-supratherapeutic or unknown-time ingestion, do not plot the nomogram; use the level alongside the ALT and INR to guide empirical treatment. [1] [4]
[1]Track the ALT and the INR as the markers of evolving hepatotoxicity. A rising ALT and a rising INR with a falling paracetamol level means established injury. The prothrombin time is the single most important prognostic marker in paracetamol-induced liver failure, and a serial prothrombin time that continues to rise after the peak of injury is an ominous sign. [10]
Management — Resuscitation
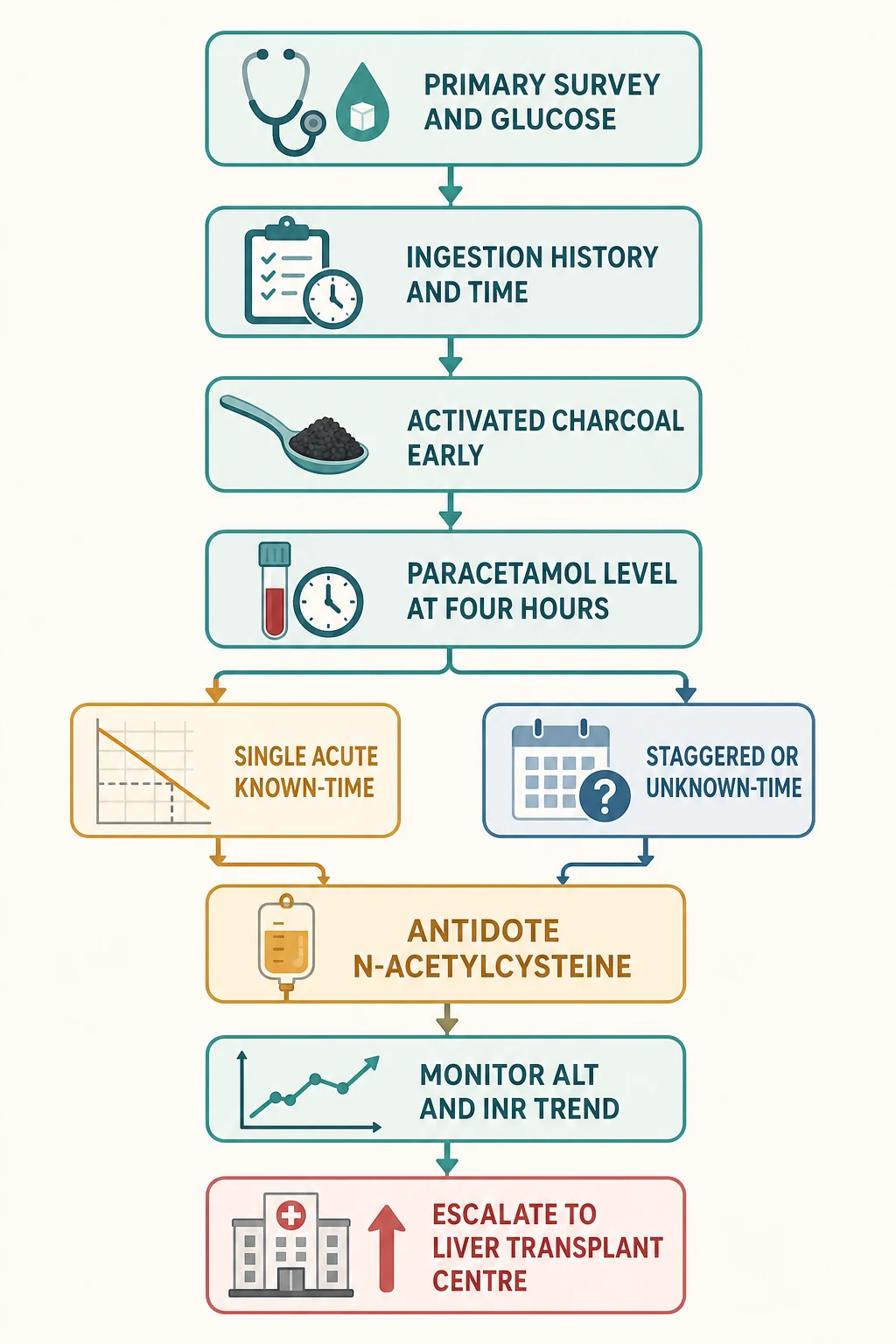
Resuscitation follows the standard poisoned-patient primary survey, then moves quickly to paracetamol-specific decontamination and antidote decisions. The first hour focuses on airway, breathing, circulation, glucose and taking the ingestion history that will drive the nomogram. [1] [4]
The first hours in paracetamol poisoning
Primary survey and glucose
Secure airway, breathing and circulation as for any poisoned child. Check bedside glucose immediately and correct a dangerous low. Take a precise ingestion history with the time, formulation, amount and co-ingestants.
Activated charcoal if indicated
Give activated charcoal at 1 gram per kilogram (maximum 50 grams) by mouth within one hour of a significant ingestion. Consider it up to two to four hours for large or modified-release ingestions, weighing benefit against vomiting and airway risk.
Time the paracetamol level
For a single acute ingestion, draw the paracetamol level at four hours or later and plot it on the Rumack-Matthew nomogram using the 150 mg per litre treatment line. Do not interpret a level drawn before four hours.
Decide on N-acetylcysteine
Start intravenous N-acetylcysteine if the level is on or above the treatment line, if the ingestion is staggered or of unknown time, if repeated supratherapeutic dosing caused toxicity, or if hepatotoxicity is already present. Give it empirically when in doubt.
Give the NAC regimen
Use the standard intravenous regimen: 150 mg per kilogram over one hour, then 50 mg per kilogram over four hours, then 100 mg per kilogram over sixteen hours, total 300 mg per kilogram over twenty-one hours, per the local protocol.
Monitor the trend and escalate
Track ALT and INR through the course. Escalate to a liver transplant centre when King's College criteria are met: arterial pH below 7.3 after resuscitation, or all three of INR above 6.5, creatinine above 300 micromol per litre and grade three to four encephalopathy.
Call the poisons centre
Contact the local poisons information centre or toxicology service early. The treatment line, NAC regimen and staggered-ingestion rules are region-specific and protocol-dependent.
Decontamination: activated charcoal
Activated charcoal reduces paracetamol absorption when it reaches the gut before absorption is complete. Its effect is greatest within one hour of ingestion, and it can be considered up to two to four hours for large or modified-release ingestions. Give 1 gram per kilogram (maximum 50 grams) orally or via nasogastric tube, weighing the benefit against the risk of vomiting and aspiration, particularly in a drowsy or seizing child. Charcoal does not replace the nomogram decision; it is an adjunct that precedes it. [1] [4]
When ABCDE becomes advanced life support
A child who becomes comatose, has a severe metabolic acidosis, develops encephalopathy with bleeding, or loses the airway needs immediate resuscitation and intensive care. The paediatric arrest-dose anchors from the resuscitation sources apply if the child arrests: intravenous or intraosseous adrenaline at 10 micrograms per kilogram (0.1 mL per kilogram of 1 in 10,000 adrenaline) every three to five minutes, and defibrillation at 4 joules per kilogram for a shockable rhythm. The full algorithm lives in the paediatric basic and advanced life support topic. [1]
[8] [10]Management — Definitive & Stepwise
Once the primary survey and decontamination are done, definitive management is the antidote decision, the NAC course, the monitoring of hepatotoxicity, and the escalation to transplant when criteria are met. This is the phase where the trend, not the snapshot, drives decisions. [1] [4]
The N-acetylcysteine regimen
The standard intravenous NAC regimen is 150 mg per kilogram over one hour, then 50 mg per kilogram over four hours, then 100 mg per kilogram over sixteen hours, giving a total of 300 mg per kilogram over twenty-one hours. This is the widely used three-bag regimen. Variants exist: the two-bag regimen simplifies the course, and high-dose or extended regimens are used in some centres for large or high-risk ingestions. Confirm the exact regimen with the local poisons information centre or toxicology service, because it is region-specific. [1] [5]
| Phase | Dose | Duration | Purpose |
|---|---|---|---|
| Loading | 150 mg per kg | Over 1 hour | Rapidly restore glutathione and conjugate NAPQI |
| Second bag | 50 mg per kg | Over 4 hours | Maintain NAC delivery during ongoing metabolism |
| Third bag | 100 mg per kg | Over 16 hours | Cover the full window of NAPQI production and binding |
| Total | 300 mg per kg | Over 21 hours | Complete standard course; extend if hepatotoxicity persists |
Intravenous N-acetylcysteine (standard regimen)
NAC is most effective when given within eight hours of a single acute ingestion. After eight hours its protective effect falls, but it continues to improve outcome even in established hepatotoxicity and acute liver failure, so a late presentation is never a reason to withhold it. At the end of the standard course, the decision to stop or extend depends on the trend of ALT and INR and the paracetamol level: if hepatotoxicity is ongoing, extend the NAC until the liver recovers or transplant is arranged. [1] [6]
Managing anaphylactoid reactions to NAC
Anaphylactoid (non-IgE) reactions to NAC are common during the loading dose and are driven by high peak NAC concentrations. They present with flushing, rash, nausea, itching and occasionally bronchospasm or hypotension. The usual response is to slow or briefly pause the infusion and give an antihistamine, then resume. Pretreatment with an antihistamine reduces the reaction rate, and two-bag and modified regimens that lower the loading peak also reduce reactions. A reaction is not a reason to abandon the antidote. [9]
Two-bag NAC regimen and anaphylactoid reactions
Clinical Toxicology
Observational study of intravenous N-acetylcysteine reactions
Key finding
A two-bag NAC regimen, antihistamine pretreatment and high presenting paracetamol levels were associated with a lower incidence of anaphylactoid reactions to N-acetylcysteine.
Practice change
Modified regimens and antihistamine pretreatment are reasonable where local protocols support them, but the standard three-bag regimen remains widely used. Confirm the local regimen with the poisons service.
High-risk and large ingestions
For large single ingestions, sustained-release formulations, or presentations with high presenting paracetamol concentrations, the standard course may be inadequate. Recent cohort and pharmacokinetic work supports higher-dose or extended NAC delivery in high-risk ingestions treated within eight hours, because these children clear paracetamol more slowly and the standard regimen can leave them under-treated. The exact threshold and regimen are protocol-dependent; involve the toxicology service early. [5] [6]
Goals and monitoring
Set explicit endpoints and watch the trend. The targets during and after the NAC course are a falling and normalising ALT, a stable or falling INR, a normal glucose, an improving acid-base balance, and a normal conscious level. The paracetamol level itself becomes uninformative once the nomogram phase is past; the ALT, INR and clinical state are the markers of recovery or deterioration. Continue monitoring in a setting matched to severity, from the ward for the well child to intensive care for established liver failure. [1] [10]
Specific Subtypes & Scenarios
The resuscitation and antidote structure stays the same, but the ingestion pattern, the age and the setting change the decision rule, the formulation risk and the safeguarding response. [1]
Single acute ingestion, known time
- Plot the four-hour level on the Rumack-Matthew nomogram
- Treat with NAC on or above the 150 mg per litre line
- Charcoal within one hour if a significant ingestion
- Most accurate and protocolised pathway
Staggered or repeated dosing
- Never plot on the nomogram
- Treat empirically with NAC
- Use the repeated-supratherapeutic risk assessment
- Higher risk of hepatotoxicity; monitor ALT and INR closely
Unknown-time ingestion
- Do not plot the nomogram against an assumed time
- Measure level, ALT and INR; treat empirically
- Stop NAC only when toxicity is excluded
- Involve the poisons centre to confirm the stopping rule
Adolescent self-harm ingestion
- Often large, staggered and co-ingested
- Take the history privately and sensitively
- Mental health and safeguarding assessment in parallel
- Do not rely on the history alone for the time and amount
Therapeutic and medication error
- Concentrated formulation or weight-based miscalculation
- Intravenous paracetamol dosing error on the ward
- Repeated dosing in a febrile, fasting child
- Apply the repeated-supratherapeutic risk pathway
Modified-release ingestion
- Absorption is prolonged and levels may peak late
- Draw levels at four hours and again at four-hourly intervals
- Treat if any level is above the line or if levels are rising
- Extended NAC and prolonged monitoring are often required
Modified-release formulations deserve particular caution. Because absorption is prolonged, a single four-hour level may underestimate the eventual peak, and concentrations can continue to rise. Draw levels at four hours and repeat at four-hourly intervals to detect a rising trend, and treat or extend NAC if any level is on or above the line or if levels are climbing. This is one situation where the nomogram must be used alongside a second level, not a single one. [1] [4]
Complications & Pitfalls
Most preventable harm in paediatric paracetamol poisoning comes from one of five errors: plotting a level before four hours, plotting a staggered or unknown-time ingestion on the nomogram, delaying NAC after the treatment line is crossed, stopping NAC too early, and failing to escalate when liver failure develops. Each is a failure of the ingestion history and the trend, not of memory. [1] [4]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Plotting a level before four hours | Absorption is ongoing and the level underestimates risk | Repeat the level at four hours or later before plotting |
| Plotting a staggered or unknown-time ingestion | The nomogram is invalid and gives a false reading | Do not plot; treat empirically with NAC |
| Delaying NAC after the treatment line | Glutathione depletion proceeds and NAPQI binds hepatocytes | Start NAC immediately on or above the line; never wait for symptoms |
| Stopping NAC too early | Ongoing hepatotoxicity is left untreated | Extend until ALT and INR are falling and the liver is recovering |
| Missing a modified-release formulation | A single four-hour level underestimates the late peak | Repeat levels at four-hourly intervals; treat if any level is above the line |
| Abandoning NAC after a reaction | An anaphylactoid reaction is mistaken for true allergy | Slow or pause, give an antihistamine, and resume; reactions are rate-related |
| Failing to escalate in liver failure | A transplantable child stays on a general ward | Apply King's College criteria and contact the liver transplant centre |
| Forgetting the safeguarding and mental health response | The cause of the poisoning is left unaddressed | Assess self-harm, storage safety and medication error in parallel |
After the acute course, watch for harm from the injury itself and from the treatment: hepatic encephalopathy, coagulopathy with bleeding, hypoglycaemia, renal failure, lactic acidosis, and, less often, NAC reactions or line complications. A child who survives the acute injury still needs follow-up of liver function and, in the case of self-harm, ongoing mental health care. [8] [10]
[1] [10]Prognosis & Disposition
Disposition follows the ingestion pattern, the level, the trend of ALT and INR, and the social and safeguarding context. Most children with a single acute ingestion treated early do well; the children who do badly are those who present late, take large or staggered ingestions, or develop established liver failure. [1] [11]
Intensive care or liver transplant centre
- Established hepatotoxicity with rising INR and encephalopathy
- King's College criteria met: pH below 7.3, or INR above 6.5 with renal failure and grade three to four encephalopathy
- Multi-organ failure, acidosis or renal failure
- Large or modified-release ingestion with a rising level despite NAC
Ward observation
- On NAC with stable or mildly abnormal liver function
- Monitoring the ALT and INR trend after a significant ingestion
- Awaiting the four-hour level after a known-time ingestion
- Co-existing medical or psychiatric concerns needing observation
Medical clearance and discharge
- Level below the treatment line for a single acute ingestion with normal liver function
- Completed NAC course with falling ALT and stable INR
- No co-ingestant toxicity and no safeguarding or mental health concern
- Carer and adolescent understand the safety-net advice and follow-up
Mortality from paracetamol poisoning is low when NAC is given early, but it remains a leading cause of paediatric acute liver failure and of transplant for liver failure, particularly among adolescents who take large staggered ingestions. The single most important prognostic marker is the prothrombin time trend: a prothrombin time that continues to rise after the peak of injury predicts a poor outcome. Give every family a clear safety net: what change to watch for, how urgently to act, and exactly where to return. [8] [10]
Special Populations
Adapt how you take the history, how you dose and how you escalate, but never lower the standard for identifying hepatotoxicity. The principles apply across ages and abilities; the differences are in reserve, communication, formulation risk and the social context. [1]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Young infant | Weight-based dosing error risk is high; check formulation strength; treat any significant exposure seriously | Confirm infant versus older-child liquid concentration before dosing or estimating |
| Adolescent | Large staggered self-harm ingestion is common; take the history privately and sensitively; mental health and safeguarding in parallel | Do not rely on the adolescent's reported time and amount alone |
| Febrile, fasting or malnourished child | Glutathione depletion lowers the toxic threshold; repeated dosing can cause toxicity without a single overdose | Use the repeated-suptherapeutic risk pathway, not the nomogram |
| Chronic illness or hepatic disease | Reserve is reduced and baseline liver function altered; lower the threshold to treat | Confirm the baseline ALT and INR before attributing a rise to paracetamol alone |
| Disability or neurodiversity | Compare with the caregiver's baseline; use adapted communication; explore accidental access | A changed behaviour or feeding pattern may be the only sign |
| Indigenous, migrant or refugee | Use professional interpreters; respect cultural and family structures; address access and storage barriers | Apply local consent and mandatory-reporting rules |
Safeguarding runs in parallel with medical care, and immediate stabilisation comes first. Accidental access to unsafe storage, a therapeutic dosing error by a carer, an intravenous medication error on the ward, and intentional self-harm each carry a different safety response. Ask only necessary open, non-leading questions, document objective findings and spontaneous words, and use the local safeguarding and mental health pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [11] [12]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The structure of management — a precise ingestion history, a paracetamol level at four hours for a single acute ingestion plotted on the Rumack-Matthew nomogram, activated charcoal when it can reach the gut, NAC on or above the treatment line, and empirical NAC for staggered or unknown-time ingestions — is strongly endorsed across the major toxicology sources. What remains region-specific is the treatment line, the NAC regimen, and the exact rule for staggered and repeated-suptherapeutic ingestions. [1] [4]
Rumack-Matthew nomogram and NAC
Journal of Toxicology. Clinical Toxicology
Landmark synthesis of the nomogram-based risk assessment and NAC treatment of acetaminophen poisoning
Key finding
The nomogram relating the serum paracetamol concentration to the time after a single acute ingestion, with a treatment line for NAC, transformed acetaminophen poisoning from a leading cause of fatal poisoning into a largely preventable cause of liver failure when treated early.
Practice change
The nomogram remains the international standard for single acute ingestions with a known time; it must not be used for staggered or unknown-time ingestions.
The nomogram's treatment line has itself evolved. The original line corresponded to a 150 mg per litre concentration at four hours in many international pathways, while the United Kingdom adopted a single 100 mg per litre treatment line to increase sensitivity at the cost of more NAC use. The principle is the same: a level at or above the line warrants NAC. Confirm the active line with the local poisons information centre before deciding. [2] [4]
On the NAC regimen, evidence supports both the standard three-bag regimen and modified two-bag and high-dose approaches. Cohort work in high-risk ingestions treated within eight hours suggests that the standard regimen can under-treat children who clear paracetamol slowly, supporting higher-dose or extended delivery in selected cases. The two-bag regimen and antihistamine pretreatment reduce anaphylactoid reactions. None of this displaces the standard regimen as the default; it refines it for high-risk groups. [5] [6]
On late and staggered presentations, the evidence is clear: NAC improves outcome even when given late and even in established acute liver failure, so a late or staggered ingestion is never a reason to withhold it. The repeated-suptherapeutic and staggered-ingestion pathways, which do not use the nomogram, are endorsed by the major toxicology guidelines. [2] [6]
Jurisdictional implementation
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne paracetamol poisoning guideline and the Australian Therapeutic Guidelines (eTG) set the local pathway. The NSW Poisons Information Centre (13 11 26) should be called early; the New Zealand equivalent is the National Poisons Centre (0800 POISON). The treatment line, NAC regimen and staggered-ingestion rules follow the local protocol; verify them rather than borrowing an international threshold.
Exam Pearls
Recognition
- The history and the level, not the early symptoms, drive risk
- Nomogram valid only for a single acute ingestion with a known time
- A level must be drawn at four hours or later to be interpretable
- Staggered, unknown-time and repeated-suptherapeutic ingestions are never plotted
Decision
- Treat with NAC on or above the 150 mg per litre treatment line
- Treat empirically for staggered, unknown-time or repeated-suptherapeutic toxicity
- Charcoal within one hour of a significant ingestion (1 g per kg, max 50 g)
- Give NAC empirically when in doubt
NAC regimen
- 150 mg per kg over 1 hour, then 50 mg per kg over 4 hours, then 100 mg per kg over 16 hours
- Total 300 mg per kg over 21 hours; extend if hepatotoxicity persists
- Most effective within 8 hours; still useful when given late
- Manage anaphylactoid reactions by slowing and giving an antihistamine, not by abandoning the antidote
Monitoring and escalation
- Track ALT and INR through the course
- Prothrombin time trend is the key prognostic marker
- King's College: arterial pH below 7.3, or all three of INR above 6.5, creatinine above 300 micromol per litre, grade three to four encephalopathy
- Contact the liver transplant centre when criteria are met
Pitfalls
- No level-before-four-hours plotting
- No staggered or unknown-time plotting
- No delayed or stopped-too-early NAC
- No reassurance from a falling paracetamol level while ALT and INR rise
- No keeping a King's College child on a general ward
“Take the ingestion history and time → charcoal within one hour if indicated → four-hour level on the nomogram for a single acute ingestion, or empirical NAC for staggered, unknown-time or repeated-suptherapeutic ingestion → NAC 150 then 50 then 100 mg per kg over 21 hours → track ALT and INR → escalate to a liver transplant centre when King's College criteria appear.”
Viva: why is the nomogram valid only for a single acute ingestion with a known time?
The nomogram assumes a single ingestion at one known moment and first-order elimination of paracetamol on a semilogarithmic scale. It converts one concentration into a risk estimate by anchoring it to the time since that single ingestion. A staggered ingestion violates the single-time assumption, a repeated-suptherapeutic history violates the single-dose assumption, and an unknown time makes the anchor meaningless. Each removes the nomogram from the decision and demands empirical treatment.
Viva: what are the King's College criteria and why do they matter?
For paracetamol-induced acute liver failure, the King's College criteria are an arterial pH below 7.3 after adequate fluid resuscitation, regardless of the grade of encephalopathy, or the combination of all three of an INR above 6.5 (prothrombin time above 100 seconds), a creatinine above 300 micromol per litre, and grade three to four encephalopathy. Meeting the criteria predicts a poor outcome without transplant and is the trigger to contact the liver transplant centre immediately, before the full NAC course finishes.
Structured oral: a staggered ingestion in an adolescent
Do not plot the nomogram. Take the history privately and sensitively, including co-ingestants and intent. Draw a paracetamol level, ALT and INR, and start intravenous N-acetylcysteine empirically on the standard regimen. Watch the ALT and INR trend. Begin the mental health and safeguarding assessment in parallel. Escalate to the liver transplant centre if King's College criteria appear. Continue NAC until the liver is recovering and the level is negligible.
References
- [1]Rumack, Barry H Acetaminophen hepatotoxicity: the first 35 years Journal of toxicology. Clinical toxicology, 2002.PMID 11990202
- [2]Bateman, D Nicholas Fifty years of paracetamol (acetaminophen) poisoning: the development of risk assessment and treatment 1973-2023 with particular focus on contributions published from Edinburgh and Denver Clinical toxicology (Philadelphia, Pa.), 2023.PMID 38197864
- [3]Prescott, L F Paracetamol (acetaminophen) poisoning: The early years British journal of clinical pharmacology, 2024.PMID 37683599
- [4]Sivilotti, Marshall L A Treating acetaminophen overdose CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne, 2022.PMID 35440504
- [5]Watson, Connor J N-Acetylcysteine Dose and Treatment Duration in High-Risk Acetaminophen Ingestions Treated Within Eight Hours: A Retrospective Cohort Study Journal of medical toxicology : official journal of the American College of Medical Toxicology, 2026.PMID 41857443
- [6]Moss, Mark J Assessment of high-dose acetylcysteine in acute high-risk paracetamol (acetaminophen) ingestion Clinical toxicology (Philadelphia, Pa.), 2024.PMID 39051728
- [7]James, Laura P Detection of acetaminophen protein adducts in children with acute liver failure of indeterminate cause Pediatrics, 2006.PMID 16950959
- [8]Squires, Robert H Jr Acute liver failure in children: the first 348 patients in the pediatric acute liver failure study group The Journal of pediatrics, 2006.PMID 16737880
- [9]Daoud, Ahmed Two-bag intravenous N-acetylcysteine, antihistamine pretreatment and high plasma paracetamol levels are associated with a lower incidence of anaphylactoid reactions to N-acetylcysteine Clinical toxicology (Philadelphia, Pa.), 2020.PMID 31601129
- [10]Harrison, Philip M Serial prothrombin time as prognostic indicator in paracetamol induced fulminant hepatic failure BMJ (Clinical research ed.), 1990.PMID 2249026
- [11]Karabacak, Busra Clinical characteristics and outcomes of pediatric paracetamol poisoning presenting to the emergency department BMC pediatrics, 2026.PMID 41998668
- [12]Vincent, F Medication errors involving intravenous paracetamol in children: experience from enquiries to the National Poisons Information Service Archives of disease in childhood, 2024.PMID 38233098